
Abstract
Social identity-related group processes are increasingly recognized as influencing psychological and physical health, yet their impact on stress-related biomarkers remains unclear. We conducted a systematic review and meta-analysis of group-based interventions examining physiological markers linked to stress and long-term health. From 1606 records, 14 studies met inclusion criteria. While interventions did not consistently improve biomarkers compared to controls, reductions in blood pressure, increased heart rate variability, and lower salivary cortisol were observed when key group processes (social support, cohesion, working alliance, and social norms) were effectively mobilized. Positive group processes were associated with more adaptive physiological functioning (r = −0.19), where lower scores reflected healthier response profiles (e.g. lower blood pressure). This review provides novel insights into how social identity processes operate in group-based interventions and their potential for shaping physiological health. We highlight the importance of designing interventions that actively foster supportive and cohesive group environments.
Introduction
Group interventions are increasingly recommended for psychological wellbeing, not only across clinical practice but also within workplace and community settings (e.g. International Society for Traumatic Stress Studies, 2018; World Health Organization [WHO], 2016; Worrall et al., 2018). Though available research highlights the psychological benefits of meaningful group memberships (Haslam et al., 2018; Muldoon et al., 2019), two key questions remain unanswered. First, it remains unclear whether any positive effects of group membership extend to health-related biomarkers, here defined as objective measures that serve as indicators of future health outcomes (Califf, 2018). Building on prior research demonstrating a positive effect of groups on subjective wellbeing, the current review aims to determine whether participating in group interventions is associated with more adaptive changes in stress-related biomarkers - such as reduced blood pressure, lower cortisol, or increased heart rate variability - that reflect lower stress and greater physiological resilience and are predictive of future health outcomes. We further aim to identify group processes that might underpin these effects.
Considering the widespread use of group interventions, identifying ways to improve their effectiveness remains an important area of research. Typically, psychological interventions are assessed regarding their content (e.g. cognitive behavioral therapy (CBT), mindfulness, stress management approaches). Instead, the current paper is informed by a social identity approach to health (Haslam et al., 2018), wherein we consider the importance of the group-based context of the intervention. Group interventions provide an avenue for new social identities to form. Social identity can be understood as a person’s internalized sense of self as a group member. Shared social identities enable group members to experience a sense of belonging, connection, and mutual understanding. The extent to which people identify in this way (e.g. as part of “us” therapy group members) can then affect how much they engage with and benefit from group processes such as social support, solidarity, meaning, and control over one’s life (Haslam et al., 2018; Kinsella et al., 2023; Muldoon et al., 2019). These processes are believed to lie at the heart of any therapeutic effects of group memberships, making them a central focus of the current review.
Consistent with this idea, research informed by social identity principles suggests that the effectiveness of a group intervention in terms of improving health outcomes depends on its capacity to foster a valued identity among its members. Indeed, a recent meta-analysis of 27 studies highlighted the importance of building participants’ social identification within an intervention group. Interventions that effectively cultivated a shared identity demonstrated more pronounced effects on psychological outcomes (e.g. stress) as well as physical health indicators (e.g. self-reported physical health and frequency of general practitioner visits; Steffens et al., 2021). On the other hand, support groups structured around an identity which individuals are reluctant to internalize (e.g. Multiple Sclerosis illness identity; Wakefield et al., 2013) and even outright reject (e.g. “victim” of childhood adversity; Lashkay et al., 2023) may have detrimental impacts on health. Even when group members internalize an identity, if that identity is stigmatized or illness-based, it can undermine wellbeing (e.g. identifying with a depression identity; Cruwys and Gunaseelan, 2016). More broadly, when group members fail to integrate, are excluded, or lack sufficient support from group members (Abrams et al., 2005; De Marco and Newheiser, 2019; Stuart et al., 2022), participation in groups can be counterproductive. Together, this evidence suggests that while certain group processes may be therapeutic, others may be detrimental to health. This underscores the value of orienting to social identities and related group processes that emerge during group interventions, particularly when assessing health impacts.
As well as affecting self-reported physical health, there is some evidence suggesting that groups impact biomarkers predictive of long-term health. These biomarkers are tightly linked to stress regulation, reflecting the functioning of the endocrine, cardiac, and immune systems. Dysregulated stress physiology carries significant long-term implications for overall health. For example, dysregulation in both the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system has been linked to cardiovascular (Fuchs and Whelton, 2020) and autoimmune (Ilchmann-Diounou and Menard, 2020) disease morbidity, and even mortality (Karl et al., 2022; Kim and Crimmins, 2020). Biomarkers linked to cardiovascular stress regulation, such as higher resting systolic and diastolic blood pressure (SBP and DBP), and lower heart rate variability (HRV) are linked with greater incidence of physical disease in the long-term, including cardiovascular disease (CVD) and diabetes mellitus (e.g. Hillebrand et al., 2013; Kubota et al., 2017; Sesso et al., 2000, respectively). Higher circulating levels of cortisol and lower levels of dehydroepiandrosterone (DHEA; both stress-related hormones) are linked with CVD risk and all-cause mortality (e.g. Crawford et al., 2019; Shufelt et al., 2010; Vogelzangs et al., 2010). Stress-related inflammatory responses also play a role: elevated circulating inflammatory markers, such as interleukin-4, interleukin-6, and C-reactive protein are linked with a higher incidence of cardiovascular and non-cardiovascular causes of death (e.g. Jha et al., 2010; Ridker et al., 2002). Equally, exaggerated physiological responses to stress are predictive of future negative physical health outcomes (for review evidence, see Turner et al., 2020).
Physiological changes can be detected through biomarkers even when people are unwilling or unable to accurately report their own health status (Aronson and Ferner, 2017). They hold the potential to minimize biases, such as individuals feeling the need to give desirable answers about their health improvement following an intervention. These benefits highlight the usefulness of biomarkers in evaluating group intervention effectiveness and demonstrate why we orient to them in this review.
