
Abstract
Difficulties regulating emotions and physiological arousal can heighten stress and anxiety in young adults, lowering quality of life (QoL). This pre-registered study examined whether maladaptive emotion regulation (e.g. expressive suppression) relates to greater emotional and arousal dysregulation (e.g. reduced heart rate variability, HRV) and poorer QoL. 101 young adults (21.1 ± 1.9 years; 73.3% female) in Malaysia completed questionnaires on emotion regulation, stress, anxiety, and QoL, while heart rate was recorded at rest and during exposure to emotion-inducing stimuli. Bootstrapped correlation and mediation analyses revealed that greater emotional dysregulation was associated with lower use of cognitive reappraisal, higher stress/anxiety, and poorer QoL. Cognitive reappraisal related to lower stress/anxiety and better QoL, whereas expressive suppression related to higher anxiety and poorer psychological QoL. Among frequent reappraisers, reduced stress and anxiety predicted better QoL. Promoting cognitive reappraisal may improve wellbeing and help young people cope with emotional challenges.
Introduction
Experiencing stress during early life increases the predisposition to anxiety disorders later in life (Lähdepuro et al., 2019). Anxiety disorders affect about 10% of the global population (Baxter et al., 2013), with recent increases in prevalence observed due to the COVID-19 pandemic (Santomauro et al., 2021) and other socio-economic factors. They are particularly detrimental to health because they often co-occur with unhealthy lifestyle behaviours and other risk factors for chronic disease, thereby amplifying both psychological and physical health burdens and reducing quality of life (QoL) (Cheah et al., 2020; Nechita et al., 2018).
Difficulties with emotion regulation (i.e. being aware of and capable of modulating the frequency, intensity, and duration of emotional responses) could explain why experiencing chronic stress leads to the development of an anxiety disorder (Aldao et al., 2010). Regulation of emotions (especially negative emotions, such as sadness or anger) can be achieved via adaptive strategies, such as cognitive reappraisal (changing the cognitive connotation of a situation and its emotional valence), acceptance, and problem solving (attempting to change the nature of a negative situation by eliminating the source of stress), or via maladaptive strategies, such as avoidance (ignoring the source of stress) and expressive suppression (suppressing facial expressions and emotional behaviours) (Cutuli, 2014).
People who are more likely to use adaptive emotion regulation strategies (e.g. cognitive reappraisal) experience better interpersonal functioning, greater wellbeing, and positive affect. Conversely, the use of maladaptive strategies (e.g. expressive suppression) leads to increased depression and anxiety, negative mood, lower social functioning and reduced psychological well-being (Boemo et al., 2022). It is also important to note that the context in which emotion regulation strategies are implemented, is likely to affect emotion regulation (Aldao et al., 2015). For example, a strategy that is adaptive for some individuals in some contexts can be maladaptive in other contexts. Moreover, the same strategy can work for some people, but not others, highlighting the importance of flexibly alternating between different strategies based on situational and individual demands (Bonanno and Burton, 2013).
Experiencing anxiety and emotional dysregulation is associated with heightened physiological arousal, whose mechanisms are governed by interactions between central and peripheral nervous systems (Jones, 2003); therefore, arousal regulation depends on both external sensory stimulation and environmental stressors, and voluntary control. The ability to efficiently regulate arousal according to the situation starts developing in early infancy and is not fully mature at least until young adulthood, parallelling the development of brain systems involved in self-regulation and learning, including the pre-frontal cortex (PFC) (Mulkey and du Plessis, 2019).
Amongst the neural systems involved in arousal regulation, the Autonomic Nervous System (ANS) is responsible for involuntary regulation of heart rate and pupil size, but also gastro-intestinal and sexual functions; (Karemaker, 2017). The Sympathetic Nervous System (SNS) is predominantly active in situations requiring quick and effective mobilisation of energetic resources (“fight or flight”), while the Parasympathetic Nervous System (PNS) is mainly responsible for maintaining and preserving energetic resources during “rest and digest” situations. While activity in the PNS results in slower and more variable heart rate and pupil constrictions, activation of the SNS results in increases in heart rate and blood pressure, and pupil dilations.
The physiological patterns associated with anxiety are predominantly related to the over-activation of the SNS – leading to increased heart rate, faster respiration rate and increased sweating – and reduced activation of the PNS, leading to sympathetic hyper-activation. This is supported by evidence that people with anxiety disorders show reduced heart rate variability (HRV; a measure of fluctuations in heart rate over time), compared to people without (Alvares et al., 2016). HRV is often interpreted as an index of the ability to self-regulate and reduce heart rate in response to stress (Beauchaine and Thayer, 2015; Quadt et al., 2022). Furthermore, recent evidence synthesis studies have shown a transdiagnostic association between lower HRV (especially at rest), difficulties in emotion regulation, and self-injurious thoughts and behaviours, in children and young people (Bellato et al., 2023a, 2023b, 2024). These recent findings, in addition to previous extensive literature (e.g. Beauchaine, 2015; Beauchaine and Thayer, 2015) suggest that HRV could be a general marker of psychopathology. What has not been previously investigated in young people – however – is the association between implementing specific emotion regulation strategies in everyday life, stress and anxiety levels, QoL, and arousal regulation patterns (HRV). Moreover, most research studies on emotion regulation have mainly included White participants from Western countries; our study was the first to involve young people from Malaysia.
