
Abstract
In Malawi, there is a need for resource-appropriate interventions that improve depression among adolescents living with HIV (ALWH) that incorporate their service delivery preferences. To understand these preferences, we thematically analyzed qualitative data from a formative study adapting an evidence-based depression intervention for ALWH in Malawi. Participants (N = 42) included ALWH experiencing depression (age 13–19, BDI-II ⩾ 13), caregivers, healthcare providers, implementors, and participants of a similar counseling intervention. Findings revealed a preference for private, clinic-based individual counseling to maintain confidentiality and avoid stigma. While desired frequency for sessions varied, participants consistently wanted young (<40), mature, trustworthy, and non-judgmental counselors. Counseling sessions should address the relationship between HIV and depression and the socioeconomic stressors resulting from living with chronic, stigmatized diseases. Results emphasize the importance of confidentiality, flexibility, and choice when providing mental health services for ALWH, and the need to train lay counselors to navigate discussions around socioeconomic stressors.
Introduction
Globally, adolescents living with HIV (ALWH), age 10–19, have lower rates of antiretroviral therapy (ART) adherence and viral suppression and higher rates of loss to follow-up than adults and children (UNICEF, 2023). This is particularly the case in countries in sub-Saharan Africa (SSA), such as Malawi, where approximately 3% of the adolescent population is living with HIV, and viral suppression estimates among those on ART range from 48% to 78% (Ciesla and Roberts, 2001; Cluver et al., 2012; Domek, 2010; Kamau et al., 2012; Kemigisha et al., 2019; Kim et al., 2017; UNAIDS, n.d). Poor engagement and retention in care among ALWH in SSA is the result of a unique combination of psychosocial and structural factors that stem from living with a stigmatized condition in a resource-limited setting during the transition to adulthood (Kim et al., 2015). Such factors also contribute to increased risk of ALWH developing mental health conditions, which in turn exacerbate poor HIV care engagement and low ART adherence (Gamassa et al., 2023; Kemigisha et al., 2019; Kim et al., 2015, 2017; Merrill et al., 2022; Mutumba et al., 2015; Olashore et al., 2021; Too et al., 2021). Depression functions as a barrier to HIV care engagement because it has the potential to disrupt motivation, cognition, social functioning, and future-oriented decision-making which are necessary for consistent clinic attendance and medication adherence (Dinaj-Koci et al., 2019; Gonzalez et al., 2011; Molinaro et al., 2021; Olashore et al., 2021)
Comorbid depression among ALWH in Malawi is high; estimates range from 18% to 26% (Kim et al., 2014; UNAIDS, n.d). Yet, mental health services for common mental disorders in Malawi and SSA at large are often unavailable due to limited infrastructure and human resource capacity (Kauye et al., 2011, 2014; Kip et al., 2022; Udedi et al., 2018; Wright et al., 2014). A growing body of research has demonstrated that task-shifting mental health interventions are an effective strategy for addressing the mental health treatment gap amongst adults, living with and without HIV, in low resource settings (Hoeft et al., 2018). In task-shifted mental health interventions, lay counselors deliver high quality care under supervision. This cost-effective strategy moves beyond a purely biomedical approach, and often incorporates sociocultural frameworks (Burgess, 2015; Petersen et al., 2012, 2013). There is substantial information on adult preferences for counseling therapy, but a scarcity of knowledge concerning counseling therapy preferences among adolescents, particularly ALWH (Brooks et al., 2022a; Myers et al., 2018; Petersen Williams et al., 2020)
Understanding counseling preferences and incorporating them into the delivery of mental healthcare for ALWH is imperative for several reasons. First, this population is particularly vulnerable to poor mental health outcomes and stigma when accessing health services (Cluver et al., 2008; Faidas et al., 2024; Kip et al., 2022; Vreeman et al., 2017). Second, ALWH are at a unique position in the life course where they are just beginning to make independent decisions about health behaviors and social relationships while navigating the transition from pediatric to adult HIV care. Third, health interventions for adolescents are most acceptable and effective when the interventions are accessible, confidential, developmentally appropriate, and contextually relevant (Embleton et al., 2024; World Health Organization, 2012). Fourth, evaluations of the few existing mental health interventions that have been adapted for ALWH in SSA have failed to provide information on the counseling or health service delivery preferences of ALWH (Bhana et al., 2021; Cavazos-Rehg et al., 2021; Dow et al., 2020; Njau et al., 2022; Vreeman et al., 2017; Willis et al., 2018). For task-shifted adolescent mental health counseling interventions to maximize their potential, ALWH must be asked about their preferences for service delivery and have those preferences incorporated into future programing.
