1University of Cincinnati, Cincinnati, OH, USA; 2Case Western Reserve University, Cleveland, OH, USA
Objectives/aim: Depression is the most common neuropsychiatric comorbidity among people with HIV (PWH), with prevalence rates 3–4 times that of non-infected individuals. We aimed to describe the relationship between depression and comorbidity diagnoses in a sample of PWH.
Methods: Cross-sectional secondary analysis of medical record and symptom data collected in an international, multisite study of physical activity patterns in PWH. We abstracted data from participant medical records to determine current diagnoses with mental health, cardiovascular, pulmonary, endocrine, neurocognitive, hepatic and cancer comorbidities. To determine the effect of depression, we used forward selection to build a regression model from a set of statistically significant (P≤0.05) candidate predictor variables. We used Poisson regression to analyse the relationship between a current diagnosis of major depressive disorder and the total number of current comorbidity diagnoses. We then used correlation matrices to identify specific comorbidity diagnoses that were significantly associated with a current diagnosis of major depressive disorder.
Results: We included data from 503 PWH for whom we had accurate chart abstraction data. Approximately 60% (n=304) were men, 55% (n=276) were Black, with a mean age of 52 (±10.41) years. Nearly half (46.32%) of the participants were diagnosed with at least one comorbid condition at the time of the study (range: 0–8 diagnoses). Major depressive disorder (P<0.001), recent higher fatigue symptom rating (P<0.01) and White race (P=0.045) had significant positive associations with being diagnosed with a greater number of comorbid conditions at the time of the study. PWH with major depressive disorder were diagnosed with significantly greater numbers of comorbidities when controlling for fatigue levels and race, and no interaction effects between major depressive disorder, fatigue, or race were found in our analysis. Major depressive disorder diagnosis was most strongly associated with cardiovascular (HTN, ischemic heart disease, valvular heart disease; P<0.001) and pulmonary (COPD, asthma; P<0.001) comorbidities. See Table 1.
(Abstract P39)
Dependent Variable: Total number of Comorbid Conditions
Poisson Regression: Relationship between Current Diagnosis of Major Depressive Disorder and Total Number of Comorbid Conditions
Significant at the level of p<0.001
Significant at the level of p<0.05
Discussion: We found that a current depression diagnosis was associated with a greater number of comorbidities, in particular cardiovascular and pulmonary diagnoses. Despite its high prevalence, depression remains under-diagnosed and under-treated in PWH. Depression is both a major risk factor and a consequence of comorbidities. Failure to address depression increases mortality and decreases adherence to treatment regimen(s). Future research should examine specific pathways between depression and comorbidities in PWH and develop interventions to promote and maintain long-term treatment in PWH who suffer from comorbid depression.
Abstract P40
Antiviral Therapy 2019; 24 Suppl 1:A95
Prevalence of HIV-associated neurocognitive disorder (HAND) in Turkey and assessment of Addenbrooke's Cognitive Examination Revised (ACE-R) test as a screening tool
V Korten1, E Harι2, U Ay2, E Tigen Tükenmez1, S Gencer3, S Akça Kalem4, A Demirtaş Tatlιdede4, İ Hakan Gürvit4
1Department of Infectious Diseases, Marmara University School of Medicine, Istanbul, Turkey; 2Department of Neuroscience, Istanbu University, Aziz Sancar Experimental Medical Research Institute, Çapa, Istanbul, Turkey; 3Lutf Kιrdar Hospital, Istanbul, Turkey; 4Department of Neurology, Behavioral Neurology and Movement Disorders Unit, Istanbul University, Istanbul Faculty of Medicine, Çapa, Istanbul, Turkey
Objectives: We aimed to determine the prevalence and associated factors for HAND among HIV-infected patients in Turkey. In addition, Addenbrooke's Cognitive Examination Revised (ACE-R) and three Simioni questions (3Qs; EACS Guidelines) were also assessed as potential screening tools for HAND.
Methods: HIV-infected patients were enrolled consecutively from two different teaching hospitals in Istanbul, Turkey, between March 2018 and September 2018. Persons with a history of confounding neurological or psychiatric disorders or active substance abuse and non-native speakers were excluded from participation. Patients underwent the two screening tools, a neuropsychological (NP) test battery covering seven cognitive domains and an assessment of activities of daily living. HAND was diagnosed according to the Frascati's criteria and applying Global Deficit Score (GDS) approach. A receiver operating characteristic (ROC) curve analysis was performed to compare the predictive accuracy of ACE-R to the NP test battery. Several demographic and disease factors were evaluated for association with HAND using a multivariate logistic regression analysis.
Results: The study population included 162 participants (median age: 43.5 years, 94% male, median education: 13 years, median nadir CD4: 295 cells/ml and median current CD4: 630 cells/ml). Plasma HIV RNA was <200 copies/ml in 158 (97.5%) subjects. The median time on ART was 3 years (IQR 1.5-6.6). HAND prevalence was 45.7% (asymptomatic neurocognitive impairment [ANI]=37.7%; mild neurocognitive disorder [MND]=7.4%; HIV-associated dementia [HAD]=0.6%) according to the Frascati criteria, and 31.5% (ANI=25.9%; MND=4.9%; HAD=0.6%) using the GDS. Memory (learning, recall; 27.2%), attention/working memory (24.7%) and planning/executive (20.4%) were the most frequently impaired domains. In ROC analysis, the ACE-R showed an area under the curve of 0.74 at a cutoff score of 89 (Figure 1). Sensitivity, specificity and correct classification rate (CCR) of screening tests for HAND diagnosis were as follows: ACE-R (62.2%, 67%, 64.8%) and 3Qs (10.8%, 88.6%, 53%). Considering only symptomatic neurocognitive disorders, ACE-R presented a CCR of 61%. In multivariate analysis, only education level (aOR: 0.84; 95% CI: 0.76, 0.92; P=<0.001) was an independent risk factor for HAND.
