
Abstract
Background
Data on low bone mineral density (BMD) in people living with HIV (PLWH) are mainly derived from younger adults; little is known about how antiretroviral therapy (ART) and alterations in the renal-bone axis relate to BMD in older PLWH.
Methods
Cross-sectional study of men > 50 years and post-menopausal women with HIV. Antiretroviral therapy exposure was stratified into four groups based on use of tenofovir disoproxil fumarate (TDF) and protease inhibitors (PI): non-TDF/non-PI, non-TDF/PI, TDF/non-PI, and TDF/PI. Bone mineral density was measured by dual X-ray absorptiometry (DXA). Bone turnover/regulatory markers and renal tubular function were analysed in stored plasma and urine samples. The association of ART exposure and bone/renal biomarkers on BMD was explored using logistic regression models.
Results
247 individuals (median [IQR] age 57 [53, 65] years; 47% female; 13% of Black ethnicity; CD4 count 643 [473, 811] cells/mm3; and 98% with HIV RNA < 200 copies/mL) were included. Bone turnover and renal tubular function differed significantly by ART exposure. In analyses adjusted for demographic and traditional renal/bone risk factors, exposure to TDF and PI was associated with a fourfold greater risk of low BMD at the femoral neck and exposure to TDF and/or PI with a threefold greater risk of low BMD at the lumbar spine. The relationship between ART and low BMD was not altered by further adjustment for bone turnover or renal tubular function markers.
Conclusions
The associations between low BMD and ART exposure (TDF vs. non-TDF and boosted vs. unboosted third agents) were minimally affected by adjustments for bone and kidney biomarkers.
Introduction
Advances in HIV therapy and care have led to a significant reduction in mortality in people living with HIV (PLWH). The consequent ageing of PLWH comes with the potential for age-related chronic comorbidities such as fractures and kidney disease1–3 and an increased risk of adverse effects of antiretroviral therapy (ART) on bone and kidneys.4–6 Low bone mineral density (BMD) and osteoporosis are common in PLWH with prevalence rates of approximately 30–60% for low BMD and 15% for osteoporosis4,7,8; low BMD is associated with an increased risk of fractures.9–12 Whilst the prevalence of chronic kidney disease (CKD) ranges from 5 to 15%13,14 subclinical renal tubular alterations, mainly characterized by an increased loss of low molecular weight proteins (LMWP) and phosphate in urine, has been reported in up to 40% of PLWH.15–17
The aetiology of renal and bone alterations in PLWH is multifactorial. Even after controlling for traditional risk factors such as smoking and low body mass index (BMI), which are more common in PLWH, HIV remains an independent risk factor for kidney disease, bone turnover, and low BMD.1,18,19 A number of studies have demonstrated reductions in BMD, occurring with initiation of both first-line and second-line ART, largely limited to the first 48–96 weeks of therapy, with somewhat greater BMD reductions with ART containing the nucleotide reverse transcriptase inhibitor tenofovir disoproxil fumarate (TDF) or ritonavir-boosted protease inhibitors (PI/r).20–28 Tenofovir disoproxil fumarate use, with or without PI/r, is one of the main risk factors for renal proximal tubular dysfunction (RTD)22,29–31 and proximal tubulopathy. 32 However, whether and how RTD contributes to reductions in BMD remain controversial, with data supporting an association mainly derived from TDF-exposed populations. No study to date has concurrently examined renal and bone function in an exclusively older population.
In the current study, we aimed to explore the relative contribution of TDF and PI/r-containing ART, and of alterations in renal and bone biomarkers, to low BMD in PLWH over 50 years of age.
