
Abstract
Over half of Australians aged ⩾ 55 years do not engage in sufficient physical activity (PA). Vigorous intermittent lifestyle physical activity (VILPA; daily activities performed at vigorous intensity) presents new opportunities to facilitate PA behaviour change amongst this population. This study aimed to explore enablers and barriers to maintaining PA in adults transitioning to retirement after a VILPA intervention, crucial for informing future interventions that extend beyond the initial uptake. Semi-structured interviews were conducted with 12 participants who had completed the VILPA intervention. Inductive content analysis was performed. All participants reported continuing to participate in regular PA 6 months after the intervention. Participants reported that enablers of PA maintenance were related to knowledge gained from the VILPA intervention, associated health benefits, supportive environments, time flexibility, goal setting, and habit formation. Barriers were reported to be illnesses, perceived lack of time, environmental constraints, views of ageing, and experiences of low mood.
Background
Over half of Australians aged ⩾ 55 years do not meet the World Health Organisation’s (WHO) physical activity (PA) recommendations (accumulate 75–150 minutes of vigorous-intensity or 150–300 minutes of moderate-intensity PA per week; Australian Institute of Health and Welfare, 2023b; World Health Organisation, 2020). Known health benefits of sufficient PA (i.e. meeting WHO recommendations) include lowered blood pressure and reduced risk of cardiovascular conditions, diabetes, and certain cancers (World Health Organisation, 2020). The WHO estimates insufficient PA accounts for 4 to 5 million preventable deaths per year (World Health Organisation, 2020). In Australia, the resulting economic burden of insufficient PA was reported to be approximately $2.4 billion in 2018–2019. Over 50% of this burden is linked to healthcare costs in people aged ⩾ 55 years (Australian Institute of Health and Welfare, 2023a; Wang et al., 2021), and therefore, promoting PA in adults aged ⩾ 55 years is a public health priority.
To promote PA and facilitate behaviour change, it is crucial to intervene at the right time. In adults aged ⩾ 55 years, the period of transitioning to retirement (recently retired in the past 6 months or planning to retire in the next 5 years) could be an opportune period to intervene in PA behaviours. This period is marked by many changes in a person’s life, such as changes in income, social circles, and health status (Barnett et al., 2012), and these life changes present opportunities to introduce cues to initiate and maintain PA. A systematic review(Barnett et al., 2012) showed that previous exercise-based interventions targeting adults transitioning to retirement showed little effect in improving PA participation on a population level. Common barriers to PA participation include illnesses (Macniven et al., 2014), fear of falling, perceived lack of time, and lack of access to facilities and costs (Pang et al., 2024; You et al., 2021). There is a need for more attractive and feasible options to encourage PA participation in adults transitioning to retirement.
In the past decade, the benefits of short bouts of PA for improving time efficiency and health outcomes have led to the development of new concepts, such as vigorous intermittent lifestyle physical activity (VILPA). VILPA incorporates short bouts of vigorous-intensity daily PA, which are already occurring in a person’s daily life, for example, climbing a few flights of stairs, bursts of fast walking from place to place (Stamatakis et al., 2021). The activities are performed at a vigorous intensity, only last 1–2 minutes per bout and do not require any special equipment. An epidemiological observational study showed that adults who do not participate in regular exercise or sports, and unintentionally engaged in VILPA three times a day had a reduction of nearly 50% in all-cause mortality (Stamatakis et al., 2022). A novel 12-week VILPA intervention was developed (Pang et al., 2025a, 2025b) using the existing evidence in VILPA (Ahmadi et al., 2023; Stamatakis et al., 2021, 2022) and in conjunction with health professionals and adults transitioning to retirement (Pang et al., 2025a). The intervention is theory-based and evidence-informed; and the full details of the intervention are published elsewhere (Pang et al., 2025c). In brief, the intervention targets insufficiently physically active adults transitioning to retirement, provides education on PA recommendations and health benefits of vigorous PA in older age, identifies individualised opportunities for VILPA in daily routines, goal setting and weekly checklists, regular reminders and self-monitoring with fitness trackers, rewards and social support, and ongoing facilitator support (Pang et al., 2025c). Preliminary findings of the intervention’s pilot testing in insufficiently physically active participants indicated that the intervention was feasible and could increase daily vigorous-intensity PA from baseline. However, whether this behaviour can be maintained following the cessation of the VILPA intervention has yet to be studied.
Changing PA behaviours is complex, and supports are needed for both initiation and maintenance of the behaviour (Dunton et al., 2022; Rhodes and Sui, 2021). Initiation refers to the period in which PA commences or increases, moving towards behaviour change over time (van Stralen et al., 2009). Maintenance of a behaviour is less consistently defined. Research suggests the boundaries between initiation and maintenance are ambiguous. Currently, there is no standardised definition or measurement of PA maintenance (Rhodes and Sui, 2021). However, it is generally considered the stage in which regular and sufficient PA is established in the long term (Kahlert, 2015). Despite the inconsistent definition for PA maintenance, a three-to-six-month follow-up period has been most adopted across the research (Amireault et al., 2013; Rhodes and Sui, 2021). Previous maintenance studies report a significant reduction in initiated PA patterns within the first 6 months of post-exercise-based intervention (Amireault et al., 2013; Rhodes and Sui, 2021). Due to the unique features of VILPA, such as short bouts of vigorous-intensity activity embedded in daily life and in the developed intervention, maintenance of PA following the intervention may offer different insights into PA maintenance than traditional exercise programmes. Knowing the enablers and barriers to PA maintenance after participating in a VILPA intervention would benefit developing strategies to sustain long-term PA behaviour change.
