
Abstract
This study explored the lived experiences of individuals from socioeconomically disadvantaged communities living with chronic pain and prescribed pain-relief medication. Using Interpretative Phenomenological Analysis, eight participants were recruited from a single primary care network in England. Two Group Experiential Themes were developed. This paper reports one: From Dismissed to Disengaged: the trauma of seeking help, with three sub-themes: (1) “Being fobbed off” – dismissal across healthcare and benefit systems; (2) “It just seemed horrible to me, to take it off me” – pain relief as withdrawn, stigmatised, or conditional; and (3) “Do I want to poke the bear?” – disengagement from services. Participants described being dismissed, losing access to medication without prior discussion, and avoiding services out of fear or futility. While most reported systemic invalidation, some described collaborative support. Findings highlight the need for trauma-informed, person-centred care that recognises the role of power and inequality in shaping chronic pain.
Keywords
Introduction
Pain is a multidimensional experience, defined by the International Association for the Study of Pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” (Raja et al., 2020). Chronic pain (CP) is classified in the International Classification of Diseases (ICD-11) as pain persisting for more than 3 months, associated with emotional distress and functional disability, and not better explained by another condition (Treede et al., 2019). Widely recognised as involving physiological, psychological, and social factors, CP is a leading reason for seeking medical support (Cohen et al., 2021).
However, CP does not affect all populations equally. A well-documented social gradient exists internationally, with individuals from socioeconomically deprived backgrounds consistently reporting higher CP prevalence and severity. In a 19-country European study (Todd et al., 2019), socioeconomically disadvantaged groups, especially women, reported significantly more CP. In the United States, CP is strongly associated with low income and rural residence (Weissman et al., 2023), and in Canada, food insecurity was the strongest predictor of CP (Men et al., 2021). These disparities are mirrored in the UK, where up to half of adults are estimated to live with CP, with higher prevalence in more deprived areas (Fayaz et al., 2016). Individuals from socioeconomically disadvantaged backgrounds tend to report greater pain severity and associated disability (Cohen et al., 2021).
In the UK, CP is mostly managed in primary care, typically within a Western biomedical framework that prioritises pharmacological treatment and accounts of pain understood separately from people’s social and emotional contexts (Cohen et al., 2021). Primary Care is delivered through the National Health Service (NHS), where General Practitioners (GPs) act as the first point of contact and the main prescribers of analgesics. GP prescribing is shaped by national guidelines, such as those issued by the National Institute for Health and Care Excellence (NICE). The latest NICE guideline for chronic pain (National Institute for Health and Care Excellence (NICE), 2021) advises against initiating opioids or gabapentinoids for the management of CP, citing limited evidence of benefit and substantial risk of harm. Despite these recent guidelines, evidence from the Department of Health and Social Care (Department of Health and Social Care (DHSC), 2020) shows that individuals from more deprived backgrounds are more likely to be prescribed opioids, raising concerns that prescribing practices may reflect and reinforce broader health inequalities. The relationship between socioeconomic deprivation and opioid prescribing is further supported by several other studies (Gallagher et al., 2024; Nowakowska et al., 2021; Ramírez Medina et al., 2024; Jani et al., 2020). These patterns suggest that CP prescribing is strongly influenced by wider social and structural inequalities, including brief, under-resourced consultations; limited continuity of care; restricted access to alternative treatments; and unconscious clinician bias (Norbury et al., 2011). Barriers such as transport, low health literacy, stigma, and intersecting vulnerabilities further exacerbate inequities (Comino et al., 2012; Ford et al., 2016).
Qualitative research highlights how CP narratives often involve feeling unheard or disbelieved, with medical encounters eliciting shame and psychological threat, which can exacerbate pain (Gilbert, 2009; Toye et al., 2017). However, the literature emphasises individual experience, overlooking systemic inequalities and socio-economic factors that shape pain and access to care (Marmot et al., 2020). Cumulative Inequality Theory offers a useful framework for understanding how disadvantage increases vulnerability to CP, as it conceptualises health as shaped by the accumulation of social disadvantage across the life course, with early inequalities compounding over time to influence stress physiology and biological vulnerability (Ferraro and Shippee, 2009).
From a prescriber perspective, recent qualitative research reported that GPs identified addiction as a central concern in opioid prescribing for CP, frequently interpreting requests for dose increases or reluctance to taper as evidence of substance misuse (Gill et al., 2022). Time pressures and system constraints, such as a fragmented healthcare system, were also identified as factors affecting good prescribing practices. Yet the voices of those most affected, people with CP in socioeconomically disadvantaged contexts, remain under-represented (Janevic et al., 2022). As such, the social, emotional, and relational meanings of pain medication, and power dynamics in healthcare, are underexplored.
