
Abstract
Many older adults spend more than half of their time in sedentary behaviors that can lead to poor health outcomes, including declines in cognitive health. However, sedentary behaviors are diverse and can lead to different health outcomes. To determine the relationships between types of sedentary behaviors and cognitive health in older adults, we analyzed associations between sedentary behaviors and cognitive health among adults 50 years and older in the United States who participated in the Health and Retirement Study. We categorized sedentary behaviors based on the four domains of the Taylor taxonomy of sedentary behaviors. We found that certain categories of sedentary behaviors were positively associated with cognitive health in this population. These results support that the Taylor taxonomy can be used to identify sedentary behaviors that promote cognitive health and inform interventions that improve the quality of life of older adults.
Introduction
Many adults spend up to 60% of their waking hours in sedentary behaviors (e.g. sitting, reclining, lying down; Dempsey et al., 2020; Department of Health and Human Services, 2018; Katzmarzyk et al., 2019; Zou et al., 2024). These behaviors expend little energy (Tremblay et al., 2017) and are a risk factor for poor health, even independent of physical activity (Gibbs et al., 2015). As a result, international and national guidelines for physical activity recommend limiting sedentary behaviors (Dempsey et al., 2020; Department of Health and Human Services, 2018; Katzmarzyk et al., 2019). However, sedentary behavior is a lifestyle factor in many domains of daily living, including transportation, occupation, and leisure time based on Ecological Models of Health Behavior (Durand and Jáuregui, 2024; Sallis and Owen, 2015) and affect all ages (Zou et al., 2024). Although sedentary behaviors affect all ages, older adults have more sedentary behaviors than other age groups (Bauman et al., 2018; Harvey et al., 2013, 2015), so they have a greater risk for poor health outcomes.
Lifestyle factors, including sedentary behavior, have different associations with cognitive health in adults. Cognitive health and function encompass a range of abilities, including memory, attention, language, reasoning, problem-solving, and decision-making (Anderson and McConnell, 2007; Chen et al., 2022; Jedrziewski et al., 2007). Lifestyle factors that have positive associations with cognitive health include physical activity (Blondell et al., 2014; Larson et al., 2006; Ludyga et al., 2020; Northey et al., 2018), a Mediterranean diet (Lourida et al., 2013; Singh et al., 2014), social interaction and contact (Fung et al., 2011; James et al., 2011; Sommerlad et al., 2019), meditation (Gard et al., 2014), cognitive activity and mental stimulation (Vemuri et al., 2014; Wilson et al., 2012), and sleeping 7–8 hours per day (Wu et al., 2018). Conversely, lifestyle factors that have negative associations with cognitive health include tobacco smoking (Anstey et al., 2007; Peters et al., 2008; Sabia et al., 2012), chronic stress (Korten et al., 2017), sleep disturbances (Blackwell et al., 2014), poor social interaction (Kuiper et al., 2015), and perceived loneliness (Sundström et al., 2019). This dichotomous relationship between lifestyle factors and cognitive health is particularly important for reducing age-related cognitive decline and the risk of mortality later in life (Buckner, 2004; Ludyga et al., 2020), performing everyday activities (Hillman et al., 2008; Ludyga et al., 2020; Pinto et al., 2023; Raichlen et al., 2022, 2023; Stillman et al., 2020; Zou et al., 2024), and supporting overall well-being and independence (Kimura et al., 2023; Ren et al., 2024). Thus, a public health priority is to identify modifiable lifestyle factors that promote healthy cognitive aging (Huang et al., 2020).
Although the relationships among physical activity, brain health, and cognitive health have been extensively studied (Hillman et al., 2008; Ludyga et al., 2020; Stillman et al., 2020), the relationships among sedentary behaviors, brain health, and cognitive health are less well understood (Pinto et al., 2023; Raichlen et al., 2022, 2023; Zou et al., 2024). However, researchers have connected the type of sedentary behavior to changes in cognitive health, albeit with mixed results (Raichlen et al., 2022; Taylor et al., 2020; Zou et al., 2024). For example, television viewing for more than 3.5 hours per day was associated with cognitive decline (Fancourt and Steptoe, 2019). Also, among adults 60 years and older, regardless of physical activity, cognitively passive sedentary behaviors (i.e. television time) were associated with a greater risk of dementia, whereas cognitively active sedentary behaviors (i.e. computer time, board games, crafting, reading) were associated with a lower risk of dementia (de Rezende et al., 2014; Raichlen et al., 2022). Also, television viewing was associated with greater depression symptoms, whereas internet use was associated with lower depression symptoms (Loprinzi, 2019). These mixed associations between sedentary behavior and cognitive health and function were summarized in a systematic review: “The current body of evidence suggests sedentary behavior is negatively associated with cognitive function; however, the associations between sedentary behavior and cognitive function are complex and largely dependent on the exposure variable and outcomes assessed” (Falck et al., 2017: 809). This complexity contributes to challenges in understanding what sedentary behaviors account for different health outcomes.
