
Abstract
Introduction
In the U.S., over half (51%) of people living with HIV (PLWH) are 50 years of age or older and this percentage should increase to 70% by 2030.1,2 To better understand the needs of this growing population, a registry and online community, called Aging with Dignity, Health, Optimism and Community (ADHOC), was launched in October 2017. ADHOC is an observational, prospective, longitudinal cohort study that utilizes an online questionnaire to capture the ageing experiences of older (≥50 years) PLWH who receive care at ten HIV clinics across the U.S.
Data collected from 1047 ADHOC participants (older PLWH) prior to the COVID-19 pandemic demonstrated that loneliness was prevalent in 50.6% of the population, symptoms of depression in 20.8%, and symptoms of anxiety in 20.7%. 3 Other studies conducted prior to the pandemic also showed that the prevalence of depression and anxiety symptoms were significantly higher among older PLWH than among HIV-negative, age-matched counterparts.4–6 Since the start of the pandemic, several studies in PLWH have documented the pandemic’s adverse mental health impact, including exacerbated depression, 7 anxiety,7,8 and loneliness. 9
To help address the mental health problems faced by older PLWH, it is important to evaluate interventions that can be disseminated widely. Previous studies have demonstrated that a series of brief, online audio mindfulness lessons improved symptoms of depression, symptoms of anxiety, and loneliness in a general US adult population with elevated stress levels.10,11 The present waitlist-controlled trial was conducted to evaluate the effectiveness of these online audio mindfulness lessons in older PLWH.
Methods
Participants
To be eligible for ADHOC, participants must have had an HIV infection and been at least 50 years of age at enrolment. ADHOC participants were primarily identified during visits to participating clinical practices in California, Washington DC, Florida, Illinois, North Carolina, Texas, Washington State, and Wisconsin.
All ADHOC participants with a 3-Item Loneliness score ≥4 (N = 683), indicating at least a minor degree of self-reported loneliness, were eligible to participate (Figure 1). Eligible participants were contacted between May 18 and June 12, 2020 and told that they could enrol in a study “designed to examine the impact of online mindfulness lessons on the well-being of people living with HIV.” Recruitment concluded when the goal of enrolling 225 participants was reached.

Participant flow in the study.
Trial design, setting, and procedures
This was a multi-site, parallel-group, waitlist-controlled trial, conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines. Both the study protocol and informed consent were approved by Ethical and Independent Review Services. Written informed consent was collected from all participants. The study is registered with ClinicalTrials.gov (Identifier: NCT04580082). All study activities, including registration and informed consent, were completed online.
At baseline (Figure 1), all participants completed a series of questionnaires designed to assess symptoms of depression, anxiety, loneliness, and social isolation. Participants who completed all the baseline questionnaires (N = 214) were then assigned to either the intervention or the waitlist control group. While the study was not initially intended to evaluate this intervention during the COVID-19 pandemic, this occurred coincidentally due to the timing of the study rollout. The first person who completed the baseline questionnaire at a given site was randomly assigned to either the intervention or control group. The next patient at that site was assigned to the opposite group, and so on. This alternating sequence was used because social distancing regulations were changing very frequently in response to the pandemic, so it was important for patients in the intervention and control groups to be paired temporally as closely as possible. Doing so prevented a possible situation that could arise if patients were randomly allocated to the intervention and control groups in a pattern where, for example, a larger number of patients were assigned to the intervention group at an earlier point in time when local COVID regulations were a certain way, and subsequent patients were assigned primarily to the waitlist group when regulations had changed.
It was also important to assign patients to the intervention and control groups at the site level because, at the time participants were assigned (June 2020), states and counties had very different COVID-related rules regarding social distancing, business lockdowns, etc. Balancing the number of patients in the intervention and control groups at each locale ensured that those patients were facing a similar set of COVID guidelines. If treatment arm assignments were not balanced at the site level, differences in the macro environment could influence the results of the study. For example, if Texas had relatively lax social distancing guidelines and more participants from Texas were randomly assigned to the control arm, while California had very restrictive social distancing guidelines and more participants from California were assigned to the intervention arm, these environmental differences could have influenced the outcomes of the study.
