
Abstract
Food allergy (FA) related distress is common in patients and caregivers, however, there is little funding for psychological support within allergy clinics. As part of the Global Access to Psychological Services for Food Allergy (GAPS) study, we explored adults’ and caregivers’ experiences with healthcare services in the UK and their FA-related psychological support needs. Semi-structured interviews were carried out with 22 adults with FA and 14 caregivers of children with FA and analysed using template analysis. Three themes were constructed from the data: “Road to diagnosis and getting past the gatekeeper,” “Support for managing FA inside and outside the healthcare system” and “The need for a holistic healthcare approach.” There is need for greater understanding of FA, particularly within primary care. Access to psychological services within the multidisciplinary healthcare allergy team would provide patients and families with the holistic care they require and reduce the need for costly private services.
Introduction
Food allergy (FA) is an immune-mediated reaction to food which is associated with notable adverse impacts on quality of life and mental health, due to anxiety related to managing this condition. FA is a public health issue and affects an estimated 3%–10% of adults and up to 8% of children worldwide (Warren et al., 2020). The Global Access to Psychological Therapies for food allergy (GAPS) study showed that across more than 20 countries, between 70% and 80% of adults and caregivers report psychological distress related to FA. However, less than 20% reported being able to access psychological support (Knibb et al., 2024a). There were significant differences across countries in relation to reported distress and support received, with the United Kingdom (UK), Canada, Australia and Brazil having high proportions of participants reporting distress compared to countries such as France and Germany. It is unclear why these differences exist, but these may be due to different health care systems, knowledge about FA or media attention focussed on FA-related deaths.
The GAPS study reported that the UK is one of the countries with the highest percentage of participants reporting FA-related distress and the lowest level of psychological support accessed (Knibb et al., 2024a). The UK benefits from the National Health Service (NHS), which provides healthcare freely at point of access (which is paid for through national insurance). Ordinarily, patients access primary care physicians first if they have health-related concerns and can be diagnosed by their General Practitioner (GP) or can be referred by their GP to secondary care hospitals. Unfortunately, allergy knowledge in primary care has been reported as suboptimal (Cabrera et al., 2024) and allergy training has only been included in the UK curriculum for doctors training to be GPs since 2019 (Collinson et al., 2023). A lack of understanding and knowledge can hinder recognition of FA and referral to specialist care. Although the UK has seen a fourfold increase in paediatric allergy clinics over the last 15 years, services are still small and there is considerable variation across the country regarding availability, resulting in long waiting lists for FA diagnostic tests in some areas (Wells et al., 2022).
There is also a recognised unmet need for psychological support for FA (Knibb et al., 2019). A recent survey found that psychologists across the UK working in allergy spent on average only 6 hours a week with FA patients and very few had a workload that was specifically for allergy (Knibb et al., 2024b). Healthcare professionals recognised the importance of psychologists and would like to refer more patients, but barriers such as funding and clear referral pathways hindered this. Indeed, in the global survey run by the GAPS study, cost was the biggest barrier to accessing psychological support across almost all countries surveyed (Knibb et al., 2024a).
In order to explore experiences with healthcare for FA and psychological support in more detail, interviews with adults and caregivers have been carried out as part of the GAPS study. Due to the high proportion of participants from the UK reporting FA-related distress and difficulties in accessing clinical care or psychological support, we present findings here from interviews in this country. The aim of this part of the GAPS study was to explore the healthcare services accessed by adults with FA and caregivers of children with FA, how (un)helpful these services were, and to identify any unmet care needs.
Methods
This study was given a favourable ethical opinion by Aston University Research Ethics Committee (REC approval number 1819).
Participants and recruitment
Participants were recruited as part of GAPS, a large multi-phase international study examining the psychological health experiences and needs of patients with FA and caregivers of children with FA. Participants reported here were recruited from the UK via adverts from patient organisations and placed on social media. Adverts contained a link to a participant information sheet and an expression of interest form. The form asked for contact details and included questions to check that participants met the following eligibility criteria: (1) adult aged 18 or over; (2) they/their child had a diagnosed FA by a medical professional; and (3) for caregivers only, their child with FA was aged 17 or younger. Participants who met the inclusion criteria were sent a link to an online consent form and a short questionnaire asking for demographic and FA information. An interview date and time was then arranged.
