
Abstract
Bias among healthcare professionals (HCPs) may shape infant feeding recommendations and influence maternal decision-making, with consequences for maternal and infant health. This study assessed implicit and explicit infant feeding attitudes among HCPs in the UK and Ireland using an online cross-sectional survey (n = 66). Demographic information was collected, implicit attitudes were measured with the Infant Feeding Implicit Association Test, and explicit attitudes with the Iowa Infant Feeding Attitude Scale. D-scores ranged from −0.88 to 0.46, indicating a general implicit bias favouring breastfeeding over bottle-feeding. Explicit attitudes were also broadly pro-breastfeeding (scores 52–85). No significant correlation was found between implicit and explicit attitudes, suggesting they may operate independently. HCPs of older age (r = 0.252, p < 0.05) and those currently breastfeeding or pregnant (r = −0.293, p < 0.05) exhibited pro-breastfeeding attitudes. Future research should investigate the underlying mechanisms and the impact of these biases on actual breastfeeding practices.
Keywords
Introduction
Infant nutrition forms the cornerstone of a child’s health and development, and breastfeeding serves as a vital aspect of this crucial stage. Extensive research (Ip et al., 2007; Victora et al., 2016) has shown the many benefits of breastfeeding for both mothers and infants. These include enhanced immune protection, reduced risk of infections and stronger maternal infant bonding; for the child specifically, breastfeeding is associated with improved cognitive development, while for mothers specifically, it predicts a lower risk of postpartum depression, breast and ovarian cancer, and type 2 diabetes (Ip et al., 2007; Takahashi et al., 2017; UNICEF Ireland, 2023). Despite these established advantages, global exclusive breastfeeding rates for the first 6 months of life remain at a concerning 40%, according to the World Health Organization (WHO) (2023). Furthermore, a WHO survey analysis revealed that only 30%–60% of infants experienced early initiation of breastfeeding within the first hour after birth, a practice highly recommended for optimal health outcomes in both mothers and babies (Takahashi et al., 2017; WHO, 2023).
According to the World Breastfeeding Trends Initiative (WBTI), Ireland and the UK together have the lowest rate of breastfeeding in the world, with less than 1% of infants still feeding at 12 months of age (World Breastfeeding Trends Initiative (WBTi), 2023). These statistics fall significantly short of the WHO recommendations of 100% exclusive breastfeeding until 6 months and continued breastfeeding in combination with appropriate complementary foods until 2 years of age and beyond. While breastfeeding was the predominant practice a century ago, according to UNICEF Ireland (2023), the widespread availability of commercial milk formula (CMF), coupled with increasingly aggressive and often manipulative marketing strategies, has emerged as a significant contemporary challenge to optimal infant feeding practices (Rollins et al., 2016).
In the UK and Ireland, breastfeeding faces significant cultural stigmatisation rooted in transgenerational practices and social norms. Irish mothers report feeling ashamed and embarrassed about breastfeeding in public and even around friends and family, with many hiding in public toilets or concealing the practice (Leahy-Warren et al., 2017). The perception that breastfeeding is embarrassing has been identified as a barrier to initiation (Tarrant et al., 2010), reinforced by social reactions where friends call it disgusting or family members disapprove (Leahy-Warren et al., 2017). Women are sensitive to their own embarrassment and to others’ discomfort (Desmond and Meaney, 2016), adopting an ‘etiquette’ of seeking private spaces despite legal protections. This cultural attitude underlies the exceptionally low breastfeeding rates of less than 1% at 12 months in the UK and 2% in Ireland (Philip et al., 2023). The shift to widespread formula use, driven by commercial marketing and institutional practices including coercive breastfeeding management in mother-and-baby homes, has left multiple generations with limited exposure. Lack of family role models and community knowledge reinforces formula feeding as the default (Bender, 2021; Tarrant et al., 2008). Multigenerational inexperience, negative attitudes, and historical trauma have normalised formula feeding whilst stigmatising breastfeeding.