This study addresses this gap, foregrounding structural, relational, and political dimensions of CP in disadvantaged communities. Understanding these experiences is critical for informing equitable care, reducing harmful prescribing, and ensuring interventions are responsive to lived realities (DHSC, 2020). As part of a wider mixed-method project, the aim of the current study was therefore to explore the experiences of individuals from socioeconomically deprived communities who live with CP and are prescribed medication to manage it.
Research design and methods
Ethical approval
Ethical approval was obtained from the university and relevant health authorities. An honorary contract with the local primary care network (PCN) allowed access to electronic records and permission to contact participants. Reasonable adjustments were considered, and all participants received an information sheet with the researcher’s contact details and a sheet signposting to local support organisations.
Theoretical framework and positionality
A qualitative idiographic approach was chosen to capture rich, in-depth accounts of individual experiences. Interpretative Phenomenological Analysis (IPA) was selected for its grounding in phenomenology, hermeneutics, and idiography (Smith et al., 2022) and its established use in health psychology and chronic pain research (Smith and Osborn, 2015). As a phenomenological method, IPA explores subjective experience; as a hermeneutic, it centres on sense-making; and as an idiographic approach, it focuses on the particular. This makes it well suited to exploring the nuanced experiences of socioeconomically disadvantaged individuals living with chronic pain. IPA is compatible with a range of epistemological orientations, including constructionist and critical positions, provided that researchers remain transparent and reflexive in their approach (Larkin et al., 2006). Social constructionism and critical theory recognise that concepts are shaped by culture, dialogue, and power, and foreground issues of control and agency (Phillips, 2023; Smith, 2011). Reflexive and transparent application allows IPA to maintain its idiographic focus while situating participants’ experiences within broader sociocultural and structural contexts (Larkin et al., 2006).
Reflexivity
The lead researcher, a trainee clinical psychologist, recruited participants and conducted data collection and analysis, drawing on her experiences with chronic pain to inform understanding of healthcare dynamics. The second and third authors provided supervision. Reflexivity was maintained through supervision and a reflective diary, attending to how the researcher’s experiences and assumptions may have shaped interpretation within the double hermeneutic, whereby the researcher makes sense of participants’ sense-making. (Smith et al., 2022).
Study design
An expert by experience with CP from a socioeconomically disadvantaged background advised on the study, shaping the interview schedule and participant materials. Semi-structured interviews allowed consistency while following participants’ narratives. Participants received a printed resource sheet of local services and a £20 honorarium, reflecting a reciprocal approach to research.
Participants
IPA emphasises idiographic depth and recommends a relatively homogenous sample to explore shared experiences in context (Smith et al., 2022). Eligible participants were adults with documented chronic pain and prescribed medication. Exclusion criteria included multi-drug use, ongoing cancer treatment, or psychosis. For professional doctorates, 6–10 participants are recommended to support reflective, interpretative depth (Smith et al., 2022). Ten interviews were conducted (six women, four men; mean age 56, range 47–76), all White British; all but one were receiving benefits and unable to work. Two male participants were excluded post-interview due to divergence from inclusion criteria: one identified as affluent, the other framed his experience as emotional rather than chronic physical pain. Their narratives, while insightful, did not align with the study’s conceptual focus. Participant characteristics are summarised in Table 1.
Characteristics of participants.
Recruitment and data collection
Participants were purposively recruited from a single GP surgery within the Primary Care Network where the lead researcher was embedded. Eligibility was based on a CP diagnosis and ⩾3 months’ repeat prescription of opioids, gabapentinoids, or antidepressants, including co-prescriptions associated with psychological distress and a recorded diagnosis of depression or anxiety. Suitability was further confirmed during interviews.
Deprivation was assessed post-participation using the Index of Multiple Deprivation (IMD), employment, benefits, and participants’ descriptions, reflecting its complex, context-specific nature (Clelland and Hill, 2019). Invitations included information, consent, and signposting information sheets directing participants to relevant support services, with follow-up after 2 weeks. Interviews were scheduled at participants’ convenience. Consent was reconfirmed at interview. Six interviews were in-person and two via video, lasting 55–80 minutes. Interviews were audio-recorded, transcribed verbatim. Transcripts were anonymised and pseudonyms assigned. Participant characteristics were drawn from records and interview notes.
Data analysis
Data analysis followed Smith et al.’s (2022) six-stage IPA process. Transcripts were read alongside audio recordings, with notes at descriptive, linguistic, and conceptual levels informing Personal Experiential Themes (PETs), which were then compared across participants to identify Group Experiential Themes (GETs). GETs were developed into a narrative through iterative engagement with the hermeneutic cycle.
