
Abstract
This study examines whether individuals’ exposure to and trust in COVID-19 vaccine misinformation can be used to segment audiences and explain variations in vaccine hesitancy and health beliefs. Using k-means clustering, a survey of 819 U.S. college students (March–May 2021) identifies four subgroups based on combinations of high or low misinformation exposure and trust: misinformation-shielded (low exposure, low trust), misinformation-vulnerable (low exposure, high trust), misinformation-resistant (high exposure, low trust), and misinformation-accepting (high exposure, high trust). These subgroups differ significantly in political ideology, vaccine hesitancy, and health beliefs. The misinformation-shielded subgroup reports more liberal views, lower hesitancy, and higher perceived efficacy, whereas the misinformation-vulnerable and misinformation-accepting subgroups perceive lower vaccine safety. Regression analyses show that perceived vaccine efficacy and perceived vaccine safety are relatively stable predictors of vaccine hesitancy. The misinformation exposure-trust framework offers a theory-based strategy for segmenting audiences and informs more targeted health interventions.
Keywords
Introduction
Although the COVID-19 pandemic officially ended in 2023, its impact is still ongoing (World Health Organization WHO [WHO], 2025). Aside from the illness itself, the COVID-19 pandemic has sparked widespread distrust and hesitancy regarding medical information and vaccination (Nelson et al., 2020). Data show that 28% of participants believed COVID-19 vaccines caused thousands of deaths, and 22% believed infection was less risky than vaccination (Van Beusekom, 2024). Yet, global estimates suggest that COVID-19 vaccination averted over 2.5 million deaths and saved approximately 14.8 million life-years between 2020 and 2024 (Ioannidis et al., 2025).
Misinformation has emerged as a communication force that undermines public trust and contributes to vaccine hesitancy (Nelson et al., 2020). Notably, 73% of people who were hesitant to get vaccinated were exposed to misinformation about COVID-19 vaccination (Neely et al., 2022). Current research on misinformation often focuses on either exposure or trust. However, accessing and consuming misinformation involves both processes to varying degrees. Individuals may be highly exposed to COVID-19 misinformation but remain skeptical, whereas others with limited exposure may still hold strong trust in it. The consequences of these distinctions remain unclear, constraining theoretical understanding of how misinformation affects individuals differently and hindering practical efforts to combat it.
Therefore, this study proposes an audience segmentation framework based on individuals’ levels of exposure to and trust in misinformation. Specifically, it aims to examine (a) whether distinct subgroups can be empirically identified using this framework; (b) whether these subgroups differ in their demographic characteristics, health beliefs, and levels of vaccine hesitancy; and (c), more importantly, whether the underlying mechanisms that predict vaccine hesitancy vary across these subgroups. This study fills the academic gap by profiling people into distinctive subgroups based on the misinformation exposure-trust framework. Results of this study give a different perspective on understanding the population that may fall for misinformation in public health. Practically, segmenting individuals based on their exposure to and trust in misinformation and identifying the mechanisms underlying vaccine hesitancy can help inform targeted communication strategies.
Literature review
Theoretical framework: Stimulus-organism-response (S-O-R)
The stimulus–organism–response (S-O-R) framework (Mehrabian and Russell, 1974) posits that external stimuli elicit individuals’ internal cognitive and emotional processes, which in turn shape behavioral responses. Guided by this framework, prior studies have examined how exposure to information or misinformation influences emotional reactions (e.g. fear, anxiety), trust in information sources, and health beliefs, all of which ultimately affect health behavior intentions (e.g. Ma et al., 2024; Xu et al., 2023).
While prior research has examined misinformation exposure and trust separately, few studies have explored how these factors relate to one another and to individuals’ health-related attitudes and behaviors across different audience segments. To address this gap, the present study investigates how exposure to COVID-19 misinformation (stimulus) and trust in such misinformation (organism) are associated with individuals’ health-related beliefs and vaccine hesitancy (response). Specifically, we aim to determine whether individuals can be meaningfully segmented based on their levels of misinformation exposure and trust.
Based on theoretical reasoning and prior literature on misinformation processing and audience segmentation (e.g. Rimal et al., 2009; Su and Shi, 2023), we conceptualize four potential subgroups that represent distinct combinations of misinformation exposure and trust: those with low exposure and low trust (misinformation-shielded), low exposure but high trust (misinformation-vulnerable), high exposure but low trust (misinformation-resistant), and high exposure and high trust (misinformation-accepting). These combinations indicate distinct psychological profiles. For example, those frequently exposed to misinformation but skeptical may differ from those rarely exposed yet trusting. Identifying such subgroups clarifies who is most vulnerable to misinformation and guides targeted health interventions. Therefore, we propose:
Demographic differences among misinformation exposure-trust subgroups
Understanding how individuals respond to health misinformation requires considering not only their levels of exposure and trust but also the demographic factors that shape these responses. Prior research has demonstrated that demographic characteristics influence individuals’ susceptibility to health misinformation (Jamieson and Albarracin, 2020; Roozenbeek et al., 2020). For instance, a systematic review of 61 studies found that conservatism, minority status, younger age, and lower education predict greater vulnerability to health misinformation (Nan et al., 2022). However, other research on COVID-19 vaccine hesitancy found that ethnicity, gender, and political ideology were not significant predictors (Lee et al., 2022), suggesting that the role of demographic factors remains complex and context-dependent.
Building on this literature, it is important to examine how demographic characteristics may differentially shape individuals’ exposure to and trust in health misinformation. Prior studies have also shown that young adults aged 18–34 tend to be more susceptible to health misinformation (Chandrasekaran et al., 2024), underscoring the need to focus on this population. By analyzing how these characteristics vary across subgroups defined by misinformation exposure and trust, researchers can better understand the social patterns underlying vulnerability or resistance to misinformation. Hence, we pose
Health beliefs and vaccine hesitancy across misinformation exposure-trust subgroups
Vaccine hesitancy is defined as the delay in acceptance or refusal of vaccines despite the availability of vaccination services (WHO, 2014). In recent years, it has emerged as a significant public health concern, further exacerbated by the spread of health misinformation on digital platforms (Garett and Young, 2021; Puri et al., 2020). Prior research has highlighted that exposure to and trust in misinformation are both critical in shaping public attitudes toward vaccines (e.g. Lee et al., 2023; Xu et al., 2023).
The Health Belief Model (HBM) provides a key framework for understanding health-related decisions. The model posits that individuals’ health-related actions are shaped by a set of beliefs regarding their susceptibility to a disease, the severity of its consequences, and the perceived benefits and barriers of taking action (Champion and Skinner, 2008; Rosenstock, 1974).
This study examines key health beliefs derived from the HBM (Rosenstock, 1974). Perceived severity refers to how serious individuals believe a health issue would be, while perceived susceptibility reflects beliefs about the likelihood of infection. Beyond perceived disease risk, beliefs about the vaccine itself are central to the HBM. Perceived efficacy captures confidence in a vaccine’s ability to prevent illness or mitigate its severity, corresponding to the HBM’s construct of perceived benefits, the belief in the effectiveness of taking a recommended health action. Perceived safety parallels perceived barriers, as lower safety perceptions indicate concerns about vaccine risks or side effects that may discourage uptake.