Group memberships can shape physiological responses to stress, with social identity processes playing a central role. Shared social identification and the support it enables have been shown to influence biomarkers associated with HPA axis functioning and cardiovascular health (Gallagher et al., 2014; Griffin et al., 2025; Haslam and Reicher, 2006; Häusser et al., 2012). These effects are thought to occur because social identities shape whether stimuli are appraised as more or less stressful (Haslam et al., 2004) and whether adequate coping resources are perceived as available (Griffin et al., 2025; Haslam et al., 2005). In experimental settings, shared social identification (Gallagher et al., 2014; Häusser et al., 2012) and the social support that flows from it (Haslam and Reicher, 2006) were linked to lower cortisol responses (Haslam and Reicher, 2006; Häusser et al., 2012) and more adaptive cardiovascular responses to stress (Gallagher et al., 2014). Evidence from large secondary datasets similarly suggests that access to multiple social identities predicts lower allostatic load (i.e. the cumulative burden on the body’s physiological systems; Gallagher et al., 2021), healthier cardiovascular responses to stress (McMahon et al., 2024a), and improved future physical health. Similarly, community group memberships and social integration have been associated with better antibody responses to vaccination (Gallagher et al., 2022; McMahon et al., 2024b). These findings demonstrate that both experimentally induced and naturally occurring social identities can have measurable effects on stress-related biomarkers and downstream health. What remains less clear, however, is whether the social identities and group processes that emerge within group-based interventions exert similar benefits. The present review addresses this question.
The present research
The present research systematically reviews the literature on group-based interventions and stress-related biomarkers, including those assessed at rest and in response to acute stressors, with particular attention to the group processes that may underlie observed effects. By building on prior reviews and meta-analyses that have examined how stress-related biomarkers cluster together and relate to psychological stress more broadly (e.g. Gu et al., 2025; Shah et al., 2024), we focus on biomarkers theoretically linked to stress and long-term health outcomes.
Group-based interventions are here defined broadly as structured group programs delivered in clinical or health-related contexts to improve coping, wellbeing, or adjustment using psychological, behavioral or supportive components. Such interventions are designed to assist an interdependent collection of individuals in pursuing shared intrapersonal, interpersonal, or task-related goals (Association for Specialists in Group Work, 2000). This encompasses group-based programs targeting both psychological and physical health conditions, in which group dynamics and processes are central to intervention effects. This framing aligns with emerging evidence that interventions for physical illness can yield psychological benefits via social identification and related group processes (e.g. Hollands et al., 2024).
Our first aim is to determine whether participation in group-based interventions is associated with adaptive changes in psychophysiological functioning (e.g. reduced stress markers at rest or more regulated physiological responses to stress). Specifically, we evaluate biomarker changes in intervention participants compared with controls, to assess the extent to which group interventions may influence stress-related biomarkers and, by extension, long-term physical health.
Second, we examine whether changes in biomarkers are associated with specific group processes, such as social support, to clarify the mechanisms through which group interventions may influence health. This approach addresses an important gap in the Social Identity Approach to Health literature which has predominantly evaluated self-reported health outcomes (e.g. Haslam et al., 2018) and provides evidence to guide clinical practice by highlighting when and how group-based formats may support stress regulation and long-term health.
Although the interventions included in this review draw on a variety of therapeutic approaches, we consider them together because our primary focus is on the group context itself, particularly the social identities and processes it generates, rather than on modality-specific techniques. This rationale aligns with broader “common factors” perspectives, which suggest that shared relational and contextual processes account for substantial variance in intervention outcomes, often beyond differences in specific techniques (de Felice et al., 2019). Consistent with this view, the present review does not aim to compare the efficacy of individual modalities but instead examines how group-based processes operate across diverse health- and wellbeing-related interventions.
Method
Preregistration
In line with best practice guidelines (Moher et al., 2015), the review protocol was preregistered on PROSPERO (registration number: PROSPERO 2023 CRD42023390747). We fully adhered to the pre-specified inclusion and exclusion criteria, the coding and data extraction, and the analysis strategy within the protocol. A deviation from the protocol comprised adding the CINAHL Complete database as a complementary source during the literature search phase.
Inclusion and exclusion criteria
For inclusion in the review, studies were required to meet the following criteria: (1) be available in English; (2) involve adult participants (i.e. over 18); (3) who were engaged in a group-based intervention conducted in an applied setting (e.g. clinical, organizational, or community contexts); (4) include quantitative measures of pre- and post-intervention biomarker(s) associated with stress regulation and downstream health (i.e. cardiovascular, inflammatory, HPA axis parameters) either at rest or in response to an acute laboratory stress task; and (5) report measures of group processes relevant to the intervention (e.g. social identification, social support). Both experimental and quasi-experimental designs were included. Studies did not necessarily require a control group; where independent group designs were used, acceptable comparators included individual-level interventions, care as usual, or waitlist controls.
Studies were excluded if they: (1) were simulation studies and laboratory experiments which manipulated group identity for the purpose of an experiment; (2) failed to report biomarkers; (3) failed to report group processes relevant to the intervention; and (4) involved child or adolescent participants.
Search strategy
The systematic literature search process is outlined below in Figure 1. A search for relevant published work was conducted via MEDLINE, PsycINFO, CINAHL Complete, and Web of Science Core Collection. The reference lists of any review articles were examined to identify additional relevant articles, as were the reference lists of all studies included in the present review. Gray literature (unpublished work) was retrieved via the ProQuest Dissertations and PsyArXiv databases. Additionally, a call for unpublished data was sent out via the authors’ academic Twitter accounts, as well as to the distribution lists of the European Association of Social Psychology, American Psychosomatic Society, Society for Psychophysiological Research, and Society for Personality and Social Psychology.