Therefore, this study aimed to explore the enablers and barriers to PA maintenance after a VILPA intervention among adults transitioning to retirement.
Methods
Research design
We used an explanatory sequential mixed-method design, using 1- and 3-month post-intervention follow-up quantitative questionnaire data to inform qualitative data collection. This design was chosen to expand the findings from post-intervention follow-up surveys, providing deeper insight into the maintenance of physical activity using semi-structured interviews (Creswell and Creswell, 2018; Fetters et al., 2013).
Ethical considerations
This study was approved by Curtin University Ethics Human Research Committee. Informed consent was gained from all participants.
Participants and recruitment
Participants (n = 17) who completed the initial VILPA intervention pilot trial were invited to participate in the 1- and 3-month follow-up surveys, and 6-month follow-up telephone interviews. Sixteen participants completed the 1- and 3-month follow up surveys and 12 individuals accepted the interview invitation. Five participants declined to participate in the 6-month follow-up telephone interviews due to time limitations and life commitments.
Procedures
One- and three-month surveys
Participants who completed the VILPA intervention completed self-reported online follow-up surveys 1 and 3 months post-intervention. The surveys (see Supplemental Material 1) included the adapted Self-Reported Habit Index questionnaire (Verplanken and Orbell, 2003), the 16-item Situational Motivation Scale (Guay et al., 2000), and the Measurement of Intention (Davis and Warshaw, 1992), and open-ended questions aimed to explore the participant’s PA habituation levels, motivations and intentions to engage in PA.
Interview question development
Findings from the 1- and 3-month follow-up surveys were used to inform and develop six semi-structured interview questions. Interview questions (see Supplemental Material 2) were structured on the broad themes of enablers and barriers, with prompts to further explore sub-themes including PA benefits, use of external tools and strategies to continue PA. The interview questions were piloted among the research group who were involved in the development, implementation and testing of the original VILPA intervention.
Telephone interviews
Participants were randomly assigned to one of three independent researchers for telephone interviews. Each interviewer conducted two pilot interviews to familiarise themselves with the interview script and to ensure consistency across interviews. Interviews were conducted using a dedicated research phone, with an approximate duration of 30 minutes. Interviews were recorded and transcribed live, via Microsoft Teams. Interviewers took field notes and made efforts to member-checking by summarising responses and checking to understand with participants (Fetters et al., 2013). Immediately following each interview, the transcription was de-identified, reviewed and cleaned to ensure the accuracy of transcription content and to maintain confidentiality.
Data analysis
One- and three-month follow-up surveys
Quantitative analysis was conducted by one researcher, independently, and peer reviewed by another researcher. The quantitative data were tabulated using Microsoft Excel to generate descriptive statistics, outlining the frequency, intensity and types of PA performed. Qualitative data analysis was conducted by three independent researchers using inductive content analysis to identify categories of enablers and barriers to PA maintenance.
Semi-structured interviews
Inductive content analysis was selected to allow the identification of emerging patterns and themes, without preconceived categories (Vears and Gillam, 2022). The transcripts were coded independently by the interviewing researcher and another researcher, assigned at random. Researchers familiarised themselves with the data by reading and re-reading the transcripts and coded the data into categories for enablers and barriers, using NVivo version 14. The transcripts were recoded independently to identify sub-categories. Following this coding process, the researchers met over the following weeks until a consensus regarding the codes was reached. This process of researcher triangulation was utilised to ensure the trustworthiness of the findings (Carter et al., 2014). The identified enablers and barriers were then matched to the appropriate categories of the COM-B model (Capability, Opportunity and Motivation).
Theoretical frameworks
The COM-B categorises human behaviour change into three components; capability, opportunity and motivation, which help understand influencing factors (Michie et al., 2011). Capability refers to physical and psychological capacity, opportunity refers to the influence of external social or environmental factors, and motivation encompasses internal and external drivers (Michie et al., 2011). The Theoretical Domains Framework (TDF) outlines 14 domains, which are expansions of the COM-B categories, providing further context to the factors influencing behaviour change (Atkins et al., 2017). Integrating the COM-B model provided a systematic approach to analyse and organise qualitative data, gaining insight into possible underlying reasons for behaviour (De Leo et al., 2021). The COM-B and TDF have been utilised in a wide variety of contexts to explore enablers and barriers to behaviour change (Flannery et al., 2018; Johnson et al., 2024; Timkova et al., 2024). Linking research findings to these well-documented frameworks enhances the rigour of this study (Johnson et al., 2020).
