
Abstract
This scoping review aimed to map current research on guilt, shame and self-perceived burden among older adults with multiple long-term conditions (MLTCs). The review followed the Joanna Briggs Institute’s (JBI) scoping reviews guidelines. Systematic searches were conducted in six databases. Paired reviewers independently screened titles, abstracts and full-texts, using pre-defined inclusion and exclusion criteria. Relevant data were extracted and reviewed by different team members. Thirty-six studies were included. Fifteen focused on guilt, three on shame, ten on self-perceived burden and eight discussed more than one of these feelings. Guilt was a predominant issue among older adults living with MLTCs. Gender, number, types and severity of comorbidities were determinant factors for feeling guilt, shame and/or burden. These findings highlight the importance of addressing self-conscious emotions in health psychology research and practice, to improve help-seeking and self-management among older adults with multimorbidity.
Introduction
According to United Nations Department of Economic and Social Affairs (UNDESA), ageing is rapidly accelerating worldwide and by 2050, the number of people aged 65 and older will have more than doubled reaching 1.5 billion, representing 16% of the global population (Padeiro et al., 2023; UNDESA, 2020). The increase in the older adult population requires long-term plans for providing care and support, that fit their needs and tailor the preventive plans. For instance, in England, health and social care for adults aged 65 years and over accounts for ~70% of the NHS spending annually and is projected to rise (Age UK, 2019; Public Health England, 2020; Stafford et al., 2018). Many older adults live with multiple long-term conditions (MLTCs), also known as multimorbidity (Age UK, 2019; Stafford et al., 2018). Globally, approximately one in three adults is diagnosed with MLTCs (Hajat and Stein, 2018). A systematic review reported that 42% of adults are diagnosed with MLTCs (Ho et al., 2022), with various disease clusters that can include both physical and mental health problems (Age UK, 2019; Department of Health, 2012). This variation emerges from the fact that there is no agreed taxonomy or definition for multiple long-term conditions or multiple chronic conditions (Hajat and Stein, 2018).
Implications of MLTCs among older adults
Previous studies reported that older adults with MLTCs had poorer quality of life (QoL) when compared with the general population (Valabhji et al., 2024; Wu et al., 2023). In addition to reduced QoL, studies found that older adults with MLTCs experienced feelings of reduced self-confidence and stigma, as well as an overwhelming burden related to the need and necessity of learning about their conditions, the daily demands of following self-management plans, and applying major changes in their daily lives (Corbett et al., 2020; Darin-Mattsson et al., 2017). While previous studies have mainly explored feelings of shame and stigma among older adults, there is less literature on self-perceived burden and possible association with poor health outcomes.
Self-perceived burden, guilt and shame
Self-perceived burden has been defined as ‘empathic concern engendered from the impact on others of one’s illness and care needs, resulting in guilt, distress, feelings of responsibility and a diminished sense of self’ (McPherson et al., 2007: 425). Self-perceived burden affects help-seeking behaviours including reporting of symptoms to healthcare professionals, relatives and caregivers (McPherson et al., 2007).
Although guilt and shame are both self-conscious emotions involving self-evaluation and reflection that engender feelings of psychological discomfort, it is important to distinguish between them (Collardeau, 2023). Miceli and Castelfranchi (2018) assert that ‘guilt implies a negative moral self-evaluation’ (p. 711). It involves feeling responsible for an act, behaviour or attitude. Shame is not related to responsibility in this way; instead, it is connected to a disjuncture between a perceived ideal and actual self, and it centres on self-worth. Similarly, Slepian et al. (2020) presents guilt as a negative evaluation of one’s behaviour, which can result in remorse or regret, whilst shame is associated with negative evaluations of the self and feeling helpless or small (Slepian et al., 2020) .
Contributing factors to feelings of guilt, shame and self-perceived burden
Emotional experiences such as shame, guilt and self-perceived burden among older adults with MLTCs do not occur in isolation; rather, they are often shaped by broader societal forces, including ageism and ableism. Ageism, defined as the stereotyping and discrimination against individuals or groups based on their age, found to influence how older adults view their health and worth, often internalising the belief that decline and dependency are inevitable (Caskie et al., 2025; Tzouvara et al., 2018). These beliefs can suppress help-seeking behaviours and reduce engagement with health services. At the same time, ableism, refers to the social prejudice that values able-bodiedness and cognitive independence, can exacerbate shame or guilt when older adults with chronic illnesses feel they can no longer meet societal expectations of productivity, autonomy, or resilience (McPherson et al., 2007; Rozanova, 2010).
Feelings of shame, guilt and self-perceived burden, can arise from personal notions of undesirable associations with weakness and can be intensified by stigma (Davidoff, 2002; McPherson et al., 2007) and ageism (Davidoff, 2002). Studies have reported internalised stigma and experienced stigma from formal and informal healthcare providers, as barriers to accessing healthcare that result in reduced QoL (Earnshaw and Quinn, 2012). Similarly, empirical evidence shows that older adults who endorsed ageist barriers including the belief that poor mental health is ‘normal’ in old age and the expectation that professionals would not take them seriously, were significantly less likely to seek mental health care, and reported higher depression and anxiety (Caskie et al., 2025). Moreover, media and public discussions on the economic and social implications of care for older adults (Davidoff, 2002; McPherson et al., 2007), can lead to feelings of guilt, shame and self-perceived burden. For instance, in a qualitative study, Clarke and Griffin (2007) reported that older adults felt judged by the surrounding society and some experienced shame because they did not meet idealised societal images of health and vitality. Similarly, Rozanova (2010) found that messages in the media were stigmatising by portraying ageing as self-reliance and healthfulness, which contributed to feelings of shame among older adults.
About this study
A better understanding of how feelings of shame, guilt and self-perceived burden might affect health service use, help-seeking, and care provision for older adults with MLTCs is needed. The idea for this research emerged from a previous project, which sought to identify research priorities for older adults with MLTCs. Those involved in this public engagement project emphasised the importance of exploring shame, guilt and self-perceived burden feelings. The scoping review reported below was the first step to explore how older adults with MLTCs experience these feelings, and how the latter influence their help-seeking behaviours and self-management of their health. This scoping review aimed to:
Map what is reported in the literature about feelings shame, guilt and self-perceived burden among older adults with MLTCs.
