
Abstract
Interest in the applications of music in health, social care and community settings are growing worldwide. Rare diseases are a major challenge for public health, particularly in paediatric populations. Previous research has demonstrated music and music medicine benefit children and young people’s health and wellbeing; however, this is under-researched in the paediatric rare disease context. This scoping review was conducted to explore music therapy and music medicine as tools to support children with rare diseases’ health and wellbeing within healthcare settings. The review investigated the current research on how music is used for children and young people with rare diseases and complex conditions and synthesised the resulting evidence. Results from this review suggest that music therapy and music medicine are beneficial for the health and wellbeing of children with rare diseases and complex conditions, including reduced anxiety, stress and pain during clinical procedures, and increased communication, social and coping skills and enhanced quality of life.
Introduction
A rare disease is characterised as a life-threatening or chronically debilitating disease with a prevalence of less than five people in 10,000 (Kole et al., 2021). Incidences of rare disease vary globally, but overall, an estimated 300 million people have a rare disease (Kole et al., 2021). Rare diseases are common collectively, but their low prevalence typically coincides with a lack of medical expertise, knowledge and research (EURODIS, 2022). Most rare diseases therefore represent a substantial unmet medical need and a major challenge for European public health (European Commission, 2017).
Approximately, 75% of rare diseases begin in childhood and are lifelong (Bavisetty et al., 2013). The complex and chronic nature of these diseases often causes significant impacts on children’s development, health and wellbeing, both physically and psychosocially (Kole et al., 2021). Previous research demonstrates that arts based activities like music are useful in disease and health management and treatment, through supporting child development and promoting the health and wellbeing of those with chronic conditions (Fancourt and Finn, 2019). Therefore, there is potential benefit in the use of music interventions for paediatric rare disease populations.
Music interventions are significant for children with rare, complex medical conditions in hospitals, offering a unique and therapeutic avenue for holistic care (Burrai et al., 2020). Music can provide comfort, emotional expression and joy for these young patients whose medical journeys are often marked by extended hospital stays and complex treatments (Pérez-Núñez et al., 2021; Sampaio, 2023). Moreover, for children with rare diseases, whose conditions may be isolating and challenging to understand, music interventions can serve as an accessible non-verbal language, fostering connection and communication. Without specialised treatments tailored to each rare condition, music becomes a versatile tool that can be adapted to these children’s individual needs and preferences, contributing to their emotional wellbeing and enriching their overall quality of life during their hospitalisation (Sampaio, 2023).
Interest in Music Therapy (MT) and Music Medicine (MM) has been expanding in paediatric and adult healthcare settings (Schmid and Ostermann, 2010). Yet, the literature suggests there is broad confusion and misunderstanding of which music-based interventions constitute MT and which, MM. MT is defined as ‘an established health profession in which music is used within a therapeutic relationship to address physical, emotional, cognitive, and social needs of individuals’ (American Music Therapy Association, 2024). Referral to a MT service is based on clinical need and is unrelated to patient’s previous enjoyment in music or musical skill. Therapy begins with a process of assessment and having identified areas of need. Following this, individualised treatment programmes are then created using music in a prescriptive way to meet identified patient goals. MT, like psychotherapy, offers the client a confidential space to explore their inner conflicts in a contained, safe way. The entire process is built on a foundation of trust and mutual respect between client and therapist, and it is from this relationship that patient’s positive outcomes derive (McIvor, 2023). A number of different approaches may be utilised by the therapist, dependent on their training, to address the client’s needs. These include psychodynamic, humanistic, behavioural, neurological, and community-based approaches (Darrow, 2008; Wheeler, 2015). An eclectic approach draws on theories and interventions from various schools of psychology to best support the client in meeting their identified goals. Intervention type, whether music listening, songwriting, verbal reflection and so on, is selected based on targeted goal areas and the therapist continually reviews and updates the approach based on clinical observations, client progress and engagement.
MM has been described as the use of music within a healthcare setting, delivered by a professional other than an MT. MM typically involves the use of music listening to support anxiety reduction in the medical setting. The literature does not outline a process of assessment within MM, nor is there a systematic therapeutic process in place (Bradt et al., 2021). Although MM may have therapeutic benefits, MM is not MT. This distinction is important for many reasons and is often misrepresented in the public domain.
The use of MT and MM in hospital settings has clinical benefits. Improved overall hospital experience and pain management was associated with MT in Roseen et al. (2017) and with MM in Ames et al. (2017). Improved sleep quality of patients was associated with MM in Momennasab et al. (2018). In palliative care settings, MT and MM have been reported to create more supportive care environments. In Pommeret et al. (2019), palliative cancer patients experienced improved satisfaction, comfort and social ties through a MM intervention. In Preissler et al. (2016), MT interventions assisted in identifying the psychosocial needs of palliative cancer patients.
