
Abstract
Music therapy (MT) has been used to support people with a variety of eating disorders (EDs), but it is unclear whether there is sufficient and robust evidence from controlled experimental studies. In this article, we report the results of a systematic review that summarises the evidence from published controlled studies where MT has been used to treat people diagnosed with any type of ED. Our results demonstrate that robust evidence concerning the effectiveness of MT for the treatment of EDs is severely lacking. Nonetheless, the evidence described in this paper warrants further investigation especially given that new treatment strategies for EDs are urgently needed. To this end, we offer a set of recommendations for future high-quality experimental studies that can inform the development of effective MT interventions and support for people with EDs.
Introduction
Eating disorders (EDs) are a type of mental disorder marked by severe disturbances in people’s eating behaviours and obsessions about their body weight, size, or shape (World Health Organization, 2019). EDs are most common during adolescence and early adulthood (although they often persist throughout life), have a severe impact on people’s physical and mental health, and can be life threatening (Chavez and Insel, 2007; Schmidt et al., 2016). Moreover, EDs frequently co-occur with other psychiatric conditions, such as anxiety, depression, or substance abuse (Herzog and Eddy, 2007; Kaye et al., 2004).
According to the most recent version of the widely used Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (American Psychiatric Association, 2013), there are five main diagnostic categories of ED: anorexia nervosa, bulimia nervosa, binge-eating disorder, avoidant/restrictive food intake disorder, pica and rumination disorder. In addition, two other categories capture clinically significant feeding and eating behaviours that do not meet the required criteria of these five categories: Other Specified Feeding or Eating Disorders (OSFED) and Unspecified Feeding or Eating Disorder (UFED). OSFED applies to cases where the clinical thresholds of the five main categories of ED are not met, although the person presents clinically significant distress and impairment (e.g. symptoms are not experienced often enough or for a sufficiently long period). UFED is a broad category that covers other feeding and eating problems that do not meet the criteria of any other categories or when there is not sufficient information available at the time of the diagnosis. A recent systematic literature review of 94 studies on the prevalence of different EDs over the 2000–2018 period and across 3 continents (Americas, Asia and Europe) (Galmiche et al., 2019) has estimated that the prevalence of lifetime EDs (proportion of individuals affected by EDs at any time in life) is 8.4% for women and 2.2% for men, although the prevalence rates of EDs vary considerably across studies as a result of a variety of methodological shortcomings (Lindvall Dahlgren and Wisting, 2016).
Treatment options vary according to the specific type of ED. In the United Kingdom, according to the National Institute for Health and Care Excellence guidelines (NICE, 2017), treatments for anorexia nervosa should include psychoeducation; involve monitoring of weight, mental and physical health and other risks linked to the disorder; be multidisciplinary; and coordinated between services and involve the carers/family. The recommended treatment options are psychological therapies, including individual ED-focused cognitive behavioural therapy (CBT-ED), Maudsley Anorexia Nervosa Treatment for Adults (MANTRA) or specialist supportive clinical management (SSCM). When these options are not adequate or possible, ED-focused focal psychodynamic therapy (FPT) is also recommended.
In relation to bulimia nervosa, NICE (2017) recommends guided self-help as the first option. If self-help is unacceptable, contraindicated, or ineffective after 4 weeks of treatment, CBT-ED is the recommended therapeutic pathway and a recent meta-analysis suggests that individual CBT-ED is the most effective treatment for bulimia nervosa (Slade et al., 2018). In relation to binge-eating disorder, NICE (2017) recommends that psychological treatments have a limited effect on body weight and that weight loss is not a therapy target in itself. Instead, binge-eating disorder focused guided self-help programmes are advised. If guided self-help is not adequate or ineffective after 4 weeks, group CBT-ED is recommended. For these three types of ED, medications are not recommended to be used as the sole treatment pathway, and recent research suggests that, at present, there is no convincing evidence about their effectiveness (Himmerich and Treasure, 2018; Slade et al., 2018).
Even though significant progress has been achieved in the development of ED-focused, evidence-based interventions, many people living with EDs do not receive treatment (Ali et al., 2017; Kazdin et al., 2017), with research suggesting that 77% of individuals do not seek ED-specific treatments for their condition (Hart et al., 2011). Furthermore, the success of current interventions for EDs is very limited (Guarda, 2008; Himmerich and Treasure, 2018). Indeed, approximately half of patients will not recover following an adequate, evidence-based treatment course (McCallum, 2010; Steinhausen and Weber, 2009) and many people with EDs do not undergo any type of treatment (Strober and Johnson, 2012; Vitousek et al., 1998). Hence, it is important to explore other forms of therapies that are effective and have the potential to be well accepted by people with EDs.