In this pre-registered study, we investigated whether young adults who predominantly use cognitive reappraisal versus expressive suppression exhibit distinct profiles in arousal regulation, anxiety and stress, psychological wellbeing, and quality of life (QoL). We recruited a convenience sample of young adults (aged 18–25) from the general population in Malaysia and tested the general hypothesis that young adults who predominantly engage in expressive suppression are more likely to experience anxiety, show reduced HRV, and have poorer QoL compared to those who are more likely to use cognitive reappraisal.
Materials and methods
This is a pre-registered study, whose protocol was submitted after receiving ethical approval and before starting participant recruitment. All participants signed an informed consent form before participating to the study and – in the consent form – provided consent for their anonymised data to be published in open-access repositories.
Participants
The study was advertised via social media and flyers posted in public university spaces, and participants were recruited via snowball sampling. Potentially eligible participants were: (a) aged 18–25 years; (b) non-smoker; and (c) without a diagnosis for any health condition known to cause alterations in cardiovascular functioning. We included both students and non-students, and participants with a mental health diagnosis. We aimed to recruit at least 100 participants for the present study. This was based on an estimated minimum sample size of 92 participants needed to detect a medium effect in a multiple regression analysis with 5 predictors (meditation analysis), with a significance level of 0.05 and an estimated power of 0.80, allowing for 10% attrition).
Procedure
This study received ethical approval from the Science and Engineering Research Ethics Committee at the University of Nottingham Malaysia; recruitment and data collection were conducted between February 2023 and July 2023. Participants were invited to attend a testing session at the Mind & Brain Development Lab, University of Nottingham Malaysia. The session was conducted in a quiet room with controlled illumination and lasted about 1 hour. A gift voucher (20 Malaysian Ringgit, equivalent to 5 USD) was given to each participant. Participants were instructed not to consume any caffeine, food, or drinks (except water), nor engage in physically demanding activities at least 3 hours before testing. Upon arrival, participants were briefed on the study procedures and, after providing written consent, they completed a battery of questionnaires (see paragraph “Materials” and Supplemental Material 1).
After completing the questionnaires, two 1.5 mm ring electrodes were placed on each wrist of the participant, and one on the earlobe as a reference, to record heart rate continuously during the testing session. A Brain Vision actiCHamp Plus electro-physiological recording system and a Brain Products BIP2AUX adapter were used. Participants were initially asked to relax while sitting in a comfortable chair for 6 minutes; with their eyes closed for the first 3 minutes and their eyes open for the last three. They were then shown a series of emotion-inducing pictures. To avoid participants disengaging and losing interest in the stimuli, we presented this as a “picture categorization task.” Coloured picture stimuli were taken from the Open Affective Standardized Image Set (OASIS; Kurdi et al., 2017), a validated database of 900 images aimed at inducing different emotional responses. Participants were asked to watch each picture for 5 seconds without looking away, followed by a 3-second break and the question “Would you have characterised the picture you have just seen as (a) Positive, (b) Negative, (c) Neutral?”. If participants chose either “positive” or “negative,” they were asked: “How positive or negative was the picture?”, on a scale from 1 to 5.
For each participant, we used the same 144 pictures, separated into 4 blocks and presented in a random sequence. Each block had 36 pictures from each category (people, animals, objects, and landscapes), counterbalanced based on valence (positive, negative, neutral). The testing session lasted approximately 30 minutes, while completion of the questionnaires took 20 minutes. The participants’ comfort was continuously monitored by the researcher.
Materials
A demographic questionnaire in English was used to collect participants’ gender, age, nationality, ethnic/racial background, highest degree, employment status, field of study/occupation, and clinical diagnoses. Participants also answered: (1) “How well do you feel you slept last night?” (from “Very badly” to “Very good”) and (2) “Did you exercise in the last 12 hours?” (“yes”/“no”).
The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004) is a 36-item self-report questionnaire assessing emotion regulation problems. Participants indicate on a 5-point Likert scale how often the items apply to themselves, with responses ranging from “almost never” to “almost always.” DERS Total Score and the following subscales were calculated: (1) Nonacceptance of emotional responses, (2) Difficulty engaging in goal-directed behaviour, (3) Impulse control difficulties, (4) Lack of emotional awareness, (5) Limited access to emotion regulation strategies, (6) Lack of emotional clarity. Higher scores indicate greater emotional dysregulation.
