
Abstract
Radiation therapy can be challenging for children and youths, regarding medical and psychosocial aspects. Music therapy is increasingly recognized as effective and appreciated biopsychosocial support in medical settings, but music therapy in pediatric radiation oncology is sparse. This exploratory pilot study aimed to explore possibilities and experiences of a music therapy service for children and youths undergoing radiation therapy. The study included quantitative and qualitative data; patients’ and parents’ self-reported scores on satisfaction with music therapy, interdisciplinary experiences and collective reflections obtained through focus group interviews, and the distribution of predicted and actual use of anesthesia for the patients during treatment. Descriptive statistics were used to report on numeric and categorical variables, and qualitative content analysis was used for the interviews. The results showed that patients and parents were highly satisfied, and more patients than predicted completed the treatment without anesthesia. Important factors were identified regarding the psychosocial assessment of patient needs, timing, interdisciplinary collaboration, and possible redistribution of resources. The study demonstrated that music therapy was well received by the patients and likely had a positive impact on the overall treatment quality. Including music therapist in interdisciplinary teams may positively impact individual adaptation of treatment and the use of resources.
Introduction
Radiation therapy is used as a treatment for children with a variety of cancer diagnoses. For many patients, radiation therapy can be experienced as unsafe and stressful, with consequences for procedure coping, the use of anesthesia, nutrition, and general treatment experience (Scott et al., 2016) and the need for systemic patient and family support is recognized (Patel et al., 2021). Music therapy (MT) is increasingly used for biopsychosocial support in medical settings and implemented as supportive treatment at many pediatric hospitals around the world, so also at Oslo University Hospital (Norwegian: Oslo universitetssykehus, hereafter OUS). So far, MT has not been established as part of the service for children and youths undergoing radiation therapy at OUS due to limited resources. At the national level, we expect an increased number of young patients undergoing radiation therapy in the coming years, due to two new proton therapy centers that will offer treatment to patients who are currently sent abroad. This study was initiated to explore the needs and possibilities for music therapy as part of the service for this patient group. It aims to inform clinical practice development and further research based on existing knowledge, here adapted in a Scandinavian healthcare setting. There is also a need for more practice and research in this field internationally.
Radiation therapy for children and youths
A sequence of radiation therapy (6–33 sessions) is divided into daily treatment fractions (5–40 minutes) 5 days a week, usually given as an outpatient service. To ensure ray precision during treatment, the patient must lie still in the same position each time. For treatment of the head or neck area, an individually adapted mask is made for the patient, fixated to the bench for each treatment (Kreftlex, 2024 [2016]). Use of radiation mask implicates a risk of anxiety, suggesting a need for individual patient support for preparation and coping strategies (Nixon et al., 2018). Due to the use of high-energy X-ray radiation during treatment, the patient is alone in the room, screen-monitored by the staff. Children might find it challenging to lie still and alone, with possible consequences of stress responses and feelings of unsafety, so anesthesia is often used to ensure immobilization. When using anesthetic for these treatments at OUS, the standard is to use sedation for the patient to sleep (propofol, supplied with fentanyl, remifentanil or alfentanil if needed due to patient discomfort). The patient is spontaneously breathing with supplemented oxygen by nasal prongs and monitored as required. In rare cases general anesthesia is needed for a more protected airway, and a LMA (laryngeal mask airway) (LMA) or ETT (endotracheal tube) is used. The drugs of choice will be the same, but possibly with more supportive drugs added to maintain adequate heart rate, reduce saliva production, reduce pain, or maintain fluids/caloric need. Patients managing without anesthesia receive the treatment without medication.
Repeated use of general anesthesia exposes children to rare but serious risks and potentially harmful long-term side effects and should be prevented when possible (Robinson et al., 2022). It limits the flexibility in the daily operation of the clinic, and increases the costs of treatment (Scott et al., 2016). The demand for fasting before anesthesia can be challenging for the family, and harmful for children with nutritional problems.
Previous findings show that pediatric cancer patients in radiation therapy benefit significantly from psychosocial support like educative teaching, parental involvement, and various coping techniques (Boik and Hall, 2020) and that play interventions with Child Life Specialists (CLS) can reduce their need for anesthesia (Scott et al., 2016). The CLS practice has relevant similarities with MT in pediatrics.