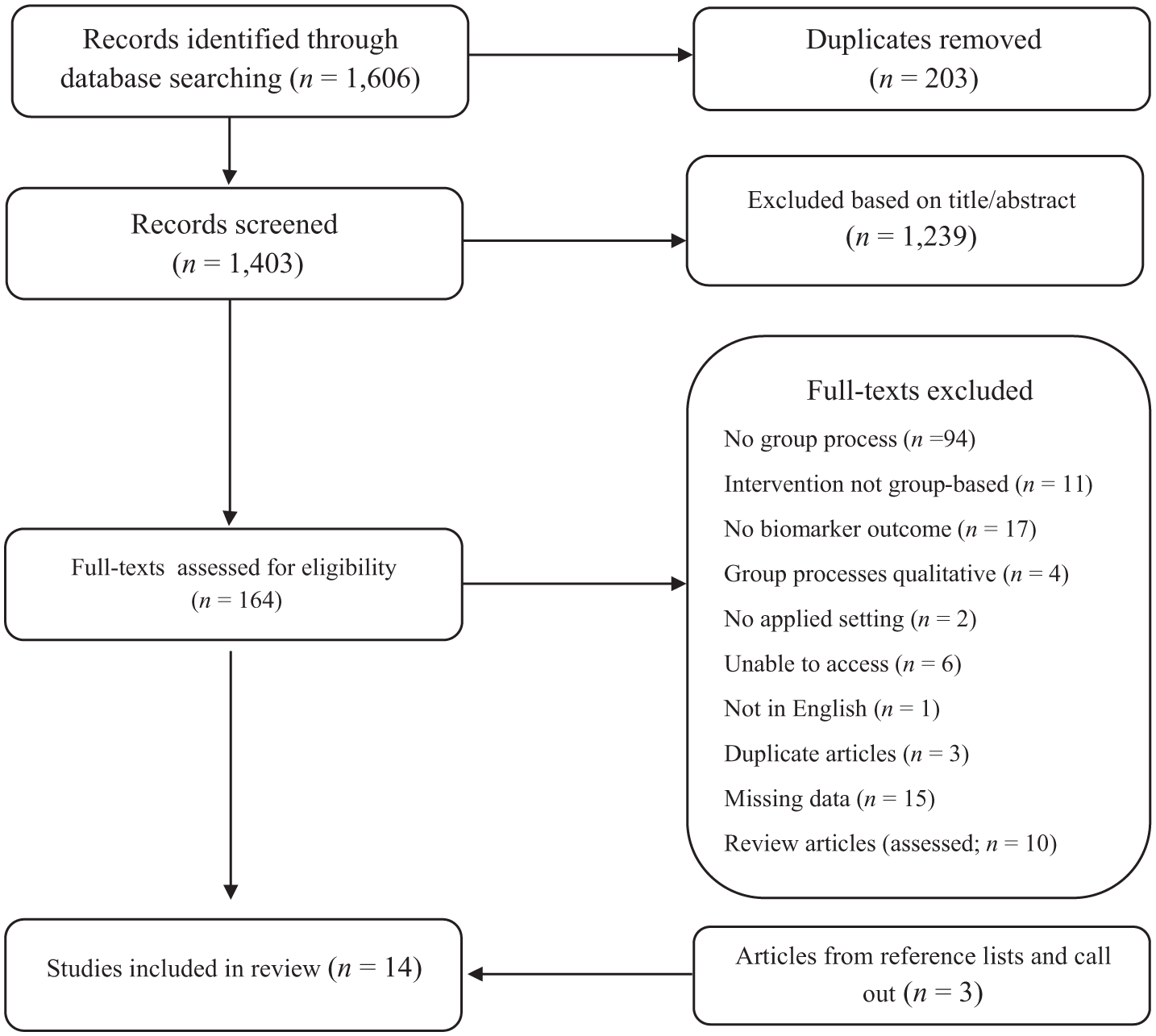
PRISMA flow chart.
To capture maximum relevant work, the search strategy was adapted with database-specific subject headings (e.g. MeSH terms in MEDLINE). In line with best practice guidelines (e.g. Lefebvre et al., 2023), a wide range of key text words was used consistently across databases to maximize the number of hits. Proximity parameters and truncation symbols were applied. See Table 1 for a sample search strategy.
Search strategy utilized in MEDLINE a .
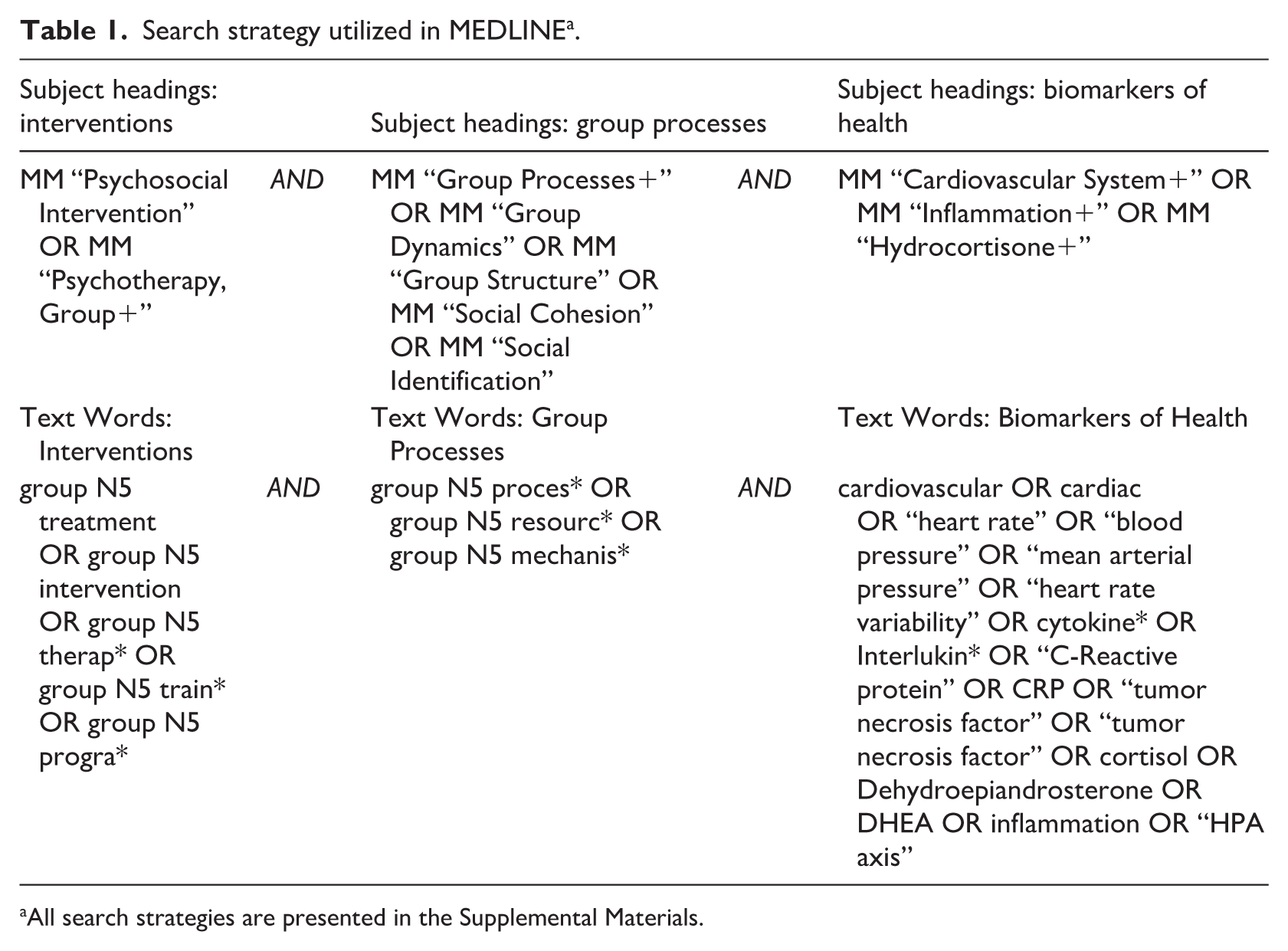
All search strategies are presented in the Supplemental Materials.