To address this gap, we conducted a qualitative study to explore depression counseling preferences among ALWH in Malawi. This study aimed to identify adolescent and stakeholder preferences for counseling setting, timing, delivery, content, and counselor characteristics to inform youth-friendly adaptation of a mental health intervention.
Methods
Study context
Data were from the formative phase of the HIV Engagement and Adolescent Depression Support (HEADS-UP) study, which was conducted among ALWH and relevant stakeholders in Malawi to understand preferences for mental health counseling and optimal strategies for peer support for HIV engagement. Findings from the formative phase were used to adapt the Friendship Bench intervention for ALWH in Malawi and enhance it with peer support for HIV engagement (Dao et al., 2025). The Friendship Bench is an evidence-based problem-solving intervention for common mental health disorders that is designed to be delivered by lay health workers (Chibanda et al., 2016). The adapted and enhanced Friendship Bench intervention will be subsequently tested in a pilot randomized control trial (Dao et al., 2025).
Study sample and recruitment
The study sample included ALWH, caregivers, and HIV care providers, as well as participants and study staff from a previously implemented Friendship Bench intervention for perinatal women living with HIV in Malawi (i.e. Periscope) (Bengtson et al., 2023). ALWH eligible to participate were: (1) ages 13–19; (2) diagnosed with clinic-confirmed HIV; (3) scored ⩾ 13 on the self-reported Beck’s Depression Inventory-II (BDI-II); (4) willing to provide consent (age 18) or assent with parental consent (ages 13–17). All ALWH were eligible for recruitment, including ART initiators, ART re-initiators, and established patients. The BDI-II has been validated for ALWH in Malawi, with a cutoff of ⩾13 demonstrating 80% sensitivity in detecting depressive symptoms (Kim et al., 2014). ALWH screening positive for depression who were ineligible based on other criteria or chose not to participate were referred to a mental health provider for psychosocial counseling. All ALWH who reported suicidal ideation were immediately referred for suicide risk assessment and followed up by the study staff to ensure engagement with care.
ALWH were recruited for in-depth interviews (IDIs), focus group discussions (FGDs), and social support mapping sessions (SSMSs) during Teen Club sessions at three HIV clinics located in peri-urban and urban Lilongwe in Malawi. All clinics were in government health facilities and were matched based on staffing levels, services offered, NGO/ancillary program involvement, patient volume, and patient population. Teen Clubs are adolescent-specific ART programs that meet two weekend days every 3 months and provide ART refills, viral load testing, and psychosocial support, which includes games and education related to ART adherence, nutrition, and sexual/reproductive health. All Teen Clubs provide age differentiated programing for participants ages 10–14 and 15–19 (Alibi et al., 2023; MacKenzie et al., 2017; McBride et al., 2019). Caregivers of ALWH were recruited for FGDs from Teen Club sessions and from routine ART clinic days at each of the study clinics. HIV care providers were also recruited for FGDs from each study clinic. Periscope staff (interventionists and research staff) and participants (young women living with HIV, aged 18–25 years, previously diagnosed with perinatal depression, who received FB counseling) were recruited for IDIs and FGDs via telephone by the research coordinator (Bengtson et al., 2023). Periscope participants (all of whom were young women living with HIV) and staff were regarded as relevant stakeholders given their proximity to ALWH, experience participating in or facilitating counseling sessions, and experience with depression and living with HIV. Using convenience sampling, sample size was structured to meet expectations for near data saturation while also considering resources and time constraints (Squire et al., 2024).
Data collection
The study team conducted 20 IDIs, 3 FGDs, and 10 SSMSs over 4 months in 2024. Semi-structured guides tailored to each participant group were developed for the IDIs and FGDs to explore experiences with depression, HIV care, social support, HIV-related stigma, preferences for mental health counseling, and peer support strategies for HIV care engagement. For the SSMSs, a study team member guided the participants through an exercise and discussion that elicited the structure and function of their social support network and how it impacts their HIV care and mental health. Across all data collection activities, our overall research question was “What are the preferences and priorities of ALWH and stakeholders regarding the design and delivery of youth-friendly mental health counseling?.” All IDIs, FGDs, and SSMSs were conducted in Chichewa, digitally recorded, transcribed, and translated into English by the study staff according to a uniform transcription protocol. All transcripts were reviewed by an interviewer for the accuracy of transcription and translation.