To address these challenges, we developed the Taylor taxonomy of sedentary behaviors (Taylor, 2022). This taxonomy classifies sedentary behavior by four domains known as SNCC: (1) social interaction (i.e. not solitary, companionship, interacting, and connecting with others); (2) novelty (i.e. refreshingly new, unusual, or different); (3) choice (i.e. volition, preferred option, power, freedom, or decision to choose); and (4) cognition (i.e. mentally stimulating and engaging). Based on the classification, ratings are assigned to each behavior that indicate the degree (low, moderate, or high) to which the domain is observed. Based on the Taylor taxonomy, sedentary behaviors that rate high on the four domains would theoretically confer the greatest health benefits, whereas sedentary behaviors that rate low on the four domains would theoretically yield the least health benefits and could even be harmful. Thus, this new taxonomy established a comprehensive, integrated, and parsimonious conceptual framework to reconcile different health outcomes of sedentary behaviors.
Initially, the Taylor taxonomy of sedentary behaviors was developed for older adults. This population has more sedentary behaviors (e.g. television viewing consumes most non-working time) and concerns about psychological health (i.e. cognitive decline and dementia) than younger adults (Bauman et al., 2018; Harvey et al., 2013, 2015; Zou et al., 2024). Also, older adults are one of the fastest-growing demographic groups worldwide (Ortman et al., 2014). Thus, the Taylor taxonomy is a practical tool to classify, differentiate, and elucidate relationships between sedentary behaviors and cognitive health in older adults. In this study, we aimed to determine the relationship between sedentary behaviors and cognitive health among adults 50 years and older using the four domains of the Taylor taxonomy. We hypothesized that certain categories of sedentary behaviors would be negatively or positively associated with cognitive health in this population.
Materials and methods
Source of data
We obtained data from the Health and Retirement Study (HRS), a longitudinal panel study that surveys people older than 50 years in the United States (Fisher and Ryan, 2018). The “Core” survey is conducted biennially, with the first wave fielded in 1992, and a new cohort of people aged 51–56 years added every 6 years. In between Core interview waves, the HRS conducts off-year or supplemental studies. We obtained data from the HRS because (1) the data were collected from older adults and (2) the dataset has variables to test our hypotheses related to cognitive health and sedentary behaviors.
Transparency and openness
Data obtained from the HRS were de-identified and did not require approval from an institutional review board.
Demographics and basic health conditions
Our study used data from both the 2019 Consumption and Activities Mail Survey (CAMS) and the 2020 Core survey of the HRS. The 2020 Core survey included data from 15,723 records. Of these records, 721 used proxy interviews without self-rated memory, word recall, and serial sevens tests. These records were excluded from the analyses. Of the remaining 15,002 records, 4105 contributed data to the 2019 CAMS. Of those 4105 records, 185 were assigned zero 2019 CAMS weights and did not contribute to any analyses. Thus, our analytic sample included 3920 records.
Basic demographics were obtained from the Tracker file (2020 Tracker Early Version 3.0) of the HRS. Work for pay (yes/no at the time of the survey) was obtained from Section J of the 2020 Core survey, and basic health conditions were obtained from Section C of the 2020 Core survey. Table 1 presents the demographic and basic health conditions of the sample population, as well as descriptive statistics of hours per week of sedentary behaviors and physical activity.
Characteristics of the sample.
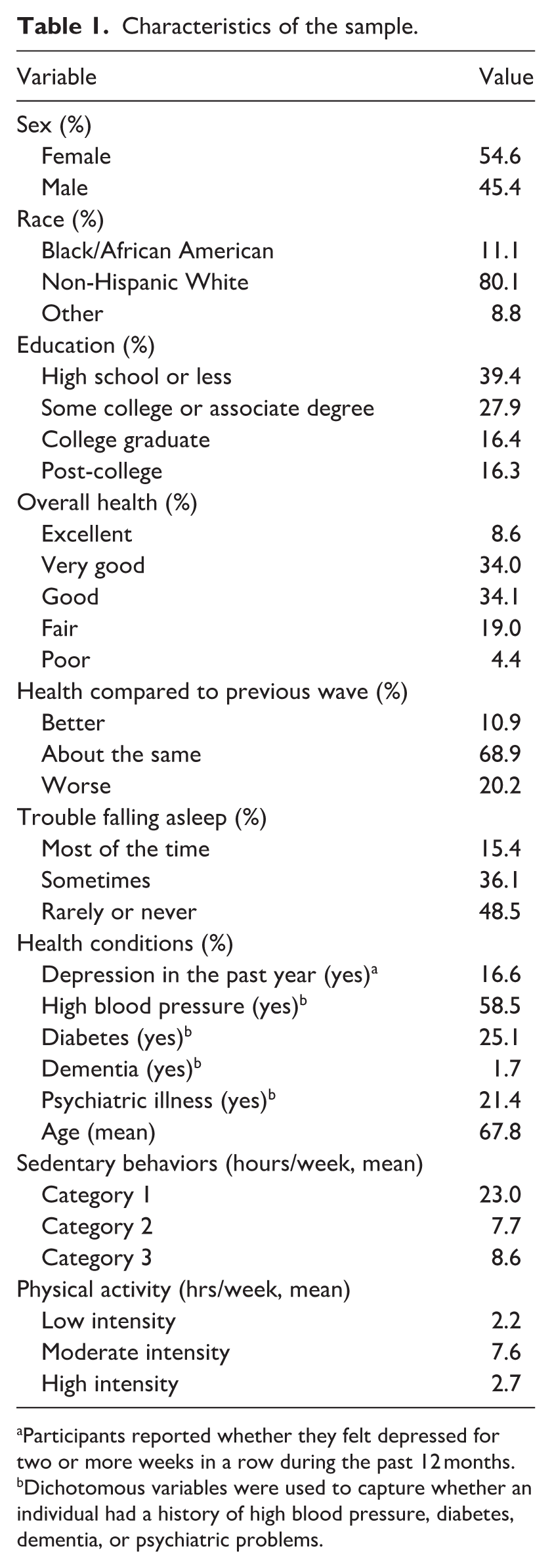
Participants reported whether they felt depressed for two or more weeks in a row during the past 12 months.