Methods
HIV-ASSORT is a sub-study of GS-US-104-0423 (EudraCT 2011-004420-35), a phase IV cross-sectional study evaluating BMD in men over 50 years of age and post-menopausal women living with HIV who had initiated and been maintained on ART regimens that either always or never included TDF, and for the past 3 years had continuously included or not included PI/r. Individuals with a history of osteoporosis prior to initiating ART or contraindications to dual X-ray absorptiometry (DXA) scanning were excluded. A total of 440 participants from 68 sites across Europe were enrolled in the study between April 2013 and October 2014. Written informed consent was obtained from all participants. Due to between-country differences in regulations, the present analyses are restricted to the 247 participants who were enrolled in Austria, Belgium, France, Germany, and Spain for whom both plasma and urine samples were available and who had provided explicit permission for use of these samples for future research. The experiments were conducted with the understanding and the consent of each participant, and the study was approved by ethics committees and local R&D departments/institutional review boards in each of the countries in which the study was conducted.
The parent study comprised a single visit. Demographic and clinical data including HIV transmission risk, details of current and prior ART and AIDS-defining illnesses, hepatitis B/C status, history of fractures, risk factors for bone disease and osteoporosis, and height and weight were recorded. Bone mineral density at the lumbar spine (BMD-LS) and femoral neck (BMD-FN) using DXA was measured within 30 days of the study visit in local hospitals or clinics and analysed by BioClinica (Newton, PA, USA). CD4 T-cell count, HIV RNA, serum creatinine, phosphate, and 25(OH)vitamin D were analysed in a central laboratory, and aliquots of plasma and urine stored at −70°C.
For the current analyses, we measured markers of bone formation (osteocalcin [OC], procollagen type 1 amino-terminal propeptide [P1NP]) and resorption (C-terminal cross-linking telopeptide of type 1 collagen [CTX-1]) in stored plasma samples using electrochemiluminescence immunoassays (Roche Diagnostics, Basel, Switzerland); markers of bone regulation (osteoprotegerin [OPG], surface-bound receptor activator of nuclear factor kappa-B ligand [sRANKL], and phosphatonin [FGF-23]) using electrochemiluminescence immunoassays (MESO QuickPlex SQ 120 Microplate reader, Meso Scale Diagnostics, Rockville, MD, USA), and parathyroid hormone (PTH) using a sandwich immunoassay with chemiluminescent detection (Abbott, Abbott Park, IL, USA).
Retinol-binding protein (RBP) was measured in urine samples using a Dissociation-Enhanced Lanthanide Fluorescent Immunoassay (DELFIA; lower limit of detection 1.4 µg/L), and type 3 carbonic anhydrase (CA3) was measured using the BIOMATIK EKU02920 enzyme-linked immunosorbent assay (ELISA; lower limit of detection 0.78 µg/L) and read on a Multiskan GO Thermofisher. 33 Urine RBP and CA3 were each expressed relative to urinary creatinine concentration retinol-binding protein/creatinine ratio (RBPCR and CA3CR, respectively). Fractional excretion of phosphate (FEPO4) was calculated using standard formulae. Serum creatinine was converted to eGFR using the Chronic Kidney Disease Epidemiology (CKD-EPI) equation. Using World Health Organization definitions of osteopenia and osteoporosis, we classified BMD into the following categories: normal BMD: T score greater than −1; osteopenia: T score −1 to −2.5; and osteoporosis: T score less than −2.5. Antiretroviral therapy was stratified into four groups based on always or never having included TDF, and current exposure to a boosted PI (to simplify notation PI in tables and figures refers to PI/r): non-TDF/non-PI; non-TDF/PI; TDF/non-PI; TDF/PI.
Statistical analyses
Descriptive analyses are presented; values are median (interquartile range – IQR) unless stated otherwise; Kruskal–Wallis tests and Chi-squared tests were used for comparison of continuous and categorical variables, respectively, across the four ART groups. The relationships between renal and bone variables were explored using the Spearman correlation coefficient. The association between ART exposure and low BMD was assessed using multivariable logistic regression models. The outcome of interest was low BMD (T score < −1) and the exposure of interest was, as per the design of the parent study, ART regimens stratified by TDF and PI. The multivariable models were fitted using a stepwise approach in which the effect of ART exposure was first adjusted for age, sex, ethnicity, BMI, and smoking status (model 1). The additional effects of bone turnover and renal tubular dysfunction on BMD were determined by adding bone (model 2) and renal (model 3) biomarkers that were significantly or weakly associated with low BMD (p < .2) after adjustment for the socio-demographic variables detailed in model 1 and/or considered of clinical relevance for low BMD. All analyses were conducted using SPSS version 24.
