
Abstract
This systematic review synthesises psychological, social, and sociocultural factors related to disordered eating behaviour (DEB) during pregnancy. A search of 5 databases (Academic Search Ultimate (EBSCO), APA PsycInfo, PubMed, Scopus, and Web of Science) identified 40 quantitative studies (28 cross-sectional, 12 longitudinal) including 11,951 women, with sample sizes ranging from 39 to 1470. Methodological quality was assessed using the Newcastle-Ottawa Scale (NOS), while results were integrated through narrative synthesis. Significant psychological factors included depressive symptoms, anxiety, body dissatisfaction, adjustment towards pregnancy, and stress. Social factors encompassed perceived social support and relationship satisfaction with a partner, while sociocultural factors included thin-ideal internalisation, drive for thinness, and appearance comparison. Further research is still needed, as understanding the psychological, social, and sociocultural factors related to DEB during pregnancy is essential for developing effective prevention and intervention strategies to ensure adequate maternal and child health.
Keywords
Introduction
Disordered eating can occur at any stage of life, including during pregnancy. It involves distorted attitudes towards food, weight, and appearance (Pereira and Alvarenga, 2007), including problematic eating patterns such as dietary restraint, binge eating, emotional eating, and purging. These features are typical of individuals with an eating disorder diagnosis (ED), also of those with disordered eating behaviour (DEB), characterised by a lower frequency and intensity of these symptoms (Romano et al., 2020). ED prevalence during pregnancy is estimated to be around 4.3% (Çiçekoğlu Öztürk and Taştekin Ouyaba, 2023), while the prevalence of DEB may be several times higher and affect up to 30% pregnant women (Donofry et al., 2021). DEB during pregnancy have adverse health effects and can contribute to excessive maternal weight gain, gestational diabetes mellitus, and gestational anaemia (Chan et al., 2019; Young and Ramakrishnan, 2020). Moreover, the consequences of DEB may continue after pregnancy and have been linked to poorer health outcomes for both mothers and children in the postpartum period (Chen et al., 2017; Christian et al., 2024). Therefore, even when psychiatric symptoms during pregnancy do not meet diagnostic criteria, they still warrant attention due to their prevalence and possible effects on health (Sharma, 2024).
Disordered eating during pregnancy is a growing area of concern in mental health research. Different forms of EDs and DEB are often examined separately, as they appear to be shaped by somewhat distinct psychological mechanisms. In pregnant women with ED, relapses and persistent symptoms often appear to stem from issues such as identity conflict, stigma and a sense of losing control (Claydon et al., 2018). While for women experiencing DEB, symptom worsening seems to be tied more closely to pregnancy-related stressors or sociocultural pressures (Gerges et al., 2023). DEB also seems to occur more frequently overall, yet it is easy to overlook in clinical settings (Bannatyne et al., 2018), and symptoms can continue or even intensify during or after pregnancy (Chan et al., 2019; Easter et al., 2015). Taken together, these patterns indicate that a clearer understanding of the psychological, social and sociocultural factors linked to DEB may be important for improving theoretical models in this research area.
A previous systematic review reported a strong link between DEB during pregnancy and symptoms of depression and anxiety. It also highlighted relationship satisfaction and social support as possible prognostic factors, although the evidence remains inconsistent (Baskin and Galligan, 2019). Although this review provided important insights into the mental health and psychosocial correlates of disordered eating, it did not include sociocultural factors and did not differentiate the evidence for pregnant women experiencing ED and DEB. In addition, disordered eating during pregnancy may be influenced by pregnancy-specific factors, such as difficulties adapting to pregnancy or anxiety about birth plans, and these should be considered as well (Rockliffe et al., 2022). However, current knowledge of the psychological, social, and sociocultural factors related to DEB during pregnancy, including pregnancy-specific ones, remains limited.
More than 50 theoretical models have been proposed to explain the development of disordered eating, many of which emphasise psychological, social and sociocultural influences (Pennesi and Wade, 2016). One of the most known is the Tripartite Influence Model, which proposes that parents, peers and the media play a central role in shaping body dissatisfaction and disordered eating (Thompson et al., 1999). Another well-known model, the Dual Pathway Model, suggests that thin-ideal internalisation leads to disordered eating through dietary restraint and negative affect (Stice, 2001). Meanwhile, the Multidimensional model of disordered eating highlights the interaction of personal, interpersonal, and sociocultural variables in predicting DEB (Tylka and Subich, 2004). Although none of these models have been empirically examined in pregnant populations, pregnancy may shape their pathways in unique ways, highlighting the need to synthesise existing evidence on psychological, social, and sociocultural factors related to DEB.