Music therapy in pediatrics
MT with hospitalized children and youths at OUS is based on a biopsychosocial approach (Dileo, 2016), to meet various needs of patients and families. MT can contribute to symptom relief, support emotional expression and processing, provide opportunities for choice, control, and mastery, as well as facilitate positive experiences (Blichfeldt-Ærø and Leinebø, 2017; Bradt, 2013; Cole et al., 2024 Lindenfelser, 2013). Music therapists may follow patients across wards, representing relational continuity in the hospital routine often perceived as fragmented (Leinebø and Aasgaard, 2016). In line with the biopsychosocial perspective and theories of stress and pain (Kozlowska et al., 2020; Melzack and Katz, 2004), patients’ experiences and coping during medical procedures are multidimensional and contextual. Clinical experiences suggest that improving routines for painful or frightening procedures with a focus on the individual child’s conditions and needs can create more predictability and a sense of control for the child. If the child is well prepared before the procedure carries out, they will be able to experience a feeling of control. Several studies have shown that preparation using hypnosis or cognitive behavioral therapy interventions reduces anxiety, helplessness, and stress during medical procedures. In this regard, it is useful to use different play materials to prepare children for painful procedures (Gjems and Diseth, 2011). Based on the human innate relational and communicative musicality, music therapy is considered a powerful approach to psychoeducational support and neurobiological regulation (Trevarthen and Malloch, 2000).
Music therapy as procedural support may be defined as “the use of music and aspects of the therapeutic relationship to promote healthy coping and decrease distress in individuals undergoing medical procedures” (Ghetti, 2012: 6). Dynamic forces in MT can be used as modulating factors for procedure experience and coping, and the need for individually tailored, ongoing adjustments of procedure support is emphasized (Ghetti, 2012; Giordano et al., 2024). A medical procedure involves an interplay of factors related to the child, the context, the music therapist, the music, the procedure, family members, and other healthcare workers. Before a procedure, a preparation and assessment process provides a mutual ground for involving patient, family, and staff to define clear roles and expectations for the procedure (Steinhardt and Ghetti, 2020). The music therapist should also have some familiarity with the medical procedure (Mondanaro, 2013). During a preparation session, the music therapist builds a relation with the patient and family and tries out various music-facilitated coping strategies. In collaboration with the music therapist, the patient plans how she or he would like to use music during the procedure. A range of music therapy interventions can be used for procedure support, including both receptive and expressive interventions. Receptive music therapy interventions can be patient or therapist-selected music listening for refocusing, music-facilitated psychoeducation, music entrainment, tension release, or music sedation. Expressive music therapy interventions can be improvisation, singing and playing on different instruments, creating soundscapes, or tension release through drumming. For long-term procedures or repeated procedures, songwriting might be a current intervention (Mondanaro, 2013).
Music therapy in radiation therapy
On a worldwide basis, MT has a recognized role in oncology and is recommended a part of standard practice (Cole et al., 2024; Facchini and Ruini, 2021; Nardone et al., 2020), but its application in radiation therapy is understudied (Nardone et al., 2020), mainly referring to adult patients (Rossetti et al., 2017), and only two studies on pediatric patients.
In the first report on MT in a pediatric radiation therapy setting, patients and families were encouraged to “play” with a music therapist next to the waiting area, to provide a means of communication, self-expression, and creativity (O’Challagan et al., 2007). Through individual case reports, the study shows a successful use of MT as a non-pharmacological anxiolytic in pediatric radiation therapy inducing stress relief, physical and psychosocial improvements, and facilitation of clinical communication.
A mixed methods RCT involving 11 pediatric patients undergoing radiation therapy (Barry et al., 2010) investigated the use of a MT CD created by the patients and music therapist, using interactive computer-based software. Results showed no significant differences between groups on distress, efficacy, or coping strategies, yet MT was considered fun, supportive, and helpful for both patients and families, providing distraction, and making patients more open to psychosocial support.
Based on the abovementioned, an exploratory pilot study was conducted on music therapy for children and youths undergoing radiation therapy, exploring the impact and experiences both from a patient/parent and an interdisciplinary perspective. The following research questions were formulated:
What were the patients’ and parents’ experiences with music therapy?
What were the interdisciplinary team’s experiences with music therapy?
What was the distribution of predicted, and actual use of anesthesia during radiation treatment for patients receiving music therapy?