Dichotomous variables were used to capture whether an individual had a history of high blood pressure, diabetes, dementia, or psychiatric problems.
Cognitive health variables
Measures of cognitive health were obtained from Section D of the 2020 Core survey. These measures included self-rated memory, word recall, and serial sevens test results. For self-rated memory, participants were asked to rate their memory at the present time as excellent, very good, good, fair, or poor. For the word-recall task, participants were shown a list of 10 nouns. Then they were asked to recall as many words as possible from the list in any order as part of the immediate word-recall task. Approximately 5 minutes later, participants were asked to recall the same nouns again as part of the delayed word-recall task. For the serial sevens test, participants were asked to subtract 7 from 100 and continue subtracting 7 from each subsequent number 5 times.
Physical activity variables
Measures of physical activities were obtained from Section A of the 2019 CAMS. For physical activities, yard work or gardening were used to capture low-intensity physical activity, walking was used to capture moderate-intensity physical activity, and sports or other exercises were used to capture high-intensity physical activity. Physical activities were measured in hours per week.
Sedentary behavior variables
In the 2019 CAMS instructions for Section A, the questions did not specifically ask about sitting. For example, none of the following question stems were part of the HRS: “how often do you perform the following activities while sitting or lying down?” and “about how much time do you spend sitting down” (Kurita et al., 2022; León-Muñoz et al., 2013; Major et al., 2023). Because sitting was not explicitly measured in the HRS, two investigators independently reviewed the list of 33 activities in the HRS to identify sedentary behaviors (e.g. behaviors in a sitting or lying posture while awake). The investigators agreed on five sedentary behaviors and then classified those behaviors into three categories based on the Taylor taxonomy (Taylor, 2022) and previous research (Compernolle et al., 2021; Kesse-Guyot et al., 2012; Kikuchi et al., 2014; Leask et al., 2015; Loprinzi, 2019; Mitsutake et al., 2020; Palmer et al., 2019; Raichlen et al., 2022, 2023; Saunders et al., 2020; Taylor et al., 2020; Toepoel, 2013; Zou et al., 2024). In the Taylor taxonomy, category 1 sedentary behaviors are repetitive and tedious, category 2 behaviors are chosen and provide moderate novelty and mental stimulation, and category 3 behaviors are socially interactive, mentally stimulating, and involve novelty (Figure 1).
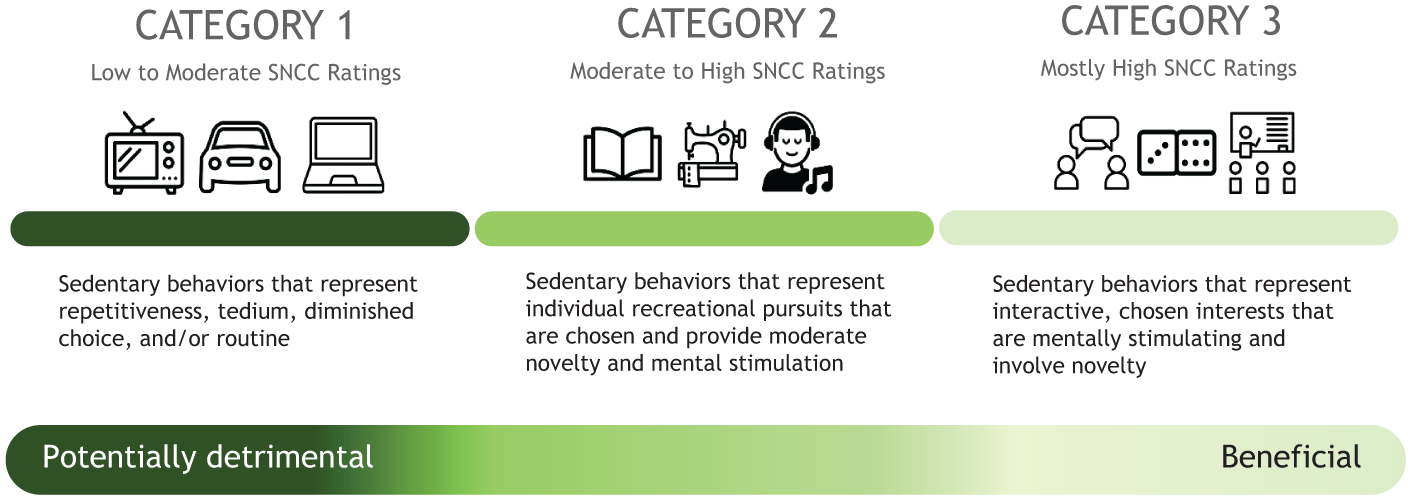
Categories of the Taylor taxonomy of sedentary behaviors. The four domains of the Taylor taxonomy are social interaction, novelty, choice, and cognition (SNCC). For each domain, sedentary behaviors are rated (low, moderate, and high) and then categorized (1, 2, and 3).