Furthermore, this study distinguishes between two types of perceived threat adapted from Kachanoff et al. (2021): realistic threat, which reflects concerns about the virus’s impact on one’s personal health, financial safety, and daily life; and symbolic threat, which captures broader concerns about threats to national values, identity, and institutions. Building on this framework, the present study conceptualizes symbolic threat at the national level as the unique nature of COVID-19 heightened concerns about national identity and values, particularly in contexts such as the United States, where the pandemic became highly politicized. This distinction enables a more comprehensive understanding of how individuals respond to the pandemic on both personal and societal levels.
Additionally, prior studies have identified multiple psychological predictors of susceptibility to health misinformation, including cognitive skills, emotional responses, trust in sources, personal values, and group identity (Nan et al., 2022; Roozenbeek et al., 2020; Scherer et al., 2021). Existing research on COVID-19 shows that misinformation exposure decreases trust in experts, increases misperceptions, and reduces compliance (Kim et al., 2023; Lee and Choi, 2024). However, no studies have examined how the combination of misinformation exposure and trust, two core predictors, relates to variations in vaccine-related health beliefs and hesitancy. Segmenting individuals into subgroups based on these dimensions enables a more nuanced understanding of how distinct psychological profiles correspond to vaccine beliefs and hesitancy. Therefore, the following research question is proposed:
Predictors of vaccine hesitancy across misinformation exposure-trust subgroups
Vaccine hesitancy is a multifaceted phenomenon influenced by a combination of psychological, social, and structural factors. Among these, health beliefs and sociodemographic as well as attitudinal factors have consistently emerged as key predictors of individuals’ vaccine hesitancy (Holt et al., 2022; Limbu et al., 2022; Saldarriaga, 2023; Silva et al., 2021). A systematic review on HBM and COVID-19 found that perceived susceptibility, cues to action, perceived severity, self-efficacy, and perceived benefits are negatively associated with vaccine hesitancy, whereas perceived barriers are positively associated with it (Limbu et al., 2022). Recent evidence further shows that political affiliation plays an important role in shaping vaccine attitudes, as Saldarriaga (2023) found through machine learning analyses of U.S. county-level data that Republican voting share was one of the strongest predictors of COVID-19 vaccine hesitancy, particularly for strong hesitancy.
Among U.S. college students, previous studies have shown that age, gender, and race are associated with vaccine hesitancy. For example, Silva et al. (2021) found that female and non-White students reported lower levels of vaccine hesitancy. Gilbert-Esparza et al. (2023) found that undergraduate students aged 27 and older exhibited greater vaccine hesitancy than those aged 18–26. In addition, American Indian or Alaska Native students showed higher hesitancy than Asian and Black students (Gilbert-Esparza et al., 2023).
Existing research suggests that the effects of key predictors may differ depending on individuals’ levels of misinformation exposure and trust (Figueiras et al., 2021; Hanson et al., 2022; Smith, 2011; Tan et al., 2015). For instance, race, education, and health status influence both the use of and trust in health information sources (Figueiras et al., 2021; Smith, 2011). Trust in healthcare providers and pharmaceutical companies predicts vaccine acceptance (Hanson et al., 2022), while exposure to health misinformation has shown delayed effects on young people’s health beliefs, intentions, and behaviors (Tan et al., 2015).
However, no empirical study has systematically examined whether the relationships between vaccine hesitancy and its predictors differ across misinformation exposure–trust subgroups. Understanding these subgroup-specific patterns is crucial for developing targeted interventions. This study addresses this gap by examining whether health beliefs and demographic factors show differential associations with vaccine hesitancy across the four subgroups. In doing so, it provides a more nuanced understanding of the psychological and social dynamics underlying vaccine decision-making in a complex information environment. Therefore,
Method
Data collection and sample characteristics
Students from four Southeastern U.S. universities completed an online Qualtrics survey between March and May 2021. This was a period when individuals were still receiving COVID-19 vaccinations based on Centers for Disease Control and Prevention (CDC) recommendations, while some had already been fully vaccinated (Centers for Disease Control and Prevention [CDC], 2021). IRB approvals were obtained from the College of Charleston (IRB-2021-03-13-223945), University of Central Florida and Florida International University (STUDY00002875), and University of South Carolina (Pro00109697).
A total of 903 responses were collected. Participants who failed the attention check, withheld vaccination status, were outside the 18–40 age range, or had response times under 1 minute or over 2 hours, were excluded. After applying these criteria, the final analytical sample consisted of 819 participants. Among participants, 64.1% were female (n = 525), with an average age of 20.5 years (SD = 2.9). The majority identified as White (n = 454, 55.4%), followed by Hispanic/Latino (n = 175, 21.4%), Black/African American (n = 78, 9.5%), and Asian (n = 44, 5.4%). Participants reported having a relatively liberal political ideology (M = 3.39, SD = 0.96; 1 = very conservative, 5 = very liberal) and fairly good health (M = 3.22, SD = 0.72), as measured by a six-item, five-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. Additionally, 28.1% (n = 230) of participants reported receiving at least one dose of the vaccine at the time of data collection.
The complete survey questionnaire is provided in the Appendix.
Measures
Misinformation exposure
This study used five widely circulated COVID-19 vaccine misinformation items from Loomba et al. (2021), representing diverse and non-overlapping themes of misinformation about vaccination (see Table 1).
Exposure and trust percentages for pieces of COVID-19 vaccine misinformation.
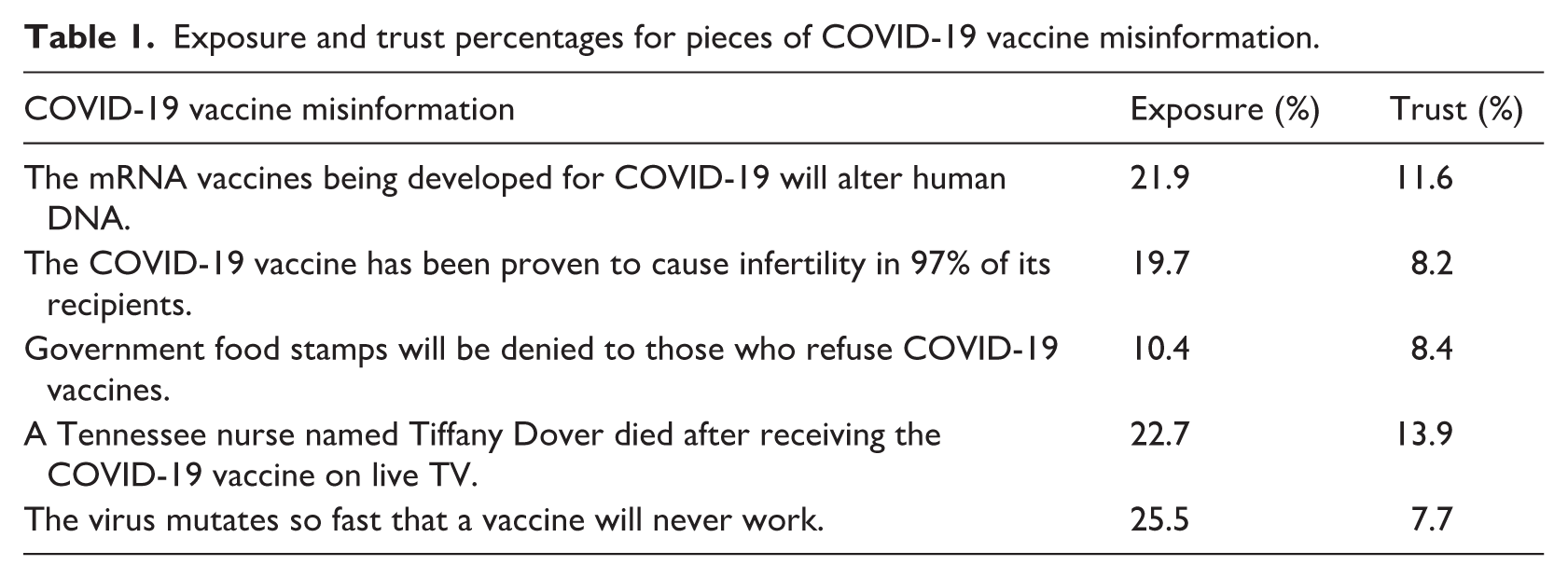
To assess misinformation exposure, participants were asked to indicate whether they had encountered similar content for each item (Neely et al., 2022). A score of 1 was assigned for each item they had seen, and 0 for those they had not. The total misinformation exposure score was computed by summing responses across all five items, ranging from 0 to 5 (M = 1.00, SD = 1.32).