Findings
Participants
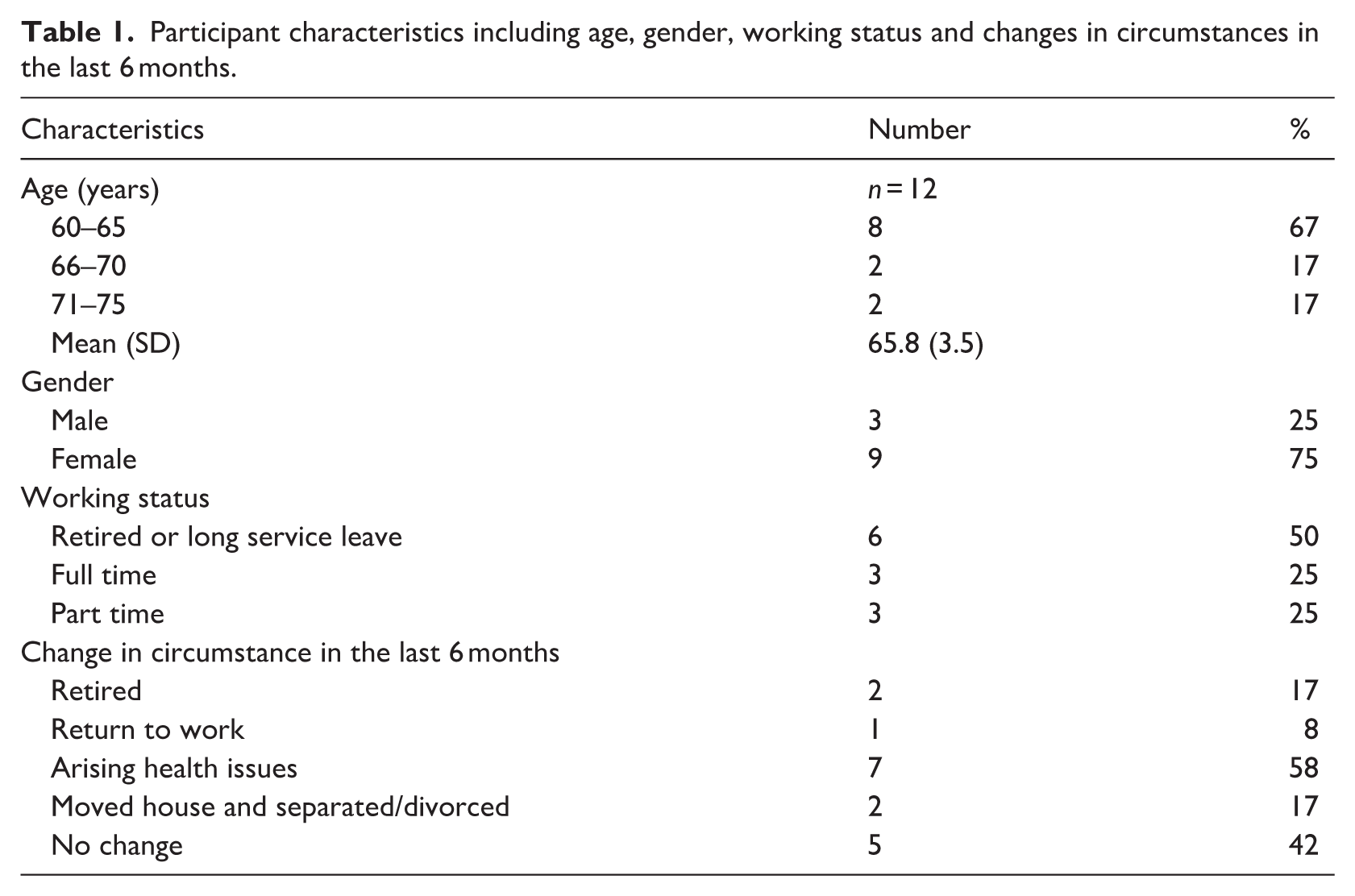
Participants ranged from aged 61 to 73 years (M = 65.8, SD = 3.5), with 75% (N = 9) females. Half of the participants were retired or on long-term leave. The remaining participants worked full- or part-time but were planning to retire within 5 years. Seven participants reported significant changes in life circumstances in the 6 months following the completion of the intervention. See Table 1 for details.
Participant characteristics including age, gender, working status and changes in circumstances in the last 6 months.
One- and three-month follow-up survey findings
At 1- and 3-months post-intervention, 16 participants completed the surveys. All participants self-reported continuing to engage in VILPA and maintaining participation in PA (See Supplemental Material 3). Commonly reported activities included walking, housework, yard work, climbing stairs, carrying shopping bags over 50 m, and moving heavy objects. Enablers of PA maintenance included education and knowledge, supportive environments (social and physical), associated health benefits of regular PA, use of fitness trackers, goal setting, effective time management, positive social interaction, and habituation of activities. Barriers to PA included health concerns, social and family commitments, perceived lack of time, poor weather, and lack of motivation. No participants reported using the original intervention checklist tool; however, they stated it was helpful as a reminder and to increase awareness of PA opportunities. The use of a fitness tracker increased from 50% (n = 8) at 1 month to 67% (n = 10) at 3 months follow-up. Useful features reported were the step counter, distance travelled, heart rate zones, and sleep and PA duration.