One such treatment pathway is Music Therapy (MT), which has been used to treat people with a variety of EDs (Pasiali et al., 2020). There is some evidence that MT can aid recovery for people experiencing anxiety, low self-worth, and body-image challenges, which are often associated with EDs (Pasiali et al., 2020). Literature in this field includes a plethora of case illustrations describing a vast number of approaches to treating people with EDs. According to Heiderscheit (2015), these approaches can be broadly classified into four core psychological approaches/theories, each related to specific beliefs about causation (indicated in brackets): (1) psychodynamic (EDs as the result of unresolved issues), (2) humanistic (EDs as the result of genetic predispositions), (3) cognitive-behavioural (EDs as the result of cognitive dysfunction), and (4) ecological (EDs as the result of responses to external pressures). Based on these theoretical approaches (and the specific individualised goals of the therapy), Music Therapists employ a variety of MT techniques to treat clients with EDs. These include improvisation, songwriting, music assisted relaxation and imagery, singing, and music performance (Pasiali et al., 2020; Heiderscheit, 2015).
Although promising, most literature reporting the use of MT to treat people with EDs is exploratory and seems to emanate from case studies and reports (c.f. McFerran and Heiderscheit, 2016). This descriptive type of evidence is rich and valuable, but it is also important to explore evidence from quantitative experimental studies to investigate the efficacy of different MT approaches to support people living with EDs. In this context, the central aim of this research is to summarise the evidence from published experimental controlled studies where MT (delivered by qualified Music Therapists) has been used to treat people diagnosed with any type of ED. As we expected evidence from experimental controlled studies to be scarce, we also aimed to offer a set of recommendations for future high-quality experimental studies in this area that could inform the development of effective interventions and support for people with EDs. Note that another relevant review on the same topic (Testa et al., 2020) was published after we commenced this work. The conclusions of that review as well as the additional contributions of our work will be also discussed.
Methods
This systematic review was conducted by a multidisciplinary team comprising a Music Psychologist, a Music Therapist, an NHS Consultant Forensic Psychiatrist (specialised in Mental Health) and three evidence synthesis experts (specialised in health-related topics).
Protocol and registration
This review was conducted and reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Statement (PRISMA 2020) (Page et al., 2021). The study was registered in the PROSPERO database (record number CRD42020215761; Coutinho et al., 2020).
Eligibility criteria
Studies were included if they met the following criteria:
The study population included people (of any age and gender) diagnosed with any type of EDs.
Interventions were described as formal MT (such as Nordoff-Robbins or any other MT model recognised by relevant professional bodies) and delivered by qualified Music Therapists (i.e. registered in relevant professional bodies, such as the British Association for Music Therapy)
A control group was present that received any other intervention, treatment as usual or was defined as a non-exposed control group.
Outcomes of the studies could be quantitative and/or qualitative, but had to be related to ED psychopathology and/or symptoms.
Studies had to be written in English, Dutch, German or French.
Studies were excluded using the following criteria:
The study simply describes a group or examines relationships between pre-existing groups and/or lacks the manipulation of one or more independent variables (e.g. systematic reviews, meta-analyses, surveys and case reports).
Information sources
A systematic search was conducted using the electronic databases of MEDLINE (Ovid), Cochrane Library, CINAHL (EBSCOhost), Embase (Ovid), PsycINFO (EBSCOhost), Scopus, RLIM, and BASE. A combination of the following free text words and Medical Subject Headings were used: music therapy, music*, feeding and eating disorders, food addiction, anorex*, bulimi* (see Supplementary Table 1). The final search was performed in May 2020.
Study selection
Two researchers (T.V.C. and E.C.) screened all the titles and abstracts independently from one another, to assess eligibility from the pre-defined criteria. Full texts were then retrieved and evaluated based on the same criteria. Reference lists were manually screened to identify additional relevant studies. Discrepancies were discussed and resolved with a third independent researcher (R.H.).