Rigour was maintained using IPA quality criteria (Nizza et al., 2021; Smith et al., 2022) and broader guidance (Levitt et al., 2018). The researcher documented assumptions in a reflective journal and employed supervision and bracketing to ensure transparency and trustworthiness.
Results
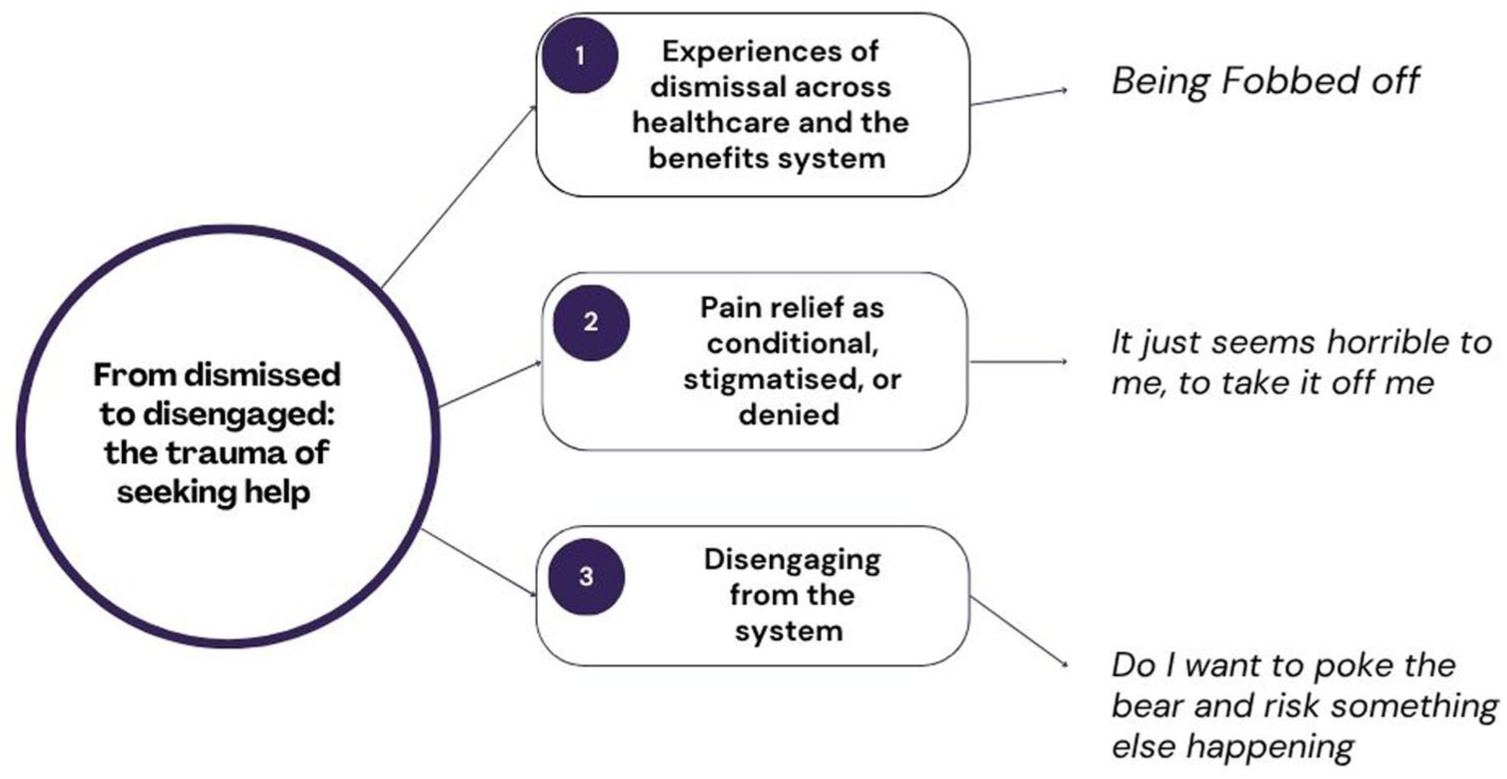
Two co-existing Group Experiential Themes (GETs) were identified. GET 1 (Figure 1), which forms the focus of this paper, captures participants’ experiences of navigating healthcare and wider systems in the context of chronic pain; particularly the trauma of repeatedly seeking help, and the emotional toll of having to fight to be seen and believed by both medical professionals and the benefits system.
GET 1.
From dismissed to disengaged: The trauma of seeking help
This GET, explored through three subGETs, captures how participants described being repeatedly dismissed, disbelieved, or “fobbed off” when seeking help for their pain. Many spoke of a “traumatic journey,” doctors being disinterested, or being made to feel like they were “pestering.” These encounters were often experienced as part of a wider battle across both medical and benefits systems. Participants described professionals who “don’t believe you,” or who used diagnoses like fibromyalgia “as an excuse to be dismissive.” Over time, participants reported disengaging entirely from services. For a couple, more trusting relationships with professionals offered a counterweight to these experiences, creating a sense of safety and trust that supported continued engagement.
