
Abstract
Despite common co-morbidity of physical and mental health conditions, they remain analytically separated. Using a hermeneutic phenomenological framework, we investigate bodily and emotional dimensions of the lived experience of physical and mental illness. The existential lifeworld framework of van Manen is used to interpret experientially based meaning-making through embodied encounters with physical illness. Ten individuals with long-term physical health conditions were interviewed. Existential lifeworlds intertwined across themes and lived-body took central position within embodied experientially based meaning-making. Embodied meanings made within emotionally charged settings shaped the physical-mental-illness cycle, with dynamic emotions unbounded by time, shaping individual lifeworlds. Changing perceptions of lived-time and lived-space were shaped by the bodily and emotional experiences of physical health conditions. Conceptualisations of self-identity and mattering challenged internal worlds. Lived-relations were experienced in mattering to others. Self-identity shaped existential changes across lived-time, lived-relations and lived-space. Embodied mental health shaped lived-things with digital technologies supporting their needs.
Keywords
Introduction
Multimorbidity (or co-morbidity) involves the co-occurrence of more than one illness in the same person (Valderas et al., 2009). The presence of mental illness in chronic illness, disease and physical illness is well documented (Pizzol et al., 2023). Research demonstrates elevated risk for mental health problems in those with both severe physical health conditions and disease (Pizzol et al., 2023), including post-traumatic stress disorder (PTSD; Andelic et al., 2010), anxiety (Max et al., 2011), and depression (Scott et al., 2007) as well as decreased self-esteem (Nosek et al., 2003), and increased social isolation (Osborne-Crowley and McDonald, 2018). Though decreased mental wellbeing is often an outcome of physical illness (Tough et al., 2017), injury (Wiseman et al., 2013) and disease (Barnard et al., 2006; Wiseman et al., 2013), mental health needs are often not considered in tandem with the physical health condition upon diagnosis and treatment (Coventry et al., 2014). Importantly, mental wellbeing, which encompasses reflective processes such as self-esteem, contributes to overall mental health (de Cates et al., 2015; Harris and Orth, 2020).
Associated physical and mental health is not conclusive, however. For instance, literature shows a complex association between physical health and self-esteem (Miyahara and Piek, 2006; Nosek et al., 2003). Some studies have sought to understand the dynamic interaction between this dual mind-body experience. For instance, greater deterioration to self-esteem, found for minor versus major disabilities (e.g. cerebral palsy), is suggested to be driven by experientially based meaning-making of physical health and changes to physical competence (Miyahara and Piek, 2006). Asmundson et al. (2002) also reported the perpetuation of chronic pain and PTSD co-morbidity through mutual maintenance, highlighting the embodied experience of physical and mental health. Other research investigates the temporal dynamics and mechanisms of this interaction. For instance, studies show changes to mental wellbeing following physical illness onset due to favourable social exchanges decreasing, limited social engagement, changes to lifestyle, family functioning and relationship quality, which impact subjective appraisals of functioning, mood and life-satisfaction (Stevens et al., 2008). Furthermore, decreased wellbeing, with physical illness, may precede mental illness onset (Ownsworth and McKenna, 2004), with changes to capabilities reducing quality of life, and increasing symptoms of anxiety and/or depression (Kalpakjian et al., 2009; Wiseman et al., 2016). Interactions between physical and mental illness are dynamic, as the presence of depression in chronic disease is associated with greater deterioration to physical health (Moussavi et al., 2007). Taken together, findings highlight a cycle of physical-mental-illness and the dynamic processes involved in mind-body experience within physical illness.
Research shows social support is key in coping with mental health and wellbeing in disability and physical injury, with nuanced factors such as relationship quality moderating the association (for systematic review see Tough et al., 2017). Enhanced social support in physical injury is shown to improve physical health and persistent pain (Prang et al., 2015). However, physical injury onset often leads to significantly higher levels of social isolation compared to the general population (Osborne-Crowley and McDonald, 2018; Prang et al., 2015). This if often attributed to social integration difficulties following injury (Andelic et al., 2010), or the effect of mental health difficulties on maintaining social relations (Matthews et al., 2016). Impairments to social functioning are often a symptom of depression, which presents difficulties for attachment, social communication and social perception (Kupferberg et al., 2016). However, the literature exploring the role of mental health support services and the mechanisms of social support in physical illness sheds little insight on experientially based meaning-making.
We postulate that a better understanding of the complexities of the day-to-day lived experiences of those with a physical health condition and mental health difficulties will open a gateway to identifying both changes in emotions following physical illness and the complexities of a physical-mental-illness cycle. This can be better understood through a phenomenological framework that can offer insight on the individuals’ existential lifeworlds (van Manen, 1997) of physical illness and the meanings given to the phenomenological experience of physical illness as it is embodied within situations and activities that form part of the individual’s lived experience. Previous studies present successful application of phenomenological inquiry to gain insight into the existential experiences related to daily life with physical illness such as systemic lupus erythematosus (Larsen et al., 2018), physical activity post-weight-loss surgery (Groven et al., 2017), and chronic back pain (Stensland and Sanders, 2018). Our study applies a phenomenological approach to generate novel insights on the lived experience of physical illness, in addition to emotional changes following physical condition onset and the complexities of the physical-mental-illness cycle.
Research aims
This study aimed to: (a) capture and ascertain the complexity of individual lived experiences of those with different physical health conditions as it is experienced day-to-day, within situations and activities; (b) gain insight into the bodily and emotional dimensions of the individual’s lifeworlds, for those with physical illness with particular attention to changes in emotions; and (c) assess the application of a phenomenologically informed approach to grant access to the individuals’ lifeworlds and their experience of physical illness and mental health difficulties.
Methods
Theoretical and philosophical perspective
The chosen methodological framework enabled recognition and investigation of the subjective lived experience of physical health conditions (Livneh, 2001). Epistemologically we draw on the phenomenology of van Manen (1997), which centres on uncovering the meaning of “the lived world as experienced in everyday situations and relations” (van Manen, 1997: 101), utilising van Manen’s Hermeneutic Phenomenological Approach (van Manen, 1990, 2014, 2017). This allowed for an interpretivist paradigm focussing on the meanings created by participants on the experienced physical health condition. The lifeworld existentials model outlined by van Manen (1997) provides a framework for interpreting the lived experiences of different phenomenon and has been applied previously to understand mental-physical co-morbidity in chronic physical illness (Coventry et al., 2014). We describe and interpret individual lifeworlds, acknowledging the subjective experience (Kitcey et al., 2022). Following a similar approach to that of Coventry et al. (2014) we draw on the phenomenological paradigm of the lived body, as articulated by Merleau-Ponty (2002). In doing so we situate the lived-body within the lifeworld of the individual however, we use van Manen’s (1997) lifeworld existential model as a methodological device to understand the individual’s experientially based meaning-making and their lifeworld existentials as they are transformed through physical illness. Our underlying theoretical premise is that meaning is embodied, as experience is bodily based and subject to ongoing change (Johnson, 2007; Merleau-Ponty, 2002). This theoretical framework was applied successfully to understand physical illness by others. For example, Groven et al. (2017) applied van Manen’s Hermeneutic Phenomenological Approach to explore phenomenologically the lifeworld existentials of physical activity following weight loss surgery placing the lived-body lifeworld as central to meaning-making.