The Emotion Regulation Questionnaire (ERQ; Gross and John, 2003) is a self-report questionnaire measuring proneness to utilise cognitive reappraisal and expressive suppression. Participants answered 10 items on a 7-point Likert scale, ranging from “strongly disagree” to “strongly agree.” Higher scores on the ERQ subscale (Cognitive Reappraisal and Expressive Suppression) indicate higher proneness to implement each emotion regulation strategy.
The State-Trait Anxiety Inventory (STAI; Spielberger, 2010) has 40 items and two subscales: (1) State Anxiety Scale (S-Anxiety) and (2) Trait Anxiety Scale (T-Anxiety). The S-Anxiety scale assesses the intensity of anxiety “at this moment,” while the T-Anxiety scale assesses the frequency of feelings “in general.” Higher scores indicate greater anxiety.
The Subclinical Stress Symptoms Questionnaire (SSQ-25; Helms et al., 2017) measures mental and physical stress over the past 4 weeks. The SSQ consists of 25 items and participants respond on a 5-point Likert scale ranging from “not at all” to “very strong.” For the SSQ-25, we calculated the subscale scores (1) Psychological Stress and (2) Physiological Stress. Higher scores indicate higher stress.
The World Health Organization Quality of Life Instrument, Brief Version (WHOQOL-BREF; Skevington et al., 2004) is a self-report questionnaire assessing physical and psychological health, quality of social interactions and support, and quality of living environment. It has 26 items and participants respond on a 5-point Likert scale from “disagree” or “not at all” to “completely agree” or “extremely.” Four WHOQOL-BREF subscale/domain scores were calculated: (1) Physical Health, (2) Psychological Wellbeing, (3) Social Relationships, and (4) Quality of the Living Environment. To be made comparable with the WHOQOL-100 (the original scale from which the WHOQOL-BREF was adapted), each subscale/domain score was multiplied by 4 and subsequently transformed to a 0–100 scale. Higher scores indicate better perceived QoL.
Outcome measures
Raw heart rate signal was firstly band-pass filtered (8–20 Hz) to minimise the impact of artefacts and high frequency noise (Fedotov, 2016), before carrying out automatic detection of cardiac beats in Brainstorm (Tadel et al., 2011). This was followed by visual correction of potentially erroneous or missing peaks. The R package RHRV was used to compute the Low Frequency (LF-HRV) and High Frequency (HF-HRV) components of HRV, which were log-normalised before conducting the analyses. LF-HRV (calculated as the absolute power of the low-frequency band of the signal, i.e. 0.04–0.15 Hz) is thought to reflect the combined sympathetic and parasympathetic influence on the heart and, specifically, baroreceptor activity during resting conditions. HF-HRV (calculated as the absolute power of the high-frequency band of the signal, i.e. 0.15–0.4 Hz) mainly reflects the parasympathetic influence on the heart and is influenced by respiration rate (Shaffer and Ginsberg, 2017), and it is the most widely used measure of HRV (Laborde et al., 2017).
Main outcome variables from the questionnaires/scales included the DERS Total score and five subscale scores, the ERQ Cognitive Reappraisal and Expressive Suppression scores, the STAI S-Anxiety and T-Anxiety scores, the SSQ-25 Psychological Stress and Physiological Stress scores, and the WHOQOL-BREF Physical Health, Psychological Wellbeing, Social Relationships, and Quality of the Living Environment scores.
Statistical analysis and hypotheses
Before conducting the main analyses, we conducted a correlation analysis between all HRV measures. Considering the very high correlation between LF- and HF-HRV measures (all r > 0.866, all p < 0.001), we only included HF-HRV measures in the analyses. Moreover, we verified if there was an effect of block (i.e. difference in HF-HRV between resting-state, task and recovery), and if this effect was mediated by certain variables, including (1) age, (2) quality of sleep the night before testing, (3) gender, (4) having a clinical diagnosis, or (5) having exercised in the 12 hours before testing. We found that none of these variables affected HF-HRV measures and that there was only a statistically significant difference in HF-HRV between the task and the post-task resting-state, with HF-HRV increasing in the post-task resting-state versus task blocks (see Supplemental Material 2). We, therefore, decided to include in the analyses, in addition to HF-HRV measures (resting-state, task), ΔHF-HRV, calculated as the difference in HF-HRV between task and post-task resting-state. In line with the original pre-registered research aims, and based on the pre-analysis checks, we aimed to test the following hypotheses.
• Reduced emotional dysregulation (DERS total score) (H1a) • Reduced proneness to use expressive suppression (ERQ Expressive Suppression scores) (H1b) and Increased proneness to use cognitive reappraisal (ERQ Cognitive Reappraisal scores) (H1c) • Reduced Anxiety (S-subscale and T-subscale scores) (H1d) and Stress (Psychological Stress and Physiological Stress subscale scores) (H1e) • Increased QoL (WHOQOL-BREF Physical, Psychological and Social scores) (H1f).
