Atherosclerotic cardiovascular events in people living with human immunodeficiency virus
F Boccara1,2, S Lang1, S Ederhy1, L Soulat-Dufour1, S Adavane-Scheuble1, Y Ancedy1, M Chauvet1, P Nhan1, JL Meynard3, MA Valentin4, L Slama5, G Pialoux6, C Katlama4, PM Girard3, A Cohen1
1AP-HP, Hôpitaux de l'Est Parisien, Hôpital Saint-Antoine, Department of Cardiology, Faculty of Medicine, Sorbonne Université, Paris, France; 2National Institute of Health and Medical Research, INSERM, UMR_S 938, UPMC, Paris, France; 3AP-HP, Hôpital Saint-Antoine, Infectious Disease Department, Paris, France; 4AP-HP, Hôpital Pitié-Salpêtrière, Infectious Disease Department, Paris, France; 5AP-HP, Hôpital Hotel Dieu, Infectious Disease Department, Paris, France; 6AP-HP, Hôpital Tenon, Infectious Disease Department, Paris, France
Background: People living with human immunodeficiency virus (PLWHIV) under antiretrovirals (ARV) have an increased risk of atherosclerotic cardiovascular disease (ASCVD) events. The factors associated with ASCVD events in this high-risk population are various, mixing traditional vascular risk factors and specific HIV-related factors and remain controversial.
Purpose: Our aim was to determine the incidence of ASCVD events in a large cohort of PLWHIV and to identify the risk factors associated.
Methods: We conducted a longitudinal observational cohort study of asymptomatic PLWHIV addressed to our preventive cardiovascular unit for non-invasive cardiovascular evaluation. The first ASCVD event was censored and included CV death, acute coronary syndromes, coronary and peripheral revascularizations (PCI or CABG or endarterectomy or limb procedures) and ischaemic strokes.
Results: From January 2003 to December 2014, 763 consecutive asymptomatic PLWHIV were enrolled (mean age of 51.3 ±8.3 years, 87% men, 90% were free of known coronary artery disease, mean left ventricular ejection fraction 60%). At baseline, traditional CV risk factors were as follows: 54% had dyslipidaemia, 43% hypertension, 35% were active smokers, 22% had family history of CAD and 11% were diabetics. Statins were prescribed in 38% of the cohort, aspirin in 14%, clopidogrel in 14%, betablockers in 14%, RAS blockers in 32%, calcium channel blockers in 8%. At baseline, median duration of HIV seropositivity was 19.8 years (14.0–23.6), 94% were under ARV predominantly protease inhibitors (68%). Median CD4 cell count was 545/mm3 (404–745) and 92% had undetectable HIV viral load. During a median follow-up of 5.8 years (3.7–8.7), 58 (7.3%) subjects had a first ASCVD event (incidence of 12.70 [9.78–16.51] per 1,000 persons-years) including 5 cardiovascular deaths, 14 ACS, 20 coronary revascularizations, 13 peripheral vascular procedures and 6 strokes) with a median time of occurrence of 3.1 years (1.5–5.1). CV death was the second cause of death (after malignancies: 12 patients, 33% causes of death) and occurred in 8 patients (25% of causes of death) followed by unexplained causes (21%), infectious disease (13%), liver disease (8%) and 2 suicides. Coronary events including coronary death, MI and stroke occurred in 39 patients (5.2%; incidence of 8.28 [6.00–11.43] per 1,000 persons-years). Conventional multivariate Cox model shows that age and tobacco were the independent risk factors associated with ASCVD events (hazard ratio [HR] 1.04, 95% CI 0.99, 1.09, P=0.05 and HR 2.17, 95% CI 1.07, 4.38, P=0.03).
Conclusions: Traditional vascular risk factors (age and active smoking) are associated with the occurrence of ASCVD events predominantly coronary artery disease in our observational cohort of PLWHIV. Cardiovascular prevention including tobacco cease action is mandatory in the ageing HIV population.
Abstract P20
Antiviral Therapy 2019; 24 Suppl 1:A64
Prognostic value of non-invasive ischaemic testing in people living with human immunodeficiency virus
F Boccara1,2, S Lang1, S Ederhy1, L Soulat-Dufour1, S Adavane-Scheuble1, Y Ancedy1, M Chauvet1, P Nhan1, JL Meynard3, MA Valentin4, L Slama5, G Pialoux6, C Katlama4, PM Girard3, A Cohen1
1AP-HP, Hôpitaux de l'Est Parisien, Hôpital Saint-Antoine, Department of Cardiology, Faculty of Medicine, Sorbonne Université, Paris, France; 2National Institute of Health and Medical Research, INSERM, UMR_S 938, UPMC, Paris, France; 3AP-HP, Hôpital Saint-Antoine, Infectious Disease Department, Paris, France; 4AP-HP, Hôpital Pitié-Salpêtrière, Infectious Disease Department, Paris, France; 5AP-HP, Hôpital Hotel Dieu, Infectious Disease Department, Paris, France; 6AP-HP, Hôpital Tenon, Infectious Disease Department, Paris, France
Introduction: People living with human immunodeficiency virus (PLWHIV) under antiretrovirals have an increased risk of atherosclerotic cardiovascular (ASCVD) events. The prognostic value of silent myocardial ischaemia in this high-risk population has been poorly studied.