Drawing on the theoretical premise of Johnson (2007, 2017) meaning is embodied through the interactions between organism-environment interactions, with meaning emerging within the flow of experience as we engage in those situations and carry forward the sense of meaning made from the current experience with past meanings. Importantly, Johnson (2007) also highlights the dynamic interactions of meaning-making as connections span past, present and future experiences, actual or imagined. This framework offers a means to explore meanings locating the centrality of the body existentially across time and situation. Moreover, in doing this we acknowledge the shifting nature of reflexivity within experientially based meaning-making. As in the phenomenological research on Toombs (1993) and Sartre (2003) the person’s position on what it means to become ill shifts from pre-reflective reception of sensations to reflective awareness of illness. The shifting levels of reflectiveness within the phenomenological experience is present in the work of Husserl (1982) and within the current study highlights the multilayered and dynamic shifting of reflectiveness within phenomenological philosophy whereby a participant’s interpretations with respect to significant health concerns are experienced against an originally taken for granted body. The shift to the reflective then means that the personal experience of the participant and their views and understanding are ingrained within the phenomenon itself. It offers a framework within the current study in which to explore experientially based meanings in a dynamic sense, as they emerge in situations and forge connections that transcend time. Specifically, this is applied in the current study to shed light on the lived experience of physical illness, its associated emotional changes, and the dynamic interactions of the physical-mental-illness cycle.
Sample and recruitment
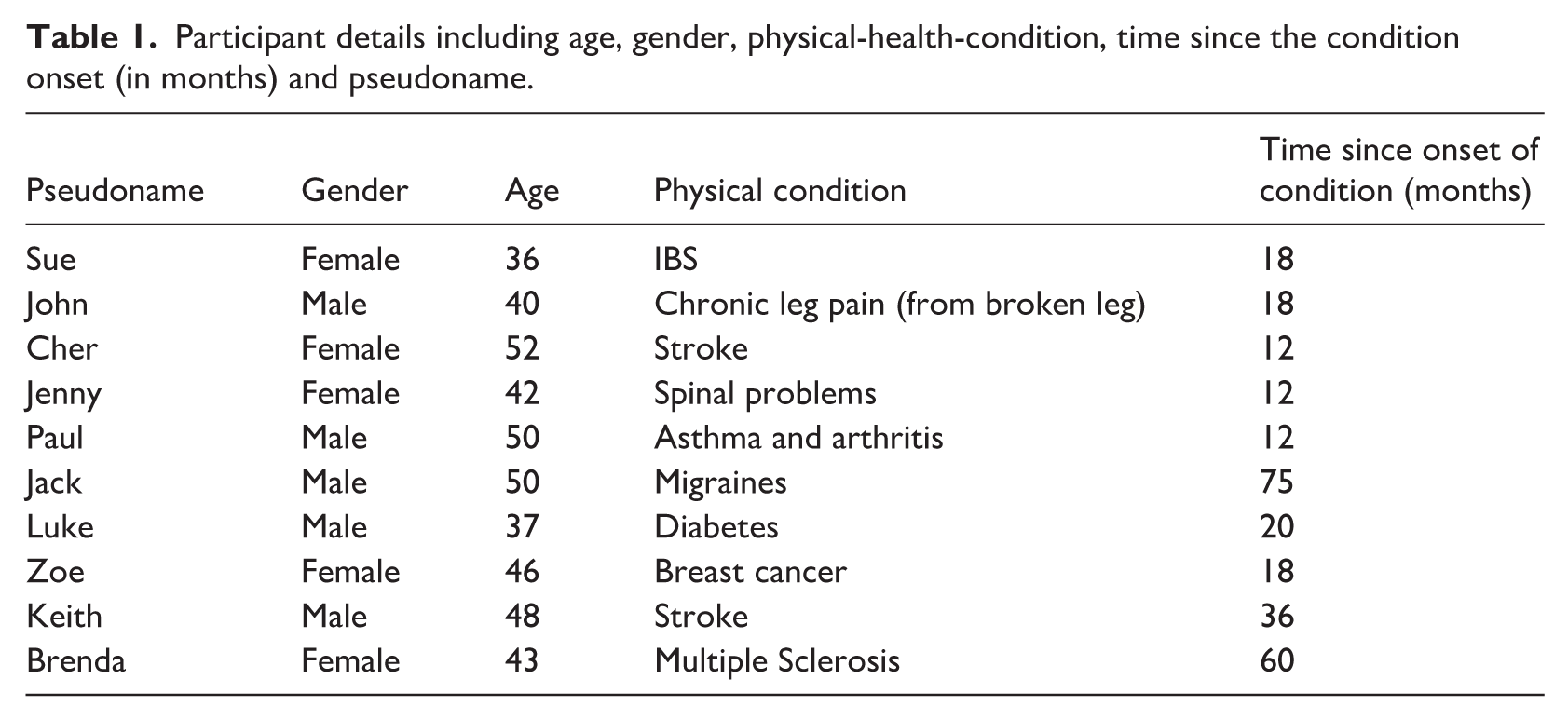
Ten individuals (aged 36-to-52 years) participated. Inclusion criteria mandated presence of a diagnosed physical health condition for 12 months minimum, AND which had led to lifestyle and wellbeing changes. Participants were excluded if they presented with severe and enduring mental health problems (psychosis and/or bipolar disorder), AND/OR those who were not English language speaking. Demographic details for participants are included in Table 1. Pseudo names are given to participants to maintain anonymity but relatability. Participants, recruited from an unrelated study, consented to receive communications regarding further studies within 24 months post-debriefing. Ethical approval for the study from local Research Ethics Committee was obtained. Signed consent was obtained to take part in the qualitative interviews. Interviews took place online to accommodate the preferred setting of the participant (Oltmann, 2016); an approach proven beneficial in previous research (Majid et al., 2017).
Participant details including age, gender, physical-health-condition, time since the condition onset (in months) and pseudoname.