Measures
Information on sociodemographic characteristics and co-morbid conditions were obtained using ADHOC registry data. For the current study, symptoms of depression were measured using the 10-item Center for Epidemiologic Studies scale (CES-D-10), which ranges from 0 to 30, with higher scores indicating greater symptoms of depression.“Depression” at baseline was defined as a CES-D-10 score ≥8. 12 Symptoms of anxiety were measured using the Generalized Anxiety Disorders scale (GAD-7), which ranges from 0 to 21, with higher scores indicating greater symptoms of anxiety. “Anxiety” at baseline was defined as a GAD-7 score ≥5. 13
Loneliness was measured two ways: the 3-item Loneliness scale (3IL) and a Daily Diary. The Daily Diary was filled out once per day for 3 days and asked participants, “How lonely did you feel today?” on a 1–7 scale, with higher scores indicating more loneliness. 11 The results for each patient were averaged across the 3 days. The Diary was used to assess loneliness on a daily basis, while the 3IL scale assessed loneliness over the previous 2 weeks.
For the purposes of secondary analyses, “lonely” at baseline was defined as a score of 6 or greater (i.e. moderate or greater) on the 3IL. 14
Intervention
The intervention consisted of 14 mindfulness audio lessons. Each lesson was approximately 20 min long and could be listened to via a downloadable app or with any internet-connected device (e.g. smartphone, tablet, laptop, or desktop). Lessons had to be listened to in sequential order, and could not be skipped or fast-forwarded, but participants could revisit previously completed lessons.
The mindfulness lessons were designed to develop three core skills: concentration (the ability to maintain focus on present-moment experiences), clarity (the ability to pinpoint exactly what you are experiencing in each moment), and equanimity (openness to experience). 11 Details regarding the development and theoretical framework behind the mindfulness lessons can be found in the Supplementary Materials associated with Lindsay et al. 10
Participants in the intervention group had access to 14 mindfulness audio lessons over 25 days. Participants could listen to only one lesson per day, unless they fell behind, in which case they could listen to one lesson every 4 hours until they caught up. Following that 25-day intervention period, access to the mindfulness lessons was blocked, and all participants were again given up to 14 days to complete the same set of questionnaires that they completed at baseline. After those 14 days, the waitlist control group had access to the audio lessons for the subsequent 25 days. Participants from both the intervention and waitlist control groups who completed all the baseline and follow-up questionnaires received a gift card.
Primary analyses examined symptoms of depression, symptoms of anxiety, and loneliness among all participants. Secondary analyses examined participants who, at baseline, had depressive symptoms; anxiety symptoms; or at least moderately loneliness. These populations were selected because they were the most likely to benefit from mindfulness activities. Exploratory analyses were conducted among subpopulations of participants who had an annual household income of less than $50,000 per year; participants who were Hispanic, Black, or female, because these populations are often marginalized in the HIV community; 15 and participants with comorbidities associated with poor outcomes after COVID-19 infection, specifically among patients with obesity, diabetes, or chronic obstructive pulmonary disease (COPD). 16 These analyses were exploratory because the study was not powered to detect significant differences in subgroups of these sizes.
Statistical analyses and power calculation
Power calculations, which accounted for the clustered design of the study, showed that at least 70 participants would have to complete all study activities in order to detect significant differences in loneliness, assuming effect sizes similar to those seen in previous research using the same mindfulness lessons.10,11 Since the study had a larger number than this in each group, the sample size used was adequate, taking into account the clustered design of the study. Loneliness, rather than symptoms of depression or anxiety, was selected for the power calculation because it was assumed that social distancing regulations might overwhelm the impact of online mindfulness lessons, and that loneliness might therefore be the least amenable to change. A 60% attrition rate was anticipated, given the length of the study and the possible lack of tech-savviness in an older population, so a total of 225 participants were enrolled.