Semi-structured telephone interview findings
Physical activity types, frequency and intensity
All 12 participants reported engaging in regular PA 6 months post-intervention. Reported activities included VILPA, such as housework, yard work, walking, playing with grandchildren, climbing stairs and increasing parking distances from shops/work. Additionally, structured exercises such as yoga, cycling, swimming, dancing, and group classes were reported by the participants. Most participants reported they were engaging in some aspect of PA daily, with the intensity ranging from moderate to vigorous intensity.
Enablers
Ten enablers of PA were identified and mapped to the COM-B and TDF, outlined in Table 2. These included the associated health benefits, knowledge and awareness, environmental factors (natural and built), positive social influences, flexibility in time use, reinforcement from external tools, goal setting and achievement, an optimistic attitude to change, experiences of emotion, and habit formation.
Enablers to PA maintenance with codes and illustrative quotes, matched to the COM-B and TDF.
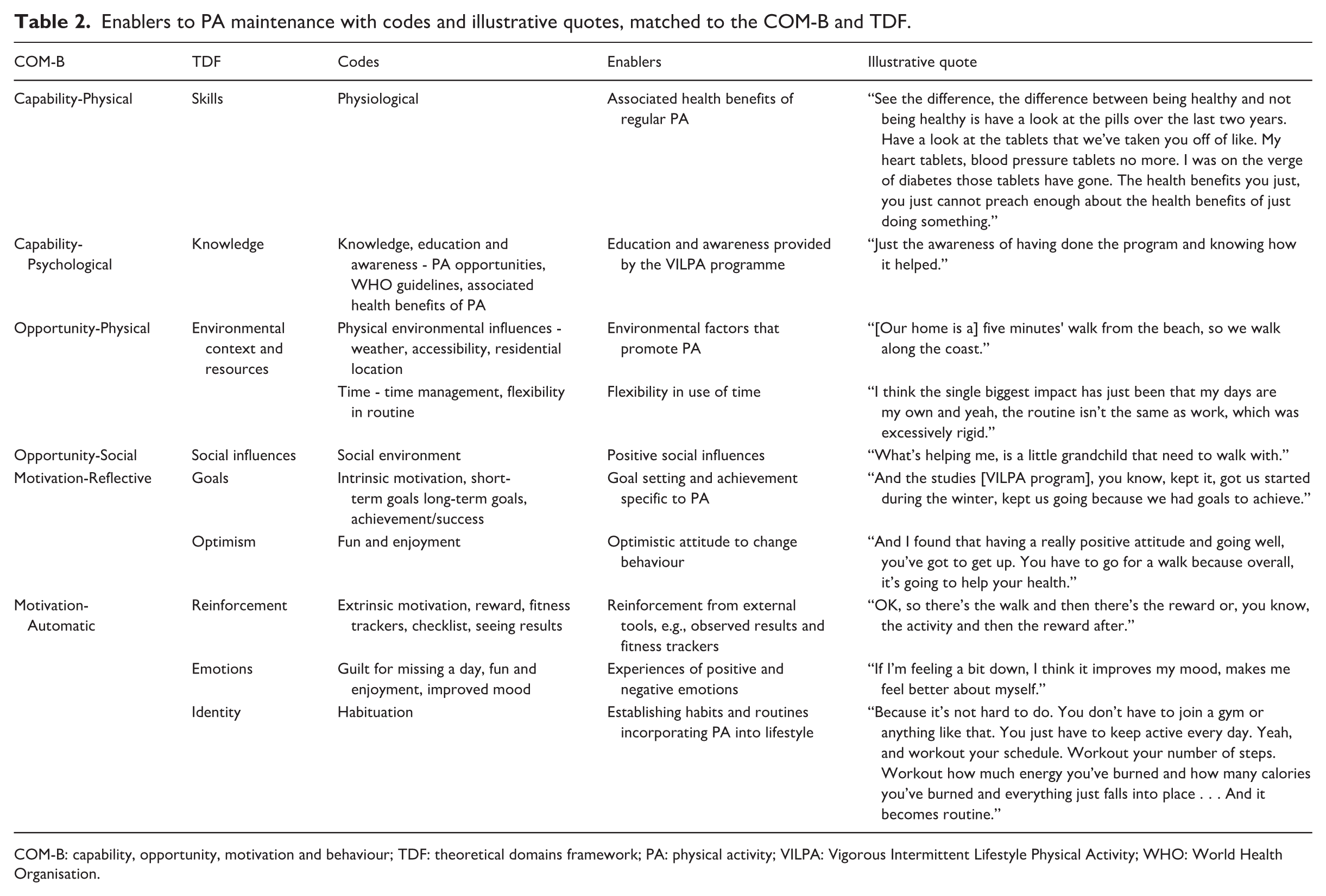
COM-B: capability, opportunity, motivation and behaviour; TDF: theoretical domains framework; PA: physical activity; VILPA: Vigorous Intermittent Lifestyle Physical Activity; WHO: World Health Organisation.