Data collection
The main aim of this qualitative study was to explore and describe the lifeworlds of people who live with physical illness. We undertook in-depth semi-structured interviews. The interview schedule consisted of key topics with open-ended questions and prompts to explore the participants’ biographical account of physical illness and the physical challenges related to the condition, as well as mental health and wellbeing, including self-esteem and social relationships. Importantly questions captured van Manen’s existential lifeworlds, including lived-time (e.g. “When and how did you begin to recognise changes to your health in relation to your condition?”), lived-relations (e.g. “How does social support change the way you cope with your illness?”), lived-body (e.g. “How has your condition affected your abilities?”), and lived-space (e.g. “How did your social life change as a result of your condition?”), as well as questions that opened up descriptive accounts of changes in emotions (e.g. “How has this condition affected you emotionally?”). Prior to conducting the study, a pilot study was carried out with the primary aim of testing the interview schedule for its effectiveness in obtaining the required responses for an interpretative phenomenological account of the participant’s lived experience of physical illness. The interview schedule served as a guide to facilitate participants’ in telling their own lifestory, using prompts as deemed necessary to gain clarification and deeper insight (van Manen, 1990, 1997). Awareness of thematic aspects was present at this stage particularly in relation to embodied meaning as the self was positioned over time as well as within the visceral and emotionally laden experience of physical illness, as meanings made were embodied in situations and activities.
Analysis
Verbatim interview transcripts (recorded via Dictaphone) served as raw data which were analysed using a hermeneutic phenomenological framework and the analytical approach outlined by van Manen (1990). Each transcript is treated as a discrete case which are then integrated at a later stage of analysis. Interviews were first transcribed using a playscript approach (Hepburn and Bolden, 2017). The key stages in the analytic process are summarised as follows: (1) Whole-interview approach: transcripts were read and re-read to capture the meaning of the entire text. Annotations and memo notes are made in parallel as we questioned the phenomenological meaning of the text as a whole; (2) Selective approach: this involves highlighting statements which capture phenomenological meanings in thematic expressions or reflective descriptive interpretative paragraphs; (3) Detailed approach: each sentence is reviewed in relation to its insight about the phenomenon or experience being described. We engaged in a process of thematic analysis and with each approach identification of emergent themes is supported with the use of memo notes. Drawing on hermeneutic phenomenology our analysis explored how lifeworld existentials interact across multiple perspectives of those with a lived experience of physical illness. Themes are considered in relation to the extant literature in the discussion section and understood in relation to the lifeworld existentials framework proposed by van Manen (1997). As part of our collaborative and self-reflective process we questioned the pertinence of each theme for the phenomenological experience to determine whether it is essential.
Validity, reliability and trustworthiness
Internal validity and reliability were assessed using internal coherence (Smith, 1996). Specifically, this is the proposition that sufficient verbatim evidence from the participant should be presented in the paper to allow the reader to interrogate the interpretation. Transcripts were looked at independently by the second author. Authors discussed their readings and came to an agreement on theme categories. Personal field journals were used during data gathering to reflect upon the dual role as researcher and interpreter. Critical self-reflection on prior knowledge and experience of the participants was central to account for presuppositions of the phenomenon within the relationship. Journal entries included reactions to interview responses, accompanying notes and general interview impressions. To enhance transparency, coherency and trustworthiness of themes authors challenged personal interpretations of the participants’ experiences, serving a dual role as critical friend within the interpretation process.
Findings
Our study revealed meanings of embodied experiences, social relations and emotional reflections in relation to physical illness. Lifeworld narratives centred on experientially based embodied meanings of living with physical illness. These were expressed in relation to the five core themes that span the existential lifeworlds framework described by van Manen’s (1997) Existential Lifeworld Model and are summarised in Figure 1.
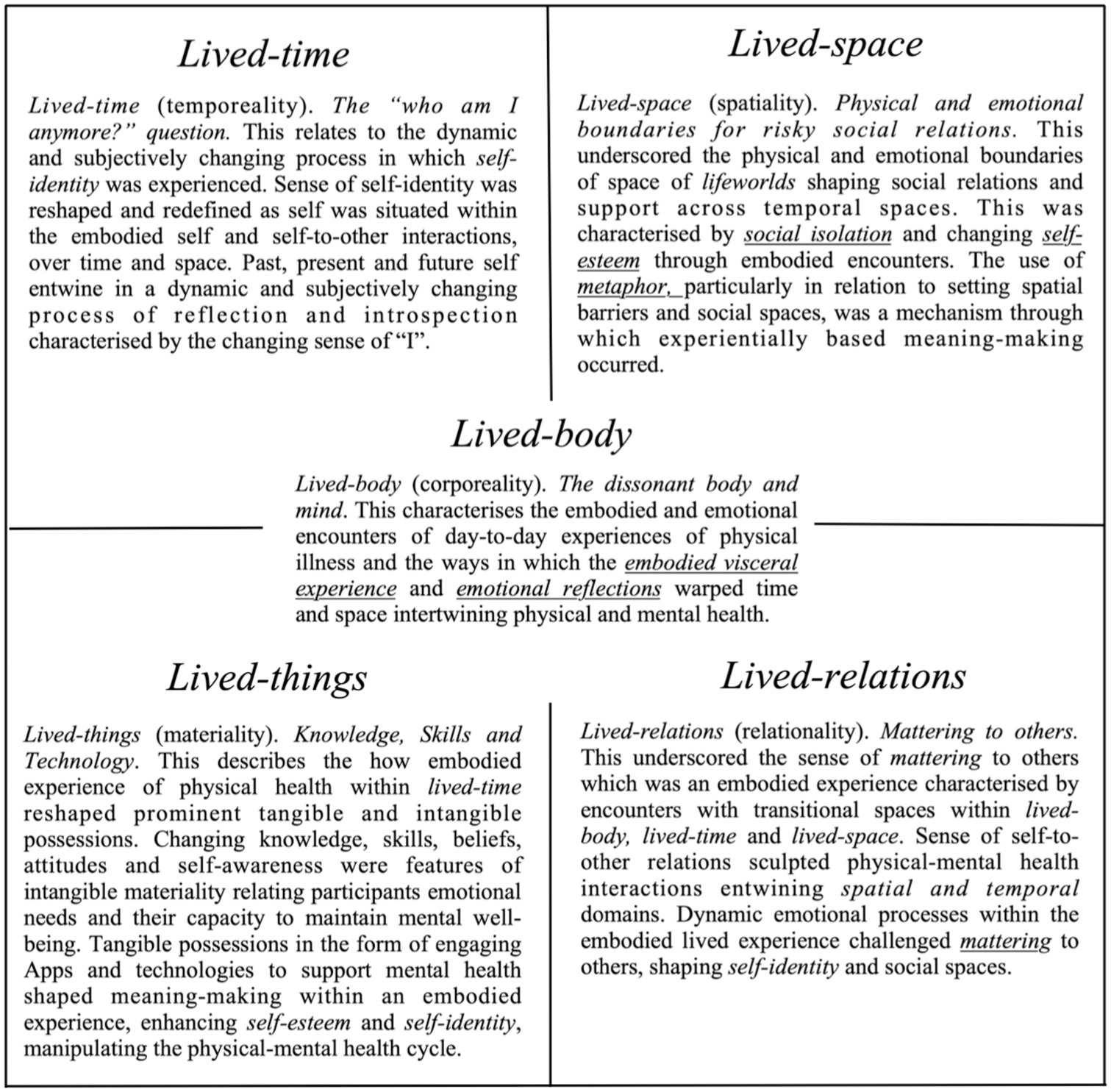
A summary of the five core themes identified are presented against the existential lifeworlds described by van Manen’s (1997) Existential Lifeworld Model.