Results
Demographics and clinical characteristics of the participants stratified by ART group.
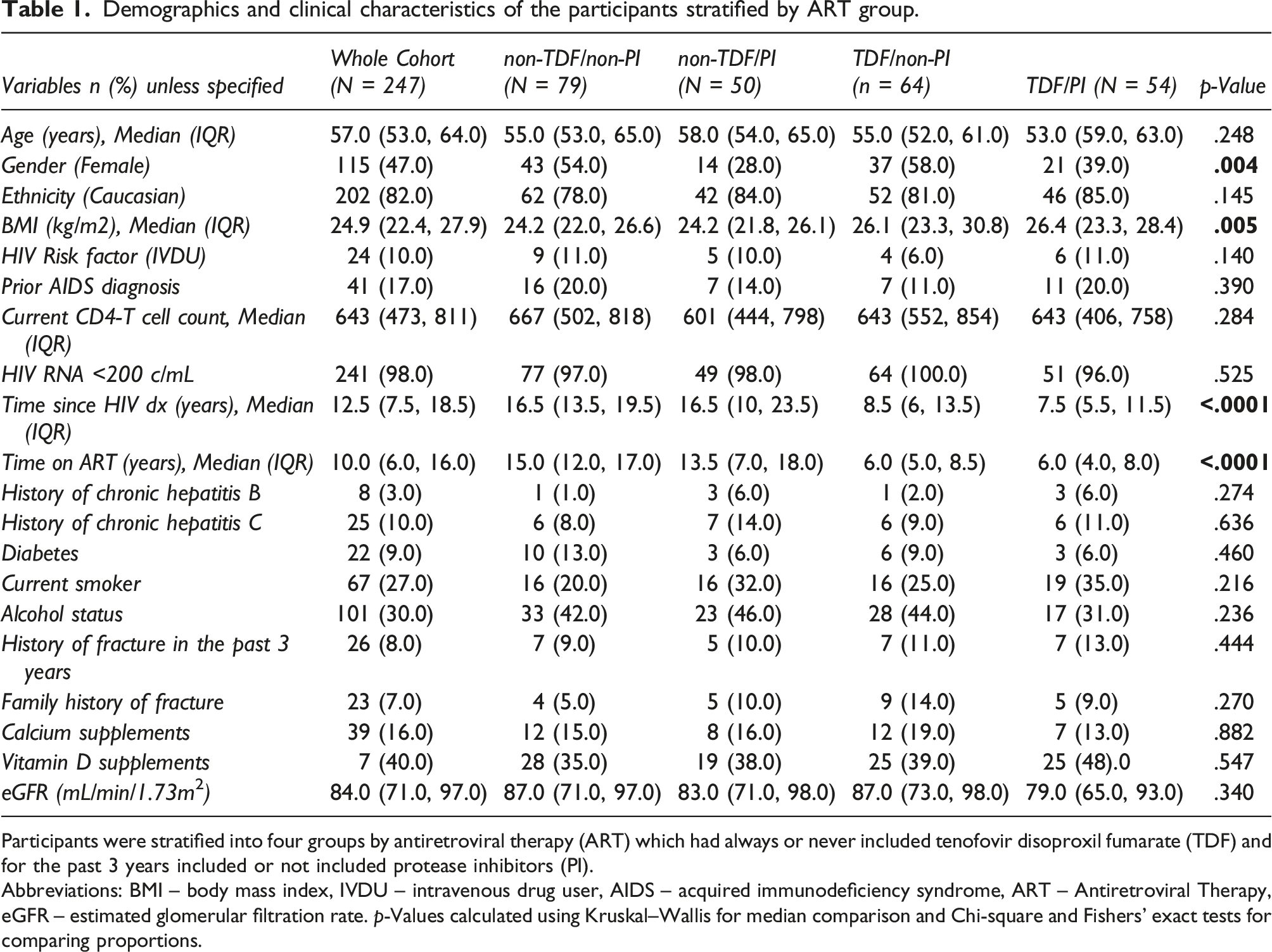
Participants were stratified into four groups by antiretroviral therapy (ART) which had always or never included tenofovir disoproxil fumarate (TDF) and for the past 3 years included or not included protease inhibitors (PI).
