The CME portions of this programme have been accredited by the European Accreditation Council for Continuing Medical Education (EACCME) and the Institute for Medical and Nursing Education (IMNE). IMNE is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
The Organizing Committee and International Medical Press would like to thank the following supporters:
ViiV Healthcare
Gilead Sciences, Inc.
Janssen
This conference was partially supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under award R13AI165238. The views expressed in conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention of trade names, commercial practices or organizations imply endorsement by the US Government.
ORGANIZING COMMITTEE
Chairs for 2021
Paddy Mallon University College Dublin, Dublin, Ireland
Morrie Schambelan University of California at San Francisco, CA, USA
Todd Brown Johns Hopkins University, Baltimore, MD, USA
Jacqueline Capeau Faculty of Medicine Saint Antoine, INSERM, Paris, France
Judith Currier University of California, Los Angeles, CA, USA
Stefan Mauss Center for HIV and Hepatogastroenterology, Düsseldorf, Germany
Peter Reiss Academic Medical Center, Amsterdam, the Netherlands
SCIENTIFIC COMMITTEE
Michael Dubé University of Southern California, Los Angeles, CA, USA
Julian Falutz Immune Deficiency Treatment Center, Montreal General Hospital, Montreal, Canada
Carl Grunfeld University of California Medical Center, San Francisco, CA, USA
Giovanni Guaraldi University of Modena, Modena, Italy
Colleen Hadigan National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, USA
Peter Hunt University of California at San Francisco, CA, USA
Donald Kotler Columbia University, New York, NY, USA
Ken Kunisaki University of Minnesota, Minneapolis, MN, USA
Jordan Lake The University of Texas, Houston, TX, USA
Jules Levin The National AIDS Treatment Advocacy Project, New York, NY, USA
Janet Lo Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA
Esteban Martínez IDIPAPS - Hospital Clinic, University of Barcelona, Barcelona, Spain
Mosepele Mosepele University of Botswana, Gaborone, Botswana
Graeme Moyle Chelsea and Westminster Hospital, London, UK
Reena Rajasuriar University of Malaya, Kuala Lumpur, Malaysia
Caroline Sabin University College London, London, UK
Janine Trevillyan Monash University, Melbourne, Australia
Sharon Walmsley University Health Network, Toronto, Canada
PLENARY SPEAKERS
Mohamed Abdel-Mohsen University of Pennsylvania, PA, USA
Gretchen Neigh Virginia Commonwealth University, VA, USA
Liesl Zühlke Red Cross War Memorial Children’s Hospital, South Africa
ROUNDTABLE: post-acute sequelae of SARS-CoV-2 infection Chairs:
Judith Currier University of California, Los Angeles, CA, USA
Steven Deeks University of California at San Francisco, CA, USA
Speakers & Panellists:
Keri Althoff Johns Hopkins University, Baltimore, MD, USA
Amitava Banerjee University College London, London, UK
Steven Deeks University of California at San Francisco, CA, USA
Robin Gorna NHS Long COVID Taskforce, UK,
Avindra Nath NIH, Bethesda, MD, USA
ORGANIZING SECRETARIAT
International Medical Press Admiral House 76–78 Old Street London, EC1V 9AZ, UK Tel: +44 20 7398 0700 Fax: +44 20 7398 0701 www.intmedpress.com/comorbidities; comorbidities@intmedpress.com
CME INFORMATION
Programme Overview
The Organizing Committee for the Workshop recognize the importance of SARS-CoV-2 and particularly the potential prolonged health consequences of this infection, now collectively referred to as Post-Acute Sequelae of SARS-CoV-2 infection or PASC. Therefore, the scope of the Workshop that formerly focused on co-morbidities of HIV now also includes those of SARS-CoV-2. The format and goals that have underpinned this successful meeting for 23 years remain. HIV is now viewed as a chronic and manageable condition, with comorbidity posing a greater threat than the development of AIDS. Increased risk for comorbidity brings challenges for physicians, who must learn to navigate the shifting field of HIV, particularly as the disease becomes increasingly pervasive. The COVID-19 pandemic has changed clinical practice in many therapy areas, including HIV. A key cause for concern among people living with HIV (PLWH) and treating physicians is whether PLWH are at increased risk of severe disease. Evidence on this remains uncertain, with large population-based studies coming to contradictory conclusions.
Given that individuals with HIV appear to be at increased risk of severe COVID-19 compared with people without HIV, education on the safety and long-term management of PLWH who have experienced COVID-19 infection is of increasing importance.
Globally, 1.8 million children are living with HIV. With modern antiretroviral therapy, children diagnosed with HIV are likely to live many years; there is evidence that children living with HIV, including those taking antiretroviral therapy are at increased risk of multisystem comorbidity and chronic disability. Physicians must be aware of the greater risks imposed on children and adolescents with HIV and be able to differentiate these from comorbidities which are more common in adults.
As well as being at greater risk for certain antiretroviral-therapy-associated toxicities, adults with HIV are also at increased risk of mental health disorders. In the USA, alcohol use among PLWH is associated with stress and depression, while in the EU, the suicide rate among HIV-positive individuals is three times higher than among people who do not have HIV.
The continually shifting challenges presented in the field of HIV demand that physicians maintain a high level of awareness of the most recent advances in therapy, and how best to translate this knowledge into optimum care for individuals living with HIV and its comorbidities today.
Intended Audience
This Workshop is aimed primarily at physicians, clinicians and researchers in the infectious disease field, particularly those involved in HIV/AIDS. General practitioners, nurse practitioners, physician assistants and other health-care workers are also encouraged to attend.
Learning Format
This virtual Workshop will utilize plenary lectures, oral abstract and oral poster presentations augmented by audio-visual enhancement. Each session will include a discussion session led by our expert faculty to address questions from the audience. Statements of credit will be issued to participants upon submission of evaluation forms. Please see the scientific programme for details of all 2021 Workshop sections.
Learning Objectives
Following attendance at this event, physicians will be able to:
• Identify HIV-related comorbidities in children and adolescents and recognize the importance of early intervention with antiretroviral therapy to improve outcomes
• Identify physical- and mental-health-related comorbidities among adults with HIV
• Describe the risks of COVID-19 in individuals with HIV and identify HIV-related comorbidities which may increase these risks
Accreditation Statement for Physicians
The 23rd International Workshop on Long-term Complications of HIV and SARS-CoV-2 has been accredited by the European Accreditation Council for Continuing Medical Education (EACCME®) for a maximum of 8 European CME credits (ECMEC®s).
Each medical specialist should claim only those credits that he/she actually spent in the educational activity. The EACCME® is an institution of the European Union of Medical Specialists (UEMS), www.uems.net
Through an agreement between the European Union of Medical Specialists and the American Medical Association, physicians may convert EACCME® credits to an equivalent number of AMA PRA Category 1 Credits™. Information on the process to convert EACCME® credits to AMA credits can be found at www.ama-assn.org/go/internationalcme.
Live educational activities occurring outside of Canada, recognized by the UEMS-EACCME® for ECMEC® credits are deemed to be Accredited Group Learning Activities (Section 1) as defined by the Maintenance of Certification Program of the Royal College of Physicians and Surgeons of Canada.
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of the Institute for Medical and Nursing Education (IMNE), and International Medical Press (IMP). IMNE is accredited by the ACCME to provide continuing medical education for physicians.
IMNE designates this live educational activity for a maximum of 3.25 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
ORGANIZING COMMITTEE AND PLENARY SPEAKER DISCLOSURES
It is the policy of IMP to ensure fair balance, independence, objectivity and scientific rigour in all programming. All individuals involved in planning (e.g. CME provider staff, faculty and planners) are expected to disclose any significant financial relationships with commercial interests over the past 12 months. IMP also requires that faculty identify and reference off-label products or investigational use of pharmaceutical and medical device products. All conflicts of interest have been mitigated and resolved using an external peer-review process.
Research funding: Janssen-Cilag, MSD and ViiV Healthcare
Consultancy fees or honoraria: Gilead, Janssen, ViiV Healthcare and MSD
Travel grants: Gilead, MSD and ViiV Healthcare
Judith Currier, MD
Advisory board: Merck & Co.
Patrick Mallon, MD, PhD
Research funding: Gilead and GSK
Consultancy fees or honoraria: Gilead, ViiV Healthcare and BMS
Speakers’ bureau: Gilead and BMS
Stefan Mauss, MD, PhD
Speakers’ bureau: AbbVie, BMS, Gilead, Janssen and MSD
Consultancy fees or honoraria: AbbVie, Janssen, MYR Pharma, ViiV Healthcare and MSD
Peter Reiss, MD
Research funding: Gilead Sciences, Janssen Pharmaceuticals, ViiV Healthcare and Merck
Consultancy fees or honoraria: Gilead Sciences, ViiV Healthcare, Merck and Teva Pharmaceuticals for scientific advisory board participation (all honoraria paid to Institution)
Morrie Schambelan, MD
Consultancy fees or honoraria: Novo Nordisk and Intercept Pharmaceuticals
Plenary Speakers
Mohamed Abdel-Mohsen
Nothing to disclose
Keri Althoff
Grants/research support: NIH
Consultancy fees or honoraria: Palladian Partners on behalf of NIH and Trio Health
Amitava Banerjee
Grants/research support: AstraZeneca
Judith Currier
Advisory board: Merck & Co
Steven Deeks
Grants/research support: Gilead and Merck
Consultancy fees or honoraria: AbbVie, Enochian Biosciences, GSK and Immunocore
Robin Gorna
Nothing to disclose
Avindra Nath
Nothing to disclose
Gretchen Neigh
Nothing to disclose
Liesl Zühlke
Nothing to disclose
PROGRAMME
Time (CET)
Title
Presenting author
Abstract
Monday 6 December 2021
17.00–17.05
Welcome from Session Chairs
Morrie Schambelan,
Sharon Walmsley
17.05–18.05
Roundtable and panel discussion: Post-acute sequelae of SARS-CoV-2 infection
Chairs: Judith Currier, Steven Deeks
Speakers and Panellists: Keri Althoff, Amitava Banerjee, Avindra Nath, Robin Gorna
18.05–18.15
Prevalence and characteristics of post-acute sequelae of SARS-CoV-2 (PASC) in non-hospitalized persons with COVID-19 enrolled in a clinical trial of early treatment (ACTIV-2)
Teresa H Evering
O01
18.15–18.25
Effect of HIV status on ICU admission and mortality among hospitalized coronavirus disease 2019 (COVID-19) patients
Yaa Adoma Kwapong
O02
18.25–18.35
Identification of distinct long COVID clinical phenotypes through cluster analysis of self-reported symptoms
Grace Kenny
O03
18.35–18.55
Round table panel discussion
18.55–19.35
Poster session
Stefan Mauss, Janet Lo
Impact of COVID pandemic and COVID disease on aging trajectories in elderly residents in nursing homes
Giovanni Guaraldi
P01
Residual symptoms and the quality of life in individuals recovered from COVID-19 infection: a survey from Pakistan
Mohammad Aadil Qamar
P02
The mystery of COVID-19 reinfections: a global systematic review and meta-analysis of 577 cases
Mohammad Aadil Qamar
P03
Voice assistance to develop a participatory research and action to improve health trajectories of people with PACS
Giovanni Guaraldi
P04
Poster discussion
Tuesday 7 December 2021
17.00–17.05
Welcome from Session Chairs
Todd Brown, Flavia Kiweewa Matovu
17.05–17.35
Plenary: Breaking the glyco-code of HIV immunopathogenesis
Mohamed Abdel-Mohsen
17.35–17.45
Markers of immune activation and inflammation in individuals with post-acute sequelae of SARS-CoV-2 infection
Michael Peluso
O04
17.45–17.55
Impact of the SARS-CoV-2 epidemic outbreak on prevention and care for HIV and other sexually transmitted infections at a large Spanish hospital
Esteban Martínez
O05
17.55–18.05
In vitro modelling of the therapeutic impact of ApoA-I mimetics on atherogenesis in post-acute COVID-19 syndrome
Theodoros Kelesidis
O06
18.05–18.15
Non-obese NAFLD is associated with higher sCD14 concentrations in adults with HIV
Jordan Lake
O07
18.15–18.25
Some INSTIs inhibit the beiging capacity of white adipose tissue in vivo and in vitro, resulting in dysfunctional hypertrophic adipose tissue
Kenza Ngono Ayissi
O08
18.25–18.35
Prevalence of functional limitation and evaluation of independency in people living with HIV at the Treichville University Hospital in Abidjan
Nadine Etoundi
O09
18.35–18.55
Panel discussion
18.55–19.35
Poster session
Jacqueline Capeau, Peter Hunt
Abacavir induces an increase in leukocyte-endothelium crosstalk in blood from HIV-infected patients
Maria Amparo Blanch Ruiz
P05
Impact on inflammatory and atherogenesis biomarkers with the 2-drug regimen dolutegravir plus lamivudine in treatment-experienced people with HIV-1: a systematic literature review
Josep M Llibre
P06
Cytokine-based predictive model of pulmonary function trajectories in people living with HIV
Ioannis Konstantinidis
P07
Cardiovascular risk knowledge stratified by predicted cardiovascular risk level in an HIV clinical cohort
Bernard Morapedi
P08
Poster discussion
Wednesday 8 December 2021
17.00–17.05
Welcome from Session Chairs
Paddy Mallon, Caroline Sabin
17.05–17.35
Plenary: Impact of stress on integrative health and disease
Gretchen Neigh
17.35–17.45
Weight gain of >10% after switching to TAF and/or INSTI is common in ATHENA cohort participants with HIV and suppressed viraemia, especially in women and those switching simultaneously to TAF and INSTI
Myrthe Lauriëtte Verburgh
O10
17.45–17.55
Factors associated with cardiometabolic parameters at 3 years in the TANGO Study, comparing a switch to dolutegravir/lamivudine vs maintenance of tenofovir alafenamide-based regimens
Rachel Batterham
O11
17.55–18.05
Abnormal transcriptomic profile of epicardial adipose tissue of people living with HIV: results from the PIECVIH study
Franck Boccara
O12
18.05–18.15
Depot medroxyprogesterone acetate is associated with lower bone mass and higher central fat in young women on tenofovir disoproxil fumarate-containing ART
Flavia Kiweewa Matovu
O13
18.15–18.25
HCV viraemia is associated with reduced hip bone mineral density and strength among African Americans with and without HIV infection
Jing Sun
O14
18.25–18.35
Frailty among people living with HIV in Botswana, sub-Saharan Africa
Ponego Lloyd Ponatshego
O15
18.35–18.55
Panel discussion
18.55–19.35
Poster session
Esteban Martínez, Ken Kunisaki
An analysis of insomnia by sex and age in people living with HIV
Christine Horvat Davey
P09
COVID-19, what impact on the mental health of students of the Faculty of Medicine and Pharmacy of Agadir?
Imane Sellam
P10
SARS CoV-2 seroprevalence and COVID-19 experience among people with HIV in India
Rifa Tazyeem Khan
P11
Poster discussion
Thursday 9 December 2021
17.00–17.05
Welcome from Session Chairs
Peter Reiss, Colleen Hadigan
17.05–17.35
Plenary: Children and adolescents: focus on HIV-associated co-morbidities – what will the future hold?
