
Abstract
The mental health of young women at risk of HIV exposure and early pregnancy, remains understudied. This study contributed to this research gap by exploring the mental health experiences of young mothers affected by HIV in South Africa. We conducted 17 semi-structured interviews with 18–24-year-old young mothers in the Eastern Cape, South Africa, 12 of whom were living with HIV. Interviews were recorded, transcribed, and analysed using a reflexive thematic approach. Young mothers showed diverse understandings and articulation of their day-to-day experiences of mental well-being. Many participants felt overwhelmed and stressed by the sudden transition into motherhood, as they were unprepared for the significant changes it brought into their lives. Additionally, this stress was heightened for young mothers living with HIV, who faced increased vulnerability to poor mental health, particularly where early motherhood intersected with the stigma associated with HIV.
Introduction
Young women living within Sub-Saharan Africa remain at the highest risk of the human immunodeficiency virus (HIV) epidemic globally, with over 20 million people living with HIV (UNAIDS, 2024). According to UNAIDS (2024), young people aged 15–24 accounted for 44% of all new HIV infections globally in 2023. Adolescent girls and young women continue to be disproportionately affected compared to males in the same age group (UNAIDS, 2024). Additionally, a survey conducted in all nine provinces in South Africa has shown that adolescent girls and young women experience high rates of unintended pregnancies, increasing the likelihood that pregnancy and motherhood co-occur with HIV (Human Sciences Research Council (HSRC) 2023). A qualitative study has highlighted various factors that contribute to HIV acquisition and unintended pregnancies in this country, including structural factors linked to gendered power relations, chronic poverty, and financial insecurity (Adeagbo, 2019). Furthermore, young mothers living in resource-limited settings are also more likely to have premature delivery, low birth weight and infant mortality (Hill et al., 2015). However, little is known about the lived experiences of young mothers affected by HIV in South Africa and how factors such as poverty, stigma and limited social support intersect with mental health to impact the psychosocial well-being of these young women.
Adolescence and young adulthood are critical phases where significant changes occur, such as the onset of puberty, exploration of identity and sexuality (Backes and Bonnie, 2019). Living with HIV and becoming pregnant during these stages entail major transitions for adolescent girls and young women, as they move into an unplanned and unknown reality with multiple new dimensions—HIV diagnosis, motherhood, and the familial and social changes linked to both (Adeagbo, 2019; Jochim et al., 2021). When an unintended pregnancy and HIV co-occur, young women may experience dual stigma, and typically have limited access to social and healthcare support services (Toska et al., 2020). In such contexts, motherhood often becomes stressful. These stressors are typically linked to the increased emotional and psychological stress of having a child while young, struggling financially, and experiencing societal stigma—while managing unfulfilled educational and career aspirations, and, in some cases, postnatal depression (Adeagbo, 2019; Jochim et al., 2021; Laurenzi et al., 2021). An unintended pregnancy may intensify existing social and contextual factors, creating additional stressors that result in poor mental health outcomes (Jochim et al., 2021). However, despite the extent of these challenges, the mental health of young women remains under-explored, especially in the context of factors that may exacerbate the effect of one another, when they co-occur—such as HIV and early motherhood (Roberts et al., 2022; Singer et al., 2017; Toska et al., 2020).
Global data indicates that a significant number of mental health conditions first emerge between the ages of 18 and 25 (Solmi et al., 2022). Poor mental health is a major contributor to the disease burden in South Africa and other parts of sub-Saharan Africa, and it is also associated with unintended pregnancies and HIV (Hill et al., 2015; Kuo et al., 2019; Vreeman et al., 2017). A study on mental health in South Africa found that one in six individuals experience mental illnesses such as anxiety, depression, and substance use disorders—with 40% of them also living with HIV (Pillay, 2019). Despite these findings, the mental health of vulnerable groups such as young women remains a neglected research and intervention gap, particularly in the context of overlapping factors such as HIV and early pregnancy (Roberts et al., 2022; Singer et al., 2017).
Importantly, the complex challenges encountered by young women affected by HIV, including pregnancy and motherhood without adequate support, are not experienced as single events, but rather as continuous and inter-related experiences. It is therefore important to explore the mental health experiences of young women in the face of multiple stressors such as HIV and motherhood to understand potential risks—but also to explore opportunities for mental health prevention and response. This study aimed to explore the experiences of pregnancy and early motherhood—particularly first pregnancies among young mothers aged 18–24 affected by HIV in the Eastern Cape, South Africa.
Methods
This study used an exploratory qualitative design to answer the following research questions:
What mental health challenges and experiences do young women aged 18–24 in the Eastern Cape encounter during the early stages of motherhood?