Misinformation trust
Similar to the measurement of misinformation exposure, participants were asked to assess the trustworthiness of the five misinformation items. They received a score of 1 for trusting an item and 0 for not trusting it. The total trust in misinformation score was derived by summing responses across all five items, ranging from 0 to 5 (M = 0.50, SD = 1.00).
Perceived severity and perceived susceptibility
Following the work of Agarwal (2014) and Witte et al. (1996), perceived severity was measured by asking participants to rate how dangerous COVID-19 was to them (1 = not dangerous, 5 = very dangerous; M = 2.86, SD = 1.29); Perceived susceptibility was measured by asking participants to indicate how likely it was for them to get infected with COVID-19 compared to others (1 = very unlikely, 5 = very likely; M = 2.78, SD = 1.08).
Perceived realistic and symbolic threat
Adapting items from Kachanoff et al. (2021), perceived realistic threat was assessed by asking participants how much of a threat the COVID-19 outbreak was to their personal health, financial safety, and day-to-day life in their local community (1 = not at all, 5 = a great deal; M = 3.56, SD = 0.84, Cronbach’s α = 0.61).
Similarly, perceived symbolic threat was measured using a five-point Likert scale (1 = not at all, 5 = a great deal). Participants were asked how much of a threat the COVID-19 outbreak was to American democracy, what it means to be American, the rights and freedoms of the U.S. population, American values and traditions, and the maintenance of law and order in America (M = 3.05, SD = 1.11, Cronbach’s α = 0.89).
Perceived vaccine efficacy
According to Nan et al. (2012) and Hwang (2020), perceived vaccine efficacy was assessed using a 6-item, 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). Representative items included: “I believe the COVID-19 vaccine is effective in preventing COVID-19” (M = 3.93, SD = 0.96, Cronbach’s α = 0.90).
Perceived vaccine safety
Adapted from Nan et al. (2012), perceived vaccine safety was measured using a four-item, five-point Likert scale (1 = strongly disagree, 5 = strongly agree). Participants rated their agreement with statements reflecting concerns about the potential risks of the COVID-19 vaccine. Representative items include: “I worry that the COVID-19 vaccine might have unknown long-term side effects.” All items were reverse-coded (M = 2.62, SD = 1.10, Cronbach’s α = 0.88).
Vaccine hesitancy
Vaccine hesitancy was measured using a two-step approach (Chaudhary et al., 2021; Shen, 2024). Participants were first asked to indicate their current COVID-19 vaccination status. Those who reported having received at least one dose of the vaccine were classified as having no vaccine hesitancy (coded as 0). For those who reported not receiving any doses, vaccine hesitancy was measured by a follow-up question: “How likely do you intend to get the COVID-19 vaccine when it becomes available to you?” Responses were recorded on a five-point scale from 1 = very likely to 5 = very unlikely (M = 1.69, SD = 1.65).
Demographic measures
Age, biological sex, race, political ideology, and health condition were included as covariates. Biological sex was coded as male (0) and female (1), and race was categorized as non-White (0) and White (1). Political ideology was measured on a five-point scale ranging from 1 = very conservative to 5 = very liberal. Health condition was assessed using a six-item Likert scale (1 = strongly disagree, 5 = strongly agree). Representative items include “My health is excellent” (Cronbach’s α = 0.68).
Data analysis strategy
First, we conducted descriptive analyses to examine data distributions and assess the reliability of measurement scales.
Second, to address
Next, we used the four misinformation exposure–trust subgroups as the independent variable. For
A series of power analyses were conducted for the regression models predicting vaccine hesitancy in the full sample (n = 819) and across four misinformation exposure–trust subgroups (ns = 56–601). A recent meta-analysis (Yenew et al., 2023) examining HBM predictors of COVID-19 vaccination intention found significant associations across all constructs, suggesting medium-to-large effect sizes (approximately f2 = 0.13–0.55). Accordingly, a large effect size (f2 = 0.35) was adopted for the present power analysis. According to G*Power, the achieved power to detect a large-sized effect (f2 = 0.35) at α = 0.05 with 11 predictors was 1.00 in the full sample. For the four misinformation exposure–trust subgroups, the achieved power ranged from 0.77 to 1.00, depending on subgroup sample size.
There were 18% missing values in the variable of perceived severity. The pattern of missing data was examined using Little’s MCAR test (Jamshidian and Jalal, 2010). Results indicated that the data were missing completely at random (p = 0.10), supporting the use of multiple imputation for handling missing values. Missing data were handled using the multivariate imputation by chained equations (MICE) method in R. Ten imputations were generated via predictive mean matching (Little, 1988). Comparison of the original and imputed data distributions indicated no substantial discrepancies (Lee et al., 2018). For the ANOVA on perceived severity, results were consistent across the 10 imputed datasets; those from the first dataset were reported as representative. For all regression analyses, pooled coefficient estimates were derived from the imputed datasets.
All statistical analyses were conducted using IBM SPSS Statistics (Version 27) and the R statistical environment. Data preprocessing and k-means clustering analyses were performed in SPSS. Linear regressions were conducted in R using the base stats package (lm). Missing data were handled via multiple imputation using the mice package (m = 10, predictive mean matching), and coefficients and R2 were pooled following Rubin’s rules. The MissMech package was used to assess the missing data mechanism (Little’s MCAR test). Additional diagnostics and tests employed car (VIF), rstatix (Levene’s test, ANOVA, post hoc), janitor (contingency tables), and dplyr for data wrangling. Data visualization was performed using the ggplot2 package.
Results
Exposure to and trust in misinformation
As shown in Table 1, participants’ exposure to individual misinformation items ranged from 10.4% to 25.5%, and trust ranged from 7.7% to 13.9%, indicating generally low levels of both exposure and trust. The most frequently encountered claim was “The virus mutates so fast that a vaccine will never work,” followed by “A Tennessee nurse named Tiffany Dover died after receiving the COVID-19 vaccine on live TV” and “The mRNA vaccines being developed for COVID-19 will alter human DNA,” each seen by over 20% of participants. The highest trust was reported for the Tiffany Dover claim, followed by the mRNA vaccine claim, with at least 10% of participants expressing trust in each.
