Patterns of inflammation and comorbidity in human immunodeficiency virus (HIV) infection: a clustering analysis from the CARDAMONE study
S Zebachi1, S Hüe2,4, L Boyer3,5, S Gallien2,4, M Surenaud2,4, J-L Lopez Zaragoza2,4, J-D Lelièvre2,4, E Audureau1
1University Paris-Est Créteil (UPEC), IMRB, CEpiA (Clinical Epidemiology and Ageing, EA 7376), Créteil, France; 2Assistance Publique Hôpitaux de Paris (AP-HP), Henri Mondor Hospital, Clinical Immunology and Infectious Diseases Department; 4IMRB, Team 16, Créteil, France; 3Assistance Publique Hôpitaux de Paris (AP-HP), Henri Mondor Hospital, Physiology-Functional Explorations Department; 5IMRB, Team 4 Créteil, France
Objectives: Since the advent of antiretroviral therapy (ART), the occurrence of AIDS-related events has steadily decreased in HIV-infected individuals. Associated with increasing life expectancy, a raise in the incidence of comorbidities such as cardiovascular diseases and metabolic complications has been reported in this population. While the role of key inflammatory markers such as interleukin-6 (IL-6), IL1-β, tumor necrolysis factor α (TNF-α) and sST2 has been discussed, less is known regarding their combinations and their complex interactions with age and other risk factors such as smoking. Therefore, we aim to better characterize and understand the associations between chronic inflammation and the occurrence of comorbidities in people living with HIV, here, through machine learning methods.
Methods: Data were drawn from the CARDAMONE study, including 241 HIV-1-infected participants under ART with comprehensive clinical, biological and functional phenotyping. With a view to identify specific patients’ profiles with similar inflammation patterns and their association with comorbidity occurrence, unsupervised clustering analyses were performed using Self-Organizing Map (SOM) artificial neural network approach, allowing two-dimensional mapping of patients and grouping those with similar inflammation features in clusters. Other clinic-biological characteristics and comorbidities prevalences were analysed as illustrative features.
Results: 4 clusters were identified: (1) gathered the heaviest smokers developing an elevated global inflammatory reaction (MCP-1, hsCRP, IL-6, IL1-β, TNF-α, sST2), (2) comprised younger subjects, mainly women, with globally low inflammatory response, (3) included younger subjects with a moderate and highly specific inflammatory response (sST2, hsCRP) despite the lowest smoking frequency but with the lowest CD4 and CD8 values, (4) grouped the oldest patients with a moderate inflammatory response. See Figure 1.
(Abstract O01)
Conclusions: Clustering analysis identified contrasted inflammation profiles with distinct associations with age, smoking and HIV-related end points. Our results confirm what has already been shown in the literature. We find here a cluster composed of smokers with a high degree of inflammation and a cluster of older people developing a different type of inflammation. The novelty here is the identification of a cluster of relatively young subjects, non-smokers, but developing a particular inflammatory profile. Our findings support the interest of unsupervised machine-learning approaches for improving our knowledge of the complex role of inflammation in HIV-infected individuals.
Abstract O02
Antiviral Therapy 2019; 24 Suppl 1:A4
Colonic microbiota exhibits disparate associations with HIV infection and sexual practices
E Verheij1,2, O Sortino3,4, I Vujkovic-Cvijin5, J Sklar5, FW Wit1,6, NA Kootstra1,7, J Brenchley4, J Ananworanich2,8,9, Y Belkaid5, M Schim van der Loeff10, P Reiss1,2,6, I Sereti4, the AGEhIV Cohort Study Group
1Amsterdam University Medical Centers, University of Amsterdam, Department of Global Health and Division of Infectious Diseases, Amsterdam Infection and Immunity Institute and Amsterdam Public Health Research Institute, Amsterdam, the Netherlands; 2Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands; 3Clinical Monitoring Research Program Directorate, Frederick National Laboratory for Cancer Research sponsored by the National Cancer Institute; 4National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), Bethesda, MD, USA; 5Metaorganism Immunity Section, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, USA; 6HIV Monitoring Foundation, Amsterdam, the Netherlands; 7Amsterdam University Medical Centers, University of Amsterdam, Department of Experimental Immunology, Amsterdam Infection and Immunity Institute, Amsterdam, the Netherlands; 8The Henry M. Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD, USA; 9United States Military HIV Research Program; Walter Reed Army Institute of Research, Silver Spring, MD, USA; 10Public Health Service of Amsterdam, Department of Infectious Diseases, Amsterdam, the Netherlands
Objective: Effective antiretroviral therapy (ART) has prolonged survival and shifted the morbidity spectrum for people living with HIV (PLWH) from AIDS-associated opportunistic infections and malignancies towards age-associated non-communicable comorbidities (AANCCs), with these being more prevalent in PLWH compared with in age-matched HIV-uninfected individuals. A key contributor to the current disease spectrum includes HIV-associated inflammation and immune activation, the aetiology of which in PLWH remains incompletely defined. Gut microbial dysbiosis is thought to be a potential important contributor, but data thus far are conflicting regarding the role that lifestyle factors, including sexual orientation and behaviour, and HIV-infection itself have on gut microbial dysbiosis.
Methods: Using 16S rRNA gene sequencing, we profiled the microbiota from fecal samples of PLWH with suppressed viraemia on ART and HIV-uninfected controls participating in the AGEhIV Cohort Study. PLWH were selected to include 40 men having sex with men (MSM), 20 men having sex with women (MSW) and 20 females (F) matched 1:1 by age, sex, sexual orientation, BMI, birth country and smoking status with HIV-uninfected controls.
Results: HIV-infection was associated with alterations in the gut microbiota including an enrichment in Enterobacteriaceae and Desulfovibrionaceae members and a depletion of short chain fatty acids-producing bacteria such as Lachnospiraceae and Ruminococcaceae. Furthermore, comparisons between MSM and non-MSM males revealed a unique MSM-associated microbiome signature characterized by an enrichment particularly in Prevotellaceae members (Figure 1), which was independent of HIV-infection. Finally, practicing receptive anal intercourse, regardless of condom use, was linked to a specific bacterial community variance independently of sex, which may explain the Prevotella-rich microbiome in MSM.
(Abstract O02)
Conclusions: Our data provide unique evidence that colonic microbiota exhibit disparate associations with HIV-infection and sexual practices.
Abstract O03
Antiviral Therapy 2019; 24 Suppl 1:A5
Higher anti-CMV IgG concentrations are not associated with longitudinal brain injury in virally suppressed people with HIV
J Underwood1,2,3, D De Francesco4, N Koostra5, MWA Caan6, JH Cole7,8, M Caan9, FWMN Wit9,10,11, DJ Sharp8, P Reiss9,10,11, CA Sabin4, A Winston1,12, the COmorBidity in Relation to AIDS (COBRA) collaboration
1Imperial College London, Division of Infectious Diseases, London, United Kingdom; 2Cardiff University, Division of Infection and Immunity, Cardiff, United Kingdom; 3Cardiff and Vale University Health Board, Department of Infectious Diseases, Cardiff, United Kingdom; 4UCL, Institute for Global Health, London, United Kingdom; 5Amsterdam University Medical Centers, Department of Experimental Immunology, Amsterdam, the Netherlands; 6Amsterdam University Medical Centers, Department of Biomedical Engineering & Physics, Amsterdam, the Netherlands; 7King's College London, Department of Neuroimaging, London, United Kingdom; 8Imperial College London, Division of Brain Sciences, London, United Kingdom; 9Amsterdam University Medical Centers, Department of Global Health and Division of Infectious Diseases, Amsterdam, the Netherlands; 10Amsterdam University Medical Centers, Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands; 11Stichting HIV Monitoring, Amsterdam, the Netherlands; 12Imperial College London Healthcare NHS Trust, Department of Genitourinary Medicine & HIV, London, United Kingdom
Objectives: People with HIV (PWH) have a higher CMV seroprevalence than HIV-negative individuals. Higher CMV IgG concentrations have been associated with poorer cognitive function in cross-sectional studies of PWH. We compared the longitudinal relationships between CMV, cognitive function and neuroimaging biomarkers in PWH and demographically-matched HIV-negative controls.
Methods: CMV-seropositive, virally-suppressed PWH and HIV-negative controls from the COBRA study were included. The relationship between anti-CMV IgG and high avidity anti-CMV IgG titres with cognitive function (standardized T-scores measured with a six-domain battery) and MRI biomarkers (volumetric, diffusion and a machine-learning derived prediction of apparent ‘brain age’), measured at baseline and after 2 years, were determined using rank regression adjusted for potential confounders.
Results: 130 PWH and 61 HIV-negative controls were included. Across the whole cohort cross-sectionally, higher anti-CMV IgG titres were associated with poorer global cognitive function and in the domains of processing speed, executive and motor function. This was only observed in PWH (largest effect size motor function: rhoadj=-0.25 [-0.41,-0.09]; P<0.01) although there were no statistically significant interactions between HIV status and anti-CMV IgG titres.
Relationships between anti-CMV IgG titres and neuroimaging biomarkers were generally weak across the cohort (rhoadj <0.15 for all; Table 1) aside from an association with increased brain-predicted age in PWH (rhoadj=0.24 [0.08,0.40]; P<0.01; HIV-status interaction P=0.02).
Relationships between baseline anti-CMV IgG titres, and longitudinal cognitive function and neuroimaging biomarkers were weak (rhoadj<0.15 for all; Table 1) with some associations being in the opposite direction to those found cross-sectionally for executive function and brain-PAD.
(Abstract O03)
Table 1. Rank regression of total anti-CMV IgG with neuroimaging biomarkers for whole cohort (n=191)
Neuroimaging biomarker
Cross-sectional
Longitudinal
rhoadj (95% CI)
P
HIV-interaction p
rhoadj (95% CI)
P
HIV-interaction p
Grey matter volume
−0.02 (−0.11, 0.08)
0.70
0.88
0.09 (−0.03, 0.22)
0.13
0.99
White matter volume
−0.01 (−0.10, 0.08)
0.84
0.14
0.00 (−0.12, 0.11)
0.94
0.05
Cortical thickness - Left
−0.09 (−0.22, 0.05)
0.20
0.35
0.03 (−0.09, 0.15)
0.65
0.47
Cortical thickness - Right
−0.11 (−0.25, 0.02)
0.11
0.33
0.06 (−0.06, 0.17)
0.34
0.86
Whole brain FA
−0.07 (−0.19, 0.05)
0.25
0.14
0.00 (−0.12, 0.13)
0.95
0.43
Whole brain MD
0.10 (−0.01, 0.22)
0.08
0.28
0.03 (−0.09, 0.14)
0.67
0.67
Brain-PAD score
0.16 (0.03, 0.30)
0.02
0.03
−0.11 (−0.23, 0.02)
0.10
0.05
Abbreviations: AD - axial diffusivity; FA - fractional anisotropy; MD - mean diffusivity; RD -radial diffusivity; PAD- Predicted age difference.