How do young women aged 18–24 experience stigma related to HIV and early motherhood in the Eastern Cape?
What factors contribute to the mental well-being of young mothers aged 18–24 living in the Eastern Cape?
Study setting
Study participants were recruited in Buffalo City Municipality, Eastern Cape Province, South Africa. The study’s research site is home to an ongoing longitudinal mixed methods study called HEY BABY (Helping Empower Youth Brought up in Adversity and their Babies and Young children) which has been following over 1000 young mothers and their children living in HIV-affected communities since 2017 (Toska et al., 2020). The Eastern Cape province has one of the highest HIV prevalence rates (18.8%) among youth aged 15–24 years (HSRC, 2023), which suggests that young women in this region are at higher risk of HIV than the average young women in South Africa. A separate study in the same region found that 71% of pregnancies among young women under 21 years were unplanned (Adeniyi et al., 2018). Overall, these studies provide an overview of the challenges related to HIV and early motherhood in the Eastern Cape emphasising the need for further investigation.
Sampling and participants
Participants were purposively recruited through the HEY BABY study participant pool, with support from the research infrastructure and team. Eligible participants were between the ages of 18–24 and had a single child between the ages of 1–3 years. Those with two or more children, those who were pregnant at the time of recruitment, or those with children older than 3 years were excluded from the study. This eligibility criteria enabled the research team to engage with a narrower scope of participants in exploring the questions of interest—young women’s experiences of pregnancy and motherhood with their first children.
Ethical considerations
This study received ethical approval from the Department of Psychology Ethics Review Committee at the University of Cape Town (PSY2022-035). Two trained research assistants experienced in working with young mothers, obtained written consent from all participants. Consent was conducted in the participants’ preferred language, either isiXhosa or English. Participants were assured of their privacy and confidentiality. Additionally, they were assured that they had the right to decline participating or withdraw in the study without any explanation. The study kept physical copies of consent without personal identifying information in a locked office, with scanned copies kept on a secure server.
Data collection
Data was collected by the lead author and two research assistants who collectively had multiple years of experience conducting research with adolescents and youth affected by HIV. Semi-structured interviews were conducted between September and December 2022 with individuals who met the eligibility criteria and consented to participate. We started by collecting sociodemographic questions to build rapport with the participants. During the interviews, open-ended questions were used to allow for flexibility and enable the participants to drive the conversation into emerging areas. Interviews were approximately 30–45 minutes long and each focused on three broad areas: (1) thoughts and feelings upon discovering about pregnancy and experiences of motherhood, (2) experiences of living with HIV (only for participants living with HIV), and (3) mental health experiences in relation to motherhood, stigma, and HIV. Additionally, interviews were mostly conducted in a mixture of isiXhosa and English, based on participants’ preference.
Data management and analysis
Immediately following the interviews, the lead author carried out transcription and translation of audio recordings. Interviews conducted in a mixture of isiXhosa and English were translated into English and transcribed verbatim, capturing all verbal and non-verbal cues such as tone and pauses. Furthermore, to ensure rigour, audio recordings were reviewed, transcripts were cross-checked and reviewed for errors. To protect their identities, all participants were given traditional South African pseudonyms at this stage.
The data were analysed using the reflexive thematic analysis approach, a data-driven method for identifying, analysing, and presenting themes from the dataset (Joy et al., 2023, pp. 1–2). The analysis involved importing all transcripts into Dedoose, a software programme for organising and analysing qualitative and mixed methods data (Lieber et al., 2021, pp. 1). Relevant sections of each transcript were transformed into codes, which were then clustered into themes based on their significance and meaning. Major themes and sub-themes were identified by the lead author through the development of a coding system. Additionally, all authors compared the different themes and organised them into coherent categories. The themes underwent further refinement and finalisation through feedback from the research team and consensus among all authors.
Trustworthiness of data
Ensuring trustworthiness in qualitative research is important in terms of establishing the credibility and reliability of qualitative findings given their subjective nature (Ahmed, 2024). The concept of trustworthiness in qualitative research includes credibility, dependability, and confirmability.
Credibility
This refers to the degree to which findings accurately reflect the participants’ actual experiences. Additionally, establishing trust and rapport with participants enables the researcher to gain nuanced insights into their experiences, behaviours, and beliefs (Ahmed, 2024). During the recruitment process research assistants informally engaged with the participants to build rapport and create an environment of mutual respect. Additionally, the research assistants had existing relationships with the participants since they were part of a larger study (HEY BABY).