The initial search for literature was carried out on the 12th of January 2023 and repeated on the 19th of August 2025. A total of 1606 records were retrieved using this search strategy. Duplicates (n = 203) were removed, leaving 1403 unique records. The title and abstract of each record were screened against the inclusion criteria by the first author. Ten percent of these records were randomly selected and assessed by a second reviewer to check agreement regarding inclusion and exclusion of articles. There were no cases of disagreement (Cohen’s κ = 1).
All potentially relevant articles, totaling 164 records (152 articles and 12 gray literature sources) were included in the full-text screening phase. The first author assessed all identified studies against eligibility criteria, with a random 10% sample also reviewed by a second author. No disagreements occurred among the review team (Cohen’s κ = 1). From this process, 11 records met the inclusion criteria. Three additional records were sourced via our call for data (n = 1) and the reference lists of included studies (n = 2), resulting in a total of 14 records with 19 independent samples.
Data extraction
The final sample of included studies is presented below in Table 2. The first author extracted the data using a standardized form on Microsoft Excel. The following information was extracted: article information (author(s), year, title, country); population (participant demographics, recruitment information, sample size); intervention (study design, type of group intervention); baseline measures (biomarkers, group processes); and post-intervention measures (biomarkers, group processes).
Overview of included studies.
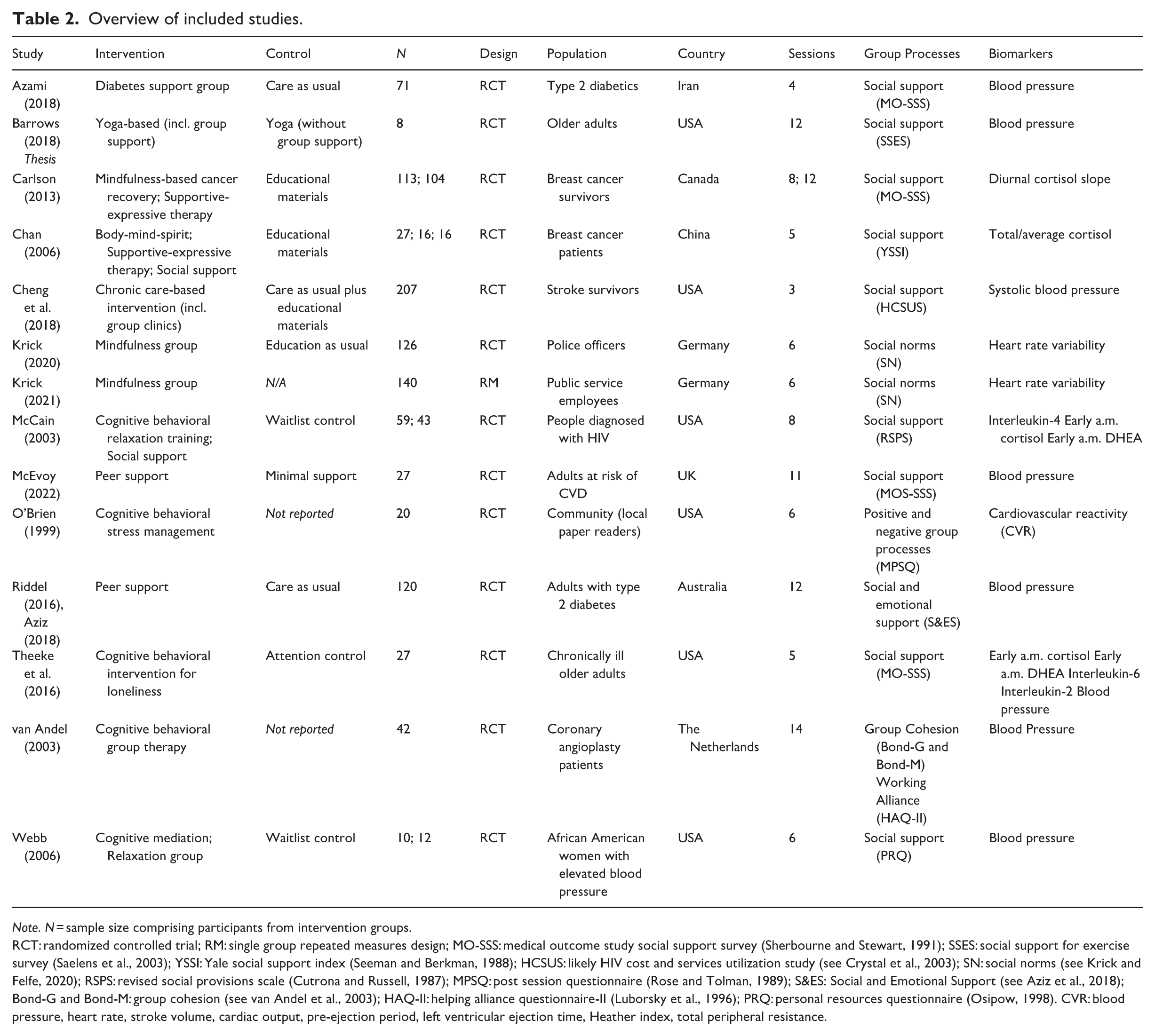
Note. N = sample size comprising participants from intervention groups.