We investigated Hypothesis 1a-f by conducting bootstrapped Pearson’s correlation analyses between several outcome measures, including HF-HRV measures, DERS total score, ERQ Expressive Suppression score, ERQ Cognitive Reappraisal score, STAI-S and STAI-T scores, SSQ-25 Psychological Stress and Physiological Stress scores, and WHOQOL-BREF Physical, Psychological and Social scores (descriptive statistics for the whole sample are reported in Table 1).
Sample characteristics.
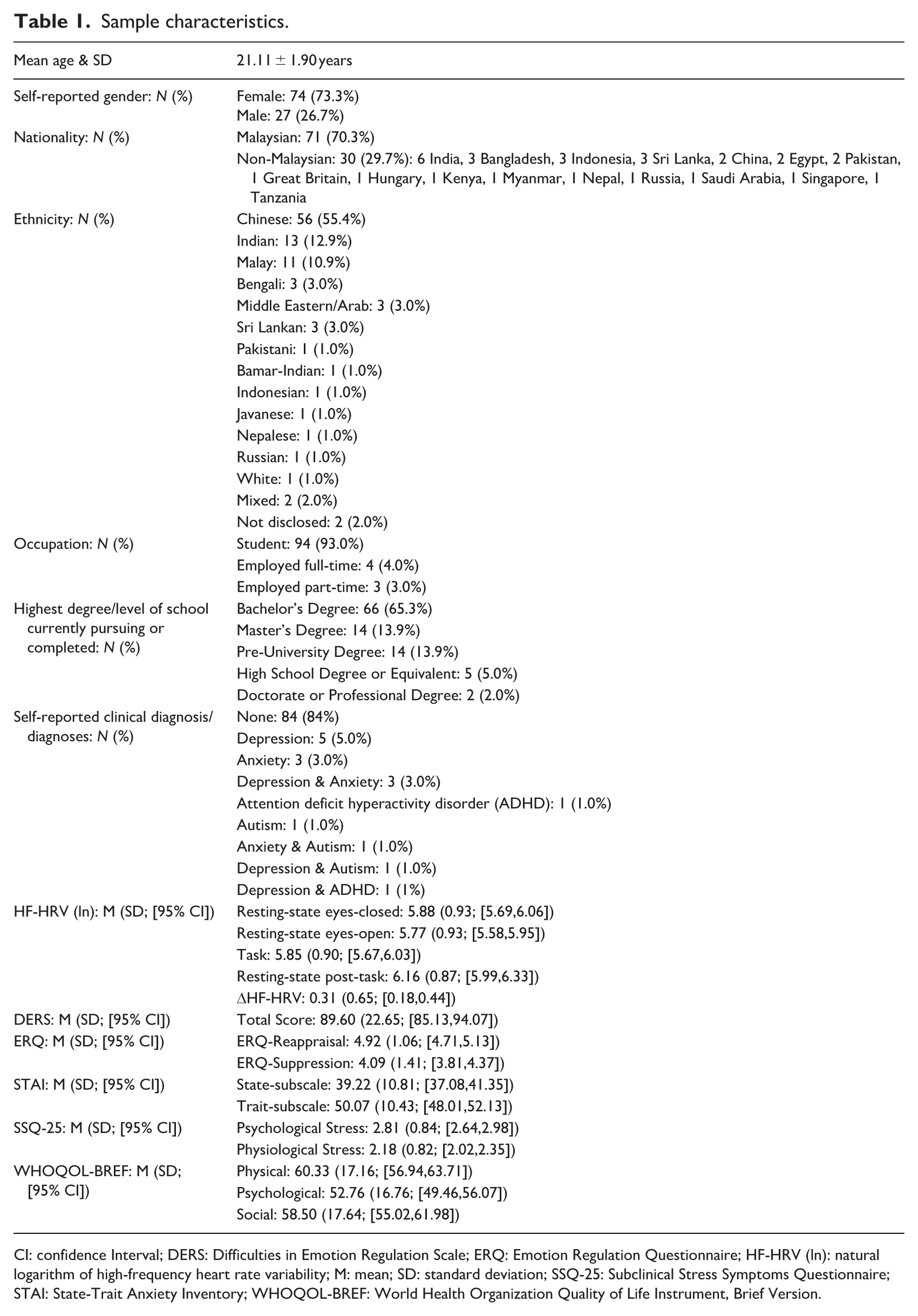
CI: confidence Interval; DERS: Difficulties in Emotion Regulation Scale; ERQ: Emotion Regulation Questionnaire; HF-HRV (ln): natural logarithm of high-frequency heart rate variability; M: mean; SD: standard deviation; SSQ-25: Subclinical Stress Symptoms Questionnaire; STAI: State-Trait Anxiety Inventory; WHOQOL-BREF: World Health Organization Quality of Life Instrument, Brief Version.