Dependability
To achieve dependability, researchers must ensure that the process is logical, traceable, and clearly documented. This allows for other researchers to reproduce the study (Ahmed, 2024). We maintained a detailed roster to systematically document each stage of the research process, ensuring transparency and consistency. In addition, qualified researchers independently reviewed the accuracy of data collection procedures, the rigor of the analysis, and the interpretation of findings. This process provided an additional layer of quality assurance and contributed to the credibility and trustworthiness of the study.
Confirmability
This refers to the guarantee that the study remains unaffected by biases or preferences of the researchers. This process includes peer debriefs, member checking and reflexive journaling (Ahmed, 2024). As a team, we held weekly debriefing sessions during the data collection and analysis phases to reflect on the interviews conducted, discuss potential referrals, and emerging themes. Debriefings also served as an opportunity to engage in reflexivity, enabling the research team to acknowledge their own assumptions and positionalities, and to consider how these could influence the interpretation of data. By creating a structured process for collective reflection, the team sought to strengthen the rigour of the study, enhance the validity of findings, and minimise the risk of researcher bias.
Researcher reflexivity
Qualitative researchers are a critical part of generating data during the research process as they are deeply embedded in the world where data collection happens (Dodgson, 2019). As the researcher, I occupied a dual insider–outsider role. As a young, childless university graduate, I differed from most participants—many of whom were still in high school or had dropped out—limiting our shared life experiences. However, I drew on elements of shared identities—being a young Xhosa-speaking African woman of similar age and cultural background which provided common understandings, ease and comfortability. I became interested in exploring mental health because, in many African contexts, there are no direct translations for these concepts. This absence of terminology often creates the impression that mental health challenges are less relevant or less prevalent in these settings. However, the lack of a direct word or translation does not mean that these experiences do not exist; rather, they may be expressed, understood, and addressed in culturally specific ways.
Results
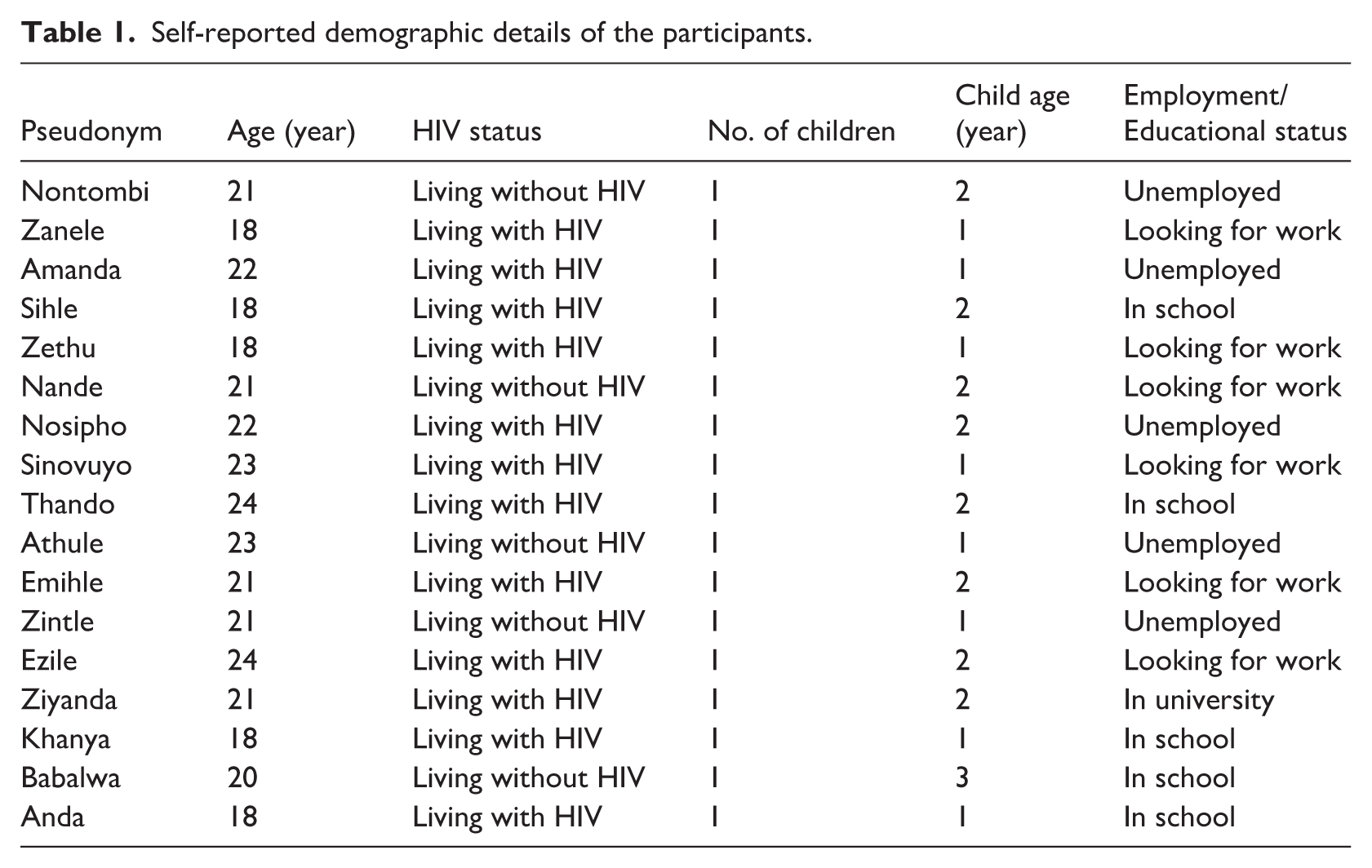
The study enrolled a total of n = 17 adolescent girls and young women, aged 18–24 years, with a mean age of 20.8 years. Of these participants, 12 (70.6%) were living with HIV, while 5 (29.4%) were living without HIV. Six participants (35.3%) were either in high school or enrolled in tertiary education, six (35.3%) were actively looking for work at the time of data collection, and five (29.4%) were unemployed and not looking for work. All participants had one child, between 1 and 3 years of age at the time of data collection. A detailed participant self-reported demographic information is shown below in Table 1.
Self-reported demographic details of the participants.
Participants shared their experiences of early motherhood, stigma and HIV as well as reflected on how these experiences affected their mental health. Three major themes were identified: (1) mental health shaped by distinct stressors during pregnancy, (2) navigating critical life events, (3) imagined futures and pathways to mental well-being.
Mental health shaped by distinct stressors during pregnancy
