Weight gain after initiation of antiretroviral therapy in acute HIV-1
H Kaur1, N Utay2, J Lake3, RC Arduino4, M Hongyu5
1UT Health McGovern Medical School, Houston, TX; 2Memorial Hermann Texas Medical Center, Houston, TX; 3McGovern Medical School, Houston, TX; 4McGovern Medical School, Houston, TX; 5University of Texas Health Science Center, Houston, TX
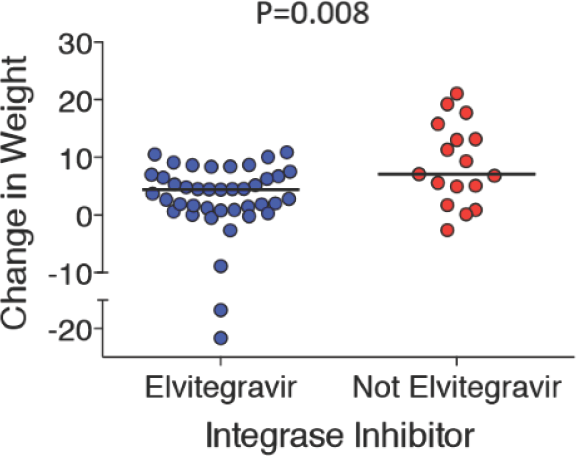
Background: Excess weight gain with integrase strand transfer inhibitors (INSTIs) has been reported in some people with chronic HIV. In antiretroviral therapy (ART)-naive people, greater weight gain over 18 months was reported with dolutegravir than other agents. We hypothesized that initiating an INSTI-based regimen during acute HIV infection (AHI) would result in more weight gain than a non-INSTI-based regimen and INSTIs other than elvitegravir (EVG) would be associated with greater weight gain than EVG.
Methods: We performed a retrospective, observational, single centre chart review analysis of adults with AHI (Feibig Stages 1–5) who were initiated on ART and followed for 48 (±12) weeks. Changes in weight between people on INSTI- versus non-INSTI regimens were compared, and in a subgroup analysis, EVG versus non-EVG and tenofovir alafenamide (TAF) versus non-TAF were compared. Chi-square, t-test or Wilcoxon rank sum test were used, when appropriate.
Results: Overall median (IQR) weight change in 61 people on INSTI was 4.53 (1.22–8.36; within-group P<0.0001) kg. Median weight change in 58 people initiated on INSTI was 4.66 (1.22–8.43; P<0.0001) kg versus 1.64 (-3.08–6.57; P=0.75) kg in 3 people not on INSTI (between-group P=0.33). Median weight change on EVG was 4.40 (0.91–6.71; P<0.0001) kg versus 7.10 (4.97–13.15; P=0.0001) kg for non-EVG INSTIs (between-group P=0.008; Figure 1). Median weight change on TAF (n=33) was 2.66 (0.81–7.53; P=0.002) kg versus 5.31 (3.72–9.34; P<0.0001) kg in non-TAF recipients (n=25; between-group P=0.06). Lower baseline CD4+ T-cell count correlated with greater weight gain (P=0.012). No association between weight gain and race (P=0.930) or gender (P=0.379) was noted.
(Abstract P01)
Conclusions: People initiating ART during AHI gained weight over 48 weeks, with persons taking INSTIs gaining more weight, though this finding did not reach statistical significance due to small sample size. Amongst INSTI-treated persons, those not on EVG gained more weight than those on EVG. While the benefits of starting ART during AHI on immune system preservation and reservoir should not be underscored, risk and consequences of weight gain following ART initiation should be discussed when initiating ART during AHI.