Data analysis
Team members developed a codebook based on the resulting transcripts, interview guide, and study objectives. Each coder then piloted the codebook individually using the same two transcripts via Dedoose. The study team reviewed the coded transcripts for inconsistencies and used consensus to revise the codebook accordingly. Six team members (two Malawian research assistants and four American research assistants (United States)) used the finalized codebook to independently code each of the remaining transcripts and resolved discrepancies through discussion during group meetings until the interrater reliability was found to be acceptable across all transcripts (Cohen’s Kappa > 0.80). All codes related to counseling preferences and mental health services were reviewed and synthesized using analytical matrices which facilitated systematic comparison of information to identify themes. Team members then developed summary memos for each theme. The coding results were reviewed within the context of the full interview transcripts to ensure an accurate interpretation.
Ethical approval
This study was approved by the Institutional Review Boards of the University of North Carolina at Chapel Hill (IRB #22-0462) and the Malawi National Health Sciences Research Committee (IRB #22201). All participants aged ⩾ 18 years provided written informed consent. All participants aged 13–17 provided written assent with their guardian’s written consent. In accordance with the NHSRC ethical standards, emancipated minors below the age of 18, who were legally married or university students, did not require guardian consent. Before study enrollment, the research staff engaged participants in a consent comprehension activity, which asked a series of questions to ensure their understanding of the study. All participants (and guardians, if present) received travel reimbursements equivalent to 10 USD. This study conformed to the principles outlined in the Declaration of Helsinki.
Results
Participant Characteristics
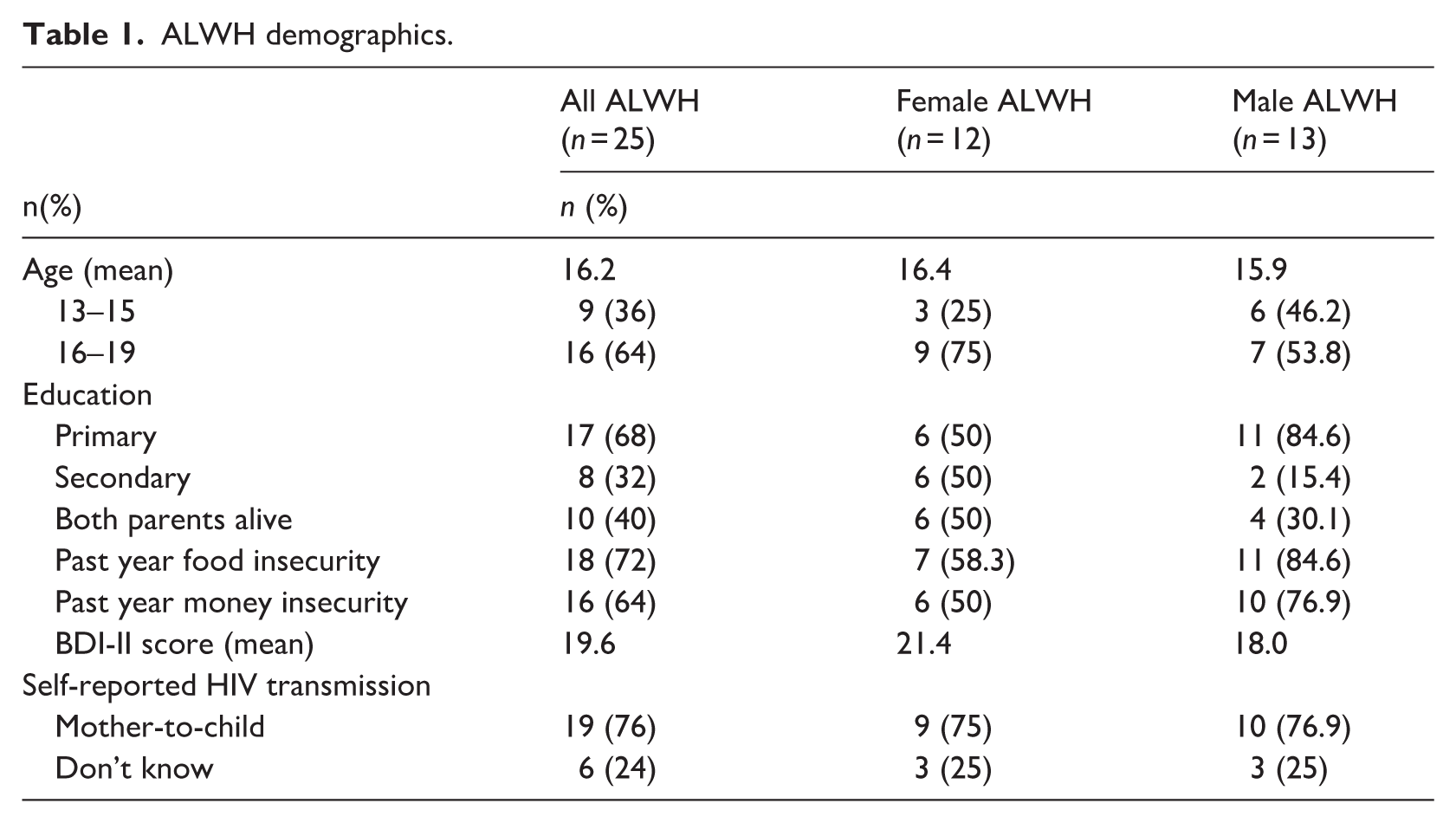
Our total sample included 42 participants. Amongst ALWH (n = 25), the mean age was 16 years, with more than half (64%) between the ages of 16–19. There was a nearly even gender distribution (52% female), approximately one-third (30%) completed primary school, less than half (40%) reported two living parents, three quarters (75%) reported food insecurity, and more than half (64%) reported financial insecurity. BDI-II scores ranged from 13 to 50 (M = 19.4). Female participants endorsed higher BDI-II scores (M = 21.4) than male participants (M = 18.0). Most participants (76%) reported acquiring HIV via mother-to-child transmission, whereas the remainder were unsure of how they acquired HIV (Table 1).
ALWH demographics.
Among caregivers (n = 4), the mean age was 47.8 years with an even gender distribution. All caregivers were married, and reported their professions as gardeners, landscapers, teachers, and businesswomen. HIV providers (n = 4) included nurses and clinicians with a mean age of 38.3 years. Periscope participants and implementors (n = 10), all of whom were female, had a mean age of 23.2 years. The one male study coordinator was 34 years old.
Counseling context
Setting