Methods
Design and ethics
This explorative pilot study included quantitative and qualitative data focusing on patient/parents’ experiences, interdisciplinary staff perspectives, and patients’ use of anesthesia. Although mixed data was collected, mixed methods was not fully applied within this limited study scope. The study is regarded primarily as explorative and descriptive, aiming at increased understanding of the possibilities and limitations of music therapy for the target population, but does not aim at investigating effect outcomes with generalized conclusions.
Ethics was performed according to national ethical guidelines (CREO, 2022), regulations, and approvals. The study was approved by the Department of Ethics at Oslo University Hospital (number 27/07301). Reporting of the music therapy intervention was guided by Robb et al. (2025) (S1). The study was funded by Fondsstiftelsen and Barnestiftelsen at Oslo University Hospital.
Participants
All patients 0–18 years (25 patients) referred to radiation treatment at OUS April 2021–July 2022 were screened for participation by the medical doctor or the nurse coordinator and referred to MT. Inclusion criteria were patients 0–18 years, with a diagnosis and treatment schedule including radiation therapy at OUS. Parents had to understand Norwegian or English, written and spoken. Exclusion criterion was severe hearing impairment. All patients within the study period were included regardless of the need for anesthesia.
Nineteen patients were asked to participate in the study. Written and verbal information about the study and invitation to participate was given by the first writer, also music therapist and project leader. Six patients declined for personal and/or medical reasons, and 13 patients were enrolled, signing a consent form. Participation was voluntary, and participants could withdraw at any time. No negative side effects were expected from participating in the project.
The interdisciplinary project team was formed in an early study phase, including radiation therapist, radiation nurses, oncologist, anesthesiologists, nurse anesthetist, and the music therapist, who is also the first writer. Collaborative interdisciplinary dialogues were integrated into all phases of the study, both formal and informal, as important elements in study planning, service development, implementation, and evaluation.
The music therapy intervention
The study took place at two different locations at OUS (1 and 2): Preparations including MT at location 1 and/or 2 as required, and the radiation treatment at location 2. The MT intervention was based on the same methods as established at OUS, now adapted to a new patient group and setting. All music therapy sessions were delivered by the same certified music therapist, with more than 10 years of experience in pediatric practice. Through facilitated MT interventions, the music therapist aimed to strengthen the patients’ resilience, promoting safety and meaningful experiences before and during radiation therapy, following three phases (Table 1).
Phases of the Music Therapy service.
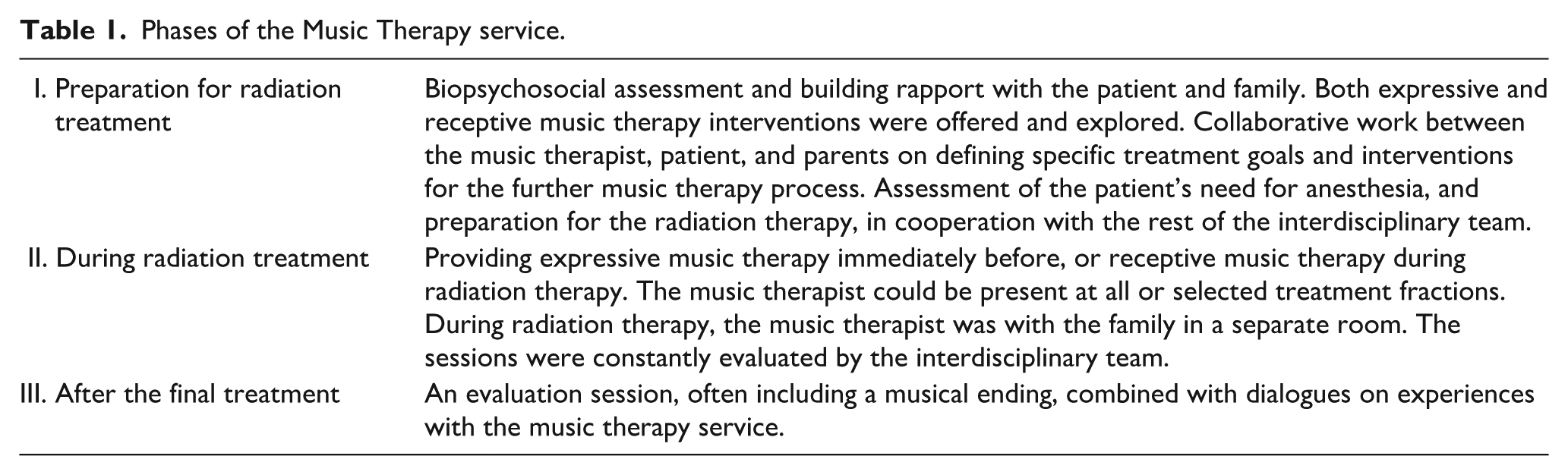
The number of MT sessions was adapted to the patient’s needs and treatment protocol. The duration of sessions was 10–30 minutes offering expressive and/or receptive MT to meet diverse patient needs independent of age and need for anesthesia. Expressive MT included improvisation, singing, and playing using percussion instruments such as mini-maracas, frame drums, and castanets. The music therapist often played the guitar. Also, an item such as a toy or animal figure could be used to catch and/or maintain attention. The music was age-appropriate and culturally relevant, based on patients’ preferences to elicit optimum engagement, often including traditional and/or popular songs. As appropriate, parents, siblings, and staff were encouraged to participate in the sessions, playing an instrument or singing. The sessions ahead of treatment took place in a secluded waiting area allowing individual therapy, or inside the treatment room for patients needing procedural support during anesthesia induction.