“Being fobbed off” – Experiences of dismissal across healthcare and the benefit systems
All participants described experiences of being “dismissed,” “left to just get on with it,” receiving “no care,” and feeling that “no one listens.” Rather than a source of support, healthcare was often experienced as indifferent or something to battle against. Maria, for instance, reflected that when it came to her pain, she was “basically left to just get on with it,” adding that it felt “like they’re just not interested at all.”
Alexia took this further and described being dismissed as worse than the pain itself:
Being dismissed. That's. . .that's the worst part of it, being dismissed, as. . .I'm not the only one that said, you know, quite a few people say, have said this, as soon as you get something like Fibro on your notes. . .hum. . .the medical people, they also get blinkers, and that's all they see [. . .] you know, it's just, (sigh) just another one of those things you've got to learn to learn to live with, you know? It's almost like, it's almost used as an excuse to be dismissive, you know. And you can't get used to it [. . .]
Alexia spoke of how she anticipated being dismissed each time she sought help and emphasised this was not just her own individual experience, “quite a few people [. . .] have said this.” Her diagnosis of fibromyalgia functioned as a clinical dead-end, clinicians “got blinkers” and dismissed her new concerns by attributing everything to it. Her claim that this was “used as an excuse to be dismissive” implied clinicians not only failed to listen to her, but chose not to.
Some participants described experiencing humiliation and shame when seeking help for their pain. Kay recounted how a male doctor dismissed her endometriosis as a “woman’s disease” and suggested pregnancy as a “cure.” Not being believed was experienced as “demeaning” and “embarrassing,” leaving her unsure of “where to turn anymore.” She experienced medical care as hostile, perceiving her GP as actively disliking her and extended this sentiment to non-clinical staff, noting that even “the receptionist’s rude” to her.
Kylie recounted experiences of neglect and de-humanisation while seeking care for her pain, evoking an experience of feeling invisible:
Neglected, like. . .. stuff her here, put her over there. I mean, I'm not a fucking dog. My dog got treated better!
She described being moved around, ignored, and compared her treatment to that of a dog. In suggesting that her dog had received more compassionate care, Kylie seemed to be articulating a rupture in dignity. Her sense of invisibility was amplified when the doctor chose not to address her directly. In this passage, her words reflected acute distress:
No one listens. And I tried telling the doctor [. . .] and he says: ‘I'm a phantom’. ‘I’m a what?’ And he turned away from me and spoke to him [partner] yeah. So then I felt even more shit; ‘So you're calling me a dog?’ And he went, ‘Yeah, something like that, a phantom dog pregnancy’. Get me out of here. Get me out of here. So it's like, what? What do I do? Where do I go?
In contrast, Dave recalled a moment of severe neglect in a neutral tone:
I recall one occasion when I actually passed out because the pain was so bad, and, uh I was left lying on the floor and I, I could not move. And wife called them 999, and, uh, she was told just to leave me on the floor until I was able to get up. Ludicrous situation.
Dave didn’t describe how this made him feel. His tone was matter of fact, consistent with the stoicism seen throughout his interview.
Experiences of invalidation extended beyond healthcare and into the benefit system. Alexia also described how the benefits system mirrored these patterns of dismissal:
I think the benefits system is also geared towards that dismissive, hum, non-belief, you know, that immediately, you speak, they don't believe what you're saying, you know? And it's so, it's not just the medical side of it, it's that side of it, but they are connected you know? And, you know, it's just like one long battle.
She described this experience as a battle to be seen and recognised. This metaphor of having to fight resonated across interviews. Alan described similar difficulties and used the same metaphor:
It was so difficult for, to get benefits with my condition because. . . they weren't recognising me really as was being ill. So I struggled for years and years and years. Literally, I had no money, you know, it's really tough. [. . .] One time it was so desperate for me, I went outside and I picked up snails and dandelions to eat. That's how bad it was, because I'd run out of plain rice. You know, it's awful, but, but now, I've been on proper benefits for probably about. . . maybe four years? When it's recognised. But it's the battle you have to go through with these people. They don't want you to be ill. [. . .] I just think about the trauma that so many people have to go through [. . .] it makes you feel like, kind of like, bit worthless I guess.
Alan described how not being recognised led to survival-level desperation, he had no money and was desperate to find food: “I went outside and I picked up snails and dandelions to eat.” Although he is now receiving support, Alan spoke in the present about the lasting impact of this period: “it’s really tough”; “it makes you feel [. . .] bit worthless,” suggesting that the experience continued to affect how he felt about himself.