Conclusions: This is the first study evaluating neurocognitive impairment in Turkish HIV population using normative data. Despite a very well controlled population, HAND is a prevalent comorbidity in HIV-infected persons in Turkey. The sensitivity of ACE-R and 3Qs as screening tools are lower than desired.
(Abstract P40)
Abstract P41
Antiviral Therapy 2019; 24 Suppl 1:A97
Reproductive and sexual health knowledge, experiences and milestones in young adults with life-long HIV
JA Aepfelbacher1, CS Chaudhury1, T Mee2, JB Purdy2, K Hawkins3, K Curl1, N Dee1, C Hadigan1
1National Institute of Allergy and Infectious Diseases; 2Critical Care Medicine Department; 3Nursing Department, NIH Clinical Center, Bethesda, MD, USA
Objective: Reproductive and sexual health outcomes of adults with perinatal human immunodeficiency virus (PHIV) have not been well-characterized to date. Little is known about the impact HIV has on this population's reproductive and sexual outcomes and satisfaction, their transmission knowledge, or their experiences with the health-care system as it pertains to family planning. Using a secure web-based platform, we assessed these questions in a cohort of reproductive aged persons living with HIV (PLWH) since early childhood compared with matched HIV-negative controls.
Methods: This is a prospective cross-sectional study of 35 adult PLWH who acquired HIV in early life and 20 matched HIV-negative controls. Quality of life, depressive symptoms, HIV transmission knowledge, sexual/ reproductive outcomes and behaviours were evaluated through self-report questionnaires.
Results: PLWH had a mean age of 29 years, 65% virally suppressed, with a mean CD4 T-cell count 527 cells/ul. PLWH scored significantly worse than controls on depressive symptoms (P=0.04) and two quality of life domains (physical domain P=0.03, level of independence P=0.0002). By contrast, PLWH scored significantly higher on questions assessing family planning transmission knowledge (P=0.002), with no differences between groups in general HIV transmission knowledge. PLWH were more likely to learn about sexual matters from health-care providers (P=0.002) and were more confident in the adequacy of their sexual/ reproductive health knowledge (P<0.05). Both groups reported inconsistent condom use (59% PLWH and 75% controls; P=0.23), but PLWH were more likely to have planned pregnancies (P=0.005) and to have discussed becoming pregnant with their partner (P<0.05) compared with controls.
Conclusions: Despite the challenges of living with a chronic and stigmatized condition, adult PLWH since childhood were knowledgeable about HIV transmission and family planning and demonstrated sexual practices and reproductive outcomes similar to age-matched controls. However, sub-optimal rates of viral suppression, inconsistent condom use and the psychosocial impact of living with HIV continue to require the attention of health-care providers for young adults with PHIV.
Abstract P42
Antiviral Therapy 2019; 24 Suppl 1:A98
Correlation between cerebrospinal fluid (CSF) and plasma concentrations of neurofilament light protein (NFL) in treated HIV infection in the COmorBidity in Relation to AIDS (COBRA) Study
J Alagaratnam1,2, D De Francesco3, H Zetterberg4,5,6,7, A Heslegrave8, J Toombs8, N Kootstra9, J Underwood1,10,11, M Gisslén12,13, P Reiss14,15,16, C Sabin3, A Winston1,2, the COmorBidity in Relation to AIDS (COBRA) collaboration
1Section of Virology, Department of Infectious Diseases, Faculty of Medicine, Imperial College London, London, UK; 2Department of Genitourinary Medicine & HIV, Imperial College Healthcare NHS Trust, London, UK; 3Institute for Global Health, University College London, London, UK; 4Department of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, the Sahlgrenska Academy at the University of Gothenburg, Mölndal, Sweden; 5Clinical Neurochemistry Laboratory, Sahlgrenska University Hospital, Mölndal, Sweden; 6Department of Neurodegenerative Disease, UCL Queen Square Institute of Neurology, Queen Square, London, UK; 7UK Dementia Research Institute at UCL, London, UK; 8UCL Dementia Research Institute and ION Dept of Neurodegenerative Disease; 9Department of Experimental Immunology, Amsterdam UMC, University of Amsterdam, Amsterdam, the Netherlands; 10Division of Infection and Immunity, Cardiff University, Cardiff, UK; 11 Department of Infectious Diseases, Cardiff and Vale University Health Board, Cardiff, UK; 12Department of Infectious Diseases, Institute of Biomedicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 13Region Västra Götaland, Sahlgrenska University Hospital, Department of Infectious Diseases, Gothenburg, Sweden; 14Dept of Global Health, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands; 15Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands; 16Stichting HIV Monitoring, Amsterdam, the Netherlands
Purpose: CSF NFL is an established biomarker of central nervous system neuro-axonal injury. A novel ultra-sensitive assay can determine plasma NFL. In untreated people with HIV (PWH), plasma and CSF NFL are strongly correlated. We assessed this correlation in antiretroviral therapy (ART)-treated PWH and lifestyle-similar HIV-negative controls, and determined factors associated with plasma and CSF NFL in PWH.