Receptive methods included listening to recorded music during treatment for patients who did not need anesthesia during radiation treatment. The chosen music was playlists from Spotify based on patient preferences, or specially composed music imagery narratives for children (Sanfi et al., 2021) played from digital devices (iPad/mobile phone) and a Bluetooth loudspeaker or the integrated loudspeaker system. Parental support while the patient received the radiation treatment was also an important part of the MT service.
Data collection
Data on patients’ and parents’ satisfaction and experiences with the MT service during the radiation treatment were obtained through a questionnaire based on 1–5 Likert-type scales (Stange et al., 2018) and open-ended questions allowing for additional responses, developed by the first and third authors, available as supplemental data (S2). After the final radiation treatment, the paper questionnaire was handed to the patient/parents by the music therapist, answered in privacy, and returned in a sealed envelope. Patients > 8 years old completed the questionnaire themself. For younger patients, the parents completed it.
Interdisciplinary experiences and reflections on the MT service were collected through two focus group interviews, which constituted the data from the interdisciplinary team. The first interview was carried out 6 months after the inclusion started, and the second after study completion. The number of interview participants relied on each team member’s opportunity to participate at the time in question, but it was ensured that all relevant professions were represented. As part of, and in line with the emphasis on continuous interdisciplinary collaboration and dialogue, the music therapist was also included. The interviews were semi-structured, allowing for dialogues on predetermined study issues, and new insights generated by the group. The team was asked to share their experiences and thoughts on the MT service related to three main areas: (1) Interdisciplinary collaboration; inclusion of patients, logistics, communication, and roles. (2) Influence of the MT service as part of the radiation therapy treatment on staff and patients/families. (3) Open feedback: experiences, observations, and thoughts related to the project. The team was especially encouraged to share any critical reflections and negative experiences. The interview guide is available as supplemental data (S3).
The interviews were performed by the third author, familiar to the music therapist as a colleague and supervisor, but not involved in the clinical practice or the interdisciplinary team at the study site. Interviews were audio-recorded upon consent using both a Zoom hand recorder H4 and a mobile phone. Data were immediately transferred to USB-sticks and deleted from other devices. All data were safely stored with access only for the authors. In addition to the abovementioned data, the music therapist documented the clinical work through session notes in the electronic medical journal, according to standard practice at the hospital. A logbook was also continuously kept, documenting the number of sessions, and type of intervention for each participant.
Prediction of patients’ need for anesthesia was categorized (yes/no/uncertain) upon admission to the pediatric oncology department based on clinical evaluation by the primary oncologist, admission nurse, and music therapist. The criteria were patient’s ability to receive instructions and lie still for a period of time, and that no physical or psychological challenges would impair this.
Patients in the uncertain category would arrive fasting for the first CT fixation appointment with the anesthesia team available as backup, and ongoing evaluation was done to assess whether the child was experiencing significant stress without anesthesia, or whether they could manage without it. Categorical data on the actual use of anesthesia (yes/no), was drawn from the electronic medical journal, as were patient age, gender, and number of radiation treatments.
Analyses
Quantitative data were analyzed using descriptive statistics, with continuous variables presented as means and range, and categorical variables presented as frequency. Responses from open-ended questions are briefly summed up in the results, and full quotes available as supplemental material (S4).