COM-B: Capability
Knowledge and awareness were identified as resounding enablers, which were linked to participation in the VILPA intervention itself. Participants reported that having completed the VILPA programme, in conjunction with gaining an increased understanding of the WHO guidelines and associated health benefits, provided greater insight into PA recommendations. Specific to knowledge gained during the VILPA intervention, participants developed an awareness of PA opportunities in daily tasks, which provided simple and accessible ways to engage in and maintain higher-intensity PA. “I’m probably more aware of things I can do where I used to cheat . . . walking from my office to the car park. . . for me is about half a kilometre. I used to amble my way through that now I walk briskly.”
The associated health benefits of regular PA, such as improved fitness, better sleep, and weight loss, were recognised to increase or maintain participants’ physical capacity, enabling continued participation in PA. “. . . It surprised me (when I started to move quicker), and then I would try to do something and think, holy smoke! That never used to happen before. And so yes, I wanna stay active. I wanna stay young if that’s the right word for me.”
COM-B: Opportunity
The physical environment was recognised to support individuals’ participation in PA, providing accessibility, convenience and safety. One participant reported, “Cos we’ve got bush over the road. A bush reserve, so I can walk in there, and I know I’m not alone.” Other participants identified that living near shops enabled them to incorporate PA into daily errands and leisure activities; “Ok, let’s walk to the shop and grab the loaf of bread . . . how about we have a coffee on the way back if we go via such and such. . ..”
Positive social influences were reported as another enabling factor, providing encouragement, increased enjoyment and a chance to try new things. One participant shared, “I’ve got one of the ladies at craft. She has encouraged me to go to do the yoga and we did the aqua aerobics together.” Pre-existing roles and responsibilities incorporated PA into associated tasks, enabling participants to achieve PA with less effort. Such roles included being a grandparent and dog owner, with one participant explaining, “And then two little (dog) heads pop up and go. . . We have to go for a walk. . . And then once you’re up and at it, then you’ve got to find other things to do anyway.”
The retirement period itself is a unique window to promote PA, due to increased flexibility in life routine and availability of time. One participant who retired within the last 6 months explained, “Well, now I have the time to do it.” Other participants who were yet to retire, prioritised time for PA and adjusted routines accordingly, “It’s allocating time. Yep, hmm that would be a big one. Yeah, that’s probably the biggest one of the biggest (enabling) factors.”
COM-B: Motivation
As part of the VILPA intervention, participants learned to set goals specific to PA achievements. Participants who had specific goals were recognised to be far more motivated to regularly complete PA, with the achievement of goals seen to have a further motivating effect. “And I had improved a fair bit (during the intervention) and my goal was to improve and do better. Yeah, and having that as an incentive, to see (the goals I set), made a huge difference.”
The use of fitness trackers was identified to be highly motivating, providing both a reminder to complete daily PA and reinforcement when PA was achieved. One participant shared, “I’d say the Fitbit out of everything. . . is the (top) thing that keeps me accountable”, with another participant reporting, “Yep, and I quite like it (fitness tracker) when the stars go off because I’ve gotten 10,000 steps.” When used long-term, fitness trackers were recognised to assist in creating automatic PA behaviour patterns, leading to habituation.
Experiences of both positive and negative emotions were recognised to increase participants’ motivation towards PA. Participants reported that the experience of negative emotions, such as guilt, was pre-emptive to their engagement in PA. “It’s a lifelong thing that, yeah, when you remember and you feel guilty if you don’t (do PA).” Comparatively, participants shared that regular PA contributed to overall improved mood and well-being, “. . .you actually feel better when you do exercise. Endorphins and all that stuff.”
Overall, participants reported positive attitudes towards PA behaviour change. This optimistic attitude appeared to boost participants’ motivation and resilience, enabling continued participation in PA. One participant with a cancer diagnosis shared their perspective, “the point is you have to be active and get over it. You have to keep moving forward. You cannot ponder having cancer. You can’t sit there and go. Woe (sad) is me.”
Barriers
Barriers to PA were reported as health issues (e.g. chronic and acute injury and illness), perceived lack of time, physical environmental influences (e.g. limited accessibility and poor weather), norms of ageing, lack of social connexion, and experiences of negative emotion and low mood. These have been mapped to the COM-B and TDF framework, outlined in Table 3.
Barriers to PA Maintenance with Codes and Illustrative Quotes, Matched to the COM-B and TDF.