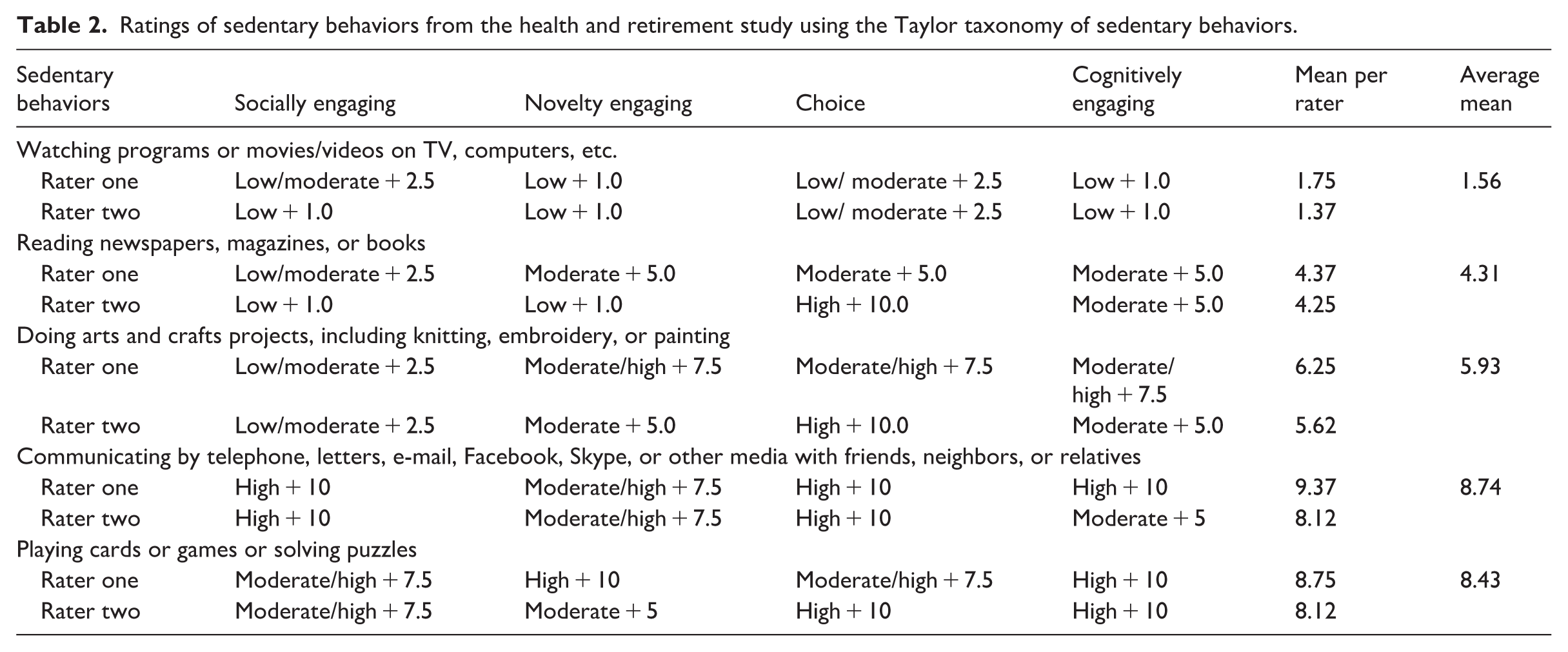
The two investigators rated each sedentary behavior on four domains from the Taylor taxonomy of sedentary behaviors (Table 2). The rating scale for each domain was high (10 points), moderate (5 points), and low (1 point). Then the means across the four domains were computed for each investigator/rater and averaged among the investigators (Table 2). Based on the average means, the investigators classified the five sedentary behaviors into three categories. Category 1 was rated low and included watching programs or movies/videos on TV and using computers (one sedentary behavior; average mean, 1.56). Category 2 was rated moderate and included reading newspapers, magazines, or books; and doing arts and crafts projects, including knitting, embroidery, or painting (two sedentary behaviors; average means, 4.31 and 5.93). Category 3 was rated high and included playing cards or games or solving puzzles; and communicating by telephone, letters, email, Facebook, Skype, or other media with friends, neighbors, or relatives (two sedentary behaviors; average means, 8.43 and 8.74; Table 2). Category 3 has a distinct emphasis on social interaction (Sommerlad et al., 2019; Toepoel, 2013). All these behaviors are engaged in while sitting or lying while awake and were measured in hours per week.