Abstract P02
Antiviral Therapy 2020; 25 Suppl 1:A16
Body weight and lipid changes after switch to dolutegravir-based regimens in IDU and non-IDU
S Savinelli1,2, A Heeney3, W Tinago2, AG Cotter2,3, ER Feeney1,2, PWG Mallon1,2
1Department of Infectious Diseases, St Vincent's University Hospital, Dublin, Ireland; 2Centre for Experimental Pathogen Host Research (CEPHR), University College Dublin (UCD), Dublin, Ireland; 3Department of Infectious Diseases, Mater Misericordiae University Hospital, Dublin, Ireland
Objectives: Increasing evidence from clinical trials and observational studies shows an association between use of integrase strand transfer inhibitors (INSTI), especially dolutegravir (DTG), and weight gain in people with HIV (PWH). Some studies have pointed out the importance of factors like female gender and Black African ethnicity in determining greater weight gain with DTG. Data on people with a history of intravenous drug use (IDU) is lacking. The aim of this study was to evaluate weight and lipid changes following switch to DTG over 96 weeks in IDU and non-IDU.
Methods: We conducted an observational, retrospective analysis on all subjects enrolled in the UCD ID cohort who were switched to DTG. Weight and lipids (total cholesterol, LDL, HDL, total cholesterol/HDL ratio) were recorded at the time of switch, 48 and 96 weeks post-switch, alongside subject's demographic and clinical data.
Paired sample t-test was used to analyse weight and lipid changes within each group at 48 and 96 weeks post-switch. Non-parametric Mann-Whitney test was used to assess the difference in weight and lipid changes between IDU and non-IDU at 48 and 96 weeks post-switch to DTG.
Results: Overall, 138 were included in the analysis. Of these, 96 patients (53 IDU and 43 non-IDU) had weight recorded at baseline and 48 weeks, and 90 patients (43 IDU and 47 non-IDU) had weight recorded at baseline and 96 weeks. All patients were of Caucasian ethnicity Demographic and clinical characteristics of the study population are summarized in Table 1.
(Abstract P02)
Patient's characteristics
IDU [N=73]
NON IDU (N=65)
Age (years): median [IQR]
48 [44 - 53.5]
49 [38-55]
Gender at birth (Male): n (%)
48 (65.75%)
50 (76.92%)
Risk factor for transmission in non-lDU (MSM): n (%)
39 [60%)
Duration of HIV infection (years): median [IQR)
15 [10.7-20]
10 [7-19]
Nadir CD4 count (cells/μL): median [IQR]
206 [127, 317]
330 [211, 412]
CD4 count at switch (cells/μl]: median [IQR]
479 [286, 641]
602 [432,718]
Detectable viral load at switch: n (%)
11 {15%)
3 (4.6%)
NRTI backbone pre-switch: n (%)*
TDF/FTC: 44 (60.2%)
TDF/FTC; 34 (52.3%)
TAF/FTC: 10 (13.7%)
TAF/FTC: 4 (6.1%)
NRTI backbone post-switch: n (%)*
TDF/FTC: 23 (31.5%)
TDF/FTC: 30 (46.1%)
TAF/FTC: 12 (16.4%)
TAF/FTC: 13 (20%)
Third agent pre switch: n (%)
INSTI; 7 (9.6%)
INSTI: 11 (16.9%)
PI: 53 [72.6%)
PI: 15 [23.1%)
NNRTI: 6 (8.2%)
NNRTI: 22 (33.8%)
Tabic 1. Demographic and clinical characteristics of study population. IDU: Intravenous Drug Users; IQR:Interquartile Range; MSW: Men who have Sex with Men; NRTI: Nucleoside Reverse Transcriptase Inhibitors; INSTI: integrase Strand Transfer Inhibitors; PI: Protease Inhibitors; NNRTl: Non-nudeaside Reverse Transcriptase inhibitors; TDF; Tenofovir disproxil fumarate; FTC: emtricitabine; TAF: Tenofovir alafenomide. *other combinations included abacovir/lomivudine or NRTI sparing regimens
The median (IQR) weight at 48 weeks was significantly higher than at baseline in both groups (IDU: 65 kg [56.3–76.9] to 69.5 kg [59.7–81.6]; P 0.007; non IDU: 73.45 kg [66.82–82.45] to 74.25 kg [67.02–86.87]; P 0.003). The median (IQR) weight at 96 weeks was significantly higher in non-IDU only (73.4 kg [66.3–82] to 77.6 kg [70.55–86.7]; P<0.001).