Assessment of quality
Two researchers (T.V.C. and E.C.) assessed the risk of bias using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). In case of uncertainty at any point during the scoring process, consensus was sought by a third reviewer (R.H.). The MMAT is a tool designed for appraising quality of studies with a mixed method design, using either qualitative, quantitative or mixed measures. This tool is able to address methodological quality of five study designs: qualitative research, randomised controlled trials, non-randomised studies, quantitative descriptive studies, and mixed methods studies. All categories include two general questions concerning the research question and five questions based on the design. Answers are given as either ‘yes’, ‘no’ or ‘can’t tell’. In addition, following the suggestion by Ackley et al. (2008) the level of evidence was determined on a 7-point linear scale (I to VII), where I represents the highest level of evidence (systematic reviews) and VII the lowest (expert opinions). While the extremes are not relevant to this review given that systematic reviews and expert opinions are excluded, the intermediate levels of this tool are still very relevant to describe and determine the level of evidence of experimental studies.
Data extraction and analysis
Extracted data included study design, participant characteristics (age, gender, diagnosis), intervention (type, intensity, duration) and outcome measures (type of outcome, timing of assessment). Results were categorised as either quantitative or qualitative. For quantitative results, mean (M) and standard deviations (SD) were extracted from pre- and post-intervention, as well as change (diff) scores. Regarding qualitative outcomes, a summary of the common themes presented in the results are reported alongside the number of participants reporting each theme.
Results
Study selection
In total, 1,992 studies were retrieved from the 8 databases. After deduplication 1234 studies remained, of which two met the inclusion criteria (Bibb et al., 2016). The study selection process is depicted in Figure 1.
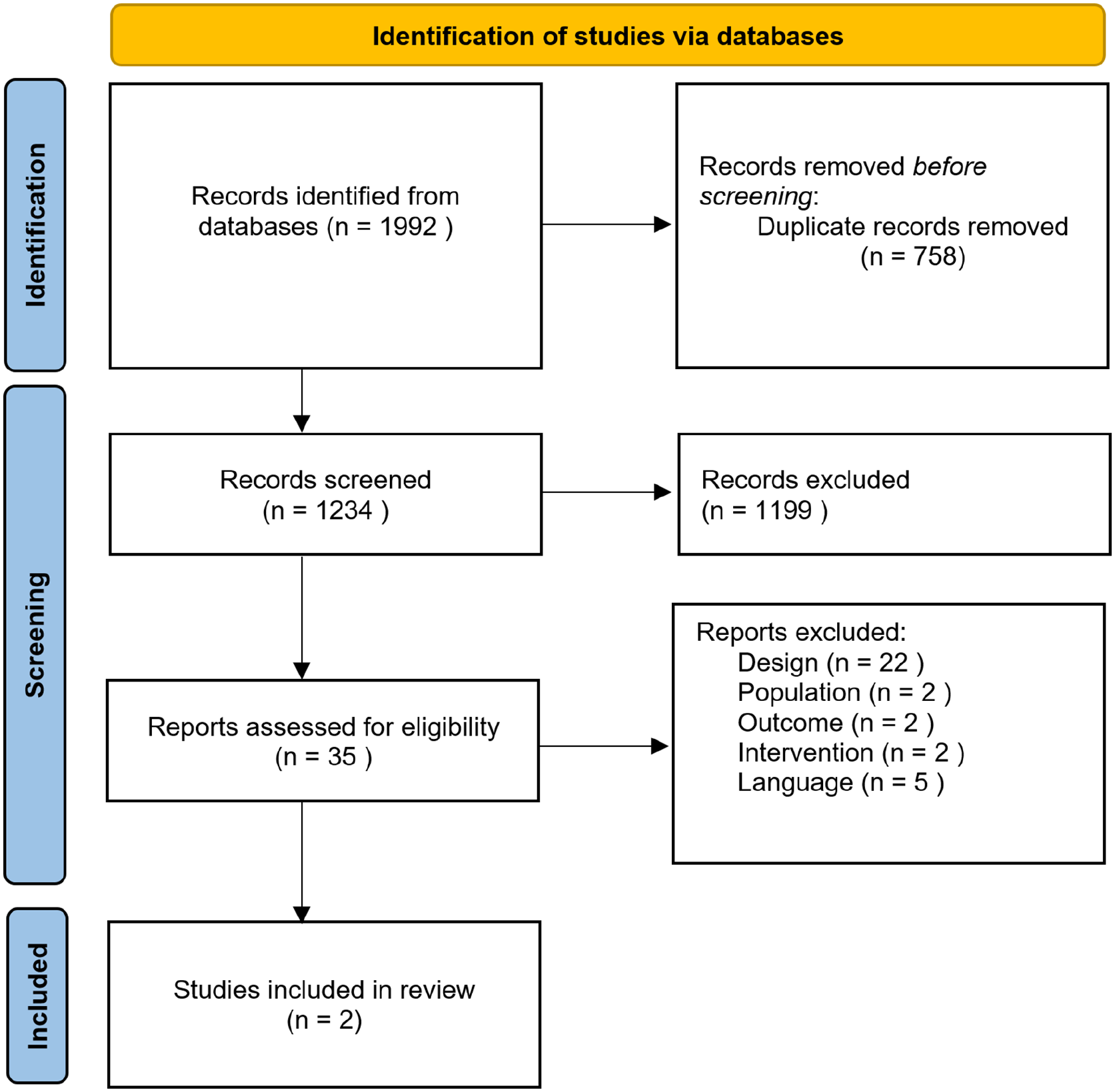
PRISMA flow diagram describing the article selection process.