Formulation of the misinformation exposure-trust subgroups (RQ1)
To address
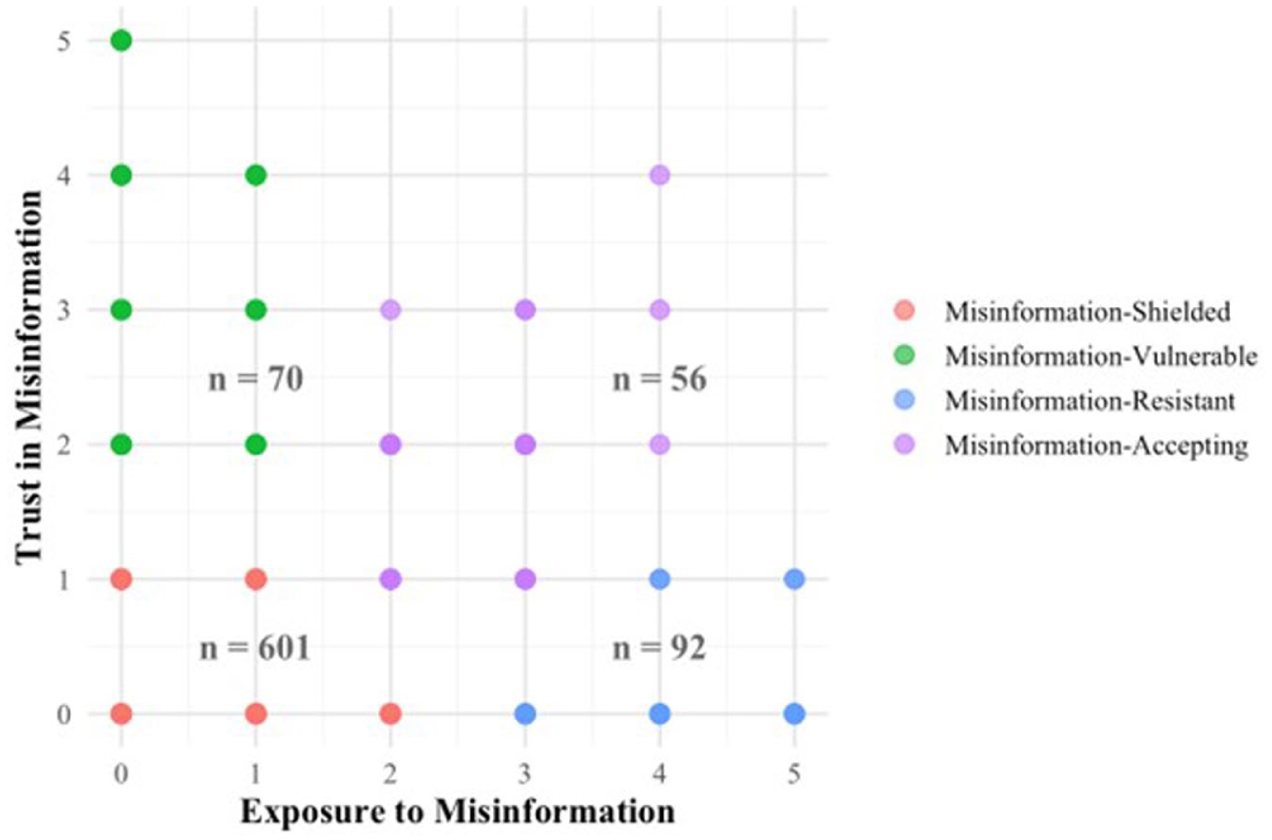
Four misinformation exposure-trust subgroups.
According to ANOVA results on misinformation exposure and trust, both exposure and trust were significantly associated with subgroups identified by cluster classification [exposure: F(3, 815) = 671.08, p < 0.001, η2 = 0.71; trust: F(3, 815) = 869.11, p < 0.001, η2 = 0.76]. As shown in Figure 1, misinformation exposure levels were significantly higher in the misinformation-resistant (M = 3.78, SD = 0.88) and the misinformation-accepting (M = 2.48, SD = 0.60) subgroups, compared to the misinformation-shielded (M = 0.52, SD = 0.71) and the misinformation-vulnerable (M = 0.26, SD = 0.44) subgroups. Similarly, trust in misinformation was significantly higher in the misinformation-vulnerable (M = 3.14, SD = 1.08) and misinformation-accepting (M = 1.48, SD = 0.71) subgroups, compared to the misinformation-shielded (M = 0.17, SD = 0.37) and misinformation-resistant subgroup (M = 0.04, SD = 0.20) subgroups. These results confirmed that the four subgroups reflected the expected patterns of misinformation exposure and trust.
Group difference in demographic characteristics (RQ2)
Means (standard deviations) or percentage of demographic variables across subgroups.
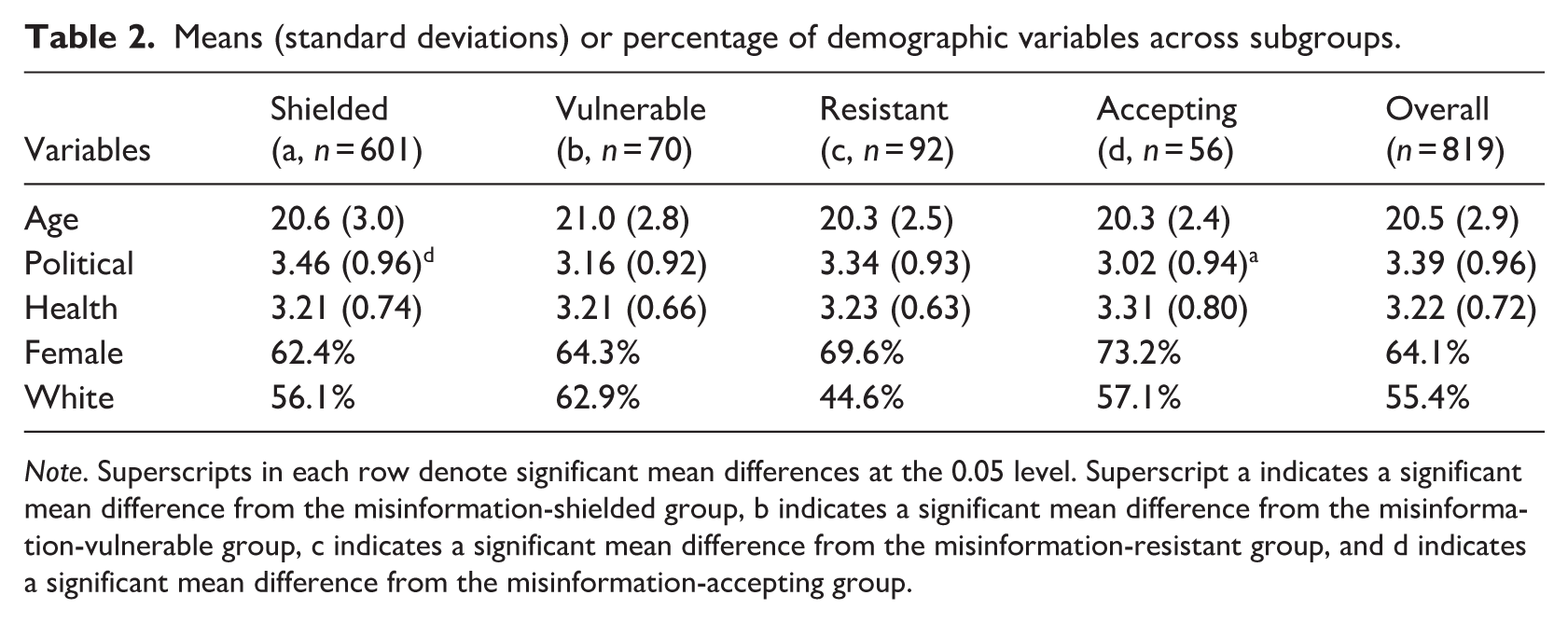
Note. Superscripts in each row denote significant mean differences at the 0.05 level. Superscript a indicates a significant mean difference from the misinformation-shielded group, b indicates a significant mean difference from the misinformation-vulnerable group, c indicates a significant mean difference from the misinformation-resistant group, and d indicates a significant mean difference from the misinformation-accepting group.