RCT: randomized controlled trial; RM: single group repeated measures design; MO-SSS: medical outcome study social support survey (Sherbourne and Stewart, 1991); SSES: social support for exercise survey (Saelens et al., 2003); YSSI: Yale social support index (Seeman and Berkman, 1988); HCSUS: likely HIV cost and services utilization study (see Crystal et al., 2003); SN: social norms (see Krick and Felfe, 2020); RSPS: revised social provisions scale (Cutrona and Russell, 1987); MPSQ: post session questionnaire (Rose and Tolman, 1989); S&ES: Social and Emotional Support (see Aziz et al., 2018); Bond-G and Bond-M: group cohesion (see van Andel et al., 2003); HAQ-II: helping alliance questionnaire-II (Luborsky et al., 1996); PRQ: personal resources questionnaire (Osipow, 1998). CVR: blood pressure, heart rate, stroke volume, cardiac output, pre-ejection period, left ventricular ejection time, Heather index, total peripheral resistance.
Quality assessment
A quality assessment was conducted by the first author, and cross-checked by a second author, to critically evaluate the evidence presented in the retrieved studies, and to speak to the reliability of the findings. For studies with randomized controlled trial designs, we used the gold-standard Cochrane risk-of-bias tool for randomized trials (RoB 2; Sterne et al., 2019). For non-randomized designs, we used the counterpart Risk of Bias in Non-randomized Studies – of Interventions (ROBINS-I; Sterne et al., 2016).
Data synthesis and analysis
Inverse variance weighting, random effects meta-analysis was conducted using the meta package (v7.0–0; Schwarzer, 2007; Schwarzer et al., 2015) in R (v. 4.4.1; R Core Team, 2022) to determine the efficacy of group-based interventions, relative to control, to improve biomarkers associated with stress and long-term health. Cohen’s d effect size estimates were calculated as M2–M1/SDpooled, utilizing data reported at post-intervention assessment (Higgins et al., 2023), with necessary conversion formulas used to derive estimates of the standard deviation in instances where the required descriptives were not reported (Higgins et al., 2023). Hedges’ g correction factor for small sample bias was applied.
As the interpretation of biomarkers varied across the outcomes (i.e. lower scores representative of better/worse long-term health), effect estimates were inverted so that across all studies, a negative effect estimate consistently indicated more adaptive stress-related physiological outcomes. When studies reported on several biomarker outcomes, outcomes were combined using formulas provided by Borenstein et al. (2021) in order to generate a composite health-related biomarker study effect estimate, thus, avoiding dependency among study estimates (Cheung, 2019). A proxy r estimate of 0.7 was used to denote the correlation between outcomes, as informed by work by Gavish et al. (2008) on the correlates of systolic and diastolic blood pressure. Multi-arm trials were collapsed so that all relevant group interventions were combined and then a summary effect estimate generated, relative to control (Borenstein et al., 2021).
A subsequent meta-analysis was then conducted to determine the association between group processes and biomarkers. Correlation coefficients were extracted, and when necessary, generated from available statistics such as standardized beta (Peterson and Brown, 2005) and the t-statistic (effectsize package; Ben-Shachar et al., 2020). The metacor function from the metafor package (v4.6-0; Viechtbauer, 2010) was used to automatically produce Fisher r-to-z transformed correlation coefficients before pooling for synthesis in meta-analysis using inverse variance, random effects modeling. A negative effect estimate indicated that positive group processes were associated with better health biomarker outcomes. Where relevant, study-level estimates were inverted to ensure consistency in the interpretation of effect across the studies.
Meta-analytical findings were evaluated in accordance with the Z statistic at 0.05 alpha level. Heterogeneity was assessed using the Cochrane Q test. Tau2 provided a measure of the extent of variation in intervention effects (Deeks et al., 2023), whilst I2 quantified the extent of total heterogeneity that was due to true differences and not sampling error, interpreted in accordance with 25%–49% = low, 50%–74% = moderate, 75% + = high (Borenstein et al., 2021). A mean weighted effect estimate and 95% confidence intervals were presented visually on Forest plots to illustrate the study-level and summary-level effect estimates. A Forest plot visually presenting the study-level and summary-level estimates, per meta-analysis, was generated.
Given the heterogeneity among studies in terms of their outcomes (see Table 2), a critical narrative analysis is also presented to give further insight into trends among studies.
Results
Key findings
Effects of group participation on health-related biomarkers
Eleven studies used randomized controlled designs with reported control group data (i.e. waitlist control, usual care, or individual intervention), allowing evaluation of whether group participation was indeed therapeutic (see Figure 2). On average, group interventions did not produce significantly better health outcomes, relative to controls, g = 0.28, 95% CI (−0.17, 0.72), Z = 1.21, p = 0.23. However, this nonsignificant effect should be interpreted with caution, as there was substantial heterogeneity (k = 11) among the study estimates, Q(10) = 119.16, p < 0.001, τ2 = 0.50, I2 = 92%.
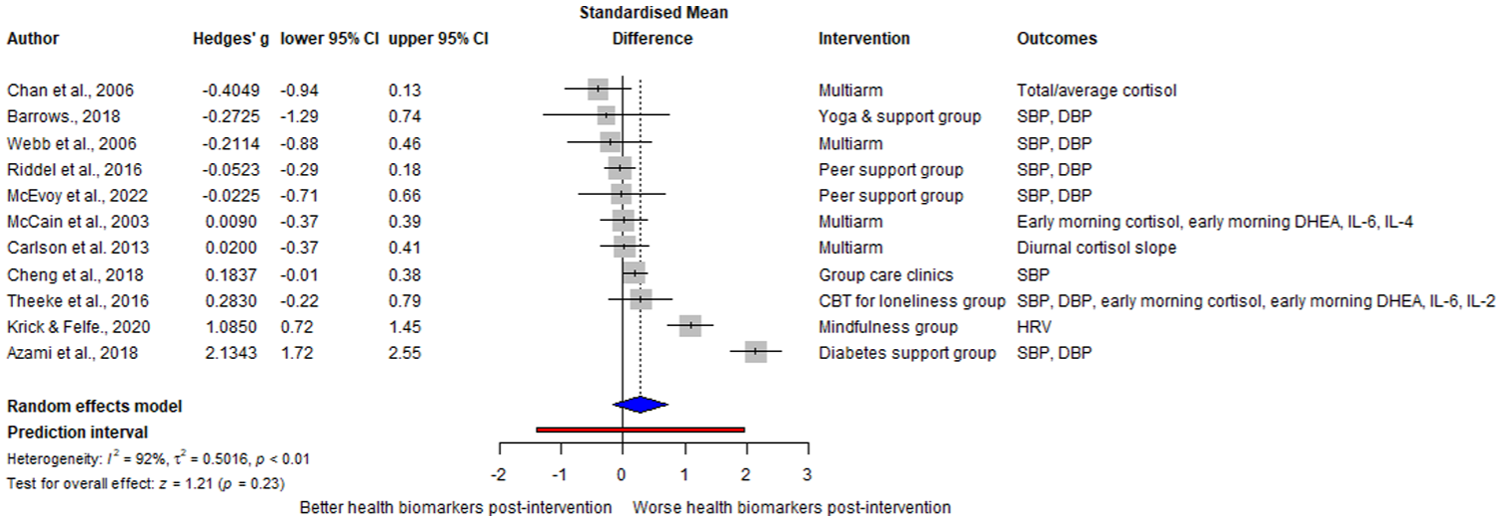
Forest plot of therapeutic group intervention efficacy for health-related biomarkers relative to control (k = 11).