In addition, there is an increasing evidence base for the use of music interventions with children in hospitals (Bradt, 2013). Prior research has demonstrated that the use of MT can improve coping skills (Moola et al., 2020; Stegemann et al., 2019), mood, communication, social skills, and quality of life (Johnson et al., 2021) and can reduce pain and anxiety during clinical procedures (Klassen et al., 2008; Stegemann et al., 2019). MM has also demonstrated benefits in pain and anxiety reduction during hospitalisation (Johnson et al., 2021; Stegemann et al., 2019). While there is a growing body of evidence regarding the beneficial effects of music for children and young people, more rigorous research is still needed on using MT and MM with children living with rare diseases.
Methods
Research questions
This scoping review of the literature aimed to map out the existing studies about the use of MT and MM with children who have rare diseases or comparable complex conditions in the healthcare setting. The study also aimed to explore and summarise the diversity of these studies, answering the following questions:
What types of MT and MM interventions were used?
In what healthcare settings have these studies been conducted?
Who were the MT and MM target population?
What types of research designs and methods were used?
Which outcomes have been described in the literature?
What were the roles and significant impacts of MT and MM on participants’ health and wellbeing?
Protocol and registration
The study was based on the Joanna Briggs Institute’s methodology for scoping reviews (Peters et al., 2020) and followed the original framework of Arksey and O’Malley’s (2005) five-stage scoping review framework, including consultations with relevant stakeholders, as proposed by Levac et al. (2010). The study protocol is available at Karpavičiūtė et al. (2022). This study was conducted as part of the SAMPI research project which aims to enable children and young people living with rare diseases to express their experience of living with a rare disease and help to identify the factors that enhance, inhibit and impact their lives (Karpavičiūtė et al., 2022).
Eligibility criteria
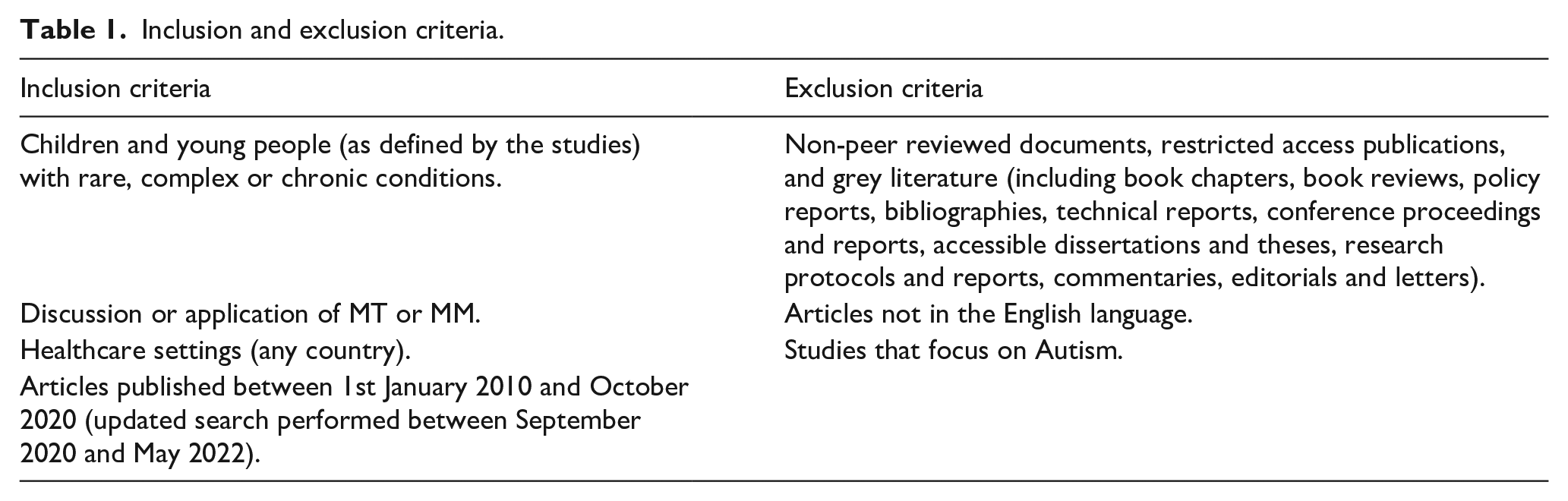
While the focus of the SAMPI project is on children with rare diseases, due to the limited number of articles on MT and MM with this cohort, children with complex conditions were also included. This is because there are similar disease burdens between these populations: rare conditions are often chronic and are of high complexity (Somanadhan et al., 2020). Studies that included adults were excluded. As the United Nations Department of Economic and Social Affairs (2013) recognises those up to the age of 24 years old as young people, studies with similar age ranges were included if the population was defined as young people, not adults, and children were also included in the studied population. Studies that looked at children with specific needs related to the autism spectrum or related disorders were excluded due to the prevalence of MT and MM among this population. Articles that included diagnostic tests commonly undergone by children and young people with rare diseases and complex conditions were included due to their relevance to this population. The period was limited from January 2010 to May 2022 to reveal present-day literature. The inclusion and exclusion criteria are detailed in Table 1.
Inclusion and exclusion criteria.