Hypothesis: To assess the relevance of targeted screening for myocardial ischaemia in asymptomatic PLWHIV with multiple risk factors at high risk for ASCVD and the prognostic value of myocardial ischaemia testing in this specific population.
Methods: Longitudinal observational cohort of asymptomatic PLWHIV addressed to our preventive cardiovascular unit for cardiovascular risk stratification. The first ASCVD event was censored and included CV death, acute coronary syndromes, coronary and peripheral revascularizations (PCI or CABG or endarterectomy or limb procedures) and ischaemic strokes. Major coronary events included coronary death, ACS and coronary revascularization.
Results: From January 2003 to December 2014, 763 consecutive asymptomatic PLWHIV were enrolled (mean age of 51.3 ±8.3 years, 87% men, mean left ventricular ejection fraction 60%). At baseline, 90% were free of known coronary artery disease, 54% had dyslipidaemia, 43% hypertension, 35% were active smokers, 22% had family history of CAD and 11% were diabetics. 750 had a non-invasive diagnostic ischaemic testing including 243 exercise treadmill tests, 292 exercise echocardiography exams, 165 dobutamine stress echocardiography exams and 21 nuclear imaging tests. 41 (5%) subjects had a positive test (electrocardiographic and/or echocardiographic or scintigraphic imaging). During a median follow up of 5.8 years (3.7–8.7), 58 subjects (7.7%) had an ASCVD event (incidence of 12.70 [9.78–16.51] per 1,000 persons-years) including 5 cardiovascular deaths, 14 ACS, 20 coronary revascularizations, 13 peripheral vascular procedures and 6 strokes. Major coronary events occurred in 39 patients (5.2%) corresponding to an incidence of 8.28 [6.00–11.43] per 1,000 persons-years. Kaplan–Meier survival curve for ASCVD events stratified according to the result of non-invasive ischaemic test is depicted in Figure 1. Negative predictive value of ischaemic tests for the occurrence of ASCVD events was 96% (95% confidence interval, 94.2, 97.3%), and similar for the occurrence of major coronary events 95.9% (95% confidence interval, 94.2, 97.3%).
Kaplan–Meier survival estimates (Abstract P20)
Conclusions: Rate of silent myocardial ischaemia was low in this high-risk HIV population. Non-invasive ischaemic testing can effectively and safely risk stratifies PLWHIV at high risk of CVD. PLWHIV with a negative ischaemic test have an excellent long-term prognosis.
Abstract P21
Antiviral Therapy 2019; 24 Suppl 1:A66
Hypertension prevalence, awareness and barriers to control among persons living with HIV in northern Tanzania: a mixed methods study
P Manavalan1, D Madut1, N Thielman1, NL Okeke1, B Mmbaga2, MH Watt3
1Duke University, Durham, NC, USA; 2Kilimanjaro Christian Medical Center, Moshi, Tanzania; 3Duke Global Health Institute, Durham, NC, USA
Objectives: People living with HIV (PLWH) have elevated risk for cardiovascular disease, necessitating focus on hypertension as a modifiable risk factor. We determined hypertension prevalence in a sample of adults engaged in HIV care in Tanzania and identified barriers to improved care.
Methods: From October to December 2018, 555 HIV-infected adults were screened consecutively at one clinic in Moshi, Tanzania. Hypertension was defined as: a single blood pressure measurement ≥160 mmHg systolic or ≥100 mmHg diastolic, two measurements at separate visits ≥140 mmHg systolic or ≥90 mmHg diastolic, self-reported hypertension diagnosis or current antihypertensive use. Participants who met criteria for hypertension completed a hypertension knowledge, attitudes and practices (KAP) survey. Separately, in-depth interviews (IDIs) were conducted with 13 participants purposively selected from two HIV clinics in Moshi, Tanzania who reported a history of high blood pressure. Interviews were coded and analyzed using NVivo.