Explore how these feelings and perceptions may affect help-seeking and health service use by older adults with MLTCs.
Identify implications for current practice, gaps in knowledge and inform recommendations for future research.
Methods
The scoping review was conducted in line with methodological guidance from the Joanna Briggs Institute (JBI; Peters et al., 2021) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al., 2018). A protocol of the scoping review was registered in Open Science Framework (OSF) at: https://osf.io/c2dgz.
Patient and public involvement and engagement (PPIE)
With the help and support from the PPIE team at Keele University, we invited four older adults with MLTCs and caregivers to comment on different components and stages of the review. Participating patients and caregivers gave feedback on the questions and objectives, on the terms used for the search, on the findings and on the interpretation of the findings. Additionally, a public co-applicant and research team member was involved in all stages of the investigation and writing of this project.
Search strategy
The search strategy was developed in line with the Participant-Concept-Context (PCC) framework. Search terms reflected the Participants (older adults aged ⩾65 years with multiple long-term conditions) and the Concept (guilt, shame, and self-perceived burden), including relevant synonyms, related constructs and controlled vocabulary (e.g. MeSH terms). No restrictions were applied regarding Context (e.g. geographical location or care setting), and therefore contextual terms were not included in the search strategy.
Searches were conducted between November and December 2022 in Medline (Ovid); text words in the titles and abstracts and the index words used were noted. This was followed by searching across the following six databases: Medline (Ovid), EMBASE (Ovid), CINAHLPlus (EBSCO), APA PsycINFO (EBSCO), AGELINE (EBSCO), and Web of Science (SCI-EXPANDED, SSCI) (Supplemental Material 3, example of search strategy). Reference lists of included articles were searched to identify additional studies. Identified records were exported to Rayyan, a software for data management, for initial title and abstract screening. The search terms were selected based on a combination of theoretical relevance and terminological consistency in the literature concerning guilt, shame and self-perceived burden.
To operationalise the search, both free-text terms and indexed terms were used. Synonyms and related constructs for guilt, shame and self-perceived burden (e.g. self-blame, embarrassment, self-stigma, perceived burden to others. . .etc.) were combined with terms relating to older age and multiple long-term conditions. Relevant MeSH and subject headings were identified for each database (See an example of full search in Supplemental Material 1).
Study selection
To decide upon the inclusion-exclusion criteria, we used the Participant-Concept-Context (PCC) strategy. The review included studies that met the following criteria:
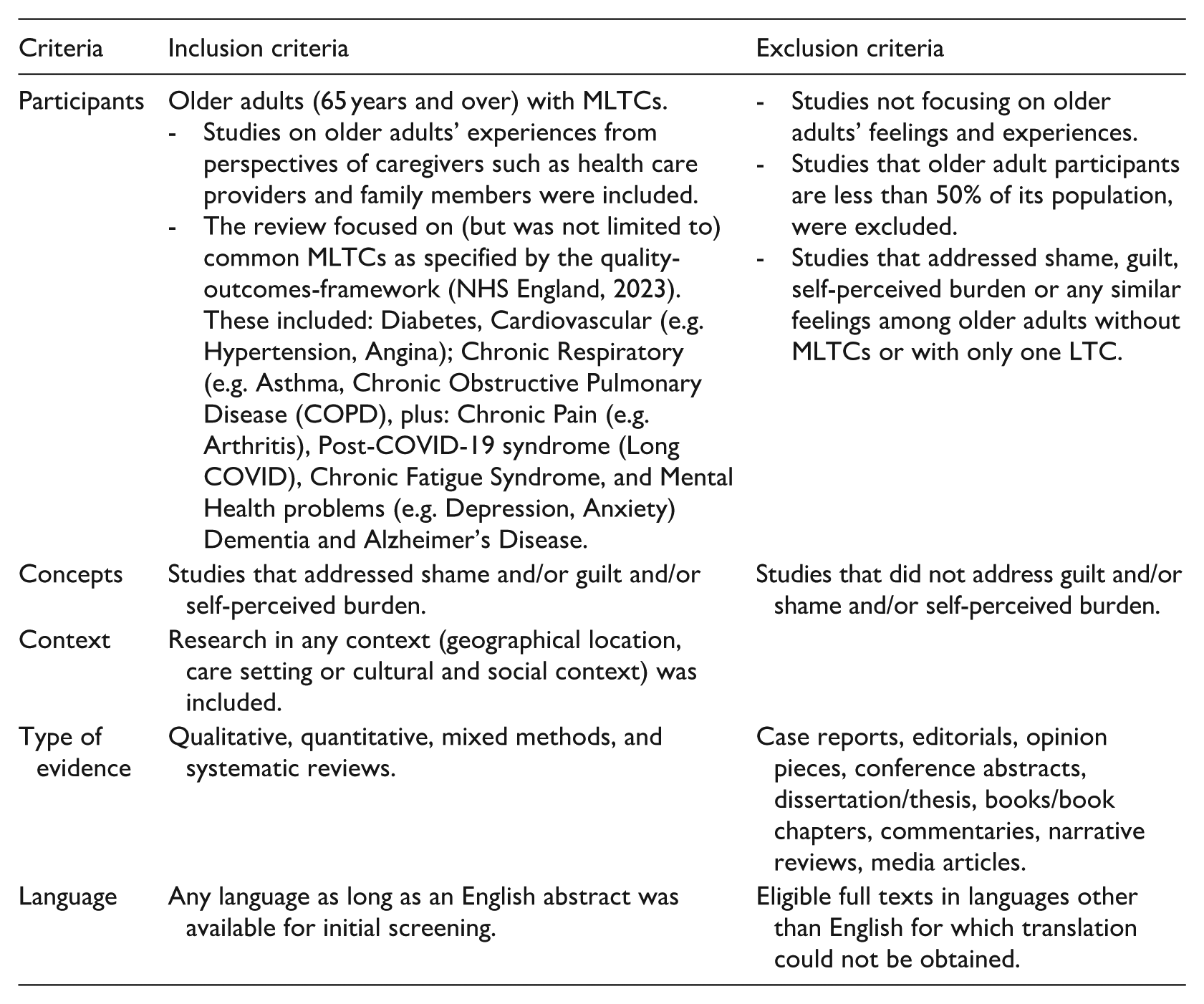
For the definition and delineation of constructs, we followed the MeSH (Medical Subject Headings) entry of each term. Accordingly, guilt was defined as ‘a cognitive emotional experience that occurs when a person believes or realises, accurately or not, that they have compromised their own standards of conduct or have violated a universal moral standard and bear significant responsibility for that violation’. Shame was defined as ‘an emotional attitude excited by realisation of a shortcoming or impropriety’. Shame was distinguished from guilt by its focus on the self rather than behaviour, which often involves feelings of worthlessness or exposure and is more associated with social devaluation. Self-perceived burden was defined as a ‘cognitive-affective state in which individuals believe their needs or existence impose hardship (emotional, physical, or financial) on others, especially caregivers. It incorporates elements of guilt, shame, and fear of causing distress, but is treated as a distinct construct due to its unique focus on interpersonal dependency and perceived social value’.