Results
Sample characteristics
The final sample consisted of 101 participants (Mean age = 21.1 ± 1.9 years; 73.3% females; Table 1). Most (93%) were students from the University of Nottingham Malaysia, and the rest of the sample (7%) included working young adults, all fluent in English. We observed heterogeneity in participants’ anxiety scores (STAI-Y scores ranged between 21 and 76), stress (SSQ-25 scores between 10 and 75), emotional dysregulation (DERS total scores between 47 and 152) and emotion regulation (ERQ scores between 4 and 42). Although it shall be acknowledged that none of the questionnaires/scales we used were validated in Malaysia, our sample reported mean ERQ and DERS scores in line with previous data reported in three Australian general community adult samples (Preece et al., 2020) and in a large sample of Italian university students (Giromini et al., 2017), respectively. However, anxiety mean scores in our sample were in the “moderate-to-severe” range (Kayikcioglu et al., 2017), and QoL mean scores were lower than previously reported in a representative sample of Australian adults (West et al., 2023).
Correlation analysis
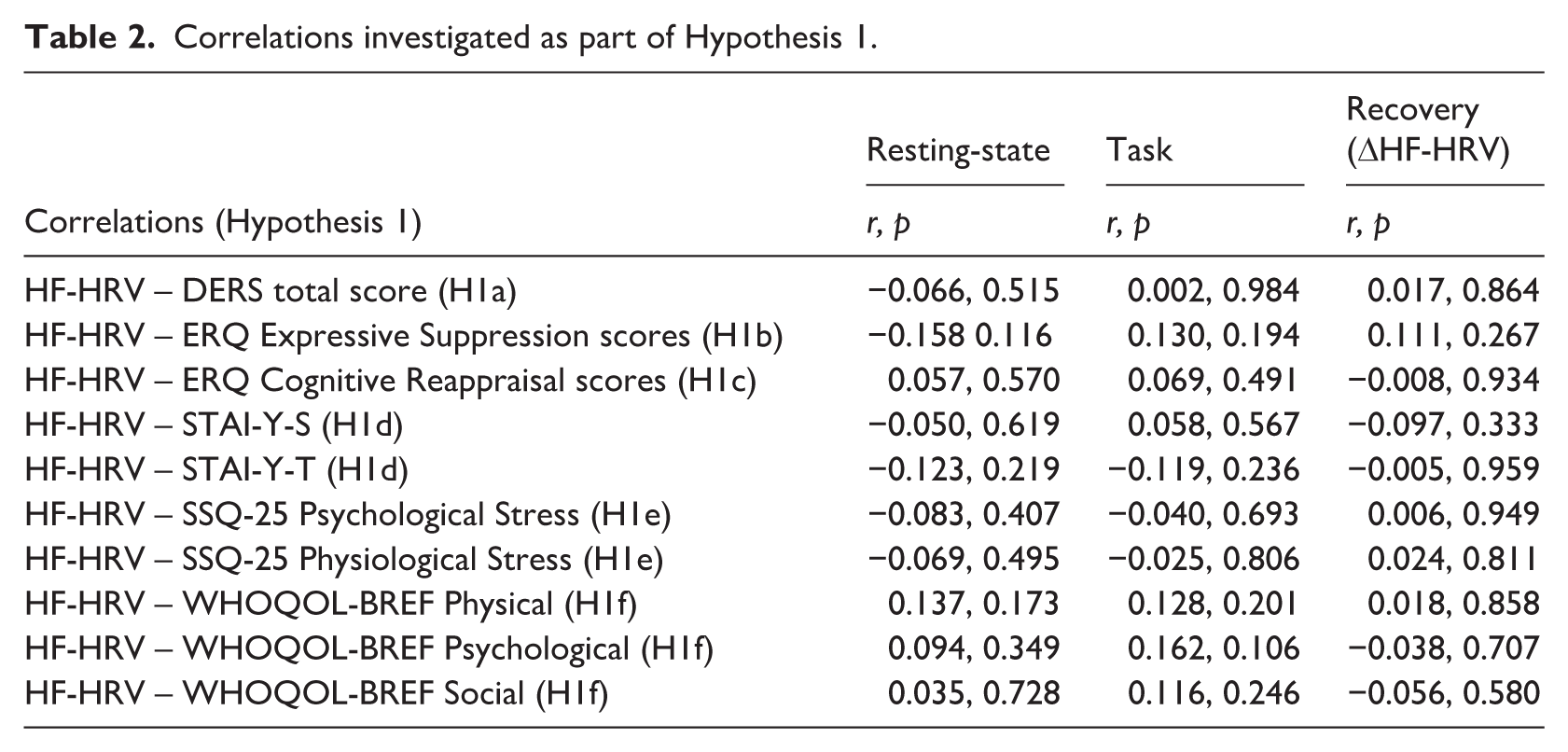
We found no statistically significant correlations between HF-HRV measures and all other measures (Table 2; see Supplemental Material 3 for full results). However, we found that participants who reported increased emotional dysregulation (DERS) were less prone to using cognitive reappraisal as an emotion regulation strategy (ERQ Reappraisal; r = −0.505), experienced increased stress (SSQ Psychological: r = −0.639; Physiological: r = 0.507) and increased anxiety (STAI-S: r = 0.579; STAI-T: r = 0.765), and reported lower QoL (WHOQOL Psychological: r = −0.699; Physical: r = −0.434; Social: r = −0.289). Furthermore, those who were more prone to using cognitive reappraisal as an emotion regulation strategy reported less anxiety (STAI-S: r = −0.473; STAI-T: r = −0.427), reduced stress (Psychological: r = −0.404; Physiological: r = 0.276); and increased QoL (Psychological: r = 0.512; Physical: r = 0.475). Conversely, those who were more prone to using expressive suppression as an emotion regulation strategy did not report more emotional dysregulation (r = 0.153; non-significant) or stress (Psychological: r = 0.145; Physiological: r = 0.153; both non-significant), but reported more trait anxiety (r = 0.240) and lower QoL in the psychological domain (r = −0.211).