Therefore, this systematic review aims to synthesise empirical research investigating psychological, social, and sociocultural factors related to DEB during a very specific period of a woman’s life – pregnancy. Following the Participants, Interventions, Comparators, Outcomes, and Study Design (PICOs) framework, this review addressed the following question: (P) pregnant women without medical conditions affecting DEB; (I) psychological, social, and sociocultural factors; (C) women differing in levels of these factors; (O) DEB during pregnancy; (S) quantitative studies with cross-sectional or longitudinal designs. When answering this question, this review can serve as a basis for the development of prevention and intervention strategies related to DEB during pregnancy, as well as shape future research in this area by identifying factors that are relevant but still need more attention. A comprehensive understanding of these factors can inform clinical practice, as pregnancy represents a critical period for intervention that may promote long-term healthy eating habits (Rockliffe et al., 2022).
Methods
Type of study
A systematic review method was used to review and synthesise the evidence on psychological, social, and sociocultural factors related to DEB during pregnancy. A systematic review design was chosen over a scoping review in order to allow for a structured and comprehensive synthesis of findings and to assess methodological quality of the included studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (updated; Page et al., 2021) and the Synthesis Without Meta-analysis (SWiM) guidelines (Campbell et al., 2020) were used to report the findings of this review.
Eligibility criteria
The inclusion and exclusion criteria were developed using the PICOs framework. Studies were included if they: (1) involved pregnant women without medical conditions affecting eating behaviour (e.g. gestational diabetes mellitus); (2) assessed DEB using validated self-report measures; (3) examined associations between DEB and at least one psychological, social, or sociocultural factor; (4) used quantitative cross-sectional or longitudinal designs. Studies were excluded if they: (1) examined eating disorders (participants had a diagnosis); (2) included only pregnant women with medical conditions or risk factors independently related to DEB (e.g. gestational diabetes, overweight, smoking); (3) did not report original quantitative data. When studies used overlapping samples, only the article with the largest dataset was retained.
Data sources and search strategy
Academic Search Ultimate (EBSCO), PubMed, Scopus, and Web of Science were searched from inception to August 1, 2024, with an updated search on 23 July 2025 including APA PsycInfo to capture psychology-related dissertations. The search strategy was developed by both review authors and employed the following terms: (‘pregnant women’ OR pregnancy OR pregnan* OR antenatal OR prenatal OR antepartum) AND (eating behavi* OR ‘disordered eating’ OR ‘disordered eating behavi*’ OR ‘eating problem*’ OR ‘eating symptom*’). The search in some databases was limited to source and population group. During the search, there were no restrictions on language, and papers written in languages other than English were translated using DeepL Translate (the full search strategy is provided in the Supplemental Material S1). Additionally, backward and forward citation searching of included studies was also performed to identify potentially missed articles.
Study selection and data extraction
Study selection and storage were made using the Rayyan tool. The duplicates were detected automatically by the programme and resolved by one author (EG). Titles, abstracts, and full texts were screened independently by both authors, with substantial inter-rater agreement (Cohen’s Kappa = 0.84). Discrepancies were resolved through discussion and a consensus on the inclusion of studies was achieved. Extracted data included the author and year of publication, the country in which the study was made, study and sample characteristics, analysed factors, outcome measure, and main results. Data extraction was completed by one author of the review (EG) and independently verified against the source articles by the other (AP).
Quality assessment of the included studies
A methodological quality analysis of included studies was performed by the first author (EG) and independently checked by the second (AP) according to quality aspects of the Newcastle-Ottawa Scale (NOS; Wells et al., 2000). NOS was initially developed for the assessment of case-control and cohort studies, but it is also suitable for the assessment of cross-sectional studies (Herzog et al., 2013). The NOS consists of three categories: ‘Selection’, ‘Comparability’, and ‘Outcome’. In the ‘Selection’ category, the appropriateness and representativeness of the research sample and participant selection are assessed. ‘Comparability’ stands for possible confounding factors, while ‘Outcome’ evaluates whether the results were determined using reliable methods. In the context of the present systematic review, we used the modified version of NOS. Full details of the modifications applied are provided in Supplemental Material S2.
Data synthesis and analysis
A narrative synthesis of the information obtained by thematic grouping across the different studies was performed. Narrative synthesis was chosen instead of a meta-analysis approach because of the substantial heterogeneity across the included studies in terms of design, outcome measures, and the wide variety of instruments used to assess psychological, social, and sociocultural factors. Additionally, narrative synthesis allows to identify consistent and conflicting evidence, highlighting patterns within psychological, social, and sociocultural domains.
Variables that were analysed in the included studies were grouped into several categories (psychological, social, and sociocultural factors) for simpler interpretation. In accordance with the literature on the topic (Tylka and Subich, 2004), psychological factors are considered as those which include a woman’s perceptions of her personality, cognitive, affective, and/or behavioural characteristics, as well as mental health indicators (e.g. depressive symptoms, anxiety, body dissatisfaction). Social factors characterise the woman’s assessment of relationship quality or interactions with others (e.g. spouse, family, peers). Sociocultural factors mean the woman’s perceptions of exposure to societal, cultural and/or media messages or influences.
