Non-alcoholic fatty liver disease (NAFLD) in HIV-monoinfected patients: results from the European ECHAM study
P Ingiliz1, L Assoumou2, S De Wit3, P-M Girard4, M A Val antin5, C Katlama5, C Necsoi3, P Campa4, AD Huefner6, J Schulze zur Wiesch6, H Rougier4, J-P Bastard7, S Mauss8, L Serfaty9, V Ratziu10, Y Menu11, D Costagliola2, G Behrens12, M Lemoine1, J Capeau7, the ANRS-ECHAM group
1Center for Infectiology, Berlin, Germany; 2Sorbonne Université, INSERM, Institut Pierre Louis d'Épidémiologie et de Santé Publique (IPLESP), Paris, France; 3Department of Infectious Diseases and Tropical Medicine, CHU Saint-Pierre, Université Libre de Bruxelles, Brussels, Belgium; 4APHP Saint-Antoine Hospital, Department of Infectious Disease and Tropical Medicine, Sorbonne University, France; 5Department of Infectious Disease and Tropical Medicine, Pitie-Salpetriere Hospital, University Paris 6, Paris, France; 6Infectious Disease Unit, University Medical Center, Hamburg-Eppendorf, Hamburg, Germany; 7Service de Biochimie, UF Bio-marqueurs Inflammatoires et Métaboliques, AP-HP, Hôpital Tenon, Paris, France; 8Center for HIV and Hepatogastroenterology, Düsseldorf, Germany; 9Department of Hepato-Gastroenterology, Hautepierre Hospital, Hôpitaux Universitaires de Strasbourg, INSERM UMR-S938, Paris Sorbonne University, Paris, France; 10Department of Hepatology, Pitie-Salpetriere Hospital, University Paris 6, Paris, France; 11 Department of Radiology, Saint-Antoine Hospital, University Paris 6, Paris, France; 12Department of Clinical Immunology and Rheumatology, Hannover Medical School, Hannover, Germany
Background: Metabolic liver disease and unexplained transaminase elevations are common features in mono-infected people living with HIV (PLWH) on antiretro-viral treatment (ART). They generally result from the presence of non-alcoholic fatty liver disease (NAFLD), a growing concern in this population. However, the real impact and role of NAFLD in inducing advanced liver disease in PLWH remains unknown.
Methods: We conducted a multicentre European study (ECHAM) in order to determine the prevalence and risk factors of liver steatosis and fibrosis in ART-controlled monoinfected PLWH over 40 years of age with either a metabolic syndrome (MetS) or persistently elevated liver enzymes or clinical lipodystrophy. Participants were prospectively enrolled and had a full liver and metabolic assessment including magnetic resonance imaging proton density fat fraction (MRI-PDFF), vibration-controlled transient elastography with also determination of CAP values (VCTE, Fibroscan®) and serological markers. Following our validation study, MRI-PDFF and CAP were used as the best diagnostic methods for the detection of moderate-to-severe liver steatosis and aspartate-aminotransferase (AST) to platelet ratio-index (APRI) of significant fibrosis.
Results: From March 2014 to November 2015, we enrolled 442 participants and analysed 402 of them: male (85%), median age 55 years (IQR 50–61), median BMI 26.0 kg/m2 (23.6–28.7), median CD4 cell count 630/mm3 (510–832), 67% met the definition of MetS. Significant liver steatosis (MRI-PDFF ≥10%), fibrosis (APRI ≥0.5), cirrhosis (APRI ≥2) were observed in 36%, 29% and 2%, respectively. Multivariable analysis iden-tified seven factors independently associated with stea-tosis: ALT (OR: 1.23 [1.16–1.31] per additional 5U), CD4 T-cell count (OR: 4.04 [1.92–8.51] per additional log2 U), ferritin (OR: 1.05 [1.03–1.07] per additional 10U), triglycerides (OR: 1.48 [1.18–1.84] per additional U), leptin (≥3.2 μg/l, OR: 2.12 [1.14–3.93]), HDL (<1 mmol/l for men, <1.3 mmol/l for women, OR: 1.83 [1.03–3.27]), non-CC PNPLA3 genetic polymorphism (OR: 1.92 [1.11–3.33]). Otherwise, three independent factors were associated with significant liver fibrosis: duration of ART exposure (OR: 1.07 [1.02– 1.12] per additional year), insulin resistance (HOMA ≥2.5, 2.04 [1.25–3.35]) and MRI-PDFF ≥10% (OR: 3.21 [1.99–5.18]).