Note that, although published separately, both sources report different outcomes of the same trial: Bibb et al. (2015) reports the quantitative results (Part I) and Bibb et al. (2016) the qualitative ones (Part II). Because of this, and given that the participants and intervention are the same, we will be referring to both sources as a single study.
Quality assessment
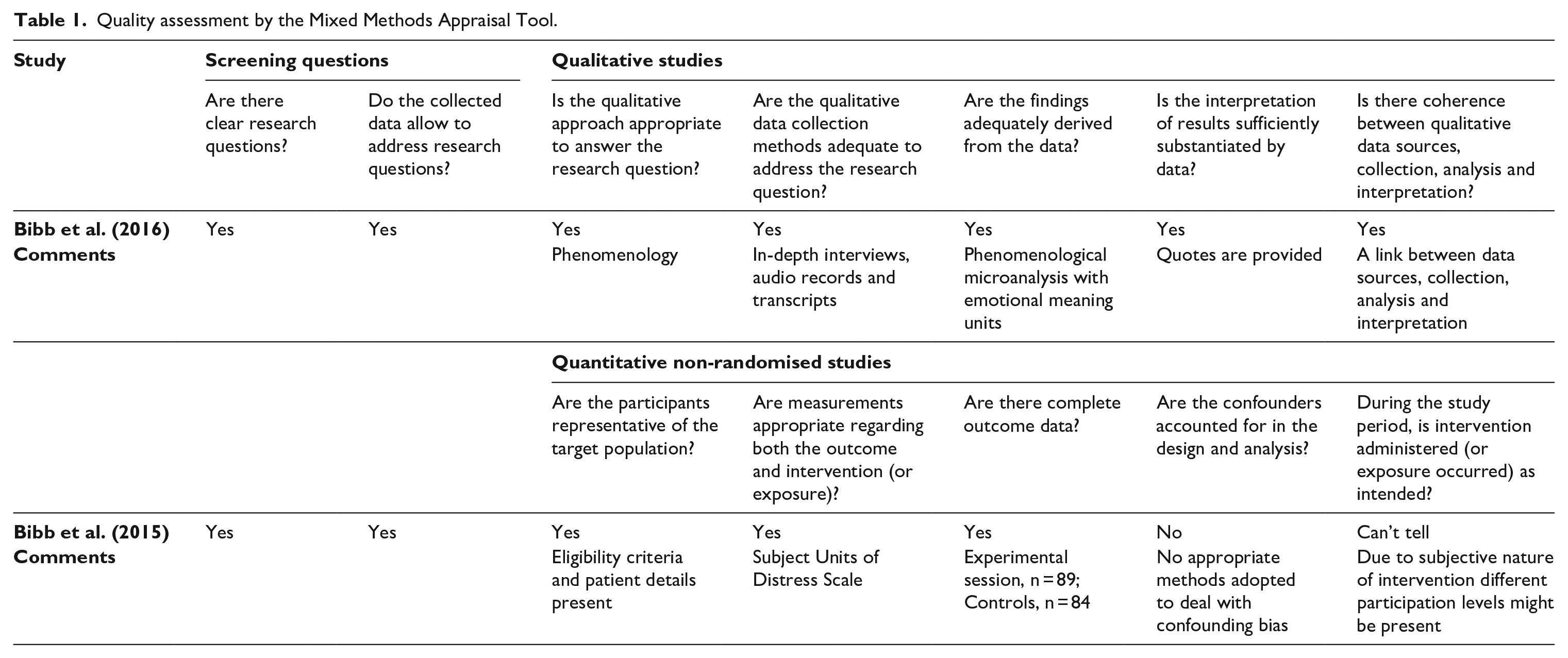
As the MMAT authors discourage researchers to calculate an overall score, an overview of the answers per questions are provided in Table 1. Part I of the study was assessed as a qualitative study and Part II as a quantitative non-randomised study. As it can be seen in Table 1, according to the MMAT, the overall methodological quality of the studies was high, and the level of evidence was rated at Level III on Ackley et al.’s (2008) hierarchy of evidence (maximum possible rating was Level II).