In the UK and Ireland specifically, several factors influence a woman’s decision to breastfeed. These include cultural and family influences, perceived difficulties with breastfeeding, and the need for practical support (Brown et al., 2011; Twamley et al., 2011). Healthcare professionals (HCPs) play a key role in the latter respect, guiding mothers through infant feeding options, and offering support and information. However, HCPs also face challenges such as lack of time and resources (Baker et al., 2021). There is a critical need for more informed and empathetic engagement from HCPs, alongside broader efforts to normalise breastfeeding within clinical and community settings (Health and Social Care Northern Ireland (HSCNI), 2015). This concern is substantiated by findings from the World Breastfeeding Trends Initiative UK (2024) Report and the WBTi (2023) Report, both of which highlight significant gaps in breastfeeding-related training at undergraduate and professional development levels. These deficiencies may contribute to a clinical environment wherein families experience care that is perceived as pressurised or lacking in continuity (Shortt et al., 2013). Surveys suggest high breastfeeding support from various HCPs, with studies surveying populations such as physician mothers (Sattari et al., 2020), reviewing support from HCPs and lay peers (McFadden et al., 2019), and consulting with multidisciplinary health staff like midwives and health visitors (HSCNI, 2015) However, breastfeeding rates in the UK and Ireland remain significantly lower than the global average. According to the WHO, 48% of infants worldwide are exclusively breastfed for the first 6 months. However, in the UK (McAndrew et al., 2012), fewer than 1% of infants continue breastfeeding at 12 months, making it one of the lowest rates globally. Ireland faces a comparable challenge, with only 2% of infants being breastfed at 12 months (Health Service Executive (HSE), 2024).
This discrepancy between reported support on the part of HCPs and observed behaviour on the part of those they advise might indicate the influence of implicit bias among HCPs WHO (2023) and UNICEF UK Baby Friendly Initiative (2023). Implicit bias refers to unconscious attitudes or preferences that subtly influence our thoughts and behaviours without our conscious awareness Greenwald and Banaji (1995). These biases can manifest in various aspects of our lives, including with respect to social groups (e.g. race, gender), objects (e.g. brands), and even abstract concepts (e.g. intelligence, risk).
Recent research investigated the presence of implicit biases among HCPs. A systematic review by FitzGerald and Hurst (2017) specifically examined implicit biases, with a primary focus on racial and ethnic biases among HCPs in the UK and Ireland. The review found that racial and ethnic minorities often received different treatment in pain management, referrals, and assessments of compliance. Implicit biases also affected communication quality, trust, and access to care, contributing to systemic inequalities despite efforts to provide fair treatment.
Research by Blair et al. (2013) found that implicit racial bias could lead to misdiagnosis in Black patients compared to White patients. Similarly, Cooke and Halberstadt (2021) demonstrated that implicit bias could influence treatment recommendations, with Black patients receiving fewer referrals for specific procedures compared to White patients with similar conditions. Furthermore, communication patterns can also be affected by implicit bias, as seen in the Blair et al. (2013) study, where physicians displayed less patient-centred communication towards Black patients compared to White patients.
Such findings indicate the potential influence of implicit bias in healthcare, emphasising the need for ongoing efforts to raise awareness and develop effective strategies to mitigate its impact on patient care. The presence of biases among HCPs, whether conscious or unconscious, could also significantly influence the advice and recommendations provided to mothers, potentially shaping their decisions (Green et al., 2015; Grol et al., 2007; McFadden et al., 2019; Spector et al., 2017). With respect to advice on breastfeeding for example, biases could manifest in problematic downplaying of breastfeeding advantages and the portrayal of formula feeding as an equally effective alternative, despite established differences in immunological and developmental benefits.
Hence, bias on the part of HCPs could negatively impact practice with respect to advice on infant feeding. To address this phenomenon, the present study examined infant feeding bias among HCPs in the UK and Ireland, specifically concerning whether there might be a tendency to favour breastfeeding or bottle-feeding. We explored explicit attitudes using an already established test, namely the Iowa Infant Feeding Attitude Scale (IIFAS), while we explored implicit attitudes using an adapted version of the IAT, which we refer to as the Infant Feeding Implicit Attitudes Test (IFIAT). In so doing, we sought to better understand the presence of implicit bias in HCPs and its potential impact on infant feeding practices. By examining these biases, we sought to provide insights that might help inform future strategies to address bias with respect to breastfeeding in healthcare settings. Ultimately, this research aims to contribute to the development of evidence-based approaches to ensure that mothers receive clear, unbiased guidance and information when making infant feeding decisions.
Methods
The present study adopted a quantitative approach utilising a survey methodology with online self-administered questionnaires to investigate implicit and explicit bias towards infant feeding among HCPs in Ireland and the UK. We included HCPs aged 18 or older who were actively involved in healthcare delivery across Ireland & the UK, including a number of allied professions (e.g. doctors, nurses, breastfeeding consultants, etc.). Ethical approval for this study was obtained from an institutional review board at the lead researcher’s university. All participants provided informed consent electronically before participating in the online survey. The study complied with institutional and international ethical guidelines for research involving human subjects. Participants were recruited through online breastfeeding-positive communities, including professional forums, social media groups, and mailing lists, with some administrators facilitating survey distribution. No physical organisations were approached. To minimise ineligible or fraudulent responses, access was restricted to users in Ireland and the UK via IP address verification; screening questions confirmed professional status and country of practice; and attention checks detected inconsistent or automated responses. Participants failing the eligibility criteria were excluded. Following Greenwald et al.’s IAT guidelines, responses with reaction times <300 ms or >10,000 ms were also removed to ensure data validity. We shared the survey through social media in breastfeeding positive communities. The survey consisted of three parts.