Methods: Differences in paired plasma (Simoa digital immunoassay, Quanterix™) and CSF (sandwich ELISA, UmanDiagnostics AB) NFL between PWH and HIV-negative controls were tested for significance using Wilcoxon's test; associations between the values (after log-transformation) were assessed using Pearson's correlation. Log-transformed plasma and CSF NFL, standardized to Z-scores, were included as dependent variables in linear regression models to identify factors independently associated with values in PWH; factors significant (P<0.05) in univariable analyses for either outcome were included in the multivariable models.
Results: We included 132 PWH (median age 56 years, 94% male, 88% White, 100% HIV-1 RNA <50 copies/ml) and 79 HIV-negative controls (57 years, 92% male, 97% White). Neither CSF (570 versus 568 pg/ml; P=0.37) nor plasma (10.7 versus 9.9 pg/ml; P=0.15) NFL differed significantly between the two groups. Plasma and CSF NFL correlated moderately, with no significant difference by HIV status (PWH: r=0.52 [95% CI 0.38,0.63]; HIV-negative: r=0.47 [0.27,0.62]; P [interaction]=0.63). In multivariable regression, older age and lower weight were each associated with higher plasma and CSF NFL Z-scores in PWH. Whereas lower plasma albumin and higher serum creatinine were associated with higher plasma NFL Z-scores, higher CSF protein was associated with higher CSF NFL Z-scores. See Table 1.
(Abstract P42)
Table: Results from multivariable linear regression to identify factors significantly associated with plasma and CSF NFL1,2 (PWH only, n=132)
Dependent variable
Independent variables
Parameter estimate (95% CI)
p-value
Log10 (plasma NFL)
Age (/10 years older)
0.60 (0.42, 0.79)
<0.001
Z-score
Weight (/5kg higher)
−0.13 (−0.18, −0.08)
<0.001
Serum creatinine (/10μmol/L higher)
0.12 (0.04, 0.19)
0.002
Plasma albumin (/10g/L higher)
−0.39 (−0.69, −0.09)
0.012
Lug10 (CSF NFL)
Age (/10 years older)
0.69 (0.50, 0.89)
<0.001
Z-score
Weight (/5kg higher)
−0.07 (−0.12, −0.01)
0.021
CSF proteto [/1g/L higher)
1.33 (0.50,2.16)
0.002
Parameter estimates reflect the associated impact (measured in standard deviations) of each independent variable in the model on the dependent variable.
Variables included in the multivariable linear regression models were age, weight, serum creatinine, plasma albumin, CSF protein, male gender, being on antihypertensive medication, duration diagnosed with HIV infection, duration on ART.
Conclusions: In PWH on suppressive ART, the correlation between CSF and plasma NFL is weaker than previously described in untreated PWH but similar to that observed in lifestyle-similar controls. Consideration of renal function and body composition may be required when utilizing plasma NFL.
Abstract P43
Antiviral Therapy 2019; 24 Suppl 1:A100
In vitro modelling of the impact of TAF on cellular bioenergetics in immune cells and hepatocytes
E Ritou1,T Kelesidis1
1David Geffen School of Medicine at University of California – Los Angeles
Objectives/aim: The mechanisms that drive differential effects of antivirals on HIV-related immune dysfunction and alterations in metabolism remain unclear. Markedly lower plasma levels of tenofovir (TFV) are thought to lead to the more favourable bone and renal safety profile of tenofovir alafenamide (TAF) compared with tenofovir disoproxil fumarate (TDF). However, it is unknown whether an increase in intracellular levels of the active metabolite, tenofovir-diphosphate (TFV-DP) with TAF (compared with TDF) may affect mitochondrial function and contribute to alterations in cellular metabolism. This study was designed to address whether TAF affects in vitro cellular bioenergetics in human peripheral blood mononuclear cells (PBMCs) and the HepG2 cell line.
Methods: Zalcitabine (ddC) has known mitochondrial toxicity and was used as positive control. PBMCs were isolated from healthy 18–40 years old participants. Standardized number of cells was used for all experiments (14,000 hepG2 cells/well and 100,000 PBMCs/well). 2-h incubation conditions with TDF and/or TAF at concentrations that have been shown to model cellular levels of TFV-DP similar to those observed in PBMCs in clinical studies with TDF and/or TAF were selected to model clinically relevant plasma exposure. The XF96 Extracellular Flux Analyzer was used to monitor cellular bioenergetics in PBMCs and HepG2 cells. A decrease in the ATP-linked respiration (ATP-OCR) and/or the maximum respiration rate (max-OCR) caused by addition of the FCCP uncoupler may suggest mitochondrial dysfunction. Results are described as median and interquartile range (IQR) and the Wilcoxon and Mann–Whitney tests were used for statistical comparison between groups.