Following assignment to the two groups, the intervention and control arms were compared on demographic and clinical characteristics using chi-squared or t tests, as appropriate. Two-way ANOVA was used at follow-up to determine between-group differences in mean loneliness, symptoms of depression, and symptoms of anxiety. The ANOVA included a term for study site because of how participants were assigned to each arm of the study. When evaluating loneliness, all individuals with loneliness were included, regardless of whether they also had symptoms of depression or anxiety. Similarly, when evaluating symptoms of depression, all individuals with symptoms of depression were included, regardless of whether they also had symptoms of anxiety or loneliness. Finally, when evaluating symptoms of anxiety, all individuals with symptoms of anxiety were included, regardless of whether they also had symptoms of depression or loneliness. Effect size was estimated using Hedge’s g. 17 Hedge’s g = 0.15, 0.40, and 0.75 are considered small, medium, and large effects, respectively. 18
All analyses used an unadjusted significance threshold of p < .05. All analyses were performed in Stata v15.1. 19
Results
Participant’s characteristics
Demographics and baseline characteristics by treatment group. a
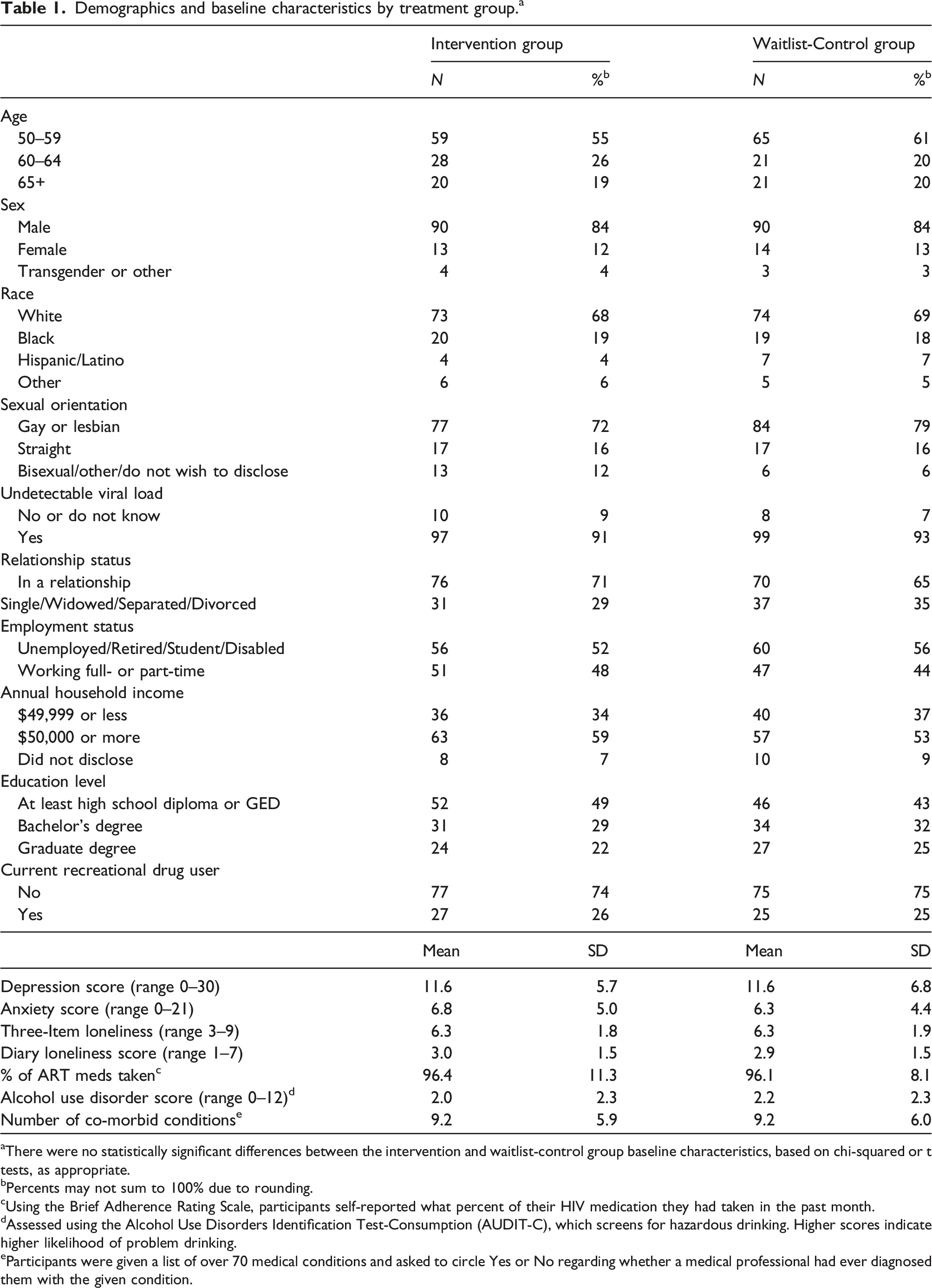
aThere were no statistically significant differences between the intervention and waitlist-control group baseline characteristics, based on chi-squared or t tests, as appropriate.