Lived body: The dissonant body and mind
For participants the experienced physical health condition involved a change to physicality namely, reduced capabilities. Meaning-making was embodied through participant-environment interactions connected to past, present and future experiences. For some participants, such as John, who experiences Chronic leg pain, the experienced pain was a constant feature:
I used to have breakdowns because of it, it’s like a whole different lifestyle and everything that you’re used to suddenly you can’t do anymore so it’s very tough, I found it really really hard to deal with cause usually I’m always on my feet. I was so down. (John)
Other participants, such as Cher and Keith (who experienced stroke), and Brenda (diagnosed with Multiple Sclerosis (MS)), lived the condition through a shift in physicality marked by a consistently different state of capabilities. The lived experience of the physical condition is accompanied by a constant vigilance to the condition, which could reoccur, for instance, in the form of further stroke or further debilitating MS episodes. The cyclical interaction between physical health condition and psychological outcomes was evident and experienced through the embodied and emotional encounters of day-to-day life, within the lifeworld existentials of lived-body, lived-space, lived-relations, lived-time and lived-things.
Paul whose physical illness includes asthma and arthritis, experienced frustration towards the symptoms associated with his physical health condition, “it stops me from doing things that I would usually do.” Meaning-making of bodily based changes within situations was an emotionally loaded experiential process, as Keith describes, “I had a stage where I was really down and depressed because of it.” Furthermore, how individuals experienced various physical activities in different situations and construct meaning from them is carried forward, with connections to past, present and future experiences, as John states, “My legs just don’t work. . .I can’t stand to look at myself in the mirror anymore.” The juxtaposition of the current state from a prior state ran throughout the narrative accounts of participants and became a common feature of experientially based meaning-making. For example, in seeking to illuminate the meanings of physical activity, Paul reveals making sense of changes from pre- to post- physical condition within social activities and hobbies, which are concrete situations and settings that are meaningful to the individual:
. . .and the gym I used as an escape too so it was like I don’t know getting away and getting out all my frustration and energy on that and setting records for myself it kept me going and it was such an amazing feeling. So now I can’t do that anymore I just feel so lazy and unmotivated and I’m not used to feeling like this it’s horrendous. (Paul)
For Paul social activities and hobbies were experienced positively pre-health condition and experientially based meaning-making becomes intrinsically connected to past experiences.
The physicality of the condition through lived-body was a visceral experience shaping the experience participants had with their body as described by Cher:
It was a bit of a battle because sometimes migraines are triggered by stress. And I was really stressed out at work because I was taking way too much on and I was getting very severe migraines and actually ended up having a minor stroke because of all the stress. (Cher)
Here, Cher whose physical health condition had been the result of stroke, describes the visceral experience as stress, which was itself an emotional reflection of the lived-body experience. This echoes the theoretical framework used in the study of Groven et al. (2017) who drew upon experientially based meaning-making in a similar vein to that in the current study, highlighting, “how individuals make meaning in concrete situations and settings is an ongoing bodily based and emotionally loaded experiential process in which past, present and future intertwine” (p. 2). This visceral experience is further captured in the words of Brenda:
Well it has made me feel more depressed and worried about my job security as I know there will be a point where the chest pains get too much for me and I won’t be able to carry as much so I don’t know how much longer I can stay in this job cause it clearly isn’t really working out for me anymore. (Brenda)
This is further captured by Jack who had previously experienced stroke, “I started getting very stressed out at work and one thing led to another and I ended up having a stroke,” and Brenda who experienced Multiple Sclerosis, “I would panic that they would see me. . .every time it would set off another relapse.” The embodied experience of the physical health condition became synonymous with mental health and constant vigilance to monitor it, as stated by Sue, “I had to be really careful how I did things and had to make sure I didn’t get stressed out and it was just a lot to deal with and very confusing and difficult.” (Sue). We note the visceral experience whereby the intuitive and physical response intertwine within the lived experience accounts of physical illness.
Lived-space: Physical and emotional boundaries for risky social relations
The lived experience of the physical condition defined the participant’s spatial boundaries in terms of the physical space they occupied. This shaped the lived-space lifeworld for the participants’ and connected lived-space and lived-relations lifeworlds. Meanings were made through the participants’ connections to and relations to others. Consequently, this shaped not only the spatial boundaries of the lived-space lifeworld, but also the emotional boundaries of the participants existential lifeworlds. The narratives of participants present a dynamic interacting flow between the lived-space and lived-relations lifeworlds which we present here to understand their experientially based meaning-making of physical health.
In a sense living with the physical condition was the extent to which the physicality of the condition created limits, which were most prominent through their relations with others. Participants experienced the physical condition as a limiting presence of others in their lives, often leading them to endlessly question what they were able to do, or should do and how others might respond to the physicality of their health condition. Participants would often place spatial limits to keep them from engaging in relations with others. These new boundaries offered protection, transforming the lived-space to accommodate depleting physical limitations and offer emotional protection from social interactions which are anticipated to yield emotionally negative outcomes. Changes in physical capability transformed the participants’ relationship with lived-space, characterised by withdrawal from social interactions physically; as Jack states, “I just don’t have the energy for it” (Luke), and “it’s just exhausting mentally and physically.” The social world of participants was smaller. As Paul explains:
Well I used to play football once a week and go the gym three times a week but I physically can’t do that anymore because of both the arthritis and asthma which is difficult for me because football was kind of the main way I socialised if that makes sense. So all my friends I would see at football and gym so because I don’t or can’t do that anymore its isolated me a bit. (Paul)
This demonstrates how physical health and its associated capability limitations shaped the participants’ social landscape, transforming the experience of both lived-space and lived-relations. The lived-body is central to the lifeworld existential model and connects lived-space and lived-relations. The activity of socialising for Paul was embodied as an emotionally laden and physically exhausting experience. This is captured in the narrative of John who states:
If my friends made plans to go out, it’s just a lot of effort cause that would mean I need to get ready which is a lot harder than you think, and then I can’t drive myself so need to get a lift, limp to the car and limp around wherever we’re going, it’s just so exhausting mentally and physically . . . small normal things like going out with your friends suddenly comes with a lot of mental and physical effort which I just don’t have the energy for. (John)
Cher also states she no longer had energy to socialise and failed to “see the point”. Socialising, now framed around mental and physical effort, led to social isolation, as also identified by Jenny who reports:
I want to spend time with them, but I just get really anxious anytime I’m out. And when I am out, I’ll try to speed it up so I can just go home but obviously that isn’t fair on my family or whoever I’m with at the time because they just want to enjoy themselves and have a good time but there’s like a barrier now and I just can’t do that anymore. (Jenny)
A barrier is also present in Jenny’s experience when she states, “I just can’t do that anymore.” Non-disclosure of the physical health condition and avoidance of social interaction was reported by participants. Lived-relations are shaped with a changing self in relation to others and the lived-body maintains an ineffable space within lived-relations characterised by what is not said. For instance, Zoe states, “I’m quite sure they do know something is up, but they haven’t said anything and neither have I” and Cher who states:
I could talk to them about it, but I haven’t because I don’t know I just feel like it’s quite embarrassing cause to be honest I’m not even sure what it is myself. Like what am I meant to say? (Cher)
The difficulty in expressing the emotional experience within a narrative challenges the lived-relations lifeworld and highlights the ineffability of the lived experience of the physical-mental-illness cycle. The lived-body within lived-relations lifeworld and the need for privacy due to embarrassment and fear of others behaving differently is expressed by Jenny:
I had no wish to meet people outside of the family and really did not want anyone to know and start feeling sorry for me. So I kept things as quiet as possible. (Jenny)
Participants expressed a lack of understanding and acceptance from their social relationships which echoed a sense of their own need to accept and come to terms with their own physical health condition and transitioning lived-body lifeworld. The physical separation came to serve as an emotional “barrier” of protection for participants’ reinforcing the sense of disconnect in the form and shape of an “outside” world. This also highlighted how participants reinforced a disconnect from a more mainstream society of normality. Here the existential spatiality of lived-relations balancing physical boundaries (spatiality) and mental (emotional) disconnect (collectively reflecting the lived-space lifeworld) reinforced nondisclosures and the construction of their own lives as “different” to those of others. Thus, lived-relations and lived-space present a dynamic interaction shaping meaning-making and the lived experience of physical-mental-illness.