The Qualitative focus group interviews were transcribed by the third author and analyzed using content analysis (Krippendorff, 2019). To reveal patterns across cases, a deductive approach was used as a starting point, applying themes from the interview guide, complemented by an inductive method allowing for unexpected themes to be uncovered. The content analysis process followed four steps:
(a) Familiarization with the data from the first interview through listening, transcribing, and reading the transcript repeatedly.
(b) Organization of main themes, categories, and subthemes through deductive and inductive coding based on the interview guide and responses. Similar or related key themes were highlighted manually with colors, and recurrent units grouped as coding units.
(c) Merging: a-b were repeated for the second interview, and the two analyses merged.
(d) Interpretation and summarizing of data: findings were discussed by authors one and three, and a third colleague, and the merged analysis refined with a review of main themes, categories, and sub-themes, responding to the study aims. Finally, a narrative summary was developed by the third author, grounded in the main themes and subthemes from the analysis. First author then returned to the original interview transcripts to ensure that the summary was congruent with the participants’ accounts of their experiences, to ensure that the interpretation of the data was reasonable and trustworthy.
Results
Study population (Table 2) and MT intervention variables (Table 3)
Patient characteristics and number of radiation treatments.

Music therapy (MT) intervention variables.
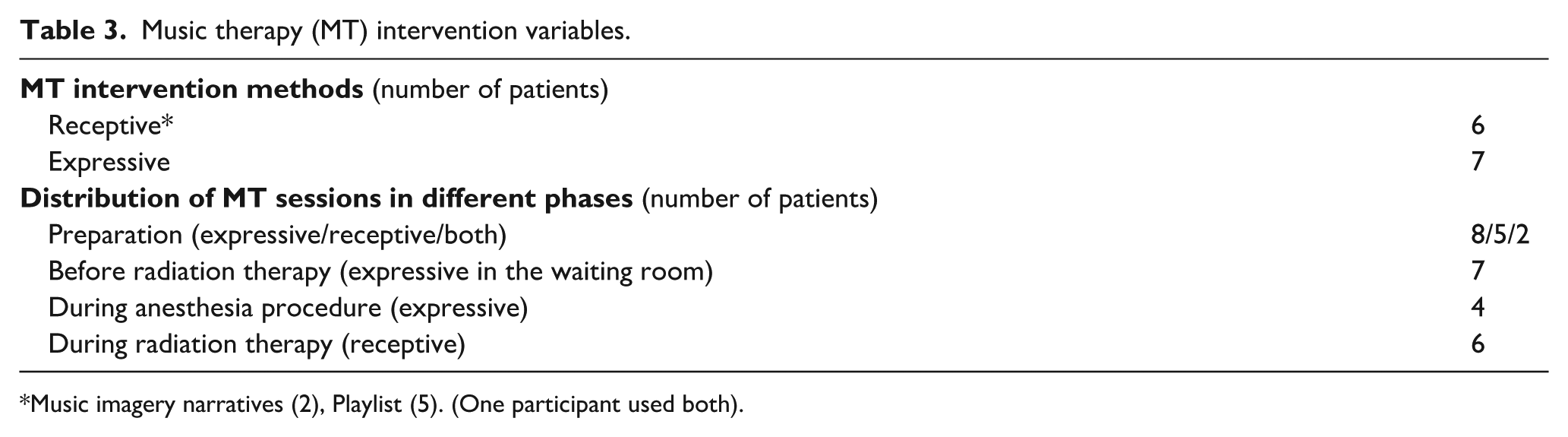
Music imagery narratives (2), Playlist (5). (One participant used both).
Patient and parents’ satisfaction and experiences
Self-reported questionnaire was obtained from 11 participants. The numeric rating of satisfaction with MT revealed a mean score of 4.82. All participants reported that they found the MT service useful and would have chosen it again. Additional written text was received from seven participants, reporting positive experiences with MT (S4). All numeric data is available as supplemental material (S5).