While these constructs might overlap, they were treated as analytically distinct for the purpose of clarity and accurate analysis and reporting of the findings.
Screening
For title and abstract review, the team used Rayyan software. In the first stage (pilot screen), four team members independently screened the titles and abstracts of 5% of the included references and discussed disagreements and inconsistencies until agreement was reached on the eligibility criteria were agreed. The remaining titles and abstracts were subsequently reviewed in pairs. Eligible full-text articles were exported and reviewed by pairs of reviewers independently via Covidence. Disagreements were discussed by reviewers until agreement was reached.
Data extraction
A customised data extraction proforma was developed. Key information extracted from each of the eligible studies included: author(s), year of publication, journal, country of origin of the conducted study, aims/purposes of the study, study design, population characteristics, PROGRESS elements, 1 findings on shame, on guilt, on self-perceived burden, health management and help-seeking, implications for practice, authors’ conclusions and reported strengths and limitations. Extracted data were independently checked for completeness and accuracy by the team, and discrepancies were resolved by discussion.
Data synthesis
Following JBI recommendations, we analysed data items by quantifying textual data and doing frequency counts of data extraction items (Pollock et al., 2023). This mainly required the use of descriptive data, such as proportions and common frequencies of type of evidence, countries and content related to the review question. Furthermore, we used basic qualitative content analysis, which is a descriptive approach to analysis of both the quantitative and qualitative studies (Peters et al., 2021). An initial descriptive table was constructed for the studies included (see Supplemental Materials 1-Table 1: Articles Characteristics), along with other detailed tables for each of the main results (See Supplemental Materials 2, Tables 2–6).
Results
Characteristics of included studies
Database searches yielded 9770 articles. Titles and abstracts were screened for eligibility, after which 471 were included for full-text review and 36 articles fully met the pre-specified criteria (See PRISMA flow chart, Figure 1).
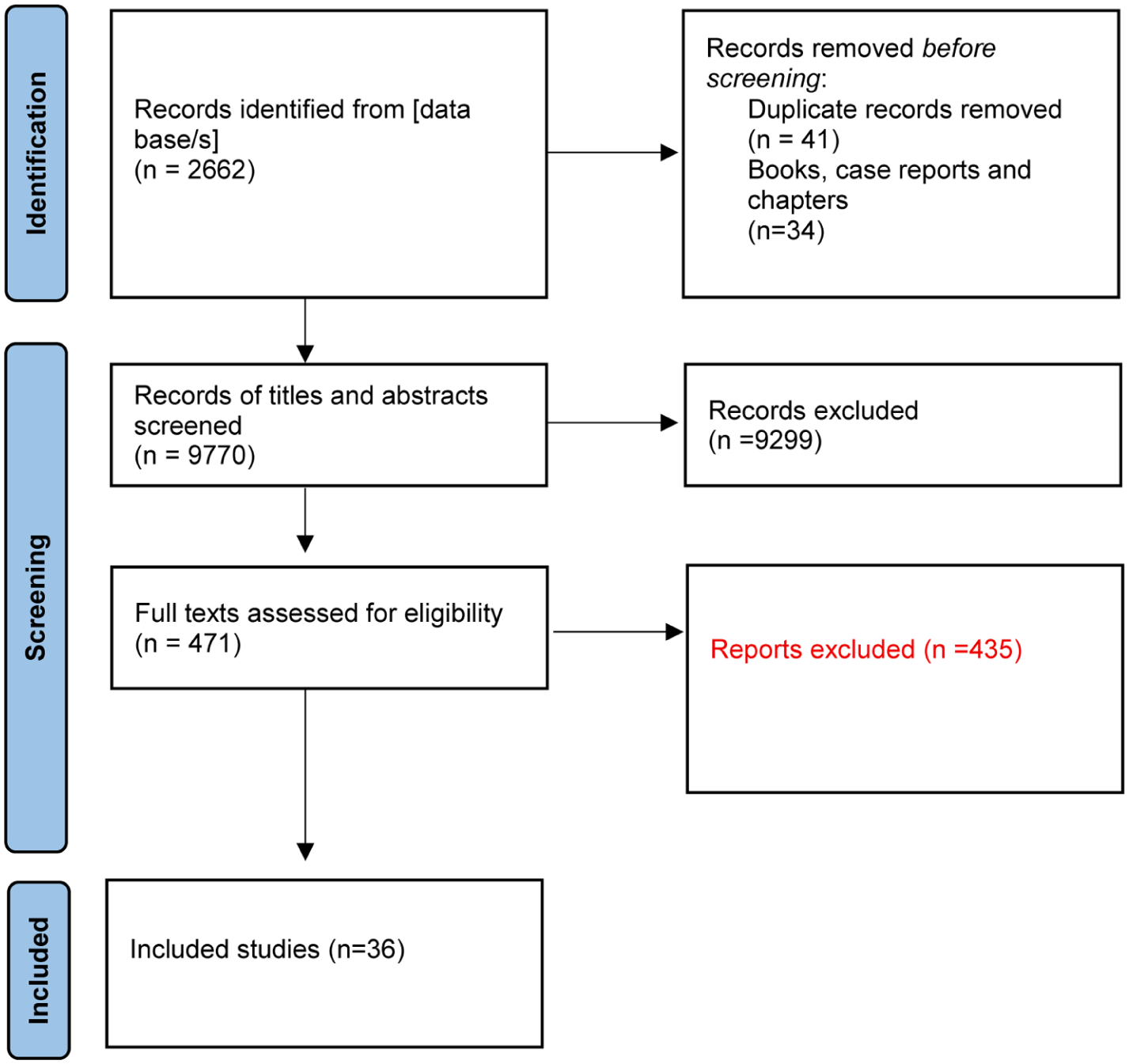
PRISMA flow chart. Study flow diagram (Adopted from Page et al., 2021).