A closer examination revealed that some group interventions improved stress-related biomarkers when compared to controls: illness-related support groups lowered systolic and diastolic blood pressure (Azami et al., 2018; Theeke et al., 2016), mindfulness increased heart rate variability (Krick and Felfe, 2020), and social support-based groups lowered salivary cortisol (Chan et al., 2006). However, seven studies found no biomarker effects across diverse modalities, including support groups, CBT, mindfulness, and relaxation (Barrows, 2018; Carlson et al., 2013; Cheng et al., 2018; McCain et al., 2003; McEvoy et al., 2018; Riddell et al., 2016; Webb et al., 2006).
Where biomarkers improved, this was accompanied by increased social support (Azami et al., 2018; Chan et al., 2006; Theeke et al., 2016), whereas lack of improvement coincided with unchanged social support (Barrows, 2018; Carlson et al., 2013; McCain et al., 2003 – CBT groups) and even decreased social support (McCain et al., 2003 – social support groups). It is notable that there was no consistent pattern linking the type or content of group intervention offered and biomarker outcomes. Indeed, among the six interventions that included content directly relevant to stress reduction (e.g. mindfulness, yoga, relaxation techniques), only two produced improvements across stress-related biomarkers (Chan et al., 2006; Krick and Felfe, 2020), indicating that the inclusion of stress-reduction content alone was often insufficient to produce biomarker changes.
Processes contributing to intervention group effectiveness
Four studies reported the direct relationship between group processes and stress-related biomarkers, while other studies measured group processes as study outcomes rather than predictors of biomarker changes. In line with the study protocol, we contacted the authors of each study that met inclusion criteria to request data to evaluate this direct relationship. Two authors provided this data (Carlson et al., 2013; Krick et al., 2021). Data from six studies were used to explore the direct role of group processes as potential underlying mechanisms of group intervention effectiveness (see Figure 3).
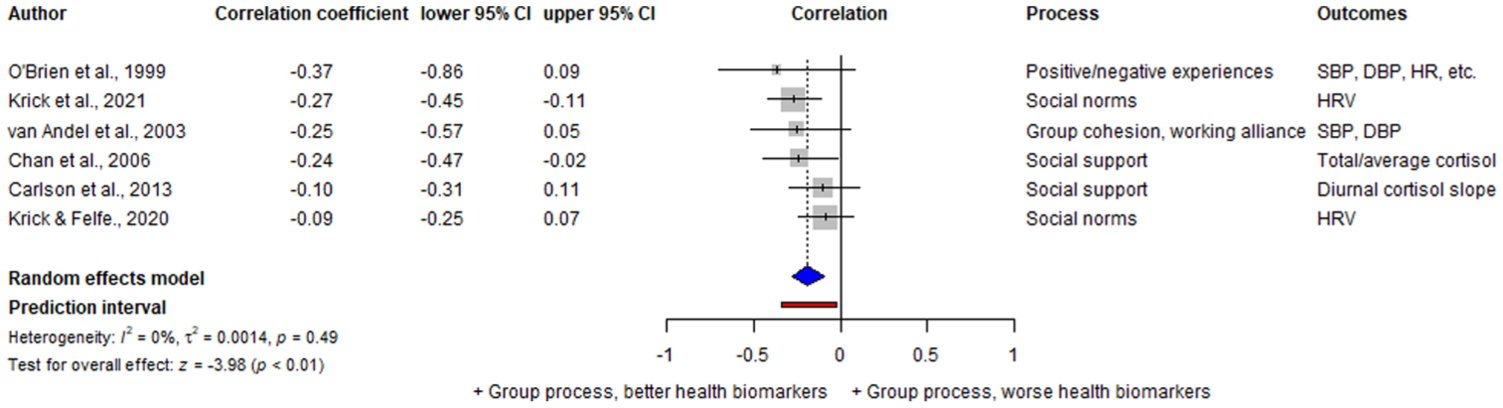
Forest plot of association between group processes and health-related biomarkers across total study samples (k = 6).
Group processes were found to have a significant, small association with health-related biomarkers, in that positive group processes were related to better biomarker outcomes, r = −0.19, 95% CI (−0.28, −0.10), Z = −3.98, p < 0.001. Non-significant heterogeneity was observed across the studies, Q(5) = 4.44, p = 0.49, τ2 = 0.001, I2 = 0%. The few studies that were available (k = 6) limit the power for further analyses and preclude a firm conclusion. Nonetheless, the prediction interval suggests that the true effect size of future studies would likely also indicate that positive group processes are associated with better health-related biomarkers.
Closer examination of CBT (van Andel et al., 2003), mindfulness (Krick et al., 2021), and supportive-expressive or social support (Chan et al., 2006) groups suggested that positive group processes contributed to biomarker improvements. Higher group cohesion (i.e. participants’ sense of belonging, commitment, and value within the group) predicted reductions in resting systolic and diastolic blood pressure, and stronger working alliance (i.e. both the individual therapist-participant relationship and the collaborative supportive dynamic within the group setting) predicted lower systolic blood pressure (van Andel et al., 2003). Greater perceived social support from close others was associated with lower post-intervention cortisol (Chan et al., 2006), while endorsement of positive social norms (i.e. perceptions that fellow group members valued participation) predicted greater improvements in heart rate variability (Krick et al., 2021).