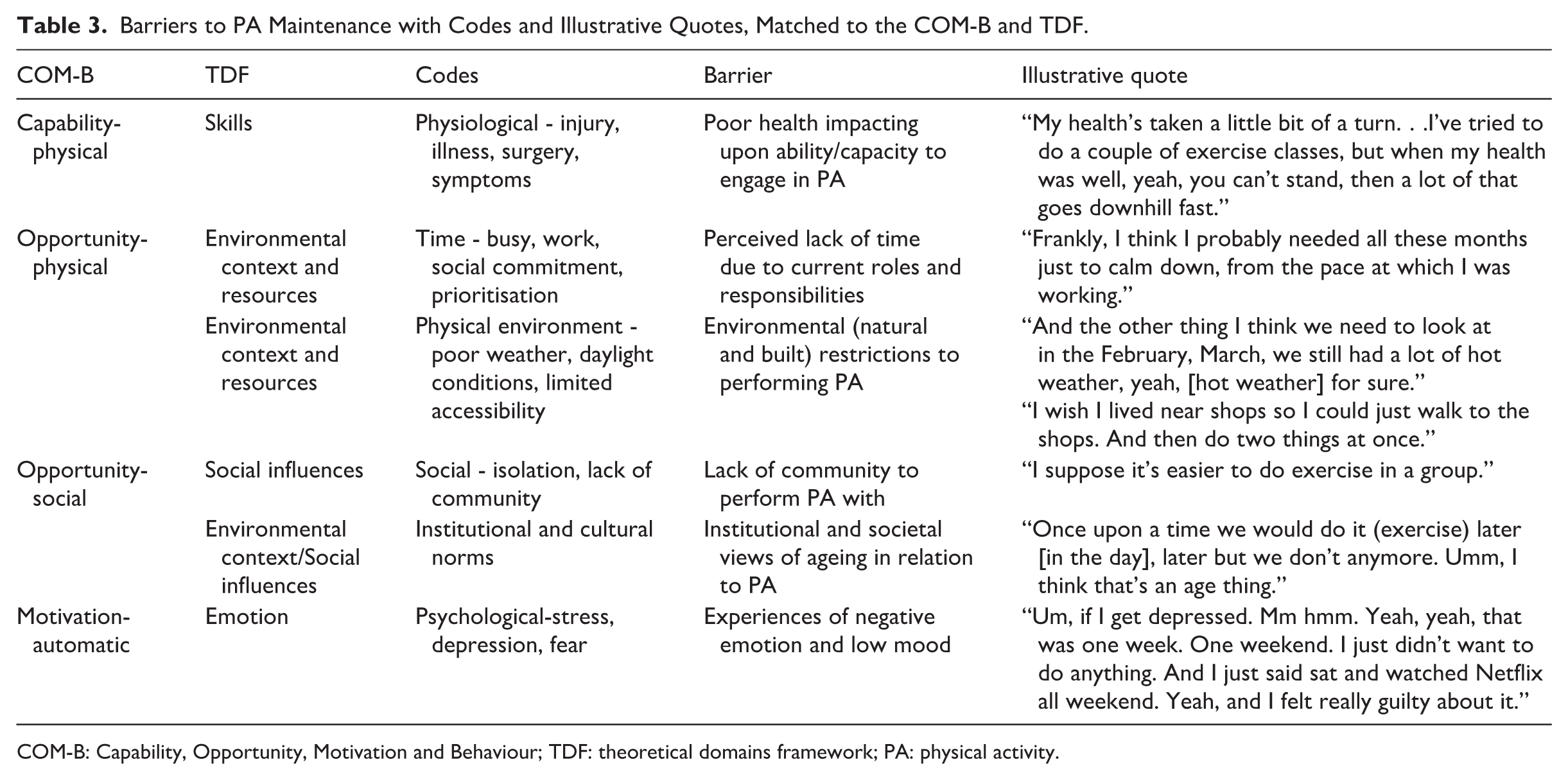
COM-B: Capability, Opportunity, Motivation and Behaviour; TDF: theoretical domains framework; PA: physical activity.
COM-B: Capability
Health issues, including acute and chronic illness and injury, impacted participants’ physical ability to complete PA. One participant stated COVID-19 inhibited participation in PA for a short duration, “I got really sick . . . for about two weeks, I didn’t do anything.” Conversely, a leukaemia diagnosis challenged one participant’s capability to engage in PA long-term, with daily symptom variability, “some days I can’t get out of bed.” Eight participants reported experiences of health illnesses, however, they continued PA despite these challenges.
COM-B: Opportunity
Time was identified as an overarching theme, including perceived lack of time, prioritisation and difficulty scheduling PA into their routine, which impacted upon participants’ ability to maintain PA consistency. Some participants reported limited opportunities to participate in PA due to conflicting commitments, such as work, family and social obligations. Despite a perceived increase in available time associated with retirement, some participants reported that the change in routine posed a barrier to PA. “Well, the first initial months (after retirement) are frantic. You think you’ve got heaps of time to do everything, and you don’t, and then just like when you work, you schedule things in. So that’s what I find myself doing now.”
The physical environment was identified as a barrier to the participants’ ability to engage in PA safely and access appropriate spaces to perform PA. Safety concerns resulted in avoidance of certain types of PA at particular times, “I get home very late . . . It’s too late to walk around the suburb . . . Like you know, you can’t quite run as fast as somebody … (the area) looks dangerous.” Residential location impacted upon accessibility and ease of PA; “I wish I lived near shops so I could just walk to the shops. And then do two things at once.” Inclement weather and seasonal daylight conditions impacted participants’ ability to complete usual outdoor activities, with one participant outlining, “Winter is always an issue, so that’s why I’m extra careful in winter.”