The included articles came from the United States (n = 13), Europe (n = 12), East Asia (n = 5), Canada (n = 3), Australia (n = 2) and Argentina (n = 2). Twenty studies used quantitative research methods, ten used qualitative research methods and six used mixed methods (Supplemental Table 1). Most of the included articles were published from 2010 onwards (n = 23), suggesting that scholarly attention to this topic is more recent (see Supplemental Table 1).
Guilt was mentioned in the highest number of articles when compared with other feelings. Specifically, it was mentioned in 15 articles (Supplemental Materials 2, Table 2), followed by self-perceived burden which was the discussed feeling in ten articles (Supplemental Materials 2, Table 3), while shame was addressed only in three articles (Supplemental Materials 2, Table 4). Moreover, eight studies reported on two or three of these feelings, that is, guilt and shame, guilt and self-perceived burden, shame and self-perceived burden, or guilt and shame and self-perceived burden (Supplemental Materials 2, Table 5). In addition, eight articles discussed health management and seven mentioned help-seeking (Supplemental Materials 2, Table 6). The conditions reported that were mentioned in the included articles were: depression, anxiety, physical disability, dementia and Alzheimer’s disease, Parkinson’s disease, diabetes, hypertension, gout, ischaemic disease, cardiovascular disease, cancer, musculoskeletal diseases, neurological and spinal cord diseases, arthritis and chronic kidney disease. Many studies mentioned comorbidities without detailing the included conditions, making it impossible to report on the included conditions numerically. Moreover, some studies mentioned only the number of conditions without providing details, naming them, or reporting prevalence among participants. This lack of details may reflect the absence of consensus on the definition and clustering of MLTCs, as well as the lack of agreed taxonomy or definition for MLTCs.
Guilt-related outcomes
Fifteen studies discussed feelings of guilt among older adults with MLTCs including depression and Parkinson’s disease (PD), depression and Alzheimer’s disease (AD), depression and anxiety, depression and arthritis and depression and cardiovascular diseases (Supplemental Materials 2, Table 2).
In the studies that included participants with depression and PD, guilt or self-blame were not associated with depression (Brown et al., 1988; Ehrt et al., 2006; Farabaugh et al., 2009; Kritzinger et al., 2015). For example, Ehrt et al. (2006) reported that patients with PD showed significantly less sadness, less anhedonia, less guilt and less loss of energy compared to patients with depression only (control subjects), but more concentration problems than depressed control subjects. They found that neither guilt, nor self-blame, nor the somatic components of depression, increased among patients with PD.
Similar results were found among patients with depression and arthritis. Gotham et al. (1986), for example found that both the PD and the arthritis groups had depression characterised by pessimism and hopelessness, decreased motivation and drive, and increased concern with health. However, the negative affective feelings of guilt, self-blame, and worthlessness were absent in both patient groups.
In contrast to physical impairments, when depression is combined with anxiety, guilt and self-blame are present (Alfaro et al., 2022; del Sequeros Pedroso-Chaparro et al., 2021; Klein et al., 2007; Lynch et al., 2000; Orgeta and Orrell, 2014). Lynch et al. (2000), for example reported that the comorbidity of anxiety and depression was associated with a greater number of depressive episodes, more negative stressors, feeling sinful, guilty, worthless, and attempted suicide. Similarly, Klein et al. (2007) reported that heart failure severity and maladaptive coping styles, including denial, self-distraction, and self-blame, negatively affect QoL and increase depressive symptoms. Hence, coping mechanisms used by older adults with MLTCs may require attention.
Among patients with AD, feelings of guilt and self-blame were indicators of major depression (Arslanoglou et al., 2019; Starkstein et al., 2005, 2008). Starkstein et al. (2008), for instance, reported that the symptoms of loss of interest/pleasure, changes in appetite or weight, changes in sleep, low energy, worthlessness or inappropriate guilt, psychomotor retardation/agitation, concentration deficits, and suicidal ideation, were all significantly associated with the presence of the DSM-IV depressed-mood criterion for major depression among people with AD. Guilt was correlated with depression severity, and more intense feelings of guilt were noted among suicidal patients whose negative emotions did not improve over time (Arslanoglou et al., 2019). Moreover, women reported more feelings of guilt compared to men. For example, Kritzinger et al. (2015) compared men and women and found differences that included more frequent endorsement of the items ‘sadness’, ‘self-hate’, ‘crying’, ‘change in self-awareness’ and ‘loss of libido’ in women. In contrast, men reported more ‘dissatisfaction’, ’social withdrawal’ and ‘work difficulties.’