Search
The databases searched included CINAHL Complete, Medline Complete, the Psychological and Behavioural Sciences Collection, and PubMed/PMC. The initial search was performed in October 2020, with an updated search performed in May 2022 to enhance the timeliness of this review. However, the Psychological and Behavioural Sciences Collection could not be accessed during the updated search; this limitation was accepted due to the limited number of returned articles from the updated search. The search strategy used in both the original and updated searches is included in Appendix 1. Non-peer reviewed literature and grey literature were not included.
Selection of sources of evidence
In the original search, four researchers (AS, SK, AO and SS) screened the studies by title and abstract independently, following recommendations provided by Levac et al. (2010). This involved a multidisciplinary team approach to selection of included articles, with discussions between researchers during the abstract review process regarding arising challenges or uncertainties. This collaborative approach added transparency and rigour to the study selection process, enhancing the reliability and validity of the overall review. In the original search, the fifth researcher (TK) resolved any disagreements through discussion and review. In the updated search, two researchers (NB and SSi) screened by title and abstract independently; these authors also reviewed the included articles from the original search. This continuity in the team ensured consistency and familiarity with the inclusion criteria, promoting a cohesive and reliable screening process. Where any disagreements arose, a third researcher (SS) resolved conflicts through discussion and review.
Data charting and results synthesis
Two researchers performed data extraction according to Braun and Clarke’s (2006) method of thematic analysis. This approach was used as it is a flexible and accessible approach that enables a rich analysis of the data, supporting the identification of similarities, differences and unexpected insights (Braun and Clarke, 2006). Relevant information was identified and coded in the studies according to emergent themes. Due to the inductive nature of this process, codes that related to each other were reviewed and grouped together as a theme. These themes were then presented to the research team for discussion and validation.
The quality of the studies included in this scoping review was assessed using the Mixed Methods Appraisal Tool (MMAT). The MMAT is a critical appraisal tool designed for the methodological appraisal of systematic and scoping mixed studies reviews (Hong et al., 2018).
Results
Study selection
From a total of 448 identified articles, a total of 19 studies were included in this review. A summary of the search process using a PRISMA diagram (Page et al., 2021) is included in Figure 1 below.
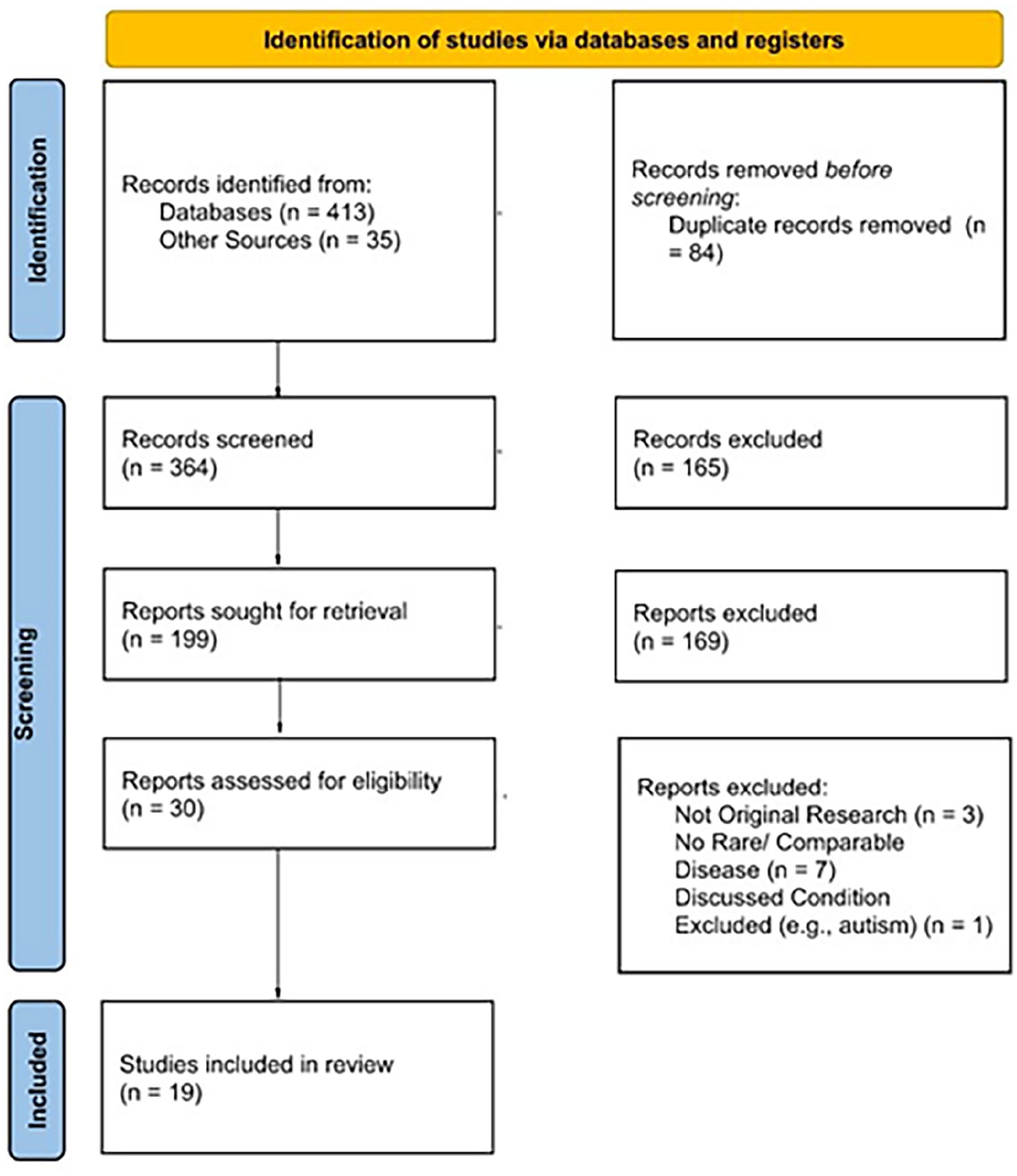
PRISMA flow diagram: search process summary.