Some participants located these patterns within longer intergenerational histories of “class-based” neglect. Maria described her father’s struggles with arthritis, and how he, too, had received little help:
My dad was crippled in arthritis, and he never used to get a lot of help either. You know, but he was of that generation, you know, he worked on the buildings and, and that, and he did, basically, knacker all his joints and that, but he never used to get a lot of help.
Her account positioned this lack of support as part of a longer pattern affecting “working-class” individuals who would exhaust their bodies and receive no support.
For other participants, disbelief had become so entrenched that even offers of support, such as pain management, were experienced as further dismissal. For Alan and Kylie, the term “management” carried the implication that their pain wasn’t real but imagined. Alan said: “I’ve even seen doctors that saying it’s my head.” Kylie’s reaction to pain management was scathing:
Are you off your fucking head? How is Pain Management gonna sort my pain? Was it? Oh, I’ll talk to myself in front of a fucking mirror, shall I? ‘You ain't got no pain. It's an illusion’. That's what they're trying to say.
Her words suggested that this offer of support was experienced as a denial of her reality, that her pain “is an illusion.”
Together, these accounts illustrate the varied ways participants made sense of what could be broadly understood as institutional invalidation. Participants described a range of dismissive experiences across both healthcare and benefit systems. One participant situated this within longer-standing, “class-based” generational expectations that healthcare would offer little to no support. Attempts to access care were often framed as “battles,” underscoring the emotional toll of repeatedly having to fight for recognition and legitimacy.
“It just seemed horrible to me, to take it off me” – Pain relief as conditional, stigmatised, or denied
Most participants described a loss of agency in decisions about their pain treatment. Medication was rarely experienced as collaborative; instead, decisions were made for participants. Some had their treatment stopped suddenly, others were denied it altogether, or medication was used as a conditional access to specialist’s services. One participant felt medication exposed her to judgement or suspicion. For example, Maria lost access to Tramadol, an opioid analgesic she felt helped. The decision was communicated without warning, over the phone:
“About six or seven months ago, I had a phone call, ‘Oh, we're taking the Tramadol off you’. Tramadol has been working brilliantly and I was like, ‘Oh, hum, why?’ ‘Well, the NHS don't want us to prescribe it anymore’. Hum, and I'm like, really upset, because I'm thinking, yeah, I can understand, like, because I know people abuse it, but I've never abused it. I've never asked for a prescription early. Always took it religiously. And they were like, ‘No’. And I was like, ‘Well, what else can I. . . have?’ And they were like, ‘Well, there isn't anything, just take paracetamol’. I was taking the paracetamol alongside the Tramadol, so you're leaving me now in . . . agony. And eventually, after a couple of phone calls, I came off the Tramadol, hum, and which was frightening me to come off it, I had to more or less fight to be able to get them to do it in a manner which was bringing me down, as opposed to just like, ‘right, we're stopping the prescription’. And I was terrified [. . .] I ended up having to fight to get them to bring me down over a couple of months. And I came off them probably completely about four, four or five months ago, hum, and was hardly leaving the house because I was in so much pain
The withdrawal was experienced as an acute loss. Maria’s concerns were brushed aside with a generic rationale, and the withdrawal left her “housebound.” She also felt personally targeted:
I felt like I’d been picked on. They’d looked at me. I’ve always done everything a doctor’s told me to do, you know, I’ve never questioned, or I was brought up in that generation where you don’t question doctors. And I just felt like, ‘Why me?’ sort of thing
Alexia shared a similar experience after relocating. Her prescription was withdrawn: “No. We're not going to prescribe that to you anymore because it doesn't work on Fibro.” She challenged this by saying, “I’m the one that’s taking it [. . .] and I’m telling you, it does work,” but her experience was dismissed.
Other participants didn’t have medication withdrawn but found it changed how they were perceived. Kay described how a fentanyl patch, also an opioid analgesic, impacted her interactions with clinicians:
Having that patch has so greatly changed how medical professionals treat me that it's almost unbelievable. As soon as anyone sees that you were on that patch, you were treated like you've done something wrong, or like you are a drug addict. Any discussions about pain, the doctors are straight away. . .hum, I can't even really think of the words. It’s like they think that you want drugs. They’re not willing to listen that you aren't managing, you're not coping at home, sleeping, or any of the problems, because of the pain medication that you're on.
Her pain became secondary to the assumption that she was abusing substances. This shift is explicitly named in the passage, where her language moves between the past and present tense. Conversations about how she was coping at home, about sleep, and pain, couldn’t happen. Her concerns about functioning were overlooked because of the implication: “they think that you want drugs.”