However, in several studies, processes were unrelated to outcomes. Social norms did not predict heart rate variability in police officers (Krick and Felfe, 2020), and social support did not predict cortisol among breast cancer survivors in mindfulness or supportive-expressive interventions, though cortisol itself did not change in these groups (Carlson et al., 2013). In a CBT stress management group, positive process ratings were unrelated to cardiovascular reactivity, but negative process ratings predicted increased reactivity (O’Brien et al., 1999).
Quality assessment
The results of the Risk of Bias tool for Randomized Trials (RoB 2; Sterne et al., 2019) and Risk of Bias in Non-randomized Studies – of Interventions (ROBINS-I; Sterne et al., 2016) are presented in Table 3. Eight out of 14 studies were assessed as having an overall low risk of bias, with six articles raising some quality concerns.
Quality assessment–randomized controlled trials (RoB 2).
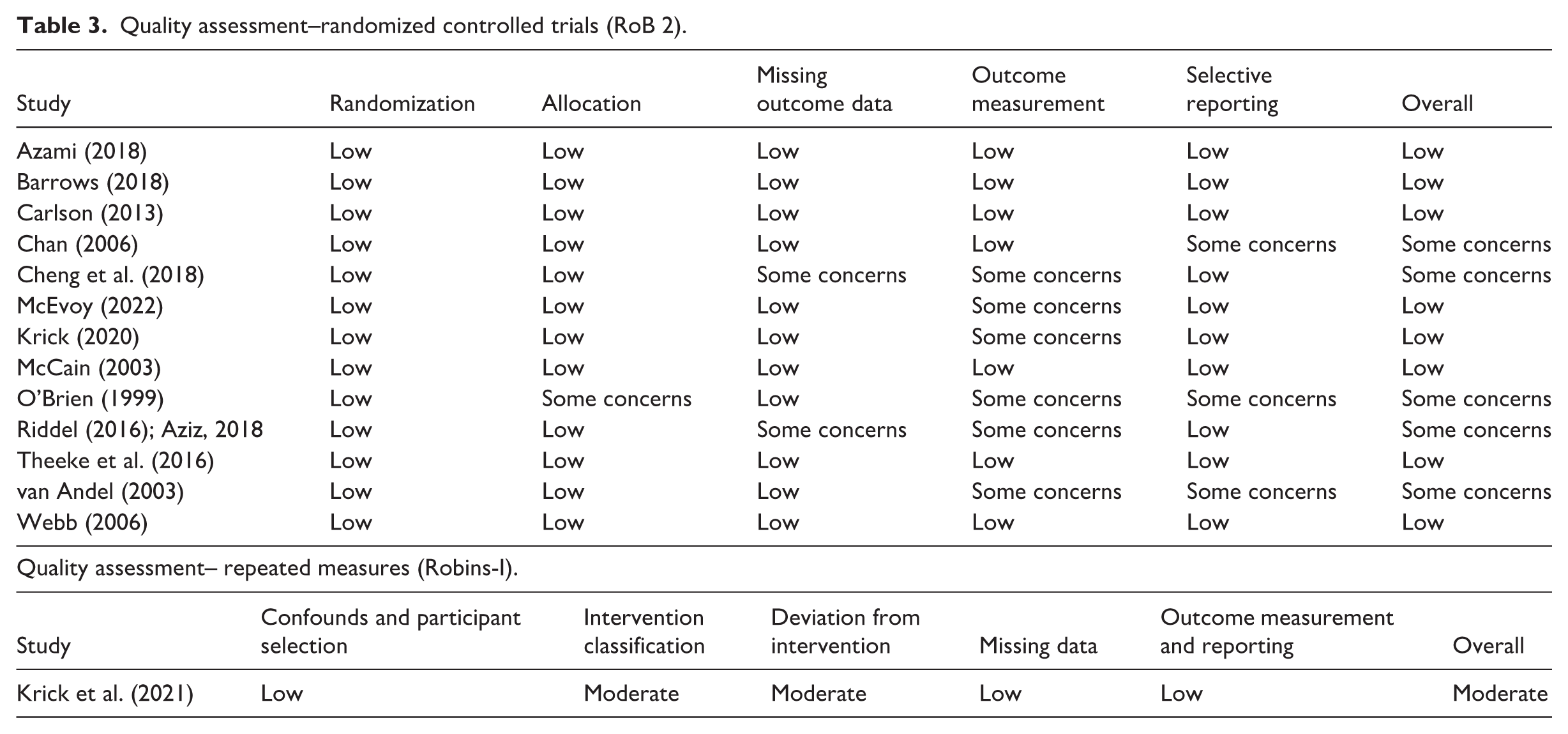
All studies reported adequate randomization processes, and there were no indicators of bias regarding assignment to intervention. Another strength across most studies was the use of well-validated protocols for biomarker measurement. The methods used to measure blood pressure, salivary cortisol, and blood-derived immune function markers are commonly used across health research and were carried out to a sufficient degree of quality. However, when it came to measuring group processes, we identified that four studies used customized measures (Krick et al., 2021; Krick and Felfe, 2020; O’Brien et al., 1999; van Andel et al., 2003). While these measures were developed using existing well-established scales, no validity analysis was reported on the author-developed items. Two studies did not clearly report which measures were used to assess processes (Cheng et al., 2018; Riddell et al., 2016).
Two studies failed to report control group data (O’Brien et al., 1999; van Andel et al., 2003), and three studies failed to report the direct relationship between social support and intervention outcomes despite its identification as a key moderator or mediator of intervention effectiveness (Cheng et al., 2018; McEvoy et al., 2018; Riddell et al., 2016). Three studies reported results that were selected from multiple eligible time-points (Chan et al., 2006; O’Brien et al., 1999) or multiple eligible analyses of the data (van Andel et al., 2003).
Discussion
This review examined whether participating in group-based interventions influences stress-related biomarkers and which group processes may drive these effects. Overall, group participation alone did not consistently improve biomarkers: some interventions showed positive changes (n = 4), while others did not (n = 7). Importantly, no clear pattern linked intervention type or content to outcomes; improvements were observed across support groups, CBT, supportive-expressive, and mindfulness groups, but similar interventions sometimes yielded no benefit.
Instead, the evidence suggests that positive group processes (including social support, cohesion, working alliance, and endorsement of social norms) were associated with biomarker improvements. For example, reductions in blood pressure coincided with greater social support and cohesion (Azami et al., 2018; Theeke et al., 2016; van Andel et al., 2003), while improvements in cortisol and heart rate variability were directly linked to social support and positive norms (Chan et al., 2006; Krick et al., 2021). These findings highlight the central role of group dynamics in shaping physiological outcomes.