Study characteristics
Most of the studies included in this review used quantitative study designs (n = 15). Studies that used qualitative methods (n = 2) were based on interviews conducted with participants or parents of participants. Two studies employed mixed methods research designs. The study designs of each article are specified in Table 2. Most studies were published from 2014 on and were based in the United States, Canada and Europe. Most studies (n = 17) were conducted in a hospital setting; one study was based in a MT Research Centre and one study focused on home care. The populations studied included children and young people with various cancers, cystic fibrosis (CF), neurological conditions, Sanfilippo syndrome, and chronic diseases including rheumatoid arthritis. Overall, participants ranged in age from 0 to 24 years, though most studies focused on children below 18 years.
Characteristics of included MT studies.
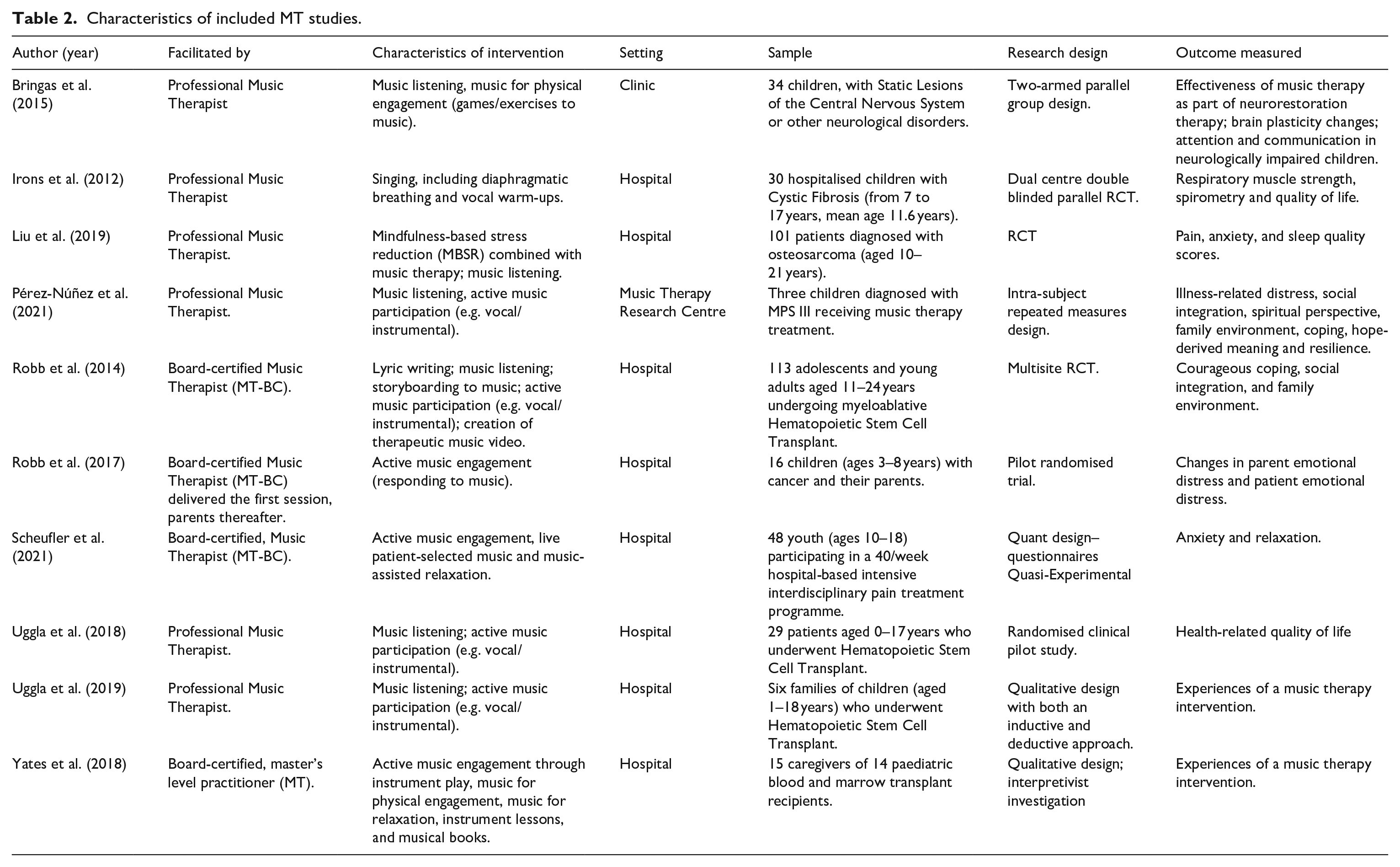
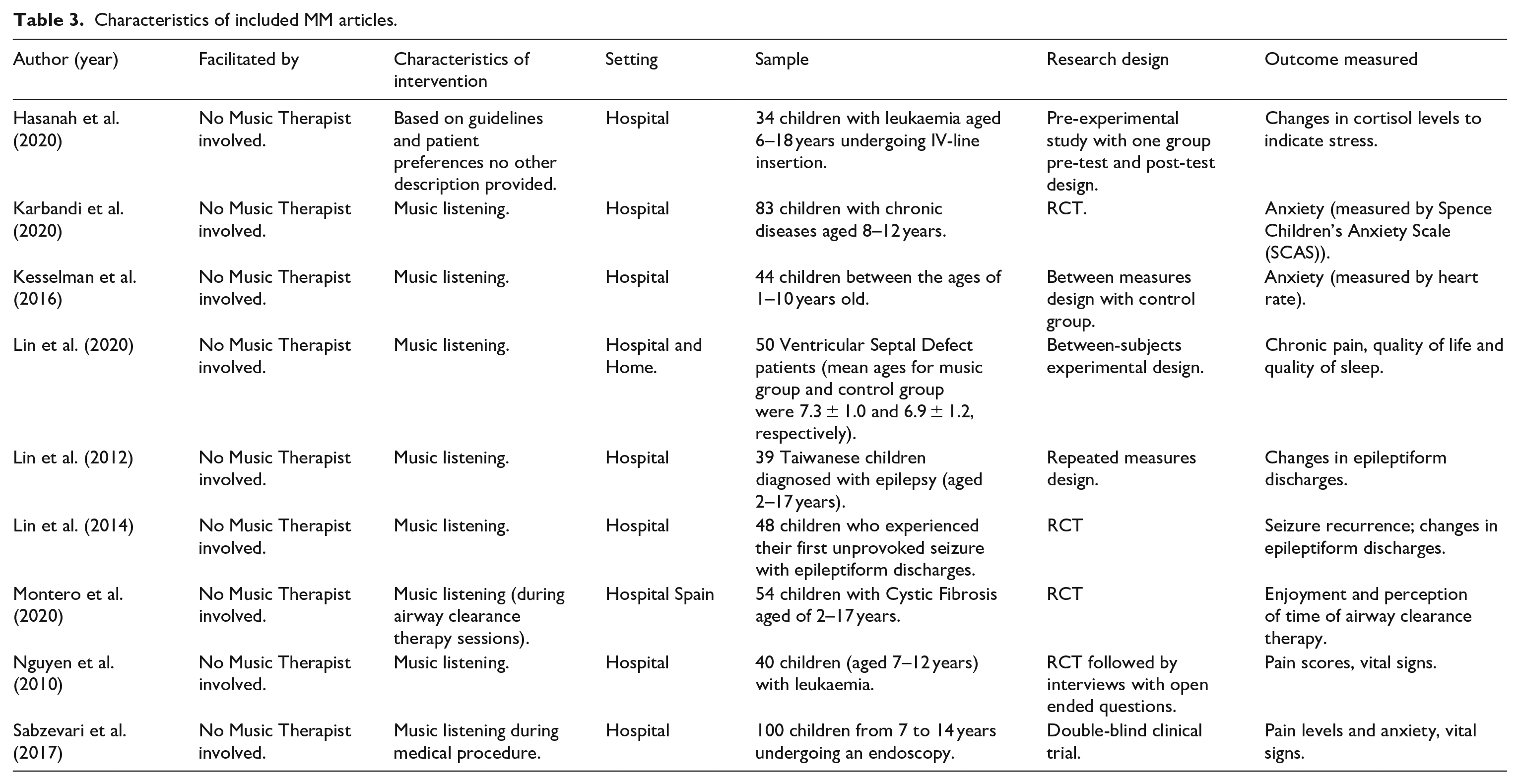
More than half of the studies (n = 10) reference a Music Therapist implementing the interventions provided in the studies. Five studies referred to their interventions as MT but were not designed or delivered by a Music Therapist. The remaining articles (n = 4) were classed as music-based interventions and did not feature any input from Music Therapists. The articles that did not feature a Music Therapist were therefore classified in this review as MM. Table 2 describes the included articles that featured MT according to the review questions, whereas Table 3 describes the included articles that featured MM. A more detailed summary table of the included studies is available as Supplementary Table A.
Characteristics of included MM articles.
According to the MMAT, overall, the quality of included studies was medium, with less than half of the studies being deemed of the highest quality. The principal areas of concern arising from the formal quality appraisal are the underreporting of complete outcome data, outcome assessors not being blinded to the intervention, and participant non-adherence to the assigned intervention. An overview of the results of the MMAT screening can be found in Supplementary Table B.