Liesl Zühlke
17.35–17.45
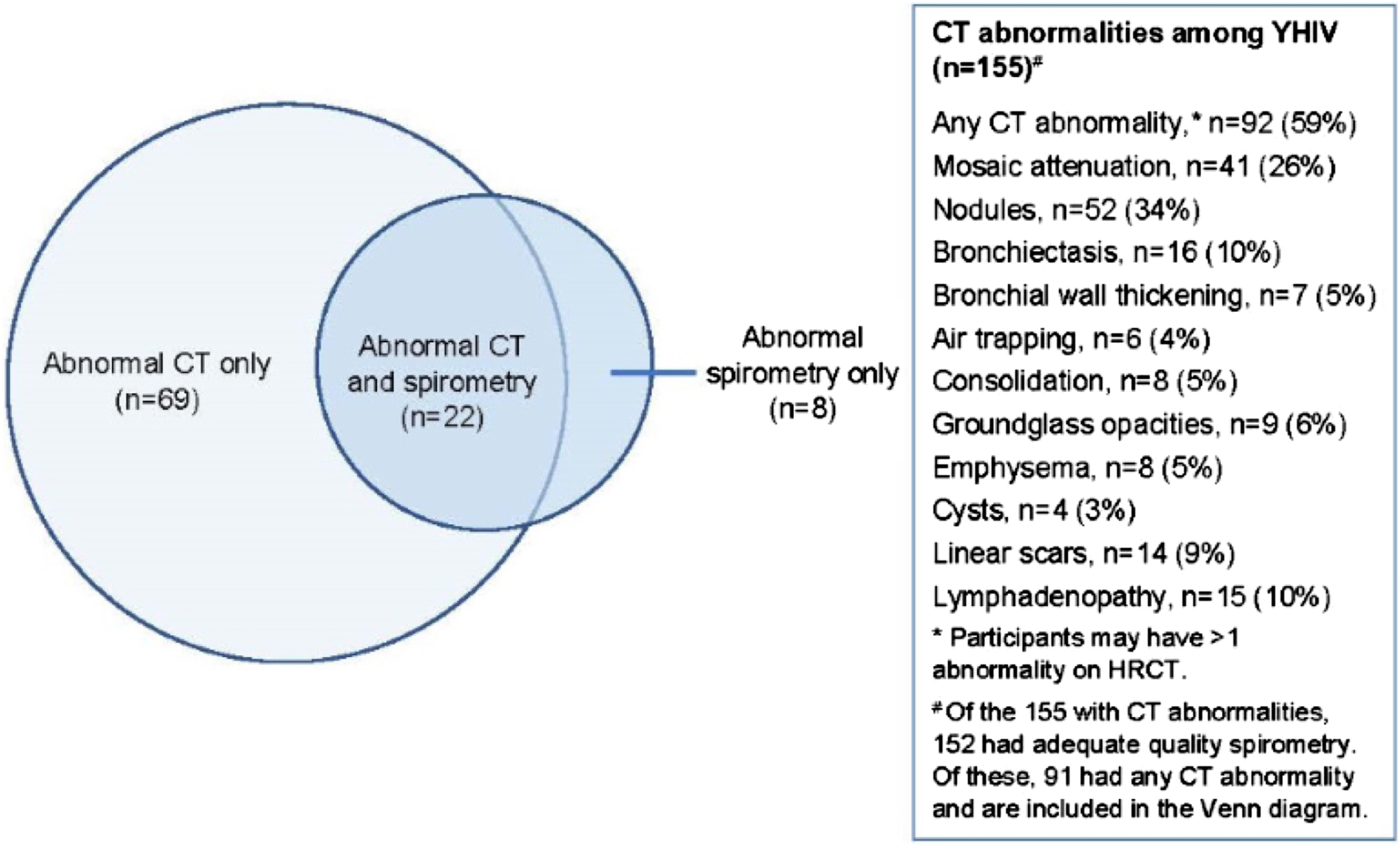
Abnormal spirometry and HRCT are common among youth with HIV in Nairobi, Kenya
Engi F Attia
O16
17.45–17.55
Trends in diabetes incidence and associated risk factors among people living with HIV in the current treatment era, 2008–2018
Amanda Willig
O17
17.55–18.05
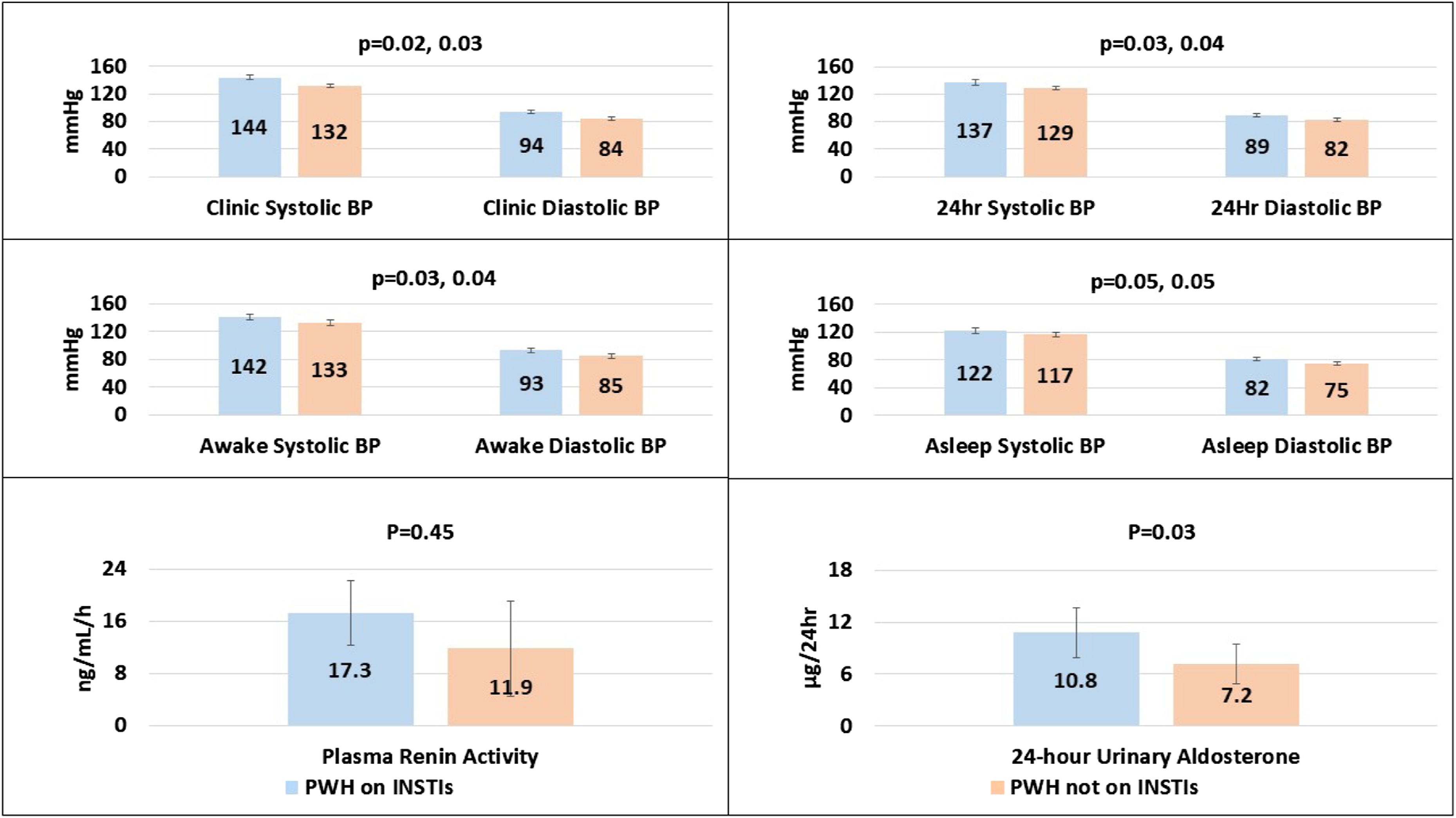
Integrase strand transfer inhibitors are associated with higher blood pressure and renin-angiotensin-aldosterone system activity
Mohammed Siddiqui
O18
18.05–18.15
Associations between HIV status and hypertension status in a high HIV prevalence population in Manicaland: a cross-sectional study of adults
Katherine Davis
O19
18.15–18.25
Inflammatory markers associated with cardiac fibrosis in people with HIV: Myocardial And Coronary Abnormalities in HIV Infection (MACHIN) Study
Hossein Bahrami
O20
18.25–18.35
Automatic retinal image analysis to predict coronary artery disease in at-risk people living with HIV
Grace Lui
O21
18.35–18.55
Panel discussion
18.55–19.35
Poster session
Julian Falutz, Giovanni Guaraldi
Increase in pro-atherogenic apolipoprotein B in people living with HIV (PLWH) following switch from tenofovir disoproxil fumarate to tenofovir alafenamide
Stefano Savinelli
P12
Patient-reported outcomes after switching to a 2-drug regimen of fixed-dose combination dolutegravir/lamivudine: 48-week results from the SALSA Study
Princy Kumar
P13
Assessment of coronary inflammation in antiretroviral treated people living with HIV infection and active HIV/HCV coinfection
Shashwatee Bagchi
P14
Depression and anxiety symptoms, treatment utilization, and virological failure among adults with HIV in rural Florida
Preeti Manavalan
P15
Poster discussion
19.35
Meeting close
MONDAY 6 DECEMBER – ORAL PRESENTATIONS
ABSTRACT O01
Prevalence and characteristics of post-acute sequelae of SARS-CoV-2 (PASC) in non-hospitalized persons with COVID-19 enrolled in a clinical trial of early treatment (ACTIV-2)
TH Evering1, B Sanusi2, N Jilg3, E Yeh2, C Moser2, J Ritz2, D Wohl4, ES Daar5, P Klekotka6, AC Javan7, JJ Eron4, J Currier8, M Hughes2, D Smith9, KW Chew8, the ACTIV-2/A5401 Study Team and Investigators
1Weill Cornell Medicine, New York, NY, USA; 2Harvard T.H. Chan School of Public Health, Boston, MA, USA; 3Massachusetts General Hospital, Boston, MA, USA; 4University of North Carolina, Chapel Hill, NC, USA; 5Lundquist Institute at Harbor-UCLA Medical Center, Torrance, CA, USA; 6Eli Lilly and Company, San Diego, CA, USA; 7National Institutes of Health, Bethesda, MD, USA; 8David Geffen School of Medicine at UCLA, Los Angeles, CA, USA; 9University of California San Diego, San Diego, CA, USA
Objectives/aim: Many persons with SARS-CoV-2 experience clinical symptoms beyond acute infection, often termed ‘long COVID’ or ‘post-acute sequelae of SARS-CoV-2 infection (PASC)’. PASC studies embedded within COVID-19 therapeutics trials provide a unique opportunity to describe the incidence, symptom burden, and impact of different antiviral therapies on PASC prevalence.
Methods: ACTIV-2 evaluates the safety and efficacy of investigational agents for the treatment of non-hospitalized adults with mild to moderate COVID-19 in a Phase 2/3 platform trial. In the inaugural Phase 2 portion, participants in the US were randomized within 10 days of symptom onset and a positive test for SARS-CoV-2 to receive the SARS-CoV-2 anti-spike monoclonal antibody bamlanivimab or placebo as a single infusion at 7,000 mg (n=94) or 700 mg (n=225). In a subsequent single-arm open-label study, 1059 participants received 700 mg of bamlanivimab. Participants completed a 13-symptom daily diary from enrollment through day 28. A long-term (LT) symptom diary with 14 additional symptoms was introduced after the study was underway and a subset of individuals completed these during follow-up every 12 weeks starting at week 12 on study. We report initial findings from available week 24 data.
Results: 605 participants enrolled August 2020 to February 2021 completed the LT diary at their 24-week visit (Phase 2: 7000 mg versus placebo (n=25); 700 mg versus placebo (n=68); open-label cohort: 700 mg (n=512)). Median age of respondents was 50 years (quartiles: 39, 60), 51% were female, 5% Black/African American, and 35% Hispanic/Latino. At study enrollment, 53% reported at least 1 high-risk comorbidity, and 0.3% were vaccinated against COVID-19. By week 24, 14% (87/605) of respondents self-reported that they had not returned to their pre-COVID-19 health with most common symptoms in this group being fatigue and smell disorder (45% and 36%, respectively). Other symptoms included breathing difficulties (30%), taste disorders (25%), musculoskeletal pain (26%) or weakness (23%), and cognitive complaints including difficulty concentrating/thinking (30%), difficulty reasoning and solving problems (21%), memory loss (25%) and insomnia (23%). Most reported their symptoms as ‘mild’. 57% (50/87) reported the presence of three or more PASC symptoms at week 24. Exploratory analyses have not shown differences in rates of reported PASC symptoms between bamlanivimab and placebo groups.
Conclusion(s)/discussion: In this study of outpatients with mild to moderate COVID-19, 14% reported that they had not returned to pre-COVID-19 health by 24 weeks after initial SARS-CoV-2 infection, with generally mild but multiple symptoms and no obvious differences between those treated with bamlanivimab versus placebo. Larger placebo-controlled studies within ACTIV-2 will allow us to further assess the potential for early antiviral therapies to mitigate PASC.
ABSTRACT O02
Effect of HIV status on ICU admission and mortality among hospitalized coronavirus disease 2019 (COVID-19) patients
YA Kwapong1, G Sharma1, J Shade2, DA Piggott3, TT Brown4, KC Wu5, AG Hays1
1Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Diseases, Johns Hopkins School of Medicine, Baltimore, MD, USA; 2Department of Biomedical Engineering, Johns Hopkins University, Baltimore, MD, USA; 3Division of Infectious Diseases, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 4Division of Endocrinology, Diabetes and Metabolism, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 5Division of Cardiology, Johns Hopkins University School of Medicine, Baltimore, MD, USA
Objective: It is not well known if people living with HIV (PLWH), admitted for coronavirus disease-2019 (COVID-19) suffer worse outcomes than HIV seronegative individuals. We aimed to evaluate intensive care unit (ICU) admission and mortality in individuals hospitalized for COVID-19 comparing PLWH to two age-matched HIV seronegative controls: HIV- immunocompetent and HIV- immunocompromised adults.
Methods: In this case-control study, we utilized data from the Johns Hopkins COVID-19 Precision Medicine Analytics Platform (JH-CROWN) Registry. The main outcome measures were ICU admission and mortality. Multivariate logistic regression models were performed to identify risk factors for ICU admission and mortality: unadjusted (model 1), adjusted for age, race, gender (model 2), additionally adjusted for hypertension, diabetes mellitus, body mass index (model 3), and further adjusted for chronic renal failure, congestive heart failure, chronic pulmonary disease and hepatitis C virus (model 4).
Results: A total of 463 patients hospitalized with COVID-19 were included: PLWH (n=151), HIV- immunocompetent adults (n=185) and HIV- immunocompromised adults (n=127). Among PLWH (mean age 53 ±14 years), the median CD4 count was 210 (Q1: 100, Q3: 375) and median HIV viral load was 0 (Q1: 0, Q3: 2,278). Compared to HIV- immunocompetent and HIV- immunocompromised adults respectively, PLWH had a higher prevalence of liver disease (35% versus 14% versus 23%), chronic pulmonary disease (44% versus 27% versus 37%; P=0.003), recreational drug use (29% versus 9% versus 15%), and hepatitis C (25% versus 4% versus 7%; all P<0.001) and were more likely to be current smokers (21% versus 15% versus 8%; P=0.009; Figure 1a). The odds of ICU admission were higher in PLWH compared to HIV- immunocompetent patients in the unadjusted model (OR 1.59, 95% CI: 1.03, 2.45) and after adjusting for age, sex, and race (OR 1.64, 95% CI: 1.04, 2.59) but there was no significant difference after further adjusting for body mass index, hypertension and diabetes mellitus (OR: 1.15, 95% CI: 0.69, 1.91). The odds of ICU admission in PLWH were however not different from HIV- immunocompromised patients. Hypertension and diabetes mellitus were predictive of ICU admission among all the groups (Figure 1b). Liver disease was predictive of ICU admission in PLWH but not in HIV seronegative controls. The odds of mortality among PLWH were similar to that of both control groups (fully adjusted model: PWLH versus HIV- immunocompetent OR 1.02, 95% CI: 0.33, 3.16; PWLH versus HIV- immunocompromised OR 0.65, 95% CI: 0.23, 1.82).
Conclusions: Among this hospitalized cohort of COVID-19 patients, PLWH had a higher prevalence of liver disease, chronic pulmonary disease, smoking and recreational drug use compared to age-matched HIV seronegative patients. PLWH had higher odds of ICU admission, but not mortality, compared to matched HIV- immunocompetent patients whereas there were no differences in mortality and ICU admission between PLWH and HIV- immunocompromised patients. Further studies may be needed to determine whether the extent or duration of recovery form COVID-19 differs by HIV status.
Abstract O02
ABSTRACT O03
Identification of distinct long COVID clinical phenotypes through cluster analysis of self-reported symptoms
G Kenny1,2, K McCann2, C O’Brien3, C O’Broin1,2, S Savinelli1,2, W Tinago1, O Yousif4, JS Lambert1,3,5, E Feeney1,2, E de Barra6,7, P Doran3, PWG Mallon1,2, the AIID Cohort Study
1Centre for Experimental Pathogen Host Research, University College Dublin, Dublin, Ireland; 2St Vincent’s University Hospital, Dublin, Ireland; 3School of Medicine, University College Dublin, Dublin, Ireland; 4Wexford General Hospital, Wexford, Ireland; 5Mater Misericordiae University Hospital, Dublin, Ireland; 6Beaumont Hospital, Beaumont, Dublin 9, Ireland; 7Department of International Health and Tropical Medicine, Royal College of Surgeons in Ireland, Dublin, Ireland
Aim: Long COVID poses a significant new challenge to global health services. This study aimed to describe self-reported symptoms from individuals with a range of initial COVID-19 disease severities presenting with long COVID, to identify patterns in presentations and correlate these with clinical observations and functional impairment.
Methods: Within the multi-centre, prospective All-Ireland Infectious Diseases Cohort study, we selected individuals with a PCR confirmed diagnosis of SARS-CoV-2 infection and symptoms persisting more than 4 weeks from acute onset of COVID-19. We performed a multiple correspondence analysis (MCA) on the commonest, self-reported symptoms and hierarchical clustering on the results of the MCA to identify symptom clusters. We then compared objective clinical findings and test results, including health-related quality of life (using SF36), Medical Research Council (MRC) dyspnoea scores and reported absence from work due to illness. Quantitative and qualitative variables were compared between clusters using the Kruskall-Wallis test and Chi square tests respectively. Data are median (IQR) unless otherwise stated.
Results: 233 individuals were included; age 43 (36–54) years, 74% were female and 77.3% reported a mild initial COVID-19 (as per World Health Organisation severity grading). Time from onset of acute COVID-19 to assessment was 18.14 (10.43–28.57) weeks. MCA and hierarchical clustering on the 12 most common symptoms revealed 3 clusters. Cluster 1 had predominantly musculoskeletal and pain symptoms, including higher proportions of joint pain, myalgia and headache, and cluster 2 had a preponderance of cardiorespiratory symptoms (chest pain, breathlessness and palpitations) and poor concentration. In contrast, cluster 3 reported significantly fewer symptoms (2 (2–3) symptoms per individual in cluster 3 versus 6 (5–7) and 4 (3–5) in clusters 1 and 2 respectively; P<0.001). Cluster 2 had the most abnormal cardiac findings including all individuals with an imaging confirmed diagnoses of pericarditis (n=6) or myocarditis (n=3), and the highest proportion of tachycardic individuals (13% in cluster 2 versus 6% and 7% in clusters 1 and 3), although this was not statistically significant (P=0.3). Clusters 1 and 2 had greater functional impairment demonstrated by significantly longer work absence (cluster 1; 10 (7.5–24) weeks, cluster 2; 12 (6–24)weeks versus and 6 (2–12) weeks in clusters 3, P≤0.01), higher MRC dyspnoea scores (cluster 1; 2 (2–3), cluster 2; 3 (2–3) and cluster 3; 1 (1–2) respectively; P≤0.01), and lower scores in SF-36 domains of general health, physical functioning, and role limitation due to physical functioning and social functioning (all P<0.05). See Figure 1.
Discussion: We have identified distinct phenotypic clusters in individuals presenting with long COVID that correlate with clinical observations and functional impairment. These data suggest the potential for contrasting pathophysiologic mechanisms associated with these phenotypes, that may require different therapeutic pathways.