Shame-related outcomes
Three studies reported exclusively on shame; two included physical comorbidities (Brown, 2015; Clarke and Bennett, 2013a) and one psychological comorbidity (Raab et al., 2015). When comorbidities were physical, participants reported that their appearance made them feel embarrassed or ashamed. This was suggested to be linked to increased social stigma, particularly when participants also had functional limitations (Brown, 2015; Clarke and Bennett, 2013a). For instance, in their qualitative study, Clarke and Bennett (2013a) reported embarrassment and feelings of shame among men and women, suggesting that gender influenced the reasons underlying these feelings. Men’s accounts reflected what may be considered typical masculine values and perceptions, including control, invulnerability, physical prowess, self-reliance and toughness, while women were more concerned with their body’s altered appearance. Men experienced their symptoms as a source of exasperation, reduced quality of life (QoL) and a growing perception of themselves as ineffectual. In contrast, women experienced their bodies as a source of frustration and embarrassment, relating both to altered physical abilities and changes in appearance. Men experienced their symptoms as a source of exasperation, decreased QoL and growing perception of themselves as ineffectual. In contrast, women experienced their bodies as a source of frustration and embarrassment, relating both to altered physical abilities and changes appearance.
When comorbidities were psychological, major depression was reported as a key factor contributing to feelings of shame and embarrassment. For example, Raab et al. (2015) found that posttraumatic negative cognitions about the self were most strongly associated with comorbid depressive symptoms and the depression-related numbing cluster of posttraumatic stress disorder (PTSD). For example, Raab et al. (2015) found that posttraumatic negative cognitions about the self were most strongly associated with comorbid depressive symptoms and the depression-related numbing cluster of posttraumatic stress disorder (PTSD). These findings suggest that posttraumatic cognitions about the self are not specific to PTSD but are more strongly related to symptoms of depression and negative affect.
Self-perceived burden-related outcomes
Ten articles discussed self-perceived burden: two reported psychological comorbidities, primarily depression and anxiety and eight reported physical illnesses (Supplemental Materials 2, Table 4). Two articles examined both physical and psychological illnesses, and two reported on depressive symptoms resulting from comorbidity, which was associated with higher likelihood experiencing self-perceived burden (i.e. depression was secondary to chronic illness and contributed to increased self-perceived burden feelings).
Across both psychological and physical disabilities, several studies reported that feelings of being a burden were higher during the early stages and declined over time (Van Orden et al., 2012; Wei et al., 2020; Williams et al., 2005). For instance, Van Orden et al. (2012) reported that burdensomeness, depression and meaning in life were significantly associated with time and were experienced more strongly during the first 2 months after diagnosis. Similarly, Jang et al. (2023) reported feelings of being a burden increased when individuals required physical and economic support but decreased when informational and emotional support was needed.
The greater the chronicity of conditions experienced, the higher the levels of depressive symptoms, which in turn increased feelings of burden (Cousineau et al., 2003; Hardman et al., 2021; Whittemore and Dixon, 2008). Cousineau et al. (2003) reported that self-perceived burden was not related to the nature of the medical condition, but rather to the number of conditions and their severity. Self-perceived burden was reflected in patients’ attempts to balance dependence and independence (Whittemore and Dixon, 2008). Moreover, physical burden was not the only form of burden reported; financial burden and concerns related to death management imposed on relatives were also identified. For example, in their study of patients with chronic obstructive pulmonary disease (COPD), diabetes, cardiovascular diseases and other chronic conditions, Cha et al. (2021) found that participants were not afraid of death but feared becoming a burden to their loved ones due to their need for assistance. This led some patients to plan their funeral and to wish to die without burdening their children. Furthermore, depressive symptoms were associated with pain severity; higher levels of pain were associated with stronger depressive symptoms, hopelessness and self-perceived burden (Wang et al., 2021). Studies examining self-perceived burden and health management identified several determinants. The primary determinants identified were age and gender (Felton and Revenson, 1987; Wei et al., 2020). For example, Wei et al. (2020) found lower levels of help-seeking among men due to stigma.
Courtenay (2000) argued that beliefs associated with masculinity, such as self-reliance, resilience and toughness may empower ageing men to take control of their health by engaging in proactive health-related behaviours. In addition, the number of comorbidities has been identified as a determinant of self-perceived burden (Cha et al., 2021; Cousineau et al., 2003; Wei et al., 2020). Health literacy (Wei et al., 2020) and economic status (Jang et al., 2023; Wei et al., 2020; Williams et al., 2005) were also identified as determinants of self-perceived burden. For example, Wang et al. (2021) reported that in rural China, unemployment, higher levels of hopelessness, depressive symptoms, and severe pain were significantly associated with self-perceived burden and elevated suicide risk. Similarly, perceived burden among Koreans was negatively associated with English-speaking ability and residence in a low-Korean-density area (Jang et al., 2023). These findings indicate that sociodemographic factors influence self-perceived burden among older adults with MLTCs.
Coexistence of multiple feelings in MLTCs
Eight studies reported the co-occurrence of more than one emotional experience. Of these three examined guilt and self-perceived burden, three examined shame and self-perceived burden and two examined guilt and shame (Supplemental Materials 2, Table 5). Most of these studies (n = 6) were qualitative, which may explain the in-depth exploration of combined feelings associated with living with MLTCs at older age. When shame co-occurred with self-perceived burden, it was often linked to visible or socially observable behaviour (Cole and Drennan, 2019; Troya et al., 2019). For example, Cole and Drennan (2019) reported that patients with dementia experienced shame related to incontinence. Self-perceived burden co-occurred with feelings of embarrassment and reluctance to disclose incontinence to family members. Similarly, Troya et al. (2019) found that shame resulting from uncontrolled behaviour was common among older adults with multiple mental and physical illness, due to social and family expectations associated with their age. In this case, loss of control, increased loneliness to avoid embarrassment and perceptions of burden intensified with age (Kvaal et al., 2014). Perceived burden sometimes prevented older adults from disclosing their illness to caregivers, particularly when financial burden was added to the ‘shameful’ nature of the behaviour (Leijten et al., 2018).