Thematic analysis
This review adheres to the thematic analysis method proposed by Braun and Clarke (2006), categorising findings into thematic groups. We undertook a preliminary reading of the included studies and developed initial patterns and themes based on the primary outcomes reported. Findings were then structured into thematic categories (Braun & Clarke, 2006). Incorporating thematic analysis into a scoping review enhances the qualitative depth of the review process, offering a nuanced understanding of the literature and contributing to generating insights that may inform both research and practice.
Following the analysis of the data, MT and MM were determined to have effects over two overarching domains:
Physiological and clinical support
Psychological wellbeing
While these domains are interconnected, they are reported for MT and MM individually to illustrate the similarities and differences in effect for these interventions.
MT
MT positively affects physiological and clinical support
MT was shown to have a positive impact on clinical symptoms including heart rate (Uggla et al., 2018), respiratory status (Irons et al., 2012), brain plasticity (through electroencephalogram) and attention (Bringas et al., 2015). It was also demonstrated to improve sleep quality (Liu et al., 2019; Robb et al., 2017) and attention levels (Pérez-Núñez et al., 2021). Reduced levels of pain perception were measured directly through accredited pain scales (Liu et al., 2019) and behavioural coding tools (Robb et al., 2017), or indirectly through qualitative interviews with patients or caregivers (Pérez-Núñez et al., 2021; Uggla et al., 2019; Yates et al., 2018). Three common mechanisms for MT to reduce pain perception emerged from the study: MT as a distraction from pain (Uggla et al., 2019), MT for mood improvement and reduced pain perception (Robb et al., 2017; Yates et al., 2018), and MT for relaxation/reduced anxiety for reduced pain perception (Liu et al., 2019; Pérez-Núñez et al., 2021). One study focused on pain alleviation through establishing long-term coping measures using MT (Scheufler et al., 2021). One study did not find a statistically significant difference in pain perception between the MT intervention and control groups (Uggla et al., 2018).
MT improves psychological wellbeing
The benefits of MT to reduce anxiety were reported in five studies using accredited anxiety scales ( Liu et al., 2019; Scheufler et al., 2021; Uggla et al., 2018; Yates et al., 2018) or associated clinical signs such as blood pressure (Pérez-Núñez et al., 2021). Stress reduction was evaluated in one study (Robb et al., 2017) which found lower emotional distress following MT. However, this study focused on music support delivered by parents following an initial MT session and found that the challenge of this activity could increase parental emotional distress. MT was found to have a positive impact on mood as reported by parents and caregivers (Robb et al., 2017; Uggla et al., 2018; Yates et al., 2018).
Emotional state was measured in four studies, demonstrating higher scores in four psychological variables which included physical, social, emotional and cognitive levels (Pérez-Núñez et al., 2021), enhanced emotional state (Irons et al., 2012) and activation of positive emotions (Uggla et al., 2019) after MT sessions. Combining mindfulness-based stress reduction with MT was reported to significantly alleviate psychological complications in participants in Liu et al. (2019).
MT was reported to improve health-related quality of life of participants in Uggla et al. (2018). A similar finding was reported in Irons et al. (2012) but this was not statistically significant. Three studies did not measure quality of life but discussed how the MT interventions in the studies could positively impact quality of life (Liu et al., 2019; Pérez-Núñez et al., 2021; Yates et al., 2018). The benefits of MT for building social connections and increasing the relationships between the patient and parents and healthcare professional, and creating a safe space, was reported in six studies (Bringas et al., 2015; Pérez-Núñez et al., 2021; Yates et al., 2018; Robb et al., 2014; Robb et al., 2017; Uggla et al., 2019). The importance of the therapeutic relationship during MT was also highlighted in Uggla et al. (2019).
MT was also beneficial for self-expression and creativity through different mechanisms including lyric writing (Robb et al., 2014), creative decision-making (Robb et al., 2017), learning and playing songs for self-expression (Uggla et al., 2019), and increased communication and creativity due to the stimulation of the MT session (Pérez-Núñez et al., 2021).
The positive effects of MT for children and young people’s ability to cope with their illness was discussed in five studies (Irons et al., 2012; Robb et al., 2014, 2017; Uggla et al., 2019; Yates et al., 2018) through providing a break in monotony and sense of normality, and encouraging engagement.
MM
MM positively affects physiological and clinical support
Similar to MT, MM was shown to positively affect clinical symptoms through music listening, including systolic and diastolic blood pressure (Sabzevari et al., 2017), heart rate (Kesselman et al., 2016; Nguyen et al., 2010) and respiratory rate, and oxygen saturation (Nguyen et al., 2010). Also noted were the positive impact of music listening on epileptiform discharges in children and young people with epilepsy (Lin et al., 2012, 2014) and improved sleep quality (Lin et al., 2020). MM was also demonstrated to reduce pain perception generally (Lin et al., 2020), and before and during diagnostic procedures such as endoscopy (Sabzevari et al., 2017) or lumbar puncture (Nguyen et al., 2010). The mechanisms of MM to reduce pain perception included distraction (Nguyen et al., 2010) and reduced anxiety (Sabzevari et al., 2017).