Conclusions: Higher anti-CMV IgG titres were not associated with short-term progressive brain injury in virally suppressed PWH. These findings and the lack of associations in HIV-negative controls suggest that the cross-sectional associations in PWH may represent type 1 errors or that CMV-associated brain injury is a static phenomenon in virally suppressed PWH.
Abstract O04
Antiviral Therapy 2019; 24 Suppl 1:A7
Bone mineral density changes in young African women on tenofovir disoproxil fumarate antiretroviral therapy and non-hormonal contraception
F Matovu Kiweewa1,2, N Kiwanuka2, M Nabwana1, E Isingel1, M Glenn Fowler3, ML Nolan1, P Musoke1,4, JM Pettifor5,6, M Beksinska6,7, TT Brown4, the BONE: CARE Study Team
1Makerere University-Johns Hopkins University Research Collaboration, Kampala, Uganda; 2Makerere University School of Public Health, Kampala, Uganda; 3Johns Hopkins University School of Medicine, Baltimore, MD, USA; 4Makerere University College of Health Sciences, Kampala, Uganda; 5MRC/Wits Developmental Pathways for Health Research Unit, Johannesburg, South Africa; 6University of Witwatersrand, Johannesburg, South Africa; 7Maternal Adolescent & Child Health Research, Johannesburg, South Africa; 8Johns Hopkins School of Medicine, Baltimore, MD, USA
Aim: There are limited prospective data on bone mineral density (BMD) changes in HIV-infected young women in low-income countries initiating tenofovir disoproxil fumarate (TDF) containing antiretroviral therapy (ART). The NIH funded BONE: CARE study (R01AI118332) enrolled HIV infected depot medroxyprogesterone acetate (DMPA), or non-hormonal contraceptive users initiating TDF-based ART, as well as an HIV, DMPA unexposed control group. We compare longitudinal data on BMD changes 2 years post TDF initiation among infected non-hormonal users compared with uninfected controls.
Methods: Women were recruited from HIV care centres and general health facilities in and around Kampala, Uganda and classified into 4 groups: A) HIV+/DMPA+/ TDF+, B) HIV+/DMPA+/TDF-, C) HIV+/DMPA-/TDF+ and D) HIV-/-DMPA-/TDF-. All HIV-infected women were ART-naive at baseline. BMD assessments of lumbar spine (LS), total hip (TH) and femoral neck (FN) were conducted using dual energy X-ray absorptiometry at semi-annual intervals. We used repeated measures analyses to compare the rate of change, calculated as the percent change in BMD per year between HIV-infected and uninfected women during the initial 2 years of ART initiation, adjusting for age, parity, education and baseline BMD.
Results: Between March 2015 and October 2017, we screened 549 women. Of the 529 women enrolled, 176 were non-hormonal contraceptive users; 109 HIV-infected and 69 uninfected. The median age was 25 (22–30) years. There was greater adjusted BMD percent decline among HIV-infected women than controls at the LS and NF compared with HIV-uninfected women (P=0.01 and 0.004 respectively) but not at the TH (P=0.716), see Table 1. Prior use of DMPA ≥2 years pre-ART initiation was not significantly associated with greater BMD loss among infected women.
(Abstract O04)
Figure: Differences in bone mineral density among 2 years post TDF initiation among infected non-hormonal users compared to un-infected controls
Body site
Crude % difference in mean BMD change (95% CI)
P-value
Adjusted % difference in mean BMD change (95% CI)
P-value
Lumbar spine
−0.75 (−1.25 to-0.27)
0.002
−0.90 (−1.46 to-0.36)
0.001
Total hip
0.086 (−0.35 to 0.53)
0.703
−0.09 (−0.58 to 0.40)
0.716
Femur neck
−0.73 (−1.38 to-0.09)
0.026
−1.04 (−1.75 to-0.33)
0.004
Adjusted for age, BMI, education and baseline BMD
Conclusions: HIV-infected non-hormonal users experienced significantly greater BMD loss at the LS and TH. Data from DMPA users in this cohort will establish the additional effect of DMPA use on BMD among women on TDF.
Abstract O05
Antiviral Therapy 2019; 24 Suppl 1:A8
Association of current estradiol use with carotid intimal media thickness among transgender women: a cross-sectional study
RC Moreira1, ACG Ferreira1, LE Coelho1, EM Jalil1, I Bensenor2, RK Friedman1, L Monteiro1, LF Eksterman1, RI Moreira1, SW Cardoso1, VG Veloso1, D Chor3, B Grinsztejn1, AG Pacheco4
1Evandro Chagas National Institute of Infectious Diseases, Oswaldo Cruz Foundation, Rio de Janeiro, RJ, Brazil; 2University of São Paulo, School of Medicine, São Paulo, Brazil; 3Department of Epidemiology, National School of Public Health, Oswaldo Cruz Foundation, Rio de Janeiro, RJ, Brazil; 4 Scientific Computing Program, Oswaldo Cruz Foundation, Rio de Janeiro, RJ, Brazil
Background: Epidemiological studies suggest that transgender population has higher burden of cardiovascular (CV) risk factors and CV disease. It is uncertain whether the use of feminizing hormone such as estradiol (E2) or ethinylestradiol (EE) affects their risk. We aimed to assess CV risk and investigate the relationship between current use of E2 or EE and carotid intima-media thickness (cIMT) in transgender women (transwomen).
Methods: Cross-sectional evaluations of transwomen in the Transcendendo cohort in Rio de Janeiro, Brazil with a valid cIMT at baseline visit, from August 2015 to February 2017. cIMT was measured by ultrasonography, following the Mannheim protocol. Increased cIMT was defined as a measurement above the 75th percentile. We tested the association of E2, EE or both with cIMT. Covariables included traditional cardiovascular risk factors, HIV status, drug use and history of feminizing procedures. Framingham and ASCVD risk scores were calculated and compared with cIMT. Adjusted logistic regression models were fitted and odds ratios (OR) were used to assess the association of current use of the three hormone categories with cIMT.
Results: 308 transwomen were included; median age was 31 years (interquartile range [IQR]=25–38), 53.8% had HIV infection. Among current hormone users (40.8%), the most frequent were estradiol (26.53%), ethinylestradiol (5.15) or a combination of both (9.18%). Median cIMT was 0.57 mm (IQR=0.52– 0.64). In participants with increased cIMT, 11 (3.97%) and 24 (8.66%) were classified as high risk by the Framingham equation and ASCVD, respectively. In the final adjusted model, age (OR=1.14, 95% CI=1.08, 1.20), systolic blood pressure (OR=1.05, 95% CI=1.01, 1.09) and estradiol use (OR=0.34, 95% CI=0.11, 0.92) were associated with cIMT.
Conclusions: A negative association between cIMT and current estradiol use was found in transgender women. The ASCVD equation identified more participants as high risk among those with increased cIMT. While conflicting results exist in the literature about estrogen replacement therapy in women, these data suggest cardioprotective effects of estradiol use without medical supervision in younger transwomen. Follow-up studies are needed to confirm its safety and it might be considered as a choice of hormone for transwomen.
Abstract O06
Antiviral Therapy 2019; 24 Suppl 1:A9
An analysis of HIV and comorbidity profiles for adults accessing health care in Khayelitsha, South Africa
R Osei-Yeboah1, O Ngwenya2, N Tiffin1,2,3
1Division of Computational Biology, Institute of Infectious Diseases and Molecular Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa; 2Wellcome Centre for Infectious Disease Research in Africa, Institute of Infectious Diseases and Molecular Medicine, University of Cape Town; 3Centre for Infectious Disease Epidemiology Research, School of Public Health and Family Medicine, University of Cape Town
Aim: To explore the HIV comorbidities profile of patients accessing public health care at Khayelitsha.
Methods: A longitudinal dataset for all individuals who accessed public health facilities at Khayelitsha from January 2016 – December 2017 was obtained from the Western Cape Provincial Health Data Centre. Descriptive and inferential statistics explored demographics, HIV cases and comorbidities, and pairwise associations between comorbidities using Pearson's product-moment correlation.
Results: Of 181,620 individuals (median age 37 years, IQR: 30–48) seeking health, 131,933 (72.6%) were females and 49,521 (27.4%) were males. Of 88,316 people living with HIV (PLHIV), 63,016 (71.4%) were female and 25,219 (28.6%) male. Males seeking health care were 1.15 (CI= 1.11, 1.16) times more likely to have HIV than females. Median age (IQR) of HIV ascertainment differed in females 35 (30–43) and males 40 (34–47), P<0.001. Tuberculosis (31.4%), hypertension (14%), mental health conditions (5.3%), diabetes (4.1%), cancers (1.81%) and chronic kidney disease (CKD; 1.7%) were the top 6 comorbidities identified, with correlations between hypertension and diabetes (r=0.24), hypertension and CKD (r=0.13) and diabetes and CKD (r=0.13); all P<0.001 in PLHIV. Whilst comorbidity clustering varied with age, median ages of ascertainment of comorbidities were younger in PLHIV than HIV-negative individuals except for tuberculosis (Table 1). Significant differences were also found between median ages of ascertainment for comorbidities in females and males with HIV. Discussion: As HIV-related mortalities decline and life expectancy increases, PLHIV face increasing burden of chronic comorbidities. This burden, in addition to existing tuberculosis, in PLHIV seeking care in South Africa is rising. Differences between female and male demographics also reflect to some extent contraceptive/ maternal care access by women in good health.
(Abstract O06)
Table 1: Median age (Interquartile range) of ascertainment of each comorbidity in HIV- and HIV* individuals
Co-morbidity
HIV-Median Age (IQR) 38(28–55)
HIV+ Median Age (IQR) 37(31–44)
P value <.001
Diabetes
57 (48.65)
43 (40.56)
<.001
Hypertension
55 (46.64)
46 (39.54)
<.001
Tuberculosis
37 (28.53)
39 (33.46)
<.001
Chronic Kidney Disease
66 (58.74)
50 (42.58)
<.001
Cervical Cancer
57 (45.65)
42 (36.48)
<.001
Chronic Obstructive Pulmonary Disease
53 (36.64)
43 (35.51)
<.001
Mental Hearth Condition
42 (29.57)
39 (32.48)
<.001
Conclusions: The emerging burden of chronic HIV comorbidities requires in-depth studies to inform adequate planning for all-encompassing health-care delivery.