Results: Hypertension prevalence was 18.9% (19.7% among women and 16.0% among men). The mean age of hypertensive patients was 50.4 (sd=10.9) years, compared with 42.2 (sd=10.5) years for normotensive patients. Among the 105 patients with hypertension, 72 (69%) were unaware of their diagnosis, 53 (50%) reported no prior blood pressure measurements and 22 (21%) reported current or prior use of antihypertensives. Of the seven patients reporting current antihypertensive use, none had a controlled blood pressure. Ninety-one hypertensive participants completed the KAP survey; 58 (64%) reported never receiving information about high blood pressure from a health-care provider, while almost all (96%) agreed to a statement that they needed more information about high blood pressure. When asked to define hypertension, only three participants provided a correct response. The majority of participants (n=86, 95%) reported stress and worries were the most common cause of high blood pressure. IDI participants also demonstrated limited hypertension knowledge. IDI participants included 11 women and 2 men with a mean age of 52.5 (sd=14.7) years, and the majority (92%) with a primary school level of education or less. Participants perceived hypertension as being caused by thinking too much, as temporary but curable, but as often fatal. All participants reported non-compliance or disengagement from hypertension care and reported receiving minimal hypertension education and counselling. For patients who received hypertension care, the HIV clinic often served as the gateway into care.
Conclusions: This study confirms a high prevalence of hypertension among PLWH in Tanzania. Absence of routine screening may result in missed diagnoses, and a lack of hypertension education and counselling may impede blood pressure control. Interventions to improve screening, treatment and control and that are integrated into existing HIV care are urgently needed.
Abstract P22
Antiviral Therapy 2019; 24 Suppl 1:A67
Hypertension control in HIV-infected individuals at Princess Marina Hospital Infectious Disease Care Clinic
T Palai1, M Mosepele1, J Mwita1
1Department of Internal Medicine, Princess Marina Hospital, University of Botswana, Gaborone, Botswana
Background: People living with HIV infection (PLWHI) are 1.5 to 2 times more likely to experience cardiovascular diseases (CVD). The extent to which treated PLWHI with a co-existent diagnosis of hypertension are adequately treated for their elevated blood pressure is not well known. The current study aimed at assessing the association between hypertension control and viral load suppression among PLWHI in Gaborone, Botswana.
Methods: This cross-sectional study was undertaken at a large Infectious Disease Care Clinic with a patient population of about 6,500 in Gaborone, Botswana. PLWHI with a known diagnosis of hypertension who were prescribed antihypertensive medications were recruited into the study. Sociodemographic, hypertension and HIV treatment data were collected. Participants had to have a viral load and blood pressure measurement in their medical record within 6 months at the time of recruitment. Viral load suppression was defined as a viral load <400 copies/ml, while hypertension control was defined as blood pressure <140/90 mmHg. Among all virally suppressed participants (main exposure), we assessed the association of viral suppression with the outcome of controlled blood pressure in univariate and multivariate logistic regression models.
Results: Among 329 participants enrolled, the mean age was 51.9 ±8.8 years and n=67.9% were female. The proportion of participants with controlled hypertension was 47.3%, and those with virological suppression was 95.4%. Hypertension control was not associated with virological suppression (P=0.8). In the final multivariate analysis, both female gender and increasing age were associated with hypertension control OR 2.3 (95% CI: 1.4, 3.9) and OR 1.0 (95% CI: 1.0, 1.1), respectively. However, being prescribed calcium channel blockers OR 0.4 (95% CI: 0.3, 0.7), beta-blocker OR 0.5 (95% CI: 0.2, 0.9), angiotensin receptor blocker OR 0.2 (95% CI: 0.0, 0.9) and living with chronic kidney disease OR 0.2 (95% CI; 0.0, 0.9) were inversely associated with hypertension control.
Conclusions: Almost half of PLWHI in this one clinic-based study in Botswana had suboptimal hypertension control despite having achieved viral suppression. Future studies should explore factors associated with the inability to attain blood pressure targets despite attempts to treat hypertension among PLWHI in this setting.
Abstract P23
Antiviral Therapy 2019; 24 Suppl 1:A68
Immune cell activation as a risk factor for hypertension in people living with HIV in sub-Saharan Africa using the recent American Heart Association and American College of Cardiology guidelines
SK Masenga1,2, A Kirabo3,4, BM Hamooya1,5, JR Koethe6, SM Munsaka2
1Mulungushi University, School of Medicine and Health Sciences, Livingstone, Zambia; 2University of Zambia, School of Health Sciences, Department of Biomedical Sciences, Lusaka, Zambia; 3Vanderbilt University Medical Center, Division of Clinical Pharmacology, Nashville, TN, USA; 4Vanderbilt University, Department of Molecular Physiology and Biophysics, Nashville, TN, USA; 5University of Zambia, School of Public Health, Department of Epidemiology and Biostatistics, Lusaka, Zambia; 6Vanderbilt University Medical Center, Division of Infectious Diseases, Nashville, TN, USA
Objectives: This study was aimed at determining factors associated with hypertension and the role of immune activation in people living with HIV (PLWH) using the new hypertension guidelines by the American Heart Association (AHA) and the American College of Cardiology (ACC) in sub-Saharan Africa.