Results
Search results
The final database search identified 7288 records. After duplicate removal, 4074 titles and abstracts were screened, and 71 full-text articles were assessed for eligibility (a list of excluded studies is provided in the Supplemental Material S3), leaving 36 articles that met the inclusion criteria. Overall, 40 studies were included in the review, with 4 studies identified through backward and forward citation searching (see Figure 1).
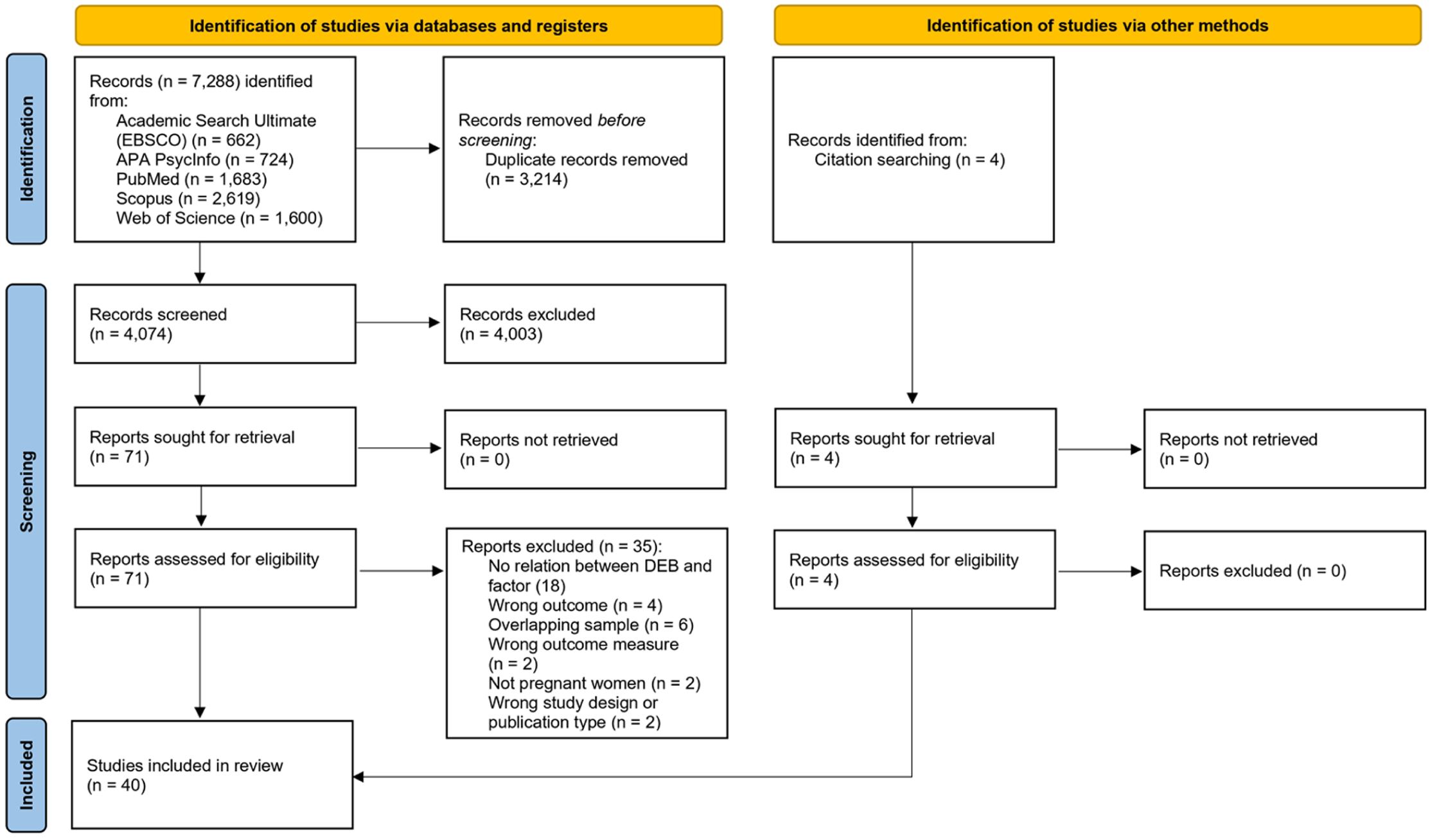
PRISMA flow diagram of the study selection process.
Characteristics of study and participants
The full characteristics of the included studies are presented in the Supplemental Material S4. The studies, published between 1999 and 2025, showed a steady increase in research on DEB during pregnancy. The studies were conducted across 15 countries, most commonly in the USA (n = 11), Turkey (n = 5), Iran (n = 4), and Australia (n = 4). The majority of the included studies used a cross-sectional design (n = 27), while others were longitudinal (n = 12). Additionally, one study provided cross-sectional data from a randomised controlled trial (van der Wijden et al., 2014).