Abstract O07
Antiviral Therapy 2019; 24 Suppl 1:A10
Integrase inhibitors dolutegravir and raltegravir exert proadipogenic and profibrotic effects and induce insulin resistance in adipose tissue and adipocytes
J Gorwood1, C Bourgeois2, V Pourcher3, F Charlotte3, G Pourcher4, M Mantecon1, C Rose1, R Morichon1, R Le Grand2, C Katlama3,5, B Fève1,6, O Lambotte2,7, J Capeau1, V Béréziat1*, C Lagathu1*
*Both authors contributed equally to this work
1Sorbonne Université, Inserm UMR_S 938, Centre de Recherche Saint-Antoine, ICAN, Paris, France; 2CEA, Université Paris Sud, Inserm U1184, ImVA, IDMIT, Fontenay-aux-Roses, France; 3AP-HP, Sorbonne Université, Hôpital Pitié-Salpêtrière, Service de maladies infectieuses et tropicales, INSERM U1136, Institut Pierre Louis d'épidémiologie et de Santé publique et d'Anatomo-Pathologie, Paris, France; 4Institut Mutualiste Montsouris, Service de Chirurgie Digestive, Paris, France; 5Sorbonne Université, Inserm, Institut Pierre Louis d'épidémiologie et de Santé Publique, Paris, France; 6AP-HP, Hôpital Saint-Antoine, Service d'endocrinologie, Paris, France; 7APHP, Hôpital Bicêtre, Service de Médecine Interne et Immunologie Clinique, Kremlin-Bicêtre, France
Objectives: There is growing evidence that integrase inhibitors (INSTI) dolutegravir and raltegravir promote peripheral and central adipose tissue/weight gain in HIV-infected individuals, but the mechanisms involved remain unknown. We aimed to assess the effect of these molecules on adipose tissue morphology, function and metabolism.
Methods: Morphology and function of subcutaneous (SCAT) and visceral adipose tissue (VAT) were studied in: HIV-infected patients from the ObeVIH study, at the time of bariatric surgery (BMI 41.8 kg/m2): 14 patients received INSTI (10 dolutegravir, 2 raltegravir, 2 elvitegravir) and 5 an INSTI-sparing regimen; and uninfected cynomolgus macaques treated or not 15 days with dolutegravir/tenofovir/emtricitabine. Human adipose stem cells (ASCs) were chronically treated with dolutegravir or raltegravir before or during adipogenesis. Adipogenic capacities, insulin response and extracellular matrix component expression were analysed.
Results: SCAT from the ObeVIH patients presented peri-lobular and peri-adipocyte fibrosis in most samples. Conversely, VAT of INSTI-treated patient presented a higher level of peri-adipocyte fibrosis than that of non-INSTI-treated patients.
Dolutegravir-treated macaques presented a higher level of fibrosis and an increased adipocyte size in both SCAT and VAT, when compared with untreated macaques. Adipogenic marker expression was increased in SCAT and VAT, whereas adiponectin expression was decreased in SCAT, suggesting that, despite a pro-adipogenic effect, dolutegravir may favour insulin resistance.
In ASCs, INSTI-treatment increased collagen 1 and 6 and α-smooth-muscle-actin expression indicating a pro-fibrotic effect. In ASC-differentiated adipocytes, dolutegravir, and to a lesser extent raltegravir, increased lipid accumulation and adipogenic marker expression, decreased adiponectin expression and induced insulin resistance.
Conclusions: We demonstrate here for the first time, by using in vivo and in vitro complementary models, that INSTI exert a direct impact on adipose tissue adipogenesis, fibrosis and insulin resistance. These results, which reveal the adipose tissue toxicity of dolutegravir and raltegravir, are important to explain fat modifications reported in INSTI-treated HIV-infected patients.
Abstract O08
Antiviral Therapy 2019; 24 Suppl 1:A11
Dolutegravir-based regimens are associated with weight gain over 2 years following ART-initiation in ART-naive people living with HIV (PLWH)
SA Ruderman1, RM Nance1, BM Whitney1, JAC Delaney1, BN Harding1, KH Mayer2, RD Moore3, JJ Eron4, E Geng5, WC Mathews6, B Rodriguez7, MS Saag8, S Lindström1, BR Wood1, AC Collier1, V Vannappagari9, C Henegar9, J Van Wyk10, L Curtis11, GA Burkholder8, MM Kitahata1, HM Crane1
1University of Washington, Seattle, WA, USA; 2Harvard Medical School, Fenway Institute, Boston, MA, USA; 3Johns Hopkins, Baltimore, MD, USA; 4University of North Carolina, Chapel Hill, NC, USA; 5University of California San Francisco, San Francisco, CA, USA; 6University of California San Diego, San Diego, CA, USA; 7Case Western University, Cleveland, OH, USA; 8University of Alabama at Birmingham, Birmingham, AL, USA; 9ViiV Healthcare, RTP, NC, USA; 10ViiV Healthcare, Brentford, UK; 11GlaxoSmithKline, Uxbridge, UK
Objectives: Previous studies have suggested that PLWH who initiate integrase-inhibitor-based regimens may gain more weight than those who initiate other antiretroviral therapy (ART). These studies have often examined classes not individual agents, been small, combined ART-experienced and naive PLWH, and did not address key potential confounders such as regimen backbone. We evaluated weight change among PLWH initiating ART in the current treatment era.
Methods: Across eight CNICS sites we identified ART-naive PLWH initiating ART between 2012–2018, including efavirenz (EFV; n=404), rilpivirine (RPV; n=347), atazanavir (ATV; n=90), darunavir (DRV; n=245), raltegravir (RAL; n=89), elvitegravir (EVG; n=981) and dolutegravir (DTG; n=295) -based regimens with a tenofovir (TDF)/emtricitabine (or lamivudine) backbone. We also examined dolutegravir-based regimens with abacavir/lamivudine (ABC; n=338). Weight change was estimated using linear mixed models adjusted for time on regimen, time on regimen x regimen interaction, age, sex, race, hepatitis C, hepatitis B, nadir CD4, smoking, diabetes, anti-psychotic medication use and site.
Results: Mean follow-up was 2.0 years. Compared with EFV, DTG/TDF was associated with a 2.6 kg (95% CI: 1.6, 3.6) per year greater weight gain while DTG/ABC was associated with a 2.1 kg (95% CI: 1.4, 2.8) per year greater gain. Other integrase-inhibitor-based regimens showed less weight gain per year. Weight gain on DTG was statistically significantly greater than EFV, RPV, ATV and EVG, but not DRV (1.8 kg per year, 95% CI: 0.9, 2.7). Generalized additive model plots suggested that weight gain on DTG occurred in the first 2 years following regimen initiation (Figure 1).
(Abstract O08)
Conclusions: DTG users had the greatest 2-year weight gain, regardless of backbone, although weight gain was not significantly higher than in DRV users. For ART-naive PLWH, potential weight gain should be considered in conjunction with the benefits of viral suppression when comparing DTG with other ART regimens.
Abstract O09
Antiviral Therapy 2019; 24 Suppl 1:A12
Switching to an integrase inhibitor containing antiretroviral regimen is not associated with above-average weight gain in middle-aged people living with HIV on long-term suppressive antiretroviral therapy, the AGEhIV cohort study
SO Verboeket1,2, A Boyd3,4, FW Wit1,2,3, E Verheij1,2, MF Schim van der Loeff1,4, N Kootstra5, M van der Valk1, P Reiss1,2,3, the AGEhIV Cohort Study
1Amsterdam UMC, University of Amsterdam, Department of Internal Medicine, Amsterdam Infection and Immunity Institute and Amsterdam Public Health Research Institute, Amsterdam, the Netherlands; 2Amsterdam UMC, University of Amsterdam, Department of Global Health and Amsterdam Institute for Global Health and Development, Amsterdam, the Netherlands; 3HIV Monitoring Foundation, Amsterdam, the Netherlands; 4Public Health Service of Amsterdam, Department of Infectious Diseases, Amsterdam, the Netherlands; 5Amsterdam UMC, University of Amsterdam, Department of Experimental Immunology, Amsterdam Infection and Immunity Institute, Amsterdam, the Netherlands
Objectives/aim: Recently, several US-based cohorts reported significant weight gain in people with suppressed viraemia after switching to an integrase inhibitor (INSTI). We evaluated changes in standardized bodyweight measurements among individuals before and after switching to an INSTI-containing regimen and compared these changes to (1) non-switching HIV-positive and (2) lifestyle-comparable HIV-negative control groups, all participants in the AGEhIV Cohort Study.
Methods: In 598 HIV-positive and 550 HIV-negative AGEhIV participants bodyweight was measured biennially using calibrated scales. Virally suppressed HIV-positive participants switching to an INSTI-containing antiretroviral regimen during follow-up were matched 1:2:2 with participants from both control groups, using a time-dependent propensity score based on gender, ethnicity, age and body mass index (BMI). Controls were matched at the visit at which the control's propensity score most resembled that of the corresponding index-participant's visit prior to INSTI-switch, also rendering a hypothetical moment of switch for the control participants. Mean yearly bodyweight changes before and after (hypothetical) switch within and between groups were compared using linear mixed-effects models. In addition, frequencies of >5% and 10% weight gain were compared between index and control groups after (hypothetical) switch using logistic regression.
Results: 119 HIV-positive participants switched to an INSTI-containing regimen (53% dolutegravir; 35% elvitegravir; 13% raltegravir) and had a bodyweight measured ≥1 times before and after switch. At the visit prior to switch, median age was 55 years (IQR 50-61), BMI 24 kg/m2 (IQR 22-26), 87% were male, and 89% were Caucasian. Median time between switch and end of follow-up was 2.0 (IQR 1.0-3.0) years. In 49% the NRTI-backbone was simultaneously modified, the majority from tenofovir disoproxil/emtricitabine to tenofovir alafenamide/emtricitabine (18%) or abacavir/ lamivudine (11%). Due to the propensity score matching, both the HIV-positive and -negative control groups were highly comparable to the index group regarding age (median 54 and 53), BMI (median 24 and 24 kg/m2), sex (91% and 84% male) and ethnicity (89% and 92% Caucasian). There were no significant differences in yearly mean change in bodyweight within or between groups before and after (hypothetical) switch (Table 1). A >5% increase in bodyweight occurred in 28 (23.5%) HIV-positive participants after INSTI initiation, and in 31 (13%; P=0.013) non-switching HIV-positives, and in 28 (11.8%; P=0.005) HIV-negative controls, after their hypothetical moment of switch. A >10% increase in bodyweight occurred in 6 (5.0%),7 (2.9%; P=0.3) and in 6 (2.5%; P=0.2), respectively.