Correlations investigated as part of Hypothesis 1.
Mediation analysis
The standardised coefficients for the direct effect of ERQ-Reappraisal scores on WHOQOL-BREF Physical, Psychological and Social scores (paths c′1, c′2 and c′3) were 0.218 (95% confidence interval = [0.060; 0.410]), 0.208 ([0.074; 0.350]), and −0.030 ([−0.254; 0.223]), respectively (Figure 1; see Supplemental Material 4 for further details). The standardised coefficients for the direct effect of ERQ-Suppression on WHOQOL-BREF Physical, Psychological and Social scores (paths c′4, c′5 and c′6) were 0.027 ([−0.072; 0.137]), −0.056 ([−0.140; 0.037]), and −0.096 ([−0.233; 0.041]). Therefore, participants who reported higher use of cognitive reappraisal as an emotion regulation strategy also reported higher psychological and physical wellbeing.
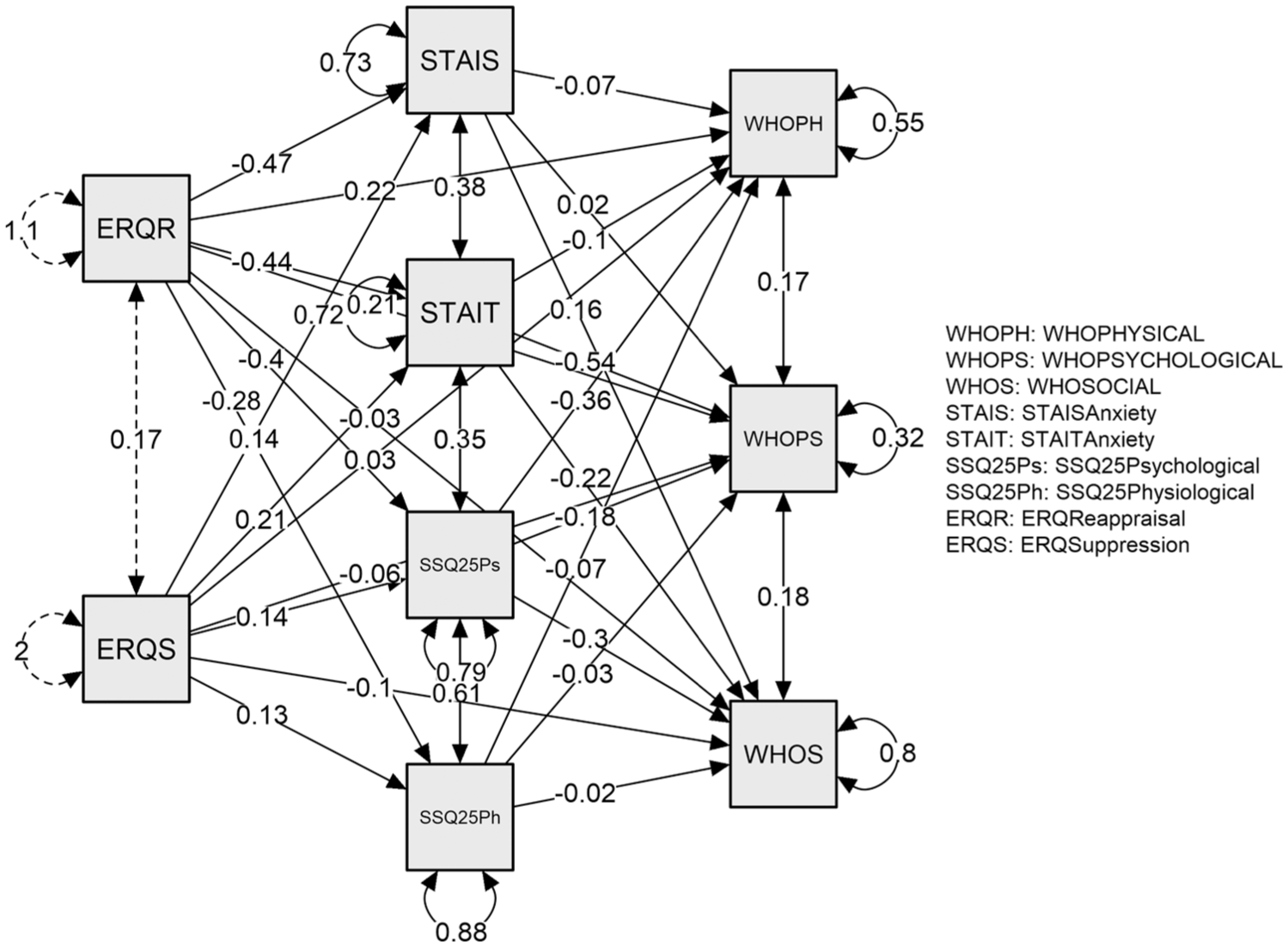
Model investigating the mediated relationship between cognitive reappraisal, anxiety and stress, and QoL (regression estimates are standardised).