We aimed to recruit 15–20 adults with FA and 15–20 caregivers, although this was flexible as data generation was informed by the principle of “informational power” which prioritises generating information-rich data with the fewest number of participants (Malterud et al., 2016).
Data generation
Semi-structured interviews with adults with FA and caregivers of a child(ren) with FA were conducted between March and August 2022 by four research assistants (one male and three female) trained in qualitative methods. One interviewer was a clinical psychology doctoral trainee, two were conducting interviews for their research project for their MSc in Health Psychology and one for their MSc in Allergy. An interview schedule was devised in advance informed by the extant literature, the expertise of the research group and the findings from the GAPS survey (Knibb et al., 2024a), which showed that FA-related anxiety was a common cause of distress, but few participants had been able to access psychological support. Interview questions explored the impact of FA on daily lives, participants’ access to and experience of support for managing FA from different healthcare professionals (including general practitioner, psychologist, nurse specialist, dietician), unmet care needs and how support could be improved. Consistent with semi-structured interview guidance (Kvale, 1983), the schedule guided conversation and included prompts, but was applied flexibly to allow for follow-up questions to unexpected responses that were broadly related to the topic of interest (see Supplemental File).
Participants knew the aims of the research, there were no relationships between interviewers and participants prior to research commencement and participants understood reasons why interviewers were carrying out the research, including if it was part of their MSc programme. Interviews were conducted online using Microsoft Teams or Zoom and lasted between 10 and 60 minutes (median = 29 minutes; mean = 31 minutes). Field notes were made and interviews were also audio recorded, transcribed verbatim with identifying features removed (e.g. references to names, people, places), and stored securely in line with data protection laws. No participants had anyone accompany them in the interview. To thank participants for their time, each received a £10 e-voucher. All participants were debriefed and advised they could withdraw at any time during the interview and up to 14 days afterwards. No participants withdrew. Participants were assigned pseudonyms which are used throughout.
Data analysis
Data were analysed using Template Analysis (Brooks et al., 2015) by CR, an experienced qualitative researcher (PhD) with expertise in health and illness experience and RCK, a Health Psychologist and expert in FA. CR read all interview transcripts with adults living with FA and selected three, which captured a range of participant characteristics, for which CR and RCK then performed preliminary coding. Three topics served as tentative a priori themes to organise the original template and guide analysis: (1) the psychological impact of living with FA; (2) what support had been provided and accessed and the perceived utility of the support(s); and (3) how support could be improved. After preliminary coding, meaningful clusters were identified and discussed, and an initial coding framework was agreed upon. CR applied the template to five more transcripts, any modifications or additions were made and agreed upon before it was then applied to the full data set for adults living with FA.
This coding template was used by CR to carry out preliminary coding on eight caregiver interviews. The template was iteratively refined to ensure it captured the breadth and depth of caregiver experiences. The modified template was discussed and agreed with RCK, and CR then applied it to the full data set for caregivers. No new themes to add to the template were identified during this process. Results of the analysis for adults and caregivers were then synthesised and all themes with supporting quotes were discussed and agreed upon by the study team. During the analysis CR completed a reflexive diary, and the development and agreement of the framework and team discussions ensured individual researcher perspectives were taken into consideration. The following results report on two aspects of the analysis: the provision, acceptability and perceived utility of the support; and improvements to support.
Results
Fourteen caregivers and 22 adults with FA took part. The majority of caregiver participants were White (76%) female (88%), had an undergraduate degree or higher (71%) and a child with FA who was aged 5–10 years at the time of interview (59%). Most children had multiple FAs (82%) and had one or more related medical comorbidities such as asthma, eczema or hay fever (76%). However, most did not have a history of anaphylaxis (59%). Similarly, the majority of adult participants with FA were White (82%), female (73%), and had an undergraduate degree or higher (82%). Most reported multiple FAs (81%), with half diagnosed during childhood (50%). The majority of adult participants had a history of anaphylaxis (81%), but 62% had no allergic reactions in the past year.