Results: After 2 h of in vitro exposure of HepG2 cells to 0.12–3.3 μM TAF, TDF and ddC,3.3 μM ddC induced a mean >30% decrease in both ATP-OCR and max-OCR compared with DMSO vehicle control (P<0.001). 1.1 μM TAF induced a mean ∼18% increase in ATP-OCR (P<0.001) and a mean ∼15% increase in max-OCR (P<0.05) compared with vehicle control. 1.1 μM TAF also induced a mean ∼>9% increase in ATP-OCR (P<0.001) compared with 0.12 and 1.1 μM TDF. 2 h of in vitro exposure of primary PBMCs to 0.12–3.3 μM TAF, TDF and ddC did not impact OCR (data not shown).
Conclusions/discussion: In the setting of delivering higher intracellular levels of TFV-DP than TDF, TAF may alter cellular bioenergetics at in vitro incubation conditions that model clinically relevant plasma exposure in hepatocytes as early as 2 h. We did not find any evidence of in vitro mitochondrial toxicity (reduction in OCR) with TAF. TAF could cause a differential metabolic reprogramming on substrate dependency in hepatocytes compared with immune cells. The clinical relevance of these in vitro findings is unknown. The effect of TAF on cellular bioenergetics in chronic treated HIV should be further explored in patients switching from TDF to TAF regimens.
Abstract P44
Antiviral Therapy 2019; 24 Suppl 1:A101
Targeting inflammation in chronic treated HIV with oral ApoA-I mimetics
W Mu1,R Heymans1,E Ritou1,P Hamid1,A Kossyvakis1,S Sen Roy1,V Grijalva1,A Chattopadhyay1,A Fogelman1,S Reddy1,T Kelesidis1
1David Geffen School of Medicine at University of California – Los Angeles
Objectives/aim: Novel therapeutic approaches are needed to attenuate inflammation that may contribute to morbidity in chronic treated HIV infection. ApoA-I peptides (such as 6F) mimic HDL, bind oxidized lipids and endotoxin and attenuate proinflammatory mechanisms. The 6F was expressed as a transgene in tomatoes (Tg6F) and reduced cardiovascular disease in mice. Tg6F can be translated to human diet. Given that preclinical data are needed to assist efforts to bring Tg6F in the clinic, we used a physiologically relevant humanized mouse model of chronic treated HIV to study whether oral apoA-I mimetics attenuate in vivo HIV- and/or ART-driven impact on inflammation.
Methods: The C57BL/6 Rag2-/-γc-/-CD47-/- bone marrow/liver/thymus mice do not develop early graft versus host disease and thus HIV- and/or ART-driven changes on inflammation can be dissected in vivo. After 4 weeks of infection with the dual-tropic 89.6 HIV-1 virus, mice (n=40) were treated with daily emtricitabine (200 mg/kg),tenofovir (208 mg/kg),raltegravir (80 mg/kg) for up to 12 weeks. Oral ApoA-I mimetics were given as Tg6F (at 0.06% by weight of diet) to HIV+/ART-treated mice (n=20) after suppression of viraemia with ART. The groups were: A (n=10): uninfected (HIV-); B (n=10): HIV+; C (n=20): HIV+,ART; D (n=20): HIV+/ART/Tg6F. Human cytokines and chemokines were determined by Luminex Assays. Results are described as median and interquartile range (Tukey's) and Mann–Whitney test was used for statistical analysis.
Results: HIV-1 induced a mean >30% reduction in plasma h-IL-1b, h-IL-6,h-IL-8,h-IL-10,h-IL-18 and h-TNF-a and a mean >25% increase in plasma h-CCL3, h-CCL5,h-CX3CL1,h-CXCL10 and VEGF in infected compared with uninfected mice (P<0.05; Figure 1). Potent ART for 12 weeks suppressed viraemia within 4 weeks and induced a mean >15% increase in human cytokines compared with HIV viraemic mice. ART induced a mean >30% increase in h-CCL2,hCXCL1,murine IL-1b and TNF-a in HIV+/ART+ compared with HIV+ and uninfected mice (P<0.05). All other murine cytokines and chemokines did not change with HIV and/or ART (data not shown). Tg6F attenuated all ART-induced increases in m-TNF-a, m-IL-1b and human cytokines and chemokines except for h-IL-6 and h-CXCL10.
(Abstract P44)
Conclusions/discussion: Our data provide unique insight about differential effects of HIV-1 versus potent ART on human cytokines and chemokines. HIV-1 reduced human cytokines (possibly through cytotoxic effects),whereas potent ART did not change or even increased cytokines and chemokines. Tg6F attenuated ART-induced increase in inflammation. Given that Tg6F binds endotoxin and bioactive lipids in the gut and is not absorbed systemically, our model confirms that gut dysfunction is a major instigator of inflammation in chronic treated HIV. Further studies are needed to determine whether oral ApoA-I mimetics can be a novel strategy to attenuate inflammation in chronic treated HIV.
Abstract P45
Antiviral Therapy 2019; 24 Suppl 1:A103
Differential impact of HIV, antivirals and oral ApoA-I mimetics on mitochondrial function in chronic treated HIV
H Vasilopoulos1,R Heymans1,W Mu1,P Hamid1,A Kossyvakis1,S Sen Roy1,V Grijalva1,A Chattopadhyay1,A Fogelman1,S Reddy1,T Kelesidis1
1David Geffen School of Medicine at University of California – Los Angeles
Objectives/aim: The mechanisms that drive comorbidities in chronic treated HIV remain unclear. Mitochondria are responsible for creating the energy needed for function of organs. Mitochondrial dysfunction likely plays a role in ageing in chronic treated HIV. HDL-associated apoA-I may attenuate mitochondrial dysfunction. Given that observational human studies cannot dissect the differential effects of HIV versus antivirals (ART) on mitochondria, we used a physiologically relevant humanized mouse model of chronic treated HIV to study whether oral apoA-I mimetics attenuate in vivo HIV-1 and/or ART-driven mitochondrial dysfunction.