Kay’s experience sat on a continuum with Kylie’s, though Kylie’s was more extreme. While Kay felt stigmatised for receiving opioids, Kylie was denied pain relief altogether and left to self-medicate. She described being in pain and receiving no help: “They give me no painkiller [. . .] I’ve got to self-medicate.” Her requests for support: “Give me the right medication. . . I need it. I'm in pain” were unmet, and she appeared to feel abandoned despite repeated attempts to seek help: “I’m just wanting help.”
Underpinning participants experiences was a shared double bind: asking for analgesia medication was to risk being seen as dependent; staying silent was to risk unrelieved pain. Alexia described how concern about medication could be used against her:
You’re nervous about coming, or somebody taking that medication away, well, ‘you must be nervous about it because you're addicted to it’. You know that’s, that’s the. . . kind of feedback attitude you get
Maria echoed this:
You're taking my Tramadol away. And like I said, the more [. . .] I protested, the more I feel they were looking at me that I was addicted to it.
Her use of “my Tramadol” conveyed ownership and reliance, reflecting how essential the medication had become. Her protest was not heard as valid but interpreted as addiction.
Ruth’s experience reflected a different version of this bind. Her pain medication was not withheld, but increased, as a condition for accessing further care:
He said: ‘I’m not going to refer you until you're, you've taken a higher dose of the gabapentin [. . .]’ That’s when it started, when I got really high. I swapped from Gabapentin to a higher dose of Pregabalin, and that's when I started falling over and dropping things. [. . .] in the end [. . .] he did refer me [. . .] but I got frustrated and really quite angry about the fact that I had to take that really high dose.
Only one participant, Elsa, described a relationship of mutual respect: “We do sit there and have chats about it.” She emphasised that her experience was different from others who felt overridden: “It’s not as if they said, ‘Well, I don't care what you say, this is what you are doing’”. While she acknowledged the doctor’s authority, “In the end it's down to them [. . .] they're the ones that can say yes or no,” she clearly valued being included in the process.
For most participants decisions about medication were seldom collaborative. Participants described medication being taken away, with no room to challenge the decision for fear of being viewed as addicted or stigmatised, or being used conditionally as a gateway to further services.
“Do I want to poke the bear and risk something else happening” – Disengaging from the system
This subGET explores participants’ experiences of disengaging from care. Dis-engagement was not a single event but a passive process where participant either wanted to protect themselves from further trauma, or simply did not see the point to request a consultation just to hear the same ineffective advice.
Alan described this long-term withdrawal as the result of what he called a “traumatic journey” through healthcare:
Engaging is, I find difficult as well, you know, I think I've gone through such a traumatic journey. It's, it's really compounded, you know, how I feel
Alan spoke of feeling anxious about going to see his GP. He reflected on how years of difficult encounters had shaped his emotional response, contributing to an enduring reluctance to seek care. He said he had not “engaged in a long, long time,” and concluded with a sense of resignation: “this is my lot.”
Ruth similarly described withdrawing from healthcare over time, after receiving repeated signals that there were no further options available to her:
Well, I’m a bit reluctant now, to be honest, because I feel like I don't want to pester people, and I haven't messaged or had a consultation for quite some time on it, because I keep feeling, really, they keep telling me there's not much else to say.
The phrase “I don’t want to pester people” suggested that Ruth may have internalised a sense of herself as a burden. She described not contacting her GP for some time, anticipating that the response would be the same: “There’s not much else to say.” Ruth also reflected on her mother’s experience of similar pain and long-term medication, recalling that “nobody helped her, nobody supported her.” This suggested a possible intergenerational strategy of disengaging from care, shaped by repeated experiences of inadequate support.
Maria’s experience of disengaging was gradual, having repeatedly been offered ineffective suggestions:
Oh there’s no point me coming and see the doctor about it, because [. . .] it's “oh, go and do some physio”. Or, you know, “oh, the amitriptyline will help it”. So now I'm just like, ‘oh, just can’t be bothered with trying to get an appointment’
Repeatedly encountering limited or generic care options left her feeling it was no longer worth trying.
Kylie expressed a more visceral rejection of healthcare, shaped by a repeated sense of dehumanisation:
Don't, don't like it, yeah, don't like it, don't like it. I'd rather not I hate coming to the doctor. I mean, even the reception staff treat me like a fucking dog, and my dog got treated better.
In this passage, Kylie articulated the depth of her emotional injury and how profoundly she felt excluded from care. The recurrence of the dog comparison across her narrative emerged as a potent metaphor for her perceived loss of personhood. In evoking this image again, Kylie revealed how healthcare interactions have made her feel othered, aligned more with an animal than a human being. Her use of the word “fucking” underscored the intensity of her anger and frustration.