bPercents may not sum to 100% due to rounding.
cUsing the Brief Adherence Rating Scale, participants self-reported what percent of their HIV medication they had taken in the past month.
dAssessed using the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), which screens for hazardous drinking. Higher scores indicate higher likelihood of problem drinking.
eParticipants were given a list of over 70 medical conditions and asked to circle Yes or No regarding whether a medical professional had ever diagnosed them with the given condition.
Outcomes
Symptoms of depression
Loneliness, depression, and anxiety outcomes in intervention group and waitlist-control group.

aHedge's g is presented only for statistically significant results.
Center for Epidemiologic Studies Depression Scale Revised (CES-D-10). Scores ranged from 0 to 30, with higher scores indicating more depression.
cGeneralized Anxiety Disorder 7-item Scale (GAD-7). Scores ranged from 0 to 21, with higher scores indicating more anxiety.
dFor Daily Diaries, participants were asked, “How lonely did you feel today?” each day for three days, and responses were averaged across the three days. Scores ranged from 1 to 7, with higher scores indicating greater loneliness.
e3-Item Loneliness (3IL) Scale. Participants rated how lonely they felt over the past two weeks. Scores ranged from 3 to 9, with higher scores indicating greater loneliness.
Secondary analyses of loneliness, depression, and anxiety outcomes in people with elevated loneliness, depression, or anxiety at baseline.

aHedge's g is presented only for statistically significant results.
bCenter for Epidemiologic Studies Depression Scale Revised (CES-D-10). Scores ranged from 0 to 30, with higher scores indicating more depression.
cGeneralized Anxiety Disorder 7-item Scale (GAD-7). Scores ranged from 0 to 21, with higher scores indicating more anxiety.
dFor Daily Diaries, participants were asked, “How lonely did you feel today?” each day for three days, and responses were averaged across the three days. Scores ranged from 1 to 7, with higher scores indicating greater loneliness.
e3-Item Loneliness (3IL) Scale. Participants rated how lonely they felt over the past two weeks. Scores ranged from 3 to 9, with higher scores indicating greater loneliness.
Exploratory analyses of outcomes in key subpopulations.

aHedge's g is presented only for statistically significant results.
bCenter for Epidemiologic Studies Depression Scale Revised (CES-D-10). Scores ranged from 0 to 30, with higher scores indicating more depression.
cGeneralized Anxiety Disorder 7-item Scale (GAD-7). Scores ranged from 0 to 21, with higher scores indicating more anxiety.
dFor Daily Diaries, participants were asked, “How lonely did you feel today?” each day for three days, and responses were averaged across the three days. Scores ranged from 1 to 7, with higher scores indicating greater loneliness.
e3-Item Loneliness (3IL) Scale. Participants rated how lonely they felt over the past two weeks. Scores ranged from 3 to 9, with higher scores indicating greater loneliness.
Symptoms of anxiety
At follow-up, the intervention group scored 1.5 points (22.4%) better than the control group on the GAD-7 (F = 4.94, p = .03); a small effect size (Hedge’s g = 0.32) (Table 2). Among the subgroup of participants with symptoms of anxiety at baseline, the intervention group scored 2.3 points (25.6%) better than the control group (F = 10.10, p < .01); a moderate effect size (Hedge’s g = 0.54) (Table 3).
In exploratory analyses among people with low income, the intervention group scored 2.0 points (27.0%) better than the control group (F = 4.24, p = .04); and among people with obesity, diabetes, or COPD, the intervention group scored 2.2 points (29.7%) better (F = 5.03, p = .03) (Table 4).