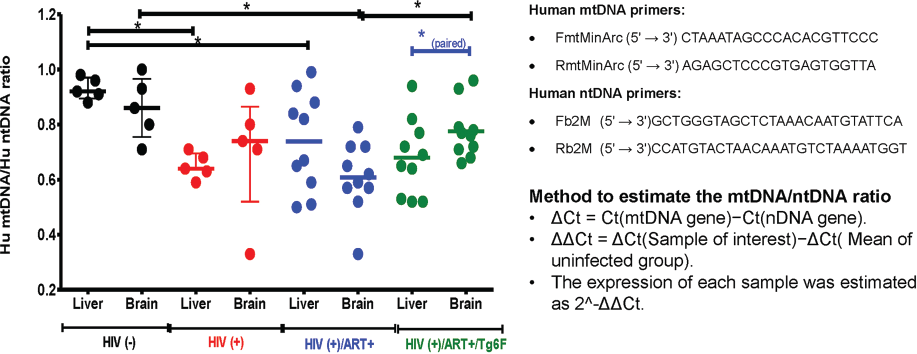
Methods: The C57BL/6 Rag2-/-γc-/-CD47-/- bone marrow/liver/thymus mice do not develop early graft versus host disease and thus HIV- and/or ART-driven changes on tissues can be dissected in vivo. After 4 weeks of infection with the dual-tropic 89.6 HIV-1 virus, mice (n=20) were treated with daily emtricitabine (200 mg/kg),tenofovir (208 mg/kg),raltegravir (80 mg/kg) for up to 12 weeks. Oral ApoA-I mimetics were given to HIV+/ART-treated mice (n=10) as a concentrate of transgenic tomatoes expressing the 6F peptide (Tg6F) at 0.06% by weight of diet. The groups were: A (n=5): uninfected (HIV-); B (n=5): HIV+; C (n=10): HIV+,ART; D (n=10): HIV+/ART/Tg6F. Reduction in mitochondrial DNA (mtDNA) levels compromises cellular function and was used as a biomarker of mitochondrial dysfunction. mtDNA copy number and the mtDNA/ntDNA ratio were determined by realtime PCR (Figure 1). Results are described as median and interquartile range and non-parametric (un)paired tests were used for statistical analysis.
(Abstract P45)
Results: HIV-1 induced a mean 28% reduction in human mtDNA/ntDNA ratio in the liver of infected compared with uninfected mice (P<0.05) but did not affect the human and murine mtDNA/ntDNA ratio in the brain (data not shown). Potent ART for 12 weeks suppressed viraemia within 4 weeks and induced a mean >20% reduction in human and mouse (not shown) mtDNA/ntDNA ratio in the liver and human mtDNA/ntDNA ratio in the brain of infected compared with uninfected mice (P<0.05). Tg6F attenuated ART-induced reduction in human mtDNA/ntDNA ratio in the brain (P<0.05) but not in the liver.
Conclusions/discussion: HIV-1 and/or potent ART had a differential direct impact on mitochondria at the tissue level (brain, liver) in vivo. Potent ART consistently induced mitochondrial dysfunction in both the liver and the brain and may be a more important (than HIV-1) instigator of mitochondrial dysfunction in chronic treated HIV. Tg6F attenuated ART-induced mitochondrial dysfunction in the brain but not in the liver. Given that Tg6F binds endotoxin and bioactive lipids in the gut and is not absorbed systemically, our model suggests that gut dysfunction may drive human neuroinflammation and mitochondrial dysfunction in chronic treated HIV. Further studies are needed to determine whether oral ApoA-I mimetics can be a novel strategy to attenuate mitochondrial dysfunction and comorbidities in chronic treated HIV.
Abstract P46
Antiviral Therapy 2019; 24 Suppl 1:A105
Subtherapeutic efavirenz concentrations positively correlate with cytomegalovirus coinfection in HIV-1-infected pregnant women
D Mhandire1,2,G Morse3,C Maponga4,K Mhandire1,5,C Dandara1,2
1Division of Human Genetics, Department of Pathology, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa; 2Institute of Infectious Disease and Molecular Medicine, University of Cape Town, Cape Town, South Africa; 3Translational Pharmacology Research Core, New York State Center of Excellence in Bioinformatics and Life Sciences, Buffalo, NY; 4University of Zimbabwe, School of Pharmacy, Harare, Zimbabwe; 5Department of Chemical Pathology, College of Health Sciences, University of Zimbabwe, Harare, Zimbabwe
Aim: Effective combination antiretroviral therapy (cART) has tremendously reduced HIV-associated morbidity, mortality and mother to child transmission (MTCT). However, the benefits of cART are threatened by comorbidities, adverse drug reactions (ADRs) and virus resistance to existing regimens. One of the most occurring comorbidities is cytomegalovirus (CMV). This project aimed to investigate the role of HIV treatment (measured by plasma efavirenz concentration and viral load) in the occurrence of CMV infection among pregnant women.