Ratings of sedentary behaviors from the health and retirement study using the Taylor taxonomy of sedentary behaviors.
Statistical analysis
The dependent variables were measures of cognitive health, including self-rated memory, word recall, and serial sevens test. The independent variable was sedentary behaviors placed in three categories. Ordinal logistic regression was used to examine the association between sedentary behaviors and self-rated memory. A positive estimated coefficient implied that a larger value in the explanatory variable was associated with a higher probability of being in a lower category rather than in a higher category. Because self-rated memory was reverse-coded (i.e. excellent is 1, poor is 5), being in a lower category implies better health. Linear regression was used to examine the association between sedentary behaviors and word recall. The total number of words recalled in immediate recall and delayed recall were the dependent variable. In each trial of the serial sevens test, participants received a 1 if the subtraction was correct and a 0 otherwise. The number of correct subtractions were summed over five trials. The serial sevens trials were treated as Bernoulli trials. Logistic regression was used to examine the association between sedentary behaviors and accuracy on the serial sevens test (i.e. the odds of making a correct subtraction).
All analyses included the same set of covariates, including physical activities, demographics, and basic health conditions. In SAS/STAT 15.1, the SURVEYREG procedure was used for linear regression, the SURVEYLOGISTIC procedure was used for binary logistic and ordinal logistic regression, and the SURVEYFREQ and SURVEYMEANS procedures were used to generate descriptive statistics. All analyses used the 2019 CAMS weights.