The use of metaphor on later reflections of the physical health condition was evident, as Sue states, “luckily. . .very few people knew what was going on behind closed doors.” This metaphorical depiction of the physical world denotes a physical separation from others. In addition, this framed the participants’ existential lifeworlds as different to others, being outside the norm or rather abnormal to that of the “outsiders”; in other words, different to those on the other side of the door. This reinforced a barrier between the participants and their social relationships, hindering their development and utility as a source of support. The participants sense of being different to others is experienced through their desire not to be labelled or treated as different; for example, Sue states, “it’s weird because I don’t want people to think aww, she’s going through such a tough time and treat me differently because of that” (Sue). An identified inner circle of social contacts was created to keep the condition in and “outsiders” out:
I’ve only told a couple people, and I tend to just keep it short and sweet. But I don’t go to them for help or support or anything like that, it’s just my family who support me. . . I can’t be bothered explaining it to other people and getting others involved really. (Luke)
Though avoidance of social interactions was primarily motivated to reduce feelings of anxiety and embarrassment, the conflicting emotions experienced led to feelings of loneliness and low mood:
It’s weird because I know I need company and I need them around because I’m so isolated and lonely, but I just don’t want the company and want to just wallow in self-pity even though I’m craving people around me it’s such a horrible feeling. It just makes me feel really depressed because obviously I’m just by myself all the time. (Jenny)
Cher also stated contradictory views towards socialising; understanding the importance of social support for mental wellbeing yet being unwilling to receive it. Consequently, this lack of social support led to symptoms of depression.
Lived-relations: Mattering to others
Sense of mattering within lived-relations was connected to physical health condition related restrictions embodied within the lifeworld existential of the lived-body and lived-space. Reflections on mattering included the sense of physical and emotional isolation. Relating the self-to-others and being a burden to others caused participants to question their own sense of mattering, commenting “they’ll be better off without me” (Paul) and expressing the belief that the individual does deem themselves to be “not worthy enough” (Sue) to gain social support. The sense of mattering to others was reflected in John’s interview:
I’d put a downer on things if I’m with them because I’d be taking my time and won’t be able to do some of the things they can do. And I’ll probably start getting frustrated with myself for it and then my mood will be horrible, so I just think it’s better for them if I’m not there. It’s sad but they’d enjoy themselves a lot more if I wasn’t there. (John)
John describes how reduced capabilities have led to him viewing himself as a burden which led to social isolation. Luke states, “I felt like my life was over and I had nothing left to offer and nothing left to do. They didn’t need me anymore. Let’s face it I was useless to them.” The sense of purpose and mattering were apparent and became a prominent theme as the interviews progressed. This feeling is also expressed by Brenda who states:
I was one of those really active mums, but the kids stopped coming to me to play with them. They knew I didn’t have the energy any more for it. I’d watch them in the garden from my chair and cry. I felt so depressed and it’s like I wasn’t really part of the family like I used to me. It would drain my energy even more. (Brenda)
Mattering to others and its impact on lived-relations was present outside the family environment in relation to work related contexts, as stated by Keith:
I didn’t feel like I had a voice anymore. They couldn’t hear me. All they saw was my face. My voice didn’t matter, and I didn’t matter. (pause). I guess I’m just too different to how I used to be. I went from the top of my game, always the one to meet outside of work for a drink and got loads of text messages from them. Now its like a I don’t matter at all. I don’t even bother trying to say anything. What’s the point in saying anything. Might as well keep myself to myself. (Keith)
A sense of mattering to self and others was expressed and experienced through social isolation and mental health difficulties with social support, normally considered a supporting factor in physical illness experienced through a negative lens. The participant’s lived-relations lifeworld was intrinsically linked to their lived-space lifeworld, with distance and barriers characterising their experienced social relations. The constant engagement of reflectivity on self-to-other meanings was experienced as a sense of mattering. Realisations of mattering became a feature of the lived-space and lived-relations lifeworlds and a framework from which the participants characterised, defined and experienced these.
Lived-time: Integration of past, present and future, “Who am I anymore?”