Methods: We conducted three cross-sectional, one systematic and one prospective study. The World Health Organization Stepwise approach to Surveillance (WHO STEPs) and the international physical activity questionnaire (IPAQ) were used to collect data for cross-sectional studies while preferred reporting items for systematic reviews and meta-analyses was employed for the systematic study. FlowJo for flow-cytometry analysis and statistical evaluations were employed to elucidate relationships between hypertension and response variables.
Results: Factors significantly associated with increased odds for developing hypertension among 226 PLWH after adjustments in multivariate logistic regression were waist circumference, sedentary lifestyle, age, body mass index, employment status, fasting blood sugar, table salt consumption and moderate physical activity, respectively (P<0.05). 94% had uncontrolled blood pressure. The new AHA/ACC criteria for hypertension shifted 26% of the originally normotensives into hypertension category. Hypertension was associated with higher neutrophil, white blood cell counts and neutrophil lymphocyte ratio (P<0.05).
IL-6 and IL-10 were associated with hypertension in a carefully selected age-sex matched group (n=38) of PLWH (P<0.05). Interleukin (IL)-17A, interferon (IFN)-γ, and higher CD4+ T-cell counts were associated with hypertension in antiretroviral-treated participants in 45 carefully selected studies from 13 unique African countries. High salt intake was associated with increased innate immune cell activation markers (CD86+, CD80+) and hypertension. See Figure 1.
(Abstract P23)
Conclusions: Targeting modifiable risk factors and adaptive immune activation could provide improved care for hypertensive PLWH, however, further research is needed to characterize the inflammatory milieu contributing to hypertension in PLWH especially in African populations where the burden of HIV is the highest.
Abstract P24
Antiviral Therapy 2019; 24 Suppl 1:A70
Virological failure as a predictor of (or risk factor for) metabolic syndrome among patients receiving antiretroviral therapy in Zambia: a cross-sectional study
BM Hamooya1,2, W Mutale2, H Halwiindi2, D Heimburger3,4, L Lipworth3, G Chongwe2, P Musonda2
1Mulungushi University School of Medicine and Health Sciences, Livingstone, Zambia; 2The University of Zambia, School of Public Health, Lusaka, Zambia; 3Department of Medicine, Vanderbilt University School of Medicine, Nashville, TN USA; 4Vanderbilt Institute for Global Health, Nashville, TN, USA
Background: HIV-infected individuals receiving antiretroviral therapy (ART) are at increased risk of metabolic related conditions/diseases. However, in sub-Saharan African countries, including Zambia, screening for metabolic syndrome (MS) is typically not embedded in the management of HIV. Amidst this is the burden of virological failure (VF) among ART patients. This study aims at determining whether MS is associated with VF among HIV patients on ART at Livingstone Central Hospital (LCH), Zambia.
Methods: We conducted a cross-sectional study of HIV-infected individuals aged ≥18 years on ART for ≥6 months, excluding pregnant women and those with known active opportunistic infection or neoplasm at LCH. We collected the following data: demographic information, physical measurements (blood pressure [BP], waist circumference [WC], height, weight), biochemical and immunological measurements, lipid profiles, fasting blood sugar (FBS), ART adherence and behavioural measurements. MS was defined as having three or more of the following: raised BP (diastolic ≥85 mmHg or systolic ≥130 mmHg or self-reported use of antihypertensives), triglycerides (TG; ≥1.7 mmol/l), WC (men ≥95 cm and women ≥80 cm), FBS (≥5.6 mmol/l) and reduced high-density lipoprotein cholesterol (HDL-c [<1.0 males; <1.3 females]). VF defined as viral load (VL) ≥1,000 copies/μl. Descriptive statistics and logistic regression were used to analyse the data.
Results: From April to June 2019, 435 participants (64% women) enrolled, with mean age 45 years (range 18–79), median CD4 absolute count (IQR 412–962) and median VL 21 copies/μl (IQR 0–507). Median time on ART was 108 months (IQR 60–144). MS was prevalent in 65/313 (21%) of participants and VF in 76/420 (18%). Of those with VF, 47% were on a fixed combination of efavirenz, emtricitabine and tenofovir. The predominant components of MS were raised BP (43%), WC (41%) and reduced HDL-c (38%). The prevalence of VF was 24% among the participants with MS. After controlling for sex, age, duration of ART and body mass index, VF was significantly associated with MS (OR 2.17; 95% CI 1.01, 4.67).
Conclusions: Metabolic syndrome and VF are prevalent among HIV patients receiving ART in Livingstone, Zambia, and an observed association between MS and VF warrants further understanding by robust study designs.