We identified three main themes from the interviews. The first, “Road to diagnosis and getting past the gatekeeper” captures participants’ experiences having their child’s or their FA diagnosed. The second theme, “Support for managing FA inside and outside of the healthcare system” discusses how participants managed FA and their experiences with healthcare. The third theme, “The need for a holistic healthcare approach” discusses the current gaps in care for FA diagnosis and management, and participant suggestions for how services and support could be improved.
Theme 1: Road to diagnosis and getting past the gatekeeper
Participants described the journey to diagnosis to be arduous and frustrating, and by its nature, necessitated the involvement of multiple healthcare professionals. Caregivers frequently characterised GPs as “gatekeepers” to the specialist allergy care required to diagnose and manage their child’s FA. A minority of caregivers, such as Tabitha, reported positive encounters with their child’s GP, where “they were very quick on it” and supported them “in terms of finding what he’s allergic to and doing skin tests.” However, the majority explained their child’s GP had little input into the diagnostic process, either because their GP quickly referred them to an allergy clinic or because the caregivers had paid for private care, thereby bypassing the NHS waiting lists and referral processes altogether. These participants framed private care as a necessity “because the provision on the NHS is so inadequate” [Brenda]. Criticism largely rested on the idea that “although GPs are going to have a good understanding, it’s not their specialism” [Lucas], or else there was a lengthy waiting time for services, “had we waited for the NHS, I think it was six months (. . .) I think our outcome would have been hugely different” [Aaron].
A number of caregivers explained that they were perceived by their GP to be over-reacting or misinformed. As Jennifer described, “[the GP was] really patronising, ‘oh, mum this is all normal you know, babies do get constipated, babies have reflux, and they do cry.’” Aisha reported feeling dismissed by her GP who “came across very flippant and very kind of unconcerned” about her child’s allergy. This inflexibility and lack of person-centred care was challenging for caregivers, who felt there was little recognition of the emotional and psychological impact that caring for a child with FA has upon them.
Adults with FA reported not being taken seriously by their GP or other healthcare professionals, or reported they received no medical or psychological support to manage their FA from their GP. As Sarah stated, “it was, ‘you’ve got anaphylaxis, here’s some EpiPens®, bye’. There was absolutely no support over it, not even telling you what you have to do, how to use the pens. We’ve got nothing.” Others reported receiving “faulty” advice from their GP regarding reintroducing allergens into their diet as they mistakenly believed they were no longer allergic to food. As Daniel said, “rather foolishly I decided to eat a bag of mixed nuts because I was told everything was fine and yeah then I had a really bad reaction to it.” Both adults and caregivers strongly endorsed the need to provide more comprehensive education for GPs relating to FA to ensure their advice was grounded in current research, and most felt their care would be improved if an annual appointment with their GP about their FA were introduced.
Theme 2: Support for managing FA inside and outside of the healthcare system
Participants reported support with FA management mostly centred on avoidance of allergens and use of emergency medication. However, for caregivers in particular, there was a sense that information provision for supporting management of their child’s FA was incomplete and precipitated them to do, “a lot of my own research and even then, I have struggles” [Rachel] to supplement and contextualise the information provided by healthcare professionals. Some caregivers, such as Jemma, had been given conflicting information that had compounded their pre-existing anxiety and guilt about their child’s FA and prolonged their child’s suffering, “[the consultant said] everything that everyone had told me to do, he said it has all been done so wrong.”
The focus on medical management was useful for some adults with FA, but for others this merely confirmed what they already knew and did not meet their need for more emotional and psychological support, as Andrea reflected, “in terms of any emotional support there wasn’t anything at all there and if anything, I felt stupid and like I was wasting their time and yeah it was absolutely no help at all.”
For the few adult participants who sought therapy, either through the NHS or privately, accessing the right type of psychotherapy was a considerable challenge. Andrea explained she had been referred to receive Cognitive Behavioural Therapy (CBT) which misaligned with her needs, “I just didn’t feel it helped and I’ve done CBT before for other things like stress with work and I understand it, I understand how it works but it just didn’t work for me.”