COM-B: Motivation
Motivation is linked strongly to emotion, mood and attitude, which directly impacted participants’ PA engagement levels. Episodes of stress, fear and depression contributed to the avoidance of PA, with one participant outlining “If I get depressed . . . I just didn’t want to do anything.” Conversely, another participant described experiencing a lack of motivation by saying, “Just laziness is the first problem I would say . . . I think it’s easier to just sit down or lie on the bed and have a snooze.”
Another barrier to participants’ motivation to engage in PA was identified as cultural and institutional norms. Stereotypes associated with older age impacted participants’ beliefs about their abilities, which reduced motivation to participate in PA. One participant stated, “When you’re going to join something on your own it’s a bit more challenging, and I think the older you get… There’s a little more fear, not fearful, but hesitant.”
Discussion
Our study provides a unique contribution to the PA literature by examining the perspectives of adults who successfully completed a novel VILPA intervention during the transition to retirement. While much of the existing research has focussed on barriers and enablers to PA initiation or within programme adherence, our findings shed light on the often-overlooked challenges of maintaining activity after structured intervention support ends. Participation in PA was found to be consistent at 1-, 3- and 6-month follow-ups, as self-reported by participants. Previous PA maintenance studies report a significant reduction in PA within 6 months of intervention completion (Amireault et al., 2013; Rhodes and Sui, 2021). This positions our study uniquely within PA maintenance research, as all participants reported maintaining regular PA 6 months after the VILPA intervention. Key enablers of PA maintenance included perceived health benefits, knowledge and awareness of PA guidelines and opportunities, supportive environments, flexible time management, positive social influences, goal setting and achievement, an optimistic attitude, feedback from fitness trackers, emotional experiences (both positive and negative), and habit formation. Barriers to PA maintenance included illnesses, perceived lack of time, environmental restraints, institutional views of ageing, lack of social connexion, and experiences of negative emotion and low mood. These barriers are consistent with previous PA maintenance research (Collins-Bennett et al., 2025).
We identified two enablers that are unique to this study, positioning the VILPA intervention as a promising strategy to facilitate and maintain PA behaviour change amongst the ageing population. Knowledge of PA guidelines and awareness of opportunities to incorporate PA into daily routines emerged as prominent enablers in our study. This differs to previous research that knowledge itself was not identified as an enabler in PA maintenance (Amireault et al., 2013; van Stralen et al., 2010). Such difference could be due to participants increasing their knowledge of PA guidelines and awareness of PA opportunities during the intervention, identified and engaged in individualised PA opportunities, and simultaneously developed their capability to identify relevant PA opportunities for themselves. The self-identified and relevant PA opportunities could be more achievable to the participants, hence, enabling their longer-term PA maintenance.
Similarly, knowledge of the associated health benefits of PA was reported as an enabler in our study, which has not been consistently reported as an enabler in the literature (Collado-Mateo et al., 2021). In our study, participants reported health benefits, such as improved fitness and weight loss, as enabling factors to PA maintenance after the VILPA intervention. This may be associated with the participants being older in age, at a stage of life to prioritise health, and a result of participants achieving improved physical functioning and health at the end of the intervention and motivated to maintain their improved health benefits long term. Participants experiencing illness also reported engaging in even very short durations of PA (e.g. a few minutes) made them feel better mentally and physically, and hence, were more willing to maintain their PA participation.
Chronic health conditions, acute illnesses or injury, were notable barriers to PA maintenance, which is widely reflected across the research (Collins-Bennett et al., 2025; Maula et al., 2019). Given that chronic illness increases with age, this result was expected amongst the research population (Wang et al., 2021). However, a key difference from our study was that participants reported continuing PA despite experiences of injury and illness. This could be largely attributed to the flexibility of VILPA and its incorporation into daily routines, paired with the enabling factor of increased awareness and capacity to identify opportunities for PA. As such, participants were able to problem-solve and adapt tasks or environments to continue PA in alternative ways.
Participants reported additional factors influencing PA maintenance, which complemented those identified in previous PA maintenance studies (Collins-Bennett et al., 2025; Kononova et al., 2019; Maula et al., 2019; Meredith et al., 2023; Seifert et al., 2017). Contextual and personal factors, such as environment, time and the experience of emotion, were reported as both enablers and barriers. Given these factors were highly individual and based on circumstance, the variation of responses between participants was expected. Other enablers reflected in previous research included goal setting and achievement, optimism, reinforcement from external tools, and habituation (Maula et al., 2019; Meredith et al., 2023). The use of fitness trackers was reported as a motivating factor in ongoing participation in PA, similar to previous research highlighted wearables fostering accountability and promoted routine and long-term adherence (Kononova et al., 2019; Seifert et al., 2017). These enabling factors pertain to the COM-B category of motivation, which is widely recognised as the underpinning factor of behaviour change (Amireault et al., 2013; Michie et al., 2011). An additional barrier was identified as norms of ageing, reflected in previous studies to influence older adults’ perceptions of identity and ability to perform PA (Meredith et al., 2023).