A chi-square test of independence was conducted to examine the association between biological sex and the misinformation exposure–trust subgroups. The result was not statistically significant [χ2 (3) = 3.69, p = 0.30], indicating that sex distribution did not vary meaningfully across subgroups. Across the subgroups, the proportion of female participants ranged from 62.4% in the misinformation-shielded subgroup to 73.2% in the misinformation-accepting subgroup. Nevertheless, these differences were not statistically significant. Similarly, a chi-square test was conducted to assess the relationship between race (White vs. non-White) and subgroup membership. The result was also not statistically significant [χ2 (3) = 6.13, p = 0.11], indicating no meaningful differences in racial composition across the four subgroups. The proportion of White participants ranged from 44.6% in the misinformation-resistant subgroup to 62.9% in the misinformation-vulnerable subgroup.
Group difference in vaccine hesitancy and health beliefs (RQ3)
Means (standard deviations) of vaccine hesitancy and health beliefs across subgroups.
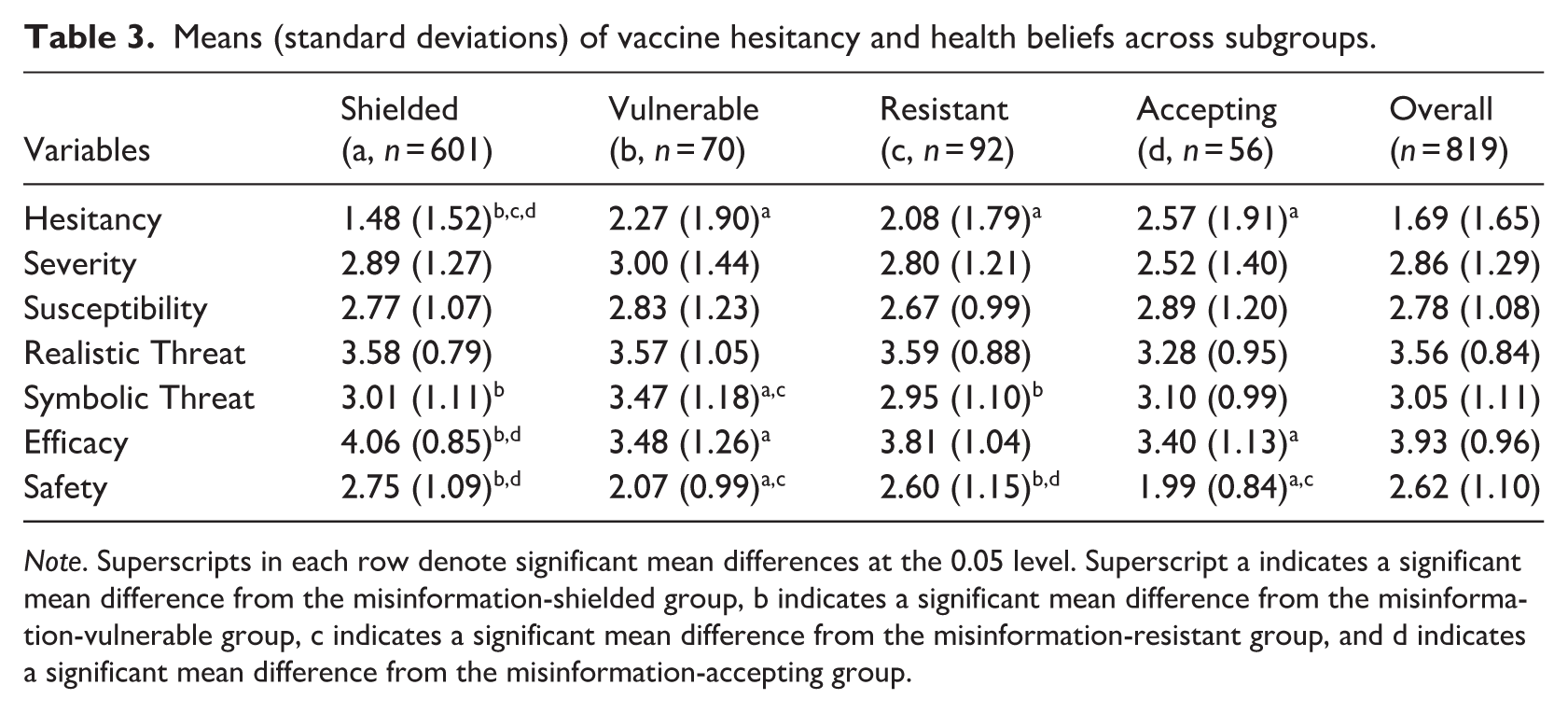
Note. Superscripts in each row denote significant mean differences at the 0.05 level. Superscript a indicates a significant mean difference from the misinformation-shielded group, b indicates a significant mean difference from the misinformation-vulnerable group, c indicates a significant mean difference from the misinformation-resistant group, and d indicates a significant mean difference from the misinformation-accepting group.
Results revealed a significant difference in vaccine hesitancy among the four subgroups [F(3, 815) = 13.89, p < 0.001, η2 = 0.05]. Post hoc comparisons showed that the misinformation-shielded subgroup (M = 1.48, SD = 1.52) reported significantly lower hesitancy than the misinformation-vulnerable (M = 2.27, SD = 1.90), misinformation-resistant (M = 2.08, SD = 1.79), and misinformation-accepting (M = 2.57, SD = 1.91) subgroups. No significant differences were observed among the latter three.
In contrast, no significant differences emerged in perceived severity [F(3, 815) = 1.73, p = 0.16, η2 = 0.01], and post hoc comparisons confirmed that all pairwise differences were non-significant. Similarly, perceived susceptibility did not differ significantly across subgroups [F(3, 813) = 0.55, p = 0.65, η2 = 0.002], indicating a generally consistent perception of susceptibility among participants.
Results for perceived realistic threat also showed no significant subgroup differences [F(3, 815) = 2.29, p = 0.08, η2 = 0.01], with post hoc comparisons confirming similar levels of perceived realistic threat across all subgroups. However, a significant difference was observed in perceived symbolic threat [F(3, 814) = 3.91, p = 0.01, η2 = 0.01]. Specifically, the misinformation-vulnerable subgroup (M = 3.47, SD = 1.18) reported significantly higher levels of perceived symbolic threat than both the misinformation-shielded (M = 3.01, SD = 1.11) and misinformation-resistant (M = 2.95, SD = 1.10) subgroups. No other comparisons reached significance.
A robust difference was found in perceived vaccine efficacy [F(3, 815) = 15.70, p < 0.001, η2 = 0.06]. The misinformation-shielded subgroup (M = 4.06, SD = 0.85) reported significantly higher efficacy beliefs than the misinformation-vulnerable (M = 3.48, SD = 1.26) and misinformation-accepting (M = 3.40, SD = 1.13) subgroups, while no significant differences were found between the misinformation-shielded and misinformation-resistant subgroups (M = 3.81, SD = 1.04) or among other comparisons.
