
Abstract
Background
Direct acting antiviral (DAAs) treatments for hepatitis C virus (HCV) have demonstrated a high rate of cure, low side effects, and short duration of treatment. This allowed for elimination of HCV for the first time starting in 2014 when they were launched. By then, hepatitis B virus (HBV) vaccines had been available for >25 years and antiviral treatments for HBV for >15 years making the elimination of HBV already feasible. In 2016, the 69th World Health Assembly endorsed the Global Health Sector Strategy for Viral Hepatitis, including a goal to eliminate hepatitis infection as a public health threat by 2030 [1], and the World Health Organization (WHO) introduced the global targets for the care and management of HCV which included a reduction in new infections and liver related deaths [2].
The Center for Disease Analysis (CDA) and the Center for Disease Analysis Foundation (CDAF—a non-profit organization that now continues CDA’s work) aimed to create a universal registry, the Polaris Observatory, to support informed decision-making at the national, regional, and global level for HCV and HBV elimination. Funded by the John C Martin Foundation since 2015, the Polaris Observatory has been providing decision support to more than 110 countries/territories considering hepatitis elimination [3].
This publication focuses on the Polaris Observatory, although the contributions made by CDA/CDAF go beyond the decision support described here. The Polaris Observatory is complemented by the Global Procurement (GPRO) Fund. Formed in 2017, GPRO helps low- and middle-income countries get access to low-cost quality diagnostics and treatment, using pooled procurement. Pricing was identified as a key barrier to viral hepatitis elimination, but through negotiated pricing and large orders, GPRO was able to reduce prices by 65–90%. Currently more than 10 countries order products through GPRO and switch to a national tender process once their volumes are large enough to negotiate low prices on their own.
However; data, analytical support, and lower prices were not sufficient to help countries adopt national elimination programs. Countries continued to struggle to build up the capabilities needed for a national hepatitis elimination program. In 2019, CDAF started a demonstration project using public private partnerships (PPP). The first was implemented in Uzbekistan where PPP was used to start a combined HCV/HBV elimination project that included recommendation of specific products for screening and treatment, simplified testing, training of primary care physicians and nurses, and electronic medical record systems. In 2020, we screened 63,000 people for HCV/HBV and linked them to care in collaboration with the Research Institute of Virology in Tashkent. This was accomplished despite a 6-month shut down of the primary care clinics due to the COVID-19 pandemic. In the last quarter of 2020, HCV/HBV screening was combined with COVID-19 testing. Task shifting training was provided by the Research Institute of Human Virology and The University of Maryland, based on the ASCEND study, [4-7] while motivational interviewing techniques were provided by the Academy for Health Coaching [8]. Due to this project, the government of Uzbekistan put out tenders to screen 500,000 people for HCV and HBV in 2021. The Ministry of Health in Uzbekistan is now leading the call for the viral hepatitis elimination program in that country. Using learnings from this project, CDA Foundation is now working on new demonstration projects in Uganda (HBV birth dose vaccination and treatment of high viral load mothers) and Kazakhstan (elimination of HCV and HBV).
Methodology
With the goal of building a good decision-support system, we worked backwards to identify the critical elements required. We interviewed UNAIDS [9], Global Funds, and the World Bank [10] to identify their key success factors and areas they would improve. We determined the following criteria for building a successful system: (1) It has to meet the needs of the countries and policy makers. (2) It needs to contain updated information—annual updates at minimum. (3) It has to be unbiased. (4) Outputs across countries need to be comparable. (5) It needs to show the impact of decisions. (6) Countries need to have ownership of the data and forecasts. (7) The data collection and analysis need to be transparent.
Methodology
Data collection and analysis
In order to support multiple countries simultaneously, we developed processes and templates for data collection, expert interviews, and analyses. All inputs were segmented into required country inputs (e.g., infections, diagnosed, genotype of the virus, and treated) and disease specific inputs (e.g., disease progression and mortality rates). For the latter, data from large longitudinal cohorts were used.
An epidemiology team was hired and trained in data collection and analysis. This included creating standard operating procedures (SOP) for analyzing national registries to estimate the number of cases alive today. In addition, SOPs and training were developed to estimate age specific prevalence from different data sources (national, regional, military recruits, premarital testing, pregnant women screening, high risk populations, and gradients across provinces/regions). All input and output forms were standardized to allow comparisons across countries. Country input data were collected and updated annually.