Hierarchical clustering of symptoms in individuals presenting with long COVID (Abstract O03)
MONDAY 6 DECEMBER – POSTER PRESENTATIONS
ABSTRACT P01
Impact of COVID pandemic and COVID disease on aging trajectories in elderly residents in nursing homes
S Braglia¹, G Dolci², G Guaraldi², B Manni¹, J Milic², C Mussi³, A Fabbo¹
¹Geriatric Service- Cognitive Disorders and Dementia Unit, Health Authority and Services of Modena; ²Infectious Diseases Clinic, University of Modena and Reggio Emilia, Modena, Italy; ³Geriatric Clinic, Biomedical Science, Methabolism and Neuroscience, University of Modena and Reggio Emilia, Modena, Italy
Objectives: The impact of both COVID pandemic and COVID disease on aging trajectories in elderly residents in nursing homes is still unexplored. The objective was to describe aging trajectories, depicted by frailty, polypharmacy, cognitive status, physical impairment and disability, in the elderly residents in nursing homes between March 2019 and October 2020.
Methods: This was a retrospective, multicentric observational cohort study that enrolled residents of four nursing homes in Modena province, Northern Italy. Patients were divided into two groups (COVID-19 and non-COVID-19) according to COVID-19 disease acquisition. Weight, frailty, polypharmacy, cognitive status, disability were collected at four time points: March 2019 (T0), October 2019 (T1), May 2020 (T2) and October 2020 (T3). COVID-19 cases occurred between T1 and T2 period. Frailty was assessed by clinical frailty scale (CFS), cognitive status by MMSE questionnaire, physical impairment with cumulative illness rating scale (CIRS) and disability by activities of daily living (ADL) questionnaire. Polypharmacy was defined through the total number of currently used drugs. T-test for independent samples was used to compare residents of nursing homes with or without COVID-19. The effect of COVID-19 infection on changes in aging trajectories over time was tested in the mixed linear model. Statistical analysis was performed using StataIC 16.1.
Results: Out of 107 residents included in the study, 15 patients died during the observational period in the COVID-19 group (versus 0). The patients’ characteristics at T0 in the COVID-19 and non-COVID-19 groups are described in Table 1. Overall, the change of CFS score was higher between T1-T2 than between T0-T1 (mean delta CFS T2-T1= 0.101, 95% CI 0.088, 0.114 versus mean delta CFS T1-T0= 0, 95% CI -0.008, 0.008; P<0.001). In particular, CFS increase was higher in COVID-19 group (0.232 versus -0.07; P=0.02). In the entire study population, weight change between T1-T2 was different to weight change between T0-T1 (mean delta weight -1.37 versus mean delta weight 0.88; P<0.001). CIRS score change was significantly higher in the period T2-T3 than in a period T1-T2 (0.03, 95% CI -0.03, 0.09 versus 0.23, 95% CI 0.14, 0.33; P<0.001). In detail, COVID-19 group had higher increase in the CIRS score in the T2-T3 period (0.469 versus -0.022; P<0.001). The interaction between time and COVID-19 infection was significantly correlated with frailty change over time (log likelihood -676.912; P=0.017) but not with body weight, polypharmacy, dementia, disability in a mixed linear model.
Conclusions: Aging trajectories of nursing home residents were negatively affected by COVID-19 pandemic, independently of COVID-19 disease. This phenomenon was more accentuated in the patients who had COVID-19, in particularly depicted by higher mortality, frailty progression and increase in polypharmacy.
Abstract P01
ABSTRACT P02
Residual symptoms and the quality of life in individuals recovered from COVID-19 infection: a survey from Pakistan
MA Qamar1, RS Martins2, RA Dhillon3, A Tharwani2, O Irfan4, QF Suriya5, JA Khan6, ABS Zubairi6, W Rizwan7
1Ziauddin University, Karachi, Pakistan; 2Medical College, Aga Khan University, Karachi, Pakistan; 3Medical College, Riphah International University, Pakistan; 4Centre for Global Child Health, Hospital for Sick Children, Toronto, Canada; 5Aga Khan University Hospital, Karachi, Pakistan; 6Department of Pulmonology, Aga Khan University Hospital, Karachi, Pakistan; 7Pediatrics, The Children Hospital and Institute of Child Health, Lahore, Pakistan
Objectives: A scarcity of literature remains regarding the patient’s health post COVID-19 infection. This study aims to fill this gap by assessing the prevalence of residual symptoms and quality of life (QoL) after COVID-19.
Methods: An anonymous online survey was administrated all over Pakistan from November 2020 to April 2021, COVID-19 survivors. The questionnaire used the 12-Item Short Form Health Survey (SF-12) to assess mental and physical quality of life (QoL). Multivariate linear regression was used to explore factors associated with mental and physical QoL scores.
Results: A total of 331 COVID-19 survivors were included. The commonest residual symptoms were body aches (39.9%), low mood (32.6%), and cough (30.2%). Better physical QoL was associated with being male (adjusted beta: 3.328) and having no residual symptoms (6.955). However, suffering from nausea/vomiting during initial COVID-19 infection (-4.026), being admitted to the ICU during COVID-19 infection (-9.164), and suffering from residual body aches (-5.209), low mood (-2.959), and chest discomfort (-4.842), was associated with poorer quality of life. Better mental QoL was associated with being asymptomatic during initial COVID-19 infection (6.149) and post-COVID (6.685), while experiencing low mood post-COVID was associated with poorer mental quality of life (-8.253 [-10.914, -5.592]).
Conclusions: Despite supposed ‘recovery’ from COVID-19, patients still face a wide range of residual symptoms months after initial infection, which contributes towards poorer QoL. Healthcare professionals must remain alert to the long-lasting effects of COVID-19 infection and aim to address them appropriately to improve patients’ QoL.
ABSTRACT P03
The mystery of COVID-19 reinfections: a global systematic review and meta-analysis of 577 cases
RA Dhillon1*, MA Qamar2*, O Irfan3, JA Gilani4, U Waqar5, MI Sajid5, SF Mahmood6
1Medical College, Riphah International University, Rawalpindi, Pakistan; 2Ziauddin University, Karachi, Pakistan; 3Centre for Global Child Health, Hospital for Sick Children, Toronto, Canada; 4Aga Khan University Hospital, Karachi, Pakistan; 5Medical College, Aga Khan University, Karachi, Pakistan; 6Section of Infectious Diseases, Aga Khan University, Karachi, Pakistan
*Contributed equally
Objectives: With disparities in vaccination, emergence of reinfection/reactivation cases coupled with newer waves and variants of COVID-19, we conducted a systematic review to assess the determinants and disease spectrum of COVID-19 reinfection.
Methods: A comprehensive search covering relevant databases was conducted for observational studies reporting polymerase chain reaction (PCR) confirmed infection and reinfection cases. Meta-analyses were performed using RevMan 5.3 for pooled proportions of findings in first infection and reinfection with 95% confidence interval (CI).
Results: Eighty-one studies reporting 577 cases were included from 22 countries. The mean age of study population was 46.2 ±18.9 years with males accounting for 45.8% while 179 (31.0%) cases of comorbidities were reported. The average time duration between first infection and reinfection was 63.6 ±48.9 days. During first infection and reinfection, fever was the most common symptom (41.4% and 36.4%, respectively) whilst antiviral therapy was the most common treatment regimen administered (44.5% and 43.0%, respectively). Overall, comparable odds of symptomatic presentation and management were reported in the two infections. However, a higher intensive care unit (ICU) admission rate was observed in reinfection compared to first infection (10 versus 3). Ten deaths were reported with 565 patients fully recovering. Respiratory failure was the most common cause of death (7/10 deaths).
Conclusions: As the first global-scale systematic review of its kind, our findings support immunization practices given increased ICU admissions and mortality in reinfections. Our cohort serves as a guide for clinicians and authorities for devising an optimal strategy for controlling the pandemic.
ABSTRACT P04
Voice assistance to develop a participatory research and action to improve health trajectories of people with PACS
A Caselgrandi1, J Milic2, F Motta2, M Belli1, M Venuta1, E Aprile1, L Gozzi2, G Burastero1, V Iadisernia1, D Yaacoub1, M Orsini3, M Pacchioni3, E Mescoli3, C Mussini2, G Guaraldi2
1Policlinico di Modena, Azienda Ospedaliero-Universitaria, Modena, Italy; 2Department of Surgical, Medical, Dental and Morphological Sciences, University of Modena and Reggio Emilia, Modena, Italy; 3DataRiver S.r.l., Modena, Italy
Background: First objective was to evaluate changes in health trajectories at 6 months follow-up in older people with post-acute COVID syndrome (PACS), prospectively evaluated with a multidimensional assessment of clusters of PACS symptoms, frailty and HRQoL. Secondary objective was to assess patients’ satisfaction and engagement in this participatory research and action study, in which a voice assistant (VA) tool was used to empower people with PACS.
Methods: This study included 50 consecutive patients, aged >50 years, previously hospitalized in March–April 2020 for severe COVID pneumonia attending Modena PACS clinic in February 2021. PACS was defined as the persistence of ≥1 cluster of symptoms, including respiratory, neurocognitive, musculoskeletal, psychological, sensory and dermatological. Enrolled patients used for 6 months a Google Nest Mini VA tool. This tool was engineered (1) to collect patient reported outcomes, (2) to promote healthy lifestyles, (3) to provide brief records about PACS and how to treat it, and (4) to collect narrative medicine records. The following patients reported outcomes (PROs) were evaluated with questionnaires at baseline and at 6-month follow-up: Depression Anxiety Stress Scale (DASS-21), Connor-Davidson Resilience Scale (CD-RISC-25), SUNFRAIL, Quality of Life (EQ-5D-5L), Insomnia Severity Index (ISI), General Health Survey (SF-36). Clinical data included frailty phenotype and assessment for sarcopenia with hand grip measured with dynamometer. At follow-up participants were asked to evaluate their satisfaction with the VA tool. Patients’ empowerment was assessed with the proportion of people acquiring a normal caloric and normal protein diet, and reduction of sedentary life and engagement with moderate and vigorous physical activity.
Results: Enrolled patients were 39 (78%) males, median age was 63 years old. 2 patients (aged >75 years) withdrew the study (4%). Table 1 shows improvements in anthropometric, symptoms, and PROs data. Patients’ satisfaction was evaluated as following: 96% of participants considered VA useful, among them: 56% appraised all the 4 utilities, 27% PROs collection in particular, 11% lifestyle promotion in particular. Moreover 44% used VA for entertainment and to cope with loneliness. Patients’ empowerment was evaluated as following: 6.4% of participants modified diet from hypercaloric to adequate caloric intake and 8.3% from hypo-protein to normal protein intake. 48% participants modified sedentary life, in detail 46% increased moderate physical activity and 22% increased vigorous physical activity, respectively.
Conclusions: In this pilot study, PACS cluster symptoms, frailty and HRQoL improved at 6 months follow up. VA tool was appraised and contributed to empower people with PACS improving lifestyle, in particular physical activity.
Funding: The study was funded by Azione Finalizzata 2020, Ministero della salute di Italia (project code: WFR: COVID-2020-12371808).
Abstract P04
TUESDAY 7 DECEMBER – ORAL PRESENTATIONS
ABSTRACT O04
Markers of immune activation and inflammation in individuals with post-acute sequelae of SARS-CoV-2 infection
M Peluso1, S Lu2, A Tang1, MS Durstenfeld3, H Ho4, SA Goldberg2, CA Forman1, SE Munter5, R Hoh1, V Tai1, A Chenna6, BC Yee6, JW Winslow6, CJ Petropoulos6, B Greenhouse1, PW Hunt5, PY Hsue3, JN Martin2, JD Kelly2, DV Glidden2, SG Deeks1*, TJ Henrich5*
1Division of HIV, Infectious Diseases, and Global Medicine, University of California, San Francisco, CA, USA; 2Department of Epidemiology and Biostatistics, University of California, San Francisco, CA, USA; 3Division of Cardiology, University of California, San Francisco, CA, USA; 4Icahn School of Medicine at Mount Sinai, New York, NY, USA; 5Division of Experimental Medicine, University of California, San Francisco, CA, USA; 6Monogram Biosciences Inc., South San Francisco, CA, USA
*Contributed equally
Objectives/aim: The biological processes associated with post-acute sequelae of SARS-CoV-2 infection (PASC) are unknown. We aimed to characterize markers of immune activation in a cohort of individuals with PASC at >90 days following COVID-19 symptom onset.
Methods: Using the highly sensitive Simoa immunoassay platform, we measured soluble markers of inflammation (TNF-alpha, IL-6, IL-10, MCP-1, IP-10, IFN-gamma) and antibodies against the SARS-CoV-2 receptor binding domain (RBD) in the San Francisco-based Long-term Impact of Infection with Novel Coronavirus (LIINC) SARS-CoV-2 recovery cohort at early recovery (<90 days) and late recovery (>90 days) timepoints. These analytes were selected based on their relevance in acute COVID-19. All individuals (n=121) had prior SARS-CoV-2 infection confirmed with nucleic acid amplification testing, were recruited through clinician or self-referral, and completed detailed symptom questionnaires during recovery. We defined PASC as the presence of one or more COVID-19-attributed symptoms beyond 90 days. We compared fold-changes in marker values between those with (n=48) and without (n=73) PASC using mixed effects models with terms for PASC and early and late recovery time periods.
Results: During early recovery, those who went on to develop PASC generally had higher levels of cytokine biomarkers including TNF-alpha (1.14-fold higher mean ratio, 95% CI 1.01, 1.28; P=0.028) and IP-10 (1.28-fold higher mean ratio, 95% CI 1.01, 1.62; P=0.038). Among those with PASC, there was a trend toward higher IL-6 levels during early recovery (1.28-fold higher mean ratio, 95% CI 0.98-1.70; P=0.07) which became more pronounced in late recovery (1.44-fold higher mean ratio, 95% CI: 1.11, 1.86; P<0.001). These differences were maintained when adjusting for age, sex, prior hospitalization status, history of autoimmune disease, and body mass index. Differences were more pronounced among those with a greater number of PASC symptoms. See Figure 1.
Conclusions: Persistent immune activation may be associated with ongoing symptoms following COVID-19. While the magnitude of the elevations detected was not dramatic, the direction was consistent across markers and suggests that these subtle immunologic differences warrant further investigation. Further characterization of these processes might identify therapeutic targets for those experiencing PASC.
Abstract O04
ABSTRACT O05
Impact of the SARS-CoV-2 epidemic outbreak on prevention and care for HIV and other sexually transmitted infections at a large Spanish hospital
E de Lazzari1,2,3, A Martínez-Mimbrero3, I Chivite1,2,3, A González-Cordón1,2,3, MM Mosquera3,4,5, M Laguno1,2,3, J Costa3,4,5, J Bosch3,4,5, JL Blanco1,2,3, M Álvarez-Martinez3,4,5, A Ugarte1,2,3, A Inciarte1,2,3, L de la Mora1,2,3, B Torres1,2,3, M Martínez-Rebollar1,2,3, J Ambrosioni1,2,3, E Fernández1,2,3, JC Hurtado4,5, J Mallolas1,2,3, JM Miró1,2,3, MA Marcos3,4,5, E Martínez1,2,3
1Departament of Infectious Diseases, HIV Unit, Hospital Clínic, Barcelona, Spain; 2Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain; 3University of Barcelona, Barcelona, Spain; 4Departament of Microbiology, Hospital Clínic, Barcelona, Spain; 5Barcelona Institute for Global Health (ISGlobal), Barcelona, Spain
Introduction: Routine medical care was drastically affected by the overwhelming irruption of COVID-19 pandemic. We comprehensively assessed the impact of the COVID-19 pandemic on the prevention and care for HIV and other sexually transmitted infections from the perspective of a major hospital providing preventive and clinical services.
Methods: We retrospectively compared clinical and laboratory data from March to December 2020 (first 10 months of the SARS-CoV-2 epidemic in Spain) versus the same period in 2019 in the setting of Hospital Clínic, Barcelona (Spain). Monthly clinical data on HIV pre-exposure and post-exposure prophylaxis users and on adults with HIV infection were retrieved from the administrative hospital database. Monthly tests for HIV, hepatitis B and C, Treponema pallidum, Neisseria gonorrhoeae and Chlamydia trachomatis, and plasma lipids and glucose were recovered from the laboratory database. De novo HIV, hepatitis B or hepatitis C diagnosis were considered whenever a person had a first known positive laboratory test.
Results: There were less (28% reduction) but more advanced (mean [sd] CD4 cell counts per mm3 at HIV diagnosis 305 [167] versus 370 [170]; P<0.001; 26 [18%] persons had AIDS-defining conditions at HIV diagnosis versus 20 [10%]; P=0.03) HIV cases and more gonorrhoea (39% increase; P<0.001) and chlamydia (37% increase; P<0.001) infections in 2020 versus 2019. In people with HIV, rates of viral load above the level of detection remained stable (11% versus 11%; P=0.147) despite less scheduled visits (25% reduction; P<0.001). However, they had less antiretroviral prescription changes (10% reduction; P=0.018), worse plasma lipids (mean total cholesterol 190 versus 185 mg/dl; P<0.001; mean LDL cholesterol 114 versus 110 mg/dl; P<0.001; mean triglycerides 136 versus 125 mg/dl; P<0.001; mean HDL cholesterol 47 versus 48 mg/dl; P=06), and an excess of mortality (29 deaths versus 11, 264% increase; P=0.006) due in great part to COVID-19 (n=11) but also to other non-COVID-19 causes.
Conclusions: In our setting SARS-CoV-2 epidemic was associated with an increase of some prevalent sexually transmitted infections, with less but more advanced de novo HIV infections, and with worse non-virological health care outcomes and higher mortality in people living with HIV.