Abstract P25
Antiviral Therapy 2019; 24 Suppl 1:A71
Modelling 2018 AHA Cholesterol Guidelines in HIV
G Ciusa1, A Malagoli1, J Milic1, M Menozzi1, F Carli1, A Raimondi1, I Franconi1, G Cuomo1, A Santoro1, G Dolci1, C Mussini1, P Raggi2, G Guaraldi1
1Università degli Studi di Modena e Reggio Emilia, Modena, Italy; 2Division of Cardiology and Mazankowski Alberta Heart Institute, University of Alberta, Edmonton, Canada
Objective: The objective was to assess statin use in people living with HIV (PLWH) in relation to the 2018 AHA Cholesterol Clinical Practice Guideline (CCPG) recommendations and related LDL targets. Data were analysed vis-a-vis the recent AHA scientific statement on prevention and management of CVD in people living with HIV.
Methods: Cross-sectional study of PLWH followed at the Modena HIV Metabolic Clinic (MHMC) in 2017–2018. Mutually exclusive groups were built according to CCPG treatment algorithms recommending high and moderate intensity hypolipaemic therapy (HIH or MIH).
Results: We included 2,123 patients (74% men, mean age 53.5 years). Mean LDL-c and 10-year risk of CV events were 114 ±33 mg/dl and 8.1 ±0.9%. Figure 1 shows the distribution of risk among 2,039 primary prevention PLWH.
(Abstract P25)
CCPG recommends HIH in groups A, C, I. HIH was prescribed in 13.8%, 40.6% and 29.5% of patients in those categories. Among the treated patients, 0%, 67.3% and 47.1% reached an LDL <100 mg/dl.
CCPG recommends MIH in groups B, G, H. MIH was prescribed in 34.2%, 18% and 22.6% of patients in those categories. Among the treated patients, 69.8%, 50% and 40% reached an LDL <100 mg/dl.
In 114 secondary prevention PLWH aged <75 years (6% of our cohort), HIH was prescribed in 34 patients (29%) and MIH in 25 patients (21.9%). Among these patients, only 26.5% reached the LDL-C target <70 mg/dl.
Discussion: In real life statins are largely under-prescribed. The recommended LDL target was reached most often in patients with diabetes mellitus type 2. AHA-PLWH statement failed in identifying recommendations that may clarify statin prescription needing in PLWH.
The recent AHA statement on CV disease in PLWH is ambiguous with regards to treatment indications and LDL goals leaving a therapeutic gap that needs to be filled to improve patients’ outcome.
Abstract P26
Antiviral Therapy 2019; 24 Suppl 1:A73
Prevalence, risk factors and outcomes of cardiovascular, metabolic and chronic kidney diseases in HIV-infected versus uninfected adults in sub-Saharan Africa: a systematic review and meta-analysis
OA Uthman1,2, A Awotiwon3, P Patel4, M Reid5, N Wearne6, PDM Katoto7, B Rayner6, R Davids8, M Estrella9, E Sobngwi10, T Brown11, JB Nachega12,13,14
1Warwick-Centre for Applied Health Research and Delivery (WCAHRD), Warwick Medical School, University of Warwick, Coventry, UK; 2Department of Global Health, Division Epidemiology and Biostatistics, Evidence-Based Health Care, Stellenbosch University, Faculty of Medicine and Health Sciences, Cape Town, South Africa; 3Knowledge Translation Unit, University of Cape Town Lung Institute, Cape Town, South Africa; 4US Centers for Diseases Control, Center for Global Health, Atlanta, Georgia, USA; 5Global Health Sciences, University of California, San Francisco, USA; 6Division of Nephrology, Department of Medicine, Cape Town, South Africa; 7Department of Medicine and Centre for Infectious Diseases, Cape Town, South Africa; 8Department of Medicine, Division of Nephrology Stellenbosch University Faculty of Medicine and Health Sciences, Cape Town, South Africa; 9Kidney Health Research Collaborative Department of Medicine, Division of Nephrology, University of California San Francisco, CA, USA and San Francisco VA Healthcare System, San Francisco, CA, USA; 10Department of Medicine, Laboratory of Molecular Medicine and Metabolism, Yaoundé Central Hospital & University of Yaoundé 1, Yaoundé, Cameroon; 11 Department of Medicine, Division of Endocrinology, Diabetes, & Metabolism, Johns Hopkins School of Medicine, Baltimore, MD, USA; 12Department of Medicine and Center for Infectious Diseases, Stellenbosch University, Faculty of Medicine and Health Sciences, Cape Town, South Africa; 13Departments of Epidemiology and International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA; 14Departments of Epidemiology, Infectious Diseases and Microbiology, University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA, USA
Background: Sub-Saharan Africa (SSA) has the highest burden of HIV in the world; more than 25.5 million Africans are living with HIV in the region, including nearly 15 million on antiretroviral therapy (ART). Expanding use of ART has led to a notable decline in HIV-associated morbidity and death in SSA. Nonetheless, people living with HIV (PWH) in SSA are at substantially increased risk for both cardiovascular and metabolic disease (CVMD) and chronic kidney diseases (CKD). Quantifying prevalence, risk factors and outcomes of CVMD and CKD in PWH in sub-Saharan African represents a pressing research priority.