Methods: A cross-sectional study collected demographic and clinical data from 175 HIV-1-infected pregnant women. CMV DNA was measured using real-time PCR. Plasma efavirenz concentrations were determined using HPLC. In addition,CYP2B6 c.516G>T and CYP2B6 c.983T>C single nucleotide polymorphisms, which are genomic markers for plasma efavirenz levels, were characterized using PCR/RFLP and TaqMan assays, respectively.
Results: Participants positive for CMV DNA (median: 847 ng/ml,25th–75th percentile: 250–3,307) were significantly (P<0.001) more likely to experience sub-therapeutic plasma efavirenz concentrations than participants negative for CMV DNA (median: 2,024 ng/ml,25th–75th percentile: 250–14,039). The median plasma efavirenz concentrations for CYP2B6 c.516T/T genotype were significantly higher than for 516G/G (P<0.001) and 516G/T (P<0.01) genotypes carriers. Median plasma efavirenz concentrations were also significantly higher (P<0.001) in CYP2B6 c.983T/C than CYP2B6 c.983T/T genotype carriers.
Discussion and conclusions: HIV and its treatment disrupt the balance between host and co-infecting microbes. Sub-therapeutic levels of antiretroviral drugs, which could be exacerbated by genetic polymorphisms in drug metabolism genes predisposes infected individuals to increased risk of CMV infection in pregnancy.
Abstract P47
Antiviral Therapy 2019; 24 Suppl 1:A106
Prevalence and risk factors of proximal tubular dysfunction and its correlation with glomerular function among children with HIV seen in Lagos University Teaching Hospital, Nigeria
J Akagu1,C Esezobor2,A Akinsulie3
1Department of Paediatrics Lagos University Teaching Hospital, Lagos, Nigeria; 2Department of Paediatrics, College of Medicine, University of Lagos, Lagos University Teaching Hospital, Lagos, Nigeria; 3Department of Paediatrics, College of Medicine, University of Lagos, Lagos University Teaching Hospital, Lagos, Nigeria
Objectives: Renal tubular abnormalities occur in children with HIV but little is known about its prevalence and risk factors in children in Africa. The few studies in children that reported proximal tubular dysfunction (PRTD) used hypophosphataemia and hypercalciuria, which are not specific to proximal tubular dysfunction. In addition, studies in adults with PRTD were done in persons, the majority of whom were receiving tenofovir, an established cause of PRTD. However, involvement of the renal tubules in HIV may be directly related to the virus and the host immunological response to the virus. Therefore, we determined the prevalence and factors associated with PRTD in children with HIV.
Methods: We included 155 children living with HIV and no recent febrile illness or known history of sickle cell disease, diabetes or cardiac disease. We determined the presence of PRTD by measuring β2 microglobulin:creatinine ratio (β2M:Cr) in freshly voided urine sample. We classified the severity of HIV infection using the WHO clinical and immunological staging criteria. For comparison, we included one age and sex-matched control for every child with HIV. Proximal renal tubular dysfunction was defined as urinary β2M:Cr>300 μg/g.
Results: The mean age of the children with HIV was 11.1 ±3.6 years and 52.7% were females. The prevalence of PRTD was 23.9% among the children with HIV and 11.6% among the controls (P=0.005). Children with HIV and PRTD were younger than those without PRTD (8.9 ±3.8 versus 11.8 ±3.3 years; P<0.001). Children with stage IV HIV disease had 64.3% prevalence of PRTD which was about three times higher than the rates in children with milder forms of HIV disease (P=0.003). Also, children with severe immunosuppression had prevalence of PRTD that was at least two times higher than in children with no or mild immunosuppression (P=0.038). In addition, children with detectable HIV viral load on polymerase chain reaction had two times the prevalence of PRTD of those without PRTD (29.6% versus 14.0%; P=0.025). Children receiving tenofovir-based HAART regimen had similar prevalence of PRTD to those on other regimens (25% versus 23.8%; P=0.606). In multiple regression analysis, the risk of developing PRTD was five times for children in stage IV (4.83 [1.01–23.08]) compared with those in stage I and 10 times (10.00 [1.58–63.45]) for those with severe immunosuppression compared with those with no immunosuppression.
Conclusions: PRT dysfunction occurs in one out of every four children with HIV irrespective of exposure to tenofovir. Children with WHO stage IV clinical and severe immunological stages of HIV were 5 and 10 times more likely to develop PRTD, respectively, than those with milder stages of HIV.
Abstract P48
Antiviral Therapy 2019; 24 Suppl 1:A107
Targeting immune activation in chronic treated HIV with oral ApoA-I mimetics
W Mu1, R Heymans1, E Ritou1, P Hamid1, A Kossyvakis1, S Sen Roy1, V Grijalva1, A Chattopadhyay1, A Fogelman1, S Reddy1, T Kelesidis1
1David Geffen School of Medicine at University of California – Los Angeles
Objectives/aim: Monocyte/macrophage (M/M)-related (rather than T-cell) inflammation and immune activation may contribute to morbidity and mortality in chronic treated HIV-1 infection. Novel therapeutic approaches are needed to attenuate M/M activation in chronic treated HIV infection. ApoA-I peptides (such as 6F) mimic HDL, bind oxidized lipids and endotoxin and attenuate proinflammatory mechanisms. The 6F was expressed as a transgene in tomatoes (Tg6F) and reduced cardiovascular disease in mice. Tg6F can be translated to human diet. Given that preclinical data are needed to assist efforts to bring Tg6F in the clinic, we used a physiologically relevant humanized mouse model of chronic treated HIV to study whether oral apoA-I mimetics attenuate in vivo HIV- and/or ART-driven alterations in human biomarkers of M/M activation (sCD163, sCD14) that predict morbidity and mortality in chronic treated HIV.