There was not a significant between-group difference in % median (IQR) weight change between baseline and 48 weeks (IDU: 2.26% [-3.81–14.93], non-IDU: 3.43% [-0.88–8.12]; P 0.954), and between baseline and 96 weeks (IDU: -0.48% [-6.06–10], non-IDU: 5.52% [0.72–13.33]; P 0.346). Of note, weight change in non-IDU at 96 weeks was >5%, which is generally considered clinically significant, whereas IDU were more likely to lose weight at 96 weeks, although with a high within-group variability. No significant change in lipid parameters between baseline and 48/96 weeks was observed in IDU and non-IDU.
Conclusions: A significant median weight gain at 48 weeks was observed following switch to DTG in both IDU and non-IDU, without any difference in % weight change between the two groups. Our results suggest that weight gain following switch to DTG might be a widespread phenomenon in patients with different sociodemographic characteristics.
Abstract P03
Antiviral Therapy 2020; 25 Suppl 1:A17
Effect of tesamorelin on diabetic retinopathy and glycaemic control in HIV-infected subjects with diabetes and central adiposity
TT Brown1,R Bedimo2,OG Goss3,CS McGary3,M de Chantal4
1Johns Hopkins University, Baltimore, MD, USA; 2VA North Texas Health Care System and UT Southwestern, TX, USA; 3Syneos Health, Somerset, NJ, USA; 4Theratechnologies, Montreal, Canada
Objectives/aim: People living with HIV (PLWH) have increased risk for excess visceral adipose tissue (VAT) which has been associated with increased risk of cardiometabolic and hepatic diseases (non-alcoholic steatohepatitis). Tesamorelin is a synthetic analogue of growth hormone releasing hormone, approved for treatment of excess VAT in PLWH. Placebo-controlled Phase III trials of tesamorelin in over 800 PLWH showed a minimal effect on haemoglobin A1c (HbA1c) in a population without diabetes mellitus (DM), but its safety in PLWH with DM has not been studied. Therefore, we conducted a Phase IV randomized, placebo-controlled, double-dummy trial in PLWH with excess VAT and DM to determine the effect of tesamorelin on glycaemic control and progression of diabetic retinopathy (DR).
Methods: PLWH with excess VAT and stable DM were randomized 2:1 to tesamorelin (2 mg/day, subcutaneous injection) or placebo for 36 months, with longitudinal assessments of waist circumference (WC) and serum IGF-1 levels. DR was assessed by Early Treatment Diabetic Retinopathy Study (EDTRS) Person scale, at baseline and at 6, 12,24 and 36 months. Significant progression was defined as 3-step or greater progression of DR in at least one eye. Glycaemic control was assessed by change in HbA1c.
Results: Overall, 127 participants were treated for an average of 16.8 ±12.6 months. The study population was 87.4% male, with a mean age of 55.2 ±8.9 years and mean WC of 111.36 ±14.40 cm. Mean HbA1c at baseline was 7.2 ±1.3% and 7.1% had DR. IGF-1 was increased from baseline in the treatment group compared with placebo throughout all 36 months, suggesting participant adherence to tesamorelin. At 12 months, WC tended to decrease in both the tesamorelin group (-3.06 ±6.13 cm,P=0.5) and the placebo group (-1.49 ±10.53 cm,P=0.5), though there was no significant difference between groups (P=0.7). No participant in either arm had development or progression of DR during the treatment period and there were no significant changes in HbA1c from baseline at 12,24 or 36 months (Table 1).