When considering psychological care to support FA management, caregivers of children of all ages had observed anxious behaviours in their child and expressed concern for their child’s psychological wellbeing. There was very little support for this, “they haven’t given us any help, we’ve asked for stuff, but I don’t know whether that’s because they think he’s not old enough, or whether they think he doesn’t fit the criteria, or they think it will sort itself out?” [Amber]. Brenda explained it was through the asthma clinic “which was much more supportive [than the FA clinic]” that her child had been able to access a psychologist to help them understand and manage their health anxieties, which had “made a profound difference to her.” However, Brenda had also “sought support for her independently from psychologists, but there’s very few that understand allergy.” To effectively support people living with FA, there was a strong feeling that psychological support must be tailored to meet their unique FA experiences and needs.
When seeking support for themselves, some caregivers, such as Lucas, questioned how useful psychological support would be for them, “I don’t know what sort of difference it would make. You know, there’s nothing they can do (. . .) so I don’t know of how much benefit it would be.” Caregivers who were able to access psychological support did so by paying privately and were full of praise for the support they received. Melissa and Aaron had paid to see a psychologist to better cope with the anxiety of caring for a child with FA. Aaron explained that over the course of several months his therapy sessions provided him with “a light bulb moment when suddenly some of this stuff clicked” which “really just helped me see end-to-end and I’m like ‘right now I get it’.”
Although few caregivers had been able to access psychological support, most caregivers endorsed greater access. Megan, for example, explained that the trauma of her baby being hospitalised continued to trouble her, “I do think there is a trauma from witnessing that event. So, there’s definitely a lot to unpack and work through and I think I could probably do with you know the help of the psychologist.” Participants were passionate that specialist psychological support should be made available for people living with FA.
Theme 3: The need for a holistic healthcare approach
Caregivers and adults with FA wanted psychological support to be embedded within a suite of support services from the point of diagnosis, “I think you should be automatically offered psychological help as well as the tests etc.” [Andrea, Adult]. Adults with FA implied that having early access to listening support and guidance for coping with FA may have ameliorated or even prevented their anxieties around food, “being able to talk to somebody about coping with it, how to cope with it, you know, living your life would just, I think would be so much better” [Heather]. More specifically, both adults with FA and caregivers endorsed psychological support with a specialist in FA and/or health anxiety as being potentially the most valuable but presently largely inaccessible care.
The need for specialist psychological support for FA was most vehemently argued by those who had previously accessed generic psychological support and who noted, “the only kind of drawback was it obviously wasn’t specialised; they weren’t specialised in allergy anxiety. So, I felt like there was limited help I could get in that aspect” [Olivia, Adult]. For caregivers, there was hope that mental health support could provide a “toolbox of coping mechanisms” [Brenda] that protects not only their wellbeing but also potentially extends to protect the child, “how to make sure you don’t pass anything on to your child or how to bring them up in a way that we’re confident about manage managing it, and they’re not too sad about their allergies, and they just accept it” [Amber].
Participants were cognisant of the pressure the NHS was under and were therefore cautious about assigning blame to an individual person or being seen as unnecessarily contributing to an already “overwhelmed system” [Megan]. Nevertheless, it was evident that some participants’ unmet needs stemmed from having insufficient time with their healthcare professional because the system is so stretched. For example, Rosie [adult] stated, “I don’t have enough time to sit with anybody and ask questions and like I’m given results but then no one can explain to me what I do next.” Rosie had struggled to get the support she needed, and despite being repeatedly referred to different specialists, the extent of her FAs and how she might manage them remained unclear. She therefore wanted to see connected multidisciplinary services and support systems in the future.
Each participant provided ideas for new or improved services and resources based on their own lived experience of FA and personal preferences (summarised in Table 1). While a small minority of participants favoured in-person support, the vast majority were amenable to online support and information, pragmatically arguing it would be more accessible and better serve their needs, “any online support if that kind of thing existed that would be great, I suppose for me that would actually be better for me because my time is limited” [Andrea]. Moreover, there was consensus that living with FA was a unique experience and flexible services that could be adapted to personal needs and demands were emphasised.
Participants’ “wish list” of services, supports, and resources to improve FA management.