Implications
Future interventions should not only aim to address the barriers identified in this study but also actively support participants in leveraging the enablers identified across the COM-B domains. Given the novel nature of the VILPA approach, interventions may benefit from incorporating strategies that help individuals recognise, personalise, and build upon these enablers in real-world settings. Education should aim to deepen participants’ understanding of PA guidelines, associated health benefits and ways to integrate PA into daily routines. However, knowledge alone is insufficient to drive sustained PA behaviour change. Interventions should prioritise capacity building – empowering people to find or create their own PA opportunities. To support this, prolonged engagement with the intervention and the provision of ongoing support are recommended. Establishing a strong community among participants is likely to encourage continued PA participation, which could be accomplished through regular in-person meetings and online messaging groups. Other recommendations include providing fitness trackers and checklist tools during intervention, to allow people to develop a sound understanding and awareness of PA requirements and how to achieve the recommendations. A combination of strategies that target each category in the COM-B model is likely to produce optimal intervention outcomes, given that behaviour change is reliant on the presence and interaction of all three categories (Michie et al., 2011).
Future interventions should aim to address the identified barriers, assisting participants to harness enablers to overcome these. As most of the identified barriers were contextual, relating to personal or environmental factors, future interventions should prioritise strategies that adapt tasks or environments to support continued PA engagement. For example, to address environmental restraints such as poor weather, activities could be performed indoors, as demonstrated by one participant who performed YouTube line dances at home during hot weather. An additional strategy to address the barrier of health illnesses is to encourage people to consult health professionals regarding performing PA alongside their health condition. Importantly, future interventions should also consider how to sustain motivation and confidence once formal support ends, particularly during life transitions such as retirement, when routines may be influx. By integrating these elements, future programmes can better promote lasting engagement with PA beyond the intervention period.
Strengths & limitations
This study contributes new and valuable insights into enablers of PA maintenance, providing potential new strategies to facilitate PA behaviour change amongst the wider retiring population. The dual use of the COM-B and TDF is another strength, providing a thorough and systematic approach to examining the influencing factors of PA maintenance. These are both well-documented models within healthcare, contributing to the rigour of this study (Flannery et al., 2018; Johnson et al., 2020; Timkova et al., 2024).
Several limitations should be acknowledged when considering the implications of this study. As PA was self-reported by participants, the accuracy (i.e. meeting the WHO PA guidelines) of the duration or levels of PA could not be determined post-VILPA intervention. As such, future research in this area should incorporate objective, device-derived measurement of PA to determine this. However, given the participants’ awareness of PA duration and intensity requirements from the VILPA intervention, it can be argued that the self-reported PA participation after the intervention may have been similar to the amount during the intervention. Another limitation to consider is the relatively small sample size, which could impact the transferability of findings. We also recognise that initial quantitative surveys were limited by the sample size and may not provide robust evidence in maintenance of PA 1- and 3-month post-intervention. However, given that recruitment was limited to participants who completed the novel VILPA intervention, findings represent a high majority (70%) of the original participants’ experiences and perspectives.
Conclusion
The VILPA intervention is characterised by short, vigorous activity bouts embedded in daily life and thus presents distinct opportunities and challenges for long-term maintenance, differing from traditional structured exercise programmes. Our findings offer valuable insights to inform the design of sustainable, scalable interventions that extend beyond initiation and are responsive to the realities of everyday life in the context of a life stage marked by changing routines, identities, and social roles. For optimal outcomes, future interventions should utilise the enablers, with a particular focus on building people’s awareness of PA opportunities in everyday tasks and increasing their capacity to seek opportunities independently. Strategies to address barriers should focus on education on the safety of PA in different weather environments and when experiencing episodes of health illness, and tasks to suit the individual’s needs to enable the continuation of PA.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261434374 – Supplemental material for Enablers and barriers to maintaining physical activity after a vigorous intermittent lifestyle physical activity intervention in adults transitioning to retirement
Supplemental material, sj-docx-1-hpq-10.1177_13591053261434374 for Enablers and barriers to maintaining physical activity after a vigorous intermittent lifestyle physical activity intervention in adults transitioning to retirement by Casey Gray, Kendrick Lim, Josephine Palladino, Belinda Rowland, Phoebe Wan, Joanne McVeigh and Bingyan Pang in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to thank all participants who took the time to engage in this research.
Ethical considerations
This study was approved by Curtin University Ethics Human Research Committee. Human Research Ethics Office of Curtin University, with approval number HRE2022-0304. All participants gave informed consent for their involvement in the study. The original pilot trial was registered with the Australian New Zealand Clinical Trials Registry, trial ID ACTRN12623000493640.
Consent to participate
All participants gave written informed consent for their involvement in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Conceptualisation: BP, JMcV. Data curation: CG, KL, BR, JMP. Formal analysis: CG, KL, BR, JMP, BP. Investigation: all. Methodology: BP, PW, JMcV. Project administration: BP, PW, JMcV. Resources: BP, JMcV. Software: BP, JMcV. Supervision: BP, PW, JMcV. Validation: all. Visualisation: all. Writing original draft: CG, KL, BR, JMP, BP. Writing review and editing: all.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded and supported by Curtin University, School of Allied Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article. Data may be available upon request to the research team.
Supplemental material
Supplemental material for this article is available online.