ABSTRACT O06
In vitro modelling of the therapeutic impact of ApoA-I mimetics on atherogenesis in post-acute COVID-19 syndrome
M Sharma1, H Vasilopoulos1, M Daskou1, T Kelesidis1
1Department of Medicine, Division of Infectious Diseases, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA
Objectives/aim: The mechanisms that drive SARS-CoV-2-related cardiovascular complications of post-acute COVID-19 syndrome (PACS) such as atherosclerotic cardiovascular disease (CVD) remain unclear. Mechanistic experimental models are urgently needed to model atherogenesis in the setting of PACS and to test novel therapeutic agents. We have previously shown that the ApoA-I mimetic peptide 4F attenuates in vitro replication of SARS-CoV-2, associated apoptosis, oxidative stress and inflammation in epithelial cells. Given that aberrant persistent viral reservoirs in macrophages, oxidative stress, inflammation and endothelial damage may be possible mechanisms of atherogenesis in PACS and established safety and antiatherogenic properties of apoA-I mimetic peptides, we hypothesized that 4F can be a novel therapy for long-term risk for CVD in PACS. We used an established model of atherogenesis to assess ex vivo the therapeutic impact of 4F on early mechanisms of atherogenesis in PACS.
Methods: Our in vitro model of atherogenesis can dissect the impact of plasma from patients with PACS on key mechanisms of early atherogenesis such as monocyte chemotaxis and monocyte-derived foam cell formation (MDFCF). Freshly isolated peripheral blood mononuclear cells (PBMCs) from healthy donors (n=6) were added to tumor necrosis factor-activated human umbilical vein endothelial cells monolayers (HUVECs) on type I fibrous collagen gels to transmigrate (% reverse migration) and form foam cells in the presence of pooled plasma, and 4F (100 µg/ml) as previously described. Pooled plasma was isolated from healthy participants (n=5 males, 18–40 years old) and patients with PACS (n=6, 50–65 years old, 2 females, 4 males) with no risk factors for CVD (hypertension, diabetes, dyslipidaemia) or inflammatory comorbidities other than prior SARS-CoV-2 infection >12 weeks prior to study participation. Study participants were recruited within UCLA CTSI. Flow cytometry assessed MDFCF (▵MFI BODIPY of CD33+ macrophages inside the gel: fluorescence intensity of BODIPY compared to negative staining control). Paired t-test was used for statistical comparison within the same donor.
Results: When media-containing PACS+ compared to control plasma was added to HUVECs, a significantly increased proportion of monocytes underwent transendothelial migration (TEM; median migrated cells 21.2 versus 6.5%, respectively) and CD33+ macrophages inside the collagen gel had increased lipid content per cell (median ▵MFI BODIPY 423 versus 128, respectively; P<0.05; Figure 1). In the presence of PACS-plasma, 4F (100 µg/ml) attenuated TEM of M/M and MDFCF but did not fully reduce TEM of M/M and MDFCF compared to uninfected controls (P<0.05 for all comparisons).
Conclusions/discussion: Plasma from patients with PACS with no CVD and CVD risk factors directly induces key mechanisms of early atherogenesis (TEM and MDFCF). 4F attenuated the ex vivo proatherogenic effects of plasma from PACS patients. Oral 4F can be a novel therapy for adverse atherosclerotic cardiovascular complications of PACS and needs to be further validated in vivo.
Abstract O06
ABSTRACT O07
Non-obese NAFLD is associated with higher sCD14 concentrations in adults with HIV
JE Lake1, H Feng2, H Miao2, P Debroy1, A Somasunderam1, NS Utay1
1University of Texas Health Science Center at Houston, Houston, TX USA; 2UTHealth School of Public Health
Background: Hepatic steatosis is highly prevalent in people living with HIV (PLWH). Additionally, non-obese (BMI <30 kg/m2), non-alcoholic fatty liver disease (NAFLD) may be more frequent in PLWH than the general population, but aetiology and risk factors are incompletely understood. Soluble CD14 (sCD14) is a marker of monocyte/Kupffer cell activation that is associated with (obese) NAFLD disease severity. We sought to understand factors associated with hepatic steatosis and non-obese NAFLD in a multi-ethnic cohort of PLWH.
Methods: In this cross-sectional, observational, single center study in Houston, TX (2017–2020), adult PLWH were approached at random and offered screening for hepatic steatosis by FibroScan® controlled attenuation parameter (CAP) measurement. Biomarkers associated with NAFLD physiology in the general population were measured centrally by ELISA. Multivariable regression modeling explored factors associated with hepatic steatosis (all participants) and the subset of PLWH with NAFLD (no heavy alcohol or viral hepatitis).
Results: Participants (n=194) were 95% non-White, 22% cisgender female, 34% transgender female, and had median age 49 years, median time with HIV 15 years and median time on ART 11 years; 5% had heavy alcohol intake, and 11% chronic HBV or HCV. Using CAP cutoffs of 248 and 260 dB/m, 58% of the cohort had any and 46% had moderate or greater hepatic steatosis, respectively. 41% of those with steatosis were non-obese. In multivariable analysis, Hispanic ethnicity and higher BMI and sCD14 concentrations were independently associated with hepatic steatosis (CAP ≥260 dB/m). In models assessing associations with non-obese steatosis and non-obese NAFLD, BMI was replaced by current smoking and hypertension, respectively. Changing the CAP cutoff to be more or less inclusive did not substantially change model results, with higher sCD14 levels consistently associated with steatosis prevalence. Additionally, sCD14 concentrations were higher among persons with non-obese NAFLD than obese NAFLD and non-NAFLD PLWH.
Conclusions: In this cohort of adult PLWH on contemporary ART, hepatic steatosis was common. Non-obese steatosis was prevalent in 20% of the cohort, a rate 5× higher than the US general population. Higher sCD14 concentrations were associated with steatosis/NAFLD in obese and non-obese PLWH, but sCD14 concentrations were the highest among PLWH with non-obese NAFLD. The physiology of non-obese NAFLD in PLWH demands further exploration.
ABSTRACT O08
Some INSTIs inhibit the beiging capacity of white adipose tissue in vivo and in vitro, resulting in dysfunctional hypertrophic adipose tissue
K Ngono Ayissi1, J Gorwood1, C Bourgeois2, O Lambotte2,3, L Le Pelletier1, M Atlan1,4, R Motterlini5, R Foresti5, B Fève1,6, J Capeau1, V Béréziat1, C Lagathu1
1Sorbonne Université, Inserm UMR_S 938, Centre de Recherche Saint-Antoine (CRSA), RHU CARMMA, Institute of Cardiometabolism and Nutrition (ICAN), F-75012 Paris, France; 2CEA - Université Paris Sud 11 - Inserm U1184, Center for Immunology of Viral Infections and Autoimmune Diseases, IDMIT department, Fontenay-aux-Roses, France; 3APHP, Hôpital Bicêtre, Service de Médecine Interne et Immunologie Clinique, Kremlin-Bicêtre, France; 4AP-HP, Tenon Hospital, Department of Plastic Surgery, F-75020 Paris, France; 5Inserm UMR_S955, Faculté de Médecine, Université Paris-Est, Créteil, France; 6AP-HP, Saint-Antoine Hospital, Department of Endocrinology, PRISIS, F-75012 Paris, France
Some HIV-infected patients receiving an integrase strand transfer inhibitor (INSTI), especially dolutegravir (DTG) and bictegravir (BIC), display an accumulation of adipose tissue (AT) leading to weight gain which is associated with increased cardiometabolic risk.
Adipose tissue (AT) plays an essential role in energy homeostasis through its storage and secretory functions. White AT, which plays a critical role in energy storage and mobilization, can be distinguished from brown and beige AT, which exert a thermogenic function linked to the expression of the uncoupling protein UCP1 and to the increased oxidation of fatty acids. The emergence of beige adipocytes in white AT (beiging) can be induced by adrenergic agents or cold and is beneficial to whole AT homeostasis by promoting energy expenditure. Indeed, by promoting energy dissipation, beige adipocytes limit hypertrophy and associated dysfunction of white adipocytes.
A few studies suggested that INSTIs could impair beiging. In agreement, we obtained preliminary data on white AT from infected macaques treated with an INSTI, DTG. We observed that the expression of several beige markers, such as PRDM16 and TMEM26 was reduced as compared to non-infected controls.
To further investigate the impact of INSTIs on beiging, adipose stromal cells (ASC) isolated from the white AT of six healthy women (age: 41.7 ±2.3 years; BMI: 25.1 ±2 kg/m2) were differentiated into beige or white adipocytes. We evaluated the consequence of ASC exposition to DTG, BIC or raltegravir (RAL) on the expression of beige markers and on adipocyte functions in derived adipocytes. ASC exposed to DTG and BIC, but not RAL, exhibited a defect in beige adipocyte differentiation in favour of a white adipocyte phenotype. Indeed, INSTI treatment decreased the expression of beige adipocyte markers such as UCP1, TMEM26 and PRDM16. Both DTG and BIC also decreased the expression of FGF21, a beige adipokine, and increased the expression of leptin, more specific to white adipocytes. These alterations were associated with increased oxidative stress, and also with mitochondrial dysfunctions characterized by an impaired respiration rate evaluated by Seahorse and a lower mitochondrial uncoupling. Finally, INSTI-treatment led to increased lipid accumulation, in favour of a whitening of beige adipocytes. Altogether, these alterations could promote the emergence of hypertrophic and dysfunctional white adipocytes in response to INSTIs.
Therefore, we show here, both in an in vivo model of macaques and in an in vitro model of human adipocytes, that some INSTIs reduced the beiging capacity of white adipocytes which was associated with adipocyte hypertrophy, oxidative stress and mitochondrial dysfunction in vitro.
Identification of therapeutic molecules capable of favouring beiging or counteracting associated dysfunctions, such as oxidative stress, could be beneficial with regard to the weight-gaining effect of some INSTIs and associated metabolic complications observed in HIV-infected persons.
ABSTRACT O09
Prevalence of functional limitation and evaluation of independency in people living with HIV at the Treichville University Hospital in Abidjan
N Etoundi1, P Debeaudrap2, Z Diallo1, F Abouo1, J Tegbe3, A Tanon1, P Coffié3
1Infectious and Tropical Diseases Department, Treichville University Hospital, Abidjan, Côte d’Ivoire; 2Institut de Recherche pour le Développement, Paris, France; 3Programme PACCI, Abidjan, Côte d’Ivoire
Background and objectives: With the expanded access to antiretroviral therapy, people living with HIV (PLWHIV) have a prolonged life expectancy and are thus exposed to age-related comorbidities, including non-communicable diseases. In addition, older PLWHIV often face functional limitation, as well as a restriction in their independence for daily activities. Despite the high prevalence of HIV infection in sub-Saharan Africa, there has been limited research on this issue. This cross-sectional study aims to estimate the prevalence of functional limitation, certain comorbidities and to assess the independence of PLWHIV followed up at the Infectious and Tropical Diseases Department of the Treichville University Hospital in Abidjan.
Methods: Participants were included if they aged ≥30 and were on antiretroviral therapy for ≥1 year. Information on participant socio-demographic characteristics, usual physical activity, alcohol use and medical and HIV history was collected. High blood pressure, peripheral neuropathy and diabetes were screened. Functional limitation was assessed using the Short Physical Performance Battery (SPPB) score, which includes a standing balance test, a 10 m gait speed test and the 5-sit-to-stand test. In addition, we evaluated patient’s independence in the instrumental activities of daily living (IADL) with the Epidemca scale. Statistical analyses used logistic and linear regressions.
Results: 181 (68%) women and 84 (32%) men with a median age of 50 years were included. The level of education attained was higher for men than for women (30% of men versus 13% of women achieved higher education; P=0.001) while the saving capacity was not significantly different (42% versus 51%; P=0.2). The median nadir CD4 was 115 cells/mm3 in men and 177 cells/mm3 in women (P=0.2) and the median duration of antiretroviral treatment was 15 and 14 years respectively (P=0.8). The frequency of hypertension was 37% in men and 23% in women (P=0.03), the frequency of obesity was 31% and 59% respectively (P<0.001) and the frequency of lipodystrophy, 7% and 16% respectively (P=0.1). Finally, 11% of men and 7% of women reported dangerous alcohol use according to the AUDIT score. 12% of participants (14% men, 12% women; P=0.8) had a suboptimal SPPB score. CD4 nadir was the only factor negatively associated with the risk of a low SPPB score (P=0.006). 93% of the participants (men: 98%, women: 91%; P=0.07) reported no difficulties to perform the following IADL activities: telephone use, shopping, medication management, finance management, house-keeping, food preparation, laundry.
Conclusions: In this relatively young study population on antiretroviral treatment for an average of 15 years, the prevalence of functional limitation was low and independent daily living maintained.
TUESDAY 7 DECEMBER – POSTER PRESENTATIONS
ABSTRACT P05
Abacavir induces an increase in leukocyte-endothelium crosstalk in blood from HIV-infected patients
MA Blanch-Ruiz1, A Sanchez-Lopez1, R Ortega-Luna1, G Gómez-García1, MA Martinez-Cuesta1, R Ferrando-Vilalta1, MJ Galindo2, JV Esplugues1, A Alvarez1
1University of Valencia, Valencia, Spain; 2Hospital Clinic of Valencia, Valencia, Spain
Aim: Abacavir (ABC) has been associated with myocardial infarction risk. We have demonstrated in vitro (in cells from healthy donors) that clinical concentrations of ABC, but not of tenofovir (TFV), exert actions that are both proinflammatory (by inducing leukocyte-endothelium interactions) and prothrombotic (by promoting the interaction of platelets with other important vascular cells such as the endothelium or neutrophils, and also by promoting thrombus formation). The aim of this study was to give physiological relevance to these data by analysing the effects of ABC on leukocyte-endothelium interactions in cells isolated from the blood of HIV-infected patients treated with TFV.
Methods: We used blood drawn from HIV-infected patients at Hospital Clínico Universitario de Valencia who had been receiving an antiretroviral therapy regime that included TFV (either tenofovir alafenamide or tenofovir disoproxil fumarate) for at least 6 months. Polymorphonuclear (PMNs) cells were isolated using a method based on density gradient and were then treated with clinically relevant concentrations of ABC (5 µg/ml, 4 h) or vehicle. After this period, the interactions of PMNs with a non-infected endothelium monolayer (rolling, rolling velocity and adhesion) were evaluated using a parallel-plate flow chamber system. By means of flow cytometry we also assessed the expression of different leukocyte adhesion molecules involved in leukocyte-endothelium interactions, such as LFA-1 (CD11a/CD18), Mac-1 (CD11b/CD18), gp150,45 (CD11c/CD18) and L-selectin (CD62L).
Results: A total of 28 patients were included in the study: age was 47.04 ±2.62 years, 92.86% were males, and CD4+ T-cell count was 774.2 ±82.24 cells/mm3. PMN rolling velocity was reduced, while rolling along and adhesion to the endothelium were significantly higher in the ABC-treated group than in the vehicle-treated group (Figure 1A–C). Moreover, ABC induced a rise in the expression of neutrophil CD11b, CD11c and CD18 (Figure 1D–F). The other leukocyte adhesion molecules analysed (i.e., CD11a and CD62L) were not modified by ABC.
Conclusions: ABC enhances PMN-endothelium interactions, thus promoting the initial phases of the inflammatory process. Furthermore, it induces the expression of leukocyte adhesion molecules Mac-1 and gp 150,45 which may be involved in the aforementioned interactions. Our results give support to an increased risk of myocardial infarction in ABC-treated HIV patients.
Leukocyte-endothelial cell interactions and Mac-1 (CD11b/CD18) and gp150,45 (CD11c/CD18) expression induced by abacavir (ABC) in HIV-infected patients (Abstract P05)
ABSTRACT P06
Impact on inflammatory and atherogenesis biomarkers with the 2-drug regimen dolutegravir plus lamivudine in treatment-experienced people with HIV-1: A systematic literature review
JM Llibre1, PE Cahn2, J Lo3, TJ Barber4,5, C Mussini6, BJ van Welzen7, B Hernandez8, C Donovan9, M Kisare10, M Sithamparanathan11, J van Wyk11
1Hospital Universitari Germans Trias i Pujol, Barcelona, Spain; 2Fundación Huésped, Buenos Aires, Argentina; 3Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA; 4Royal Free London NHS Foundation Trust, London, UK; 5University College London, London, UK; 6AOU Policlinico, University of Modena and Reggio Emilia, Modena, Italy; 7University Medical Centre Utrecht, Utrecht, the Netherlands; 8ViiV Healthcare, Madrid, Spain; 9ViiV Healthcare, Research Triangle Park, NC, USA; 10GlaxoSmithKline, Nairobi, Kenya; 11ViiV Healthcare, Brentford, UK
Objectives/aim: Even in the setting of sustained antiretroviral therapy (ART)-mediated virological suppression, HIV is associated with some persistent inflammation, contributing to an increased risk of non-AIDS-related comorbidities. HIV-associated inflammation may be driven by several factors including bacterial translocation, coinfections, and ongoing viral replication and persistence. Other host factors such as comorbidities and lifestyle characteristics may also contribute to inflammation. The 2-drug regimen dolutegravir plus lamivudine has demonstrated rapid viral load decline and durable, non-inferior efficacy compared with 3- and 4-drug regimens (3/4DRs) in both ART-naive and ART-experienced people with HIV-1 (PWH), with no differences in low-level viraemia, viral blips, or virological control in sanctuary sites and reservoirs. The objective of this systematic review was to summarize randomized controlled trial (RCT) and real-world evidence evaluating inflammatory and atherogenesis biomarkers with dolutegravir plus lamivudine in treatment-experienced PWH.
Methods: Ovid MEDLINE®, Embase®, PubMed, and Cochrane library databases were searched for studies published from 1 January 2013 to 14 July 2021. Additional searches were performed to identify relevant data presented at the 2021 International AIDS Society (IAS) Conference on HIV Science and IDWeek™ 2021. Eligible studies included real-world evidence and RCTs evaluating switch to dolutegravir plus lamivudine in treatment-experienced PWH aged ≥18 years that included data on CD4+/CD8+ ratio or inflammatory and atherogenesis biomarkers C-reactive protein, soluble CD14, interleukin-6, soluble CD163, D-dimer, fatty acid binding protein-2, or soluble vascular cell adhesion molecule-1.