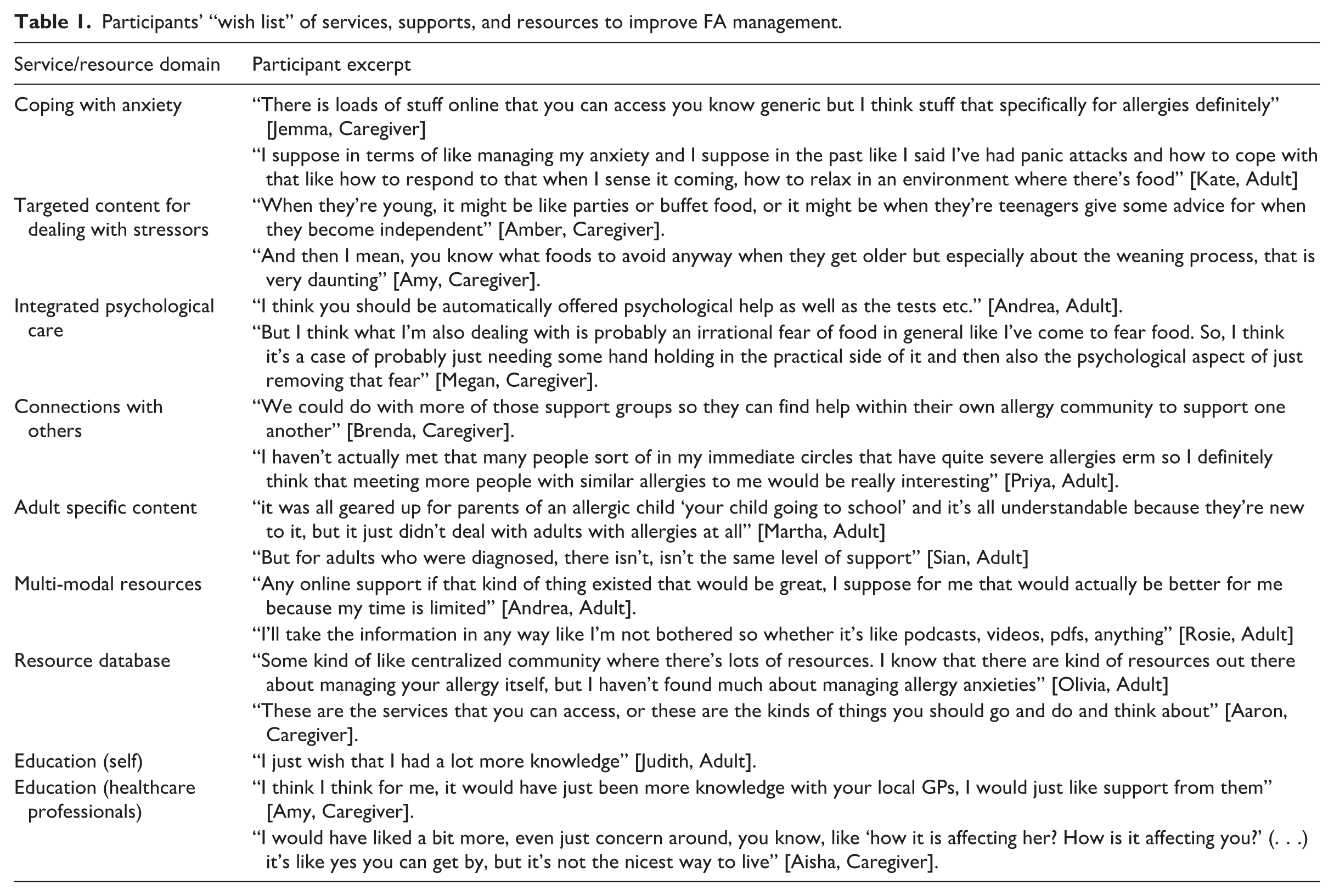
Caregivers and adults with FA recognised the importance of education; for themselves, healthcare professionals, and the public. Indeed, fact sheets and guidance documents of all descriptions were discussed, from how to recognise allergic symptoms to understanding and navigating risk, and how to have discussions with friends, family, and educational institutions about FA. Ultimately, participants wanted their struggles and unmet needs to be recognised.
Discussion
This study explored the healthcare experiences and psychological support needs of adults and caregivers managing FA. The impact of FA on the quality of life and mental health of patients and caregivers is well established (Golding et al., 2021, 2022; Westwell-Roper et al., 2022), but the experiences of support from healthcare providers regarding diagnosis and management of FA is less well known. This study is the first to provide an in-depth understanding of those experiences, identifying where support may be lacking and what patients and caregivers would like to see improved. The three themes discussed here illustrate the challenges patients and caregivers faced in getting a diagnosis and having the impact of FA on their lives recognised by primary care physicians, the lack of psychological support within secondary care, the need to look outside of their healthcare team in order to find the help they needed, and the plea for a holistic approach to healthcare, where their needs can be addressed without recourse to costly private care.