(Abstract 009)
TABLE. Change in bodyweight by group before and after real or hypothetical switch to INSTI
Mean yearly change in body weight within each group, before and after real or hypothetical moment of switch to INSTI
Before switch
After switch
N
kg/year
95% CI
kg/year
95% CI
INSTI switch
119
0.11
−0.11,0.33
0.17
−0.22,0.55
Continuation NNRTI/PI-based regimen
238
0.14
−0.06,0.33
0.22
0.02,0.42
HIV-negative
238
0.08
−0.12,0.29
0.18
0.00,0.36
Difference in mean yearly change in bodyweight after vs. before real or hypothetical moment of switch to INSTI within each study group
Δ kg/year
95% CI
P
INSTI switch
0.06
−0.37,0.48
.8
Continuation NNRTI/PI-based regimen
0.08
−0.18,0.34
.5
HIV-negative
0.09
−0.16,0.35
.5
Difference in mean yearly change in body weight between study groups before real or hypothetical switch to INSTI
Δ kg/year
95% CI
P
INSTI switch vs. continuation NNRTI/PI-based regimen
−0.03
−0.32,0.27
.9
INSTI switch vs. HIV-negative
0.02
−0.28,0.33
.9
Difference in mean yearly change in body weight between study groups after real or hypothetical switch to INSTI
Δ kg/year
95% CI
P
INSTI switch vs. continuation NNRTI/PI-based regimen
−0.05
−0.49,0.38
.8
INSTI switch vs. HIV-negative
−0.01
−0.44,0.41
.9
Reported results were calculated from a linear mixed-effects model with bodyweight as the outcome, and the 3-way interaction-term studygroup*time*before/after switch as predictor variable. Abbreviations: CI, Confidence Interval; NNRTI, Non-Nucleoside Reverse Transcriptase Inhibitor; PI, Protease Inhibitor
Conclusion(s)/discussion: We found no evidence for above-average weight gain in virologically suppressed patients switching to an INSTI-containing regimen. However, clinically relevant weight gain upon switching to INSTI may be a relatively rare phenomenon deserving further investigation.
Abstract O10
Antiviral Therapy 2019; 24 Suppl 1:A14
Impact of the reproductive/hormonal status on weight, fat and insulin resistance in HIV-infected women switching from a PI regimen to dual raltegravir-etravirine therapy: results from the ANRS163-ETRAL trial at 48 and 96 weeks
L Assoumou1,N di Clemente2,S Fellahi2,L Beniguel1,J-P Bastard2,B Feve2,H Fromentin3,C Katlama1,D Costagliola1,J Capeau2
1Faculty of Medicine, Sorbonne University, Inserm UMR_S1136,IPLESP, Department of Infectious Diseases, Pitié-Salpétrière Hospital, APHP, Paris, France; 2Faculty of Medicine, Sorbonne University, Inserm UMR_S938,CRSA, ICAN, Paris, France; 3ANRS, Paris, France
Objectives: The ANRS 163 ETRAL trial (NCT02212379) has previously shown the viral efficiency of a dual raltegravir/etravirine therapy in 165 PI-controlled ageing HIV-infected individuals followed-up for 96 weeks. While lipid and bone parameters improved, patients gained weight, trunk and limb fat and increased insulin resistance. In a sub-study, we evaluated whether these anthropometric/ metabolic modifications were dependent upon sex, and upon the reproductive/menopausal status.
Methods: 48 women were included. Fat mass and bone mineral density were evaluated by DEXA at D0,W48 and W96. We recorded the menopausal status with a questionnaire. To assess the reproductive status, ovarian reserve was evaluated in 40 women by the level of the anti-Müllerian hormone (AMH, Gen II, ELISA) at D0 and W48. Insulin resistance was measured at D0,W48 and W96 by using the HOMA-IR index. We separated women into three groups according to their AMH level (detectable or not) and menopausal status. Baseline values and percent changes from baseline were compared between groups using Mann–Whitney and Kruskal–Wallis tests.
Results: ETRAL patients were 117 men and 48 women, median age 52 years. BMI, total, trunk and limb fat mass similarly increased in men and women at W48 and W96 (Table 1),indicating a global fat gain at the limb and trunk level. Baseline HOMA-IR was similar in men and women. It increased in men and women at W48 and in men at W96 (Table 1). Lipid parameters improved similarly (increased HDL, decreased triglycerides) in men and women at W48 and W96. As well, there was no gender differences in the evolution of bone mineral density at the hip and lumbar level from D0 to W96.
Regarding reproductive/menopausal status,12 women (30%,age 46 years) had reproductive activity with ovarian reserve (group 1,AMH >0.06 ng/ml),6 (15%,47 years) were premenopausal with no ovarian reserve (group 2,AMH <0.02 ng/ml) and 22 (55%,54 years) were post-menopausal (group 3). Baseline BMI and fat repartition did not differ between the three groups. At W48 and W96,BMI, total and trunk fat increased in groups 2 and 3 but not in group 1. Moreover, HOMA-IR worsened in groups 2/3 but tended to improve in group 1 (Table 1). The evolution of limb fat, bone and lipid parameters was not different according to the group (except increased HDL in groups 1/2 but not 3 at W96).
(Abstract O10)
Table: Comparison of BMI, total fat and HOMA-IR according to sex and to reproductive/menopausal status in the ANRS163-ETRAL study
n
Baseline
% change at W48
% change at W96
BL vs W48
BL vs W96
BMI kg/m2
Men
117
24.1(22.5-25.7)
1.5(−1.3-5.3)
2.8(0-6.5)
0.000
0.000
Women
48
24.9(22.5-29.2)
1.6(−1.9-4.6)
1.8(−1.8-6.8)
0.043
0.010
P-value
0.094
0.758
0.510
Total fat kg
Men
71
16.7(11.9-22)
1.8(−2.7-21.6)
11.8(0-22.5)
0.001
0.000
Women
22
25.7(17-38.1)
6.4(0.6-18.1)
6.8(−2.5-21.9)
0.025
0.023
P-value
0.000
0.539
0.492
HOMA-IR
Men
110
1.7(1.2-2.4)
1.6(−17.2-43.6)
15.2(−12.8-59.4)
0.017
0.000
Women
46
1.9(1.2-3.2)
13.7(−28.7-80.9)
3.5(−25.4-32.4)
0.025
0.731
P-value
0.450
0.442
0.074
BMI kg/m2
Reproductive activity
12
27.7(23.6-34.1)
−1(−4.6-1.6)
−1(−5.5-2.6)
0.333
0.594
Premenopausal/Postmenopausal
28
24.9(22.5-27.7)
2.7(0-9.2)
2.3(0-6.9)
0.009
0.005
P-value
0.302
0.018
0.074
Total fat kg
Reproductive activity
5
36.5(30.6-39.3)
0.6(−6-1.5)
−2.6(−8.9-2.1)
0.893
0.500
Premenopausal/Postmenopausal
12
23.9(17-36.3)
16.6(4.5-22.2)
17.3(2.8-28.2)
0.008
0.012
P-value
0.343
0.020
0.035
HOMA-IR
Reproductive activity
12
3(1.8-4)
−42.6(−61-0.1)
−40.2(−54.4–1.6)
0.239
0.084
Premenopausal/Postmenopausal
27
1.7(1-2.8)
40.8(−8.6-87.7)
16.8(−6.2-50.3)
0.002
0.022
P-value
0.051
0.003
0.004
Conclusions: Fat gain and insulin sensitivity seem to be related to the reproductive/menopausal status. Women with reproductive activity and a remaining ovarian reserve would be protected from raltegravir/etravirine-induced weight gain and associated insulin resistance while pre- and post-menopausal women increased weight, fat and insulin resistance, as did men. A role for the oestrogen/androgen status should be considered in the impact of antiretroviral drugs on weight gain. This sub-study was supported by a grant from ANRS/MSD.
Abstract O11
Antiviral Therapy 2019; 24 Suppl 1:A16
Environmental exposures are associated with increased respiratory morbidity among persons living with HIV (PLWH)
S Raju1,HC Ramamurthi2,TT Brown1,GD Kirk1,2,MC McCormack1
1Department of Medicine, School of Medicine, Johns Hopkins University, Baltimore, MD, USA; 2Department of Epidemiology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA
Objectives: Chronic lung disease has emerged as an important comorbidity for PLWH. HIV has been described to increase susceptibility to cigarette smoke, leading to lung injury. Indoor air pollutants related to particulate matter (PM),nitrogen dioxide (NO2) and second-hand smoke (SHS) are common exposures as well which increase lung inflammation and lead to lung injury. While studies suggest that HIV alters susceptibility to smoking, the impact of indoor air pollutants among PLWH is unknown. We aimed to a) determine the association between sources of indoor air pollution and respiratory outcomes in a cohort of PLWH at risk for both pollutant exposure and lung disease, and b) describe how HIV modifies the impact of pollutants.
Methods: We analysed cross-sectional data from the Study of HIV Infection in the Etiology of Lung Disease (SHIELD) in Baltimore, MD, USA, consisting of both PLWH and HIV-uninfected participants. Participants complete lung function testing and questionnaires about environmental exposures; including SHS, NO2 producing appliances (gas stoves/ovens),pest allergens (rodents, cockroach),mould and occupational exposures (vapours, dust, fumes). Respiratory symptoms captured through the American Thoracic Society-Division of Lung Diseases (ATS-DLD) questionnaire included: chronic cough, wheeze, phlegm and experiencing ≥2 wheezing attacks/year. We utilized logistic regression to determine associations between sources of indoor air pollution and respiratory outcomes, after adjusting for potential confounders (demographics, smoking status, injection drug use, lung function-FEV1,household income and HIV status). We generated interaction terms to determine effect modification by HIV serostatus.
Results: Of 1997 participants, 1,109 (55.5%) were PLHW. Among PLWH 48.4% had undetectable viral load. Pollutant exposure was common, with 1,490 (74.6%) using NO2 producing appliances,646 (34.2%) with significant occupational exposures, and 1,373 (68.3%) noting household SHS. A number of exposures were associated with chronic respiratory symptoms after adjusting lung function and traditional risk factors. Occupational exposures (OR 1.37; P=0.007),mould (OR 1.79; P<0.001) and pest allergens (OR 1.37; P=0.016) were associated with higher odds of chronic phlegm and other symptoms. PLWH were notably more susceptible to the effects of SHS and NO2 producing appliances (Figure 1). NO2 exposure was linked to increased odds of chronic wheeze and wheezing attacks among PLWH (OR 1.41; P=0.023),but not in uninfected participants (OR 0.97; P=0.869; P-interaction =0.040). Regular household SHS exposure was associated with greater risk for chronic phlegm (OR 1.43; P-value =0.015),even after accounting for personal smoking status, but only among PLWH (P-interaction =0.045). Among PLWH, we did not detect effect modification by viraemia status.
(Abstract O11)
Discussion: We describe in a cohort of PLWH that indoor environmental exposures are common and associated with greater respiratory morbidity. PLWH may also be more susceptible to the effects of NO2 and SHS, indoor environmental exposures which are modifiable. These results suggest that future studies of HIV-associated lung disease should involve more detailed environmental monitoring to increase our understanding of the full impact of indoor air pollution in PLWH.