Young mothers described their mental health as shaped by unique and interrelated stressors during pregnancy and early motherhood.
Diverse understandings and experiences of mental health
Participants were asked about their understandings of the concept of mental health, and how they would describe their own mental health in their own words. These descriptions were diverse and captured different understandings of mental health, which were related to lived experiences and social interactions. Participants’ understanding of mental health was influenced by various factors, including cultural background, personal beliefs, and societal norms. Generally, these understandings were very personal, and removed from more technical or clinical psychological language. Nosipho explained her understanding of mental health as “when your brain is tired” (Nosipho, 22 years, living with HIV). Nontombi described her mental health in relation to complex emotions she experienced as a young mother. These emotions resulted from the guilt she experienced after she became pregnant and due to a lack of support from both her family and her child’s father.
You are facing challenges, and you are blaming yourself, you feel guilty because no one supports you. (Nontombi, 21 years, living with HIV)
Another young woman, Sinovuyo, described her mental health based on her experience of living with HIV. According to Sinovuyo, accepting her HIV status and adhering to her antiretroviral therapy (ART) translated into positive mental health: It [mental health] means I must continue taking my treatment so that I can be healthy.’.’.Like not thinking too much or be emotional about the fact that I am living with HIV. (Sinovuyo, 23 years, living with HIV)
Emotional and psychological transitions
Participants described pregnancy and motherhood as complex life transitions, noting that their pregnancies were often unplanned, leaving them feeling unprepared. Many shared that they faced significant difficulties in adjusting to these unexpected realities, and managing this transition was often perceived as both stressful and overwhelming: It was actually hard to accept it [motherhood], it took me a long time to deal with the fact that I am a mother. (Athule, 23 years, living without HIV) I felt stuck and like my life is going to change, I won’t be able to go out with my friends anymore. (Anda, 18 years, living with HIV)
Furthermore, young women described experiencing conflicting emotions about their new realities of having to balance individuality (taking care of their own needs as young women) and parenting (taking care for the physical and emotional needs of the child). Additionally, given that most of these young women’s pregnancies were unplanned, they expressed concerns about their ability to be adequate and capable parents to their children. Nontombi and Nande described these feelings of uncertainty and doubt in their own ways: I’m doubting myself because I’m not supposed to be a mother, I didn’t plan to be a mother. (Nontombi, 21 years, living without HIV) What has changed is that I am full of self-doubt. I’m doubting myself and sometimes I feel like I’m not good enough. So sometimes it’s difficult. (Nande, 21 years, living without HIV)
Moreover, some participants expressed feelings of regret, frustration, and self-blame. Feelings of regret were specifically related to how participants’ lives had changed since they became pregnant. Additionally, feelings of frustration and self-blame emerged from missed opportunities as a result of parenting—having to take care of a child made accessing opportunities such as employment even more complicated for these young women.