Broadly, participants felt that health clinics would serve as the best location for counseling. For many participants, clinics were viewed as a familiar place that was already frequented by ALWH receiving ART. Hosting counseling at health clinics would lower the burden on ALWH “because the hospital is a place which is easy to access, and whenever you are at hospital you always feel at ease, and this makes you comfortable to talk” ( The hospital is most ideal because they can be getting it [counseling] together with the other HIV care services and also it is a good place where they can tackle all the issues like drug adherence. . . for example, a person has depression and defaulted in his treatment, what’s next? It means the clinician should prescribe or see him. So it can be like a one stop place where all the services can be accessed. . . like issues of family planning, safe motherhood. . . and whatever, name it –
Most participants viewed health clinics as a relatively private setting for counseling compared to their homes or other community locations, which were largely regarded as lacking confidentiality, making ALWH feel more vulnerable to stigmatizing attitudes from friends, family, and other community members. As one Periscope participant reported, “at home or community would not be ideal because it always attracts attention from people and when they hear what you were discussing they will take it and spread about it all over. As such, people start to stigmatize” ( I would be so worried and I can feel bad . . .because she [another clinic attendee] will go around and spread the news that she saw me at hospital receiving counselling and they can discriminate me. If I go to the clinic I want it to be private so they will not know –
Finally, irrespective of participants’ individual preferences for counseling location, most agreed that counseling must occur somewhere tailored to youth. The incorporation of youth-friendly activities like sports and games was frequently cited as integral to retaining youth in care. Some participants mentioned how existing Teen Clubs at local clinics, similar to the ones they were recruited from, would be a natural fit for youth-tailored counseling. In the clinics we have places like youth friendly corners, they were created because youth receiving health services is problematic. Unless when they are suffering from disease like malaria they can mix up with elders. But for diseases like sexually transmitted diseases a lot of youths are shy. So I was thinking that counselling should be done in places that were established for that like the youth friendly corner, where only youths would be meeting and there wouldn’t be other people who can make them shy and fail to open up properly. . . We can just add that since we have teen clubs, where youths report every weekend. So during that time on weekends, when they are all alone I think that is also a good time to give them actual counselling. –
Timing and frequency
Participants prioritized times that would be highly accessible to the youth. For some participants, this meant keeping counseling exclusively to the weekends, especially Saturdays, as “a lot of people [are] free and are at home and we don’t go to school, but if you choose week days you won’t have anyone attending because they will be busy with school” (
There were mixed preferences regarding whether counseling sessions should be aligned with ART medication pick-up. Some ALWH and stakeholders have suggested that synchronizing these appointments could streamline the process to decrease time at the clinic and limit transportation costs. Alternatively, other participants expressed that separate days should be set aside for counseling because ART clinic sessions are already too hectic: Because when we come to get our medication there a lot of activities and it is easy to miss help. While when it is a special day there is no chance that you can miss because it is something you arranged before and nothing will come to disturb you.