Abstract O12
Antiviral Therapy 2019; 24 Suppl 1:A18
HIV infection and smoking: functional PET imaging reveals early pulmonary perfusion abnormalities
P Kohli1,2,M Kone1,VJ Kelly1,KA Hibbert1,2,B Corleis3,J Cho4,D DeFaria-Yeh5,DS Kwon2,3,6,B Medoff1,2,R Scott Harris1,2,T Winkler7
1Division of Pulmonary and Critical Care at Massachusetts General Hospital; 2Harvard Medical School; 3The Ragon Institute of MGH, MIT and Harvard; 4Department of Internal Medicine and, Carver College of Medicine and, The University of Iowa; 5Division of Cardiology at Massachusetts General Hospital; 6Division of Infectious Disease at Massachusetts General Hospital; 7Department of Anesthesia at Massachusetts General Hospital
Rationale: COPD is the most common non-infectious pulmonary disease amongst people living with HIV. Studies suggest that the development of COPD is accelerated in this population. Although prior investigation has established an association between chronic HIV infection and the development of COPD independent of smoking, the cause for this enhanced susceptibility remains unclear. Because pulmonary perfusion alterations have been demonstrated with the development of COPD, multimodal functional imaging may detect early physiological abnormalities in the distribution of pulmonary perfusion in these susceptible individuals.
Methods: We used low dose computed tomography (LDCT) and positron emission tomography (PET) in 46 subjects,23 with documented HIV infection. We collected anthropometrics, lung function and smoking history for all subjects. LDCT was used to assess the quantity and location of low-attenuation areas in the lung at mean lung volume. Global and regional perfusion in each subject were analysed using dynamic PET scans of intravenously infused nitrogen-13 (13NN). After removal of image noise, vertical and axial gradients in perfusion were calculated. We tested for a difference in the total spatial heterogeneity of perfusion (CV2Qtotal) and the heterogeneity caused by its components (CV2Qtotal = CV2Qvgrad [vertical gradient] + CV2Qzgrad [axial gradient] + CV2Qr [residual heterogeneity]) between clinical groups, based on HIV infection and smoking.
Results: Of the 23 subjects with documented HIV infection, 21 had low to undetectable viral loads (<100 copies/ml), 19 were on antiretroviral therapy (ART) and 12 were current smokers. There were no significant differences in demographic parameters between subjects living with and without HIV. All subjects had minimal radiographic evidence of emphysema by visual assessment and % HU<-950 at mean lung volume (MLV). Compared with controls, nonsmokers living with HIV had a significantly greater CV2Qr/CV2Qtotal (0.36 versus 0.48; P=0.05) and reduced CV2Qvgrad/CV2Qtotal (0.46 versus 0.65; P=0.038). Current smokers, independent of HIV status, had a significantly reduced CV2Qvgrad/CV2Qtotal compared with nonsmokers (0.36 versus 0.6; P=0.002). Amongst smokers, there was no significant difference in CV2Qvgrad/CV2Qtotal between those living with and without HIV (0.39 versus 0.34; P=0.58), despite a trend towards an attenuated slope of vertical perfusion gradient in smokers living with HIV. See Figure 1.
Conclusions: In subjects living with well-controlled HIV and minimal radiographic emphysema, both HIV infection and smoking are associated with an increased perfusion heterogeneity and a reduction in the vertical gradient of perfusion. These data indicate the onset of subclinical pulmonary perfusion abnormalities prior to the development of significant lung disease in these susceptible individuals.
(Abstract O12)
Abstract O13
Antiviral Therapy 2019; 24 Suppl 1:A20
Cigarette smoking disproportionately impairs nitric oxide signalling in pulmonary artery endothelial cells in HIV: role of viral and host factors
S Aggarwal, JM Wells, I Ahmad, S Matalon, SL Heath
University of Alabama at Birmingham, Birmingham, AL, USA
Rationale: HIV-associated pulmonary arterial hypertension (HIV-PAH) is a well-recognized severe cardiovascular complication of HIV infection with an adverse prognosis irrespective of the stage of disease. The prevalence of PAH in individuals with HIV is several fold greater than individuals without HIV infection. This high rate of HIV-associated PAH has not declined in the current era of antiretroviral therapy. Moreover, the exact pathogenic mechanism that links HIV to PAH is not known.
Objective: Compared with general population, overwhelming percent of people with HIV are cigarette smokers. Therefore, the objective of this study is to determine whether cigarette smoking (CS) disproportionately impairs the pulmonary artery endothelial cell (PAEC) function and increases the risk of HIV-PAH.
Hypothesis: Studies have shown that the circulating HIV-1 viral accessory protein, Negative factor (Nef), binds to the host C-X-C motif chemokine receptor 4 (CXCR4) on endothelial and other cells. We hypothesized that CS increases CXCR4-Nef interaction, which results in the downstream impairment of endothelial nitric oxide synthase (NOS3) dependent vasodilation and the development of HIV-PAH.
Methods: Smokers and non-smokers with and without HIV-1 infection were recruited at the University of Alabama at Birmingham HIV 1917 clinic. All HIV-positive patients were on ART and had low blood viral loads (20–500 copies/ml). General demographic characteristics were not significantly different between groups (age range 47–55 years; race distribution 50–77% African American). Plasma was separated from blood obtained from these individuals and endothelial cell function markers, nitrite/nitrate ratio (stable metabolic products of nitric oxide), cGMP and prostacyclin were measured in plasma. To determine the role of CS in Nef-CXCR4 interaction, human PAECs (HPAECs) were treated with recombinant Nef protein in the presence or absence of cigarette smoke extract (CSE) ex vivo, and CXCR4 levels and CXCR4 binding to Nef were measured. It was also determined whether Nef impaired NOS3 expression, plasma membrane translocation, posttranslational modification, and function in HPAECs and whether the pharmacological inhibition of CXCR4 by AMD3100 attenuated Nef signalling.
Results: HIV-positive smokers had significantly lower plasma levels of nitrite/nitrate, cGMP and prostacyclin compared with HIV-positive non-smokers or HIV-negative smokers, suggesting that smoking adversely effects endothelial function in HIV-positive individuals compared with HIV-negative individuals. Further, exposure to 2% of CSE increased CXCR4 protein levels in HPAEC and increased CXCR4-Nef interaction when these cells were treated with recombinant Nef. Exposure of cells to CSE and Nef also reduced plasma membrane expression of NOS3, and cellular nitrite/nitrate and cGMP levels. Treatment of cells with AMD3100 abrogated effect of Nef on cells.
Conclusions: The data suggests that CS dependent Nef/CXCR4 signalling is an important driver of endothelial dysfunction in HIV and CXCR4 inhibition can be a potential therapeutic target for HIV-PAH.
Abstract O14
Antiviral Therapy 2019; 24 Suppl 1:A21
Changes in bone mineral density over 2 years in men who have sex with men on tenofovir disoproxil fumarate-based HIV pre-exposure prophylaxis: longitudinal cohort data
J McAllister1, S Holliday1, R Richardson1, K Hesse1, S Comben1, A Carr1
1HIV/Immunology Unit, St. Vincent's Hospital, Sydney
Objectives: Tenofovir disoproxil fumarate (TDF)-based HIV pre-exposure prophylaxis (PrEP) can reduce bone mineral density (BMD) by 1-2% or more over 12 months. Minimal longer-term data are available.
Methods: Men who have sex with men (MSM) initiating daily TDF-emtricitabine (FTC) PrEP through a PrEP demonstration project were offered BMD assessment by dual-energy X-ray absorptiometry (DXA) using a single scanner at baseline and after completing 1 and 2 years of PrEP. Hip data are the mean of left and right hip results. We excluded participants who ceased PrEP or who received antiresorptive therapy. Mean changes were assessed using paired t-tests.
Results: Of 185 men with baseline scans, 118 (64%) and 51 (43%) men were assessed at a median (IQR) of 420 (391-449) and 824 (776-885) days on PrEP. The mean (SD) ages and body mass index (BMI) of those men that had baseline BMD assessment compared with the 282 that did not was 35 (10) and 32 (9) years (P<0.05) and 25 (4) and 25 (4) kg/m2, respectively (P>0.05). Changes in BMD are shown in Table 1. No participant experienced a low trauma fracture during the study.
Conclusions: Over 12 months, a substantial proportion of MSM on daily HIV TDF-FTC PrEP lose ≥3% BMD at all measured sites over 24 months. There may be a plateau in loss after 12 months. Long-term studies of TDF-based PrEP in MSM are warranted.
Abstract O15
Antiviral Therapy 2019; 24 Suppl 1:A22
Limitations of FRAX equation for predicting low bone mineral density or bone loss progression among people living with HIV: the role of secondary causes of osteoporosis
P Vizcarra1, M Monsalvo1, M Fontecha1, JM del Rey2, M Rosillo2, JL Casado1
1Department of Infectious Diseases, Ramon y Cajal Hospital, Madrid, Spain; 2Department of Biochemistry, Ramon y Cajal Hospital, Madrid, Spain
Objective: We assessed the usefulness of the Fracture Risk Assessment (FRAX) tool to identify HIV-infected patients with low bone mineral density (BMD) and bone loss progression. We further evaluated the effect of secondary causes of osteoporosis and HIV-related factors on FRAX results.
Methods: Longitudinal study of 217 consecutive patients (mean, 45.8 years, women 24%) included after whole-body dual X-ray absorptiometry (DXA) scan. Low BMD and osteoporosis were defined as a femoral neck or spine T-score <2 and <2.5, respectively. The risk of major osteoporotic and hip fracture was calculated by FRAX equation, considering HIV as a secondary cause of osteoporosis, without/with femoral neck BMD data. The threshold for high-risk of fracture was defined as >3% for hip and >10% for lumbar spine.
Results: A low femoral neck and spine BMD was observed in 56% and 64% of patients, respectively. FRAX without BMD data did not identify any patient aged <75 at high risk of fracture. The inclusion of BMD data increased the estimated fracture risk (up to +221% in individuals with osteoporosis), though only two patients reached the current high-risk threshold for fracture. Moreover, the estimated fracture risk decreased in the oldest patients (−33%) and in individuals with normal BMD (−93%) after including BMD data. Conversely, FRAX results increased significantly with the inclusion of BMD data among individuals with classical and HIV-related secondary causes of osteoporosis (Figure 1). Notably, patients with lower BMD and higher FRAX score at baseline had less bone decline in a consecutive DXA scan (rho=0.21; P=0.008).
Estimated fracture risk by FRAX computed without and with bone mineral density (BMD; Abstract O15)
Conclusions: FRAX equation without BMD data does not identify HIV-infected patients with low BMD, delaying DXA assessment. After including femoral neck BMD, most patients remain below the current high-risk threshold for fracture. Different secondary factors, classical and HIV-related, affect fracture risk estimation by FRAX in this population.