Methods: We searched electronic databases (Ovid MEDLINE and EMBASE) from 1985 to July 2018. We included studies that reported prevalence estimates for any CVMD and CKD in SSA and information on HIV status and treatment status. We used random-effects meta-analyses to pool prevalence estimates.
Results: A total of 89 studies involving 263,262 participants were included in the meta-analysis. Prevalence estimates were reported in 41 studies on hypertension (HTN), 29 on type 2 diabetes mellitus (T2DM), 14 on metabolic syndrome (MS), 9 on cardiovascular disease (CVD) and 22 on CKD. The reported prevalence estimates varied greatly within countries, between countries and within regions: HTN (5.2% to 45.0%), T2DM (0.9% to 28.1%,), MS (2.1% to 20.4%) and CKD (0.6% to 53.3%). There was no significant difference in the prevalence of HTN and T2DM between HIV-infected and -uninfected participants. The prevalence of MS (OR=1.66, 95% CI 1.01, 2.72, 2 studies) and CKD (OR=2.30, 95% CI 1.12, 4.72, 6 studies) were higher in HIV-infected participants than HIV-uninfected participants. PWH who were treatment-experienced were significantly more likely to be hypertensive than those who were treatment-naive (OR=2.66, 95% CI 1.58, 4.77). There was no significant difference in the prevalence of T2DM, MS and CKD among people living with HIV that were treatment-experienced compared with those who were treatment-naive.
Conclusions: The burden of CVMD and CKD among PWH in SSA is high, although there are wide variations within and across countries and regions. A better understanding of the complex interplay of genetic, environmental and HIV-factors in the pathogenesis of these comorbidities is essential. Furthermore, rigorous implementation science to determine optimal screening, prevention and treatment strategies in PWH in SSA is also critical.
Abstract P27
Antiviral Therapy 2019; 24 Suppl 1:A74
People living with HIV are more likely to be screened for cardiovascular disease risk factors than other members of the general population in Botswana – a community-based study
OJ Molefe-Baikai1, P Melamu2, JT Tlhakanelo3, K Motlhatlhedi3, S Lockman2,4,5, M Mosepele1
1Faculty of Medicine, Department of Internal Medicine, University of Botswana and Department of Medicine, Princess Marina Hospital, Gaborone, Botswana; 2Botswana Harvard AIDS Institute Partnership, Gaborone, Botswana; 3Faculty of Medicine, Department of Family Medicine and Public Health, University of Botswana; 4Department of Immunology & Infectious Diseases, Harvard TH Chan School of Public Health, Boston, USA; 5Division of Infectious Diseases, Brigham & Women's Hospital, Boston, USA
Objectives: People living with HIV (PLWH) are more likely to experience cardiovascular diseases compared with members of the general population. Therefore, we aimed to assess whether PLWH were more likely to have previously been screened for cardiovascular disease risk factors (CVDRF) compared with those without HIV.
Methods: A population-based, cross-sectional study was conducted among individuals aged 16 to 64 years across 22 communities in Botswana between February and August 2017 as part of a larger community-based HIV prevention trial. Participants were asked if they were screened for and counselled about CVDRF (history of hypertension or blood pressure check, blood glucose and cholesterol measurements, weight check and weight control, tobacco smoking and cessation, alcohol use and physical activity) in the last 3 years. HIV testing was offered to those with unknown HIV status. Multivariate logistic regression analysis controlling for age and sex, was used to assess the relationship between CVDRF screening and HIV status.
Results: Among 3,981 participants enrolled, 2,547 (64%) were female, and 1,196 (30%) were PLWH (93% already on ART). PLWH were more likely to report previous screening for diabetes (25% versus 19%; P<0.001), elevated cholesterol (17% versus 12%; P<0.001) and to have had their weight checked (76% versus 55%; P<0.001) than participants without HIV. PLWH were also more likely to have received counselling on salt intake (42% versus 32%; P<0.001), smoking cessation (66% versus 46%; P<0.001), weight control (38% versus 29%; P<0.001), physical activity (46% versus 34%; P<0.001) and alcohol consumption (35% versus 23%; P<0.001) than those without HIV. Overall, HIV-positive status was significantly associated with screening and counselling for CVDRF (AOR 1.84, 95% CI: 1.46, 2.32).
Conclusions: PLWH were almost two times more likely to have been previously screened for CVDRF indicating a need for scale-up of integrated management and prevention of CVD in those without HIV.