Modeling scenarios to understand action and impact—the basis of good decision making
Hepatitis C virus and hepatitis B virus Markov models were developed to measure the impact of decisions on disease burden and mortality averted. An event-based forecasting approach was used to enable policy makers to incorporate the impact of multiple events (increase in screening and treatment) over time. The outputs of the HCV and HBV models were validated in countries with robust data using national incidence, hepatocellular carcinoma (HCC) rates, and mortality estimates. The models were developed in Microsoft Excel for transparency, ease of training and to minimize the cost (software purchase and training), to countries. Our continuous improvement processes ensured that the models evolved over time to meet the needs of the collaborating countries and improve the accuracy of the forecasts.
The Polaris HBV and HCV Markov models are unique in that they are not calibrated to HCV/HBV country reported outcomes. Instead, the models are calibrated to country specific epidemiology data (prevalence by age and gender, diagnosed, and treated). The outputs of the model are then compared against reported disease burden data. If sufficient numbers of discrepancies across multiple countries are found, then the calculations are re-examined to find a better fit across all countries. Examples included updating HCV progression rates to find a better fit with reported HCC cases in countries with robust national registry data, and updating the HBV transition rates when experts pointed out that incidence of HCC does not decline with treatment as quickly as the reductions observed in HCV-treated cohorts. In addition, we provide a free copy of the HCV/HBV models and free training to modelers in collaborating countries. Thus far, we have trained over 40 modelers across the globe. As these modelers work with our Markov models, they request additional functionalities which require model updates. To date, the calculations in the HCV model have undergone 90 revisions and updates since inception, while the HBV model has undergone 200 revisions/updates. These updates allow us to better meet the needs of our collaborators and improve the accuracy of our forecasts. That said, the changes in input country specific assumptions (prevalence and treated) have had the largest impact on our forecasts since we started the Polaris Observatory.
Economic impact models were also added to the models to estimate the budgetary requirements for different elimination scenarios as well as incremental cost effectiveness ratio (ICER), cost per disability adjusted life years (DALY) averted, cost per quality adjusted life years (QALY), and return of investment (ROI). The economic model was flexible enough to support discussions with the Ministries of Health, Ministries of Finance, development banks and global donors.
Results
Collaborations with countries and territories across the world
Polaris Observatory has been in operation since 2015. Annually, we update and forecast disease burden in 110 countries for HCV and 135 countries for HBV. We collaborate with over 1000 national experts in these countries for our annual updates. A map of countries currently covered by the Polaris Observatory is shown in Figure 1. In addition to national level, we also provide provincial level analyses and/or support for Pakistan, Mexico, US, Russia, Australia, and China. Countries collaborating with polaris observatory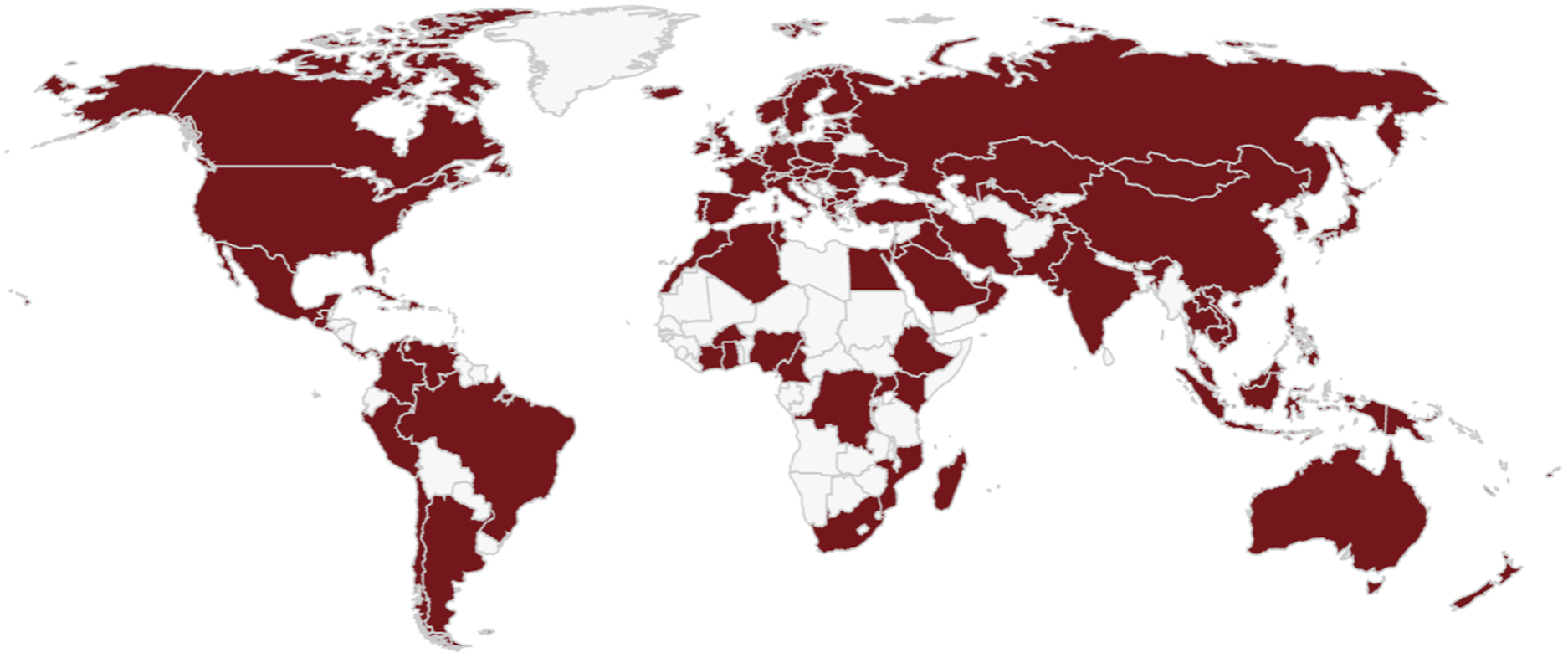