Using MRI-PDFF as a reference, the CAP technique (cutoff 280 dB/m), had good accuracy (0.86 [0.82–0.90]) for the diagnosis of moderate-to-severe steatosis.
Conclusions: MRI-PDFF and CAP (280 dB/m threshold) are valuable tools for identification of steatosis in ART-controlled monoinfected PLWH with either a metabolic syndrome or unexplained liver enzyme elevation or lipodystrophy. Significant liver steatosis is frequent and is associated with classic features of the metabolic syndrome and a high CD4 cell count. Liver fibrosis is common and some patients develop cirrhosis. Independent risk factors for liver fibrosis are duration of ART exposure and insulin resistance together with hepatic steatosis, indicating that metabolic liver disease and ART participate in liver fibrosis in this at-risk population which therefore requires screening and monitoring.
Abstract O02
Antiviral Therapy 2020; 25 Suppl 1:A2
Progression of liver disease in the post direct-acting antiviral (DAA) era of HCV therapy among those with and without HIV
O Belliveau1, M McLaughlin1, H Masur2, S Kottilil1,3, C Hadigan1
1NIAID, National Institutes of Health, Bethesda; 2CCMD, National Institutes of Health, Bethesda; 3Institute of Human Virology, University of Maryland, Baltimore, USA
Objectives: Highly effective direct-acting antiviral (DAA) therapy has led to successful HCV clearance for the overwhelming majority of treated patients with and without HIV. HIV coinfection has been shown to increase rates of liver disease progression in chronic HCV, yet little is known about long-term prognosis for persons living with HIV (PLWH) after HCV clearance. This study aims to characterize all-cause mortality and progression of liver disease in patients with chronic HCV with and without HIV in the post-DAA era.
Methods: We conducted a prospective longitudinal cohort study of 443 participants infected with HCV (n=199 coinfected with HIV) in the greater Washington, DC region. Participants were seen annually for laboratory assessments, HIV–HCV viral load determination and HCC screening as indicated. Progression of liver disease was defined as a new development of varices, ascites, jaundice, portal hypertension, hepatic encephalopathy, hepatocellular carcinoma, liver transplant or cirrhosis after enrolment. We used SAS JMP version 14 for statistical analyses.
Results: At time of enrolment, median age was 58 years. The median duration of follow-up was 39.4 months. The cohort was 74% male and 81% Black. More than half of participants (72%) achieved sustained virological response (SVR) either at enrolment or prior to progression of liver disease, censoring or death, and 16% had a diagnosis of cirrhosis at baseline. There was no difference between PLWH and those without HIV with regard to all-cause mortality, progression of liver disease or incidence of liver-related events (death or disease progression). HCV viral clearance with achievement of SVR was associated with reduced mortality (P<0.0001), reduced progression of liver disease (P<0.0001) and reduced incidence of liver-related events (P<0.0001). Further, presence of cirrhosis was also associated with liver disease progression events (P<0.0001) and incidence of any liver-related event (P<0.0001) as well as mortality (P=0.005). BMI category, sex, history of diabetes, current smoking and history of intravenous drug use were also evaluated and were not found to be associated with overall incidence of liver-related events. See Figure 1.
(Abstract O02)
Conclusions: This study affirms the importance of HCV treatment and subsequent viral clearance in protecting against progression of liver disease and mortality. In this cohort study, PLWH had similar long-term outcomes and HIV was not shown to affect liver disease progression or mortality.