MM supports psychological wellbeing
Five studies considered the impact of MM on anxiety (Karbandi et al., 2020; Kesselman et al., 2016; Nguyen et al., 2010; Sabzevari et al., 2017). Reduced anxiety was reported through accredited anxiety scales (Karbandi et al., 2016; Nguyen et al., 2010), through associated clinical symptoms such as blood pressure and heart rate (Kesselman et al., 2016; Sabzevari et al., 2017) or visible relaxation (Pérez-Núñez et al., 2021). Reduced anxiety levels due to MM use were reported during diagnostic interventions (Kesselman et al., 2016; Nguyen et al., 2010; Sabzevari et al., 2017) and during treatment procedures (Hasanah et al., 2020). Stress reduction was measured through lower cortisol levels in Hasanah et al. (2020), though the results were not statistically significant. Montero-Ruiz et al. (2020) measured participants’ increased enjoyment and decreased perception of time taken of their treatment routine when listening to specifically recorded music. The impact of MM on quality of life was only measured in one study (Lin et al., 2020), which concluded that MM improves medium-to-long term quality of life postoperatively.
MM was noted in one study to assist self-management through enhancing enjoyment and reducing the perceived time taken of a medical treatment, therefore, improving compliance and establishing it as a positive experience (Montero-Ruiz et al., 2020).
Discussion
Results from this review indicate that engaging in MT and MM benefits children and young people with rare diseases during hospitalisation. The most reported outcome in the publications included in this review was the positive impact of MT and MM on anxiety and stress reduction, and improvement in mood and psychological wellbeing. This is supported by the literature, as Stegemann et al. (2019) have demonstrated the positive effects of MT and MM on levels of stress parameters as observed in heart and respiratory rates in children and young people in healthcare contexts, as well as improving mood and regulation. Klassen et al. (2008) also report that music is effective in reducing anxiety and pain during clinical procedures in children and young people, which is similarly described in this review.
The reported benefits of MT and MM for pain perception are also in line with the literature; for example, Moola et al. (2020) found in their review that MT had a positive impact on pain perception in children and youth with disabilities and chronic conditions in outside hospital settings. Benefits to clinical symptoms, including reduced systolic blood pressure and heart rate are similarly noted in Kobus et al. (2022). Findings in this review around self-management and coping with an illness are echoed in previous research which has reported MT as effective in improving communication and social skills in childhood and adolescence (Moola et al., 2020; Stegemann et al., 2019).
This scoping review has demonstrated that the benefits of MT and MM are not limited to the paediatric population living with rare diseases as parents and caregivers can both benefit from these types of interventions (Pérez-Núñez et al., 2021; Yates et al., 2018). This is supported in the literature (Edwards, 2016) and demonstrates the importance of MT as child and family-centred approaches to care. However, placing parents in facilitation roles for these interventions has the potential to negatively affect their emotional states. Thus, removing caregivers from the role of facilitator and returning to the Music Therapist-delivered intervention provides more benefits for caregivers, for example, the opportunity to relax and enjoy what was reported as a normalising, shared experience (Robb et al., 2017).
While in this review both MT and MM were demonstrated to have similar benefits, there was a lack of clear differentiation between the two. The clearest difference between MT and MM was illustrated in the types of interventions used – while MT interventions involved several different methods of engaging with the music (e.g. active music engagement, participation in music-making, lyric writing, music listening, etc.), MM studies primarily encompassed music listening only without the involvement of a Music Therapist. The types of interventions highlight the key characteristics that separate the two approaches. MT studies involved the development of a therapeutic relationship between the participant and the Music Therapist to attain patient goals, while MM was used in a more generic singular way through utilising music listening experiences. This may be significant when identifying the differences between the uses of MT and MM in clinical settings and may contribute to avoiding the misrepresentation of MM as MT in the literature in the future.
In addition to the reported benefits of MT, the findings from this review also identify MT and MM as unique tools which can support various clinical procedures and patient goals in hospital settings. Some of the studies included in this review consisted of using music to support the client’s engagement and acceptance of medical interventions (Montero-Ruiz et al., 2020), Mindfulness Based Stress Reduction (MBSR; Liu et al., 2019) and distraction cards (Karbandi et al., 2020). As each child with a rare disease presents in a unique way, further research is needed to determine the effect of using music and other creative therapy modalities in the treatment of children with rare diseases.
It is clear from this review that there is limited knowledge of using music interventions to support children and young people with rare diseases based in Europe, especially the United Kingdom and Ireland. No articles identified for review were based in the United Kingdom or Ireland. This suggests a gap in the policy and healthcare pathways for rare diseases in these countries. As this population faces significant challenges, including physical and intellectual disabilities, frequent hospitalisations, stigmatisation and challenges in developing coping strategies and resilience, among others (Somanadhan et al., 2023), the use of music-based interventions could contribute to improving both physical and psychological impacts of living with rare diseases. Music Therapists are trained to work therapeutically and sensitively with individuals with complex medical needs and as such, are well placed to devise and support healthcare pathways by offering an alternative, capacity driven and family-centred intervention for children with rare disease in healthcare settings.