Studies that reported guilt and self-perceived burden found that the higher number of comorbidities and greater condition severity were associated with stronger feelings of guilt and perceptions of being a burden (Dyeson, 2000; Eckerblad et al., 2015; Lee-Jen and Tusaie, 2004). For example, Eckerblad et al. (2015) found that among participants with MLTCs who reported more than 12 symptoms, perceptions of burdening others were associated with feelings of guilt. Greater dependency was associated with higher levels of guilt, particularly in relation to partners or children. Uncontrolled dependency resulting from severe and multiple chronic conditions may increase self-perceived burden, as patients may have limited alternatives to seeking help. Furthermore, an increase in the number of conditions was associated with higher likelihood of depression, which in turn was linked to greater self-perceived burden (Lee-Jen and Tusaie, 2004). A lack of support from caregivers amplified these feelings, particularly when combined with poorer health status, fewer financial resources and lower levels of spiritual activity among older adults (Dyeson, 2000). Studies examining guilt and shame primarily focused on physical conditions (Francis et al., 2019; Kong et al., 2019). These studies reported that a lack of symptoms control and failure to achieve health goals were associated with feelings of shame and guilt. Guilt and shame were linked to reduced treatment adherence due to embarrassment about disclosing perceived failure to healthcare professionals and were associated to delays in seeking help.
Health management and help-seeking
Twelve articles discussed health management and help-seeking (Supplemental Materials 2, Table 6). Of these, three addressed both topics, five focused solely on management, and four focused on help-seeking. Most of these articles (n = 8) used qualitative methods, three used quantitative methods and one used mixed method. Most studies (n = 11) included more than three conditions, which were primarily physical or a combination of physical and psychological conditions. Only one study included two psychological conditions (Orgeta and Orrell, 2014). Most studies focused guilt (n = 7), followed by self-perceived burden (n = 6), and lastly shame (n = 5). Half of the studies (n = 6) examined one feeling, whereas the other half examined two. None included all three feelings (guilt, shame and self-perceived burden). Findings related to both management and help-seeking indicated that challenges in help-seeking led to the development of specific self-management strategies. For example, Hardman et al. (2021) found that having MLTCs created challenges in accessing multiple healthcare professionals, particularly for individuals living in remote areas. This led patients to individually appraise and adjust to treatment, without always consulting healthcare professionals. Similarly, Clarke and Bennett (2013a) found that the need to consult several healthcare professionals due to MLTCs, and discuss numerous conditions, could have negative consequences, such as social isolation and avoidance of others. They argued that, within neoliberal societies, responsibility for health management is placed on the individual, who may then be blamed and labelled as accountable for their health conditions.
In addition to MLTCs acting as a barrier to help-seeking, guilt combined with self-perceived burden was associated with avoidance of help-seeking and reduced agency in shared decision-making (Dyeson, 2000; Francis et al., 2019). The tension between the need to seek help and the shame associated with asking for it, in some cases, associated with self-harm, but in others with expressions of self-agency, such as attempts to control symptoms when possible, as observed in cases of incontinence among older adults with dementia at the early to middle stages (Cole and Drennan, 2019; Troya et al., 2019).
Barriers to engagement in treatment and health management included anxiety, administrative delays and feeling disadvantaged when patients’ opinions were not included in health professionals’ decision-making processes (Francis et al., 2019; Kong et al., 2019; Orgeta and Orrell, 2014). Reported modifiers for self-management included acceptance of health problems and coping strategies such as resilience, taking responsibility and preparing family members for the implications of illnesses (Cha et al., 2021; Cole and Drennan, 2019; Hardman et al., 2021; Leijten et al., 2018). For example, Cha et al. (2021), reported that preparing family members for death and funeral arrangements helped patients with severe chronic illnesses to cope with self-perceived burden.
Discussion
This scoping review highlights differences in experiences of shame, guilt and self-perceived burden among older adults with MLTCs. While depression was the most frequently investigated morbidity in the included studies, self-perceived burden was the most commonly reported feeling among older adults with MLTCs compared with guilt and shame. These emotional experiences cannot be fully understood without considering the role of systemic ageism and ableism. Ageism, in particular, may normalise suffering and emotional distress in older adults, discouraging help-seeking and reinforcing the belief that their needs are burdensome (Caskie et al., 2025; Tzouvara et al., 2018). Ableism, which devalues individuals with physical or cognitive impairments, may intensify feelings of shame or guilt when older adults are unable to meet standards of independence and productivity that dominate healthcare and societal narratives (Davidoff, 2002; McPherson et al., 2007; Rozanova, 2010). These structural forms of stigma contribute to the internalisation of guilt, shame and self-perceived burden, and shape how older adults engage with care systems. This scoping review found that increased guilt among older adults was more prevalent when depression co-occurred with anxiety (Coplan et al., 2015; Kupper et al., 2012). Coplan et al. (2015) for example showed that comorbid anxiety and depression predicted poorer outcomes, including higher rates of treatment resistance, than either disorder occurring alone. Treatment resistance may also be reflected in reduced help-seeking and increased self-isolation, which were identified as an outcome in the studies included in this review. Included studies reported feelings of guilt and self-blame among patients with AD and comorbid depression. Depression and cognitive impairment, such as AD, are both common in old age and frequently co-occur (Korczyn and Halperin, 2009). Depression can appear at the early stages of AD, as a psychological reaction to cognitive decline. However, past studies suggest that late-life depression is also a risk factor for AD (Invernizzi et al., 2022). The early occurrence of depression among people with AD, which has been associated with guilt and self-blame, may be explained by greater awareness of the burden placed on caregivers during the initial stages of the disease. Comparisons of these feelings across different stages of AD are challenging, as patients gradually lose capacity to participate in research during the later stages of the disease. Studies included in this review did not find feelings of guilt to be common among people with PD. However, studies suggest that feelings of shame may result from motor and non-motor symptoms, as well as from self-inadequacy related to loss of autonomy, the need for help, and a damaged body image (Angulo et al., 2019). Studies that reported shame primarily focused on physical conditions or a combination of physical and psychological conditions, rather than solely psychological. This pattern may be linked to the visibility of the physical conditions and to other sociocultural factors such as gender. Previous studies have reported a positive association between self-perceived stigma and the visibility of physical chronic conditions, such as arthritis and multiple sclerosis, which also limit functional ability (Brown, 2015; Joachim and Acorn, 2000). This association may be further compounded by ableist assumptions that equate disability with dependency and loss of social value (McPherson et al., 2007; Rozanova, 2010). A very recent study found that the erosion of self-worth may be understood as emerging from the interaction of shame and helplessness. Shame related to mobility impairments (such as wheelchair use) and heightened sensitivity to others’ gaze can discourage older adults from leaving their homes, thereby intensifying social isolation. At the same time, perceiving oneself as a financial or caregiving burden on adult children may reinforce feelings of guilt and self-blame. Together, these interconnected emotional experiences may contribute to withdrawal from social life and reduced engagement with support services.