Abstract O03
Antiviral Therapy 2020; 25 Suppl 1:A3
Distinct lipidomic signatures between persons living with HIV and seronegative persons: combined analysis of the ACTG 5260s and the MACS/WIHS Combined Cohort Studies
J Jao1, LC Balmert2, S Sun3, GA McComsey4, TT Brown5, PC Tien6, J Currier7, JH Stein8, Y Qiu9, IJ Kurland9, D LeRoith10
1Northwestern University Feinberg School of Medicine, Department of Pediatrics, Division of Pediatric Infectious Diseases, Department of Medicine, Division of Adult Infectious Diseases; 2Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Division of Biostatistics; 3Ann and Robert H. Lurie Children's Hospital of Chicago, Department of Pediatrics, Division of Pediatric Infectious Diseases; 4University Hospitals Cleveland Medical Center and Case Western Reserve University, Cleveland, OH, USA, Department of Pediatrics, Department of Medicine; 5Johns Hopkins University, Baltimore, MD, USA, Department of Medicine, Division of Endocrinology, Diabetes, and Metabolism; 6University of California, San Francisco, Department of Medicine and Department of Veterans Affairs Medical Center, Division of Infectious Diseases; 7University of California, Los Angeles, CA, USA, Department of Medicine, Division of Infectious Diseases; 8University of Wisconsin School of Medicine and Public Health, Department of Medicine, Cardiovascular Medicine Division; 9Albert Einstein College of Medicine, Bronx, NY, USA, Stable Isotope and Metabolomics Core Facility, Department of Medicine, Fleischer Institute for Diabetes and Metabolism; 10Icahn School of Medicine at Mount Sinai, Department of Medicine, Division of Endocrinology
Objectives/aims: HIV and antiretroviral treatment (ART) cause metabolic derangements, but the distinct effects of HIV infection and ART on specific metabolic pathways are not known. We assessed the association of HIV and ART on the metabolome and lipidome.
Methods: We performed widely-targeted metabolomic and lipidomic profiling of plasma from ART-naive persons living with HIV (PLHIV) before and after initial ART therapy in the AIDS Clinical Trials Group study A5260s and in HIV-seronegative participants from the Multicenter AIDS Cohort Study/Women's Interagency HIV Study Combined Cohort. For this analysis, PLHIV who did not meet criteria for successful treatment (HIV RNA level <20 copies/ml by 24 and through 96 weeks of ART with no ART interruptions) were excluded. HIV-seronegative participants were frequency-matched by age, sex, race and body mass index (BMI). Metabolites and lipid subspecies were measured via mass spec-trometry (Sciex 6500+ QTRAP). Orthogonal partial least squares discriminant analysis (OPLS-DA) and volcano plots were used to assess if differences in metabolites and lipid subspecies discriminated between HIV-seronegative participants and ART-naive PLHIV as well as ART groups.
Results: Of 435 participants, 218 were PLHIV (75 randomized to RAL-based, 77 to DRV/r-based, 66 to ATV/r-based ART) and 217 were HIV-seronegative. All PLHIV received a backbone of tenofovir/emtricitabine. Prior to ART initiation, PLHIV were slightly younger (37 versus 44 years), compared with seronegative participants, but race, sex, BMI and history of dyslipidae-mia were similar between groups. In addition, 58 (27%) PLHIV had CD4 count <200 cells/mm3 and 49 (22.5%) had an HIV RNA level >100,000 copies/ml. OPLS-DA indicated that metabolites and lipid subspecies could distinguish between individual comparisons of HIV-seronegative participants with ART-naive PLHIV, PLHIV after 96 weeks of raltegravir (RAL)-based ART and PLHIV after 96 weeks of darunavir/ritonavir (DRV/r) or atazanavir/ritonavir (ATV/r)-based ART. Volcano plots of the metabolites identified by OPLS-DA with variable importance in projection (VIP) values >1 demonstrated that ART-naive PLHIV had a unique lipidomic imprint primarily driven by higher levels of triacylglycerols (TAGs) having polyunsaturated fatty acid (FA) side chains (Figure 1A), suggesting an inflammatory predisposition. RAL-based ART was associated with a shift in the lipidome such that unsaturated TAGs were lower compared with HIV-seronegative participants (Figure 1B). However, DRV/r- or ATV/r-based ART promoted a shift in the lipidome characterized by both higher unsaturated TAGs and higher saturated TAGs with shorter mono/saturated FAs, compared with HIV-seronegative participants (Figure 1C), suggesting both a lipogenic and inflammatory propensity.