Abbreviations: BMI – body mass index, IVDU – intravenous drug user, AIDS – acquired immunodeficiency syndrome, ART – Antiretroviral Therapy, eGFR – estimated glomerular filtration rate. p-Values calculated using Kruskal–Wallis for median comparison and Chi-square and Fishers’ exact tests for comparing proportions.
Bone mineral density
Bone Mineral Density stratified by ART group.

Data from 228 of 247 (92%) participants with DXA measurements available. Low BMD: T-score <−1; Osteopenia: T-score<−1 to −2.5; Osteoporosis: T-score<−2.5.
Abbreviations: ART – antiretroviral therapy, TDF – tenofovir disoproxil fumarate, PI – boosted protease inhibitor, BMD-LS – bone mineral density at the lumbar spine, BMD-FN– bone mineral density at the femoral neck. p-Values calculated using Kruskal–Wallis for median comparison and Chi-square and Fishers’ exact tests for comparing proportions.
Renal biomarkers
Median (IQR) eGFR was 84 (71, 95) mL/min/1.73m2, and 10% of participants had eGFR <60 mL/min/1.73m2, with no differences between the four ART exposure groups (Table 1). Biomarkers of RTD, RBPCR, CA3CR, and FEPO4 differed by ART exposure, with the highest levels observed in the TDF/PI group (Figure 1), and by gender (Table S2). Retinol-binding protein/creatinine ratio and CA3CR were correlated with BMD-FN (RBPCR: r = −0.158, p = .018; CA3CR: r = −0.134, p = .05), but not with BMD-LS. No correlation was found between FEPO4 and BMD-FN or BMD-LS (see Table S3). Boxplots for renal and bone biomarkers by ART group. Comparison of renal and bone biomarkers per by antiretroviral therapy (ART) group. Renal biomarkers (RBPCR and CA3CR) were measured in urine samples; bone turnover and bone regulation markers were measured in plasma samples. Data are shown as median with interquartile ranges and min and max. Abbreviations: RBPCR – retinol-binding protein/creatinine ratio, CA3CR – type 3 carbonic anhydrase (CA3)/creatinine ratio, FEPO4 – fractional excretion of phosphate, OC – osteocalcin, CTX-1-C – terminal cross-linking telopeptide of type 1 collagen, P1NP – procollagen type 1 amino-terminal propeptide, PTH – parathyroid hormone, FGF-23 – phosphatonin, OPG – osteoprotegerin, sRANKL – surface-bound receptor activator of nuclear factor kappa-B ligand, TDF – tenofovir disoproxil fumarate, PI – boosted protease inhibitor.
Bone biomarkers
Biomarkers of bone turnover also differed by ART groups (Figure 1), with higher measurements in the TDF groups (CTX-1 and P1NP) or TDF/PI group (OC) as compared to the non-TDF groups. No between-group differences were observed in other markers of bone regulation OPG, RANKL, and FGF-23. Increased bone turnover and higher levels of bone regulatory hormones were observed in female participants (Table S2). Increased bone turnover was correlated with lower eGFR and higher RBPCR, CA3CR, and PTH (Table S3). Increased bone turnover also correlated with lower BMD-LS and BMD-FN and higher PTH correlated with lower BMD-FN but not BMD-LS (Table S3).