Sample sizes of included studies varied substantially, from 39 to 1470 participants, with a total of 11,951 women represented across all studies. The mean maternal age across samples ranged from 24 to 33, reflecting a typical reproductive age group. Women participated in the included studies at different stages of pregnancy, mostly on the second or third trimester. Some longitudinal studies followed women across all trimesters, while one cross-sectional study collected retrospective data about pregnancy after birth (Czech-Szczapa et al., 2015).
Methodological quality assessment
After conducting a quality assessment, 10 longitudinal studies were identified as high quality, while 2 were rated as moderate quality. All scored highly on selection and outcome domains, but some lacked confounder control. Among cross-sectional studies, 5 were rated very good, 13 good, and 10 satisfactory. Most used validated measures and appropriate analyses but often lacked sample size justification and information on non-respondents. Thus, the overall quality of the included studies was acceptable. The quality assessment ratings for each study are provided in the Supplemental Material S2.
Outcome measures
Most of the included studies assessed overall DEB during pregnancy (n = 22). Additionally, specific DEB types were analysed, and most of them can be classified into two categories. The first category is DEB which is related to caloric restriction (e.g. eating restriction, dieting). The second category includes DEB which is related to a much higher caloric intake (e.g. binge eating, emotional eating). Alongside these categories, orthorexia nervosa behaviour, purging, and picky eating were also examined. The DEB was measured using a wide variety of self-report inventories – a total of 15 different instruments were employed (the full list of DEB measures used in the included studies is provided in Supplemental Material S5). The most commonly used self-report measure of DEB was EDE-Q (Fairburn and Beglin, 1994), employed in 20 studies.
Between-trimester comparisons of DEB
Only half of the longitudinal studies compared DEB across trimesters, resulting in conflicting findings. Calpbinici (2025) and Christian et al. (2024) found no significant differences between trimesters. Other studies reported trimester-specific changes: emotional eating was higher in the third trimester than in the second (Çelik et al., 2023), and dieting and eating restraint increased as pregnancy progressed (Yamamiya and Omori, 2023). Conversely, some studies found a decline in DEB, with women in later pregnancy stages reporting lower levels (Dryer et al., 2020) or a consistent decrease from pre-pregnancy to the third trimester (Chan et al., 2019).
Psychological factors
Depressive symptoms
Depressive symptoms were the most frequently examined factor (n = 20; the main results of the included studies are provided in the Supplemental Material S6). Eleven studies found that higher levels of depressive symptoms were significantly related with higher overall DEB (Baskin et al., 2020; Chan et al., 2019; Christian et al., 2024; Dryer et al., 2020; Gerges et al., 2023; Gonçalves et al., 2015; Hecht et al., 2021; Meireles et al., 2017; Riquin et al., 2019; Samra and Dryer, 2024; Tremblay, 2015). This relation was observed in both cross-sectional and longitudinal studies; however, four studies did not find significant association (Carter et al., 2000; O’Byrne, 2017; Shakeri et al., 2020; Turton et al., 1999). Several studies also reported associations between depressive symptoms and specific DEB types, including eating restriction (Blouin et al., 2024; DiPietro et al., 2003; Sandoval, 2024; Tremblay, 2015), overeating (Blouin et al., 2024), binge eating (Sandoval, 2024; Soares et al., 2009), purging (Sandoval, 2024), and hedonic hunger or addictive-like eating (Betts et al., 2021).
Anxiety
Anxiety was analysed in 15 studies. Ten studies found that anxiety was associated with higher overall DEB (Baskin et al., 2020; Chan et al., 2019; Christian et al., 2024; Gerges et al., 2023; Gonçalves et al., 2015; Kordi et al., 2014; Meireles et al., 2017; Samra and Dryer, 2024; Shakeri et al., 2020; Soares et al., 2009), while two reported no association (Carter et al., 2000; O’Byrne, 2017). Pregnancy-specific anxiety was also significantly associated with DEB (Dryer et al., 2020; Tremblay, 2015). One study further reported a link between anxiety and increased eating restraint in response to weight gain (DiPietro et al., 2003).
Stress
Stress was examined in six studies using pregnancy-specific stress, stressful life events, or perceived stress. A significant association between stress and higher overall DEB (Betts et al., 2021; Çelik et al., 2023; He et al., 2023; Palmer, 2019) and eating restriction (DiPietro et al., 2003) has been found. Additionally, Tremblay (2015) reported that less stress history was related to higher levels of eating restraint, while pregnant women with more stressful life events reported more bingeing behaviour.