(Abstract O03)
Conclusion: ART-naive PLHIV have a unique lipidomic signature primarily composed of higher unsaturated TAGs, suggesting an inflammatory state ameliorated by RAL-based ART. In PLHIV on ART, we observed ART class lipidomic response differences (RAL versus DRV/r or ATV/r) compared with HIV-seronegative persons that may identify individuals at higher risk for derangements in specific metabolic pathways involving lipogenesis.
Abstract O04
Antiviral Therapy 2020; 25 Suppl 1:A5
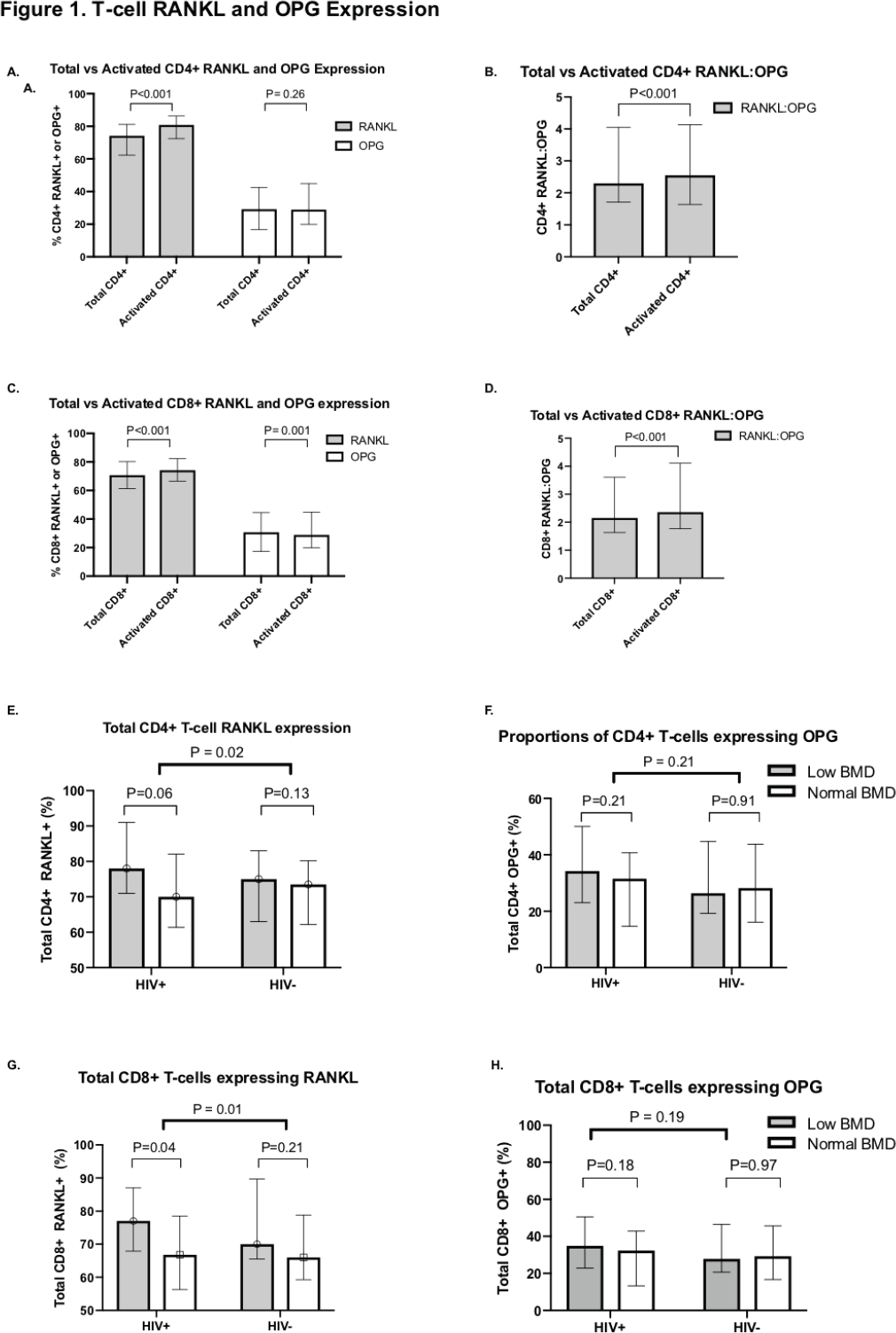
Relationships between T-cell activation, RANKL and OPG expression and low bone mineral density in HIV+ and HIV- subjects in the HIV UPBEAT cohort
T McGinty1,2, W Tinago1, A Landay3, J Martinson3, C Prior2, B Doak2, A Macken1, G Sheehan1,2, J Lambert1,2, AG Cotter1,2, PWG Mallon1,6, the HIV UPBEAT (Understanding the Pathology of Bone Diseases in HIV-infected Subjects) Study Group
1Centre for Experimental Pathogen Host Research, School of Medicine, University College Dublin, Ireland; 2Mater Misericordiae University Hospital, Dublin, Ireland; 3Department of Immunology, Rush University Medical Centre, Chicago, USA; 4St. Vincents University Hospital, Elm Park, Dublin, Ireland
Introduction: Persistent immune activation, despite antiretroviral therapy (ART), in people with HIV (PWH) has been implicated in the development of serious non-AIDS events including low bone mineral density (BMD). T-cells express receptor activator of NF-kB ligand (RANKL) and osteoprotegrin (OPG), the cytokines controlling bone resorption and formation, respectively. We explored relationships between T-cell activation, RANKL and OPG expression and low BMD in PWH and HIV- subjects within the HIV UPBEAT cohort.
Methods: HIV UPBEAT, a single-site, prospective, cohort study, recruited PWH and HIV- subjects from similar backgrounds. Demographics, clinical history, lumbar spine (LS) and femoral neck (FN) BMD measured by dual X-ray absorptiometry (DXA) were recorded. T-cell activation (CD4/CD8+ CD38+HLA-DR+) and T-cell RANKL and OPG expression were evaluated in cryopreserved PBMCs by flow cytometry. Low BMD was defined as T-score <-1 in those >40 years or Z-score <-2 in those <40 years. Logistic regression was used to explore associations between covariates and LS or FNBMD, respectively.