Associations with low BMD
In a model including age, gender, ethnicity, BMI, and current smoking status, and using non-TDF/non-PI as the ART reference group, exposure to TDF/PI was significantly associated with low BMD at both femoral neck and lumbar spine. By contrast, exposure to TDF/non-PI and PI/non-TDF was associated with lower BMD-LS, but not BMD-FN (Figure 2, model 1). The observed associations between the ART groups and low BMD were not altered by adjustments for time since HIV diagnosis and time on ART. Further adjustment for bone turnover (OC, CTX-1, and PTH; Figure 2, model 2) also did not alter the observed associations. Similarly, adjustment for RBPCR and CA3CR did not alter the association between ART and BMD (Figure 2, model 3). None of the renal and bone biomarkers remained associated with low BMD after adjustment for demographic/clinical variables, and further adjustment for ART exposure (Table S4). Of the non-HIV risk factors for low BMD (older age, female gender, non-black ethnicity, and low BMI), only BMI remained independently associated with low BMD in fully adjusted models. Adjusted logistic regression models to assess the associations between ART exposure and low BMD (T-score<−1) at the femoral neck and lumbar spine.
Discussion
The HIV-ASSORT cohort comprises a heterogeneous cohort of older PLWH with adequate representation of both genders and receiving different types of ART including, uniquely, a group never exposed to TDF. Most previous studies have included people with prior TDF exposure in the non-TDF group, and some of these may have stopped TDF for kidney and/or bone toxicity. Hence, the comparison of TDF versus non-TDF regimens in such studies may be affected by residual effects of prior TDF exposure on kidney and bone.
In this study population, exposure to ART rather than levels of bone turnover or renal tubular biomarkers best predicted low BMD in analyses adjusted for demographic factors, BMI, and current smoking status. Exposures to non-TDF/PI, TDF/non-PI, and TDF/PI were all associated with increased odds of osteopenia of the LS. They were also associated with increased odds of osteopenia at the femoral neck although this was only statistically significant for TDF/PI. This may reflect a more pronounced effect of these ARV’s on trabecular versus cortical bone, or limited power of our study to detect similar differences at the femoral neck. 34
Despite significant differences in markers of bone turnover, renal tubular function, and PTH between the four ART groups, none of these markers substantially modified the association between ART and low BMD at either site. The mechanisms underlying the association between renal tubular dysfunction and low BMD in PLWH remain unclear. While PIs may affect BMD through effects on osteoclast/osteoblast activity, 35 TDF may affect bone indirectly through mitochondrial toxicity within proximal tubules, resulting in loss of vitamin-D-binding protein, phosphate wasting, and increased bone turnover. 36 However, consistent with previous studies, 30 we observed no association between FEPO4, a measure of tubular phosphate wasting, and markers of bone turnover or BMD. Low molecular weight proteinuria is a more specific marker of RTD. 37 Data from the HIV UPBEAT Cohort, which includes PLWH and HIV-negative individuals from similar demographic backgrounds in Ireland, observed that RBPCR was the only renal parameter that distinguished HIV-positive and negative populations, with RBPCR also predicting lower BMD in the whole cohort. 38 Data from the Brighton Cohort (UK) similarly identified an association between RBPCR and BMD in HIV-positive men, all of whom were receiving TDF. 30 The explanation for the differences in associations between RBPCR and BMD in these cohorts as compared to the present analyses likely lies in differences in study design. In addition to the differences noted above, these cohorts also differed from the HIV-ASSORT cohort in their inclusion of participants under 50 years of age. The HIV-ASSORT cohort was also more heterogeneous in terms of ART regimens compared to the Brighton Cohort, which comprised an exclusively TDF-treated population.