We have trained >40 national experts across the globe to use our models to internally support their national and provincial governments. Since 2015, we have offered free 2-weeks training at our office and have provided regional trainings when multiple countries could come together.
The Polaris Observatory has influenced national hepatitis elimination programs in nearly every country shown in Figure 1.
Outcome and progress
By providing reliable and up-to-date country specific data and analyses, demonstrating the impact of decisions, and providing costing estimates of national programs, our collaborating countries are well-informed for making decisions to pursue a national HBV/HCV elimination program. Regardless of the decision, the policymakers and national stakeholders are provided with analyses that showed the impact of making, not making, or delaying a decision [11,12].
We have completed economic impact analyses for HCV in 55 countries and for HBV in 25 countries to support financing decisions. In Egypt, these analyses led to discussions with the World Bank to apply for a loan to support the national program. In Mongolia, a patient co-pay program was developed, while in Australia a fix annual budget model was implemented. Spain expanded screening programs once our analyses showed that sustained treatment needed additional screening of the population and the cost of screening would be offset by the hospitalization cost savings.
The Observatory also supported global health organizations (World Health Organization (WHO), WHO regional offices, US CDC, Medicine Patent Pool, and Gavi). The Polaris Observatory data were used in the last two WHO viral hepatitis reports as well as regional reports [13,14]. The country collaborations have resulted in over 100 peer reviewed publications focusing on hepatitis C and B making CDA/CDAF the most prolific publisher of hepatitis C and B data and analyses [15]. Although these publications account for less than 10% of all analyses completed and data generated, they rendered attention from national policy makers to take action.
The Observatory also helped countries keep track of how they are progressing against the World Health Organization (WHO) targets [16]. Our annual list of countries on track to eliminate HCV and HBV are closely watched [17] and was influential is getting countries in the European Union to remove treatment restrictions in 2017–2018. In the US, a number of states including Colorado and Washington removed their restrictions because of the analyses we conducted for the state health department. The annual updates allowed us to provide up-to-date global and regional data to national agencies to notify travelers of endemic countries [18], and national blood banks of the likelihood of HCV and HBV infection among blood collected among migrants. The analyses conducted by Polaris enabled us to estimate the global prevalence of HBV and HCV in the pediatric population and women of childbearing age to support programs targeting a reduction in mother to child transmission [19-21].