(i) Demographics questionnaire
Demographic data (age, gender, professional role, years of clinical experience, and country of practice) were collected using a structured questionnaire developed for this study. Items were informed by demographic measures used in previous research on healthcare professionals’ infant feeding attitudes (McFadden et al., 2019; Sattari et al., 2020) ensuring relevance and comparability. Standardisation was achieved through identical fixed-response questions presented in a uniform order with predefined response options. The questionnaire was administered online via a single platform with consistent instructions, and completion of all demographic items was required before progressing to the IIFAS and IFIAT measures. The questionnaire was pilot tested with healthcare professionals before data collection, leading to minor wording refinements to improve clarity.
(ii) Infant Feeding Implicit Association Test (IFIAT)
In the IFIAT, participants were required to categorise the concepts of breastfeeding versus bottle-feeding in two separate conditions. In one condition, images of breastfeeding (Figure 1) had to be paired with positive attributes (Table 1) and images of bottle-feeding (Figure 2) with negative attributes (Table 1). In a second condition, bottle-feeding images had to be paired with the positive attributes and breastfeeding with negative ones.

Target concept 1: stimuli of breastfeeding.
List of positive/negative attributes used in the IFIAT.

Target concept 2: stimuli of bottle-feeding.
This test is an adaptation of the Implicit Association Test (IAT), originally developed by Greenwald et al. (2003) to measure automatic associations between concepts. The D-score is a metric used in the IAT to quantify the strength of an implicit association between two concepts. In the present study, the D-score was based on the difference in reaction times between