The first theme highlighted the lack of knowledge and understanding of FA within primary care and that on occasion doctors could be dismissive of the experiences discussed by their patient. Dismissal of concerns of caregivers by healthcare providers has been reported as often occurring in paediatric primary care settings, with concerns mostly relating to the child’s physical health (Tager et al., 2023). Adult patients with other long-terms conditions such as chronic back pain have also described feelings of dismissal and discouragement, particularly where healthcare practitioners use generic reassurance or do not communicate effectively (Braeuninger-Weimer et al., 2019). Good communication between patients and doctors is an important aspect of quality healthcare and can enhance shared decision making, improve patient satisfaction and patient outcomes (Street et al., 2009). This is particularly important when discussing a potentially life-threatening condition such as FA (Abrams et al., 2020).
A lack of knowledge regarding FA in primary care has been identified in the literature as a barrier to timely diagnosis and support with FA management (Cabrera et al., 2024). Some of the adults in this study had been diagnosed as children, when knowledge regarding FA was arguably much poorer than at present. The addition of allergy education to the curriculum for doctors training to be GPs in the UK may benefit patients presenting with allergy symptoms and reduce the instances of faulty advice reported in this study. However, the need to recognise the emotional impact FA has on people’s lives still needs to be acknowledged and enquired about during a primary care consultation.
The lack of perceived support from healthcare was discussed by adults and caregivers, with adults in particular emphasising the limited support they had been able to access to help them manage food allergy as an adult. This led some participants to seek out their own information, particularly via internet searches. Although there are trustworthy sites such as those run by patient organisations, there is considerable misinformation regarding FA and its management available for people to access. Having a supportive and knowledgeable primary care physician could reduce this risk. Having to navigate the healthcare system was obviously a burden for both adults and caregivers. This has been reported for other long-term conditions such as cystic fibrosis and kidney failure, with caregivers experiencing frustration over inconsistent communication, lack of proactive support or personalised care (Missel et al., 2025).
A lack of support regarding the emotional impact of FA could result in psychological issues not being addressed in a timely way. Early intervention for FA anxiety and worry is necessary in order to optimise quality of life, minimise adverse impacts on mental health, and mitigate greater intervention at a later stage (Knibb et al., 2024c). Anxieties around food allergy in caregivers can also transfer to the child (Polloni and Muraro, 2020) and so it is important to ensure support is given when needed. Some participants resorted to paying for support privately, but this is not something that is in financial reach for all, resulting in inequalities in the care people receive. Cost has been identified as one of the biggest barriers to accessing psychological support across many countries (Knibb et al., 2024a).
A lack of knowledge was not just confined to primary care physicians but also to psychologists. FA is not included in any curriculum for clinical or health psychology training and a lack of knowledge of the condition can hamper appropriate tailoring of therapy. A recent survey of psychologists working in allergy clinics in the UK showed that most learning about FA occurred “on the job” and from colleagues and few had received any specific training (Knibb et al., 2024b). When accessing psychologists privately, it can be difficult for patients to find someone with appropriate knowledge regarding the impact of FA and how that can be managed in a therapeutic way. Training in the psychological impact of FA and relevant therapeutic techniques should therefore be made available for psychologists, in addition to clear referral pathways. The evidence for effective therapies for FA is growing, with a recent systematic review showing promise for Cognitive Behavioural Therapy. The review advocates a stepped-care model of therapy depending on the complexity and level of difficulties experienced by the patient (Knibb et al., 2024c).
The need for more holistic healthcare is therefore extremely important and is something participants in this study felt was needed. They suggested that a psychologist should be included in the multidisciplinary allergy team, which would ensure timely and knowledgeable advice and support regarding managing their or their child’s FA. Participants also expressed a desire to have access to support in other ways, such as online materials. The next stage of the GAPS study aims to address these needs by creating an online support tool to help adults and caregivers manage FA-related anxiety and the impact of FA on day-to-day life.