Delivery
Participants consistently preferred individual over group counseling sessions, but a few did endorse group counseling for collaborative learning. Some participants also suggested that counseling sessions could be incorporated into existing Teen Club meetings which would make it feel less like going to the clinic. Discussing with them about how daily life is like when you are a youth or youths frequently staying in groups. . . and can talk about things that can change their lives or their problem of having depression for a long time. In a group I am not alone and can learn from others if I am not shy. - When you are just yourself with someone, when he is telling you something you don’t take it seriously. When it is in a group you get attracted and start to think that it is a serious issue because it concerns a larger number of people as you hear from other people’s experience and how they handled it. . . so you have a chance to learn and improve your health. . . from other people’s testimonies like other would say I have heard about this that when you live with depression and when you meet a friend to talk to it helps a lot. –
Some other recommendations to improve counseling delivery included establishing counseling help lines that youth could call that would provide counseling on demand, flexibility in attending sessions, limit stigmatizing experience at health clinics, and eliminate transportation cost for ALWH. You can establish helplines on where a youth can call, helpline is helpful especially in circumstances where others are shy or not comfortable to meet the counselor in person or be seen at the clinic and also you can access it anywhere anytime and you don’t need to organize transport money –
Counselor characteristics
Age
Across participant groups, most individuals expressed their preference for an older, more mature counselor. The preferred age varied greatly and was often between the ages of 20–40 years old. Participants felt that counselors in this age range could take charge, foster trust, and serve as role models. Despite preferring older counselors, participants still agreed that younger (i.e. ⩽40 years) counselors would still be relatable to youth. Notably, almost all participants noted that the counselors should not feel “elderly” in affect, mindset, or dress. Many ALWH indicated that a large age difference would serve as a barrier to openness to speaking about personal issues. For example, Do not be using elderly people the youth. It should be all about the youths so that the youths should be open that if there is something they want to say, they should be able to say. . .He or she shouldn’t be an elder above 40 going upwards, youths will be failing to be open. -
Occupation
Many participants, particularly ALWH, expressed the sentiment that counselors should be an existing authority figure in youths’ lives. Authority figures could command attention and respect from youth, which could facilitate greater knowledge transfer and behavior change.
Various authority figures were mentioned across participant groups (i.e. village chiefs and teachers), but there was a consistent preference for healthcare providers as counselors. Healthcare providers were viewed as most likely to maintain confidentiality. Additionally, many ALWH reported existing relationships with specific healthcare providers, which might facilitate comfort and openness during counseling sessions. Furthermore, participants felt that healthcare providers had an adequate knowledge base to counsel youth on a range of topics including HIV transmission, medication adherence, and coping with depression. We did not find a relationship between AWLH age and counselor occupation preference; that is, both younger and older ALWH reported preferring authority figure with qualities similar to those described above. “They should be people at the clinic. Because at the clinic there are people who studied the mind of a person so they can help you unlike other places who haven’t studied people, so it can be difficult to help you. Since you know that they work at the clinic they subscribe to strict code of ethics so they can’t be going about to people and expose you, and you feel comfortable by how they welcome you.
Qualities of counselor
Participants’ preferences were largely aligned with their descriptions of the necessary qualities for an effective counselor. All groups overwhelmingly reported that counselors needed to be calm, kind, and able to maintain confidentiality. A counselor should be someone who the youth could trust to not inform their families or communities of their HIV status and/or mental health condition: Mainly I think they should be people who know how to keep a secret. Because most of the time, a person who is a counselor has to be someone who can keep a secret. It happens that the counselor is talking to someone who drops all his or her problems to the counselor. So the counselor has to be a person who knows how to keep things a secret and also honors privacy and confidentiality.