the two conditions described so that if a participant was faster in the first condition than the second, then this showed a pro breastfeeding bias (=a negative D score). In contrast, if they were faster in the second condition than the first, then this indicated a pro bottle-feeding bias (=a positive D score). Larger D-scores showed stronger bias. The full range of the IAT is from −2 to +2.
Developing a mobile-friendly IFIAT presented unique challenges due to the limitations of screen size and user interaction methods compared to traditional desktop computers. To address these challenges, we improved the IFIAT interface so that it automatically adapted to various screen sizes and resolutions. Buttons and other interactive elements were enlarged and spaced appropriately, and instructions were summarised and presented in clear, concise and easy to-read fonts. These changes facilitated a smooth user experience for participants and ensured reliable data collection regardless of the device used to access the IFIAT.
(iii) Iowa Infant Feeding Attitude Scale.
This online measure assessed participants’ explicit attitudes towards breastfeeding. The Iowa Infant Feeding Attitude Scale (IIFAS) de la Mora et al. (1999), is a well-established tool in this domain. Participants were presented with a set of 17 pre-defined statements about breastfeeding practices and asked to indicate their level of agreement/disagreement using a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree; Figure 3).
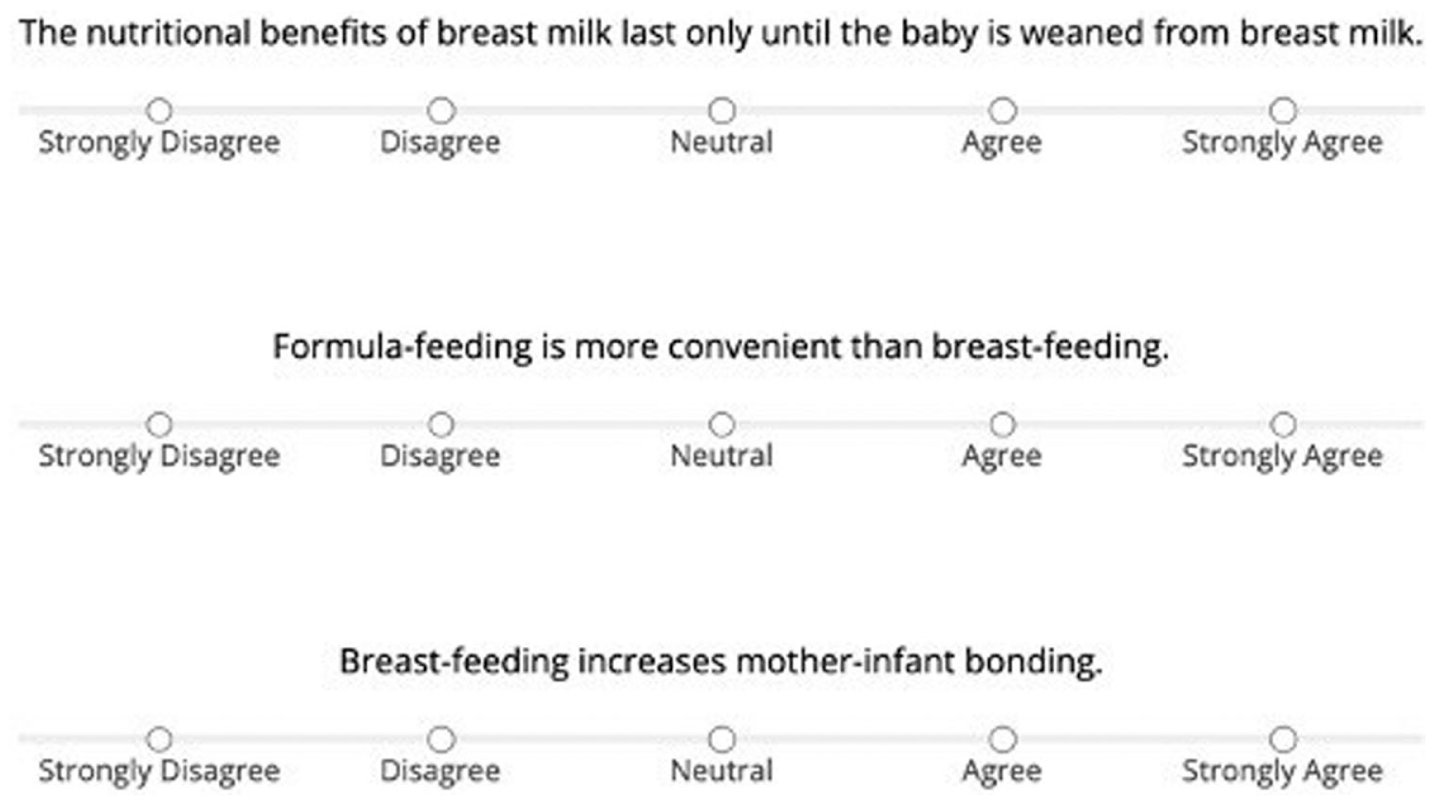
Example predefined Likert scale statements assessing attitudes towards breastfeeding practices.
Results
Table 2 shows information on participants that was collected via the demographic questionnaire. A total of 66 HCPs, aged 24–71 years (M = 43.95, SD = 10.67), were included in the survey. To ensure data quality, participants who did not complete the entire survey or who completed the IFIAT too quickly (responses took less than 300 ms) or too slowly (responses took more than 10,000 ms) were excluded.