Finally, perceived vaccine safety also varied significantly across subgroups [F(3, 815) = 15.39, p < 0.001, η2 = 0.05]. The misinformation-shielded subgroup (M = 2.75, SD = 1.09) and the misinformation-resistant subgroup (M = 2.60, SD = 1.15) reported significantly higher safety beliefs than the misinformation-vulnerable (M = 2.07, SD = 0.99) and misinformation-accepting (M = 1.99, SD = 0.84) subgroups.
Group difference in predictors of vaccine hesitancy (RQ4)
Multivariable linear regression models predicting vaccine hesitancy.
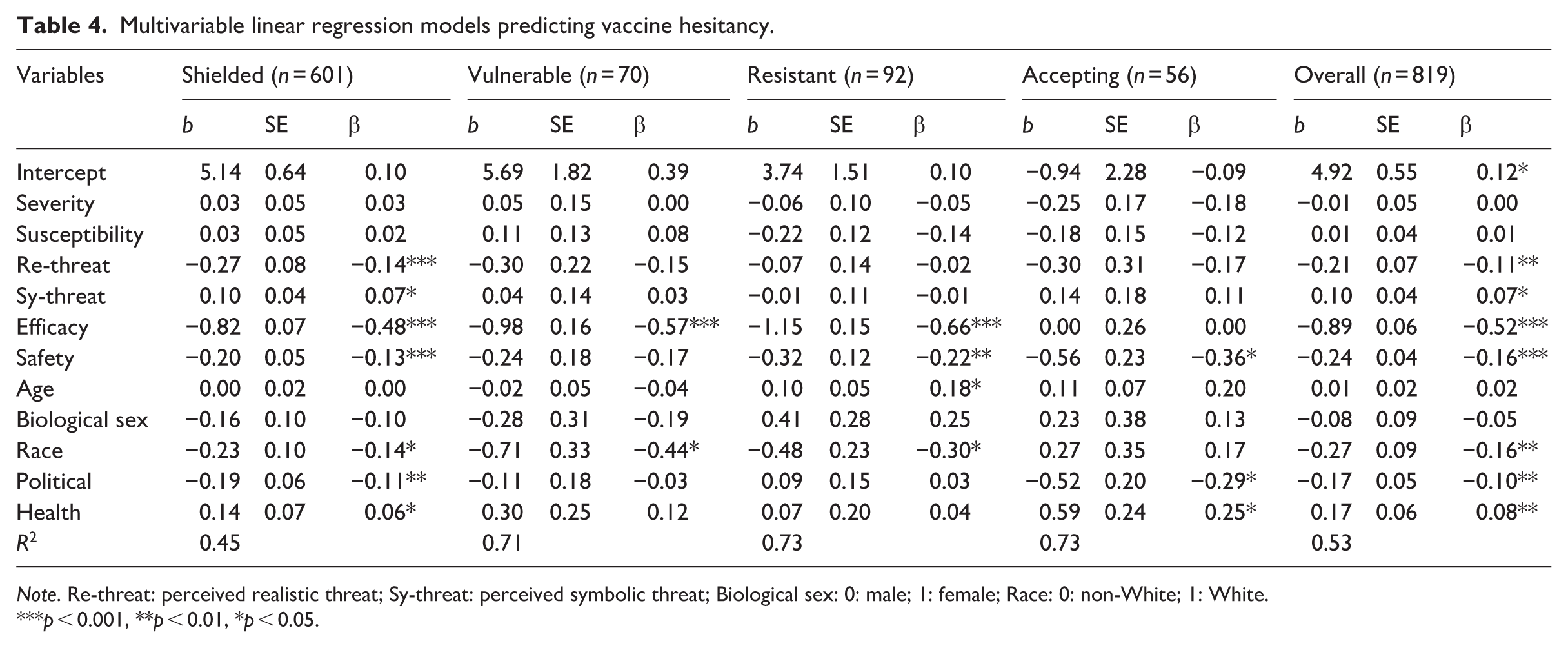
Note. Re-threat: perceived realistic threat; Sy-threat: perceived symbolic threat; Biological sex: 0: male; 1: female; Race: 0: non-White; 1: White.
p < 0.001, **p < 0.01, *p < 0.05.
Moreover, regression results revealed distinct patterns of association across the four subgroups. In the misinformation-shielded subgroup, several variables were significantly associated with vaccine hesitancy. Perceived symbolic threat (β = 0.07, p = 0.02) and health condition (β = 0.06, p = 0.046) were positively related to vaccine hesitancy. In contrast, perceived realistic threat (β = −0.14, p < 0.001), perceived vaccine efficacy (β = −0.48, p < 0.001), vaccine safety (β = −0.13, p < 0.001), race (β = −0.14, p = 0.02), and political ideology (β = −0.11, p = 0.001) were negatively associated with vaccine hesitancy. For the misinformation-vulnerable subgroup, only perceived vaccine efficacy (β = −0.57, p < 0.001) and race (β = −0.44, p = 0.04) were significantly and negatively associated with vaccine hesitancy. No other health belief or demographic variable showed a significant relationship. Regarding the misinformation-resistant subgroup, age (β = 0.18, p = 0.045) was positively associated with vaccine hesitancy. Conversely, perceived vaccine efficacy (β = −0.66, p < 0.001), vaccine safety (β = −0.22, p = 0.009), and race (β = −0.30, p = 0.04) were negatively associated with vaccine hesitancy. Among individuals in the misinformation-accepting subgroup, health condition (β = 0.25, p = 0.03) emerged as a significant positive predictor of vaccine hesitancy. In contrast, perceived vaccine safety (β = −0.36, p = 0.02) and political ideology (β = −0.29, p = 0.02) served as significant negative predictors (see Table 4).
Discussion
This study identifies four subgroups based on individuals’ exposure to and trust in COVID-19-related misinformation. Our findings outline their demographic and psychographic profiles and reveal distinct psychological mechanisms underlying vaccine hesitancy across these groups. These patterns inform both theoretical understanding and practical interventions.
Misinformation exposure–trust framework
In this study, we conceptualize individuals’ susceptibility to COVID-19 vaccine misinformation through two interrelated dimensions: misinformation exposure and trust. Rather than viewing these as transient media behaviors or state-level effects, we treat them as relatively stable psychological traits and cognitive structures linked to demographic factors and, more importantly, to vaccine-related health beliefs and hesitancy.
Through cluster analysis, we identified four misinformation exposure–trust subgroups: misinformation-shielded (low exposure, low trust), misinformation-vulnerable (low exposure, high trust), misinformation-resistant (high exposure, low trust), and misinformation-accepting (high exposure, high trust). The misinformation-shielded subgroup comprised the largest portion of participants (73.4%), while the remaining groups each accounted for 6.8%–11.2%. Although most participants appeared relatively protected from misinformation’s influence, a notable minority exhibited high exposure, high trust, or both.
The clear differentiation among these four subgroups indicates that misinformation exposure and trust are not necessarily aligned. Some individuals remain unexposed yet skeptical (shielded), whereas others encounter little misinformation but trust it highly (vulnerable), suggesting that susceptibility may stem more from cognitive or motivational factors than from exposure itself. Conversely, misinformation-resistant individuals demonstrate that high exposure does not necessarily translate into belief acceptance, possibly reflecting stronger critical thinking toward unverified sources. In contrast, misinformation-accepting individuals combine both high exposure and high trust, representing a high-risk subgroup that should be prioritized for corrective or inoculation-based interventions.