Participants also noted the need for a counselor who was “youth-friendly” and non-judgmental. Counselors considered relatable to youth were reported to be more likely to increase receptivity to counseling and to increase the chances of retention in care. Some participants suggested that younger counselors might ensure relatability, while others reported that any counselor, regardless of age, could take steps to become more “youth-friendly”: They should be speaking the same way the youths are speaking so that it should be like they are suiting, things like those. . .Maybe when it comes to dressing, it should be the same way the youths like their fellow youth to be dressing like. For instance, if someone puts on a suit as if he or she is going to meet up with the president the youth will be failing to be open because of the people they have met what and what. But they should be in line with what the youths want; how the youths want that person to be like now and when they grow up. The person should be the same way the youths are. –
Caregivers, HIV providers, and Periscope participants also emphasized the importance of counselors not being ALWH’s caregivers. They reported that having adult role models who could listen patiently without being harsh or jumping to conclusions, as caregivers might be prone to doing, would encourage ALWH to feel comfortable and open in discussing their thoughts and feelings. Parents are harsh they always want to show that they are in control of their children. . .but as a parent you see that the response is totally different when one is harsh, or one is polite. Counselors are more able to control being polite and the youth will appreciate the help and next time open up to them again. – The way parents talk they start to bring in irrelevant factors into consideration, like I know you are doing this because you have so and so. . . parents are too quick to jump into conclusions and then a young person does not want to talk. Counselors should not do those things and it will be good. – Counselors should be patient and understanding because sometimes they [patients] might tell you issues that sound crazy and insensible like someone would tell you that they have stopped taking drugs without any good reason. . .a grandmother would be upset so you can not tell them. I hope the counselor would not be like that. –
Finally, a minority of participants suggested that counselors should also be living with HIV. ALWH felt that counselors living with HIV would be more capable of empathizing with them and tailoring counseling content to their lived experience: But when a person who has HIV is telling the youth, us youth can understand quickly because the person also takes medication. And also for a person with no HIV to be talking to one with HIV, the way that person might talk wouldn’t be helpful because that person might lack necessary skills to help a person understand properly like the depression problem, how to take medication and so on. However, if it’s from someone who is taking medication and is passing through the same thing, that person would know that this person is passing through this because of this. –
Counseling content
Content
Participants consistently expressed the need for counseling that examined the intersection between depression and HIV. While counseling was initially intended to focus primarily on depression, participants emphasized how HIV and depression are often inextricably linked. Participants spoke about how a lack of HIV education can elevate feelings of depression and recommended that counseling sessions cover information about HIV, common causes of depression, and adaptive coping strategies. Some are depressed because of things like those that they got the virus from parents but they didn’t explain to them properly or they their friends do not come to their house or they are feeling down because they have not told their boyfriend their status so the counselor should discuss all of those things. –
Outside of depression and HIV stressors, many participants conveyed the need for counseling that provided practical assistance to ALWH (i.e. helping individuals find jobs, food, etc.) because many ALWH face problems with unemployment and food insecurity, which exacerbate their existing HIV and depression. So I think apart from giving them counselling sessions only, it’s good to give them some strategies that can help them find their daily bread so that taking medication should not be a problem. . .many times a lot of them had the desire to take medication but because of not finding enough there was a problem. . .So maybe if there was a way to help with this situation in counselling I think that would be helpful. –
Discussion
This qualitative study aimed to identify preferences for mental health counseling amongst AWLH, caregivers, healthcare providers, and previous clients and implementors of a mental health counseling intervention in Malawi. Most participants preferred clinic-based delivery and individual counseling sessions to maintain their privacy and avoid stigmatization. The suggested frequency of counseling sessions ranged from daily to four times a month, and ALWH were mixed on whether counseling should occur on ART medication pick-up days or on separate days. All participant groups consistently reported that counselors should be young (age < 40 years), mature, and discreet authority figures who can engage with youth with relatable affect, dress, and non-judgmental attitudes. Suggested content for counseling sessions included acknowledging the bidirectional relationship between depression and living with HIV and providing coping strategies for both conditions as well as common socioeconomic stressors.
The need for privacy and confidentiality was a consistent theme across the reported preferences for counseling contexts and counselor qualities. The preference for counseling in individual sessions, private clinic settings, and via telephone was often rooted in the desire to avoid being seen and stigmatized by family, friends, and community members. Similarly, the most frequently named counselor quality was trustworthiness. Participants, particularly ALWH, emphasized the importance of ensuring that counselors would not inform their families, friends, and communities of their HIV status or mental health condition, either through good intention or through gossip. These results are aligned with existing literature on the relationship between stigma and healthcare engagement amongst ALWH in Malawi and across sub-Saharan Africa (Enane et al., 2020; Faidas et al., 2024; Kim et al., 2015; Kip et al., 2022; Zanoni et al., 2021). Stigma is an established barrier to HIV and mental health care treatment and often driven by misinformation, fear of infection, social ramifications, and judgment as well as internalized blame and stereotyping (Embleton et al., 2023). The World Health Organization’s guidance for youth friendly health services recommends the implementation of policies and procedures that guarantee client privacy and confidentiality not only during consultation but also during registration, record-keeping, and referrals (World Health Organization, 2012). The current 2020–2030 Malawi National Youth Friendly Health Services Strategy mentions that client rights include privacy and confidentiality, but does not provide strategies for how to implement these client rights during service provision (Malawi Ministry of Health, n.d). Future research into how mental health counseling interventions can ensure privacy and confidentiality for ALWH during all stages of service provision is essential for decreasing stigma and increasing the likelihood that ALWH initiate and complete treatment.