Changes to physical ability brought about practical limitations and through it altered perceptions of the self in relation to the individual’s sense of self (identity) and others (mattering). This latter phenomenon is pertinent to a sense of self, with respect to financial-related responsibilities within the family. In this context matters of mental health are expressed and understood in relation to social situations, the self and job-security. Here, self-identity is understood within lifeworld existential framework in relation to lived-time as self-identity meaning-making is embodied and reconceptualised across past, present and future self-environment interactions and experiences. One participant highlights the embodied experience of self-esteem which is intertwined with their sense of self-identity over time. Self-esteem which is existentially separate to that of self-identity and can be understood in relation to the existential lifeworld of the lived-body. Physical illness challenged individuals’ self-esteem, and sense of self-identity around an active lifestyle, as Luke states:
I just feel a lot less capable and a lot less put together if that makes sense. Which makes me feel like a bit of a failure. . .makes me feel so lazy and like I’m not doing anything with my life anymore and everything is just falling apart. I can’t hold down my job, took its toll on my relationship with my wife and I can’t even hold myself together either. So, I’m also letting myself down because this isn’t who I thought I would be, giving up like this. (Luke)
Participants highlighted the impact of the condition on their sense of self with physical limitations leading individuals to question their own identity. For instance, Cher comments:
Because of how much it’s affected my memory and my concentration and everything I’m not capable in any way. Nowhere near what it used to be like and I honestly hate it. It’s horrible it’s like I’m stuck in an old person’s body (laughs). It’s not mine anymore. (Cher)
This account highlights the fragility of self-identity, characterised by low self-esteem, which is driven by a lack of cognitive capabilities because of the stroke. Here the meaning of self-identity is embodied with the sense of the “I” being stuck within the lived body which is experienced as a stranger to the “I” or self. The disconnect between mind and body and the confinement of the physical self, experienced as spatial restrictedness led to negative emotional reflections of the self and the participants disconnect from their own body and with that their own physical health condition. In a sense the participant physically separated their self-identity from the physical health condition over time. Corporeality was experienced by participants as a lack of self-assurance and coherence for their dissonant body and mind. A similar comment was made by Brenda whose reflections on self-identity were entirely negative due to the MS condition:
Honestly, I’m starting to think of myself as a crippled old woman who isn’t capable of anything, and my confidence has just completely dropped because I don’t know what I’ve got left to be confident about. (Brenda)
This was further echoed in the words of Jenny who stated, “I just wasn’t me anymore.” The change in capabilities led participants to feel incapable with little confidence. Echoed in these words is the sense of a shattered self-identity as identity is intertwined with the limitations imposed by the physical health condition. This was aptly summed up by Keith who said, “I don’t even know who I am anymore, I used to be so upbeat and full of energy. What I’ve become, who is this person?”
Lived-time captures the temporal qualities of the lived experience of the physical health condition which is also embodied in the future self. This is demonstrated in the participants’ reflections of the emotionally laden and mentally taxing phenomenon as they place the self and the experienced phenomenon in the future. For instance, Paul states:
It made me feel quite depressed because I started worrying about my how I would not be able to support my wife and kids and I began to overthink the situation to the extent I would argue with my wife. (Paul)
Present mental health becomes synonymous with physical health and current emotional states including worry, depression and panic are experienced within the experiential process of meaning making as the condition is experienced in the future self. This is further highlighted by Keith who had experienced stroke, “It made me feel quite depressed because I started worrying about my how I would not be able to support my wife and kids.” Here, the embodied present visceral experience of physical health which is captured within the lived-body is positioned and framed as part of the future self and demonstrates the reflective awareness of illness as part of that future self. This also highlights the experiential lifeworld of lived-relations as participants reflect on mattering to others within the future self.
Lived-things: Knowledge, skills and technology
Lived-things lifeworld captured the comprehension of and contributed to transitional changes in all existential aspects of the participant’s lifeworlds, a finding which echoes that of Narushima et al. (2018) within their phenomenological study on lifelong learning in vulnerable old people. The individual’s experience of physical illness within lived-time reshaped prominent tangible and intangible possessions that van Manen (2014) noted as extensions of our bodies and mind. Intangible materiality shaped experiences of mental health support. Within lived-things intangible materiality related to later life learning with improved knowledge and skills, attitudes and sense of self for some participants. However, for others beliefs of an entwined physical-mental-illness cycle framed the experiential qualities of their emotional needs characterised as “inevitable” and served as a barrier to support seeking which becomes unjustifiable. Jack stated that he, “wouldn’t even think of going to someone professional about it cause I’m just bound to go through this side of it so I don’t see the point of it.” This is further discussed by John who states:
I haven’t been to a counsellor or doctor about the emotional side cause I don’t know I just feel like everyone who loses a leg or something it’s inevitable that there’s gonna be an emotional side to it but I just think you’re bound to go through it so just kinda deal with it. (John)
Experiencing delays to support reconceptualised the sense of self in relation to physical illness, with sense of control shaping attitudes towards mental health needs. Access to psychological support was met with frustration and shaped the lived-time and lived-things lifeworlds as Jenny states, “I referred myself to mental wellbeing services, but the waiting list was so long that I was only offered an appointment after I went back to work, nearly a year later.” A similar experience was reported by Cher, “had I got the help I needed earlier on, the period of ill health may not have been as prolonged.”
Existential processes within lived-things shaped experiential meanings of the lived-body and lived-space lifeworlds as physical illness challenged lived-space posing practical limitations to sources of support. Coping mechanisms led to many seeking alternative psychological support services via the use of tangible possessions, namely technology. Tangible possessions were brought into meanings participants made on their own self-esteem and self-identity as immersion within engaging Apps or digital mental health support services took place. This is highlighted by Jack who states:
Apps on my phone helped me to do brain training, mindfulness and of course research about where to get help. Without the use of my phone and internet, my experience would have been far, far worse, as I would have been depending on others to support me where the structures did not exist, only privately. (Jack)
Transitions took place within lived-space as sense of emotional and physical space underpinned the use of digital technologies as support; as Paul states, “The use of technology was also really good way to keep challenging my brain as I was very cut off from things and my instinct was to do nothing.” Jenny gained a sense of empowerment in the ability to challenge herself and gain control over aspects of her mental wellbeing through technology. This was considered more effective than relying on mental wellbeing services as Jenny states, “I took matters into my own hands and used this calm app to help me with my anxiety.” This sentiment was shared by Brenda who reported on the use of another App to support her wellbeing which was held as an embodied experience:
. . .its a good alternative whilst you’re waiting for that appointment which seems like miles away. . . It just helps give you a bit of breathing time and think things through calmly without it building up. So essentially a therapist I guess but an online version and you’re doing it yourself which I think is a pretty good way forward. (Brenda)
The use of Apps to reduce anxiety related symptoms was shared by Sue, “I downloaded this mindfulness app which was good. . . I see how it could help and it did calm me down sometimes and it took me out of those moods at times.” Lived-things were reshaped during experiential meaning-making and indeed lived-things did reshape compensatory changes across the existential lifeworlds. This demonstrates the possibility for technology to act as an alternative to traditional psychological support due to its effectiveness in reducing anxiety and allowing individuals to regain control over their mental wellbeing and mental health.
Discussion
The main aim of this qualitative study was to explore and describe the existential lifeworlds of those with different physical health conditions with particular emphasis on changes to emotions and mental health. Our interpretivist phenomenological approach and application of the lifeworld existentials model proposed by van Manen (1997) within our analysis offers a powerful framework and gateway to the lived experiences of physical illness, and the coalescent bond between physical-mental-illness interactions. Phenomenological insights from experientially based meaning-making describe explicit interacting physical-mental-illness associations and provide greater insight on the mechanisms by which deteriorations to physical health are so often both tangibly and intangibly linked to deteriorations in mental health. Moreover, we reflect on the process driven nature of their interaction when we consider meaning making within van Manen’s (1997) lifeworld existentials model. We discuss the identified existential lifeworlds used by participants to describe lived experiences of physical illness and interpret their relevance with reference to existing literature. We first note the key contributions that our methodological approach yielded in this phenomenological study on the lived experience of physical health conditions and the physical-mental-illness cycle.