I mean everything didn’t go well like I was looking for a job, but I had to stop and take care of the baby.’.’.I don’t feel okay. I mean if I didn’t have a baby, I would’ve found a job by now. (Sinovuyo, 23 years, living with HIV)
Stressors linked to material and psychosocial needs
For several young mothers, there was a close connection between tangible, material stressors and their mental health. The connection between material stress and mental health emerged particularly from conversations around finances and resources available to them. As a result, young mothers described financial strain—being unable to afford necessities for the baby such as food, diapers, and clothing—as one of the main stressors affecting their mental health. Participants described the stress they experienced when they did not have financial means to provide for the child’s needs, particularly when the father of the child was also unemployed or unpresent: It’s stressful sometimes because I do run out of nappies when the father of the baby doesn’t have money, so I end up stressing. (Sinovuyo, 23 years, living with HIV) I am unemployed, and father of the baby is also unemployed so we would struggle sometimes with baby stuff. (Nosipho, 22 years, living with HIV)
For Nosipho, the father of her child was not actively involved in their child’s life and therefore did not provide any form of support. Nontombi’s family was also unable to assist financially, as they were dependent on social support grants: We are really struggling, and this baby doesn’t have a father, he ran away.’.’.So being a mother is not okay, there should be someone assisting you. Yes, I’m a mother but I need support cause I’m unemployed, I’m just sitting in this township. (Nontombi, 21 years, living without HIV)
Furthermore, for most of the young women, though not all, the father of the child either denied paternity, or was largely absent in the child’s life even if they did acknowledge their paternity. Young women described the shame, blame and stress they faced when their partner denied paternity of the child: So, let me talk about myself, my baby’s father decided not to be a part of our child’s life. So I raised my child by myself with the help of my grandmother.’.’.What would I do, cause his father denied him, so what would I do? (Amanda, 22 years, living with HIV)
Consequently, some of the young women had difficulties with accepting that they would be single parents. Despite his initial denial, Zintle hoped that the father of her baby would eventually acknowledge the paternity after birth: He denied the pregnancy and I said okay if you say so, but you will see when the baby is born. (Zintle, 21 years, living without HIV)
With the child’s father absent, the young woman and her family had to shoulder the financial and primary caregiving responsibilities for the child, creating significant challenges. This situation often placed a heavy burden on the young woman, who had to navigate the demands of parenting while potentially managing other responsibilities such as finding employment or returning to school.
Navigating critical life events
Coming to terms with HIV status from a young age
For participants living with HIV, learning about their HIV status at a young age marked a life-changing moment in their lives. The young women in this study shared that they all acquired HIV perinatally and learned of their status at various stages of their lives. Most of them found out between the ages of 7 and 13. Their parents or adult caregivers had kept their HIV status hidden to shield them from stigma. However, when they eventually learned the truth, they felt confused, hurt, and betrayed: I was hurt but I was still young, I didn’t know that this is something you live your entire life with. (Amanda, 22 years, living with HIV)
Additionally, one participant learned of her HIV status at the age of 16 when she went to the clinic for a pregnancy test. Prior to this, she had been taking medication, but she believed it was for diabetes. Khanya’s caregiver had encouraged her to take the medication, but never explained the actual reason for it.
They asked if I knew my status and I said yes but I was not aware. I said sugar diabetes then they said, no you don’t have sugar diabetes, you have HIV. But my aunt was not telling me that I have HIV.’.’.Yes, I was told that I must take medication and I was asking myself, what are these pills for? then I was told at the clinic that I have this problem like this HIV, that’s how I found out. (Khanya, 18 years old, living with HIV)
In summary, these findings emphasise the harmful effects of secrecy and non-disclosure regarding HIV on the well-being of those affected by the virus. Moreover, keeping HIV status hidden does not only negatively impact the mental and emotional health of individuals living with HIV but also contribute to the ongoing stigma and discrimination surrounding the condition.