Demographic characteristics of participants.
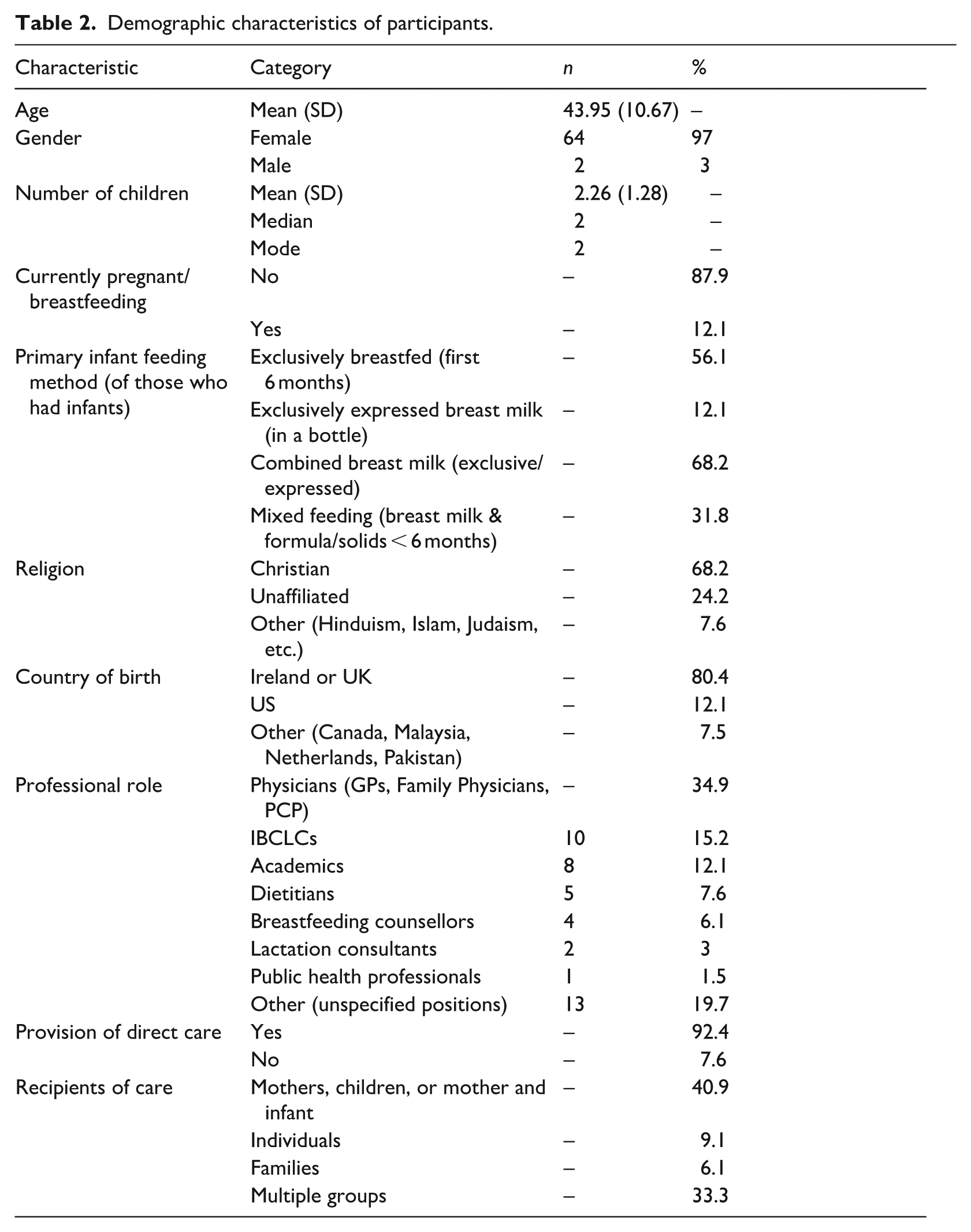
The most common recipients of care were mothers, children, or mother and infant (40.9%), followed by individuals (9.1%) and families (6.1%). A considerable proportion of respondents (33.3%) provided care to multiple groups.
Participants reported having between 0 and 6 children, with a mean of 2.26 children (SD = 1.28). The median number of children was 2, and the most frequently reported number was 2. Only 12.1% of respondents reported being pregnant or breastfeeding at the time of the study. Most respondents (56.1%) reported exclusively breastfeeding their infants in the first 6 months. Another 12.1% exclusively expressed breast milk in a bottle. Combined, these groups represent 68.2% of respondents who primarily relied on breast milk for infant feeding. A significant portion (31.8%) of respondents reported mixed feeding, combining breast milk with formula or solids introduced before 6 months.
IFIAT D-scores ranged from −0.88 to 0.46 (indicating implicit attitudes towards breastfeeding), with a mean of −0.37 (SD = 0.2775). These scores were consistent with the typical range observed in IAT research, falling within the −1 to +1 range. This aligns with established norms and provides confidence in the reliability of the measurement (Karpinski and Hilton, 2001). The negative mean suggests a tendency towards implicit bias in favour of breastfeeding among HCPs in our sample.
Figure 4 shows IFIAT D-scores. Most scores in the distribution fall on the negative side, suggesting a mild to moderate preference for breastfeeding or against bottle-feeding amongst the HCPs surveyed, while a few participants exhibited neutral or slight biases towards formula feeding.