The phenomenology of physical-mental co-morbidity was articulated through embodied and emotional encounters with day-to-day life experiences leading to several key findings: 1. van Manen’s Existential Lifeworld Model formed a sound theoretical framework from which to capture and interpret experientially based meaning-makings of physical illness and emotional changes; 2. social isolation was poignant across physical and emotional dimensions shaping existential and embodied experiences in lived-space, lived-relations and lived-things; 3. sense of mattering to others and reflections on self-identity shaped existential lifeworlds and emerged as factors that conceptually linked physical health condition and mental health difficulties; 4. lived-things reshaped compensatory changes across the existential lifeworlds particularly in relation to newly adopted coping strategies as physical illness challenged lived-space, with practical limitations to social activities and support services increasing social isolation; 5. dynamically changing emotions and emotional reflections experienced in the lived-time lifeworld pattern experientially based meaning-making and intertwine with physical health as the visceral experience of physical illness is embodied; and 6. by applying a Hermeneutic Phenomenological Approach we can untangle and gain insight into the complex and dynamic relationship between physical and mental illness.
Lived body: The dissonant body and mind
Meaning-making, in relation to the changed body, emerged through interactions with the environment and situation. Importantly this is positioned within an emotionally loaded experiential process in keeping with Leder (1990) who argued that surroundings are experienced through a particular mood. For many participants sensations of illness within an emotionally loaded situation were intertwined over time, with the experienced physical illness embodied as a visceral experience that then became a core part of the physical-mental-health cycle. The experience of physical illness as an embodied experience was often associated with visceral responses to changes in physicality. This is consistent with the phenomenological study by Coventry et al. (2014) who report the role of visceral responses within mental-physical multimorbidity. That participants displayed symptoms of depression and anxiety following the physical health condition is consistent with the literature (Barnard et al., 2006). Participants also experienced reduced self-esteem and self-identity as emotional reflections were experienced in lived-time. Although there is little research around the interaction between physical illness and self-esteem, previous studies have highlighted a correlation between them (Nosek et al., 2003; Sowislo and Orth, 2013). Miyahara and Piek (2006) stated individuals with minor disabilities were more likely to display low self-esteem in relation to physical competence, while those with major disabilities do not. As in other studies (Paz et al., 2017) findings show low self-esteem hindered social interactions leading to social isolation.
As was seen in the participants outlined by Groven et al. (2017) the lived experience of physical activity for those participants in the current study involved a sense of being capable and involves a sense of joy and awareness of their opportunities expanding into lived-space and lived-relations. It is framed by participants in their experience of the physical health condition to divide a prior “normality” and “normal” state from their current “abnormal” and different bodily state. Changes to the lived-body lifeworld as experienced in various settings and situations creates an ongoing change of embodied meaning-making and sense-making supporting the theoretical framework from which the current study is based (see Johnson, 2007; Merleau-Ponty, 2002; Merleau-Ponty et al., 2013).
Lived-space: Physical and emotional boundaries for risky social relations
Changes to lived-space were often entwined with lived-relations, characterised along physical and emotional dimensions. Participants avoided social activities, driven by physical capabilities and the emotional load of socialising. This shaped the lived-space lifeworld as the experience of physical illness is embodied across social space with social isolation and emotional isolation core in shaping the individuals’ lived-space. The association between physical health and social isolation is prevalent, for example, Andelic et al. (2010) found that 33% of physically injured patients displayed major difficulties with social integration that leads on to social isolation. Consistent with the literature (e.g. Baek, 2014; Matthews et al., 2016) social isolation was often self-generated, resulting in low mood and symptoms of depression. Moreover, social isolation and depression have an interactive effect that perpetuates the cycle (Mucci et al., 2020). Social isolation creates a barrier between individuals and critical social support, compromising wellbeing and mental health and consequently reinforcing self-isolation.
That participants engaged in social activity less now, since their physical condition, than they did pre-condition is less important to our phenomenological approach than the meaning of such activities from the reality of those engaging in them. How participant’s experience physical and social activities and construct meaning around these is central to gaining insight into the interactive nature of the physical-mental-health cycle. By situating the embodied experience of physical health within van Manen’s existential lifeworld model we draw on the phenomenological insights of the participants’ existential lifeworlds that give meaning to their physical health. More pointedly this approach allows greater insight into the physical-mental health interactions by drawing on the theoretical insights of others, for example, Johnson (2007), Leder (1990) and Groven et al. (2017) whom situate the emotional state experienced as a dynamic and subjectively changing process of reflection in which emotionally loaded and experiential meaning take place and in which past, present and future intertwine.
Lived-relations: Mattering to others
Mattering to others involves viewing ourselves as a significant part of the world, where we perceive that others care about us, would seek advice from us and be distressed at our demise (Elliott et al., 2004; Rosenberg and McCullough, 1979). Feelings of not mattering to others can have a detrimental impact to mental health, being linked to depressive symptoms (Taylor and Turner, 2001) and suicidal ideation (Elliott et al., 2005). Mattering to others is positively related to self-esteem and psychological well-being (Marshall, 2001; Rosenberg and McCullough, 1979). Importantly mattering has been explored in relation to physical illness, such as cancer (Davis et al., 2019). We found that the sense of no longer “mattering” in physical illness was an embodied experience with feelings of depression, low mood and self-isolation emanating from this. Spatial boundedness and changes to lived-body experience were integral to sense of self-to-other-relations. Furthermore, self-identity was articulated through mattering to others and their role in lived-relations within family and work-based settings, playing a key role in mental health difficulties. This parallels the phenomenological work of Strauss (1976) suggesting self-identity experienced through lived-relations is embedded within the bodily basis of chronic illness. Participants developed a heightened sense of mattering to others, primarily family responsibilities, raising feelings of anxiety due to physical health limitations. Anxiety was largely attributed to job insecurity due to restricted capabilities, a finding which is consistent with other literature (Max et al., 2011; Ownsworth and McKenna, 2004). Our study revealed further insight into this association showing that the sense of mattering influenced emotional changes in relation to job insecurity.
Lived-time: Intergration of past, present and future, “Who am I anymore?”