Results: Of 219 subjects, 107 (48.8%) were PWH (68% male, 34% African, age 47 [39–53] years, 30% smokers, 100% on ART) and 112 were HIV- (48% male, 17% African, age 50 [44–56] years, 15% smokers). Compared with the HIV- group, PWH had an increased prevalence of low BMD (40 [37%] versus 14 [11%], P<0.001) and higher CD4/CD8+ T-cell activation (both P=0.004).
Activated CD4/CD8+ T-cells had significantly higher RANKL, but not OPG, expression resulting in a higher RANKL:OPG ratio compared with total CD4/CD8+ T-cell RANKL:OPG (P<0.001; Figure 1). Despite higher CD4/CD8+ activation in PWH, neither CD4/CD8+ RANKL/OPG expression nor respective RANKL:OPG ratios differed between PWH and HIV- subjects.
(Abstract O04)
In the subgroup with low LSBMD, CD4/CD8+ RANKL, but not OPG, expression was altered, largely attributable to increased CD4/CD8+ RANKL expression in PWH (Figure 1).
Low LSBMD was associated with being HIV+ (OR 5.76 [2.37,14.0]; P<0.001) and increased total CD4/ CD8+ RANKL expression (OR [per 5% increase] 5.25 [5.05,5.45], P=0.01 and 5.20 [5.05,5.40], P=0.01, respectively).
In analysis adjusted for HIV+ status, age, gender, ethnicity, BMI and smoking status, being HIV+ was independently associated with low LSBMD (OR 3.30 [1.34,8.14]; P=0.008). Both higher CD4+ (OR 5.19 [5.03,5.35]; P=0.02) or CD8+ (OR 5.15 [5.0,5.30]; P=0.02) RANKL expression remained independently associated with low LSBMD. In our final model, both being HIV+ and higher CD4/CD8+ RANKL expression were independently associated with low LSBMD. We did not find any associations between HIV status, CD4/CD8+ RANKL or OPG expression and FNBMD.
Conclusions: Despite effective ART, PWH who had low LSBMD had significant increases in CD4/CD8+ RANKL expression, without corresponding OPG increases compared with HIV- subjects. This data supports a role for the dysregulation of T-cell RANKL/OPG axis in bone loss in PWH, in particular at the LS, which may be driven by persistent T-cell activation.