There was considerable variation in participants’ preferences for counseling session availability and frequency, as well as the delivery mode of individual counseling sessions. Availability preferences were often discussed in relation to convenience and alignment with AWLH’s school schedule or ART pick-up schedules. Some participants only wanted counseling sessions on weekends and during Teen Clubs while others wanted them available every day of the week and separate from Teen Club days. Those who wanted maximum availability and frequency reported that they weren’t sure of their schedules, when they might feel like talking to someone, and had previous experiences of counselor unavailability. The results coincide with findings from other studies amongst adolescents which found that participants might be more likely to engage in mental health treatment when counseling appointments were flexible, accommodated their schedules, and allowed them to discuss issues at their own pace (Cluver et al., 2022; Hodgkinson et al., 2014; Mokitimi et al., 2022). The large proportion of AWLH who preferred frequent counseling sessions may also reflect the high levels of a mental health distress and isolation that coincide with living with two stigmatized, chronic diseases in a low-resource setting during a period of emotional, physical, and social transition (Cluver et al., 2022). Participant interest and suggestions for varied delivery modes of counseling (i.e. in-person, telephone, 24/7 hotline, group support) reinforces the value of differentiated models of service delivery for adolescents and emphasizes the importance of providing adolescents with a range of choices to facilitate engagement in treatment and prevention options that best fit their evolving needs and lifestyles (Bhushan et al., 2023; Maskew et al., 2022; Ramraj et al., 2023; Seekles et al., 2023)
ALWH preferences for mental health counseling highlighted potential challenges of providing task-shifted counseling for this population and the limitations of eliciting feedback from a young population who have never been exposed to psychotherapy. ALWH, as well as other participants groups, emphasized that HIV and depression are inextricably linked, and their combined effect must be addressed during counseling sessions. However, many of the related stressors AWLH mentioned were socioeconomic such as poverty, food insecurity, unstable housing, unemployment, violence, and limited school fees. This highlights importance of training counselors to navigate discussion of these challenges, particularly when clients or counselors might feel that counseling is insufficient (Broström et al., 2021; Eskin et al., 2008; Hollister et al., 2022; Van't Hof et al., 2011; Wallén et al., 2021). When our interviewers asked ALWH to provide details on counseling preferences and ideal counselor qualities, the interviewers needed to significantly probe for elaboration with younger participants and with participants who had never engaged with mental health counseling. Our study team interviewers and study psychiatrist suggested that the limited concrete preferences for mental health counseling might reflect the development stage of our young participants and the lack of exposures to mental health as a concept or counseling as a method of treatment. Other studies have similarly found that open-ended qualitative questions can be difficult for young adolescents to comprehend given that their ability to reason through hypothetical or future situations and articulate answers is still developing (Bassett et al., 2008; Duncan et al., 2009; Mack et al., 2009; Poole and Peyton, 2013; Wallén et al., 2021). These results suggest that future intervention design could potentially incorporate structured orientation to counseling, use concrete and developmentally appropriate communication strategies, and provide additional guided facilitation early in sessions to support adolescents with limited prior exposure to psychosocial services.