It is important to note that five of the studies that featured MM referred to the intervention as MT (Hasanah et al., 2020; Karbandi et al., 2020; Lin et al., 2020; Montero-Ruiz et al., 2020; Nguyen et al., 2010). However, as clarity was not provided as to whether a Music Therapist was involved, these studies were categorised in this review as MM. The presence of a Music Therapist in delivering a music-based intervention defines MT, due to the relational nature of the intervention. This is not to say that there is a hierarchy of music-based interventions; this review demonstrates the opposite by highlighting the clear benefits of both MT and MM. While MT can facilitate therapeutic change, MM can also be utilised for affirmation and health promotion, with both being valuable tools for health. Both can provide physiological, physical, emotional or relational experiences depending on the context and needs of the patient (Bonde, 2011). However, to ensure the safety of both vulnerable patients availing of MT and working Music Therapists, it is crucial that MT is recognised as an allied health profession. This ensures MT services are delivered by a qualified, regulated Music Therapist, promoting the highest professional standards among Music Therapists (Keating, 2020). To this end, a recommendation of this review is for the global protected use of the professional title, Music Therapist and term, Music Therapy.
Study limitations
There are several potential limitations to this review. These include limitations of inclusion criteria, such as English-language requirements, date of publication and lack of grey literature, which may have led to the exclusion of relevant literature. Furthermore, the diverse interventions and methodologies of the included studies made the comparison of study results more difficult. However, these limitations are not considered significant enough as to misrepresent the research in this field and are therefore accepted by the authors.
Conclusion
This scoping review investigated the current research on how music is utilised for children and young people with rare diseases and complex conditions in paediatric healthcare settings and synthesised the resulting evidence of the impact of MT and MM. Evidence on the use of MT and MM in paediatric populations is still emerging, but results from this study suggest that using MT and MM is beneficial for the health and wellbeing of children with rare diseases and complex conditions. These benefits include reduced anxiety, stress and pain during clinical procedures, as well as an increase in communication, social and coping skills and quality of life. Parents and caregivers of children and young people with rare diseases and complex conditions can also benefit from the use of MT and MM in paediatric healthcare settings.
Based on the findings, the authors propose that the involvement of professional Music Therapists in MM research would be of particular benefit given their area of expertise and support more accurate reporting on the use of MT and non-MT interventions, which would enhance emerging research in this area.
Supplemental Material
sj-docx-1-bjm-10.1177_13594575241258820 – Supplemental material for The impact of music on health and wellbeing of children and young people with rare diseases in healthcare settings: A scoping review
Supplemental material, sj-docx-1-bjm-10.1177_13594575241258820 for The impact of music on health and wellbeing of children and young people with rare diseases in healthcare settings: A scoping review by Shannon Sinnott, Niamh Buckle, Alison Sweeney, Simona Karpavičiūtė, Amy O’Neill, Thilo Kroll and Suja Somanadhan in British Journal of Music Therapy
Footnotes
Author contributions
SS, TK, AS, AO contributed to conceptualisation (ideas; formulation or evolution of overarching research goals and aims). NB, SSi, SK, SS contributed to data curation (management activities to annotate (produce metadata), scrub data and maintain research data (including software code, where it is necessary for interpreting the data itself) for initial use and later re-use). NB, SSi contributed to formal analysis (application of statistical, mathematical, computational, or other formal techniques to analyse or synthesise study data). SS, AS contributed to Funding acquisition (acquisition of the financial support for the project leading to this publication). NB, SSi, SS, AS, AO contributed to Investigation (conducting a research and investigation process, specifically performing the experiments, or data/evidence collection). TK, SS contributed to Methodology (development or design of methodology; creation of models). SS, AS contributed to Project administration (management and coordination responsibility for the research activity planning and execution). SS, AS contributed to Resources (provision of study materials, reagents, materials, patients, laboratory samples, animals, instrumentation, computing resources, or other analysis tools). N/A contributed to Software (programming, software development; designing computer programmes; implementation of the computer code and supporting algorithms; testing of existing code components). SS, TK contributed to Supervision (oversight and leadership responsibility for the research activity planning and execution, including mentorship external to the core team). SS, TK contributed to Validation (verification, whether as a part of the activity or separate, of the overall replication/reproducibility of results/experiments and other research outputs). NB, SSi, AS, SS contributed to Visualisation (preparation, creation and/or presentation of the published work, specifically visualisation/data presentation). NB, SSi contributed to Writing – original draft (preparation, creation and/or presentation of the published work, specifically writing the initial draft (including substantive translation). NB, SSi, AS, TK, SS contributed to Writing – review & editing (preparation, creation and/or presentation of the published work by those from the original research group, specifically critical review, commentary or revision – including pre- or post-publication stages).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to express our sincere gratitude to our funder, Children’s Health Foundation at Children’s Health Ireland, for their support.
Supplemental material
Supplemental material for this article is available and can be accessed by contacting the authors.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.