Our results are consistent with the findings of randomised controlled clinical trials, where the discontinuation of TDF has been associated with improvement in BMD at the lumbar spine and hip in the absence of changes in renal tubular function as assessed by either RBPCR or phosphate reabsorption.39,40 Similarly, several randomized controlled trials have reported increases in bone turnover markers, both at treatment initiation and treatment switch, coinciding with decreases in BMD that persist to 48–96 weeks, particularly in relation to TDF exposure.27,28,41,42 However, long-term studies are scarce, particularly in older individuals. Within our cohort, with a median ART duration of 10 years, markers of bone turnover correlated with lower BMD at the hip and spine, and the highest levels of bone turnover were observed in those receiving TDF. Overall, these data suggest that the effects of TDF on BMD are likely mediated by multiple pathways and not explained solely through the consequences of its effects on the renal tubules. Bone remodelling is also affected by the state of immune activation and inflammation associated with HIV infection, even in the setting of effective ART. 43 This complex interaction is likely influenced by other parameters, including traditional risk factors for low BMD and fragility fracture. Post-menopausal women living with HIV are particularly at risk for osteoporosis as a result of the additive effects of oestrogen-depletion and the effects of the HIV infection itself.44,45
Our study has several limitations. The cross-sectional design limits determination of causality, and the clinical relevance of the observed renal and bone alterations, in terms of overall outcomes such as fragility fracture, remains to be defined. We did not measure markers of inflammation or immune activation, which might explain differences seen between the two BMD anatomical sites. Despite these limitations, this is one of the largest studies to date examining renal and bone alterations in older PLWH, including an adequate representation of post-menopausal women, a population at particular high risk of bone loss and fractures. We demonstrated an association between renal tubular dysfunction and changes in bone turnover that ultimately had minimal impact on BMD. In older PLWH, low BMD appears to be largely attributable to traditional risk factors and the effects of ART on BMD.
Conclusion
In these cross-sectional analyses, the associations between low BMD and exposure to ART (TDF vs. non-TDF and boosted vs. unboosted third agents) were minimally affected by adjustments for bone and kidney biomarkers. Treatment with TDF/PI combined was a predictor of low BMD-FN while TDF with or without PI predicted low BMD-LS. These data support measurement of BMD to evaluate fracture risk, rather than measurements of biomarkers, in older PLWH exposed to TDF- and/or PI-based ART so that TDF- and/or PI-sparing regimens can be considered for those with low BMD and/or increased fracture risk.
Supplemental Material
Supplemental Material - The renal-bone axis in older people living with HIV on stable antiretroviral therapy: A sub-analysis of the GS-US-104-0423 study
Supplemental Material for the renal-bone axis in older people living with HIV on stable antiretroviral therapy: A sub-analysis of the GS-US-104-0423 study by Elena Alvarez, Lucy Campbell, Willard Tinago, Alejandro Garcia-leon, Ian Walsh, Jennifer J Brady, Keith Burling, Sebastian Noe, Marie F Neuville, Francois Jouret, Farid Jamshidian, Hiba Graham, Martin Rhee, Paddy W Mallon, and Frank A Post in Antiviral Therapy.
Footnotes
Acknowledgements
The authors gratefully acknowledge all participant subjects that took part in the GS-US-104-0423 study and other investigators and study staff who facilitated this research project.
The study was conducted as collaboration between Gilead Sciences and the co-author’s academic institutions.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P. W. Mallon has received honoraria, travel grants, and/or research funding from Merck Sharpe and Dohme, Gilead Sciences, ViiV Healthcare, Janssen and Bristol Myers Squibb. F. A. Post-reports grants and personal fees from Gilead Sciences, ViiV Healthcare, Janssen Pharmaceuticals and MSD outside the submitted work. F. Jouret and M. F. Neuville are Fellows of the Fonds de la Recherche Scientifique (FNRS), Belgium. F. Jamshidian, H. Graham, and M. Rhee are employees of Gilead Sciences. All other authors declared no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present work was supported by Gilead Sciences (CO-UK-311-187).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.