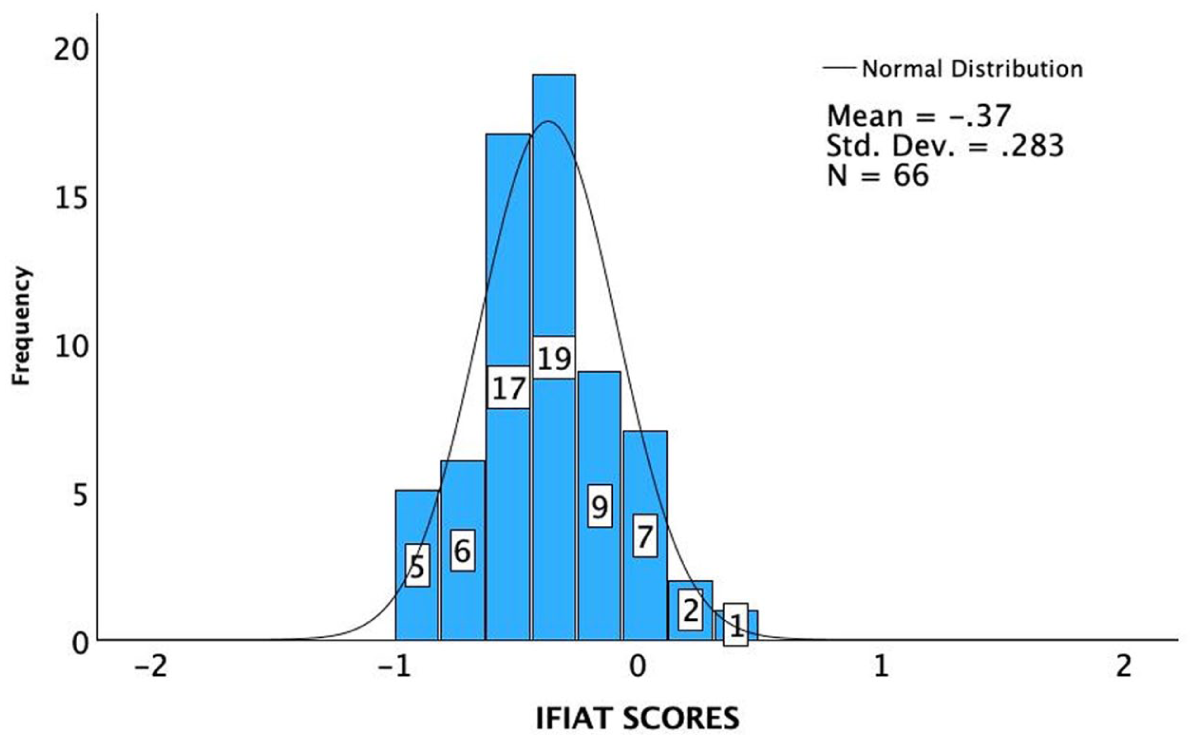
Implicit bias towards breastfeeding.
Explicit attitudes measured using the reversed IIFAS score (Min = 17, Max = 85), exhibited a range of 52–85, with a mean of 74.53 (SD = 7.34). This indicates an overall positive and supportive attitude towards breastfeeding in the explicit measures. The reliability of the IIFAS used to assess attitudes towards breastfeeding was evaluated using Cronbach’s Alpha. The analysis included all 17 Likert items, with a total of 66 valid cases, representing 100% of the sample. No cases were excluded. Cronbach’s Alpha for the IIFAS was 0.786, indicating acceptable reliability (Cronbach’s Alpha > 0.70). The distribution of IIFAS scores is shown in Figure 5. This distribution shows a slight positive skew, with a tendency towards higher scores.
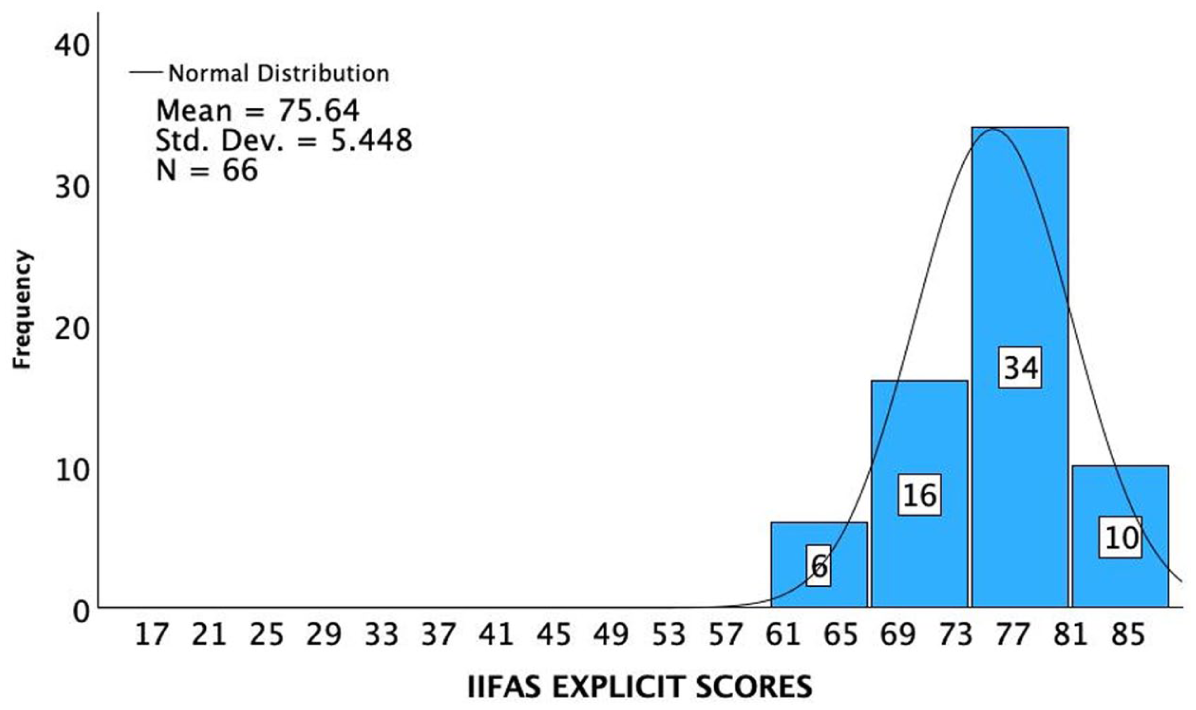
Explicit bias towards breastfeeding.