Abstract P28
Antiviral Therapy 2019; 24 Suppl 1:A75
Adiponectin levels linked to subclinical myocardial fibrosis in PLWH
J Balmaceda1, T Yeramosu1, CY Liu2, JB Purdy1,C Hadigan1
1National Institute of Allergy and Infectious Diseases, NIH, Bethesda, MD, USA; 2Radiology and Imaging Sciences, NIH, Bethesda, MD, USA
Aim: Impaired myocardial function and heart failure with preserved ejection fraction (HFpEF) are increased in persons living with HIV (PLWH) and remains an area of active research. Previously, we demonstrated that global intramyocardial fibrosis by cardiac MR imaging (CMR) was increased in PLWH without known cardiovascular disease (CVD) and may serve as a marker of subclinical myocardial injury. Adiponectin is an adipocyte-specific cytokine with metabolic effects including insulin sensitivity, and potential protective effects in CVD. However, research has demonstrated that adiponectin levels are elevated in patients with chronic heart failure. This study aims to characterize the relationship between myocardial fibrosis, adiponectin and related metabolic parameters to better understand the pathophysiologic mechanisms of myocardial injury in PLWH.
Methods: We completed a cross-sectional study of 87 PLWH and 28 healthy matched controls without known CVD (median age 48 years, 28% women). Myocardial fibrosis (quantified as extracellular volume index) was measured by CMR (partial results previously reported). Laboratory determinations included metabolic parameter, adiponectin, brain natriuretic peptide (BNP) as well as HIV viral load, CD4 count.
Results: While there was no difference between PLWH and controls in age, sex, BMI, prevalence of metabolic syndrome, adiponectin or BNP levels, myocardial fibrosis index was increased in PLWH (P=0.02). There was a significant positive correlation between adiponectin and myocardial fibrosis (r=0.26; P=0.004) and BNP (r=0.25; P=0.009). In a multivariate regression analysis that included BMI and BNP, adiponectin (P=0.04), sex (P<0.0001) and HIV status (P=0.02) were significant factors associated with myocardial fibrosis.
Conclusions: While adiponectin classically has been described as metabolically protective, the present study, as well as research in non-HIV populations, suggest that the relationship between adiponectin levels and cardiovascular health is more complex. We identify a significant correlation between higher adiponectin levels and myocardial fibrosis in both PLWH and healthy controls, but it remains unclear if this is causal or compensatory. Adiponectin may be a useful serological biomarker for subclinical myocardial fibrosis in future research.
Abstract P29
Antiviral Therapy 2019; 24 Suppl 1:A76
In vitro modelling of the impact of TLR4-LOX-1 cellular signalling in atherogenesis in chronic treated HIV
E Ritou1, T Kelesidis1
1David Geffen School of Medicine at University of California – Los Angeles
Objectives/aim: The mechanisms that drive HIV-related atherosclerosis (CVD) in chronic treated HIV remain unclear. Serum factors (such as bioactive lipids) from HIV+ individuals on potent antiretroviral therapy (ART) may drive atherosclerosis. Oxidized lipids are danger-associated molecular patterns than can interact with pattern recognition receptors such as Tolllike receptor 4 (TLR-4) and lectin-type oxidized LDL receptor 1 (LOX-1). We hypothesized that increased TLR4-LOX-1 cellular signalling is a key mechanism of atherogenesis in chronic treated HIV. Given that observational human studies cannot dissect differential impact of HIV versus antivirals on key mechanisms of atherogenesis, we used an established model of atherogenesis to assess ex vivo the role of the TLR4-LOX-1 axis in early mechanisms of atherogenesis in the presence of plasma from HIV+ individuals on potent ART.