Political ideology emerged as an important demographic factor shaping the exposure–trust structure, with the misinformation-shielded subgroup being significantly more liberal than the misinformation-accepting subgroup. This pattern aligns with Rasul and Ahmed’s (2023) findings that conservatives hold more negative perceptions of vaccines. Such ideological divides in misinformation exposure and trust likely reflect broader partisan differences in attitudes toward science and vaccination (Calvillo et al., 2020). Accordingly, vaccine-related attitudes may represent expressions of individuals’ overarching worldviews rather than mere issue-specific knowledge or perceptions.
Interestingly, no significant subgroup differences were found in age, biological sex, race, or health conditions. This demographic homogeneity challenges assumptions about the demographic determinants of misinformation vulnerability (Dhanani and Franz, 2022). One possible reason is that college students are typically similar in age, education, and socioeconomic background (Jager et al., 2017; Wild et al., 2022), leading to limited variance in these attributes and reduced explanatory power of demographic factors. Instead, variations in COVID-19–related health beliefs may better account for subgroup differences within this relatively uniform population.
Health belief differences across misinformation exposure–trust subgroups
Our results reveal significant subgroup differences in vaccine hesitancy, with the misinformation-shielded group reporting markedly lower hesitancy than all others. This supports the protective effect of both low exposure to and low trust in misinformation. Notably, the misinformation-vulnerable, misinformation-resistant, and misinformation-accepting groups exhibited comparable levels of hesitancy despite differing exposure–trust patterns. This suggests that either high exposure or high trust alone may be sufficient to heighten vaccine hesitancy.
The significantly stronger perception of vaccine efficacy among the misinformation-shielded subgroup and the higher perception of vaccine safety among the misinformation-shielded and misinformation-resistant subgroups underscore the close relationship between these vaccine beliefs and misinformation trust, with exposure playing a secondary role.
The lack of significant differences in perceived severity, susceptibility, and realistic threat across subgroups was unexpected, suggesting that these beliefs may be shaped by factors beyond misinformation exposure and trust, such as personal experiences or broader public health messaging. This highlights the nuanced role of the HBM (Subedi et al., 2025) in explaining health-related attitudes and behaviors.
Group differences in the mechanisms behind vaccine hesitancy
The most revealing finding is the distinct pattern linking health beliefs, demographics, and vaccine hesitancy across subgroups. Among the misinformation-shielded subgroup, hesitancy appears more reflective, associated with both realistic and symbolic threats. This suggests that their hesitancy stems from broader considerations, such as personal livelihood and national values. Vaccine-related beliefs consistently predict hesitancy. Vaccine efficacy predicts hesitancy in all but the misinformation-accepting subgroup, where high exposure and trust may override its influence, while vaccine safety remains significant in all but the misinformation-vulnerable subgroup. Their high trust despite low exposure may reflect deeper institutional distrust, indicating that hesitancy may arise more from skepticism toward science than from safety concerns.
Personal identity factors such as health condition and political ideology significantly predict vaccine hesitancy in the misinformation-shielded and misinformation-accepting subgroups, where aligned exposure and trust (both low or both high) may reduce cognitive dissonance (Festinger, 1957). This alignment allows identity factors to serve as shortcuts guiding health decisions. In contrast, the misaligned misinformation-vulnerable and misinformation-resistant subgroups likely experience greater dissonance and depend more on vaccine-related beliefs, as shown by the stronger effects of efficacy and safety perceptions. Prior studies have also suggested that cognitive dissonance may help explain vaccination attitudes, as individuals often resist or reinterpret vaccine information that conflicts with their preexisting beliefs or social identities (e.g. Equils et al., 2023; Pearce and Cooper, 2021).
Practical implications
Our findings have important implications for audience segmentation and tailored communication addressing vaccine hesitancy. The misinformation exposure–trust framework effectively differentiates subgroups with varying levels of hesitancy, identifying priority targets for intervention. Compared with the misinformation-shielded group, the misinformation-vulnerable, misinformation-resistant, and misinformation-accepting groups show higher hesitancy and thus warrant tailored strategies. Broadly, interventions should aim to reduce misinformation exposure and trust through algorithmic adjustments (Zhang et al., 2025), corrective messaging (Bode and Vraga, 2018), or media literacy initiatives (Droog et al., 2025). At the subgroup level, strategies should align with key determinants: for instance, emphasizing vaccine efficacy for the misinformation-vulnerable, combining efficacy and safety messages with transparency for the misinformation-resistant, and prioritizing safety for the misinformation-accepting. Overall, the exposure–trust framework offers a stepwise approach, from identifying subgroups to targeting their psychological determinants, for designing effective interventions to mitigate vaccine hesitancy.
Limitations and future directions
Despite its contributions, this study has several limitations that also suggest directions for future research: First, the clustering analyses were data-driven and relative to this sample’s distribution; thus, the identified clusters and criteria may not be directly generalizable. Future studies should replicate the clustering framework with larger and more diverse samples to test the stability and external validity of these subgroup patterns. Second, regarding sampling, participants were college students from four universities in the southeastern United States, where vaccine hesitancy may differ from other regions (Maleki and Ghahari, 2024). This limits generalizability to broader populations. College students also tend to be younger, more educated, and more media literate, showing greater discernment toward misinformation (Hargittai and Hinnant, 2008; Jones-Jang et al., 2021), resulting in a disproportionately large misinformation-shielded subgroup (73.4%). Future work should include participants across age, education, and geographic contexts to enhance representativeness and statistical balance across clusters. Third, misinformation exposure was measured by the diversity rather than the frequency of misinformation encountered, which may have affected subgroup classification. For example, those repeatedly exposed to a single misinformation type may differ from those encountering multiple types. Additionally, the relatively low reliability of the perceived realistic threat measure (α = 0.61) may limit related findings. Vaccine hesitancy was defined behaviorally, classifying vaccinated individuals as non-hesitant; although consistent with WHOs’s (2014) definition, this may underestimate hesitancy among those vaccinated under external mandates. Future research should refine these measures to strengthen construct validity and reliability.