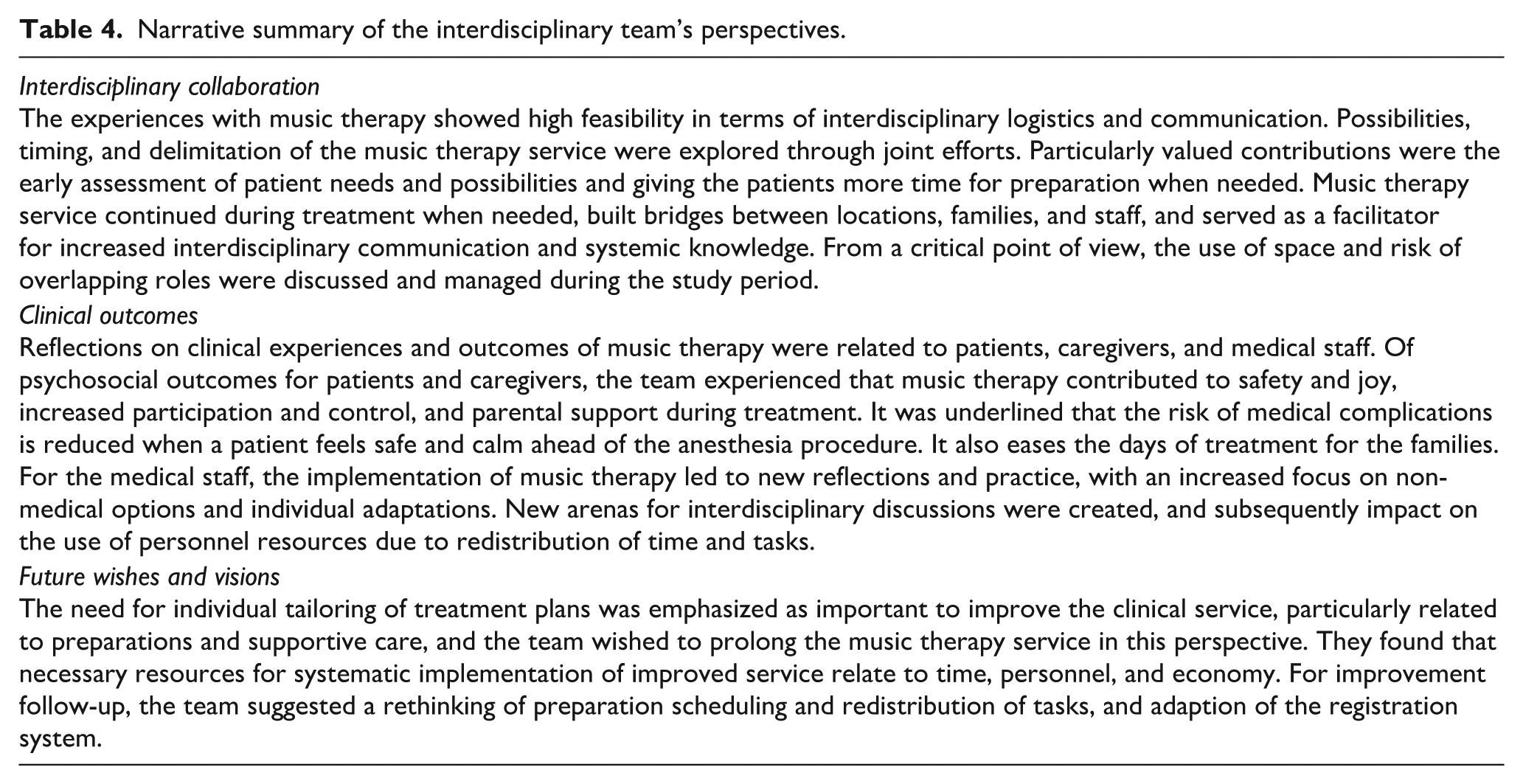
Interdisciplinary team experiences and reflections
Focus group interview 1 was completed with 10, and 2 with 5 participants from the interdisciplinary team. The narrative summary of the results is presented under the heading of the three main themes from the analysis (Table 4). It is important to note that the summary represents the group’s perceptions, not indisputable evidence of structural issues, effects, or the patients’/families’ perspectives. A complete overview of main themes, categories, and subthemes from the analysis is available as supplemental material (S6).
Narrative summary of the interdisciplinary team’s perspectives.
The use of anesthesia during radiation treatment
Results showed that all patients categorized as unsure about the need of anesthesia, managed without. For one patient who was originally categorized to use anesthesia, thorough preparation including music therapy resulted in treatment being performed without medication (Figure 1).