Quality assessment by the Mixed Methods Appraisal Tool.
Study overview
A total of 18 participants (1 male and 17 females) with ages ranging from 20 to 58 years took part in the included study. The intervention was conducted within the Body Image Treatment & Recovery Service in the Adult Acute Psychiatric Unit of the Austin Hospital in Melbourne (Australia). It consisted of post-meal supported MT group sessions for the inpatients, delivered by a Registered Music Therapist. The sessions lasted 1-hour and were held immediately after lunch, twice per week. During these sessions, participants were encouraged to participate in musical activities (singing, listening to, and writing songs) and talking to others about music. The goal of these sessions was to move the focus away from the mealtimes and allow the participants to develop coping skills through music.
The study included a control condition consisting of structured post-meal support therapy (treatment-as-usual). These group sessions were delivered by nursing and allied health staff took place 3 days per week after mealtime, and focused on the discussion of feelings, providing encouragement to focus on achieving the goals of admission and group activities (e.g. games, art). Note that the same participants participated in both conditions: 2 days a week of MT and 3 days a week of treatment-as-usual.
Results summary
The aim of the study was to evaluate the impact of MT on post-meal subjective distress (measured using the Subjective Units of Distress Scale; SUDS) and to understand participants’ experiences of MT during the same period. The authors employed a mixed-method approach using (1) a quantitative non-randomised pre-post design comparing MT with treatment as usual following mealtime (reported in Bibb et al. (2015); Part I) and (2) a qualitative component consisting of semi-structured interviews (conducted after participants were discharged from the hospital) that explored their experience of MT after mealtime (reported in Bibb et al. (2016); Part II). The results of the study are summarised in Table 2.
Summary of the included studies.
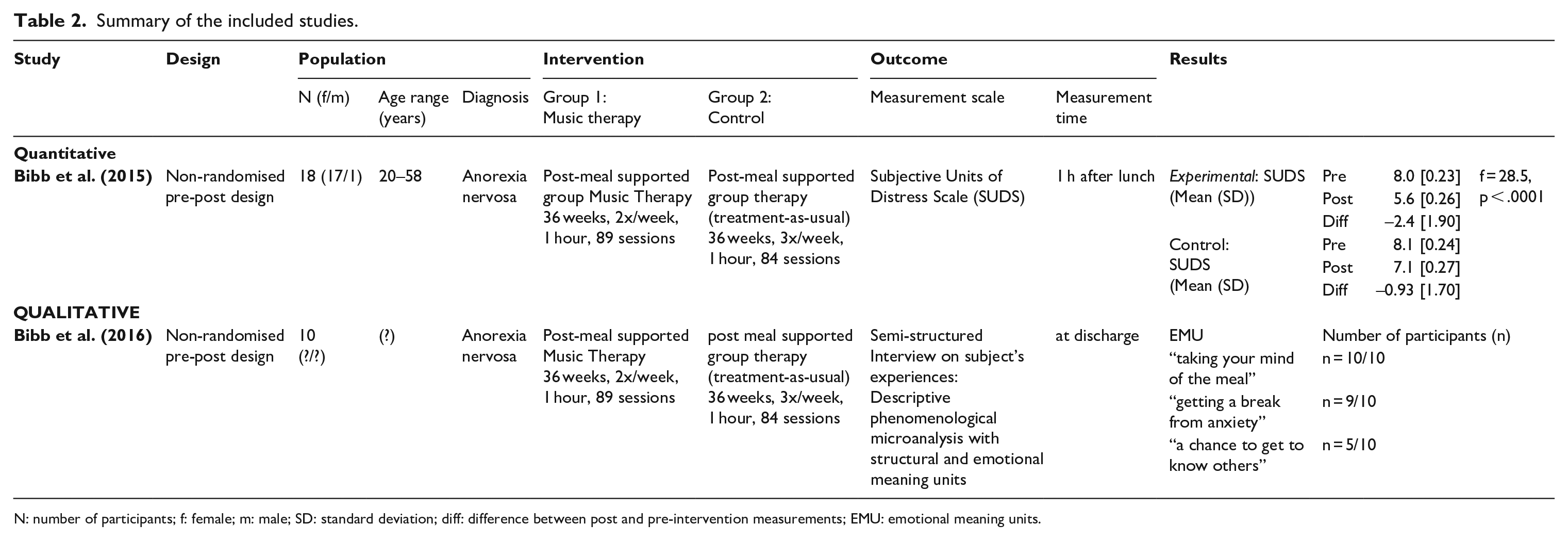
N: number of participants; f: female; m: male; SD: standard deviation; diff: difference between post and pre-intervention measurements; EMU: emotional meaning units.