Loneliness
At follow-up, there were no statistically significant differences between the intervention and waitlist control groups using the Daily Diary or the 3-Item Loneliness Scale (Table 2). However, significant improvements in Daily Diary scores were seen in the subpopulation of participants with at least moderately elevated loneliness scores at baseline (F = 9.60, p < .01), a moderate effect size (Hedge’s g = 0.55) (Table 3). There were no statistically significant differences in other subpopulations (Table 4).
Lesson listening behaviour and participant feedback
Within the intervention group, 85% of participants listened to all 14 lessons, and 92% listened to 10 or more. Within the waitlist control group, 80% listened to all 14 lessons, and 85% listened to 10 or more. These differences in number of lessons completed by the intervention and waitlist control groups were not statistically significant (Χ2 = 9.01, p = .77). Satisfaction survey data from all participants showed that 74% found the lessons useful or very useful, 80% were glad or very glad they listened, and 87% were interested in participating in future lessons.
Discussion
The results of this waitlist-controlled trial show that a series of brief, online audio mindfulness lessons was effective at reducing symptoms of depression and anxiety among older PLWH with some degree of loneliness at baseline. In addition, improvements in daily loneliness were seen among people with elevated baseline loneliness levels. The improvements in symptoms of depression, anxiety, and loneliness were particularly notable because this study took place during the early height of the COVID-19 pandemic, when external factors may have made symptoms of depression, anxiety, and loneliness worse.7–9 In surveys conducted after the study was complete, participants reported high satisfaction with the program. Overall, the results suggest that this effective, easily disseminated intervention may reduce symptoms of depression, anxiety, and to a lesser degree, loneliness among older PLWH. Not only were the changes found statistically significant, the effect sizes of these improvements suggest they may also have been clinically significant.
To measure the clinical significance of the findings, the effect sizes of this intervention on patients with symptoms of depression were compared with the effect sizes seen with selective serotonin reuptake inhibitors and with other mindfulness-based interventions. In this study, the effect size as measured by the Hedge’s g, among participants who had symptoms of depression at baseline, was 0.69 (a moderate, and nearly large, effect size). This compared favourably with a review of 74 registration trials submitted to the FDA for approval of 12 antidepressant agents, which found that the pooled effect size in published studies was 0.41. 20 Moreover, when the full FDA dataset for these 74 studies was analyzed (i.e., not just published studies, but unpublished studies as well), the pooled effect size was only 0.31 (a small effect size).
The effect size of these mindfulness lessons also compares favourably to published studies of other mindfulness-based therapies (MBT). A review of 8 waitlist-controlled MBT studies targeting depression had a mean effect size of 0.53, again as measured by the Hedge’s g. 21 The review also found that the duration of treatment and assigned homework practice time did not impact the efficacy of MBT. A separate meta-analysis of MBT found a mean treatment time of 18.8 h and often required in-person classes. 22 Given that, the much briefer (approximately 4.7 h) and more easily accessed online audio mindfulness lessons used in this study, which produced comparable effect sizes, is an attractive alternative.
To our knowledge, this is the first study to examine the impact on mental health outcomes of a self-administered (i.e., not involving a live group, facilitated, or in-person component) online mindfulness intervention among older PLWH. While other published studies looked at some aspects of this approach, none studied this delivery method in this population. Other studies have examined (1) in-person mindfulness training programs for PLWH who are not exclusively older, (2) self-administered, online interventions for stress or medication adherence for adult PLWH but not focused specifically on mindfulness, (3) mindfulness interventions among adults (age 18+) with other chronic conditions, and (4) mindfulness interventions among older adults (age 60+) without HIV.
In-person mindfulness training programs for PLWH who are not exclusively older
With regard to previous literature examining in-person or facilitated mindfulness training among adults age 18+ living with HIV, one meta-analysis of 16 studies (N = 1049, mean age = 42 years) found significantly less symptoms of anxiety and fewer depressive symptoms among those who received a mindfulness-based intervention compared to controls when outcomes were assessed ≤4 weeks post-intervention, but no differences when outcomes were assessed ≥5 weeks post-intervention. 23 Another meta-analysis of 7 studies that examined adults with HIV (N = 620, age range 25–64 years old) found that people who received a mindfulness-based intervention experienced less depression after both 8 weeks and 6 months. 24 Two studies in that meta-analysis examined anxiety, but the authors did not find evidence that mindfulness-based interventions improved anxiety. Again, it is important to note that all the studies included in these meta-analyses involved in-person activities, such as group sessions or retreats, and did not involve online activities.