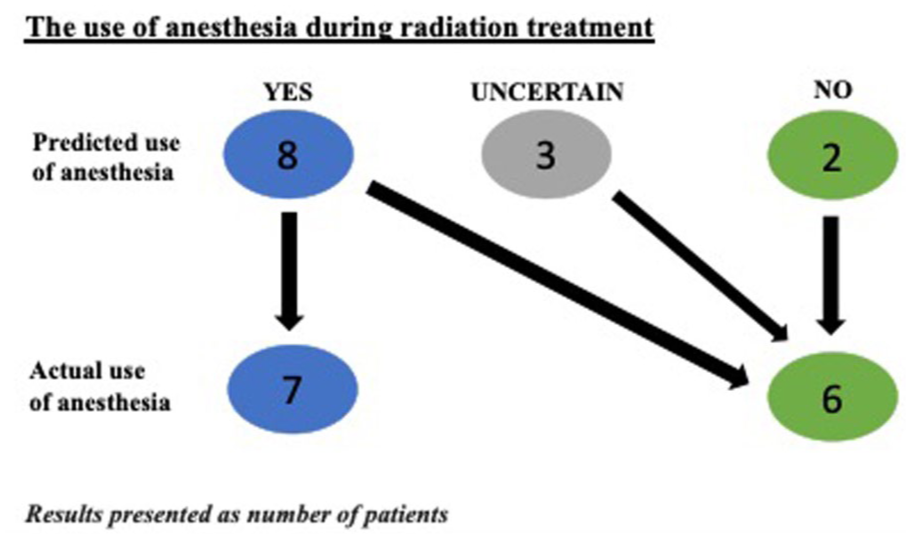
The process of predicted and actual use of anesthesia for the patients during radiation treatment, presented as number of patients.
Discussion
This study aimed to explore the experiences of MT for the current population and staff at OUS. Radiation therapy is known to be connected to stress and anxiety for both the children and their families. In this study, MT was unanimously reported as a useful therapeutic approach and found to be feasible and well received by patients, families, and staff. The results showed a positive impact related to early assessment of psychosocial needs and promising tendencies related to the use of anesthesia. The study suggested that MT service improved patient sense of safety, coping, and involvement, as well as interdisciplinary collaboration and development, enabling a redistribution of hospital resources.
Clinical outcomes
The participants utilized the non-medical coping strategies, and the relational continuity with the music therapist in the study was highlighted. Many participants reported on the importance of the relationship with the music therapist, writing about anticipation, having “something to look forward to.” Although distinct measures on symptoms were not part of the current study, the findings on modulation of anticipation is in line with previous research of adolescents in chemotherapy treatment (Giordano et al., 2024). Participants appreciated the flexibility within the various interventions and the pure positive focus of making music together. Through preference based music activities and dialogue MT provided a chance for personal choice and control for the patient, affording a tool for coping, in line with previous findings of stress relief, physical and psychosocial improvements in similar settings (O’Callaghan et al., 2007) and examples of modulating mechanisms of MT in procedure support (Ghetti, 2012). The current study results also suggest an impact on patients’ need for anesthesia. There is no certainty as to why all patients initially categorized with an unsure need for anesthesia, managed without. Playful assessment, dialogues and planning, and acknowledging patient- and parent resources through the music therapy service aimed to optimize predictability and control for the families and might have influenced and strengthened coping strategies and feeling of safe care. Despite the predicted, a 4-year-old patient was able to complete a long series of treatment fractions without anesthesia due to early assessment individualized preparation, and interdisciplinary family support. Although being a single case, this suggests a reassessment of established expectations related to age and coping, and a possible effect of improved individual tailored support for patients through the MT service. In sum, the study supports previous findings and characteristics from comparable studies of MT and related psychosocial support (Boik and Hall, 2020; Cole et al., 2024; O’Callaghan et al., 2007; Scott et al., 2016), and adds to existing knowledge by pointing to clear benefits of early assessment and preparation.
Interdisciplinary collaboration
With the music therapist offering relational continuity between locations, the study created an opportunity to build bridges across sites for both family and staff. The music therapist became a facilitator for increased interdisciplinary communication and systemic knowledge, because of the opportunity to meet the patient early in the hospital stay. The human resources for children in radiation therapy are not permanently allocated at the current site, which may explain why the impact of MT on the redistribution of time and tasks was an appreciated factor for the interdisciplinary team. This proved decisive when a patient managed radiation therapy without anesthesia during a particularly busy period and points toward an interdisciplinary perspective on the potential of MT that should be further utilized.