The meta-analysis found no overall advantage of intervention groups compared to controls, with most trials (n = 7) showing no biomarker improvements. Notably, when group processes were reported longitudinally, null biomarker effects coincided with no improvement in social support - the most frequently studied process (Barrows, 2018; Carlson et al., 2013; McCain et al., 2003). In two trials where blood pressure did not improve (Cheng et al., 2018; Webb et al., 2006), social support was not reported. While one study found positive processes did not influence cardiovascular reactivity (O’Brien et al., 1999), negative group dynamics (e.g. conflict and anger) were linked to maladaptive stress responses.
These results suggest that simply being allocated to a group intervention may be insufficient to improve stress-related biomarkers. Consistent with the social identity approach to health (Haslam et al., 2018), intervention success may instead depend on group dynamics and processes. Prior work suggests that outcomes are likely influenced by the extent to which members identify with the group (Steffens et al., 2021; Wakefield et al., 2013), viewing membership as an important part of their self-concept, thereby enabling benefits from positive group processes (Haslam et al., 2018; Kinsella et al., 2023; Muldoon et al., 2019). Notably, no included studies directly measured social identification, highlighting a gap in applying this framework to therapeutic group outcomes.
An interesting disparity in our findings was observed concerning the impact of social norms on heart rate variability. Positive social norms (defined as “positive expectations and attitudes” of group members toward the mindfulness–based intervention; Krick et al., 2021:223) contributed to improved heart rate variability in a sample of public service employees (Krick et al., 2021), but not in police officers (Krick and Felfe, 2020). These conflicting findings may reflect differences in social identity content (Robertson et al., 2024). Police identity has been associated with traditionally masculine social norms (du Plessis et al., 2021), emphasizing stoicism and emotional control (Grupe et al., 2021). In these contexts, seeking help and engaging in mindfulness might be perceived as a sign of vulnerability. Thus, positive social norms toward mindful practices may be less prevalent, mitigating their impact on heart rate variability. An important avenue for future research could therefore be to examine a range of group processes and determine which ones are most health-protective across different group interventions (with different associated social identities).
Together, these findings contribute to the advancement of the social identity approach to health (Haslam et al., 2018) by moving beyond self-reported health outcomes, and synthesizing evidence linking group processes to stress-related biomarkers. They also have practical implications, identifying group processes that may be leveraged by facilitators to promote health. Facilitators may prioritize building a positive and cohesive group identity (e.g. “us in recovery”), establishing positive social norms that are relevant to the group (e.g. attending group meetings, engaging in group activities), encouraging group members to collaborate (i.e. working alliance), and supporting each other both within and outside of the group environment (i.e. social support). Indeed, these recommendations echo previous work on “social scaffolding” in community groups (Haslam et al., 2019).
Strengths, limitations and future directions
This review makes an original contribution by examining how specific group processes relate to objective biomarkers of stress. Incorporating studies from multiple countries (Iran, USA, Canada, China, Germany, UK, Australia, and the Netherlands), it addresses a globally relevant question and extends the social identity approach to a novel domain of physiological outcomes and long-term physical health. By highlighting that group processes, rather than intervention content per se, may drive health improvements, the review provides actionable insights for theory, practice and policy.
Several limitations warrant consideration. First, heterogeneity in designs, populations, and biomarkers complicates interpretation (Higgins et al., 2002), and limited reporting transparency may increase the risk of selective reporting. Future research should adopt open science practices, including pre-registration and data sharing (Forstmeier et al., 2017; Nosek et al., 2018; Tedersoo et al., 2021). Second, some interventions targeted stress directly (e.g. mindfulness, yoga), meaning biomarker changes may partly reflect individual rather than group-level mechanisms. Although no consistent pattern linking intervention content and outcomes emerged, direct comparisons of group versus individual formats and component network meta-analyses could clarify mechanisms of action (Barrows, 2018; Petropoulou et al., 2021).
Third, although social support was frequently assessed, measures often failed to specify its source. Only one study isolated support from group members (Riddell et al., 2016). Future work should measure group-derived support explicitly. Finally, no studies assessed social identification, despite evidence that it shapes engagement and benefit from groups (Steffens et al., 2021). Including these measures would clarify when and for whom group processes are most beneficial.
Conclusion
This systematic review advances the social identity approach to health by identifying processes through which group interventions may influence physiological stress markers and, in turn, long-term health. Our findings suggest that cultivating social support, cohesion, working alliance, and positive social norms may positively influence cardiovascular and endocrine biomarkers linked to stress.
However, improving evidence quality is essential to understand how the group format can be harnessed to promote health. We thus encourage future research to systematically measure group processes and social identification across diverse therapeutic contexts. Given the growing prevalence of group interventions across clinical practice and workplace programs, such research holds promise in enhancing their effectiveness and ultimately contributes not only to psychological wellbeing, but also better physical health outcomes.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261436307 – Supplemental material for Group processes and physiological health in group-based interventions: A systematic review
Supplemental material, sj-docx-1-hpq-10.1177_13591053261436307 for Group processes and physiological health in group-based interventions: A systematic review by Alžběta Lebedová, Siobhán M. Griffin, Elayne Ahern and Orla T. Muldoon in Journal of Health Psychology
Footnotes
Ethical considerations
This systematic review was conducted using publicly available published and gray literature. No new human or animal data were collected, and no direct interaction with participants occurred. The review adhered to established ethical guidelines for research integrity, including accurate data representation, proper citation of sources, and compliance with relevant reporting standards (e.g. PRISMA).
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
1. Alžběta Lebedová contributed to the study conception; design; execution; data acquisition, analysis, and interpretation; article writing.
2. Siobhán M. Griffin contributed to the study conception; execution; data acquisition and interpretation; article revision.
3. Elayne Ahern contributed to the study execution; data analysis and interpretation; article revision.
4. Orla T. Muldoon contributed to the study conception; data interpretation; article revision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alžběta Lebedová and Orla T. Muldoon are funded by the European Research Council (ERC) under an Advanced Grant (Grant agreement No. 884927) awarded to Orla T. Muldoon. The funding source had no role in the study design, data acquisition, analysis, interpretation, or writing of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.