Body dissatisfaction and fear of weight gain
All 12 studies on body dissatisfaction reported significant associations with higher DEB (Blouin et al., 2024; Dığrak et al., 2025; Gerges et al., 2023; Gonçalves et al., 2015; Kiani-Sheikhabadi et al., 2019; Lai et al., 2005; Meireles et al., 2017; Nagl et al., 2019; Palmer, 2019; Riquin et al., 2019; Samra and Dryer, 2024; Sandoval, 2024). Positive body image before or during pregnancy was linked to lower purging, restriction, and binge eating (Sandoval, 2024) and less overall DEB (Dryer et al., 2020). Studies of weight-gain attitudes showed that negative attitudes and fear of weight gain were associated with dietary restraint (Kiani-Sheikhabadi et al., 2019; Savard et al., 2021), susceptibility to hunger (Savard et al., 2021), and overall DEB (Czech-Szczapa et al., 2015). However, Baker et al. (1999) and van der Wijden et al. (2014) found no significant associations.
Adjustment towards pregnancy
Adjustment towards pregnancy here includes studies that analyse how well a woman adapts to pregnancy and motherhood or what attitudes she has towards them. Higher DEB was associated with negative attitudes towards pregnancy, motherhood, and the baby (Baskin et al., 2020; Gonçalves et al., 2015). Pregnancy-specific uplifts were related to lower DEB (DiPietro et al., 2003; Gerges et al., 2023), while pregnancy-specific struggles were linked to higher levels (Gerges et al., 2023). Pregnancy planning yielded mixed results: two studies reported no association (Chan et al., 2019; Lai et al., 2005), whereas others found unplanned pregnancy related to orthorexia nervosa behaviour (Calpbinici, 2025; Sökmen and Miabi, 2025).
Personal traits and self-esteem
Higher DEB was associated with self-compassion (Baskin et al., 2021; Christian et al., 2024), impulsivity (Nansel et al., 2020), and negative perfectionism (Christian et al., 2024; Kiani-Sheikhabadi et al., 2019). Personality traits including openness, extraversion, and conscientiousness were linked to various forms of DEB, while neuroticism was associated with external eating only (Shakeri et al., 2020). Positive perfectionism (Kiani-Sheikhabadi et al., 2019) and general life satisfaction (He et al., 2023) were linked to lower DEB. However, findings on self-esteem were inconsistent (Chan et al., 2019; Meireles et al., 2017).
Other variables
Momentary negative mood (Tremblay, 2015), anger (DiPietro et al., 2003), emotion regulation difficulties (Stein et al., 2025), and obsessive-compulsive symptoms (Mohamadirizi et al., 2015) were related to higher DEB. Childhood emotional abuse predicted higher emotional eating, while childhood physical abuse and emotional neglect were linked to lower restraint eating (Stein et al., 2025).
Social factors
The relationship with a partner was examined in seven studies; only one found that lower relationship satisfaction was associated with higher DEB (Baskin et al., 2020). Six studies reported no association with partner relationship, marital satisfaction, spousal support, communication, or intimate partner violence (Chan et al., 2019; DiPietro et al., 2003; Lai et al., 2005; O’Byrne, 2017; Sökmen and Miabi, 2025; Stein et al., 2025). Perceived social support was examined in five studies: two reported protective effects (Christian et al., 2024; Gerges et al., 2023), while three found no significant relationships (Chan et al., 2019; O’Byrne, 2017; Taştekin Ouyaba and Çiçekoğlu Öztürk, 2022).
Sociocultural factors
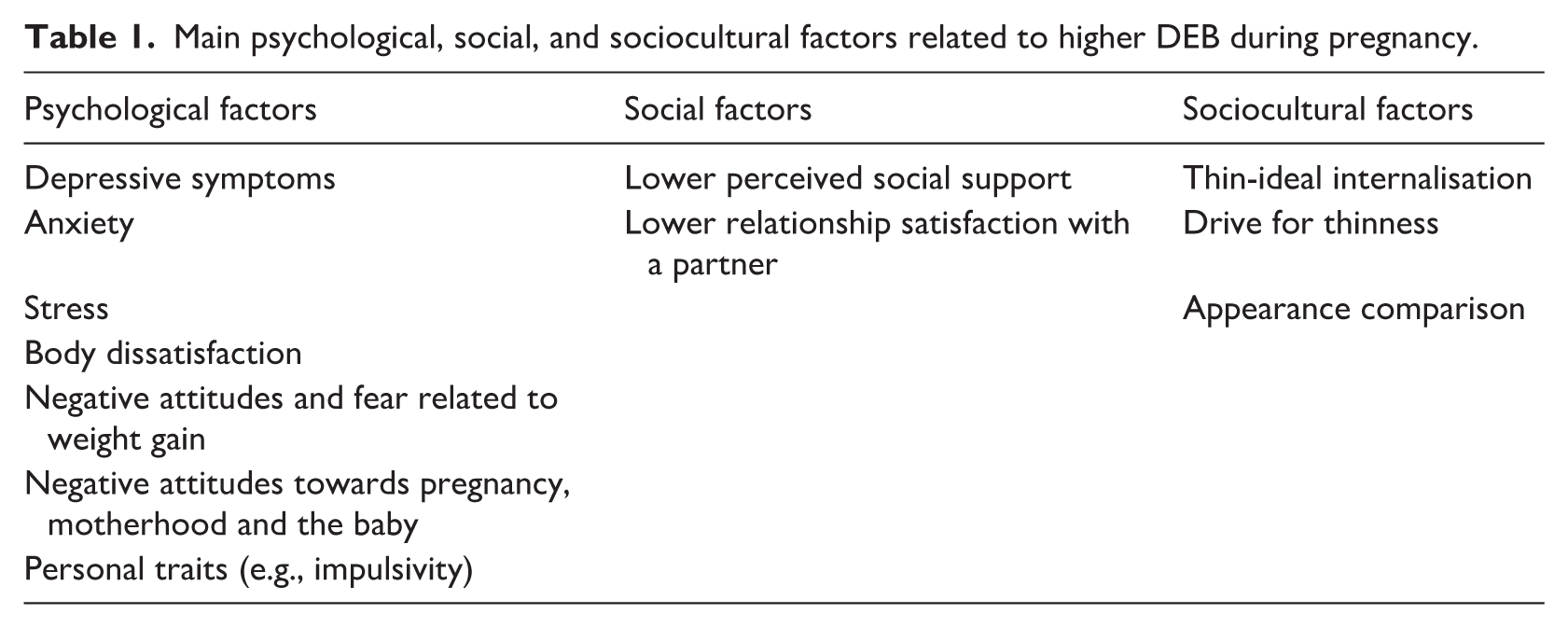