Kay described avoiding doctors even when in “blinding agony,” due to intense anticipatory anxiety:
So I find that unless I am in blinding agony, and even if I am, I just sometimes still won't call. I don't go to the doctors on a regular basis because of this. And then, if for whatever reason I absolutely have to go, I will be so anxious and upset that I won't sleep. When I'm coming up to it, there are times when in 1h to go, I just can't go. Like I'm physically shaking because I get so distressed at having to go. And I know it sounds so pathetic for an adult to be that upset going to the doctors.
She recalled sleepless nights and physical symptoms of distress before appointments: “I'm physically shaking because I get so distressed.” Her language suggested shame around this response: “I know it sounds so pathetic for an adult.” Over time, Kay had come to believe that “nothing I say is going to make any difference.”
Alexia’s experiences reflected a state of ambivalence about seeking help. Her account suggested that healthcare had become unpredictable and potentially harmful:
Sometimes I think yes. Sometimes I think no. Again, it’s. . .you are nervous of poking that sleeping dog, you know, it's. . .would I be happier just carrying on carrying on, or. . .do I want to poke the bear and risk. . .something else happening, you know.
Alexia drew on two powerful metaphors of a “sleeping dog” and a “bear” to convey the danger she associated with asking for help from her doctor. In her experiences, seeking support from healthcare was unpredictable and potentially harmful, and she weighed the cost of re-engaging.
In contrast, Dave and Elsa described rare, positive examples of continuity and trust. Dave felt listened to and supported, saying the doctors “always try to sort something out,” and that he was “really happy with the health service.” His comments suggested consistency and a sense of being cared for. Elsa described having stayed with the same GP for nearly three decades, despite moving house. She emphasised that her GP had “known me all this time” and described the relationship as “absolutely brilliant.”
This subGET has shown that, for most participants, the act of disengaging from the healthcare system developed gradually. Except for two participants who described longstanding and trusting relationships with their doctors, most spoke of repeated encounters where their pain was minimised, their treatment options limited, or their concerns met with disbelief. These experiences accumulated over time and shaped participants’ relationships with care. For some, disengagement manifested quietly, as a reluctance to call the GP or a belief that appointments were pointless whilst others described avoidance linked to anxiety or distress.
Discussion
This study explored the lived experiences of individuals with CP from socioeconomically disadvantaged backgrounds who are prescribed pain-relief medication. Central to participants’ accounts was the impact of healthcare and welfare systems, captured in the Group Experiential Theme (GET 1): “From dismissed to disengaged,” comprising three sub-themes: (1) experiences of dismissal across healthcare and benefits, (2) pain relief as conditional, stigmatised, or denied, and (3) disengagement from services.
Most participants described repeated experiences of invalidation in healthcare encounters, including disbelief, disregard, and indifference, although two participants also reported positive or supportive experiences. Medically unexplained diagnoses, such as fibromyalgia, were often experienced as clinical dead-ends. These encounters reflect prior research on disbelief and the need to “prove legitimacy” in CP (Nicola et al., 2021; Toye et al., 2013; Kool et al., 2009), but this study situates them within structural power and socioeconomic marginalisation. Participants described being perceived as less credible or deserving, echoing Fricker’s (2007) concept of epistemic injustice whereby individuals from marginalised communities are systematically disbelieved and not listened to in their capacity as experts of their own pain.
Medication decisions were often unilateral, dismissing participants’ embodied knowledge. Abrupt withdrawal led to functional decline, while continued prescriptions were accompanied by judgement and suspicion. Participants experienced a double bind: requesting pain-relief risked being labelled as “drug-seeking”; but remaining silent meant enduring ongoing CP. These dynamics, framed through Bourdieu’s (1991) symbolic violence, reflect subtle mechanisms reinforcing social hierarchies and marginalisation, especially in disadvantaged groups (Brooks et al., 2015; Nichols et al., 2020).
Most participants gradually disengaged from healthcare, driven by repeated dead-ends, fear of burdening staff, or futility. Anticipatory anxiety and physical symptoms before appointments exemplified how healthcare settings became unsafe. Only two participants reported supportive GP relationships; others experienced mistrust, withdrawal, and significant consequences for pain management. Disengagement can delay treatment, exacerbate pain, and widen health inequalities, with evidence of higher A&E attendance and emergency admissions in deprived areas (Care Quality Commission, 2024; Joseph Rowntree Foundation, 2024).