Part I (quantitative data reported in Bibb et al. (2015)) shows significant reductions in distress (according to the SUDS) for both MT (M (Post-Pre) = 2.40; SD = 1.90) and control (M (Post-Pre) = –0.93; SD = 1.70) groups, and that this reduction was significantly larger in the MT sessions than the control group (f = 28.5, p < .0001). In relation to the qualitative data reported in Bibb et al. (2016), all participants interviewed (N = 10) reported that MT helped them to take their mind off the meal. Example statements included ‘it’s easier to get distracted from the uncomfortable feeling after meals’, ‘it’s a good distraction from the experience of having eaten’, ‘it’s a way to distract from other things and worries’. Almost all participants interviewed (N = 9) also reported a reduction in anxiety – they stated that ‘you get a break from anxiety for that time, and you feel lighter at the end’ and it helped them to relax. Furthermore, half of the participants interviewed (N = 5) described MT as a chance to get to know others (e.g. ‘it is easier with music because it just kind of opens up your heart straight away and it’s really helpful to engage with other people’). Taken together, both qualitative and qualitative results indicate that MT is associated with an improvement in participants’ post-meal stress and anxiety levels. This seemed to be related to MT distracting the participants from meal-related and other negative thoughts, inducing relaxation, and facilitating socialisation.
Discussion
Our findings show that only one controlled trial has examined the effectiveness of MT interventions for people living with EDs. This study reported that group MT immediately after meals was associated with a reduction in post-meal anxiety in a group of inpatients with anorexia nervosa, and that this intervention was more effective than standard post-meal support therapy. Moreover, participants reported that MT sessions helped them to forget about meals, reduce anxiety and connect to others.
Clearly robust evidence concerning the effectiveness of MT for the treatment of EDs is severely lacking. However, the evidence described in this paper, the positive indications from various uncontrolled studies (cf. Testa et al., 2020) and the many case studies reported in the literature (cf. Heiderscheit, 2015) warrant further investigation about the effectiveness of MT for EDs. It seems that new treatment strategies for EDs require urgent investigation, particularly given the high, and increasing, prevalence rates (Galmiche et al., 2019). Nonetheless, in order to develop a robust and consistent body of evidence for MT, there are a few key factors that need to be considered in the design of these studies.
Directions for future studies
Although a variety of types of evidence contribute to MT literature and its clinical effectiveness (like other arts therapies), MT is not predominantly based on the biomedical hierarchical model of evidence-based practice (Bradt, 2012). We suggest that future research in this area should adopt robust experimental methodologies in order to provide high-quality evidence, that is, the type of evidence may be required by MT employers and healthcare commissioners and providers. In this context, we suggest that the priority for future evaluations should focus on randomised control trials (RCTs) as they allow attribution of the observed effects to the treatments being compared. Moreover, control groups should also be chosen carefully and we suggest that they include not only the typical support provided in specific settings, but also the recommended types of treatment by national health organisations (e.g. NICE, 2017). We also suggest that the practical guidelines for the design and implementation of RCTs created by Bradt (2012) for MT researchers are an important starting point to design rigorous studies that adequately estimate MT treatment benefits while adapting their design to the realities of MT practice. If MT is integrated within a complex service provision, then the researchers would be well-advised to take account of guidelines for complex interventions (e.g. Skivington et al., (2021)).