Thin-ideal internalisation was consistently significantly related to dieting, eating restraint (Dryer et al., 2020), and overall DEB (O’Byrne, 2017; Yamamiya and Omori, 2023). Pressure for thinness similarly correlated with dieting and overall DEB (Lai et al., 2005; Yamamiya and Omori, 2023). Internalised weight bias was linked to emotional eating (Çelik et al., 2023), while perceived sociocultural pressure predicted overall DEB (Dryer et al., 2020). Social appearance concerns were positively associated with DEB (Gerges et al., 2023). Media-based social comparison was also related to higher DEB (Samra and Dryer, 2024), with appearance comparison predicting dieting and restraint at different stages of pregnancy (Yamamiya and Omori, 2023). Negative body-related conversations were similarly associated with higher DEB (Dryer et al., 2020). Finally, traditional gender role attitudes were positively related to DEB (Lai et al., 2005). A summary of the main psychological, social, and sociocultural factors related to higher DEB during pregnancy is provided in Table 1.
Main psychological, social, and sociocultural factors related to higher DEB during pregnancy.
Discussion
This systematic review synthesised empirical research investigating psychological, social, and sociocultural factors related to DEB during pregnancy. The findings highlight the complexity of DEB during this period and its association with a wide variety of important factors. The significant psychological factors identified were depressive symptoms, anxiety, stress, body dissatisfaction and fear of weight gain, adjustment towards pregnancy, personal traits, and other variables like emotion regulation, life satisfaction, and obsessive-compulsive symptoms. Important social factors detected include relationship satisfaction with a partner and perceived social support. Noteworthy sociocultural factors include thin-ideal internalisation, drive for thinness, perceived sociocultural pressure, appearance comparison tendencies and media and pregnant celebrities’ influence. Further examination of these and other factors would be beneficial for developing a robust and well-grounded theoretical model explaining DEB during pregnancy.
Depressive symptoms and anxiety were one of the most frequently analysed psychological factors associated with DEB during pregnancy. Most studies showed significant positive associations between these variables and DEB. While there are several possible explanations for the relationship between anxiety/depression and DEB (Puccio et al., 2017), among the most supported ones is emotional dysregulation: the tendency to use disordered eating as a coping mechanism for distress in individuals with depressive or anxiety symptoms (Brechan and Kvalem, 2015). Several authors have argued that the relationship between these variables may be bi-directional (Puccio et al., 2017), especially given the consistently reported comorbidity between DEB and symptoms of depression or anxiety (Hughes et al., 2013). Evidence in this area is not entirely consistent, as some studies have failed to show a clear association. These mixed findings have led researchers to consider whether the link between depression, anxiety and DEB during pregnancy might be shaped by other factors, such as self-compassion or social support (Christian et al., 2024).
Although stress has been examined less often than depression or anxiety, several studies still point to a clear link between stress and DEB. Stress is relatively common in pregnancy (Pais and Pai, 2018) and can shape eating behaviour in different ways, including biological ones. For instance, activation of the HPA axis leads to cortisol release, which tends to increase cravings for high-calorie foods (Chami et al., 2019). This mechanism appears relevant during pregnancy as well: higher stress levels have been associated with more frequent reward-related eating (Betts et al., 2021) and emotional eating (Çelik et al., 2023). It has been suggested that food-related reward-seeking may partly compensate for the reduced neural response to reward experienced under stress (Born et al., 2010). Because pregnancy brings numerous psychological and physiological changes, stress is not unexpected, and DEB may operate as one way of coping, similar to patterns observed in depression and anxiety (Çelik et al., 2023).