Abstract O16
Antiviral Therapy 2019; 24 Suppl 1:A24
DXA scan versus FRAX score for the evaluation of fracture risk in a cohort of elderly people living with HIV
M Mazzitelli1,2, B Pereira1, T Muramatsu3, M Chirwa1, S Mandalia1, M Boffito1,4, A Milinkovic1, G Moyle1
1Research and Development Department, Chelsea and Westminster Hospital, London, UK; 2Medical and Surgical Sciences Department, ‘Magna Graecia’ University, Catanzaro, Italy; 3Department of Laboratory Medicine, Tokyo Medical University Hospital, Tokyo, Japan; 4Imperial College, London, UK
Background: Osteoporosis and fractures increase morbidity and mortality in people living with HIV (PLWH). EACS guidelines recommend routine assessment of fracture risk using FRAX, and dual-energy X-ray absorptiometry (DXA) scan only for those with FRAX over 10%, even though it can underestimate fracture risk in PLWH. Objective of our study was to evaluate level of concordance of DXA results (T score of the spine and of the femur) and FRAX in a population of PLWH over 50 years of age.
Methods: DXA scan results of PLWH who attended specialist over 50s clinic in Chelsea and Westminster Hospital between January 2009 and December 2018 were collected as well as demographic and clinical characteristics. FRAX was calculated using Sheffield algorithm. Mean and standard deviation were calculated. For univariate analysis Wilcoxon test was used.
Results: 744 patients were included, 92.9% were male, mean age of 56 ±5 years. Prevalence of osteoporosis (in the spine and/or in the femur) was 12.2% and osteopenia 63.7%. A statistically significant association was found between age and time of exposure to boosted protease inhibitors and osteoporosis in the femur (P<0.05). Two out of 744 cases FRAX major was >10% indicating need to perform DXA scan according to EACS guidelines (Table 1), while 90/91 (98.9%) patients with osteoporosis had a normal FRAX score. Even when FRAX score was calculated considering HIV as a risk factor of secondary osteoporosis and using BMD results, only 1.5% (11/744) patients had FRAX score >10%.
(Abstract O16)
Risk of Fracture with FRAX Major
DXA results (Spine) n (%)
DXA results (Femur) n (%)
Normal
Osteopenia
Osteoporosis
Normal
Osteopenia
Osteoporosis
Normal (<10%)
353 (47.4)
307 (41.4)
82 (11)
353 (47.4)
365 (49.2)
24 (3.2)
Perform DXA (10-20%)
1 (0.1)
0 (0)
1 (0.1)
0 (0)
1 (0.1)
1 (0.1)
Refer for treatment (>20%)
0 (0)
0 (0)
0 (0)
0 (0)
0 (0)
0 (0)
Risk of Fracture with FRAX Major calculated with HIV and BMD
DXA results (Spine)
DXA results (Femur)
Normal
Osteopenia
Osteoporosis
Normal
Osteopenia
Osteoporosis
Normal (<10%)
351 (47.2)
304 (40.9)
74 (9.9)
353 (47.4)
361 (48.5)
15 (2)
Perform DXA (10-20%)
3 (0.4)
3 (0.4)
9 (1.2)
0 (0)
5 (0.7)
10 (1.4)
Refer for treatment (>20%)
0 (0)
0 (0)
0 (0)
0 (0)
0 (0)
0 (0)
Discussion: Our results show that the FRAX score may not be a reliable screening tool for fracture risk in PLWH. Most patients with osteoporosis in our cohort had a normal FRAX score. These findings were maintained when BMD results and HIV infection were included in the FRAX calculation tool. Bone fracture screening in PLWH over 50 years of age requires optimization.
Abstract O17
Antiviral Therapy 2019; 24 Suppl 1:A25
Development and validation of a comorbidity index for people living with HIV and its ability to predict frailty and mortality
D De Francesco1, SO Verboeket2, E Verheij2, J Underwood3, E Bagkeris1, FW Wit2, A Winston3, P Reiss2, CA Sabin1, the POPPY study and the AGEhIV cohort study
1Institute for Global Health, UCL, London, UK; 2Department of Global Health and Division of Infectious Diseases, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands; 3Division of Infectious Diseases, Imperial College London, London, UK
Objectives: Despite the increasing prevalence of multi-morbidity in people living with HIV (PLWH), there is no tool designed specifically for PLWH to assess overall comorbidity burden. We developed and externally validated a comorbidity burden index (CBI), specific to PLWH, assessing its cross-sectional association with health status and ability to predict mortality and frailty.
Methods: We developed the CBI deriving weights for each of 65 comorbidities and their pairwise interactions from age-adjusted regression coefficients reflecting the independent association with self-reported physical health in PLWH enrolled in the POPPY (development) cohort. Predictive performance of the CBI were compared against the comorbidity count and the VACS index in the AGEhIV (validation) cohort. Spearman's correlation and the C-statistic assessed associations of indices with physical/mental health (SF-36), adapted Fried frailty phenotype prevalence and 4-year incidence, and 6-year all-cause mortality. These were compared across indices using the Steiger's and DeLong tests, as appropriate.
Results: The development and validation cohorts included 1,073 (85% males, 16% Black Africans, median [IQR] age of 52 [47–59] years) and 598 (88% males, 14% Black Africans, median [IQR] age of 53 [48–59] years) PLWH, respectively. Of the three indices, the CBI demonstrated the strongest associations with physical and mental health (Table 1); these associations were significantly stronger than those of the VACS index (both P-values <0.001) but not of those of the comorbidity count (P=0.08; P=0.16). At baseline, 11.4% of PLWH were frail; frailty incidence and death rate were 19.5/1,000 and 12.0/1,000 person-years, respectively. Cross-sectionally, the CBI showed a stronger association with frailty than either the VACS index (P=0.02) or the comorbidity count (P=0.27). Whilst prospective associations with frailty development and mortality were strongest for the comorbidity count, the difference with associations of the CBI were not significant (P=0.55 and P=0.12, respectively).
(Abstract O17)
Table: Association of the CBI, comorbidity count and VACS index with patient-reported physical and mental health, frailty, frailty development and mortality in the validation cohort with p-values comparing the associations of the comorbidity count and VACS index with those of the CBI.
Index
Physical health
Mental health
Frailty
Frailty development
Mortality
rho (95% CI)
p vs. CBI
rho (95%CI)
p vs. CBI
C-statistic (95%CI)
p vs. CBI
C-statistic (95% CI)
p vs. CBI
C-statistic (95% CI)
p vs. CBI
CBI
−0.34 (−0.41, −0.26)
−0.18 (−0.26,-0.10)
0.73 (0.66, 0.79)
0.62 (0.52, 0.72)
0.66 (0.56, 0.75)
Comorbidity count
−0.30 (−0.38, −0.22)
0.08
−0.15 (−0.23,-0.07)
0.16
0.71 (0.63, 0.78)
0.27
0.64 (0.54, 0.74)
0.55
0.71 (0.62, 0.79)
0.12
VACS index
−0.07 (−0.15, 0.02)
<0.001
0.10 (0.02, 0.19)
<0.001
0.63 (0.56, 0.70)
0.02
0.55 (0.44, 0.66)
0.32
0.67 (0.56, 0.77)
0.84
Note: for physical and mental health scores, higher scores indicate a more favourable health state
Conclusions: The proposed CBI, specifically developed in PLWH showed strong associations with quality of life, frailty and mortality when externally validated. These findings justify support the construct validity of the CBI and its use when adjustment for comorbidity is needed and when evaluating the effectiveness of interventions.
Abstract O18
Antiviral Therapy 2019; 24 Suppl 1:A26
In vitro modelling of the therapeutic impact of statins and ApoA-I mimetics on atherogenesis in chronic treated HIV
E Ritou1, T Kelesidis1
1David Geffen School of Medicine at University of California - Los Angeles
Objectives/aim: The mechanisms that drive HIV-related atherosclerosis (CVD) in chronic treated HIV remain unclear. Serum factors (such as bioactive lipids) from HIV+ individuals on potent antiretroviral therapy (ART) may drive atherosclerosis. Statins may have a favourable impact on CVD in chronic treated HIV but may be inadequate as single therapeutic strategy. ApoA-I peptides (such as 4F, 6F) mimic HDL, bind oxidized lipids and endotoxin and attenuate proatherogenic mechanisms such as monocyte/macrophage (M/M) chemotaxis. The 6F was expressed as a transgene in tomatoes (Tg6F) and reduced CVD in mice. Tg6F can be translated to human diet. Given that preclinical data are needed to assist efforts to bring Tg6F in the clinic, we used an established model of atherogenesis to assess ex vivo the therapeutic impact of statins and Apo-AI mimetics on early mechanisms of atherogenesis.
Methods: Our in vitro model of atherogenesis can dissect the impact of HIV-plasma on key mechanisms of early atherogenesis such as monocyte chemotaxis and monocyte-derived foam cell formation (MDFCF). Freshly isolated peripheral blood mononuclear cells (PBMCs) from healthy donors (n=6) were added to tumour necrosis factor-activated human umbilical vein endothelial cells monolayers (HUVECs) on type I fibrous collagen gels to transmigrate (% reverse migration) and form foam cells in the presence of pooled plasma, atorvastatin (50 and 500 μM) and/or 4F (10–100 μg/ml) as previously described (PMID: 28926407). Pooled plasma was isolated from healthy participants (18–40 years old) and HIV+ males (40–60 years old) with no known inflammatory comorbidities other than HIV or risk factors for CVD and on stable potent ART. Flow cytometry assessed MDFCF (ΔMFI BODIPY of CD33+ macrophages inside the gel: fluorescence intensity of BODIPY compared with negative staining control). Paired t-test was used for statistical comparison within the same donor.
Results: When media-containing HIV+ compared with HIV- plasma was added to HUVECs, a significantly increased proportion of monocytes underwent transendothelial migration (TEM; median migrated cells 16 versus 4.9%, respectively) and CD33+ macrophages inside the collagen gel had increased lipid content per cell (median ΔMFI BODIPY 673 versus 342, respectively; P<0.05; Figure 1). In the presence of HIV-plasma, both atorvastatin (at both 50 and 500 μM) and 4F (at both 10 and 100 μg/ml) attenuated TEM of M/M and MDFCF (P<0.05 for all comparisons). The combined treatment with 4F (100 μg/ml) and atorvastatin (50 μM) reduced TEM compared with 50 μM atorvastatin alone (P<0.05).
(Abstract O18)
Conclusions/discussion: HIV plasma from patients on potent ART with no clinical CVD directly induces key mechanisms of early atherogenesis (TEM and MDFCF). Both atorvastatin and 4F attenuated the ex vivo proatherogenic effects of HIV plasma. The combination of statins and oral apoA-I mimetics can be a novel therapeutic strategy for atherosclerosis in chronic treated HIV and needs to be further validated in vivo.