Another key feature that we believe is important for future research in this area is the adoption of mixed methods in RCTs. One the one hand, quantitative measures of specific outcomes related to the theoretical framework adopted, and the hypothesised mechanisms of action (Robb et al., 2011), can provide much-needed robust evidence. On the other hand, qualitative evidence can be used to better understand the measured outcomes, identify other outcomes relevant to the participants prior to or after the study, as well as to further explore different aspects related to feasibility, acceptability and implementation of MT interventions. It can also help to inform strategies to improve recruitment and retention rates (Cathain et al., 2013; see also Richards et al. (2019) regarding the integration of quantitative and qualitative data and findings in the context of RCTs). More generally, qualitative evidence can also allow Music Therapists to better measure outcomes related to the diverse philosophical and theoretical orientations of their clinical approaches (O’Callaghan, 1996). A parallel economic evaluation would inform decision-making of potential commissioners and providers of new MT services.
Another important aspect to consider is the types of data to be collected in these studies. As discussed by Attia and colleagues (Attia et al., 2017), there is lack of consistency in clinical diagnosis tools and outcome measures used, and adequate follow-up assessments are rare. Furthermore, the characteristics of treatment are often ill defined. In this respect, Attia and colleagues provide a set of guidelines and materials that should be considered for the design of new evaluation tools. These include information about participants characteristics (age, sex, ethnicity and race, and socio-economic status), the use of specific tools for diagnosis of EDs (e.g. DSM-5), the measurement of core features of the illness (and eventually functional assessments), detailed documentation of intervention characteristics, and follow-up assessment to determine the effectiveness of the interventions for supporting people living with EDs.
Limitations
There are a few limitations of this review that should be acknowledged. First, during the systematic literature search, only studies written in English, Dutch, German, or French were included. It is therefore possible relevant studies and important information was missed during the search process. Second, we only included studies in which the therapy was delivered by qualified Music Therapists. Whereas in this review we did not come across papers where this was an issue, it is possible that in future reviews relevant studies may be excluded if they do not report therapist credentials. Third, this review only includes one study and therefore no strong conclusions can be taken regarding the role of MT to help people living with EDs. This is relevant not only because there is little evidence in general, but also because there are a variety of MT approaches (i.e. methods and treatment models) that are not represented in this review. Finally, as mentioned in the introduction, between our search date and submitting this article, one relevant systematic review was published on the use of music for the treatment of EDs (Testa et al., 2020). Unlike our review, Testa and colleagues focus on music interventions more generally (e.g. music listening) including those not involving MT. Furthermore, they did not restrict their selections to controlled studies. The current review provides a focused summary of methodologically robust evidence from controlled studies that implement MT interventions for EDs. In addition, we have developed a comprehensive search strategy (that can be used in future updates of this review) and provide guidance for the future designs of rigorous evaluation studies.
Conclusion
In this review, we aimed to compile evidence from controlled studies that could shed light on the potential benefits of MT for the treatment of EDs. Only one study met our criteria, indicating that robust evidence on the effectiveness of MT interventions for people living with EDs is severely lacking. Nonetheless, evidence from this trial suggested that MT has the potential to help people living with EDs cope with post-meal anxiety, taking their minds off mealtimes and connect to others. Given the existence of other types of evidence from case reports and uncontrolled studies suggesting positive benefits of MT for individuals living with EDs, we suggest that future research attempts to generate more high-quality evidence on the effectiveness of MT interventions. In this article, we have outlined a series of factors that need to be considered for developing a robust and consistent body of evidence for MT for EDs.
Supplemental Material
sj-docx-1-bjm-10.1177_13594575221110193 – Supplemental material for Music therapy interventions for eating disorders: Lack of robust evidence and recommendations for future research
Supplemental material, sj-docx-1-bjm-10.1177_13594575221110193 for Music therapy interventions for eating disorders: Lack of robust evidence and recommendations for future research by Eduardo Coutinho, Tamaya Van Criekinge, Greg Hanford, Rajan Nathan, Michelle Maden and Ruaraidh Hill in British Journal of Music Therapy
Footnotes
Acknowledgements
This work was partially supported by the University of Liverpool’s Knowledge Exchange & Impact Voucher scheme (2020).
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.