Results: Overall, 4 publications representing 2 RCTs (dolutegravir/lamivudine: SALSA, n=246; TANGO, n=369) and 6 publications of real-world evidence (dolutegravir plus lamivudine: n=1,000) were eligible for inclusion. All real-world studies evaluated CD4+/CD8+ ratio, while only 1 assessed inflammatory and atherogenesis biomarkers. Across both RCTs, no consistent pattern of change in biomarkers was observed between dolutegravir/lamivudine and 3/4DR comparators throughout the studies, with the exception of reductions in soluble CD14 (favoured dolutegravir/lamivudine in SALSA at week 48 and in TANGO at weeks 48 and 144) and IL-6 (favoured TAF-based regimens in TANGO at weeks 48 and 144; Figure 1). In the one real-world study evaluating changes in inflammatory biomarkers (n=67), median soluble CD14 levels significantly decreased at week 48 post-switch to dolutegravir plus lamivudine (P<0.001). Levels of other biomarkers (including IL-6) remained stable. In all of the real-world studies, increases in CD4+/CD8+ ratio were reported after switch to dolutegravir plus lamivudine (follow-up, 12-60 months).
Conclusions/discussion: Evidence from 2 large RCTs and 1 real-world study showed no consistent impact on inflammatory and atherogenesis biomarkers with a switch to dolutegravir plus lamivudine versus 3/4DR comparators. Increases in CD4+/CD8+ ratio were also reported post-switch. These data suggest there is no evidence of an impact on inflammation after switching from a 3/4DR to dolutegravir/lamivudine. Future research on the clinical relevance and long-term consequences of changes in inflammatory biomarkers in PWH is needed.
Abstract P06
ABSTRACT P07
Cytokine-based predictive model of pulmonary function trajectories in people living with HIV
I Konstantinidis1, T Lovelace2, R DeSensi1, P Benos2, K Kunisaki3, C Rinaldo4, A Morris1, SM Nouraie1
1Division of Pulmonary, Allergy and Critical Care, University of Pittsburgh; 2Department of Computational and Systems Biology, University of Pittsburgh; 3Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, University of Minnesota; 4Department of Infectious Diseases and Microbiology, University of Pittsburgh Graduate School of Public Health
Aims: Poorly controlled HIV infection is associated with accelerated pulmonary function decline. We have previously applied group-based trajectory models (GBTM) to describe pulmonary function trajectories and determined that adverse trajectories were associated with worse symptoms, functional status, and survival in people living with HIV (PLWH). We sought to quantify multivariable association between plasma cytokines and trajectory group membership and determine whether a cytokine-based model predicted group membership.
Methods: People living with HIV recruited from the Pittsburgh Acquired Immunodeficiency Syndrome Center for Treatment and the Pittsburgh sites of the Multicenter AIDS Cohort Study and Women’s Interagency HIV Study with ≥3 PFT measurements (post-bronchodilator FEV1, FVC, and DLCO) from 2008–2019 were included. GBTM incorporating participant attrition identified ‘low and slow decline’ versus ‘high and rapid decline’ trajectories for FEV1 and FVC each and ‘high’ versus ‘low’ trajectories for DLCO. We used standardized baseline value of 18 plasma cytokines in stepwise backward logistic regression in a training subset of observations to identify cytokines associated with adverse trajectories at α=0.05 level. We then created a predictive model using significant cytokines for each PFT trajectory and evaluated discrimination based on ROC AUC in a validation set.
Results: 227 participants contributed 1438 PFT measurements over median 8.4 years. Cytokines associated with increased risk for ‘low and slow decline’ FEV1 trajectory were IL-6 (aOR 3.03, 95% CI 1.59, 5.76), CRP (aOR 2.50, 95% CI 1.54, 4.06) and MIP-1b (aOR 2.03, 95% CI 1.13, 3.64); IL-8 was associated with decreased risk (aOR 0.34, 95% CI 0.17, 0.70). IL-6 (aOR 2.06, 95% CI 1.13, 3.75), IL-5 (aOR 2.40, 95% CI 1.01, 5.68), MIP-1b (aOR 2.63, 95% CI 1.25, 5.50), and CRP (aOR 3.42, 95% CI 1.93, 6.07) were associated with increased risk and IL-8 (aOR 0.32, 95% CI 0.12, 0.82) and MCP-1 (0.05, 95% CI 0.01, 0.56) were associated with decreased risk for ‘low and slow decline’ FVC trajectory. Cytokines associated with the ‘low’ DLCO trajectory were IL-6 (aOR 1.89, 95% CI 1.09, 3.29), ET-1 (aOR 2.11, 95% CI 1.30, 3.42), and IL-2 (aOR 3.43, 95% CI 1.05, 11.18), whereas IL-17a was associated with decreased risk (aOR 0.20, 95% CI 0.06, 0.66; Figure 1). The ROC AUC for the multivariable predictive models were 0.66 for FEV1, 0.63 for FVC and 0.55 for DLCO.
Conclusions: Nine plasma cytokines were associated with PFT trajectories in persons living with HIV with higher IL-6 being a common risk factor for adverse FEV1, FVC and DLCO trajectories and higher CRP and MIP-1b being shared risk factors for adverse FEV1 and FVC trajectories. Predictive models for FEV1 and FVC showed fair discriminating ability. Validation of these associations in a larger sample of PLWH is needed for further mechanistic understanding of HIV-associated lung disease pathogenesis and to allow improved predictive modeling.
Funding sources: U01-AI035041, R01HL090339.
Plasma cytokines associated with adverse PFT trajectories (Abstract P07)
ABSTRACT P08
Cardiovascular risk knowledge stratified by predicted cardiovascular risk level in an HIV clinical cohort
B Morapedi1, OJ Molefe-Baikai2, M Mosepele2
1Department of Internal Medicine, Mafikeng Provincial Hospital, Mafikeng, South Africa; 2University of Botswana, Department of Internal Medicine, Gaborone, Botswana
Objectives: To assess knowledge of cardiovascular disease (CVD) risk among people living with HIV (PLWH) and to determine the association between knowledge and predicted 10-year CVD risk.
Methods: We conducted this cross-sectional study in a tertiary hospital in Gaborone, Botswana between March and October 2017. We enrolled 206 PLWH aged 40–79 years who had been on combined antiretroviral therapy (cART) for more than 6 months. Patients with prior CVD and/or on statin therapy were excluded. Cardiovascular knowledge was assessed using the Heart Disease Fact Questionnaire (HDFQ). Predicted 10-year CVD risk level was established using the Atherosclerotic Cardiovascular Disease (ASCVD) risk calculator. Odds ratios were used to assess the association between CVD risk knowledge and predicted CVD risk level.
Results: Of the 206 PLWH enrolled, 118 (57.3 %) were male with a median age of 50 years (IQR 43–58). Median time from HIV diagnosis and duration of first cART was 13 (IQR 10–17) and 12 (IQR 9–15) years respectively. The median (IQR) CD4 T-lymphocyte count was 578.50 cells/mm3 (302.4–854). 196 (95.1%) had suppressed viral loads (HIV RNA <400 copies/ml). The mean (SD) score for knowledge on the HDFQ was 73.49% (±13.26) while 44 (21.4%) were identified to have high predicted 10-year CVD risk defined as a score of more than or equal to 7.5 %. A high predicted 10-year CVD risk was not associated with a high CVD risk factor knowledge (score of >70% on the HDFQ; OR 1.119, 95% CI: 0.885, 1.414; P-value =0.31). Similarly, a low predicted 10-year CVD risk was also not associated with high CVD risk knowledge level (OR 0.770, 95% CI: 0.469, 1.263; P-value =0.32).
Conclusions: CVD risk knowledge was high overall. However, being at higher risk for CVD was not associated with increased awareness of CVD risk factors (assessed as knowledge) indicating a gap that needs to be addressed. Similarly, those at a lower risk for CVD did not score high on CVD risk knowledge, suggesting that factors other than their CVD knowledge contribute to their low 10-year predicted risk of CVD. Larger studies are required to validate inventories of CVD knowledge and CVD prediction tools to inform interventions to improve CVD health among PLWH in different settings.
WEDNESDAY 8 DECEMBER – ORAL PRESENTATIONS
ABSTRACT O10
Weight gain of >10% after switching to TAF and/or INSTI is common in ATHENA cohort participants with HIV and suppressed viraemia, especially in women and those switching simultaneously to TAF and INSTI
ML Verburgh1,2, FWNM Wit1,3, A Boyd3,4, P Reiss1,2, M van der Valk1,3
1Amsterdam University Medical Centers, Department of Infectious Diseases, Amsterdam Infection and Immunity Institute, Amsterdam, the Netherlands; 2Department of Global Health, Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands; 3HIV Monitoring Foundation, Amsterdam, the Netherlands; 4Department of Infectious Diseases, Public Health Service of Amsterdam, Amsterdam, the Netherlands
Objectives: To determine factors associated with >10% weight gain in people living with HIV (PLHIV), participating in the Dutch national ATHENA HIV cohort, who switched to TAF and/or INSTI whilst virally suppressed, and to investigate its effect on metabolic parameters.
Methods: All ART-experienced, but TAF- and INSTI-naive adults in ATHENA who switched to a TAF- and/or INSTI-containing regimen whilst virally suppressed for >12 months, and with ≥1 available weight measurement within 24 months pre-switch and ≥1 measurement ≥2 months post-switch, were identified. Individuals with comorbidities/co-medication known to be associated with weight change were excluded. Analyses were stratified by switch to only TAF, only INSTI or simultaneously to TAF+INSTI. Individuals were censored when subsequently discontinuing TAF and/or INSTI, or when starting either of these two for the first time. Weight in the 24 months pre- and post-switch was modelled using mixed-effect linear regression. Factors associated with >10% weight gain were assessed using parametric survival models. Changes in glucose, lipid levels and blood pressure post-switch were modelled using mixed-effect linear regression and compared between those with and without >10% weight gain.
Results: We identified 1,544 PLHIV who switched to TAF; 2629 to INSTI and 981 to TAF+INSTI, with >10% weight gain post-switch observed in 8.8%, 10.6% and 14.4%, respectively. In those individuals, the adjusted mean increase at 24 months post-switch was significantly greater in those who switched to TAF+INSTI (+10.24 kg; 95% CI, 8.75, 11.74) than to only TAF (+9.38 kg; 95% CI, 7.93, 10.83 kg; P<0.001) or only INSTI (+9.59 kg; 95% CI, 8.69, 10.49 kg; P<0.001). Across all three strata, women, both of Western European and sub-Saharan African origin, had a higher risk of >10% weight gain compared to Western European men (Table 1). Moreover, weight loss prior to switch and age <40 years were associated with a higher risk. Weight gain >10% was not associated with any particular INSTI agent. At 24-months post-switch, increases in both glucose and systolic blood pressure were minor across groups (maximum mean increase +0.38 mmol/l and +3.30 mmHg, respectively). Significantly greater mean increases in total cholesterol, LDL-cholesterol and triglycerides occurred in those with versus without >10% weight gain after switch to TAF (+0.63 versus +0.33; +0.38 versus +0.19; +0.67 versus +0.41 mmol/l) or TAF+INSTI (+0.46 versus +0.19; +0.49 versus -0.01; +0.70 versus +0.11 mmol/l). In those switching to only INSTI, these same mean levels all decreased for those with versus without >10% weight gain (–0.12 versus -0.21; –0.17 versus -0.22; -0.23 versus –0.30 mmol/l).
Conclusions: Experiencing >10% weight gain after switching to TAF and/or INSTI was common in our national cohort of treatment-experienced virally suppressed PLHIV, and most frequent in those switching to both drugs simultaneously. Women in general were at higher risk. Changes in metabolic parameters were significantly larger, yet modest, in those with compared to without >10% weight gain.
ABSTRACT O11
Factors associated with cardiometabolic parameters at 3 years in the TANGO Study, comparing a switch to dolutegravir/lamivudine versus maintenance of tenofovir alafenamide-based regimens
RL Batterham1, N Espinosa2, C Katlama3, M McKellar4, S Scholten5, D Smith6, M Ait-Khaled7, N George8, LA Gordon9, R Moodley7, B Wynne9, J van Wyk7
1UCL Division of Medicine, London, UK; 2Hospital Universitario Virgen del Rocío, Sevilla, Andalucía, Spain; 3AP-HP, Hôpital Pitié-Salpêtrière, Service de Maladies Infectieuses et Tropicales, INSERM-Sorbonne Universités, Paris, France; 4Department of Medicine, Duke University School of Medicine, Durham, NC, USA; 5Praxis Hohenstaufenring, Cologne, Germany; 6Albion Centre, Sydney, Australia; 7ViiV Healthcare, Brentford, UK; 8GlaxoSmithKline, Bangalore, India; 9ViiV Healthcare, Research Triangle Park, NC, USA
Objectives/aim: TANGO is a randomized controlled trial that showed non-inferior efficacy of switching to dolutegravir/lamivudine compared with continuing 3/4-drug tenofovir alafenamide-based regimens (TBR; elvitegravir/cobicistat [66%], rilpivirine [12%], dolutegravir [11%], and boosted darunavir [7%]) in virologically suppressed adults over 3 years. At week 144, overall increase in adjusted mean weight (2.2 versus 1.7 kg) and proportion of participants with ≥10% weight increase (13% versus 12%) in the dolutegravir/lamivudine versus TBR groups were similar. Here, we provide in-depth analyses of cardiometabolic parameters and associated baseline factors.
Methods: Shifts in BMI categories from baseline to week 144 were derived. Adjusted mean change (or adjusted geometric mean ratios for log-transformed end points) from baseline to week 144 for weight, leptin, HOMA-IR, fasting insulin, and HbA1c were compared between treatment groups using mixed-model repeated measures (MMRM). For metabolic syndrome, HOMA-IR ≥2, FIB-4 ≥1.45, and Framingham risk score ≥10%, logistic regression model adjusting for relevant baseline variables was used for comparison between treatment groups. Exploratory subgroup analyses (MMRM or logistic regression as appropriate), including prior tenofovir alafenamide duration, boosting status, and baseline BMI, were also performed.
Results: Twenty-four (8%) and 17 (6%) participants shifted from baseline BMI <30 kg/m2 to post-baseline ≥30 kg/m2 in the dolutegravir/lamivudine and TBR groups, respectively. Adjusted change from baseline in leptin was similar between treatment groups (geometric mean ratio (95% CI): dolutegravir/lamivudine, 1.21 [1.11, 1.33]; TBR, 1.21 [1.12, 1.31]) with magnitude of increase aligned with baseline BMI categories (dolutegravir/lamivudine: 11%, 23%, and 45%; TBR: 11%, 22%, and 47%, for participants with BMI <25 kg/m2, 25 to <30 kg/m2, and ≥30 kg/m2, respectively). Adjusted changes in lipids favoured the dolutegravir/lamivudine group, mostly observed in the boosted subgroup. Adjusted changes in HOMA-IR, fasting insulin, and HbA1c were small and similar between groups. Logistic regression analyses for ≥10% weight increase, metabolic syndrome, HOMA-IR ≥2, FIB-4 ≥1.45, and Framingham risk score ≥10% demonstrated no evidence of difference between treatment groups (dolutegravir/lamivudine: TBR odds ratios [95% CI], 1.11 [0.68, 1.80], 0.99 [0.59, 1.68], 0.79 [0.50, 1.26], 1.39 [0.63, 3.06], and 0.92 [0.56, 1.49], respectively). Analyses by subgroups for ≥10% weight increase (baseline BMI and prior tenofovir alafenamide duration), HOMA-IR ≥2 (baseline BMI category), metabolic syndrome (boosting status), and FIB-4 ≥1.45 (boosting status) showed no evidence of treatment difference in any subgroup. Baseline factors associated with these endpoints are summarized (Figure 1).
Conclusions/discussion: After 144 weeks, weight gain and cardiometabolic parameters in the dolutegravir/lamivudine group were similar to the TBR group and generally stable for both groups, except for lipids which favored dolutegravir/lamivudine in the boosted subgroup. The similar changes in leptin between groups suggest no excess gain in fat versus lean mass in either group. Results underscore the importance of known risk factors in the clinical management and prevention of adverse outcomes in PLWH on lifelong ART.
Abstract O11
ABSTRACT O12
Abnormal transcriptomic profile of epicardial adipose tissue of people living with HIV: results from the PIECVIH study
F Boccara1,2, R Alili3, C Poitou3, C Lagathu1, V Béréziat1, L Le Pelletier1, C Vigouroux1, P Leprince4, A Cohen2, J Capeau1
1Sorbonne Université, GRC n°22, C²MV-Complications Cardiovasculaires et Métaboliques chez les patients vivant avec le Virus de l’immunodéficience humaine, Inserm UMR_S 938, Centre de Recherche Saint-Antoine (CRSA), Institute of Cardiometabolism and Nutrition (ICAN), F-75012 Paris, France; 2APHP, Saint-Antoine Hospital, Department of Cardiology, GH APHP-Sorbonne Université F-75012 Paris, France; 3Sorbonne Université, Inserm, Nutrition and obesities: systemic approaches (NutriOmics), and APHP Nutrition Department, Pitié-Salpétrière Hospital, CRNH Ile-de-France, GH APHP-Sorbonne Université, F-75013 Paris, France; 4APHP, Pitié-Salpétrière Hospital, Department of Cardiac surgery, GH APHP-Sorbonne Université F-75013 Paris, France
Background: Increased epicardial adipose tissue (EAT) volume has been associated with increased risk of coronary artery disease (CAD) in people living with HIV (PLWH). However, the underlying mechanisms remain unknown. We conducted the PIECVIH study to compare EAT properties between PLWH and HIV-negative patients undergoing coronary artery bypass graft (CABG).