Effect of tesamorelin on DR and HbA1c (Abstract P03)
Tesamorelin
Placebo
P-value
% of participants with ≥3-step progression on ETDRS person (compared with baseline)
Both eyes [n]
0 [18]
0 [14]
1.0
One eye [n]
0 [181
0 [14]
1.0
Difference of HbA1c from baseline (%)
12 months (n)
0.09 ±0.86 (39)
0.14 ±0.76 (29)
0.98
24 months (n)
0.07 ±1.02 (20)
0.36 ±1.03 (20)
0.25
36 months (n)
0.00 ±1.64 (26)
0.62 ±1.75 (20)
0.39
Discussion/conclusion: No difference in progression of retinopathy or glycaemic control was observed over 36 months in PLWH with excess VAT and DM randomized to tesamorelin compared with placebo, providing additional evidence for the safety of tesamorelin in this population.
Abstract P04
Antiviral Therapy 2020; 25 Suppl 1:A18
Dietary habits and impact on cardiovascular disease risk in HIV infection
P McGettrick1,2, R McGrath1, W Tinago2, J O'Brien3, N Mahon4, L Lawler5, A Cotter1,2, T McGinty1, E Muldoon1, J Lambert1,2, G Sheehan1,2, C Sabin6, P Mallon1,2
1Department of Infectious Diseases, Mater Misericordiae University Hospital, Dublin, Ireland; 2Centre of Pathogen Host Research, School of Medicine, University College Dublin, Dublin, Ireland; 3Department of Radiology, University Hospital Limerick, Limerick, Ireland; 4Department of Cardiology, Mater Misericordiae University Hospital, Dublin, Ireland; 5Department of Radiology, Mater Misericordiae University Hospital, Dublin, Ireland; 6Research Department of Infection and Population Health, University College London, London, United Kingdom
Background: People living with HIV (PWH) have twice the risk of cardiovascular disease (CVD) compared with the general population with data on dietary intake, a measure of socioeconomic status and a contributor to CVD risk, limited in PLWH. We aimed to investigate differences in dietary intake, calculated by food frequency questionnaire (FFQ), between PLWH and CVD risk matched controls and examine associations between HIV and subclinical CVD measured by coronary CT angiography (CCTA), adjusting for these differences.
Methods: The UPBEAT CAD substudy, examining CVD risk in PWH, enrolled participants with and without HIV over 40 years with no CVD history, matched on HIV status and CVD risk factors. Participants underwent an FFQ and CCTA to assess for subclinical CVD. Nutritional data were calculated using Nutritics dietetics software (Dublin 2020). Data are reported as median (IQR). Between-group comparisons and associations between variables and subclinical CVD were calculated using Mann–Whitney U test and logistic regression, respectively.
Results: 99 participants were included, of which 51 were PWH, median age was 49.8 (45.6–55.8) years, 73.5% male, 76.5% Caucasian and 22.4% were current smokers. PWH had lower HDL cholesterol (1.27 [1.0–1.3] versus 1.4 [1.1–1.6] in HIVneg; P=0.017), were less likely to have a family history of CVD (37% versus 58% in HIVneg; P=0.036) and more likely to be on statin therapy (49%, versus 12%, respectively; P<0.01). Other demographics and cardiovascular risk factors were similar between the groups.
Based on FFQ, PLWH had less daily intake of protein (93.2 [83.7–141.6] g versus 127.2 [98.8–181.4] g; P=0.043), caffeine (382.7 [,197] mg versus 3,325 [,633] mg; P=0.049) and alcohol (4 [0.02– 13.48] g versus 8.9 [2.9–15.39] g; P=0.035) in PWH and HIVneg, respectively. There was no difference in total daily calorie, carbohydrate, sugar, fbre, cholesterol and fat intake between groups.
Prevalence of any coronary plaque was similar between the two groups (PWH; 33%, HIVneg 40%; P=0.494). On univariate analysis comprising the whole cohort, there was no association between either food group intake (Figure 1) or HIV status with presence of total plaque (OR 0.75 [95% CI 0.329,1.711]) or non-calcified plaque (OR 3.1 [95% CI 0.712,13.6]; P=0.132). Adjusting for difference in dietary intake between the two groups, HIV status remained not associated with either total plaque (OR 0.874 [95% CI 0.351,2.181]) or non-calcified plaque (OR 0.474 (95% CI 0.100, 2.255).