Methods: The C57BL/6 Rag2-/-γc-/-CD47-/- bone marrow/liver/thymus mice do not develop early graft versus host disease and thus HIV- and/or ART-driven changes on M/M activation can be dissected in vivo. After 4 weeks of infection with the dual-tropic 89.6 HIV-1 virus, mice were treated with daily emtricitabine (200 mg/kg), tenofovir (208 mg/kg), raltegravir (80 mg/kg) for up to 12 weeks. Oral ApoA-I mimetics were given as Tg6F (at 0.06% by weight of diet) to HIV+/ART-treated mice (n=20) after suppression of viraemia with ART. The groups were: A (n=10): uninfected (HIV-); B (n=10): HIV+; C (n=20): HIV+, ART; D (n=20): HIV+/ART/Tg6F. Plasma levels of human sCD14 and sCD163 were determined by Luminex Assays. Results are described as median and interquartile range (Tukey's) and Mann–Whitney test was used for statistical analysis.
Results: HIV-1 induced a mean 59% and 56% reduction in plasma h-sCD14 and h-sCD163, respectively, in infected compared to uninfected mice (P<0.05). Potent ART for 12 weeks suppressed viraemia within 4 weeks and induced a mean 49% and 38% increase in h-sCD14 and h-sCD163 (P<0.05) in HIV+/ART+ compared with HIV+ mice (P<0.05). Tg6F attenuated ART-induced increases in h-sCD14 and h-sCD163 (P<0.001). See Figure 1.
(Abstract P48)
Conclusions/discussion: Our data provide unique insight about differential effects of HIV-1 versus potent ART on human M/M activation. HIV-1 reduced h-sCD14 and h-sCD163 (possibly through cytotoxic effects), whereas potent ART increased h-sCD14 and h-sCD163. Our mechanistic data complement prior observational human studies that M/M activation persists in chronic treated HIV despite potent ART. ART rather than HIV-1 per se may contribute to elevated M/M activation in chronic treated HIV. Tg6F attenuated ART-induced increase in M/M activation. Given that Tg6F binds endotoxin and bioactive lipids in the gut and is not absorbed systemically, our model con-firms that gut dysfunction is a major instigator of M/M activation in chronic treated HIV. Further studies are needed to determine whether oral ApoA-I mimetics can be a novel strategy to attenuate M/M activation in chronic treated HIV.
Abstract P49
Antiviral Therapy 2019; 24 Suppl 1:A108
Age- and sex-related differences in concomitant diseases and use of co-medication in patients with treated HIV infection in Germany
B Funke1, CD Spinner2, S Esser3, H-J Stellbrink4, A Stoehr5, E Wolf6, K Martin1, V Witte1
1MSD Sharp & Dohme GmbH, Medical Affairs, Haar, Germany; 2Technical University of Munich, School of Medicine, University Hospital rechts der Isar, Department of Medicine II, Munich, Germany; 3University Hospital Essen, University of Duisburg-Essen, Clinic for Dermatology, Essen, Germany; 4Infectiology Center Hamburg (ICH), Hamburg, Germany; 5if Institute for Interdisciplinary Medicine, Hamburg, Germany; 6MVZ Karlsplatz, Munich, Germany
Background: Demographic ageing of HIV-infected populations poses new challenges to physicians. Advancing age is associated with (multiple) chronic diseases and need for co-medication.
Methods: BESIDE was a cross-sectional study evaluating the prevalence of concomitant diseases and prescription and over the counter co-medication in people living with HIV (PLWH) on antiretroviral therapy from 2016–2017. Regional distribution of study sites (n=20), consecutive recruitment and age-stratified sampling ensured a representative sample of the PLWH population in Germany.
Results:n=453 PLWH were enrolled: female 22%, median age 46 years (y), median time living with HIV 9 y, CDC C 15%, median CD4 count 650 cells/μl. Among the top three comorbidities per age group, vitamin D deficiency (29% overall) and depressive episodes (28% overall) were consistently reported across age groups. The third most common comorbidity differed: in younger PLWH, acute respiratory infections (<30 y, 11%) and gastro-oesophageal reflux disease (30–39 y, 8%) were most prevalent, while for older PLWH, hypertension was increasingly reported (40–49 y, 12%; >60 y, 41%).
Women more often (f/m, difference Δ>5%) suffered from nutritional anaemias (11%/4%), other nutritional deficiencies (39%/28%), bone density/structure disorders (9%/1%) and thyroid gland disorders (10%/4%). Conversely, metabolic disorders (10%/21%), sexually transmissible infections (2%/9%), polyneuropathies/ peripheral nervous system disorders (1%/7%) and dorsopathies (2%/8%) were more common in men.