Stigma linked to HIV and pregnancy
Participants spoke about experiences of HIV stigma and pregnancy stigma that negatively affected their mental health. However, for most participants, these two were not experienced simultaneously: some experienced either pregnancy stigma or HIV stigma, with only a few having described experiencing both of these stigmas. Athule shared that she experienced pregnancy-related stigma, which led her to intentionally isolate herself from others as a way to protect herself from further judgement within the community: There were a lot of people that were looking at me. So, I actually stayed at home during my pregnancy and there were also people that were gossiping about me. (Athule, 23 years, living without HIV)
Additionally, some of the young mothers described experiencing pregnancy-related stigma from their friends’ mothers and other elderly people within the community. These parents stigmatised pregnant girls and young women; they also had concerns that these young women would encourage or influence their own children into becoming pregnant at a young age. Zanele described how this experience made her feel: Some mothers used to say so-and-so’s child is not educated, she loves men, and she is now pregnant. So, things like that used to hurt me a lot. (Zanele, 18 years, living with HIV)
Furthermore, for young mothers living with HIV, the combined experience of HIV-related and pregnancy-related stigma was deeply overwhelming, regardless of whether the HIV stigma was a past experience or still ongoing. For young women who experienced both ongoing HIV-related stigma and pregnancy, their stories suggested that they developed internalised stigma in addition to perceiving stigma from others. This was the case for Ziyanda: her experience of externalised stigma contributed to the development of internalised stigma. Due to the stigma surrounding HIV, she had not fully come to terms with her HIV status; she experienced low self-esteem and struggled with trust issues when it came to disclosing her status to those close to her. In addition to these thoughts, Ziyanda was concerned about how people in the community talked about her, considering that her own family stigmatised her and discriminated against other people living with HIV.
I do live around people who talk negatively about HIV and things like that. For example, at home I do hear them.’.’. and I feel bad when they gossip about someone living with HIV and then I think for sure, in other households, this is how they talk about me. They do talk badly even in my presence, and they know about it, so I don’t know how they think I feel when they talk about someone else like that, who is in the same situation as me. (Ziyanda, 21 years, living with HIV).
In a similar experience, another young woman, Anda, expressed how one of her peers at school told her that they would never associate themselves with someone living with HIV. This made Anda think about how her classmates would respond and treat her if they were to discover her HIV status: One of them said they would never be friends with someone living with HIV and I was shocked cause here I am, and they talk to me, but I was wondering how they would react if they were to find out. (Anda, 18 years, living with HIV)
Furthermore, fear of HIV stigma was also expressed by young women living without HIV. One of the young women, Babalwa, was concerned about how people in her community might perceive her if she were to acquire HIV.
Let’s say maybe I have HIV like, how will people treat me if ever I told them my status? How will they treat me, how will they look at me? (Babalwa, 20years, living without HIV).
Social isolation was a protective technique utilised by these young women to protect themselves from further stigma, particularly pregnancy-related stigma. During this isolation period, young women described feeling lonely, sad, and emotionally distressed. Despite the fact that the majority of participants did not explicitly describe mental health in clinical language, some of them expressed experiencing symptoms of depression, anxiety, and suicidality. Suicidality, in particular, was expressed with reference to HIV-related stigma. One of the participants, Amanda, described having suicidal thoughts and attempting suicide due to stigma she experienced within her social environment from her friends and people in the community: I once attempted suicide because of such things.’.’. People disclosed my private issues and I wanted to kill myself. (Amanda, 22 years, living with HIV)
In summary, young women reported experiencing stigma that made it difficult for them to disclose their HIV status, particularly within close relationships. This stigma significantly impacted their mental health and overall well-being, creating barriers to open communication and support from those around them.
Imagined futures and pathways to mental well-being
The final theme presents findings on how young mothers imagine pathways to mental well-being and stability. Young mothers described the different types of support they received from people in their social environments, as well as how that support enabled them to pursue their educational ambitions.
Having a support system contributed to the well-being of the young mothers who participated in the study. As a result, some of the young mothers described positive experiences of early motherhood, despite acknowledging that their pregnancies were unplanned. The support of family members, the child’s father, and friends was reported as crucial in helping young mothers navigate conflicting emotions: It [motherhood] wasn’t too difficult for me because I had a supportive family. (Thando, 24 years, living with HIV) Okay the kind of support that I get at home.’.’.. Like if they were different people, they would expect me look for someone that will take care of the baby when I’m at school. So, my grandmother looks after the baby when I’m at school. (Sihle, 18 years old, living with HIV)
Despite the stressors and conflicting emotions which emerged from the challenges of early motherhood without sufficient resources and support, most young women expressed feelings of happiness and fulfilment about their parenting experiences. Additionally, the young women also shared their positive experiences of motherhood and celebrated their positions as mothers which demonstrated their agency.