Self -identity became experienced over time as a process of reflection and introspection with self-identity experienced as a dynamic and subjectively changing process in which self-other-relations became defined and adapted. The experiential meaning of the self and the individual’s sense of self-identity were reshaped and redefined as the sense of self was situated over time and space. The past, present and future self are entwined in a dynamic and subjectively changing process of reflection and the changing sense of “I,” which is aptly captured by one participant who questioned, “Who am I anymore?” Disruptions to ontological security impairs self-identity (Bury, 1982) and the physical illness imposed limitations that challenged self-identity preservation (Charmaz, 1995). Whilst the aim of phenomenological inquiry is not to generate hypothesis against which can be tested, one can only wonder whether resolution of the self-identity is a prerequisite to successful social relations. In the sense that solidification of a positive self-identity might enhance a sense of mattering to others (and the self), as well as levels of social engagement, transforming the spatiality of physical health as it is experienced within the lived-space lifeworld.
Lived-things: Knowledge, skills and technology
Explicit recognition of a physical-mental-illness interaction and associated emotional changes experienced through physical illness was voiced by participants. In addition, participants report barriers between self- and others, both physically and emotionally. Lack of support provision identified within the study concords previous research, showing dissatisfaction with the psychological support received (Owens et al., 2002), and lack of communication between medical professionals who treated physical and mental health conditions as distinct and separate conditions rather than intertwined (Pickelsimer et al., 2007). Often participants resorted to digital technologies as a means of accessing psychological support and found digital technologies including Apps to be effective in reducing mental health symptoms such as anxiety. The use of Apps for their intended purposes is constantly evolving (Bakker et al., 2016; Torous et al., 2014). Further insight is needed regarding how these technologies can be tailored to meet individual and patient population needs including physical illness. Our findings revealed that coping strategies were considered upon mental health difficulties being experienced rather than a proactive preventative approach.
Methodological evaluation
The emphasis on fluid dialogue to establish narrative within the interview was encouraged. Our epistemological basis, stemming from hermeneutic phenomenology drew on that of van Manen (1997) which offers the theoretical framework of lifeworld existentials as a lens through which to explore this lived experience. In doing this insight into experientially based meaning-making of physical illness was gained. Findings highlight the relevance of lived-body, lived-space and lived-human-relations within our interpretive (hermeneutic) phenomenological methodological approach which are intertwined within the ideographic narratives and across themes.
Our hermeneutic phenomenological approach provided a meaningful framework from which to explore the experientially based meaning-making of physical health as demonstrated in the use of semiotics by participants themselves. For instance, within participants’ lifestory, Cher’s experienced physical health condition shows use of metaphor to describe the experience as a “battle,” something which she refers to again in describing the experienced physical illness of stroke. Such metaphor is present in the experiences reported by other participants (e.g. where Sue recounts the physical illness as experienced “behind closed doors”). This suggests that participants engage in a natural process of hermeneutics, interpreting the “texts” of their own life as it is experienced. In this way, the participant experiences the physical illness within their own linguistic reflections which becomes part of the phenomenon itself. This aligns to Heidegger’s (1962) hermeneutic phenomenology which posits that prepositions or pre-understanding are part of being. It is also concordant with van Manen’s hermeneutic phenomenology (van Manen, 2014), as van Manen states, “phenomenology describes how one orients to lived experience, hermeneutics describes how one interprets the “texts” of life, and semiotics is used to develop a practical writing or linguisitic approach to the method of phenomenology and hermeneutics” (van Manen, 1990, p.4).
Within the context of van Manen’s Hermeneutic Phenomenological Approach (van Manen, 1990, 2014, 2017) we wonder about the world of the participant’s ordinary experience with the aim to grasp the phenomenon. If we consider the account of the lived experience voiced in the narrative of `Paul, who experiences asthma and arthritis, Paul describes an emotionally loaded phenomenon which we can refer to in the findings of lived-body. Meaning-making is embodied, and the past and present intertwine within an emotionally loaded context. The past is described positively (e.g. “amazing feeling,” “getting out all my frustration and energy”), and the present is experienced as a dynamic process from their pre-reflective sensations to reflective awareness of illness, concordant with the theoretical framework of Sartre (2003) and Toombs (1993). We encourage phenomenological enquiry to encapsulate a broader, dynamic approach to phenomenological research that is sensitive to shifting levels of reflective awareness from pre-reflective reception of sensations to reflective awareness of illness. We demonstrate this can be done within a Hermeneutic Phenomenological Approach. Using the current methodological approach, we gain a deeper insight into the lived experience of the individual as experienced in situations and activities transcending the confines of time. Moreover, we highlight the utility of the Hermeneutic Phenomenological Approach in our findings which demonstrate the use of metaphor to describe the emotionality of the lived experience of physical illness and mental illness (e.g. “behind closed doors” metaphor). In addition to this is the loss of words to describe the experienced phenomenon and associated sequelae, which is described by participants in their sense of not knowing how to describe their emotional reflections or the experienced phenomenon. This characterises an ineffable state within the process of meanings-made in the embodied experience and encompasses an experience that cannot be fully captured within a traditional dialogue form of enquiry. This perhaps borders the edge of qualitative enquiry as a methodological approach to explore the lived experience of physical and mental illness; however, using a Hermeneutic Phenomenological Approach we were nonetheless able to highlight its existence as a component of physical and mental health. Given this finding, the methodological approach could be extended further utilising none-dialogue based approaches, primarily creative forms of expression, such as the visual arts (Goble, 2016; Gupta and Zieske, 2024) to fully explore the phenomenological experience of physical and mental health and in particular the cyclical self-perpetuating nature in which they exist. This combined approach has been used previously to explore trauma related events, including the experience of pregnancy loss (McMorrow, 2024), and offers a promising direction for further investigation of the current research aims and indeed those trauma related phenomenological experiences that induce the sense of the ineffable.
Conclusion
Findings show the utility of a hermeneutic phenomenological approach to explore the complexities of living with physical illness and the phenomenology of bodily and emotional dimensions of their existential lifeworlds. The observed relationship between physical and mental health highlights the need for a more holistic approach to health care plans that can support experiential qualities of emotional change. This may include potential applications for the integration of accessible technologies to cope with experienced mental health needs. Our findings contribute to a greater understanding of the mechanisms through which people cope with physical illness to support their mental health and wellbeing. Findings showed that loss of capabilities and the subsequent change in lifestyle accompanying physical illness influenced internal cognitive reflections on self-identity and mattering to others through lived-relations and can be harnessed with tailored intervention strategies to support positive experiences of their lived-relations.
Footnotes
Acknowledgements
This research was conducted with the support of Edge Hill University whose resources and governance were crucial to the study. The authors would like to offer a personal thanks to the participants for their time and engagement in the study.
Ethical considerations
Ethical approval for the study was granted by the Institutional Research Ethics Committee
Consent to participate
Informed consent to partake in the research was provided by all participants.
Consent for publication
Informed consent for publication was provided by the participants.
Author contributions
Both authors contributed to all aspects of data collection. Author JP was responsible for study conception, study design, methodological design and procedure, analysis, interpretation of findings and discussion, and the development and production of the manuscript and revisions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Transcripts are not publicly available due to restricted permissions granted by participants.