Abstract O19
Antiviral Therapy 2019; 24 Suppl 1:A27
Could coronary artery features during acute coronary syndrome predict major cardiac events in people living with human immunodeficiency virus?
R Robert1, Y Cottin1, V Potard2, M Mary-Krause2, S Lang3, M Chauvet3, S Ederhy3, L Dufour-Soulat3, Y Ancedy3, S Adavane-Scheuble3, P Nhan3, P-M Girard4, D Costagliola2, A Cohen3, F Boccara3,5, the PACS-HIV (Prognosis of Acute Coronary Syndrome in HIV-infected patients) investigators
1Cardiology Department, University Hospital, PEC 2, Univ. Bourgogne Franche-Comté, Dijon, France; 2INSERM, Sorbonne Université, Institut Pierre Louis d'Épidémiologie et de Santé Publique (IPLESP), Paris, France; 3AP-HP, Hôpitaux de l'Est Parisien, Hôpital Saint-Antoine, Department of Cardiology, Faculty of Medicine, Sorbonne Université, Paris, France; 4Infectious Disease Department, AP-HP, Hôpitaux de l'Est Parisien, Hôpital Saint-Antoine, Faculty of Medicine, Sorbonne Université, Paris, France; 5National Institute of Health and Medical Research, INSERM, UMR_S 938, UPMC, Paris, France
Introduction: Patients living with human immunodeficiency virus (PLHIV) who undergo percutaneous coronary intervention (PCI) have a substantial risk of recurrent ischaemic events after ACS.
Hypothesis: Our hypothesis was that angiographic features and SYNTAX scores could predict recurrent ischaemic events in PLHIV.
Methods: We conducted a nested case-control study from the PACS-HIV study (prospective, multicentre study on the prognosis of ACS in HIV+ in France) comparing coronary angiography features between PLHIV and matched HIV- patients (age, sex and type of ACS) with a first ACS undergoing PCI. Coronary angiograms at baseline were off-line analysed blinded to the HIV status.
Results: The cohort included 60 PLHIV and 107 HIV-(median age 47 years [41–56], male sex 95%). Cardiovascular risk factors were well balanced between the two groups (high tobacco consumption 63%). Illicit drug use was more frequent in PLHIV (20% versus 5%, P=0.006). STEMI was the predominant type of ACS (55%) follows by NSTEMI (23%) and unstable angina (22%). In terms of the number of vessel disease (VD) there was no significant difference between PLHIV and HIV- subjects with predominant 1 VD (48% versus 43%), 2VD (33% versus 33%), 3 VD (15% versus 12%), P trend =0.86. Of note, PLHIV had a higher rate of coronary artery aneurysms as compared with HIV- (15% versus 4%; P=0.009). PLHIV had higher number of significant coronary lesions (median 2 [1–3] versus 1 [1–2]; P=0.04). However, the initial SYNTAX score was not different between the two groups (12.4 ±9 versus 11.5 ±7.8 in PLHIV and HIV- respectively; P=0.42). By contrast, the residual SYNTAX score after PCI was significantly higher in PLHIV (4.7 ±7 versus 2.7 ±4.9; P=0.04). The rate of MACCE was not different between the two groups after 36 months of follow-up. However, a trend toward a higher rate of recurrent ACS was observed (HR: 3.80; 95% CI: 0.96, 15.00; P=0.06). Neither angiographic features nor the SYNTAX initial or residual score were associated with MACCE or recurrent ACS.
Conclusions: PLHIV had higher numbers of significant coronary lesions and aneurysms with higher residual SYNTAX score after PCI as compared to HIV-. However, the SYNTAX score was not associated with MACCE or recurrent ACS after a long-term follow-up.
Abstract O20
Antiviral Therapy 2019; 24 Suppl 1:A28
Risk factors for incident hypertension within 1 year of initiating antiretroviral therapy (ART) among people with HIV
TJ Moore1, DM Long2, GA Burkholder3, A Willig3, C Wyatt4, P Muntner1, ET Overton3
1Department of Epidemiology, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Biostatistics, University of Alabama at Birmingham, Birmingham, AL, USA; 3Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Medicine, Duke University, Durham, NC, USA
Background: While hypertension (HTN) is a common comorbid condition among persons with HIV and a contributor to cardiovascular disease and CKD risk, the association of antiretroviral therapy (ART) with the risk for HTN remains unclear. We examined the prevalence and risk factors for hypertension in a cohort of ART-naive participants initiating ART on randomized clinical trials through the AIDS Clinical Trial Group between 1999 and 2011.
Methods: We determined the prevalence of HTN among 4,617 treatment-naive PWH randomized to different ART regimens and followed in the AIDS Clinical Trials Group Longitudinal Linked Randomized Trials (ALLRT) study, and the incidence of HTN at 48 weeks among 3,809 participants who were normotensive at study entry, defined as having a systolic blood pressure (SBP) <140 mmHg, diastolic blood pressure (DBP) <90 mmHg, no diagnosis of HTN, and not taking any antihypertensive medications. We assessed the role of baseline factors, including randomized ART agents, in the development of HTN at 48 weeks using Poisson regression models. Incident HTN was defined as blood pressure ≥140/90, clinical diagnosis of hypertension, or receipt of antihypertensive medications.
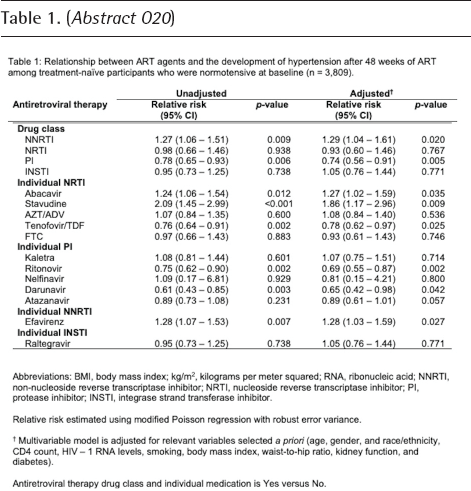
Results: At baseline, 808 participants (17.5%) were hypertensive and excluded from the analysis. After 48 weeks, 438 additional participants (11.5%) developed HTN. Receiving an NNRTI was associated with an increased risk of incident hypertension (adjusted relative risk [aRR] 1.29, 95% CI: 1.04, 1.61), while the risk was lower for PI use (aRR 0.74, 95% CI: 0.56, 0.91; see Table 1). Regarding specific ART agents, abacavir, stavudine and efavirenz were associated with an increased risk of developing hypertension (aRR: 1.27 [95% CI: 1.02,1.59], 1.86 [95% CI: 1.17,2.96] and 1.28 [95% CI: 1.03,1.59], respectively), while tenofovir disoproxil fumarate (TDF), ritonavir and darunavir were associated with a decreased risk (aRR: 0.78 [95% CI: 0.62,0.97], 0.69 [95% CI: 0.55,0.87] and 0.65 [95% CI: 0.42,0.98], respectively). Additionally, lower baseline CD4 count, older age, higher BMI, being male, Black race and current smoking were associated with an increased risk for developing hypertension.
(Abstract O20)
Table 1: Relationship between ART agents and the development of hypertension after 48 weeks of ART among treatment-naïve participants who were normotensive at baseline (n = 3.809).
Abbreviations: BMI, body mass index: kg/m2. kilograms per meter squared; RNA, ribonucleic acid; NNRTI, non-nucleoside reverse transcriptase inhibitor, NRTI. nucleoside reverse transcriptase inhibitor; PI, protease inhibitor: INSTI, integrase strand transferase inhibitor.
Relative risk estimated using modified Poisson regression with robust error variance.
Multivariate model is adjusted for relevant variables selected a priori (age. gender, and race/ethnicity. CD4 count, HIV- 1 RNA levels, smoking, body mass index, waist-to-hip ratio, kidney function, and diabetes).
Antiretroviral therapy drug class and individual medication is Yes versus No.
Conclusions: Findings suggest traditional factors, advanced HIV disease and certain ART agents contribute to the development of HTN after ART initiation. Strategies to address modifiable risk factors, such as smoking and obesity, can be employed to decrease the consequences of HTN. Future research will explore the effects of newer ART agents and the specific mechanisms by which specific ARTs contribute to HTN.
Abstract O21
Antiviral Therapy 2019; 24 Suppl 1:A29
The relationship between diabetes and depressive symptoms in men with or at risk for HIV
RC Basil1, TT Brown1, S Haberlen1, LH Rubin1, M Plankey2, J Becker3, JE Lake4, FJ Palella5, S Sarkar1
1Johns Hopkins University, Baltimore, MD; 2Georgetown University Medical Center, Washington, DC; 3University of Pittsburgh Medical Center, Pittsburgh, PA; 4University of Texas Health Sciences Center, Houston, TX; 5Northwestern University Feinberg School of Medicine, Chicago, IL
Objectives: To compare the prevalence of comorbid diabetes and depressive symptoms between men with (HIV+) and without (HIV-) HIV disease and to determine the associations between glycaemic control and depressive symptoms.
Methods: We conducted a cross-sectional analysis using data collected during a single semiannual visit (October 2017 to March 2018) from HIV+ and HIV- men participating in the Multicenter AIDS Cohort Study (MACS). The exposure of interest was glycaemic status, categorized as normal for fasting blood glucose (FBG) <100 mg/dl, prediabetes for FBG 100–125 mg/dl and type 2 diabetes (defined by self-report, report of diabetes medication use, or FBG ≥126 mg/dl for ≥2 consecutive visits prior to the current visit). Type 2 diabetes was further categorized as controlled (HbA1C <7.5%) or uncontrolled (HbA1C ≥7.5%). The primary outcome was elevated depressive symptoms, as defined by a Center for Epidemiologic Studies Depression Score (CES-D score) ≥16. A modified Poisson regression model with robust variance was used and adjusted for study site, age, race, education status, HIV-serostatus, body mass index, hypertension, dyslipidaemia, smoking, alcohol use, illicit drug use and depression treatment, which included current or prior antidepressant medication use or history of hospitalization for depression or consultation with a mental health professional. Interaction of glycaemic status and HIV-serostatus was tested. Stratification by depression treatment was conducted to determine whether glycaemic status was associated with suboptimal depression treatment. A model limited to HIV+ men was adjusted for HIV-specific variables, which included current CD4 lymphocyte count, detectable HIV viraemia and ART type.