Methods: The PIECVIH study is a cross sectional prospective study performed in one center (Sorbonne University hospital group, Paris, France) enrolling 11 ART-controlled PLWH and 11 matched (age +/- 3 years and sex) HIV-negative patients requiring CABG. During surgery, EAT and thoracic subcutaneous fat samples were taken. Transcriptomic analyses were performed in samples in which mRNA extraction led to enough mRNA of excellent quality i.e., in 7 PLWH and 7 HIV-negative samples for thoracic subcutaneous fat and 9 PLWH and 8 HIV-negative samples for EAT. The expression of 30 genes, related to inflammation, immune activation, fibrosis and adipokines, was evaluated and related to the expression of the reference gene 18S.
Results: The mean age of the cohort was 59.8 years old (100% male). The cardiovascular risk profile was quite similar between both groups including 66% smokers, 64% had hypercholesterolaemia, 36% hypertriglyceridaemia and 56% hypertension. However, HIV-negative subjects had a higher prevalence of diabetes than PLWH (73% versus 18%; P=0.002) whereas body mass index was lower in PLWH (23.2 versus 27.5 kg/m²; P=0.017). Regarding transcriptomic analysis, the level of expression of all the tested genes was not different between PLWH and HIV-negative subjects in subcutaneous fat. Conversely, in EAT, the relative expression of IL-6 and CCL2 was 3-5-fold higher in samples issued from PLWH than from HIV-negative: respectively 0.46 versus 0.13 (P=0.03) and 1.13 versus 0.24 (P=0.03). Moreover, only in EAT and only in PLWH, the expression of CCL2 was highly related to the expression of collagen genes: COL6A3 (R=0.807, P=0.009), COL1A1 (R=0.726, P=0.027), COL6A2 (R=0.810, P<0.0001). As well, CCL2 was strongly related to the macrophage activation marker CD163 in EAT of PLWH (R=0.832, P=0.006). Moreover, CD163 was strongly related to markers of fibrosis: COL6A2 (R=0.901, P=0.0009), COL6A3 (R=0.955, P<0.0001) and to VEGFA (R=0.657, P=0.05) involved into vascularization. Regarding cardiovascular parameters, in EAT of PLWH but not of HIV-negative patients, COL6A3 was positively associated (R=0.721, P=0.03) and CD163 and CCL2 tended to be positively associated with the Gensini score (R=0.626, P=0.07 and R=0.629, P=0.07), evaluating the severity of CAD. Thus, the fibrotic phenotype and the abnormal immune activation profile of epicardial fat could be related to the cardiovascular status in PLWH.
Conclusions: Inflammation of EAT was enhanced in PLWH. Immune activation represented by CCL2 and CD163 was strongly with fibrosis and vascularization, stressing for a dysfunctional and fibrotic EAT in PLWH which could be responsible for accelerated coronary atherosclerosis.
ABSTRACT O13
Depot medroxyprogesterone acetate is associated with lower bone mass and higher central fat in young women on tenofovir disoproxil fumarate-containing ART
FK Matovu1,2, M Nabwana1, E Isingel1, JA Babirye1, N Kiwanuka2, D Scholes3, P Musoke1,2, MG Fowler4, ME Beksinska5, JM Pettifor6, TT Brown4, the BONE: STAR Study Team
1Makerere University-Johns Hopkins University (MU-JHU) Research Collaboration, Kampala, Uganda; 2Makerere University College of Health Sciences, Kampala, Uganda; 3Kaiser Permanente Washington Health Research Institute, Seattle, USA; 4Johns Hopkins University School of Medicine, Baltimore, USA; 5Maternal Adolescent & Child Health Research Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, RSA; 6SAMRC/Wits Developmental Pathways for Health Research Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, RSA
Background: The contraceptive depot medroxyprogesterone acetate (DMPA) is associated with lower bone mineral density (BMD) and higher fat mass among women in the general population. The bone and body composition effects of DMPA among women with HIV, virally suppressed on antiretroviral therapy (ART) are unclear.
Methods: We enrolled ART experienced Ugandan women aged 20–40 years based on their contraceptive use and included DMPA users and non-hormonal contraceptive users. Dual energy x-ray absorptiometry was used to measure fat and lean mass, trabecular bone score (TBS), and BMD (lumbar spine [LS], total hip [TH] and femoral neck [FN]). BMD Z-scores were created using a Ugandan reference population without HIV. Multivariable linear regression was used to assess the association between DMPA use and bone and body composition variables.
Results: Of the 311 virally suppressed women on TDF-containing ART, 186 used DMPA and 125 used non-hormonal contraception. The median age (IQR) was 31.1 (27.7–34.5) years, with a median duration of DMPA use among current users of 43.5 (34–72) months. DMPA use was independently associated with significantly lower mean BMD Z-scores at all sites; -0.911 versus -0.317 (8% difference in mean BMD) at the LS, -1.067 versus -0.756 (4% difference) at TH, and -1.018 versus -0.699 (4% difference) at FN; P<0.001). A higher proportion of DMPA users (26.3%) had low BMD (Z-score ≤ −2 at any of the three sites) compared to non-hormonal users (16.8%); P=0.048. DMPA use was associated with lower TBS, a measure of bone quality, but this was no longer statistically significant after adjustment for LS BMD. Trunk fat was higher in DMPA users compared to non-users (12.3 versus 10.8 kg; P=0.034), but total fat and lean tissue were similar between the groups (P>0.05). See Table 1.
Conclusions: Among young HIV-infected women in Uganda receiving TDF-containing ART, DMPA use was associated with lower lumber spine and hip BMD and tended to be associated with higher central fat. The reversibility of these changes after DMPA discontinuation in this population requires further evaluation.
Abstract O13
ABSTRACT O14
HCV viraemia is associated with reduced hip bone mineral density and strength among African Americans with and without HIV infection
J Sun1, S Langan1, K Moseley2, D Piggott2, S Demeri3, J Pena-Dias2, L Wehbeh2, J Garza2, AG Abraham4, TT Brown1,2
1Department of Epidemiology, Johns Hopkins University, Baltimore, MD, USA; 2Department of Medicine, Johns Hopkins University, Baltimore, MD, USA; 3Department of Radiology, Johns Hopkins University, Baltimore, MD, USA; 4Department of Epidemiology, University of Colorado, Anschutz Medical Campus, Aurora, CO, USA
Objectives: HCV infection has been associated with an increased risk of fracture. However, it is unclear whether the relationship is a direct effect of chronic HCV infection or is confounded by behaviours common to people at risk for HCV (for example, drug use, alcohol use, smoking, poor nutrition) which may also impact bone. We performed a comprehensive assessment of bone density, bone strength, and bone turnover in a cohort of people who inject drugs and had been exposed to HCV (that is, HCV antibody positivity) to determine the association between HCV viraemia and bone health.
Methods: We recruited participants from the AIDS Linked to the IntraVenous Experience (ALIVE) cohort based on their HIV and HCV viraemia status (HIV-/HCV-, HIV+/HCV-, HIV-/HCV+, HIV+/HCV+). Those who had successful HCV treatment were excluded. Areal BMD T-score (spine, femoral neck, hip) and trabecular bone score (TBS) were measured by dual-energy x-ray absorptiometry (DXA). Bone strength of the hip was estimated with hip structural analysis derived from quantitative computed tomography (QCT). Bone turnover and systemic inflammation were assessed with serum markers from the same visit (carboxy-terminal collagen crosslinks [CTX], osteocalcin, procollagen 1 Intact N-Terminal Propeptide [P1NP], tumor necrosis factor-alpha receptor 1 [TNF-r1], TNF-r2, high sensitivity interleukin 6 [HSIL-6], and soluble CD163). Alcohol, tobacco and injection drug use information was collected through ALIVE study visit surveys. We used multivariable linear regression models to evaluate the association of HCV viraemia with bone parameters.
Results: Of 289 enrolled (59 [20%] HCV-/HIV-, 126 [44%] HCV+/HIV-, 31 [11%] HCV-/HIV+, and 73 [25%] HCV+/HIV+), 64% were male, and the median age was 57 years (interquartile range: 51–61); all were African American. HCV viraemia was associated with higher levels of inflammatory markers (TNF-r2, and sCD163 levels [all P<0.05]). HCV viraemia was also associated with lower BMD T-score at the total hip (P=0.016) and a non-significant trend towards lower BMD T-score in the femoral neck (P=0.08; Figure 1). Models controlled for demographic factors, HIV status, BMI, risk behaviour (smoking, alcohol and injection drug use), and serum vitamin D level. No interactions were observed by HIV status. Additional adjustment for inflammatory markers (TNF-r1, TNF-r2, sCD163, HSIL-6) attenuated the association between HCV viraemia and femoral neck and total hip BMD. HCV viraemia was also associated with reduced bone strength at the hip (decreased section modulus at narrow neck of the hip [P=0.03] and increased buckling ratio at the intertrochanteric region [P=0.06]). HCV viraemia was not associated with lumbar spine BMD or trabecular bone score.
Conclusions: Chronic HCV viraemia was independently associated with lower bone density and bone strength at the hip, which may be related to increased systemic inflammation. Further studies should determine whether successful HCV treatment improves bone health among people with HCV.
Marginal estimated mean and 95% confidence interval1 of bone mineral density by HCV viremia among ALIVE participants (Abstract O14)
ABSTRACT O15
Frailty among people living with HIV in Botswana, sub-Saharan Africa
P Ponatshego1, K Molebatsi2, S Lockman1,4, N Youssouf1,3, M Montano4, M Mosepele1,2
1Botswana Harvard AIDS Institute Partnership; 2University of Botswana; 3London School of Hygiene and Tropical Medicine; 4TH Chan School of Public Health, Harvard University
Objectives: HIV is associated with a heightened burden of frailty. However, little is known about frailty among HIV cohorts in sub-Saharan Africa. We determined the prevalence and predictors of frailty in a population of individuals living with HIV in Botswana.
Methods: We conducted a cross-sectional study of people living with HIV over the age of 40 years, on ART in Gaborone, Botswana. Frailty was assessment by the Fried’s frailty criteria, comprising three or more of the following: weight loss (≥4.5 kg in the previous year), low physical activity (considered present if participant had none or low (<3 MET) physical activity once or less per week), self-reported exhaustion (experiencing ≥3–4 times/week that ‘everything I do is an effort’ or ‘sometimes I just cannot get going’), weak grip strength (grip strength adjusted for BMI/gender) and slowness (walking time by gender/height). To identify risk factors of the dichotomized frailty, we first fitted simple logistic regression models using available demographic, socio-economic and HIV-related variables as predictors. All predictor variables with P-values of 0.2 or less were included in multivariable regression models. We reported adjusted odds ratios, corresponding 95% confidence intervals and P-values.
Results: We enrolled 1017 virally suppressed participants, median age 51 (IQR= [57–45]) years, 484 (47.6%) females in Gaborone, Botswana. In this cohort, median HIV disease duration was 14.8 (IQR= [17–10.9]) years, with a median CD4 nadir of 134 (IQR= [195–70.5]) cells/ul, current median CD4 count of 607 (IQR= [796–449]) cells/ul. The overall prevalence of frailty was 59/1017 (5.8%). Main contributors to composite diagnosis of frailty were low physical activity (57 (96.6%)), weak grip strength (44 [74.6%]) and weight loss (35 [59.3%]). In the final multivariable models, being older (aOR (actual estimates are 1.005 [1.003, 1.007]) =1.00 [1.00, 1.01]; P=0.001), having average monthly income less than $100 (aOR [actual estimates are 1.005 (1.003, 1.007)] =1.06 [1.03, 1.10]; P<0.001) and chronic kidney disease (aOR=1.45 [1.11, 1.90]; P=0.007) were all independent predictors of frailty.
Conclusions: Our findings are consistent with results from other studies which show frailty prevalence varying greatly between geographic locations. Further research in our setting is needed to identify context-specific frailty and pre-frailty phenotypes among younger HIV cohorts and assess feasibility of novel interventions to prevent and/or limit progression of frailty in Botswana.
WEDNESDAY 8 DECEMBER – POSTER PRESENTATIONS
ABSTRACT P09
An analysis of insomnia by sex and age in people living with HIV
C Horvat Davey1, AR Webel2, A Willig3, DM Long3, JD Cleveland3, J Fleming4, G Burkholder3, MS Saag3, H Crane2
1Case Western Reserve University, Cleveland, OH, USA; 2University of Washington, Seattle, WA, USA; 3University of Alabama at Birmingham, Birmingham, AL, USA; 4Johns Hopkins University, Baltimore, MD, USA
Objective: People living with HIV (PLWH) are disproportionally impacted by sleep disorders compared to the general population. Sleep disorders, including insomnia, are associated with impaired cognition and functioning, poor treatment adherence and reduced quality of life. Female sex and older age are each associated with more frequent insomnia in the general population, yet conflicting evidence exists regarding sex and age differences for insomnia in PLWH. In turn, it is imperative to recognize the impact biological factors such as sex and age may have on insomnia in PLWH to better understand the biological underpinnings of this symptom.
Methods: We examined the association of sex and age with insomnia among adult (≥18 years) PLWH enrolled in the Impact of Physical Activity Routines and Dietary Intake on the Longitudinal Symptom Experience of People Living with HIV (PROSPER-HIV) study. Patient-reported insomnia was measured by the HIV Symptom Index. Sex and age were obtained from the patients’ medical record. Sex was defined as sex at birth. Linear regression analyses were used to determine the relationship of insomnia with sex and age.
Results: Participants (n=314) were approximately 55 years old (+/- 10.6), 28% were female and 58% were African American/Black. Insomnia was experienced by 57% of participants (70% male versus 30% female), of those 43% reported being bothered by their insomnia, while 14% did not feel bothered by insomnia. Sex (standardized β=0.076, P=0.184) nor age (standardized β=-0.011, P=0.853) were associated with insomnia in PLWH.
Conclusions: More PLWH reported insomnia compared to the general population estimate of 30%. Importantly, previously reported sex and age differences in insomnia prevalence were not observed among PLWH, which provides important information for future management of insomnia. Future studies should consider the influence of other environmental and biological factors when assessing and developing targeted strategies to improve sleep disorders such as insomnia.
ABSTRACT P10
COVID-19, what impact on the mental health of students of the faculty of medicine and pharmacy of Agadir?
I Sellam1, M Elfane2
1University Hospital Center Souss Massa of Agadir, Agadir, Morocco; 2University Hospital Center Souss Massa of Agadir, Agadir, Morocco
Introduction: The impact of the COVID-19 pandemic on mental health is obvious and several surveys report negative effects on people's mental health. However, there are few studies examining the mental health of students during the pandemic. The objective of our work is to assess the impact of the COVID-19 pandemic on the mental health of medical students in Agadir.
Material and methods: This is a descriptive and analytical cross-sectional study carried out among medical students of the Faculty of Medicine and Pharmacy of Agadir. Data collection was done using a web questionnaire on the Google Forms platform. Anxiety and depression were assessed by the Hospital Anxiety and Depression scale (HAD) score, and the screening for Post Traumatic Stress Disorder (PTSD) by the PCL-S score.
Results: Of the 88 participants, 78.4% (n=69) were female, the average age was 21 years. Forty-three (48.9%) students had comorbidities: anxiety in 22.7% (n=20), depression in 15.9% (n=14), sleep disorder in 17% (n=15), asthma in 8% (n=7), diabetes in 2.3% (n=2), heart disease in 1.1% (n=1) and hypothyroidism in 1.1% (n=1) of cases. Eight students (9%) were chronic smokers, 5 students (5.7%) were cannabis users, and one student had a history of self-injury. 78.4% (n=69) of our students had COVID-19. 68.1% (n=47): mild form in 24.6% (n=17), moderate form in 3.4% (n=3) and mild form severe in 1.13% of cases. 62% (n=43) retained clinical symptoms after recovery; dominated by asthenia in 23% (n=10), anosmia in 32% (n=14), myalgia in 13.9% (n=6) arthralgia in 18.6% (n=8) and loss of appetite in 20.9% (n=9) of cases. 43% (n=38) of the students had no anxiety-depressive syndrome (HAD score between 0 and 8), 27% (n=30) had a score between 8 and 11 and 26% (n=23) had a definite anxiety-depressive syndrome (HAD score over 11). Symptoms of PTSD were found in patients in 38 students whether 43.18%.
Conclusions: The effects of the pandemic on mental health will persist for a long time. Thus, psychological follow-up and early psychosocial support strategies should be considered for students.
ABSTRACT P11
SARS CoV-2 seroprevalence and COVID-19 experience among people with HIV in India
RT Khan1, A Pradeep1, AK Srikrishnan1, SH Iqbal1, M Anderson2, GA Cloherty2, MA Rodgers2, CA Devaraj1, R Balakrishnan1, KS Kumar1, L Prasad1, V Murugesan1, R Varan3, S Saravanan1, SS Solomon1,4
1YRGCARE, Chennai, India; 2Abbott Pandemic Defense Coalition, USA; 3Emory School of Arts and Science, Atlanta, USA; 4Johns Hopkins School of Medicine, Johns Hopkins University, Baltimore, USA
Objectives/aim: To examine the exposure to SARS CoV-2, access to testing, response to public health interventions and long-term sequela of SARS CoV-2 infection among people with HIV in India.
Methods: We conducted a cross-sectional analysis of randomly selected PWH who access routine care at a community health clinic in Chennai. Enrolled participants are aged 5 years and older; individuals actively symptomatic for influenza-like illness (ILI) and those with a history of ILI in the past 2 weeks were excluded. The study is designed to follow-up participants for 24 months to examine the longevity of immune response to natural infection and immunization. We present the results of the first 6 months (December 2020 – May 2021). Study data were collected and managed using REDCap data tools. 244 PWH were tested for anti-N SARS CoV-2 IgG (quantified with the Abbott IgG assay with Architect i1000). All analyses were carried out using STATA statistical software (v.15 Stata Corp., College Station, TX, USA).