This study has some limitations to consider. The majority of participants interviewed were well educated White British women. Although proportions in terms of ethnicity may be similar to the UK population (England and Wales Census, 2021), experiences discussed here may be different compared to people from different ethnic or socio-economic groups. All participants were recruited through patient organisations which may have introduced some selection bias. Individuals with FA who engage with such organisations may have different experiences with healthcare to those who do not. Although we had rich data from the interviews, adults in our sample had less experience of clinical or psychological care for their allergy than caregivers and so their discussion focussed more on the lack of support. It would therefore be useful for future research to recruit adults from clinics in order to explore their experiences in more detail. We focussed specifically on the UK for this paper, particularly due to the high levels of distress and low levels of support reported from the UK. Experiences of these participants might be different compared to those in other countries, with different healthcare systems. Analysis of interviews in other countries carried out as part of the GAPS study is ongoing and it will be of interest to see if experiences are different in GAPS participants from other parts of Europe, USA, Canada, Australia, or Brazil.
Although focussed on the UK, our findings provide guidance for any healthcare practice. With FA affecting up to 10% of the population globally (Warren et al., 2020), it is important for any primary care physician to have up-to-date knowledge about FA but also understand how it can affect the mental health and quality of life of patients and caregivers. In the UK, the GP with extended role (GPwER) training is now available for allergy through the Royal College of General Practitioners and should be considered. The need for trained psychologists who can work within allergy clinics is also clear, which could be provided by bespoke professional development modules offered through professional bodies. In order to reduce health inequalities, access to low cost or freely available support to address the impact of FA on mental health is needed. It is hoped that the online support tool being developed as part of the GAPS project may go some way to address this deficit in psychological support.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261429012 – Supplemental material for The healthcare experiences and psychological support needs of adults and caregivers managing food allergy
Supplemental material, sj-docx-1-hpq-10.1177_13591053261429012 for The healthcare experiences and psychological support needs of adults and caregivers managing food allergy by Caity Roleston, Jennifer L. P. Protudjer, Linda J. Herbert, Christina J. Jones, Chris Warren, Helen A. Brough, Mahboob Miah, Nicola O’Donnell, Hodan Omar, Wendy Ennifer, Mary JaneMarchisotto and Rebecca C. Knibb in Journal of Health Psychology
Footnotes
Ethical considerations
This study was given a favourable ethical opinion by Aston University Research Ethics Committee (REC approval number #1819).
Consent to participate
All participants gave written informed consent.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
Study concept and design, RC Knibb, LJ Herbert, CJ Jones, JLP Protudjer, HA Brough, C Warren, MJ Marchisotto; Data collection, RC Knibb, N O’Donnell, Mahboob Miah, Hodan Omar, Wendy Ennifer; Analysis of data, C Roleston, RC Knibb; Interpretation of data, all authors; Drafting of the manuscript, C Roleston, RC Knibb; Critical revision of the manuscript for important intellectual content, all authors. All authors approved the final version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Aimmune, Novartis, National Peanut Board and European Academy of Allergy and Clinical Immunology.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RCK: research funding from the National Institute for Health Research, Aimmune, National Peanut Board, Novartis and the Food Standards Agency and honoraria from Nutricia, Viatris, Stallergenes Greer and DBV Technologies. RCK is also Chair of the British Society for Allergy and Clinical Immunology Psychology Special Interest Group for Psychology. JP: Section Head for Allied Health, and Co-Lead, Research Pillar, for the Canadian Society of Allergy and Clinical Immunology; sits on the steering committee for Canada’s National Food Allergy Action Plan, and reports consultancy for Ajinomoto Cambrooke, Nutricia, Novartis and ALK-Abelló. HB: research funding from the NIH (NAIAD) and speaker honoraria from DBV Technologies, Stallergenes Greer, Viatris and (NICE) National Institutes for Health and Care Excellence. MJM: sits on the National Peanut Board Food Allergy Advisory Council and reports consultancy for Novartis. CJJ: research funding from the National Institute for Health Research, the Food Standards Agency and Innovate UK, and honoraria from the National Institute for Health Research, Mead Johnson, Nutricia, and Allergy UK.
Data availability statement
Data is not available due to ethical considerations.
Supplemental material
Supplemental material for this article is available online.