Ageism and ableism intersect to construct older adults with MLTCs as ‘less than’ in social and healthcare contexts, shaping how they internalise shame and guilt related to their conditions (Clarke and Griffin, 2007; Davidoff, 2002). These intersecting stigmas may magnify the emotional burden experienced by older adults with MLTCs. Additionally, media portrayals, healthcare practices, and policy frameworks often reinforce ideals of successful ageing tied to physical activity, self-reliance, and mental clarity, marginalising those who do not conform to these ideals (Clarke and Griffin, 2007; Davidoff, 2002). As a result, older adults may come to view themselves as burdensome, particularly when they require sustained care.
Moreover, previous studies have reported higher levels of shame among males than females, whereas feelings of guilt were more commonly reported among females than males (Brown, 2015; Clarke and Bennett, 2013a; Lee-Jen and Tusaie, 2004). Previous studies suggest that these differences reflect masculine perceptions of the body among men, emphasising their physical prowess and self-reliance, whereas women tend to be more concerned with their altered appearance (Clarke and Bennett, 2013a) and social roles as carers within their families (Clarke and Bennett, 2013b; Sanders and Power, 2009). Self-stigma and social stigma are major barriers to help-seeking among older adults, particularly when individuals believe that seeking treatment may further intensify stigma (Johnson and Conner, 2019; Tzouvara et al., 2018). In line with findings on shame, most studies in this review reported self-perceived burden primarily when comorbidities involved physical long-term conditions. Past studies have also linked self-perceived burden to physical symptoms such as pain and physical weakness (Kowal et al., 2012; Mavaddat et al., 2014). We argue that the visibility and immediacy of physical symptoms may contribute to higher levels of self-perceived burden among older adults with physical comorbidities, compared with those with mental health comorbidities. Moreover, physical disabilities often require direct and continuous support from relatives, which may further intensify self-perceived burden among patients.
Studies that included more than one feeling most often examined self-perceived burden and were predominantly qualitative. When shame co-occurred with self-perceived burden, it was related to visible behaviours that led to embarrassment among older adults due to a lack of control. Consistent with these findings, past studies not specifically focused on comorbidities have reported embarrassment among older adults due to a lack of control over behaviours, such as in early-stage dementia patients (Aldridge et al., 2019) and urinary incontinence (Cole and Drennan, 2019; Yan et al., 2022).
Guilt was associated with self-perceived burden when the severity and number of comorbidities increased. Previous studies have also reported a correlation between the number and severity of chronic conditions and feelings of guilt, as the increasing illnesses burden augments the need for help and support, particularly among individuals with physical conditions (LeBlanc and Jacelon, 2018; Pedroso-Chaparro et al., 2021). Similar to studies that examining multiple feelings in this review, the majority of studies addressing help-seeking and management were also qualitative. Interactions between qualitative researchers and participants can facilitate an in-depth understanding of lived experiences (Malagon-Maldonado, 2014) and the complex interplay between different feelings. Britten (2011) argued that better conceptual and explanatory development could be achieved through qualitative syntheses, which offer opportunities to build a cumulative evidence base. This scoping review provides evidence for the need for further qualitative studies on guilt, shame and self-perceived burden among older adults with MLTCs.
Implications for practice
Health care providers: The findings of this review reinforce the need for healthcare professionals to consider the psychological implications of comorbidities among older adults. In particular, the evidence highlights the importance of case-finding for anxiety and depression, as the co-occurrence of these conditions is associated with increased feelings of guilt, shame and self-perceived burden. Wei et al. (2020) recommended early screening and assessment to prevent delayed or absent help-seeking, which may otherwise contribute to deterioration in both physical and mental health. Adopting a preventive approach to addressing these feelings may reduce their severity, improve treatment adherence and enhance patients’ QoL.
Given that older adults may not be aware of ‘synergistic’ treatments and how different conditions interact, Hardman et al. (2021) recommended supporting older adults in understanding these interaction. They also recommended cross-disciplinary intervention approaches for older adults with MLTCs, including the involvement of family members in care processes (Cha et al., 2021). Healthcare providers should use sensitive communication, empathetic, non-judgemental language to reduce feelings of guilt or shame, especially when discussing disease management, setbacks or care needs. Individualised care planning represents an additional actionable strategy, particularly when it acknowledges emotional experiences linked to gender roles and identity (e.g. masculinity and independence in men; caregiving identity in women). Understanding how ageism and ableism intersect with emotional distress is therefore crucial for developing more inclusive and empathetic healthcare models for older adults with MLTCs. furthermore, healthcare providers can further support self-management by encouraging meaningful activity while offering appropriate levels of support to avoid overburdening individuals, especially those experiencing cognitive decline or emotional distress. Among the gaps identified in this review is the limited focus on pain as a contributing factor to feelings of guilt, shame and self-Perceived burden. Wang et al. (2021) proposed that regular screening for pain, depressive symptoms, hopelessness and perceived burden, using simple but sensitive questions or scales, may be vital for prevention and early detection of suicide risk among older adults. Families and Informal Caregivers: Understanding the emotional Impact of MLTCs is essential for families and informal caregivers. Caregivers should be aware that feelings of being a burden, shame or guilt may lead to withdrawal, self-isolation, or in some cases self-harm among older relatives. Attention to changes in behaviours and interpersonal relationships is therefore important. Moreover, family caregivers are encouraged to foster open dialogue by creating a supportive environment in which older adults can express needs and emotions without fear of judgement. Lastly, caregivers can support one another by distributing care responsibilities, thereby reducing the likelihood that the older adult feels like a burden on a single family member. This may include drawing on community or formal care resources to reduce dependency pressures and preserve dignity.