This suggests that a significant portion of HCPs held pro-breastfeeding attitudes. The spread also indicated some diversity in these attitudes, with outliers on both sides of the distribution. Figure 6 shows the relationship between implicit bias, as measured by IFIAT scores, and explicit attitudes, assessed using the IIFAS. A Pearson’s correlation coefficient of (r = −0.054, p > 0.05) indicated no significant correlation, suggesting that implicit and explicit attitudes were independent in this context. This suggests that in some cases, HCPs might consciously endorse breastfeeding but still hold unconscious biases that might potentially influence their clinical interactions and recommendations. Explicit attitudes were positively correlated with respondent age (r = 0.252, p < 0.05) while implicit attitudes were negatively correlated (r = −0.293, p < 0.05) with respondents’ current breastfeeding or pregnancy status.
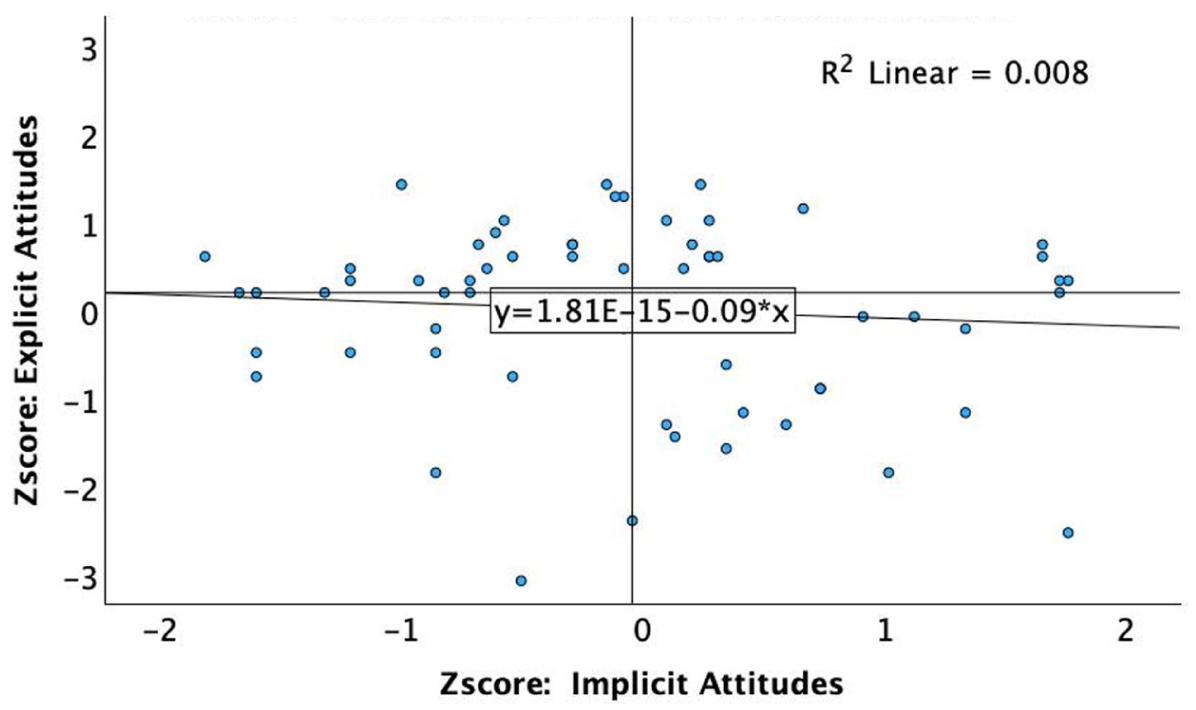
Scatter plot between D scores and explicit attitudes.
Discussion
Our study explored both implicit and explicit infant feeding bias among HCPs using an adaptation of the IAT (the IFIAT) and the IIFAS scale, respectively. Findings revealed a spectrum of bias towards breastfeeding (and/or against bottle-feeding), with a sizeable portion of HCPs exhibiting a pro-breastfeeding tendency for both implicit and explicit attitudes. However, the distribution of D-scores and the IIFAS histogram also indicated some diversity in attitudes, with some participants showing a bias against breastfeeding.