Results
To determine the relationship between sedentary behavior and cognitive health, we analyzed three categories of sedentary behaviors and three measures of cognitive health. For self-rated memory, we found a positive association between categories 2 and 3 sedentary behaviors and self-rated memory (category 2: p = 0.018; category 3: p = 0.005). More hours of category 2 or 3 sedentary behaviors were associated with greater self-rated memory. The association between category 1 sedentary behaviors and self-rated memory was not significant (p = 0.156; Table 3).
Associations between sedentary behaviors and self-rated memory and word recall.
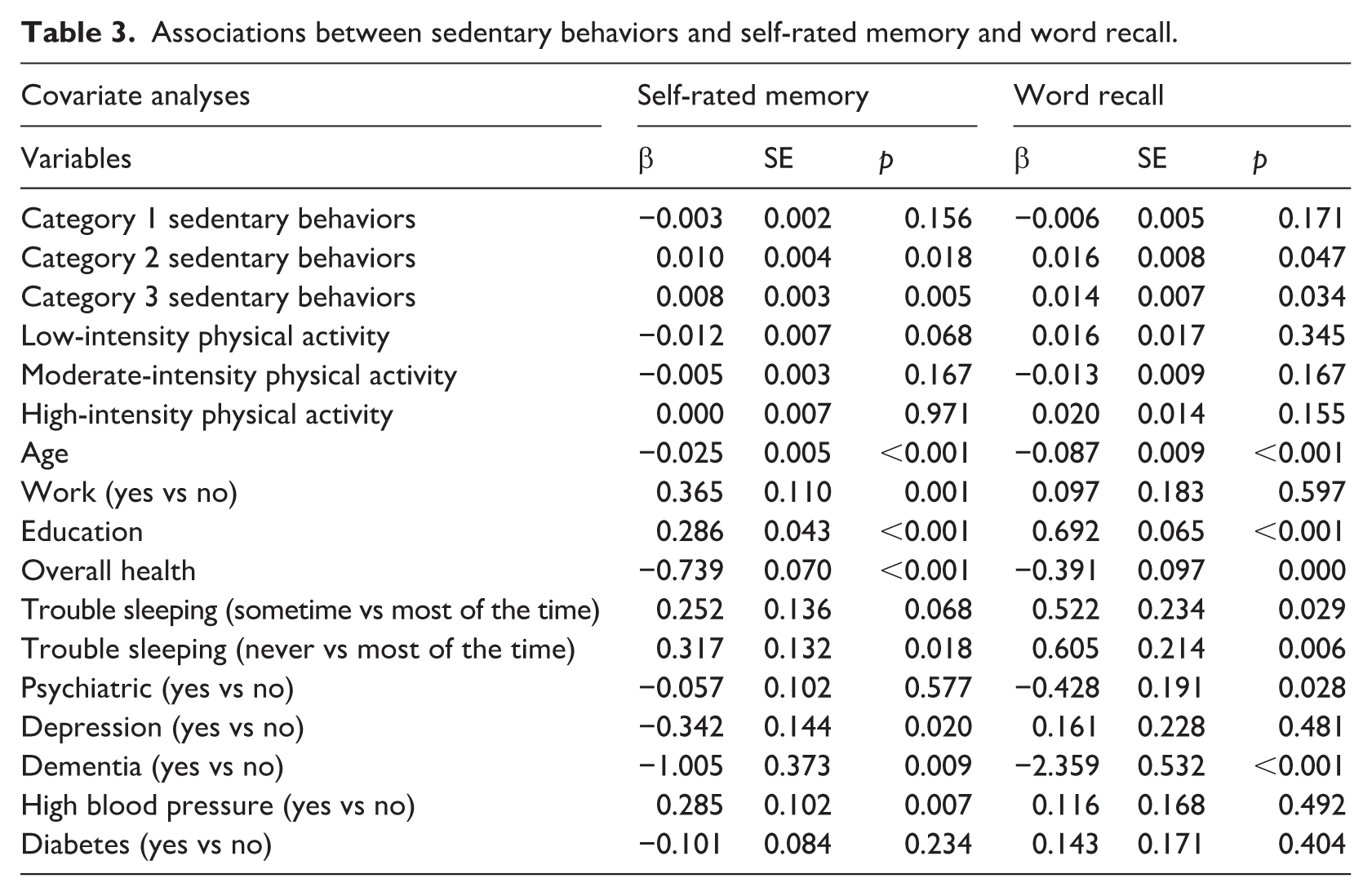
For word recall, we found that more hours of category 2 or 3 sedentary behaviors were associated with more words recalled (category 2: p = 0.047; category 3: p = 0.034). The association between category 1 sedentary behaviors and word recall was not significant (p = 0.171; Table 3). For subtraction, more hours of category 2 sedentary behaviors were associated with greater odds of performing a correct subtraction (p = 0.029). The association between category 1 and 3 sedentary behaviors and the odds of performing a correct subtraction were not significant (category 1: p = 0.209; category 3: p = 0.239; Table 4).
Associations between sedentary behaviors and accuracy in the serial sevens task.
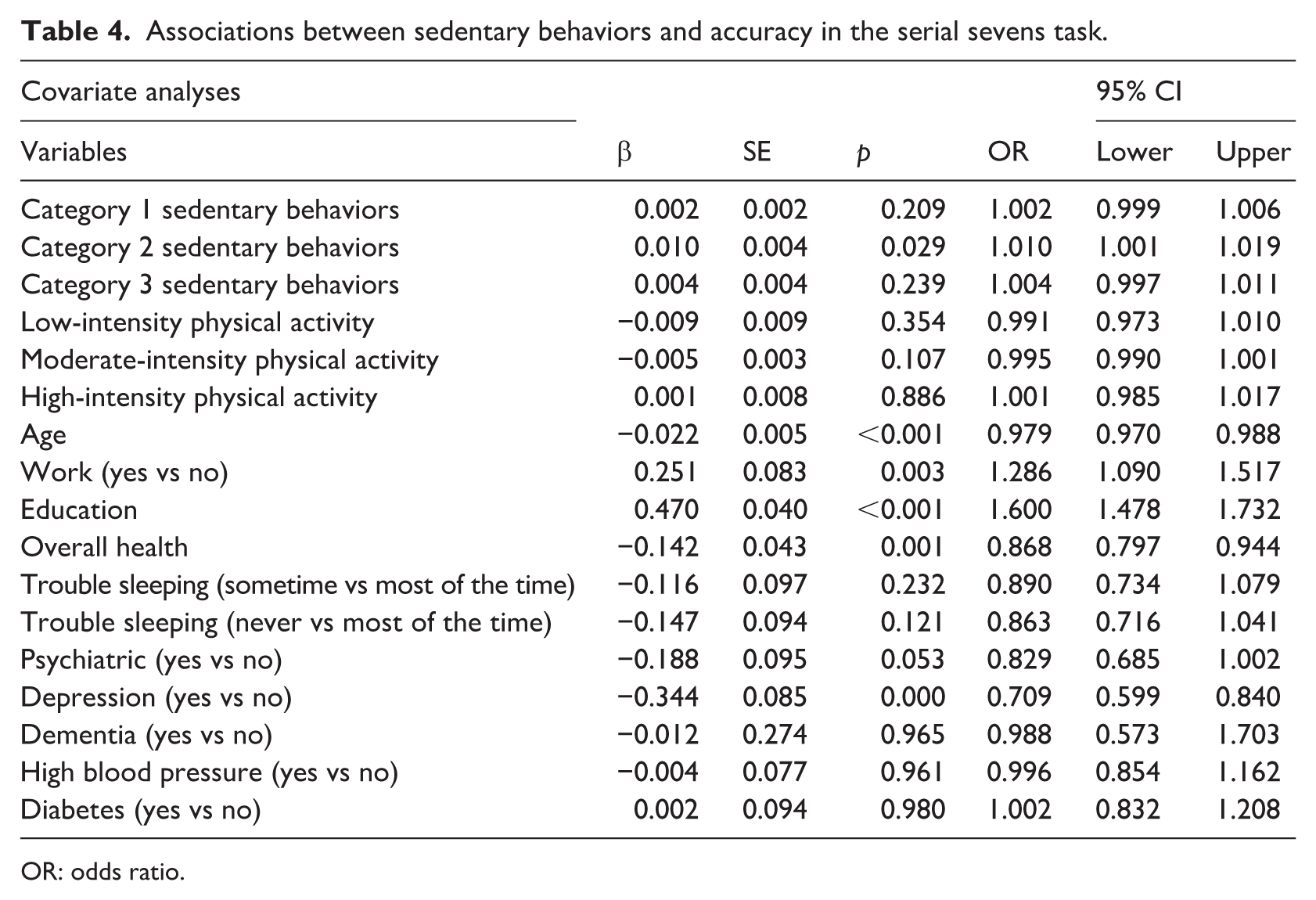
OR: odds ratio.