Results: Overall, 393 ART-exposed people with HIV were enrolled. 62.3% (n=245) identify as cis-women, 37.2% (n=146) as men and 0.5% (n=2) as transgender. Median age was 45 years (IQR 37–51). 67.2% (n=317) reported never having been tested for CoV-2 with RT-PCR. Of 151 individuals with access to SARS CoV-2 RT-PCR, 19.2% (n=29) were symptomatic for ILI and 27.3% (n=42) were detected positive for SARS CoV-2. 83.3% (n=35) did not seek medical care, 11.4% (n=4) were hospitalized for supplemental oxygen and recovered without any complications. 10.4% were seropositive for anti-N SARS CoV-2 IgG (cutoff =1.4); higher seroprevalence was observed in individuals over 45 years and cis-women. 12.5% (n=45) reported being vaccinated against SARS CoV-2; 77.65 received COVIShield, 20.4% received COVAXIN and 2% were unaware of the type of vaccine they received. See Figure 1.
Conclusion(s)/discussion: Testing total antibodies (IgG/IgM/IgA) against N, S1, RBD antigens of SARS CoV-2 using a multi-antigen assay could offer better insights into longevity of immune response to natural infection and immunization among PWH. The overt evidence of low access to testing, hesitation to seek medical care and uptake of vaccination among PWH warrants enhanced efforts to scale-up equitable access to differentiated models of integrated HIV/COVID care.
Abstract P11
THURSDAY 9 DECEMBER – ORAL PRESENTATIONS
ABSTRACT O16
Abnormal spirometry and HRCT are common among youth with HIV in Nairobi, Kenya
EF Attia1, LE Ellington2, JS Zifodya3, E Maleche-Obimbo4, D Omondi5, J Lukorito5, SE Eskander5, M Nderitu5, G Kicska1, M Rosenfeld2, MH Chung6, K Crothers1
1University of Washington, Seattle, WA, USA; 2Seattle Children’s Hospital, Seattle, WA, USA; 3Tulane University, New Orleans, LA, USA; 4University of Nairobi, Nairobi, Kenya; 5Coptic Hope Center for Infectious Diseases; 6Emory University, Atlanta, GA, USA
Objectives: There is a high prevalence of abnormal spirometry among youth with HIV (YHIV). However, the relationship between functional abnormalities detected by spirometry and structural abnormalities identified by chest imaging remains incompletely understood. We determined the association of abnormal high-resolution computed tomography scans of the chest (HRCT) with abnormal spirometry and identified risk factors associated with chronic lung disease (CLD) defined by the presence of concurrent spirometry and HRCT abnormalities.
Methods: We analyzed data from 10–19-year-old YHIV receiving care at the Coptic Hope Center for Infectious Diseases in Nairobi, Kenya. Participants underwent pre- and post-bronchodilator spirometry and HRCT. We defined pre- and post-bronchodilator abnormal spirometry patterns as: obstructive (FEV1/FVC z-score <-1.64), restrictive (FVC z-score <-1.64 and FEV1/FVC z-score >-1.64), or undefined abnormal (FEV1/FVC z-score >-1.64, FEV1 z-score <-1.64 and FVC z-score >-1.64). A radiologist with expertise in thoracic radiology performed semi-quantitative interpretations of HRCT. We generated log binomial models using modified Poisson regression with robust error variances, adjusted for age and sex, to determine relative risk of: (1) abnormal HRCT associated with abnormal spirometry; and (2) risk factors for CLD. A priori, these risk factors included noxious exposures (satellite-level PM2.5; indoor biofuel burning; secondhand smoke), HIV-related variables (current and nadir CD4, CD8, CD4/CD8; WHO HIV class) and log10-transformed serum biomarkers of immune activation (sCD14), endothelial activation (sICAM-1, sVCAM-1) and inflammation (CRP, SAA).
Results: Among 155 YHIV (44% female; median age 15 years [IQR 13–18]), all were on antiretroviral therapy with well-controlled HIV (median CD4 576 cells/µl [IQR 359–787]). Of these, 152 had adequate quality spirometry, and 30 (20%) had an abnormal spirometry pattern: 12 (8%) obstructive, 14 (9%) restrictive, 4 (3%) undefined abnormal. Overall, 92/155 (59%) had at least one HRCT abnormality (Figure 1). Twenty-two had both spirometry and HRCT abnormalities. Presence of an abnormal spirometry pattern was associated with a 30% greater risk of a HRCT abnormality (RR 1.30 (95% CI 0.99, 1.71); P=0.06). We could not evaluate associations of individual abnormal spirometry patterns and HRCT abnormalities because of the small numbers of overlapping findings in these categories. Secondhand smoke exposure (2.24 [1.05-4.74]; P=0.04), current CD4 <200 cells/µl (2.83 [1.19-6.76]; P=0.02), and CRP (1.69 [1.04-2.74]; P=0.03) were associated with a greater risk of CLD.
Conclusions: Spirometry and HRCT abnormalities were common, although radiographic abnormalities were often present without spirometric abnormality. However, most YHIV who had abnormal spirometry also had ≥1 HRCT abnormality. When defined by overlap of abnormal spirometry and HRCT, CLD features were heterogeneous in terms of functional and structural abnormalities. Secondhand tobacco smoke exposure, HIV-related immunosuppression and inflammation are strongly associated with a greater risk of CLD among YHIV, highlighting potential interventions to mitigate the burden of CLD in this vulnerable population.
Abstract O16
ABSTRACT O17
Trends in diabetes incidence and associated risk factors among people living with HIV in the current treatment era, 2008–2018
AL Willig1, G Spieler2, AO Westfall1, DM Long1, A Cherrington1, N Funderburg3, GA Burkholder1, JL Raper1, ET Overton1
1University of Alabama at Birmingham, Birmingham, AL, USA; 2Vanderbilt University, Nashville, TN, USA; 3The Ohio State University, Columbus, OH, USA
Objective: People with HIV (PWH) have an increased risk for diabetes mellitus (DM). Our objective was to characterize DM prevalence and incidence in a cohort of PWH living in the Southern United States, and to evaluate both traditional and HIV-specific risk factors contributing to incident DM.
Methods: We conducted a retrospective longitudinal cohort study of a Southeastern US academic HIV clinic. All PWH age >18 years of age who attended at least one clinic visit between 2008 and 2018 were included for DM prevalence reporting. Those with at least two visits were evaluated for DM incidence. Laboratory, demographic, clinical, medication and diagnoses data were extracted from the Clinic EMR. Time to DM incidence was computed from the entire clinic population for each study year. Univariate Cox proportional hazard models were developed to evaluate associations between each baseline factor and time to DM. Multivariable Cox proportional hazard regression models with time-dependent covariates were created to evaluate the independent association between significant parameters from univariate analyses and time to incident DM.
Results: 4,113 PWH were included in analyses. We identified 252 incident DM cases, with incidence increasing from 1.04% to 1.55% during the 10-year study period. DM prevalence increased from 8.8% in 2008 to 14% in 2018. In multivariable analysis, BMI classification, liver disease, and dyslipidaemia were associated with incident DM (Figure 1). Additional associated factors included lower CD4 cell counts, duration of HIV infection, exposure to non-statin lipid lowering therapy, steroid exposure, and integrase inhibitor use.
Conclusions: Diabetes incidence is increasing at an alarming rate among PWH. Both traditional (body weight, steroid exposure) and HIV-related (CD4 count, use of integrase inhibitors) risk factors were associated with an increased hazard of incident DM. Notably, several of the risk factors identified such as body mass index and comorbid diseases (dyslipidaemia, liver disease) are modifiable and should be targeted for intervention.
Factors associated with increased risk of diabetes diagnosis among people receiving care for HIV in the Southern United States, 2008–2018 (Abstract O17)
ABSTRACT O18
Integrase strand transfer inhibitors are associated with higher blood pressure and renin-angiotensin-aldosterone system activity
M Siddiqui1, ET Overton1, P Muntner1, E Judd1, S Oparil1, G Burkholder1
1University of Alabama at Birmingham
Objectives/aims: People with HIV (PWH) treated with antiretroviral therapy (ART) have a higher prevalence of hypertension than similarly aged HIV-negative individuals (50% versus 30%) and the diagnosis of hypertension increases the risk of cardiovascular events and all-cause mortality. The integrase strand transfer inhibitor (INSTI) are most common ART in PWH. INSTIs have been linked to weight gain and higher levels of inflammatory markers. Weight gain and inflammation influence downstream pathways, which may activate the renin-angiotensin-aldosterone system (RAAS), causing higher BP and increased risk for hypertension. To what extent current ART agents, specifically INSTIs contribute to higher BP and its mechanism remain undefined. The current analysis is designed to test the hypothesis that PWH with hypertension taking INSTI-based ART have higher 24-h ambulatory BP and RAAS activity compared to PWH with hypertension not taking INSTIs.
Methods: Sixty-five PWH (35 receiving INSTI-based ART and 30 non-INSTI-based ART) with diagnosed hypertension were recruited from the University of Alabama at Birmingham 1917 HIV Clinic. We excluded individuals who were diagnosed as having secondary causes of hypertension including primary aldosteronism, renal artery stenosis, pheochromocytoma and use of illicit/recreational drugs. Study measurements included automated office BP, 24-h ambulatory BP monitoring, plasma renin activity and 24-h urinary aldosterone levels.
Results: PWH with hypertension taking versus not taking INSTIs were younger (49 ±10 versus 55 ±9 years), more likely female (80 versus 70%) and of similar ethnicity (77 versus 80% African American) compared to those not taking INSTIs. In addition, PWH with hypertension taking versus not taking INSTIs had higher body mass index (31 ±7 versus 24 ±6 kg/m2) and a higher prevalence of dyslipidaemia (37 versus 17%), diabetes mellitus (23 versus 10%) and obstructive sleep apnoea (20 versus 6%). The group taking INSTIs had higher mean office systolic/diastolic BP (144/94 versus 132/84 mmHg), 24-h systolic/diastolic BP (137/89 versus 129/82 mmHg) and awake systolic/diastolic BP (142/93 versus 133/85 mmHg) when compared to PWH not taking INSTIs. Biochemical testing showed non-suppressed plasma renin activity (17.3 and 11.9 ng/ml/h) and higher 24-h urinary aldosterone levels (10.8 versus 7.2 mcg/24 h) – a marker of increased RAAS activity in the group taking INSTIs. These differences persisted after adjustment for age, sex and race. See Figure 1.
Conclusions/discussion: PWH and diagnosed hypertension taking INSTIs have higher office BP and 24-h ambulatory BP with physiologic upregulation of the RAAS compared to those not taking INSTIs. These findings suggest that RAAS activity may contribute to elevated BP in PWH taking INSTIs. If true, RAAS blockers would be important medication class in the treatment of hypertension and to reduce cardiovascular and renal risk in PWH on INSTIs.
Abstract O18
ABSTRACT O19
Associations between HIV status and hypertension status in a high HIV prevalence population in Manicaland: a cross-sectional study of adults
K Davis1, L Moorhouse1, R Maswera2, P Mandizvidza2, T Dadirai2, T Museka2, C Nyamukapa1,2, M Smit1, S Gregson1,2
1Imperial College London, London, UK; 2Biomedical Research and Training Institute, Harare, Zimbabwe
Objectives/aims: Hypertension is the leading modifiable cause of death and disability worldwide. Globally, there is some evidence that people living with HIV (PLHIV) might be at higher risk of hypertension. However, it has also been suggested that in African countries PLHIV may experience a lower prevalence of hypertension. Detailed information about how the burden of hypertension differs by HIV status remains scarce across the region, constraining understanding of whether HIV is a risk factor for hypertension. To begin to bridge the data gap, this study examined whether HIV status and antiretroviral therapy (ART)-exposure were associated with hypertension in Manicaland, Zimbabwe, and whether access to hypertension treatment differed by HIV status.
Methods: Cross-sectional data from the most recent survey round of the Manicaland Study, a general population open cohort HIV sero-survey, were analysed. During the round, a household census was performed, then all women aged 15–24 years and all men aged 15–29 years, as well as a random sample of two-thirds of older adults, were eligible to complete a survey and undergo HIV testing. Hypertension was defined as reporting a previous diagnosis by a doctor or nurse. All data was gathered between July 2018 and December 2019. In the analysis, survey responses were weighted using data from the household census, then Chi-squared tests and logistic regression were used to explore whether HIV status and ART-exposure were associated with hypertension. Differences in reported uptake of, and payment for, hypertension treatment by HIV status were examined using Chi-squared tests.
Results: The analysis included 9780 participants. Weighted HIV prevalence was 11.1% (95% confidence interval: 10.4%, 11.7%). In univariate analyses there was no evidence of a difference in weighted hypertension prevalence between PLHIV and HIV-negative people (14.1%, 11.9%, 16.3% versus 13.3%, 12.6%, 14.0%; P=0.503) or between ART-exposed and ART-naive PLHIV (14.8%, 12.0%, 17.7% versus 12.8%, 9.1%, 16.4%; P=0.388). Adjusting for socio-demographic variables did not alter this (odds ratios: HIV status: 0.87, 0.69, 1.09; P=0.234, Figure 1; ART-exposure: 0.83, 0.53, 1.30; P=0.411). The proportion of hypertensive people receiving treatment, and paying out-of-pocket, did not differ by HIV status; 43.4% (40.6%, 46.3%) of people treated paid out-of-pocket.
Conclusion(s)/discussion: No association was found between HIV and hypertension or between ART and hypertension in Manicaland, suggesting that other risk factors, such as physical inactivity, may be more important in this population. In contrast with results from other African nations, there was no evidence that PLHIV had an advantage in obtaining hypertension treatment; identification of reasons for this could be valuable in supporting development of accessible services. Finally, care costs were often borne by affected people, indicating a need to improve financing mechanisms. Zimbabwe is re-orienting its health system towards control of non-communicable diseases; these results should be fully accounted for during the process.
HIV status as a determinant of hypertension, results from a fully adjusted logistic regression model (Abstract O19)
ABSTRACT O20
Inflammatory markers associated with cardiac fibrosis in people with HIV: Myocardial And Coronary Abnormalities in HIV Infection (MACHIN) Study
H Bahrami, A Banayan, F Khan, P Reddy, A Minasian, A Javed, K Nayak, MP Dube
University of Southern California, Department of Medicine (Divisions of Cardiovascular Diseases and Infectious Diseases), Los Angeles, CA, USA
Objectives: To determine the association of markers of monocyte activation and microbial translocation with myocardial fibrosis (MF) in people with HIV (PWH) and controls.
Methods: Circulating biomarkers that have been associated with monocyte/macrophage activation (soluble CD163 [sCD163]) and microbial translocation (soluble CD14 [sCD14], intestinal fatty acid binding protein [I-FABP]) were measured in 92 participants: 54 virologically suppressed PWH and 38 HIV- controls (mean age 47 ±14 years, 28% female). Myocardial structure and function were assessed using CMR (GE 3.0T; acquisition: RT-Hawk, Heart Vista Inc; analysis: cvi42, Circle Inc, v5.10). Our protocol included cine, pre-contrast, 12-min post contrast T1 mapping and late gadolinium enhancement (LGE). 12-min extra cellular volume (ECV) maps were generated from T1 maps and higher value for ECV was used as a measure for MF.
Results: PWH had significantly higher levels of sCD163 than controls (mean ±SD: 78 ±6 versus 54 ±5 ng/dl; P-value <0.01). The association of sCD163 with diffuse MF detected by ECV was modified by HIV infection (P-value for interaction: 0.05). Log-sCD163 levels were significantly correlated with ECV in PWH (regression coefficient: 9; P=0.01), but not in controls (P=0.74). The association of sCD163 with ECV remained significant even after adjusting for age, gender, race, and LV function (P=0.02) and history of protease inhibitor and abacavir use to the models (P=0.02). LGE was not significantly associated with sCD163 levels. I-FABP and sCD14 were the only biomarkers related to microbial translocation that were significantly higher in PWH. The percentage of participants in upper tertile of I-FABP levels was higher in PWH compared to controls (47% versus 17%, respectively, OR: 4.4; P=0.01). Participants with upper tertile of I-FABP had a significantly higher odds of myocardial fibrosis (defined as ECV above median) compared to controls (OR: 5.9; P:.02) after adjustment for HIV status, age, gender, and race. Furthermore, participants with high I-FABP also had higher extent of MF (ECV values) compared to controls (adjusted regression coefficient 6.7%; P<0.01). Importantly, while HIV infection was significantly associated with presence and extent of MF, these associations were not significant when I-FABP was added to the models, suggesting the possible role of I-FABP in increased MF in HIV infection. I-FABP levels were not significantly associated with presence of overt scar measured by LGE in MRI. PWH had significantly higher levels of sCD14 compared to controls (2,027 ±636 versus 1,767 ±358; P<0.05), even after adjustment for age, gender, and race (P=0.04). However, sCD14 levels were not associated with systolic function, LV mass, MF, or LGE.
Conclusions: Biomarkers indicating monocyte/macrophage activation and microbial translocation may play a role in increased risk of myocardial fibrosis in virologically-suppressed PWH.
ABSTRACT O21
Automatic retinal image analysis to predict coronary artery disease in at-risk people living with HIV
G Lui1, H Leung2, S Li3, CK Wong4, V Wong1, J Lee3, T Li1, T Ho1, YY Chan1, PW Lee1, KT Wong2, B Zee3
1Department of Medicine and Therapeutics, The Chinese University of Hong Kong; Prince of Wales Hospital, Hong Kong SAR; 2Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Hong Kong SAR; 3The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong SAR; 4Department of Chemical Pathology, The Chinese University of Hong Kong; Prince of Wales Hospital, Hong Kong SAR
Objectives: Traditional risk prediction tools underperform in people living with HIV (PLWH) and are not adequately validated in Asian populations. Features of retinal vasculature correlated with the risk of cardiovascular diseases in some populations. This study aimed to determine the performance of automated retinal image analysis in predicting coronary artery disease (CAD) in PLWH in an Asian population.