Most research on MT in pediatrics set focus directly on patients’ well-being related to QoL, management of procedures, pain, and anxiety. The current study’s exploration and findings on interdisciplinary collaborative practice and benefits can be seen as an expansion and contribution to existing knowledge in the field. Cole et al. (2024) discuss how more education is needed to allow music therapy to be considered by patients, parents, and staff. In the current study new arenas for interdisciplinary discussions were created through the project leading to new reflections and practice, with an increased focus on non-medical options and individual adaptations (Leinebø and Aasgaard, 2016; Patel et al., 2021). Interdisciplinary collaboration is often challenging, but fundamentally important in pediatrics, and should be systematically explored in future larger studies.
Limitations
One limitation of this study is that it includes a small sample and generalization is not possible. It is also generally challenging to compare due to differences in the radiation treatment, for example, number and duration of sessions, and/or use of mask. As in most MT studies, the study could not be blinded, implicating a risk of bias. The younger patients’ perspectives are primarily represented by parents’ answers on their behalf, and the respondents may have been influenced by their relationship with the music therapist. As an explorative study, a more in-depth collection of data would have been profitable. Video analyses could have added valuable data but are ethically challenging in this context. The risk of bias is particularly prominent in the focus group interviews where the music therapist participated. Continuity in the collaborative team dialogue and transparency in reporting were emphasized here, which can also be seen as important for relevant reporting of the process. Cost–benefit analysis comparing music therapy with the use of anesthesia was not included in this study due to limited project resources but should be included in future studies systematically comparing music therapy with anesthesia for the current population.
Conclusion
This pilot study is the first of its kind in Scandinavia, showing that MT before or during radiation therapy constituted a meaningful and highly appreciated service for this patient population. The results also indicate that MT can increase treatment quality through improved interdisciplinary collaboration, allowing better individually tailored treatment and support. The potential of music therapy to reduce the need for anesthesia should be further explored in future studies. We suggest MT for this patient population to provide an opportunity for improved patient care and interdisciplinary collaboration, possibly with positive consequences for hospital resources in the larger picture. For future studies, it would be of interest to include more participants and sites to ensure safer numbers and data, and to include cost–benefit analyses. There is also a need for more detailed, in-depth investigations of modulating factors in MT interventions and for controlled studies comparing MT to standard treatment.
Supplemental Material
Supplemental_material_1 – Supplemental material for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study
Supplemental material, Supplemental_material_1 for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study by Julie Mangersnes, Margit Louise Fremmerlid and Stine Camilla Blichfeldt-Ærø in British Journal of Music Therapy
Supplemental Material
Supplemental_material_2 – Supplemental material for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study
Supplemental material, Supplemental_material_2 for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study by Julie Mangersnes, Margit Louise Fremmerlid and Stine Camilla Blichfeldt-Ærø in British Journal of Music Therapy
Supplemental Material
Supplemental_material_3 – Supplemental material for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study
Supplemental material, Supplemental_material_3 for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study by Julie Mangersnes, Margit Louise Fremmerlid and Stine Camilla Blichfeldt-Ærø in British Journal of Music Therapy
Supplemental Material
Supplemental_material_4 – Supplemental material for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study
Supplemental material, Supplemental_material_4 for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study by Julie Mangersnes, Margit Louise Fremmerlid and Stine Camilla Blichfeldt-Ærø in British Journal of Music Therapy
Supplemental Material
Supplemental_material_5 – Supplemental material for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study
Supplemental material, Supplemental_material_5 for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study by Julie Mangersnes, Margit Louise Fremmerlid and Stine Camilla Blichfeldt-Ærø in British Journal of Music Therapy
Supplemental Material
Supplemental_material_6 – Supplemental material for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study
Supplemental material, Supplemental_material_6 for MustRa—Music therapy for children and youths undergoing radiation therapy: An exploratory pilot study by Julie Mangersnes, Margit Louise Fremmerlid and Stine Camilla Blichfeldt-Ærø in British Journal of Music Therapy
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were funded by the Fondsstiftelsen and Barnestiftelsen at Oslo University Hospital.
Data availability statement
In this study, all numeric data and all responses from open-ended questions are available in full length as supplemental material. The interview guide and a complete overview of main themes, categories, and subthemes from the analysis are available as supplemental material. The complete transcripts of the focus group interviews are not available.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.