I’m happy about my life. Now I know that I have a someone to live for. (Ezile, 24 years, living with HIV) It [motherhood] has a positive impact because you get to experience a lot of things, things you didn’t know.’.’. (Anda, 18 years, living with HIV)
In the context of unintended pregnancies, having a support structure such as family and friends plays an important role in young mother’s lives. Support also enabled them to process and deal with their internal emotions as they transitioned into motherhood. Additionally, many of the young women remained optimistic about their future and aspired to pursue further studies: I want to study law and build a house for my family and have a nice life somewhere. (Sihle, 18 years, living with HIV)
These young mothers saw education as an opportunity to regain control over their lives and create a better future, not only for themselves, but also for their children. Consequently, the pursuit of education was seen as a means to empower themselves, break the cycle of adversity, and build a brighter future for their families.
Discussion
Our findings illuminate the complexities of mental health challenges experienced by young mothers affected by or living with HIV, which are shaped by intersecting factors. Young mothers, regardless of their HIV status, described stressors which negatively affected their mental health—such as limited financial and psychosocial support, the double burden of HIV stigma and stigma associated with being a young mother, having to discontinue school following pregnancy, and other challenges of early motherhood. They did so in words that were grounded in personal experiences rather than scientific or clinical language linked to mental health. Additionally, this study highlights the need for a more nuanced understanding of the mental health issues faced by this population. It is evident that young mothers affected by and living with HIV have diverse and unique experiences when it comes to their mental health.
Pregnancy and childbirth involve a transition and the need to adapt to new a reality for every woman (Adeagbo and Naidoo, 2021). However, our study found that young women experience additional challenges due to the unplanned nature of their pregnancies. Young women’s pregnancies are unique as they experience a transition from girlhood into motherhood while simultaneously undergoing critical developmental changes (Wycoff et al., 2024). Consequently, they struggle to cope with their new roles and responsibilities as young mothers. Similar findings were demonstrated in previous qualitative research which explored young women’s experiences of early motherhood (Adeagbo, 2019; Mjwara and Maharaj, 2018). These studies have also shown that young mothers experience challenges with managing their own personal needs and the demands of raising a child.
Furthermore, young women in this study described experiencing intense and complex emotions regarding early motherhood such as fear, regret, and guilt. Feelings of guilt and uncertainty were specifically linked to structural changes and material challenges. Most participants either had to drop out of school or put their job search and furthering studies on hold—meaning that they perceived pregnancy and motherhood as burdens that would negatively impact their future.
Several studies in South Africa have indicated that young mothers frequently worry about how early motherhood will affect their future plans, particularly regarding unachieved educational and career goals (Jochim et al., 2021; Mjwara and Maharaj, 2018). Additionally, it is notable that most worries emerged from financial struggles as their unintended pregnancy added to the financial burden of the household. These findings are in line with previous research which has shown that young women are not only disappointed with the unintended nature of their pregnancies, but are more concerned about the impact of additional financial costs for an already-constrained household income (Mjwara and Maharaj, 2018; Wycoff et al., 2024). Notably, in such contexts unintended pregnancies may also exacerbate existing contextual factors such as poverty and food insecurity, creating additional stressors that result in poor mental health outcomes for young mothers (Jochim et al., 2021; Wycoff et al., 2024).
Moreover, living with HIV as a young woman presents with several emotional, social, and psychological challenges. Young women in this study reported experiencing profound levels of stigma and shared different ways in which they negotiated and navigated living with HIV. While some young women gradually accepted their HIV status, many participants in the study found this process to be challenging and detrimental to their mental health, leading some to either suicide attempts or experience of suicidal thoughts. These findings highlight the importance of recognising that the impact of stigma can extend far beyond a single incident or experience (Prizeman et al., 2023). Consequently, the memories and emotions associated with stigmatising incidents can resurface in various ways, potentially triggering anxiety, depression, or suicide ideation at later stage (Prizeman et al., 2023). Other qualitative studies have found that levels of HIV stigma remain high in South Africa, particularly among young women living with HIV (Brittain et al., 2023; Waldron et al., 2021), with diverse impacts such as social isolation, discrimination, psychological distress, and a reluctance to seek care or disclose their status.
Furthermore, young mothers who received social and financial support from their families indicated better overall mental health, regardless of their HIV status. This finding suggest that in the context of unintended pregnancy having a support structure, such as family and friends, plays an important role in young mothers’ lives. Social and financial support not only assisted them with raising their children, but also enabled them to process and deal with their internal emotions as they transitioned to motherhood. This finding highlights the importance of support in providing stability for young mothers and their children in the context of unintended pregnancy, it is also a protective factor enabling better mental health outcomes (Willan et al., 2020). Consequently, successfully navigating the transition into motherhood is likely to be influenced not only by individual factors, such as personal agency, but also by the support and resources available within one’s social environment (Willan et al., 2020). Additionally, this suggests that supporting young mothers requires a comprehensive approach that goes beyond individual empowerment, but also address structural factors such as financial support, childcare, education and access to healthcare.