Policy Makers: There’s a clear need to integrate mental health considerations into MLTC frameworks. National care models for older adults with MLTCs should include routine psychological screening and emotional support as standard practice. Moreover, policymakers should also promote gender-sensitive and culturally safe interventions through funding programmes that recognise the role of cultural norms and gender in shaping emotional experiences and care preferences. In addition, holistic and cross disciplinary care that integrate services and involve families enhance awareness and responsiveness to older adults’ needs. Investment in training and workforce development is also essential to equip healthcare providers and caregivers with the skills needed to address psychosocial aspects of MLTCs, including guilt, shame and self-perceived burden.
Strengths and limitations
This scoping review demonstrates strong methodological rigour and transparency by adhering to Joanna Briggs Institute guidance and PRISMA-ScR reporting standards, with a pre-registered protocol enhancing reproducibility and credibility. The comprehensive search strategy across six major databases, combined with the use of both controlled vocabulary and free-text terms, ensured broad coverage of multidisciplinary literature relevant to older adults with multiple long-term conditions (MLTCs). Inclusion of qualitative, quantitative, mixed-methods studies and systematic reviews allowed for a nuanced mapping of evidence, which is particularly appropriate for exploring complex emotional constructs. A key strength is the clear conceptual distinction between guilt, shame and self-perceived burden, addressing a common limitation in prior research where these emotions are often conflated. The integration of Patient and Public Involvement and Engagement (PPIE) throughout the different stages of the study further strengthened the relevance, culture competence and interpretive validity of the findings. Importantly, the scoping review addresses an underexplored psychosocial dimension of multimorbidity and identifies critical gaps, providing valuable direction for future research, practice, and policy.
Despite these strengths we acknowledge several limitations. As a scoping review, this study did not include formal appraisal of the methodological quality or risk of bias of the included studies, limiting the ability to assess the strength of the evidence or draw causal inferences. Considerable heterogeneity in how MLTCs were defined and reported across studies (particularly regarding type, severity, and clustering of conditions) restricted comparability and depth of condition-specific analysis. The evidence base was uneven, with substantially fewer studies addressing shame compared to guilt and self-perceived burden, resulting in less robust conclusions for this construct. Although studies from multiple countries were included, most were conducted in high-income Western contexts, which may limit cultural transferability. Additionally, older adults with advanced cognitive impairment or late-stage disease were underrepresented, and some studies relied on limited quantitative indicators of emotional experiences, potentially underestimating their complexity. Finally, language and publication bias may have been introduced by reliance on studies with English abstracts and the exclusion of grey literature.
Conclusion
This scoping review deepens understanding of the psychological burden experienced by older adults with MLTCs, highlighting how guilt, shame and self-perceived burden intersect with gender, condition severity, and societal expectations. By drawing attention to these often-overlooked emotional dimensions, the review underscores the need for holistic, person-centred approaches in both care planning and research. The findings also reveal critical gaps in the literature, particularly regarding pain and emotional burden and point to the need for further qualitative inquiry to inform interventions that address both physical and psychological well-being in later life.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261425329 – Supplemental material for Guilt, Shame and Self-Perceived Burden among Older Adults with Multiple Long-Term Conditions: A Scoping Review
Supplemental material, sj-docx-1-hpq-10.1177_13591053261425329 for Guilt, Shame and Self-Perceived Burden among Older Adults with Multiple Long-Term Conditions: A Scoping Review by Suhad Daher-Nashif, Tamsin Fisher, Shoba Dawson, Stephanie Tierney, Julia Hamer-Hunt, Jacky Forsyth, Carolyn Chew-Graham, Anne-Marie Boylan and Opeyemi O. Babatunde in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053261425329 – Supplemental material for Guilt, Shame and Self-Perceived Burden among Older Adults with Multiple Long-Term Conditions: A Scoping Review
Supplemental material, sj-docx-2-hpq-10.1177_13591053261425329 for Guilt, Shame and Self-Perceived Burden among Older Adults with Multiple Long-Term Conditions: A Scoping Review by Suhad Daher-Nashif, Tamsin Fisher, Shoba Dawson, Stephanie Tierney, Julia Hamer-Hunt, Jacky Forsyth, Carolyn Chew-Graham, Anne-Marie Boylan and Opeyemi O. Babatunde in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053261425329 – Supplemental material for Guilt, Shame and Self-Perceived Burden among Older Adults with Multiple Long-Term Conditions: A Scoping Review
Supplemental material, sj-docx-3-hpq-10.1177_13591053261425329 for Guilt, Shame and Self-Perceived Burden among Older Adults with Multiple Long-Term Conditions: A Scoping Review by Suhad Daher-Nashif, Tamsin Fisher, Shoba Dawson, Stephanie Tierney, Julia Hamer-Hunt, Jacky Forsyth, Carolyn Chew-Graham, Anne-Marie Boylan and Opeyemi O. Babatunde in Journal of Health Psychology
Footnotes
Acknowledgements
We thank the PPIE team and participants for their valuable feedback at different stages of the study; We also thank the stakeholders for their reflections and feedback on the findings.
ORCID iDs
Ethical considerations
Ethics approval was not required for this review article as no data were collected from participants.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
Conceptualisation: All authors; Searching and data curation: SDN, OOB, SD; Reviewing title and Abstract: SDN, TF, OOB, SD, JF; Reviewing full texts: SDN, TF, OOB, SD, JF; Data extraction: SDN, TF; Reviewing full texts and the extracted data: All authors; Writing original draft: SDN, OOB, TF, SD, ST; Revising the final draft: All authors; All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the National Institute for Health and Care Research (NIHR) School of Primary Care Research (grant number 605). CCG is part-funded by the NIHR Applied Research Collaboration West Midlands (NIHR200165). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be available in the Supplemental Materials.
Supplemental material
Supplemental material for this article is available online.