Self-administered, online interventions for stress or medication adherence for adult PLWH but not focused specifically on mindfulness
In terms of self-administered, online interventions for adult PLWH, not focused specifically on mindfulness, Brown et al. examined the impact of a single, 90-min, computerized stress management intervention on 60 women living with HIV. 25 At follow-up 1 month later, there were no significant differences in depressive symptoms between women who received the intervention and those in the waitlist control group. Another study used a computer-delivered, single-session cognitive behavioural HIV medication adherence intervention. 26 The intervention included optional modules designed to improve stress and mood management, however, fewer than half of the participants completed them. At follow-up, there were no significant differences in stress or mood between the intervention and waitlist control groups.
Mindfulness interventions among adults (age 18+) with other chronic conditions
Systematic reviews have examined the effects of mindfulness interventions among people with health conditions other than HIV, such as cancer, heart disease, and obesity.27–31 One review of 16 studies concluded that mindfulness-based interventions could help alleviate symptoms of depression in people with physical health conditions, and that interventions that were self-administered via computer were as effective as those delivered by a psychologist/psychotherapist, counsellor, peer, or investigator. 31 A second review, which examined the results of 17 studies, found that online mindfulness lessons produced significant improvements in depression and anxiety in people with chronic conditions. 29 Several of the studies in that review included email, text chat, or telephone interactions with a therapist, or a group forum, limiting their comparability to this study.
Mindfulness interventions among older adults (age 60+) without HIV
Finally, two reviews examined the effects of mindfulness interventions in older adults.32,33 Both reviews, which examined the results of 25 studies in total, found that mindfulness interventions produced significant improvements in depression relative to control groups. Only one review also looked at anxiety. That review found no evidence of improvements in anxiety, based on an analysis of only three studies. 32 Moreover, all studies in both reviews included in-person activities, again limiting their comparability to the present study.
Limitations
A possible limitation of this study was the enrolment strategy. The first 225 people who responded and met the inclusion criteria were enrolled, which might have led to volunteer bias, 34 though a comparison of enrollees versus non-enrollees from the ADHOC database showed no differences in terms of age, sex, race, symptoms of depression, symptoms of anxiety, income, or comorbidities. Also, because this study occurred during the pandemic, it is unclear how findings would have differed in the absence of this unusual circumstance.
Participation in this study was limited to people with basic computer or smartphone literacy and Internet access, which limits generalizability of the intervention. Another possible limitation was that participants were reimbursed with a gift card if they completed all the questionnaires and at least 10 of the lessons, which may have increased adherence. However, to receive the gift card, participants were required to complete multiple pre- and post-mindfulness training questionnaires, which would not be necessary outside of a research setting.
Further research will be needed to determine whether similar benefits are seen in younger PLWH. It will also be important to determine the durability of the response and whether maintenance of these benefits requires ongoing practice of the mindfulness techniques. Of note, one review of mindfulness-based therapies had a mean follow-up time of 28.92 weeks, 21 and the results at follow-up were similar to those seen at the end of treatment, which may bode well for the lasting impact of these lessons.
Conclusion
This study is the first to show that a series of brief, online mindfulness lessons led to improvements in mental health outcomes among older PLWH. This was true even in the face of the COVID-19 pandemic. The intervention can be delivered online, in a scalable fashion. As such, it holds promise, both as a way to supplement strained mental health resources (American Psychological Association, 2023) 35 with minimal disruption to provider workflow, and as a way to bring relief to older PLWH both during and after the pandemic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jeff Berko and Peter Mazonson received research funding from ViiV Healthcare to develop ADHOC and collect data. Maile Karris and Lynsay Ehui received research support from ViiV Healthcare. Cassidy Gutner, Andrew Zolopa, and Duncan Short are employees of ViiV Healthcare. Frank Spinelli was an employee at ViiV Healthcare at the time the research was conducted, and the manuscript was prepared. He is currently an employee of Gilead Sciences.
Clinical Trial Registration
ClinicalTrials.gov Identifier: NCT04580082.