Counseling preferences across ALWH and stakeholder groups converged on the role of counselors but diverged on expectations for counselor availability and counselor role scope. Most participants consistently emphasized the central role of counselors as trusted individuals who can provide emotional support, problem solving assistance, and linkage to services. However, ALWH and caregivers expressed a desire for frequent, flexible counseling sessions, sometimes beyond formal clinical encounters. In contrast, counselors and implementors highlighted structural constraints, including workload, staffing limitations, and the need to maintain defined professional boundaries to ensure sustainability of services. These differing preferences suggest a disconnect between relational continuity valued by ALWH and caregivers and operational feasibility emphasized by counselors and implementors. Other studies examining the provision of lay counseling or peer support for youth have suggested that structured staff supervision, establishment of working roles and personal boundaries, defined parameters of service, and investment in training and mental health support might mitigate staff concerns and preserve relational trust while aligning with implementation realities (Brooks et al., 2022b; Dorsey et al., 2019; Gusdal et al., 2011; Löfving Gupta et al., 2021; Wallén et al., 2021)
To enhance trustworthiness, we employed multiple strategies aligned with established qualitative criteria (Shenton, 2004). Credibility was strengthened through long term engagement by the investigator and study team with the research setting, methodological triangulation (IDIs, FGDs, and SSMSs across multiple stakeholder groups), systematic codebook development with team consensus, high interrater reliability (Cohen’s Kappa > 0.80), verification of coding interpretations against full transcripts, and expert review of findings. Transferability was supported by providing a detailed description of the study context, participant characteristics, sampling procedures, and recruitment activities. Dependability was ensured through structured data collection procedures using semi-structured guides, a uniform transcription protocol, documented codebook piloting and refinement processes, and systematic coding via Dedoose. Confirmability was addressed through investigator triangulation involving six team members from two countries, consensus-based resolution of discrepancies through group discussion, use of analytical matrices for systematic comparison, and transcript accuracy verification by interviewers who were present during data collection and fluent in both Chichewa and English
This study had several important limitations. First, with a small purposively selected sample, our findings cannot be generalized to a wider population. As ALWH were sampled from urban and suburban clinics in Lilongwe, we cannot determine to what extent these findings represent the experiences of ALWH across the country, particularly in rural regions. The purpose of these interviews was not to produce generalized findings but rather to describe in depth the mental health counseling preferences of ALWH in this setting. Second, Periscope participants may face mental health challenges due to multiple conditions (HIV, pregnancy, childbearing, early parenthood, etc.); therefore, their experiences may not be reflective of the general ALWH population. Third, while care was taken to ensure comfort and anonymity, we sampled participants from facilities where they receive care or have been employed. Thus, it is possible that responses could be subject to social desirability biases. Finally, the transcripts were translated from Chichewa to English. As with any translation, there was undoubtedly some level of information and understanding lost during the translation process. To minimize information loss, transcripts were reviewed by the study team members who conducted the interviews for transcription and translation accuracy, as they were fluent in Chichewa and English and presented for the interviews. Despite these limitations, this study provides valuable insights into the mental health counseling preferences of ALWH experiencing depressive symptoms in Malawi.
Conclusion
This study provides insights into preferences for mental health counseling amongst AWLH and relevant stakeholders in Lilongwe, Malawi. The results are novel in that they explore the mental health counseling preferences of a population experiencing two chronic stigmatized diseases in a low-resource setting during a unique developmental period. Findings demonstrate the desire for clinic-based delivery and individual counseling sessions to maintain privacy and avoid stigmatization. There was considerable variation in preferences for counseling session availability, frequency, and delivery mode; however, there was consistency in preferring that counselors were youth-friendly, trustworthy, and non-judgmental. Participants emphasized the importance of addressing the bidirectional relationship between HIV and depression during counseling sessions, as well as numerous socioeconomic stressors. Taken together, our findings emphasize the importance of discretion, flexibility, and choice when providing mental health services for AWLH, as well as the need to train counselors, particularly task-shifted lay counselors, to provide and extend these services in low-resource settings.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Boards of the University of North Carolina at Chapel Hill (IRB #22-0462) and the Malawi National Health Sciences Research Committee (IRB #22201). This study conformed to the principles outlined in the Declaration of Helsinki.
Consent to participate
All participants aged ⩾ 18 years provided written informed consent. All participants aged 13-17 provided written assent with their guardian’s written consent. In accordance with the NHSRC ethical standards, emancipated minors below the age of 18, who were legally married or university students, did not require guardian consent. Before study enrollment, the research staff engaged participants in a consent comprehension activity, which asked a series of questions to ensure their understanding of the study. All participants (and guardians, if present) received travel reimbursements equivalent to 10 USD.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
NLB led the conception, design, and drafting of the manuscript. JD, GMS, HSH, TP, and LR coded data. JD and JK conducted analyses and contributed to drafting the manuscript. NLB, SM, HM, BWP, MAS, GMS, and BNG were involved in data collection and management of the parent study. NLB and BNG acquired the funding and designed the parent study. All authors (NLB, JD, JK, SM, GMS, HSH, TP, LR, HM, KK, MU, BWP, MAS, BNG) have reviewed the paper, provided comments and edits, and have read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Mental Health (R34MH130232, K01MH130226).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.