Modeling provided unique capabilities by enabling us to forecast the future based on a set of informed assumptions. This approach helped us make a few very important observations [1]. Countries with a low HCV prevalence will not achieve the WHO targets despite expanded elimination programs. This was highlighted in an editorial drafted by the Polaris Observatory collaborators [22] which ultimately lead to the adoption of absolute elimination targets by WHO [23]. Unfortunately, the new targets disadvantage countries with a high prevalence, but allowing countries the option to use relative or absolute targets would resolve this problem [2]. The Polaris Observatory was also the first to identify a large disconnect between the HBV programmatic targets (diagnose 90% of the population and treat 80% of the eligible population) and WHO impact targets (65% reduction in mortality). We ran the WHO elimination strategy for all country models and found that no country will achieve a 65% reduction in mortality by implementing the programmatic targets using the current treatment guidelines. This had to do with the definition of HBV treatment eligibility. Currently, only 20–30% of the total HBV infected population is eligible for treatment which greatly limits the impact of treatment. The current eligibility criteria were developed to identify and treat those at the highest risk of disease progression. In fact, 70–80% of the diagnosed patients are informed that they are not eligible for treatment, get lost to follow up, and only show up when they present with advanced liver disease where treatment has a limited impact on progression to decompensated cirrhosis and hepatocellular carcinoma. We have been outspoken about expanding HBV eligibility to treating all HBV patients (similar to treating all HIV patients), but that debates continues [3]. We also identified the large number of countries who will eliminate HBV using the classical definition of elimination, which is a decrease in incidence, using HBV vaccination programs. The WHO absolute targets require countries to achieve an HBV prevalence of ≤0.1% among ≤5 years-old [23]. The Polaris Observatory studies projected that 84 countries will reach this goal before 2030 using their existing HBV prophylaxis program [17]. Our forecasts included the impact of birth dose, three dose, and catch-up vaccination as well as the use of hepatitis B immunoglobulin (HBIG) and treatment of pregnant women to reduce mother to child transmission. However, the same projections highlighted the sheer number of chronic HBV infections in the adolescent population that were not exposed to HBV vaccination at birth or catch-up vaccination. Globally, we estimated that there were 415,000 chronic HBV infections due to vertical transmission, 627,000 infections among <18-years-old due to horizontal transmission, and only 104,000 chronic HBV infections among adults (>18 years-old) due to horizontal transmission. Although there has been a global effort to expand birth dose vaccination, this data suggests that catch up vaccination in the pediatric population is also important.
The Polaris Observatory has also made an impact in hepatitis B and C treatment and diagnostic pricing. After a national hepatitis elimination plan is established, we collaborate with the national reimbursement agencies to estimate the prices and volumes which will make national elimination cost effective or highly cost effective. By providing decision-making data to national government who successfully negotiated prices with manufacturers and took action to implement national programs, Egypt, Mongolia, Australia, Saudi Arabia, Spain, Taiwan, New Zealand, and Brazil are all benefiting from lower costs for diagnosing and treating viral hepatitis thus broaden the national programs to include more patients.
Through supporting countries across multiple regions, we identified the importance of screening to support viral hepatitis elimination. After the launch of DAAs, a key concern for many countries was that treating every HCV infected person coming in for treatment during the first year of launch would bankrupt the national health system. Our data from countries that had launched DAAs first, showed that in fact, countries must worry about the opposite—running out of patients to treat. Countries like Egypt, the US, France, and Spain initiated national screening programs to offset this expected drop.
Summary
Polaris Observatory is an example of impactful private-public partnership where funding by the John C. Martin Foundation allowed support for informed decision-making by public agencies and national governments who would not/could not support such programs on their own. The catalytic funding allowed the Polaris Observatory to demonstrate the utility of such a program resulting in other donors (ZeShan Foundation, EndHep2030, CDC Foundation, Association of State and Territorial Health Officials, Gilead Sciences, and AbbVie) to support this work. The Polaris Observatory is now supported through a portfolio of funders while our work and outputs remain independent to continue support for viral hepatitis elimination by year 2030.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Member of advisory boards for Gilead, AbbVie, Abbott, Merck, Janssen, Roche, and VBI Vaccines. All proceeds were donated to Center for Disease Analysis Foundation. CDA/ CDAF has received research funding from Gilead, Assembly Biosciences, AbbVie, Intercept, Pfizer, and Roche. CDAF has received grants from John C. Martin Foundation, Zeshan Foundation, EndHep 2030, CDC Foundation, Association of State and Territorial Health Officials, Vaccine Impact Modeling Consortium, World Hepatitis Alliance, New York, Idaho and District of Columbia Departments of Public Health, and World Health Organization.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.