Body dissatisfaction and fear of weight gain have been consistently linked to DEB during pregnancy, and most studies report significant associations. Pregnancy involves substantial bodily change, some of which are among the most visible and rapid shifts since puberty (Sebastiani et al., 2020). Although these changes are completely natural and expected, they can still shape how women view their bodies, and some may find them challenging to accept (Gonçalves et al., 2015). Social expectations around appearance often continue into pregnancy (Yamamiya and Omori, 2023), and these pressures can heighten worries about weight gain. In turn, such concerns may contribute to increased stress and anxiety, which can exacerbate DEB (Savard et al., 2021).
Adjustment to pregnancy also appears to be relevant. Several studies have indicated that higher levels of DEB during pregnancy are associated with more negative attitudes towards motherhood, pregnancy and the baby. Baskin et al. (2020) revealed that depression and anxiety significantly mediate the relationship between these negative attitudes and DEB. Hence, a positive view of pregnancy and anticipation of motherhood is an integral process, closely related to DEB (Easter et al., 2011). Although pregnancy planning and maternal-foetal attachment were not identified as key predictors, they warrant further investigation, as women who struggle to identify with their pregnancy are more likely to develop DEB, especially if they have a history of such behaviours (Tierney et al., 2013).
A variety of personal traits have been identified as important factors related to DEB during pregnancy. These include self-compassion, maladaptive perfectionism, impulsivity, and certain personality traits such as openness to experience, extraversion, conscientiousness, and neuroticism. However, research on personal traits and self-esteem in the pregnant population is limited, with only a few studies supporting these links. Although the underlying mechanisms may differ, some evidence points to personal characteristics that signal a genetic vulnerability to DEB (Koren et al., 2014). Other studies have suggested that DEB may also function as a way of regulating emotions, particularly when individuals struggle with a critical or negative inner voice (Braun et al., 2016). Further exploration is needed, particularly focussing on specific types of DEB, as different personal characteristics may be associated with different forms of DEB (Shakeri et al., 2020).
Moving further with social factors, the relationship with a partner during pregnancy and its correlation with DEB revealed conflicting results. While one study found that lower relationship satisfaction was related to increased DEB, other studies reported no significant relationship between DEB and marital satisfaction or spousal support. Additionally, perceived social support from a significant other, family and friends was also examined: two studies confirmed its relevance to DEB, while one did not. Despite these discrepancies, a supportive social environment during pregnancy is important. Poor relationship quality with a partner or close contacts can increase feelings of isolation and lack of support, which may contribute to DEB during pregnancy (Baskin and Galligan, 2019). Social support may help buffer psychological distress and could therefore reduce the likelihood of DEB during pregnancy. Nonetheless, the nature of these associations remains insufficiently understood and warrants further investigation, particularly in the context of pregnancy.
Attention has increasingly shifted towards the sociocultural influences that may play a role in DEB during pregnancy. Thin-ideal internalisation and the drive for thinness have been linked to dieting, restrictive eating, and broader patterns of disordered eating. Even in pregnancy, when weight gain is expected, some women describe feeling that their changing bodies move them further from sociocultural standards of thinness (Yamamiya and Omori, 2023). These pressures seem to persist throughout pregnancy and may contribute to more restrictive forms of DEB. Media portrayals, such as idealised images of pregnant celebrities, can reinforce appearance-based comparisons, which are also related to DEB (Yamamiya and Omori, 2023). Although current findings point to the importance of these sociocultural influences, more systematic research is still needed to understand how they operate in pregnancy.
This systematic review highlighted that DEB during pregnancy is mostly related to pregnancy-specific factors: prenatal depression, pregnancy-specific anxiety and stress, body dissatisfaction and fear of weight gain, adjustment towards pregnancy, as well as pregnant celebrities’ influence. This suggests that predictors of DEB during pregnancy may be different from other life stages because of the specificity of pregnancy as a period. It is also important to note that many of the factors identified in the systematic review (both pregnancy-specific and not) are modifiable through prevention or intervention strategies, which should be developed in order to reduce DEB during pregnancy.
The factors identified in this review align with established models of disordered eating. The Dual Pathway Model (Stice, 2001) suggests that thin-ideal internalisation leads to body dissatisfaction, which contributes to disordered eating through dietary restraint and negative affect. Our findings support this model, indicating that body dissatisfaction, thin-ideal internalisation, and negative emotions are associated with disordered eating behaviours during pregnancy. The Tripartite Influence Model (Thompson et al., 1999) highlights the influence of parents, peers, and media, and our review further emphasises the importance of relationships with partners, significant others, and social media. Additionally, we identify pregnancy-specific variables, suggesting that current frameworks could be expanded to address challenges unique to pregnancy.