When analysing the mediating effects of anxiety/stress variables on such associations (see Supplemental Material 4 for full results), we observed that psychological stress (SSQ-Psychological) was a significant mediator of the association between ERQ-Reappraisal and WHOQOL-BREF Physical (higher reappraisal scores were associated with lower psychological stress and this was associated with increased QoL). Furthermore, trait anxiety (STAI-Y) was a significant mediator of the association between ERQ-Suppression and WHOQOL-BREF Physical (higher expressive suppression scores were associated with increased anxiety and this was associated with lower QoL). Total effects and total indirect effects of ERQ-Reappraisal and Suppression scores on WHOQOL-BREF Physical, Psychological, and Social scores were statistically significant (reported in full in Supplemental Material 4), suggesting that participants with higher proneness to use cognitive reappraisal and less proneness to use expressive suppression reported higher QoL (Figure 1).
Discussion
We explored the associations between emotion regulation strategies, HRV, stress, anxiety, and QoL in young adults from the general population in Malaysia. Although we did not find an association between HRV and emotion regulation or psychological measures, our study highlighted that using cognitive reappraisal to regulate emotions in young adulthood is linked to more positive wellbeing and QoL outcomes.
Our findings are in line with previous literature (e.g. Aldao et al., 2010; Boemo et al., 2022) suggesting that adaptive and maladaptive emotion regulation strategies are differently associated with how young adults cope with stress and anxiety, as well as with varying wellbeing outcomes. Emotional dysregulation is increasingly recognised as a key psychological phenomenon, due to its transdiagnostic nature and potential role in the onset and maintenance of mental health challenges during adolescence and young adulthood (Easdale-Cheele et al., 2024; Kessler et al., 2007). While causal relationships cannot be confirmed, it is plausible that learning to adopt adaptive emotion regulation strategies in response to stress or negative emotions may equip children and young people with socio-emotional skills that enhance academic, professional, and social outcomes, ultimately improving QoL.
Equipping young people with effective emotion regulation skills is essential to increase resilience and coping capacity. Simultaneously, ensuring conditions that support good QoL may foster the development of age-appropriate regulation skills. Difficulties in emotion regulation can be highly impairing, sometimes contributing to self-harm, suicide, or substance abuse (Paulus et al., 2021). However, the specific factors influencing the maturation and strengthening of emotion regulation across development, and its relationship with QoL, remain unclear and warrant further investigation. Future research should examine the potentially negative impact of social determinants, such as poverty or discrimination, which may affect emotion regulation development and negatively affect QoL (Fortuna and Shah, 2023). Further research is therefore needed to elucidate this association and, if possible, the directionality, to further inform the design of specific interventions to promote the acquisition of emotion regulation skills in children and young people.
Although prior research has linked weaker arousal regulation to psychopathology and mental distress (Beauchaine and Thayer, 2015; Bellato et al., 2023a, 2024), we did not find associations between emotion regulation, psychological measures, and HRV in this study. Our sample primarily consisted of a general population, with few participants reporting mental health difficulties or neurodevelopmental disorders. Even among participants with self-reported clinical diagnoses (e.g. anxiety, depression, ADHD, autism; 16% of the sample), HRV measures did not differ from those without diagnoses, despite lower psychological QoL and marginally higher anxiety. Larger samples, or those enriched with participants with clinical diagnoses, may be needed to detect HRV differences associated with emotion dysregulation.
A strength of this study is its inclusion of an ethnically diverse sample of young adults. Malaysia is a middle-income country where public resources are limited and support to young people with psychological and mental health difficulties may be lacking. We were able to involve mostly Malaysian participants and about 30% of participants were from 17 other nations, with 14 ethnicities overall represented in the study. This is uncommon in research on emotion regulation (or psychology research in general); most studies on this topic have included White participants from Western or High-Income countries (see, e.g. Shahidin et al., 2022).