(Abstract P04)
Conclusions: These results, the first to examine dietary impact on CVD risk in PWH, suggest differences in dietary intake may not predict subclinical CVD in PWH.
Abstract P05
Antiviral Therapy 2020; 25 Suppl 1:A20
Frailty in ageing people living with HIV: a matched controlled study
L Lellouche1, C Berr1, L-A Gutierrez1, P Leclercq2, O Zaegel-Faucher3, L Bernard4, M Vassallo5, C Barbuat6, A Ozguler7, M Zins7, V Petrov-Sanchez8, J Reynes9, A Makinson9
1INSERM, University of Montpellier, Neuropsychiatry: Epidemiological and Clinical Research; 2Infectious Disease Unit, University Hospital of Grenobles Alpes, and Fédération d'Infectiologie Multidisciplinaire de l'Arc Alpin, Université Grenoble Alpes; 3Clinical Immuno-Hematology Department, Aix-Marseille University, Sainte-Marguerite University Hospital, Marseille; 4Infectious Diseases Unit, University Hospital Tours; 5Department of Internal Medicine, Cannes General Hospital; 6Infectious Diseases Department, University Hospital, Nîmes; 7INSERM, Paris Descartes University Population-based Epidemiological Cohorts Unit, Villejuif; 8ANRS (France Recherche Nord & Sud Sida-HIV Hépatites), Unit for Basic and Clinical Research on Viral Hepatitis and HIV, Paris; 9Infectious and Tropical Diseases Department, University Hospital Montpellier, Institut de Recherche et Développement, INSERM, University of Montpellier, all in France
Objective: Data on the relationship between HIV infection and frailty syndrome are limited. We compared the prevalence of frailty among middle-aged people living with HIV (PLHIV) with controlled HIV-unexposed individuals.
Methods: This cross-sectional multicentric study consecutively included 200 PLHIV from the ANRS EP58 HAND 55-70 Study and 1,000 HIV-uninfected individuals from the French national CONSTANCES cohort, matched on age, sex and education level. To be included, PLHIV were aged 55–70 years, had controlled HIV disease (HIV viral load <50 copies/ml and a lymphocyte T-CD4 level >200 cells/μl for the last 24 and 12 months, respectively). A pre-defined quota of a third of participants per 5 years age ranges (55–59; 60–64; 65–70) were included. Our main outcome was a measure of frailty (>2 items) and pre-frailty (one or two items) using a proxy of the 5-item Fried score. Multivariate logistic regression was performed to assess the association between HIV and frailty/pre-frailty, adjusting for demographic, social, behavioural and comorbidity con-founders. This study was sponsored by Inserm-ANRS (Institut national de la santé et de la recherche médicale - France REcherche Nord & Sud Sida-hiv Hépatites).
Results: Full outcome measures were available for 192 PLHIV and 822 HIV-unexposed individuals. The median age was 62 years and 84.9% were male. Among PLHIV, the median CD4 cell count was 645.5 cells/μl. The prevalence of frailty was 5.73% in PLHIV versus 1.73% in controls, and of pre-frailty 57.29% versus 52.19%. HIV was statistically associated with pre-frailty/frailty when adjusting on the matching variables of age, gender and education level (OR=1.92; CI95%=1.40, 2.62). After adjusting for social and behavioural factors and comorbidities, HIV was not signifi-cantly associated with pre-frailty/frailty (OR=1.26; 95% CI=0.87, 1.83). Frailty/prefrailty in PLHIV was associated with active smoking, chronic kidney disease, depression and abstinence in alcohol use disorder. Conclusions/discussion: Prevalence of frailty is increased in an ageing PLHIV with well controlled HIV disease, but other factors than HIV are predominant. Longitudinal studies are however still needed in middle-aged PLHIV with controlled HIV viraemia to assess possible links between HIV and frailty.