Interpreting the findings of this review requires careful consideration of both the methodological challenges involved in assessing DEB during pregnancy and the extent to which results are consistent across different study designs. Although there is still no gold-standard measure for DEB in pregnancy (Stephens et al., 2025), researchers tend to rely on a range of available instruments. This diversity, however, can complicate the interpretation and replication of findings related to DEB and its psychological, social and sociocultural correlates. Systematic reviews (Bannatyne et al., 2021; Stephens et al., 2025) have noted that many studies use general disordered eating questionnaires which do not capture pregnancy-specific experiences. As a result, certain behaviours that emerge uniquely during pregnancy may be under-represented in existing assessments.
Most studies included in this review were cross-sectional, but their findings were largely in line with those from longitudinal work. Both types of design identified depressive symptoms, anxiety and body dissatisfaction as prominent predictors of DEB during pregnancy. Longitudinal analyses added further clarity by showing that some factors, such as negative attitudes towards pregnancy, were significant only at particular time points, whereas others (e.g. depressive symptoms) remained predictive throughout all trimesters. These findings imply that cross-sectional research can detect meaningful associations, but longitudinal approaches are better suited to understanding when these relationships emerge and how stable they are over time.
The findings of this review have important implications for both clinical practice and future research. Clinicians working with pregnant women should be attentive to the possibility of DEB and consider the psychological, social, and sociocultural factors that may contribute to its development. Several of these factors are also associated with broader mental health difficulties, indicating that addressing them could support women’s overall psychological well-being and not solely reduce DEB. For instance, targeting depressive symptoms and body image dissatisfaction during pregnancy may reduce DEB levels and might also help prevent postpartum depression (Riesco-González et al., 2022). Future studies should investigate these factors across all trimesters and rely more on longitudinal approaches to gain a clearer understanding of how DEB develops over time. In addition, most studies included in this review assessed DEB as a single construct; however, different types of disordered eating behaviour may involve distinct psychological mechanisms and therefore warrant further examination. Also, more attention should be addressed towards how these factors predict DEB not only separately, but working in conjunction, moderating or mediating each other.
Several limitations of the studies included and also of this review itself should be noted. The majority of the included studies were cross-sectional, allowing only to report factors related to DEB during pregnancy, but limiting the ability to draw causal inferences. Additionally, the reliance on a large variety of self-report measures for assessing DEB and psychological, social, and sociocultural factors in the included studies may introduce bias. Also, some of the included studies did not demonstrate that their samples were representative of the wider pregnant population and did not include sample size calculations, raising questions about generalisability of the results. Adjustment for key confounders, such as pre-pregnancy BMI, parity, or socioeconomic status, was inconsistent across studies, limiting the interpretability of observed relations. Most of the included studies represent Western cultures, so there may be more important variables related to DEB in non-Western societies.
Continuing on the limitations of this review, it was not preregistered, which may reduce its transparency and replicability. The review search strategy focussed on overall DEB during pregnancy rather than on specific types of it, which may have led to missing some relevant articles. Additionally, while the NOS is widely recognised and used for quality assessment in systematic reviews, it has some limitations (e.g. lack of comprehensive manuals), especially when applied to cross-sectional studies (Luchini et al., 2017). Also, this review cannot provide a synthesis of women’s subjective experiences of DEB during pregnancy, as qualitative studies were not included. Additionally, narrative synthesis without meta-analysis limits the ability to quantify effect sizes.
By synthesising the existing knowledge on psychological, social, and sociocultural factors related to DEB during pregnancy, this review indicates several important directions for further research. First of all, most of the factors should be analysed further, especially those for which existing findings are contradictory or significant associations are supported by only a few studies. Second, research on DEB-related factors should focus more on pregnancy-specific aspects and aim to integrate psychological, social, and sociocultural factors into theoretical models explaining DEB. Finally, future research should employ more reliable measures and longitudinal designs to better understand the relationships between psychological, social, and sociocultural factors and DEB during pregnancy.
Conclusions
DEB during pregnancy is an important part of mental health research and practice that requires further investigation, as poor nutrition during this period can have harmful consequences for the health of the mother and child. Further studies investigating psychological, social, and sociocultural factors related to DEB during pregnancy would help to develop theoretical models that would contribute to a better understanding of this phenomenon and more effective prevention and intervention planning.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261442874 – Supplemental material for Psychological, social, and sociocultural factors related to disordered eating behaviour during pregnancy: A systematic review
Supplemental material, sj-docx-1-hpq-10.1177_13591053261442874 for Psychological, social, and sociocultural factors related to disordered eating behaviour during pregnancy: A systematic review by Erika Gibė and Aidas Perminas in Journal of Health Psychology
Footnotes
Ethical considerations
Ethics approval was not required for this review article as no data were collected from participants.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
EG prepared the first version of the manuscript, conducted the search, and extracted data from the articles. Both authors developed the search strategy, reviewed studies for eligibility, and assessed methodological quality. AP reviewed the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data will be given by the corresponding author upon request.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.