Methods: We performed a prospective study enrolling adult PLWH with at least one cardiovascular disease risk factor (including hypertension, diabetes, dyslipidaemia, smoking and obesity). All participants underwent clinical assessment of traditional cardiovascular risk factors, coronary CT angiogram, and retinal imaging with automated analysis of retinal vasculature. The primary outcome was coronary atherosclerosis, defined as presence of any plaques in any coronary artery segment. Secondary outcome was obstructive CAD, defined as 70% or more stenosis of the lumen caused by any lesion. We determined the associations of traditional cardiovascular risk factors and retinal characteristics with the primary and secondary outcomes using stepwise logistic regression analyses. Different models involving traditional and retinal factors were evaluated, and we compared their performances by comparing the area under curve (AUC) of receiver operating characteristic (ROC) curves using Delong method.
Results: We included 115 adult PLWH in the analyses. Mean (± standard deviation) age was 54 ±10 years, 89% male, median (interquartile range/IQR) duration of HIV diagnosis was 12 (7–17) years, 95% had undetectable HIV RNA, and median (IQR) CD4 count was 632 (451–840) cells/mm3, while 52 (45%) had hypertension, 46 (40%) had diabetes, 52 (45%) had dyslipidaemia and 27 (24%) were smokers. Seventy-one (62%) had coronary atherosclerosis and 23 (20%) had obstructive CAD. Coronary atherosclerosis was associated with male sex, older age, dyslipidaemia, hypertension, lower CD4:CD8 ratio, lower HDL cholesterol, and higher triglyceride. Obstructive CAD was associated with older age, dyspnea, lower total cholesterol, lower LDL cholesterol, and higher sCD163. Multiple retinal characteristics were associated with coronary atherosclerosis (including bifurcation coefficient of artery, central retinal arteriolar and venular equivalents, and venous asymmetry index), and obstructive CAD (including bifurcation coefficient of venule, arteriole-venule ratio, bifurcation coefficient of artery, atrial fibrillation, tortuosity and arteriole occlusion). For the prediction of coronary atherosclerosis, the model including both traditional cardiovascular risk factors and retinal characteristics had the highest AUC and was significantly better than that including either clinical or retinal characteristics alone. For the prediction of obstructive CAD, the models including retinal characteristics alone or in combination with traditional risk factors performed significantly better than traditional risk factors alone (Figure 1).
Conclusions: Automated retinal image analysis had better performance in predicting coronary atherosclerosis and obstructive CAD than traditional cardiovascular risk factors alone in adult PLWH at risk of CAD.
Abstract O21
THURSDAY 9 DECEMBER – POSTER PRESENTATIONS
ABSTRACT P12
Increase in pro-atherogenic apolipoprotein B in people living with HIV (PLWH) following switch from tenofovir disoproxil fumarate to tenofovir alafenamide
S Savinelli1,2, D Kasianenko3, AA Garcia Leon2, W Tinago2, AG Cotter2,4, I Walsh5, M Fitzgibbon5, C Sabin6, PWG Mallon1,2, ER Feeney1,2, the UPBEAT Study Group
1Department of infectious Diseases, St Vincent’s University Hospital, Dublin, Ireland; 2Centre for Experimental Pathogen Host Research (CEPHR), University College Dublin (UCD), Dublin, Ireland; 3School of Medicine, University College Dublin (UCD), Dublin, Ireland; 4Department of Infectious Diseases, Mater Misericordiae University Hospital, Dublin, Ireland; 5Department of Clinical Biochemistry & Diagnostic Endocrinology, Mater Misericordiae University Hospital, Dublin, Ireland; 6University College London (UCL), London, United Kingdom
Objectives: Tenofovir alafenamide (TAF) has been associated with weight gain and adverse lipid profiles compared to tenofovir disoproxil fumarate (TDF). The impact of TAF on apolipoprotein (Apo) composition is largely unknown. We compared Apo and lipids between PLWH who switched from TDF to TAF (TDF-TAF) compared to those continuing TDF (TDF-TDF). Methods: Retrospective analysis on PLWH enrolled in the UPBEAT study who were on TDF at baseline and with available data and follow-up samples. ApoA1, ApoB and Lp (a) were measured on plasma by immunoturbidimetry at baseline (T0) and between year 3 and 5 of study follow-up (T1), following switch to TAF in TDF-TAF group. Subjects with exposure to TDF of 2–5 years between the two time points were included. Within- and between-group differences in Apo and lipids were compared using Wilcoxon signed rank test and linear regression, adjusting for T0 values and socio-demographic/clinical variables. Values are n (%) or median (IQR).
Results: 52 PLWH (36 TDF-TDF, 16 TDF-TAF) were included. Differences between TDF-TAF and TDF-TDF groups included: male sex 12 (75%) versus 19 (52.8%); age (46 [41–55] versus 38 [34–47] years); Caucasian ethnicity 12 (75%) versus 21 (58.3%); diabetes 3 (18.8%) versus 2 (5.6%); hypertension 6 (37.5%) versus 6 (16.7%); cardiovascular disease (CVD) 0 (0%) versus 3 (8.3%); duration of ART at T0 (years, 8.13 [6.13–13.35] versus 2.78 [1.03–6.72]). Exposure (years) to TDF between T0 and T1 was 2.86 (2.58–3.48) in TDF-TAF versus 2.43 (2.15–3.62) in TDF-TDF. Exposure to TAF (years) in TDF-TAF was 1.1 (0.54–1.72). Observation time between T0 and T1 (years) was longer in TDF-TAF than in TDF-TDF (4.01 [3.59–4.59] versus 2.42 [2.15–3.62]). Virological suppression at T1 was 16 (100%) in TDF-TAF versus 34 (94.4%) in TDF-TDF. Third agent use at T1 in TDF-TAF versus TDF-TDF was: NNRTI 3 (18.8%) versus 18 (50%); PI 1 (6.3%) versus 12 (33.3%); INSTI 12 (75%) versus 6 (16.7%). Values of Apo and lipids did not change significantly between T0 and T1 within each group, except for ApoB which showed a small (0.17 g/l) but significant increase in the TDF-TAF group (P=0.007), and a non-significant decrease in the TDF-TDF group (Table 1). TDF-TAF switch remained associated with higher levels of ApoB at T1 (B coefficient 0.199, 95% CI [0.53, 0.345]; P=0.009), after adjustment for values at T0 and demographic/clinical confounders.
Conclusions: Despite no change in other lipid and lipoprotein parameters, PLWH switching to TAF had an increase in levels of pro-atherogenic ApoB, which remained associated with TDF-TAF switch after adjustment for socio-demographic and clinical characteristics. Limitations include lack of information on TDF exposure prior to T0 and short exposure to TAF post switch. Further studies are needed to explore the potential impact of such changes on CVD risk in PLWH.
ABSTRACT P13
Patient-reported outcomes after switching to a 2-drug regimen of fixed-dose combination dolutegravir/lamivudine: 48-week results from the SALSA Study
P Kumar1, AE Clarke2, C Jonsson-Oldenbüttel3, M García Deltoro4, S Di Giambenedetto5, C Brites6, L Hocqueloux7, P-L Lu8, J Oyee9, A Oglesby10, J Priest10, E Blair10, B Wynn10, LA Gordon10, E Letang11, J van Wyk11, LA Evitt11
1Georgetown University Medical Center, Washington, DC, USA; 2Royal Sussex County Hospital and Brighton & Sussex Medical School, Brighton, UK; 3MVZ Karlsplatz, Munich, Germany; 4Infectious Disease Service, Consortium General University Hospital of Valencia, Valencia, Spain; 5Fondazione Policlinico Universitario Agostino Gemelli IRCCS, UOC Malattie Infettive, and Dipartimento di Sicurezza e Bioetica, Sezione di Malattie Infettive, Università Cattolica del Sacro Cuore, Rome, Italy; 6Universidade Federal da Bahia, Salvador, Brazil; 7Centre Hospitalier Régional d’Orléans, Orléans, France; 8Kaohsiung Medical University, Kaohsiung, Taiwan; 9GlaxoSmithKline, Brentford, UK; 10ViiV Healthcare, Research Triangle Park, NC, USA; 11ViiV Healthcare, Brentford, UK
Objectives/aim: In the SALSA study (NCT04021290), switching to the 2-drug regimen (2DR) dolutegravir/lamivudine was non-inferior in maintaining virological suppression at week 48 compared with continuing 3- or 4-drug (3/4DR) current antiretroviral regimen (CAR; including pharmacokinetic boosters) in treatment-experienced adults, with high virological suppression in both groups. There were no confirmed virological withdrawals, and dolutegravir/lamivudine demonstrated good safety and tolerability. Patient-reported health outcomes through week 48 are presented.
Methods: SALSA is a randomized, open-label study of virologically suppressed (HIV-1 RNA <50 c/ml) adults on stable 3/4DR for ≥3 months who switched to dolutegravir/lamivudine or continued CAR for 52 weeks. Secondary end points included change from baseline in patient-reported treatment satisfaction and symptom bother, assessed by HIV Treatment Satisfaction Questionnaire (HIVTSQ) and symptom distress module (SDM), respectively, at weeks 24 and 48. For HIVTSQ, high scores represent greater treatment satisfaction (range, 0–60); for SDM, low values indicate less symptom bother (range, 0–80).
Results: Overall, 493 participants were randomized to switch to dolutegravir/lamivudine (n=246) or continue CAR (n=247). At baseline, participants in both groups reported comparable HIVTSQ total scores (median [range]: dolutegravir/lamivudine, 58.0 [24–60]; CAR, 58.0 [34–60]) and lifestyle/ease (dolutegravir/lamivudine, 29.0 [8–30]; CAR, 29.0 [15–30]) and general satisfaction/clinical sub-scores (dolutegravir/lamivudine, 29.5 [12–30]; CAR, 29.0 [17–30]). In participants who switched to dolutegravir/lamivudine, mean increases in HIVTSQ total score and lifestyle/ease and general satisfaction/clinical sub-scores through Week 48 were higher than in those continuing CAR (Figure 1). Treatment satisfaction was high in both groups: >95% of participants reported that they would recommend their present treatment to others (dolutegravir/lamivudine, 99%; CAR, 97%) and would be satisfied continuing their present treatment (dolutegravir/lamivudine, >99%; CAR, 96%). At baseline, SDM scores were comparable between groups (median [range]: dolutegravir/lamivudine, 6.0 (0–59); CAR, 4.0 [0–47]). The dolutegravir/lamivudine group had small improvements in SDM score compared with CAR at weeks 4 and 24 and a similar SDM score at week 48 (Figure 1).
Conclusions/discussion: Participants switching to dolutegravir/lamivudine reported greater early improvements in treatment satisfaction and less symptom distress compared with those continuing CAR, observed as soon as 4 weeks after switch and remaining stable through week 48. Participants in the dolutegravir/lamivudine and CAR groups had been using antiretroviral therapy for an estimated median of 5.3 and 5.9 years, respectively, at SALSA baseline, indicating that dolutegravir/lamivudine switch is associated with improved treatment satisfaction in participants with substantial antiretroviral therapy experience. These findings further support greater patient satisfaction with use of the 2DR dolutegravir/lamivudine versus 3/4DRs.
Abstract P13
ABSTRACT P14
Assessment of coronary inflammation in antiretroviral treated people living with HIV infection and active HIV/HCV coinfection
J Jeudy1, P Patel2*, N George1*, S Burrowes3, J Husson1, J Chua1, RG Weiss4, S Bagchi1
1University of Maryland School of Medicine, Baltimore, MD, USA; 2University of Florida College of Medicine, Gainesville, FL, USA; 3Boston University School of Medicine, Boston, MA, USA; 4Johns Hopkins School of Medicine, Baltimore, MD, USA
*Authors contributed equally to the manuscript work
Objective: Persons living with HIV (PLWH) and coinfected with hepatitis C (dually-infected PLWH) are at increased risk of cardiovascular disease (CVD). Peri-coronary inflammation, measured by fat attenuation index (FAI) on coronary CT angiography (CCTA), independently predicts cardiovascular risk and FAI changes respond to local plaque rupture after percutaneous coronary intervention in the general population. FAI has not been studied in dually-infected PLWH, or in persons asymptomatic for CVD. We tested whether peri-coronary inflammation is increased in mono- or dually-infected PLWH asymptomatic for CVD, and whether inflammation changes over time.
Design: Cross-sectional analysis to determine FAI differences among groups. Longitudinal analysis in monoinfected PLWH to assess changes in inflammation over time.
Methods: Age- and sex-matched mono- and dually-infected PLWH virologically suppressed on antiretroviral therapy (ART), and without prior CVD and matched controls underwent CCTA. Dually-infected PLWH had detectable serum HCV quantitative viral loads and were HCV treatment-naive. Peri-coronary FAI was measured around the proximal right coronary artery (RCA) and left anterior descending artery (LAD). Follow-up CCTA was performed in 22 monoinfected PLWH after 20.6–27.4 months. A multivariable regression analysis was performed to evaluate the association between serostatus and mean FAI adjusting for potential confounders: age, sex, race, LDL-c, lipid lowering medication use and body mass Index (BMI) (<30 and ≥30). A sensitivity analysis was performed after removing six patients who had extreme BMI values (BMI ≥40) in the control group. We examined the change in mean FAI values in RCA and LAD coronary arteries separately from first to second visit using Wilcoxon signed rank test. We investigated associations between baseline and follow-up hs-CRP levels and between integrase strand transfer inhibitor (INSTI) with FAI changes in mono-infected PLWH using adjusted models. The associations between virologic control and other ART classes with FAI change were considered but not possible because all PLWH maintained undetectable viral load at follow-up, two participants received protease inhibitors and four received non-nucleoside reverse transcriptase inhibitors.
Results: 101 participants (48 women) were studied (60 monoinfected PLWH, 19 dually-infected PLWH and 22 controls). In adjusted analyses, peri-coronary FAI did not differ between seropositive groups and controls, in either the primary or sensitivity analyses. Peri-coronary FAI values significantly progressed between baseline and follow-up in monoinfected PLWH (RCA: P=0.001, LAD: P≤.001), despite maintenance of virological suppression. FAI progression in monoinfected PLWH was not associated with baseline or follow-up hsCRP values, or with INSTI use.
Conclusions: Mono- and dually-infected PLWH without history of CVD do not have significantly worse peri-coronary inflammation, assessed by FAI, compared to matched controls. However, peri-coronary inflammation in monoinfected PLWH significantly increased in approximately 2 years. FAI measures may be an important imaging biomarker for tracking asymptomatic CVD progression and assessing response to preventive and therapeutic interventions in PLWH.
ABSTRACT P15
Depression and anxiety symptoms, treatment utilization, and virological failure among adults with HIV in rural Florida
P Manavalan1, A Kwara1, AS Ritter1, Y Li2, Z Zhou2, BW Pence3, RL Cook2
1University of Florida, Division of Infectious Diseases and Global Medicine, Gainesville, FL, USA; 2University of Florida, Department of Epidemiology, Gainesville, FL, USA; 3University of North Carolina, Department of Epidemiology, Chapel Hill, NC, USA
Objectives: In persons with HIV (PWH) in the rural South, a population critically affected by the HIV epidemic, depression and anxiety may undermine efforts to End the HIV Epidemic. Yet, little is known about the proportion of PWH in the rural South with depression and anxiety symptoms who are not on treatment, persistent symptoms despite treatment, or successful treatment. This study sought to examine the proportion of PWH from rural Florida with depressive or anxiety symptoms, those who received treatment, and the association between untreated symptoms and virological failure.
Methods: We analysed cross-sectional survey data from PWH recruited across 9 clinical and community settings in Florida. Analysis was limited to participants residing in rural areas, defined based on the Census-5 Digit Zip Code Tabulation Area (ZCAT-5) classification. Moderate depressive or anxiety symptoms were defined as having a Patient Health Questionnaire-8 (PHQ-8) score ≥10 or a Generalized Anxiety Disorder-7 (GAD-7) score ≥10 respectively. Mild depressive or anxiety symptoms were defined as PHQ-8 or GAD-7 score between 5–9. No depressive or anxiety symptoms were defined as PHQ-8 or GAD-7 score <5. Treated depression and/or anxiety was defined as self-reported receipt of antidepressant medication or counselling within the last 6 months. Individuals receiving treatment were classified as having uncontrolled (PHQ-8 or GAD-7 score ≥5) or well-controlled (PHQ-8 or a GAD-7 score <5) depressive and anxiety symptoms. Bivariate analysis using logistic regression was done to examine the association between untreated depressive and anxiety symptoms and virological failure defined as most recent viral load ≥200 copies/ml obtained in the past year.
Results: From 2014–2018, 198 PWH residing in rural areas (35% between 45–54 years, 60% male, 46% Black, 10% Latinx) were enrolled. Of these participants, 147 (75%) met criteria for depressive and/or anxiety symptoms and/or received depression or anxiety treatment: 62 (34%) had moderate depressive or anxiety symptoms, 59 (33%) had mild depressive or anxiety symptoms, and 60 (33%) had no depressive or anxiety symptoms. Among the 81 (43%) participants receiving depression or anxiety treatment, 67 (83%) had uncontrolled symptoms and 14 (17%) had well-controlled symptoms. Untreated depression or anxiety symptoms (OR 3.7, 95% CI 1.3, 10.1; P=0.01) were associated with virological failure in comparison to participants without depression or anxiety.
Conclusions: This study confirms a high burden of depressive and anxiety symptoms in a sample of rural participants from the South. However, only a subset were on treatment, and even fewer had achieved symptom control. Untreated depressive and anxiety symptoms were associated with virological failure. Interventions to address untreated depression and anxiety are urgently needed to improve HIV outcomes for PWH in the rural South.