Despite the diverse challenges and conflicting emotions experienced by young mothers, participants in this study were able to continue with their lives, held clear ambitions for the future, and were adamant about achieving their goals. Similar findings were reported in another study, which demonstrated that young mothers exercise agency by navigating multiple individual and structural barriers—choosing to continue their education during pregnancy and after childbirth despite facing shame and discrimination (Pillay, 2021).
Moreover, some of the young women in this study had positive experiences of motherhood, particularly those with existing support structures. For some, early motherhood presented an opportunity for self-growth, motivation, and maturity. Similar findings have been demonstrated in previous studies (Adeagbo, 2019; Mjwara and Maharaj, 2018). These findings suggest that positive experiences of early motherhood are also significant, and merit further discussion.
Limitations
The study has several limitations that merit consideration. All participants were interviewed at one timepoint, and no follow-ups were made. Following up on some participants could have potentially strengthened our insights into changes in experiences of mental health over time. In addition, the study did not include mothers younger than 18 years old due to ethical and logistical challenges of conducting research with minors on such a sensitive topic. Including a variety of young moms could have provided a broader overview or understanding of their mental health experiences. Finally, the findings are based on lived experiences of young mothers from the Eastern Cape, Buffalo City Municipality. Therefore, they cannot be transferred to other settings.
Implications for further research
This section presents a number of important considerations for future research. Firstly, future research could use a longitudinal approach to investigate how young women transition into motherhood and how they experience mental health over a certain time period. Mental health is not a static state, but rather a dynamic process that can change and evolve over time. Thus, it is important to explore young mothers’ mental health trajectories over a long period of time in order to understand their adjustment processes. Additionally, by studying the adjustment processes of young women affected by or living with HIV over an extended period, researchers can gain a deeper understanding of how their mental health fluctuates and how they adapt to various challenges and life transitions. This longitudinal approach will allow for a more comprehensive understanding of the factors that contribute to mental health outcomes along the life course and coping mechanisms of young mothers as well as understand the challenges faced during this period.
Secondly, the study sample included young women living with HIV and young women living without HIV. This aspect of the study, in addition to its qualitative nature, limits the scope by which overarching conclusions can be made about the mental health of young mothers more broadly. Further research could narrow their scope by focusing on either young women living with HIV or young women living without HIV, instead of having both sub-groups in the same sample. In particular, understanding the experiences of young women who acquire HIV during pregnancy or breastfeeding is an important research gap. In this way, future studies may be able to take a deeper dive into the unique mental health experiences of these two different groups of women.
Conclusion
In conclusion, this study contributes to the body of literature on how early motherhood, HIV stigma, and the social changes that precede these experiences affect young women’s mental health. In exploring the mental health experiences of young mothers affected by HIV, we found that mental health for this important group is a complex and multifaceted issue that is influenced by various factors, including the stigma of HIV and early motherhood, relationships with families and friends, and future goals and aspirations. It is essential to address these factors holistically and provide support, education, and resources to empower individuals to maintain positive mental well-being despite the challenges they may face. Furthermore, young mothers affected by HIV require tailored support from healthcare workers who understand the dual pressures of early parenting and living with a chronic condition. Ensuring that mental health services particularly counselling—are freely available is critical for promoting their wellbeing and reducing the emotional burden they often carry.
Footnotes
Acknowledgements
We would like to thank the entire HEY BABY team for their support and valuable contribution towards the success of this project. Special thanks to Lulama Sidloyi, Bongiwe Saliwe, Babalwa Taleni, Babalo Gqaleni-Ntozonke, and Dr Jane Kelly for their support with fieldwork management and data collection. Lastly and most importantly, we would like to extend our sincere gratitude to all the young women who participated in this study. We deeply appreciate your willingness to share your personal and emotional experiences with us.
Ethical considerations
The Ethics Review Committee of the Department of Psychology at the University of Cape Town approved this study (PSY2022-035).
Consent to participate
Respondents gave written consent for review and signature before starting interviews.
Participants gave both verbal and written consent to participate in the study.
Consent for publication
Participants gave informed consent for their anonymised data to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the UKRI GCRF Accelerating Achievement for Africa’s Adolescents (Accelerate) Hub [ES/S008101/1] and the University of Cape Town’s Financial Aid Office.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available upon request.*