Results: The study included 920 HIV+ men (mean age [sd] 55 [11] years) and 840 HIV- men (mean age [sd] 61 [12] years). HIV+ men had greater prevalence of both elevated depressive symptoms (28.5% versus 20.1% among HIV- men; P<0.001), and diabetes (12.83% versus 11.31%; P=0.330). The concomitant prevalence of diabetes and elevated depressive symptoms did not differ by HIV-serostatus (P=0.516). Compared with normal glycaemic status, the adjusted prevalence ratios of elevated depressive symptoms were 1.06 (95% CI 0.82, 1.37) in men with prediabetes, 1.21 (95% CI 0.89, 1.65) in men with controlled type 2 diabetes and 1.55 (95% CI 1.06, 2.28) in men with uncontrolled type 2 diabetes (Table 1). These associations did not differ by HIV-serostatus (P=0.59). Uncontrolled type 2 diabetes was associated with elevated depressive symptoms among participants with a history of depression treatment but not for those without a history of depression treatment. HIV-specific variables were not associated with elevated depressive symptoms.
(Abstract O21)
Table 1. Prevalence Values and Prevalence Ratios of Elevated Depressive Symptoms by Glycemic Status
Prevalence of Elevated Depressive Symptoms, n (%)
Prevalence ratio (95% CI)
P value
Glycemic Status
Normal
258 (23%)
REF
Prediabetes
74 (25%)
1.06 (0.82, 1.37)
0.677
Type 2 diabetes, controlled
42 (30%)
1.21 (0.89,1.65)
0.231
Type 2 diabetes, uncontrolled
22 (40%)
1.55 (1.06, 2.28)
0.024
Adjusted for age, study site, race, education, body mass index, HIV-serostatus, hypertension, dyslipidemia, alcohol use, smoking, illicit drug use, and depression treatment.
Conclusions: Both controlled and uncontrolled diabetes were independently associated with depressive symptoms, regardless of HIV serostatus. Longitudinal studies are needed to examine whether the relationship between glycaemic status and incident elevated depressive symptoms differs by HIV serostatus.
Abstract O22
Antiviral Therapy 2019; 24 Suppl 1:A31
Risk for incident diabetes is greater in pre-diabetic men with HIV than without HIV: the Multicenter AIDS Cohort Study
L Slama1,3, B Barrett2, A Abraham2, FJ Palella Jr3, L Kingsley4, JP Viard1, JE Lake5, TT Brown2, the Multicenter AIDS Cohort Study (MACS)
1APHP, Hotel Dieu Hospital, Infectious Diseases Unit F-75004, UPMC Paris 6, France; 2Johns Hopkins University, Baltimore, MD, USA; 3Feinberg School, Northwestern University, Chicago, IL, USA; 4University of Pittsburgh, School of Medicine, Pittsburgh, PA, USA; 5Univeristy of Texas, Houston, TX, USA
Background: Abnormalities in glucose metabolism contribute to the pathogenesis of ageing-related comorbidities in people with HIV (PWH). Hyperglycaemia below the diabetic range has been termed pre-diabetes mellitus (pre-DM) and may be more common in PWH compared with those without HIV. It is unclear whether the progression from pre-DM to DM differs by HIV serostatus.
Methods: Fasting glucose (FG) was measured at each semi-annual visit among men in the Multi-center AIDS Cohort Study (MACS) since April 1999. Men who had confirmed pre-DM, defined as an FG 100–125 mg/dl (baseline visit), were included. Men with prevalent DM at the baseline visit were excluded. Incident DM was defined as an FG ≥126 mg/dl, confirmed at a subsequent visit with anti-DM medication use or a second FG ≥126 mg/dl; self-reported DM, confirmed at a subsequent visit with anti-DM medication use or two FG ≥126 mg/dl; or report of anti-DM medication use at a visit. We used binomial transition models to determine whether the progression from pre-DM to DM from one visit to the next differed by HIV serostatus, after adjustment for age, race/ethnicity, body mass index (BMI) and hepatitis C virus (HCV) infection.
Results: Between 1999 and 2018, 1,548 men (772 with HIV [MWH], 776 men without HIV) with pre-DM were included. At baseline, MWH were younger (median 48 versus 51 years; P<0.01), had lower BMI (median 25 versus 27 kg/m2; P<0.01), were more likely to be non-White (44% versus 28%; P<0.01), and were more likely to be HCV-infected (9% versus 5%; P<0.01) than men without HIV. Over a median of 12 years of follow-up (Q1, Q3 8, 14), 22% (166/772) of pre-DM MWH and 22% (169/776) of pre-DM men without HIV developed DM. In adjusted analyses, the probability of developing DM among men with pre-DM was 40% (95% CI: 10%, 80%) higher among MWH than men without HIV (P=0.02).
Conclusions: Among men with pre-diabetes, HIV serostatus was associated with increased risk of incident diabetes after adjustment for competing DM risk factors. Given the increased risk, diabetes prevention strategies in PWH may be particularly effective and should be investigated.
Abstract O23
Antiviral Therapy 2019; 24 Suppl 1:A32
Comparing a risk score against physiological markers for predicting diabetes incidence in HIV+ individuals
KI Galaviz1, MF Schneider2, PC Tien3, MK Ali1, K Althoff2, T Brown2
1Emory University, Atlanta, USA; 2Johns Hopkins University, Baltimore, USA; 3University of California, San Francisco, CA, USA
Purpose: To compare the performance of a clinical diabetes risk score with physiological markers for predicting diabetes incidence in HIV+ and HIV- individuals.
Methods: We determined 10-year diabetes incidence (defined as self-reported diabetes medication use) in HIV+ and HIV- participants from the Women's Inter-agency HIV Study and the Multicenter AIDS Cohort Study. For each participant, we obtained baseline values for the Finnish Diabetes Risk Score (FINRISC), Homeostasis Model Assessment for Insulin Resistance (HOMA-IR), HOMA for β-cell function (HOMA-β), and triglycerides/HDL cholesterol ratio (TG/HDL). Discrimination of each model was assessed using the Harrell C-statistic. Calibration was assessed by comparing the observed versus the predicted cumulative probabilities of developing diabetes (determined from 1-Kaplan-Meier) in each tertile of the distribution.
Results: We included 2,499 men (1,285 HIV+ and 1,214 HIV-, median age =44 years, 60% non-Hispanic White, 25% non-Hispanic Black) and 2,408 women (1,812 HIV+ and 596 HIV-, median age =41, 12% non-Hispanic White, 62% non-Hispanic Black). Over 10 years of follow-up, 10% of HIV+ men, 9% of HIV- men, 11% of HIV+ women, and 12% of HIV- women developed diabetes. FINRISC had the best discrimination, though it performed better in HIV- participants (men c=0.74 [95% CI 0.69,0.78], women c=0.75 [0.70,0.80]) than in HIV+ participants (men c=0.68 [0.62,0.73]), women c=0.70 [0.66,0.74]). HOMA-IR discrimination was similar by HIV status but better in men (HIV+ c=0.70 [0.65,0.75]), HIV- c=0.72 [0.67,0.77]) than in women (HIV+ c=0.65 [0.61,0.69], HIV- c=0.67 [0.60,0.74]). TG/HDL and HOMA-β had poor discrimination (c<0.7 and <0.6, respectively). Regarding calibration, FINRISC underestimated risk among HIV- men in the highest risk tertile, while HOMA-IR and TG/HDL underestimated risk among all participants in the highest risk tertiles. HOMA-β was well-calibrated.
Conclusions: In HIV+ men, FINRISC predicted incident diabetes similarly to physiological markers. In HIV+ women, FINRISC was superior.
Abstract O24
Antiviral Therapy 2019; 24 Suppl 1:A33
Restless legs syndrome and health-related quality of life in HIV: results from the POPPY Sleep Substudy
KM Kunisaki1,2, D DeFrancesco3, C Sabin3, A Winston4, PWG Mallon5, J Vera6, F Post7, I Williams3,8, E Bagkeris3, N Doyle4, W Khalil1,2, S Redline9,10,11, the Pharmacokinetics and Clinical Observations in People Over Fifty (POPPY) Study
1Minneapolis VA Health Care System, Minneapolis, USA; 2University of Minnesota, Minneapolis, USA; 3University College London, London, UK; 4Imperial College London, London, UK; 5University College Dublin, Dublin, Ireland; 6Brighton and Sussex University Hospital, Brighton, UK; 7Caldecot Centre, King's College Hospital, London, UK; 8Mortimer Market Centre, Central and North West London NHS Foundation Trust, London, UK; 9Brigham and Women's Hospital, Boston, USA; 10Beth Israel Deaconess Medical Center, Boston, USA; 11 Harvard Medical School, Boston, USA
Purpose: Restless legs syndrome (RLS) is a sleep disorder characterized by leg dysasthesias, typically relieved by movement, with sequelae that may include daytime sleepiness, mood problems, functional impairments and decreased work productivity. RLS often responds to dopaminergic drugs, suggesting a central nervous system (CNS) aetiology. Given the high burden of sleep symptoms and CNS disorders in persons with HIV (PWH), we evaluated RLS prevalence and associations with health-related quality of life (QoL) in PWH and lifestyle-similar HIV-negative controls.
Methods: A subset of POPPY participants (PWH ≥50 y/o, PWH <50 y/o and HIV-negative controls ≥50 y/o) completed standardized RLS and QoL questionnaires. RLS was defined using international consensus guideline criteria. Sleep-related QoL was assessed with PROMIS questionnaires. Physical and mental health QoL was evaluated with SF-36 scores. Logistic regression was used to compare RLS prevalence in PWH and controls. QoL in those with and without RLS were compared using Wilcoxon tests.
Results: Of 435 participants (220 older PWH [median age 60 years], 99 younger PWH [45 years] and 116 older HIV-negative [60 years]), RLS criteria were met by 77 (35%), 33 (33%) and 25 (22%) of the groups, respectively. In analyses adjusted for age, sex and race, PWH were more than twice as likely to meet RLS criteria than controls (aOR 2.4 [1.4 to 4.1]; P=0.002). Of the 110 PWH with RLS (55% of whom reported symptoms at least 2–3 times/week), only 7 (6%) reported a diagnosis of RLS and 3 (3%) reported a history of RLS medication treatment. PWH with RLS reported worse sleep-related QoL and poorer physical and mental health QoL compared with PWH without RLS (Table 1; all P-values <0.001).
(Abstract O24)
Table: Differences in patient-reported questionnaire scores among those with and without restless legs syndrome (RLS) as assessed by International Restless Legs Study Group criteria#. For PROMIS questionnaires, higher scores indicate more disturbance or impairment. For SF-36 measures, lower scores indicate worse quality of life.
Answered yes to all of the following questions. 1) At any time in the day or night, do you have unpleasant sensations in your legs (such as unpleasant crawling or creeping sensations in the feet. calves or thighs) combined with an urge or need to move your legs?’. 2) Do they occur mainly or only at rest?. 3) Do they improve with movement?. and 4) Are they worse in the evening or night than in the morning?’
Conclusions: Among PWH, RLS is common, associated with health-related QoL impairments, and rarely diagnosed or treated. Further research is needed to understand risk factors for RLS and the effects of RLS treatment.