Given the significant role universities play in young adults’ lives, it is important to allocate resources to support students, particularly during high-stress periods (e.g. first-year transition, exam periods) or when they struggle to process and regulate negative emotions. Future research could evaluate low-resource interventions, such as self-paced online programmes, that help students identify and implement emotion regulation strategies in daily life to support wellbeing, QoL, and academic, professional, and social functioning.
Some limitations of our study should be addressed in future research. Our sample was mainly comprised of university students, with only 7% non-students, limiting generalisability to the wider Malaysian population. Although the sample size provided sufficient power (>80%) to detect medium effects, its small and unrepresentative nature may explain the non-significant associations with HRV. Additionally, the cross-sectional design precludes causal inferences and limits interpretability of mediation analyses. Future research should employ designs that control for unmeasured confounds, such as longitudinal or genetically sensitive studies, to clarify directionality and causality.
Conclusion
In conclusion, our findings underscore the importance of adaptive emotion regulation, particularly cognitive reappraisal, in promoting wellbeing and QoL in young adults. While HRV was not associated with emotion regulation in this general population sample, the study highlights the potential benefits of fostering adaptive regulation strategies and the need to better understand developmental and social factors influencing emotional skills. Interventions that support emotion regulation (especially in resource-limited or diverse settings) may play a crucial role in enhancing psychological resilience and life outcomes in young people.
Supplemental Material
sj-pdf-1-hpq-10.1177_13591053261433384 – Supplemental material for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults
Supplemental material, sj-pdf-1-hpq-10.1177_13591053261433384 for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults by Chern Yi Marybeth Chang, Marieke De Vries, Madeleine J Groom, Giorgia Michelini and Alessio Bellato in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053261433384 – Supplemental material for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults
Supplemental material, sj-pdf-2-hpq-10.1177_13591053261433384 for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults by Chern Yi Marybeth Chang, Marieke De Vries, Madeleine J Groom, Giorgia Michelini and Alessio Bellato in Journal of Health Psychology
Supplemental Material
sj-pdf-3-hpq-10.1177_13591053261433384 – Supplemental material for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults
Supplemental material, sj-pdf-3-hpq-10.1177_13591053261433384 for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults by Chern Yi Marybeth Chang, Marieke De Vries, Madeleine J Groom, Giorgia Michelini and Alessio Bellato in Journal of Health Psychology
Supplemental Material
sj-pdf-4-hpq-10.1177_13591053261433384 – Supplemental material for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults
Supplemental material, sj-pdf-4-hpq-10.1177_13591053261433384 for The association between emotion regulation strategies, anxiety, autonomic arousal, and quality of life in Malaysian young adults by Chern Yi Marybeth Chang, Marieke De Vries, Madeleine J Groom, Giorgia Michelini and Alessio Bellato in Journal of Health Psychology
Footnotes
ORCID iDs
Ethical considerations
This study received ethical approval from the Science and Engineering Research Ethics Committee at the University of Nottingham Malaysia on 1st December 2022 (reference: CCYM161122).
Consent to participate
All participants signed an informed consent form before participating to the study.
Consent for publication
Participants – in the consent form – provided consent for their anonymised data to be published as part of future scientific articles.
Author contributions
Conceptualisation: AB; Data Curation: CYC, AB; Formal Analysis: CYC, AB; Funding Acquisition: AB; Investigation: CYC, AB; Methodology: AB; Project Administration: AB; Resources: AB; Software: CYC, AB; Supervision: AB; Validation: AB; Visualisation: CYC, AB; Writing – Original Draft Preparation: CYC, AB; Writing – Review & Editing: CYC, MdV, MG, GM, AB.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by the Faculty of Science & Engineering (FOSE) at the University of Nottingham Malaysia (reference: FOSE Pump Priming Grant 2022).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Bellato declares: (a) funding from the National Institute for Health and Care Research (NIHR208319) and the Academy of Medical Sciences (NGR2\1430), (b) honoraria from the Association for Child and Adolescent Mental Health (ACAMH) for educational activities, (c) honoraria as Joint Editor of JCPP Advances, (d) consultancy honoraria from the Cyprus Research and Innovation Foundation, Swiss National Science Foundation, and Wallenberg Foundation, and (e) travel reimbursements from the ACAMH and the International Brain Research Organization (IBRO); none of this related to the present project. He is also member of the NHS England ADHD taskforce. The other authors declare no conflict of interest.
Data availability statement
The protocol (uploaded on 27th January 2023) and associated data (uploaded after the end of study, which was conducted between February and July 2023) are available at https://osf.io/qjmvn/. Data were analysed using IBM SPSS Statistics 29 and JASP (![]() ).
).
Supplemental material
Supplemental material for this article is available online.