Footnotes
Appendix
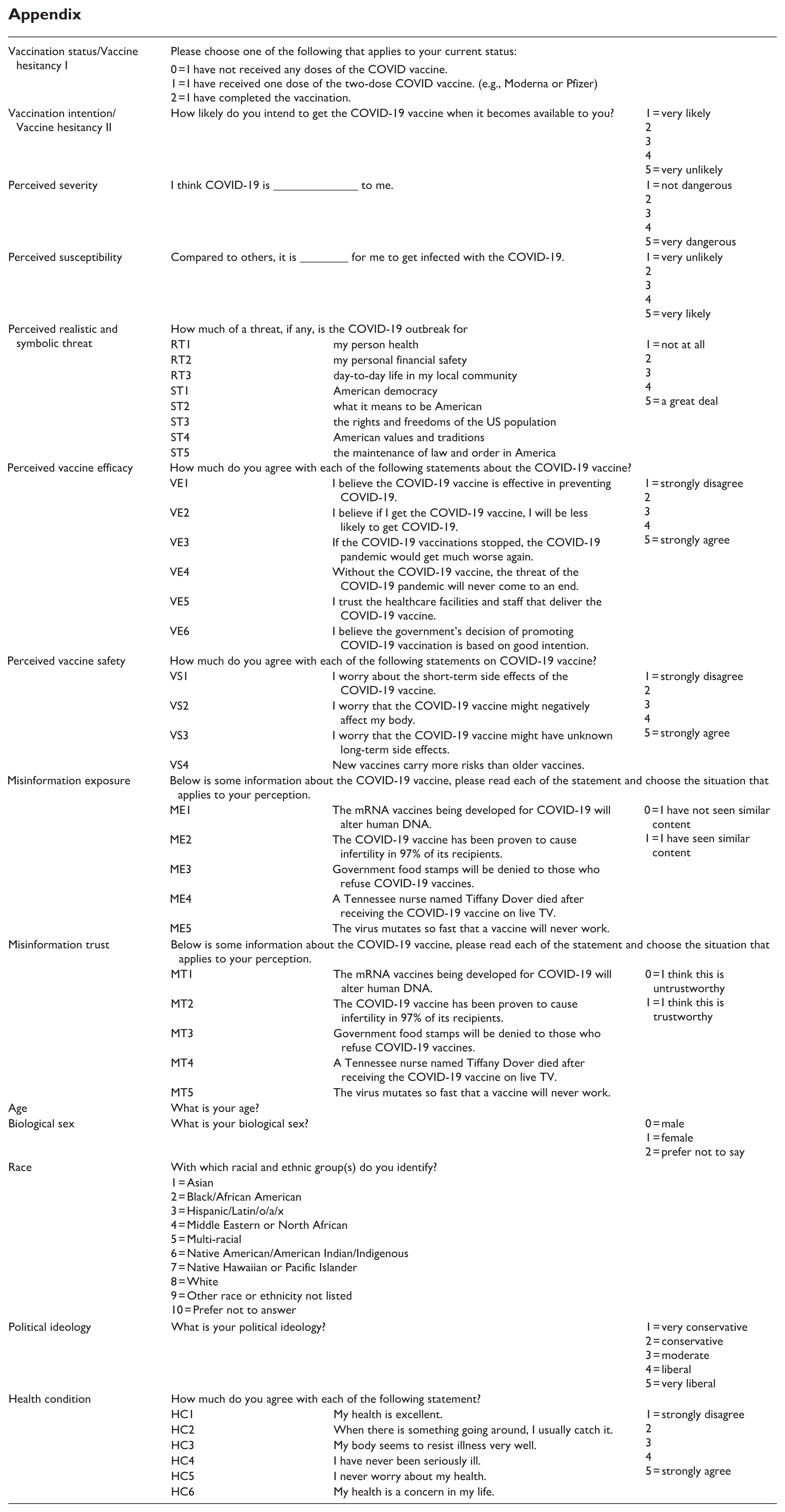
| Vaccination status/Vaccine hesitancy I | Please choose one of the following that applies to your current status: | ||
| 0 = I have not received any doses of the COVID vaccine. 1 = I have received one dose of the two-dose COVID vaccine. (e.g., Moderna or Pfizer) 2 = I have completed the vaccination. |
|||
| Vaccination intention/Vaccine hesitancy II | How likely do you intend to get the COVID-19 vaccine when it becomes available to you? | 1 = very likely 2 3 4 5 = very unlikely |
|
| Perceived severity | I think COVID-19 is ______________ to me. | 1 = not dangerous 2 3 4 5 = very dangerous |
|
| Perceived susceptibility | Compared to others, it is ________ for me to get infected with the COVID-19. | 1 = very unlikely 2 3 4 5 = very likely |
|
| Perceived realistic and symbolic threat | How much of a threat, if any, is the COVID-19 outbreak for | ||
| RT1 | my person health | 1 = not at all 2 3 4 5 = a great deal |
|
| RT2 | my personal financial safety | ||
| RT3 | day-to-day life in my local community | ||
| ST1 | American democracy | ||
| ST2 | what it means to be American | ||
| ST3 | the rights and freedoms of the US population | ||
| ST4 | American values and traditions | ||
| ST5 | the maintenance of law and order in America | ||
| Perceived vaccine efficacy | How much do you agree with each of the following statements about the COVID-19 vaccine? | ||
| VE1 | I believe the COVID-19 vaccine is effective in preventing COVID-19. | 1 = strongly disagree 2 3 4 5 = strongly agree |
|
| VE2 | I believe if I get the COVID-19 vaccine, I will be less likely to get COVID-19. | ||
| VE3 | If the COVID-19 vaccinations stopped, the COVID-19 pandemic would get much worse again. | ||
| VE4 | Without the COVID-19 vaccine, the threat of the COVID-19 pandemic will never come to an end. | ||
| VE5 | I trust the healthcare facilities and staff that deliver the COVID-19 vaccine. | ||
| VE6 | I believe the government’s decision of promoting COVID-19 vaccination is based on good intention. | ||
| Perceived vaccine safety | How much do you agree with each of the following statements on COVID-19 vaccine? | ||
| VS1 | I worry about the short-term side effects of the COVID-19 vaccine. | 1 = strongly disagree 2 3 4 5 = strongly agree |
|
| VS2 | I worry that the COVID-19 vaccine might negatively affect my body. | ||
| VS3 | I worry that the COVID-19 vaccine might have unknown long-term side effects. | ||
| VS4 | New vaccines carry more risks than older vaccines. | ||
| Misinformation exposure | Below is some information about the COVID-19 vaccine, please read each of the statement and choose the situation that applies to your perception. | ||
| ME1 | The mRNA vaccines being developed for COVID-19 will alter human DNA. | 0 = I have not seen similar content 1 = I have seen similar content |
|
| ME2 | The COVID-19 vaccine has been proven to cause infertility in 97% of its recipients. | ||
| ME3 | Government food stamps will be denied to those who refuse COVID-19 vaccines. | ||
| ME4 | A Tennessee nurse named Tiffany Dover died after receiving the COVID-19 vaccine on live TV. | ||
| ME5 | The virus mutates so fast that a vaccine will never work. | ||
| Misinformation trust | Below is some information about the COVID-19 vaccine, please read each of the statement and choose the situation that applies to your perception. | ||
| MT1 | The mRNA vaccines being developed for COVID-19 will alter human DNA. | 0 = I think this is untrustworthy 1 = I think this is trustworthy |
|
| MT2 | The COVID-19 vaccine has been proven to cause infertility in 97% of its recipients. | ||
| MT3 | Government food stamps will be denied to those who refuse COVID-19 vaccines. | ||
| MT4 | A Tennessee nurse named Tiffany Dover died after receiving the COVID-19 vaccine on live TV. | ||
| MT5 | The virus mutates so fast that a vaccine will never work. | ||
| Age | What is your age? | ||
| Biological sex | What is your biological sex? | 0 = male |
|
| Race | With which racial and ethnic group(s) do you identify? | ||
| 1 = Asian |
|||
| Political ideology | What is your political ideology? | 1 = very conservative |
|
| Health condition | How much do you agree with each of the following statement? | ||
| HC1 | My health is excellent. | 1 = strongly disagree |
|
| HC2 | When there is something going around, I usually catch it. | ||
| HC3 | My body seems to resist illness very well. | ||
| HC4 | I have never been seriously ill. | ||
| HC5 | I never worry about my health. | ||
| HC6 | My health is a concern in my life. | ||
Ethical Considerations
IRB approvals were obtained from College of Charleston (IRB-2021-03-13-223945), University of Central Florida and Florida International University (STUDY00002875), and University of South Carolina (Pro00109697).
Consent to participate
Participants provided informed consent prior to participating in the survey.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data underlying this article will be shared at a reasonable request to the corresponding author.*