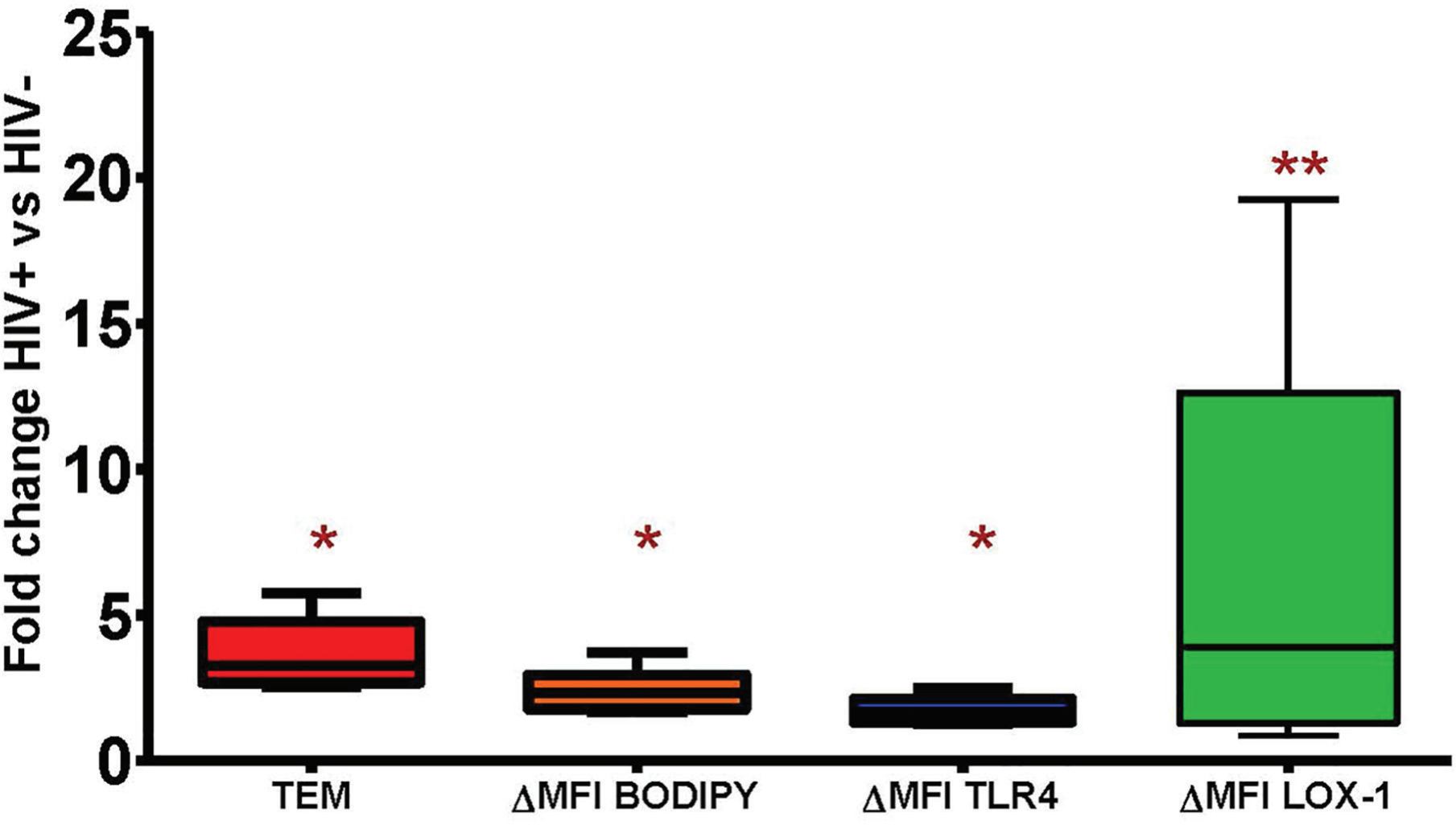
Methods: Our in vitro model of atherogenesis can dissect the impact of HIV plasma on key mechanisms of early atherogenesis such as monocyte chemotaxis and monocyte-derived foam cell formation (MDFCF). Freshly isolated peripheral blood mononuclear cells (PBMCs) from healthy donors (n=6) were added to tumor necrosis factor-activated human umbilical vein endothelial cells monolayers (HUVECs) on type I fibrous collagen gels to transmigrate (transendothelial migration [TEM] or % reverse migration) and form foam cells in the presence of pooled plasma, as previously described. Pooled plasma was isolated from healthy participants (18–40 years old) and HIV+ males (40–60 years old) with no known inflammatory comorbidities other than HIV or risk factors for CVD and on stable potent ART. Flow cytometry assessed MDFCF (ΔMFI BODIPY of CD33+ macrophages inside the gel: fluorescence intensity of BODIPY compared with negative staining control) and cellular levels of TLR4 and LOX-1 in CD33+ myeloid cells. Paired t-test was used for statistical comparison within the same donor (HIV+ plasma versus HIV- plasma).
Results: When media-containing HIV+ compared with HIV- plasma was added to HUVECs, a significantly increased proportion of monocytes underwent transendothelial migration (TEM; median migrated cells 16 versus 4.9%, respectively) and CD33+ macrophages inside the collagen gel had increased lipid content per cell (median ΔMFI BODIPY 673 versus 342, respectively; P<0.05). Compared with HIV plasma, HIV+ plasma induced a mean 3.6-fold increase in TEM, a mean 2.4-fold in MDFCF, a mean 1.75-fold increase in TLR4 and a mean 8.3-fold increase in LOX-1 in CD33+ macrophages inside the collagen gel (P<0.05 for all paired comparisons; Figure 1).
(Abstract P29)
Conclusions/discussion: HIV plasma from patients on potent ART with no clinical CVD directly induces key mechanisms of early atherogenesis (TEM and MDFCF) in parallel to increases in membrane protein levels of TLR4 and LOX-1 in macrophages within the collagen gel (ex vivo model of arterial wall). The role of the TLR4-LOX-1 axis in atherosclerosis in chronic treated HIV needs to be further studied in vivo.