Findings showed that implicit biases related to breastfeeding among HCPs did not correlate with their explicit attitudes, indicating a potential disconnect between internal biases and expressed beliefs. This is consistent with previous findings reported in Karpinski and Hilton (2001), which showed no correlation between unconscious and self-reported attitudes. This suggests that in some cases HCPs might consciously endorse breastfeeding but still hold unconscious biases that might potentially influence their clinical interactions and recommendations. Specifically, while HCPs demonstrated strong pro-breastfeeding attitudes on the IIFAS, their implicit associations measured by the IFIAT were considerably weaker and more neutral, despite their explicit endorsement of breastfeeding. This dissociation may reflect social desirability bias, inflating explicit pro-breastfeeding attitudes, given professional expectations to align with WHO (2023) guidance. By contrast, Ireland’s entrenched formula-feeding culture and persistently low breastfeeding rates (Bender, 2021; Philip et al., 2023) may continue to shape automatic associations not fully addressed by professional training. Limited exposure to successful breastfeeding in clinical practice, alongside awareness of structural barriers such as inadequate parental leave and postnatal support (Baker et al., 2021), may contribute to neutral implicit responses despite explicit endorsement of breastfeeding benefits.
This explicit–implicit divergence has clinical relevance, as unconscious neutral biases may subtly influence counselling behaviours and non-verbal communication, potentially weakening breastfeeding support in practice. This discrepancy suggests the need for further investigation into the factors that might shape these divergent attitudes. Future qualitative research might uncover the specific dimensions of bias, which could then inform subsequent studies, using an adapted IFIAT, perhaps incorporating a modified set of attributes, for example, to explore these biases in greater depth.
The finding that HCPs of older age tend to have more positive explicit attitudes towards breastfeeding is intriguing. This may be due to generational differences in attitudes towards breastfeeding, or it may reflect changes in healthcare education and practice over time. Further research is needed to explore this relationship.
Perhaps unsurprisingly, HCPs currently breastfeeding or pregnant were found to exhibit pro-breastfeeding implicit bias. This suggests that personal experience can play a significant role in shaping implicit attitudes. More intriguing was the finding that older HCPs reported more positive breastfeeding attitudes, contradicting expectations that younger, recently trained professionals would demonstrate stronger support given contemporary emphasis on breastfeeding in healthcare education and updated WHO guidelines (UNICEF UK Baby Friendly Initiative, 2023; WHO, 2023). Research typically assumes recent training correlates with adherence to evidence-based guidelines (Linares et al., 2018), suggesting younger HCPs would show greater pro-breastfeeding attitudes. Our findings challenge this assumption. Older HCPs’ positive attitudes may reflect accumulated clinical experience witnessing long-term health outcomes, or training when breastfeeding was more visible in Irish clinical practice (Tarrant et al., 2008). Younger HCPs’ less positive attitudes likely reflect socialisation in contemporary Ireland, where formula feeding is normalised across generations (Bender, 2021; Philip et al., 2023), with limited breastfeeding exposure in personal or clinical environments. Younger professionals may also be influenced by debates framing ‘breast is best’ messaging as mother-shaming, tempering their support despite evidence- based guidelines.
Qualitative research exploring how HCPs’ attitudes evolved across their careers, what experiences shaped their views, and how cultural context influenced professional socialisation would clarify whether age effects reflect cohort differences, experience accumulation, or shifting professional norms, which are critical for designing targeted interventions addressing implicit bias.
The limitations of our study include the relatively small sample size and the dependence on self-reported data among pro-breastfeeding communities. Future research with larger and more diverse samples, employing both quantitative and qualitative approaches, could offer a more comprehensive understanding of infant feeding bias among HCPs. Addressing this gap is an important step towards ensuring that healthcare attitudes and practices remain aligned with current scientific evidence on breastfeeding (Rollins et al., 2016; Takahashi et al., 2017; UNICEF UK Baby Friendly Initiative, 2023; Victora et al., 2016).
Footnotes
Acknowledgements
The authors acknowledge the support of Atlantic Technological University (ATU) for funding this research. We thank Dr James Connolly (Computing, ATU) for guidance on the technological and empirical aspects of the study, and Dr Ian Stewart (Psychology, University of Galway) for expertise in research design and infant feeding bias methodologies. We also thank Dr Sarah Brennan (Breastfeeding Medicine) for her insights from a healthcare perspective and assistance with participant recruitment. We are grateful to all healthcare professionals who participated in this study.
Ethical considerations
Ethical approval for this study was granted by the Atlantic Technological University Research Ethics Committee.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the President’s Scholarship from the Atlantic Technological University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.