Several covariates reached significance. Worse self-rated health was associated with worse self-rated memory (p < 0.001), less words recalled (p < 0.001), and lower odds of performing a correct subtraction (p = 0.001). Participants who “rarely or never” had trouble sleeping tended to self-report better memory (p = 0.018) and word recall (p = 0.006) than participants who had trouble sleeping “most of the time.” Older adults who reported depression in the past 12 years were less likely to perform a correct subtraction (p < 0.001) and tended to rate their memory as worse (p = 0.024). Older adults who were working for pay were more likely to perform a subtraction correctly (p = 0.003) and tended to rate their memory better (p = 0.001; Tables 3 and 4).
We performed separate analyses with uncategorized sedentary behaviors and the same model specifications (including the same set of covariates). Total hours of uncategorized sedentary behaviors were not significantly associated with self-rated memory (p = 0.303) or word recall (p = 0.406). In contrast, total hours of uncategorized sedentary behaviors were positively associated with the odds of a correct subtraction (p = 0.005). A possibility is that (1) uncategorized sedentary behaviors masked the association between sedentary behaviors and subtraction; and (2) category 2 sedentary behaviors (p = 0.029) drove the association between uncategorized sedentary hours and accuracy on the subtraction measure (Supplemental Table 1).
Discussion
In this study, we analyzed the relationship between categories of sedentary behavior (based on the four domains of the Taylor taxonomy) and cognitive health. We found no associations between category 1 sedentary behaviors and cognitive health. Conversely, we found positive associations between categories 2 and 3 sedentary behaviors and cognitive health. These results support that certain categories of sedentary behaviors based on the Taylor taxonomy of sedentary behaviors are associated with cognitive health.
Other studies also found that diverse sedentary behaviors had different associations with cognitive health. Among adults aged 70–79 years in the United States, longer reading times were positively associated with cognitive health, but television viewing had no association (Major et al., 2023). Also, among healthy adults aged 45–60 years in France, computer use was positively associated with better performance on cognitive measures (Kesse-Guyot et al., 2012). Furthermore, among adults 60 years and older in Scotland, England, and Wales, television time was associated with a greater risk of all-cause dementia, whereas computer time was associated with a lower risk of all-cause dementia (Raichlen et al., 2022). Conversely, among adults aged 61–70 years in the Netherlands, television, reading, or creative time was not associated with cognitive health (Wanders et al., 2021). These contrasting findings may be due to (1) differences in measures of cognitive health among studies or (2) cultural differences among countries that influence cognitive health and sedentary behaviors (Kesse-Guyot et al., 2012; Major et al., 2023; Raichlen et al., 2022; Wanders et al., 2021).
These differences also highlight that the relationships between sedentary behaviors and cognitive health in older adults are complex and inconsistent (Major et al., 2023; Olanrewaju et al., 2020; Taylor et al., 2020; Wanders et al., 2021). These challenges were summarized in a recent review of sedentary behavior and lifespan brain health in middle-aged (40–65 years old) and older (>65 years old) adults (Zou et al., 2024). To overcome these challenges, we can use the Taylor taxonomy of sedentary behaviors. This taxonomy is more comprehensive than previous approaches that emphasize cognitively active and passive sedentary behaviors (Hallgren et al., 2020; Raichlen et al., 2022; Saunders et al., 2020; Wingood et al., 2024; Zhou et al., 2022; Zou et al., 2024).
The physiological effects of sedentary behaviors are well documented and consistent (Pinto et al., 2023). In contrast, sedentary behaviors are not associated with consistent cognitive, mental, psychological, and emotional health outcomes. These different outcomes may be due to the diversity of sedentary behaviors. To distinguish between health-promoting and health-compromising sedentary behaviors, guidelines are needed to inform health policy, intervention development, and physician recommendations. These guidelines would help to increase health-promoting and decrease health-compromising sedentary behaviors (Aunger et al., 2018; Chase et al., 2020; Chastin et al., 2021).