Most common drugs used across all ages were vitamin supplements (32% overall). Anti-inflammatory/anti-rheumatic agents (16%) also belonged to the top three drugs in all age groups, except >60 y where antithrombotic agents were more frequent (30%). In addition, younger patients received vaccines (<30 y, 9%) and used psychoactive drugs (30–39 y, 10%; 40–49 y, 12%), whereas in older patients renin-angiotensin system agents (50–59 y, 21%; >60 y, 30%) ranked higher. Women more commonly used (f/m, Δ >5%) antianaemia preparations (14%/6%), vitamins (38%/30%) and mineral supplements (10%/5%); men more commonly used antithrombotic agents (4%/11%), renin-angiotensin system agents (7%/14%) and lipid modifiers (6%/12%).
Conclusions: Although prevalence of concomitant diseases and use of co-medication among PLWH in Germany are high across gender and all ages, the disease and drug patterns change in an age- and sex-related manner.
Abstract P50
Antiviral Therapy 2019; 24 Suppl 1:A109
Comparable effectiveness of raltegravir-based dual therapy versus other regimens in patients switched for maintenance
K Martin1, B Funke1, T Wuensche2, T Lutz3, H Jaeger4, V Witte1
1MSD Sharp & Dohme GmbH, Medical Affairs, Haar, Germany; 2Praxis Wuensche, Berlin, Germany; 3Infektiologikum Frankfurt, Frankfurt am Main, Germany; 4MVZ Karlsplatz, HIV Research and Clinical Care Centre, Munich, Germany
Background: In clinical practice raltegravir is used in nuke-free dual therapy. Here, we compared profiles and 48-week treatment outcomes of patients on RAL-based dual versus other RAL-based ART in a historical German real-life cohort.
Methods: The WIP study was a real-life, prospective, observational cohort study with data collection from 2010–2014. Safety and efficacy outcomes of RAL-based ART in a population enriched for ageing patients (274, 61% ≥50 years) were documented. Detailed methods are described elsewhere.
Results: The cohort included 77 (17%) patients on dual and 372 patients on other ART. 85% were male, no differences by treatment group. Compared with patients on other ART, patients initiated on RAL-based dual therapy were on average 3.9 years older and suffered more likely from hypertension (26% versus 18%), coronary artery disease (12% versus 4%) and renal insufficiencies (10% versus 4%) at baseline. They were less frequently therapy-naive (17% versus. 22%) or pretreated with suppressed viral load (VL; 45% versus 51%) but more often failing (35% versus 22%). Dual therapies mainly included a PI (94%, 72/77); most other regimen combinations included NRTI (77%, 287/374). Treatment outcomes of dual versus other ART differed slightly: 48-week virological response (VL<50 c/ml; early DC [discontinuation]=failure) was numerically lower in therapy-naive patients (69% versus 76%). However, in virologically suppressed patients switched for maintenance efficacy of RAL-based dual therapy was high and comparable to other RAL-based regimens (83% versus 81%; Table 1).
Conclusions: Patients on RAL-based dual versus other ART showed differing comorbidity profiles and RAL utilization patterns. While outcomes in therapy-naive and pretreated failing patients were less favorable, response rates in virologically suppressed patients were high and comparable supporting the concept of maintenance switch to RAL-based dual therapy to avoid drug toxicities or intolerances.
Abstract P51
Antiviral Therapy 2019; 24 Suppl 1:A110
Gender-specific analysis of a German cohort of HIV-infected patients on raltegravir-based therapy shows distinctive baseline comorbidity profiles of women versus men but no impact on treatment outcomes
K Martin1, B Funke1, U Naumann2, K Ummard-Berger2, V Witte1
Background: HIV-infected women are facing specific needs in the context of antiretroviral therapy. For a better understanding, we performed a gender-specific post hoc analysis for patients on raltegravir (RAL)-based therapies in the German real-life cohort WIP.
Methods: The WIP study was a prospective, observational, multicentre cohort study in routine clinical care with data collection between 2010 and 2014. Safety and efficacy outcomes of RAL-based antiretroviral therapy in a population enriched for ageing patients (274, 61% ≥50 years) were documented. Detailed methods are described elsewhere.
Results: The cohort included 69 (15%) female and 382 (85%) male HIV-infected patients. Mean age was 51 years in both groups. At RAL initiation women and men were 13% versus 23% therapy-naive, 49% versus 51% pretreated with virological suppression and 33% versus 23% without virological suppression. At baseline, female patients suffered more frequently from depression (23% versus 16%) as well as chronic HCV infection (20% versus 9%) and male patients more often from cardiovascular diseases including hypertension (15% versus 20%) as well as lipid abnormalities such as hypercholesterolaemia (6% versus 11%) and hypertriglyceridaemia (1% versus 6%). Concomitant medications at baseline were consistent with these comorbidity profiles. No gender-specific differences in RAL-based therapy were observed in women versus men: RAL was combined with PI in 17% versus 16%, with NRTI in 64% versus 64% and with others in 19% versus 20%. Regarding treatment outcomes, virological response rates were comparable between women and men (Table 1).
Conclusions: In this German real-life cohort, characterization of female versus male patients demonstrated divergent comorbidity profiles and minor differences in utilization patterns of RAL-based therapy. Nevertheless, in both women and men similar and high response rates comparable to clinical trial results could be observed.