Cumulative Inequality (CI) Theory (Ferraro and Shippee, 2009) provides a framework for understanding how CP is shaped by structural forces accumulating over time. Disadvantage accrues through prolonged exposure to risk, restricted resources, and limited agency, situating pain within a broader life course of hardship and marginalisation (Marmot et al., 2020). Poor healthcare, welfare stigma, and service cuts delay diagnoses and constrain treatment options (Alexiou et al., 2021). Participants described repeated invalidation and disenfranchisement, undermining self-efficacy and shaping pain management. CI theory also highlights intergenerational disadvantage, echoed in participants’ accounts. CI theory intersects with psychobiological models, linking systemic invalidation and prolonged stress to CP. Chronic stress responses, HPA axis dysregulation, and inflammation contribute to persistent pain. Shame, elicited by disenfranchisement in healthcare encounters, activates the threat system, reinforcing emotional distress and CP (Gilbert, 2017). Central sensitisation, heightened by sustained stress and social threat, may biologically amplify the pain experience (Nijs and Van Houdenhove, 2009). Participants’ accounts thus illustrate how systemic invalidation exerts both psychological and embodied effects on CP.
Clinical implications
These findings highlight broader structural inequality within UK primary care. Current health policies, particularly increased scrutiny around long-term opioid use, place GPs under pressure to limit prescribing (Gill et al., 2022). Patients may be unaware of these prescribing constraints, reflecting wider limits on how informed and involved they are in decisions about their care and, whilst clinically justified, such policies intersect with socio-economic deprivation in ways that disproportionately disadvantage those living in poverty.
Participants’ accounts reveal the profound impact of systemic dismissal, disbelief, and moral judgement on people with chronic pain with socioeconomic disadvantage (Hui et al., 2021). These experiences shape self-perception, expectations of care, and engagement with services, often leading to disengagement as a protective response. Abrupt or unilateral opioid withdrawal was frequently experienced as traumatic, contrary to guidelines recommending gradual tapering and shared decision-making (DHSC, 2020; Oliva et al., 2020; Taylor et al., 2021; US Food and Drug Administration (FDA), 2019).
Findings highlight the need for trauma-informed, person-centred care, combining pharmacological and non-pharmacological support in socio-economically deprived communities. Efforts to reduce opioid prescribing should be matched with access to physiotherapy, psychological input, peer support, and pain education, to reduce inequality in pain outcomes (Cohen et al., 2021; NICE, 2021).
Strengths and limitations
This study provides an idiographic exploration of chronic pain within socioeconomic disadvantage, centring voices often marginalised in healthcare. By foregrounding lived experience, it highlights how pain is shaped by social, economic, and political conditions. IPA enabled nuanced engagement with individual meaning-making and systemic factors, while recruitment through a PCN enhanced ecological validity. Limitations include lack of statistical generalisability, a homogenous sample (White British, predominantly female, mean age 56) from a single PCN, and inherent interpretative influence of the researcher’s positionality (Bernardes et al., 2023; Smith and Osborn, 2003). Some experiential threads remain unexplored, and findings offer limited insight into racial, cultural, regional, or younger adult experiences. Despite this, the study contributes meaningfully to understanding chronic pain, inequality, and power, supporting theoretical transferability (Smith and Osborn, 2003).
Future research
This study highlighted the role of power in chronic pain management among socioeconomically disadvantaged groups. Future research should explore other marginalised populations, including women, racialised communities, and those excluded from care, such as individuals with insecure immigration status or in the criminal justice system, where power imbalances are sharpest.
Conclusion
This study examined the lived experiences of people from disadvantaged socioeconomic backgrounds managing chronic pain with prescribed medication. By centring voices often marginalised in healthcare, it highlighted how poverty, stigma, and systemic disadvantage shape both the experience of pain and access to care. Participants described repeated dismissal, disbelief, and moral judgement, contributing to distress and disengagement, while some reported the benefits of consistent, compassionate care. Findings underscore that pain is not only physical but shaped by power and inequality. They support trauma-informed, reflective approaches that recognise how socioeconomic disadvantage and marginalisation influence the experience and treatment of chronic pain.
Footnotes
Acknowledgements
CM gratefully acknowledges, Professor Richard Byng, Dr Annily Dee, and Dr Josh Valroso, for their review of the study proposal and for providing field supervision.
Ethical considerations
The study was approved by the Health Research Authority and Health and Care Research Wales (HCRW) (IRAS: 338938) on October 9th, 2024.
Consent to participate
All participants provided written informed consent prior to participating.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Author CM made a substantial contribution to the acquisition and analysis of the data for the study. All three authors made substantial contributions to the design of the work, interpretation of the data, drafting the work, and revising it critically for content. Author CM had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All of the authors gave final approval of this version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stuart Spicer and Charley Hobson-Merrett were supported by the National Institute for Health and Care Research Applied Research Collaboration South West Peninsula (NIHR PenARC). The views expressed are those of the authors and not necessarily those of the NIHR.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author, CM, upon reasonable request.