The lifestyles of older adults are diverse and include working status (e.g. full-time, part-time, retired, caring for grandchildren or great-grandchildren) and living arrangements (in retirement communities, with adult children, in independent or memory care facilities). These lifestyle factors impact the types, amounts, and ways that sedentary behaviors accrue (Aunger et al., 2018). Also, lifestyle factors can influence older adults’ independence and quality of life, which can promote healthy lifestyles and reduce burdensome healthcare costs (Ortman et al., 2014). These considerations have global implications that affect health outcomes, as well as families, businesses, public health professionals, healthcare providers, clinicians, employers, policy makers, and the public (Ortman et al., 2014). With the Taylor taxonomy, we can better understand how diverse lifestyle factors in older adults affect cognitive health and other health outcomes (Taylor, 2022).
Although physical activity improves health (Department of Health and Human Services, 2018; El-Kotob et al., 2020; McLaughlin et al., 2020), these opportunities are not always available or possible for older adults with physical activity restrictions. These adults would benefit from understanding how distinct types of sedentary behaviors influence different health outcomes so they can choose behaviors that best support their health. For example, in our study, categories 2 and 3 sedentary behaviors were positively associated with cognitive health. Thus, older adults who want to optimize their cognitive health could participate in more categories 2 and 3 sedentary behaviors.
A fundamental premise of the Taylor taxonomy of sedentary behaviors is that no sedentary behavior is intrinsically healthy or harmful—context matters. For example, sitting while watching television may be associated with lower muscle activity and energy expenditure than sitting while using a computer (Raichlen et al., 2022). Also, television viewing often occurs in the evening, and this timing can be detrimental for cardiometabolic physiology (Raichlen et al., 2022). However, television viewing for more than 3 hours per day protected against impaired memory over 6 years (Wingood et al., 2024). Also, television viewing can provide relaxation, entertainment, and an escape from difficult life circumstances (Fancourt and Steptoe, 2019). These differences may be due to television viewing being both an alert (i.e. watching fast-paced changes in images) and passive interaction (i.e. consuming content without active engagement; Fancourt and Steptoe, 2019). To document the context of sedentary behaviors, the Taylor taxonomy addresses the five essential questions: what (behavior), why (purpose), where (location), when (time), and with whom (social setting; Chastin et al., 2013).
Based on the Taylor taxonomy of sedentary behaviors, any sedentary behavior can be reconfigured into a healthier engagement. For example, viewing television programs that are educational (i.e. cognition), promote understanding of others (i.e. novelty), and include discussions about the program content (i.e. social interaction and choice) can be a healthier sedentary behavior (Taylor, 2022; Wingood et al., 2024) than television viewing that is primarily passive and contributes to social isolation (Toepoel, 2013).
Sedentary lifestyles are ubiquitous, particularly among older adults who are sedentary 65%–80% of their waking time (Bauman et al., 2018; Harvey et al., 2013, 2015; Wullems et al., 2016). Also, sedentary behavior has more deleterious effects for people who are physically inactive (Department of Health and Human Services, 2018; Katzmarzyk et al., 2019). However, more research is needed to better understand the relationships among sedentary behaviors and light-intensity, moderate-intensity, and vigorous-intensity physical activity (Dempsey et al., 2020; Department of Health and Human Services, 2018; Katzmarzyk et al., 2019; Kikuchi et al., 2014). For example, one question is how to “balance” these behaviors for better health (Dempsey et al., 2020). One recommendation is to reduce discretionary sedentary time to fewer than 2 hours per day. Concomitantly, individuals should engage in moderate-intensity to vigorous-intensity physical activity 150 minutes per week (Falck et al., 2017). Another recommendation is to replace sedentary behavior with light-intensity physical activity (e.g. moving during television commercials), which reduces all-cause mortality (Dohrn et al., 2018).
Sedentary behavior and physical activity also have different challenges with correlates (i.e. factors and conditions that enable or impede) and measurements (Bauman et al., 2018; Chastin et al., 2015). For example, different sedentary behaviors have unique psychosocial, behavioral, environmental, sociocultural, and socio-economic correlates that can inform intervention development. To improve correlates and intervention research, the four domains of the Taylor taxonomy can be helpful (Taylor, 2022). Also, questionnaires are one measure of sedentary behavior (Bauman et al., 2018). However, an alternative measure is video recording a person’s sedentary behavior (e.g. a wearable camera could measure pattern-specific sedentary behaviors). This approach documents important characteristics and context (Kurita et al., 2022), and verifies social interaction (face-to-face or virtual), novelty, and choice (domains of the Taylor taxonomy). This approach can lead to greater understanding of sedentary behaviors and cognitive health.
Our study has several strengths. First, we empirically evaluated the Taylor taxonomy of sedentary behaviors (Taylor, 2022) among a large, representative sample of people 50 years and older in the United Sates. This older group spends more time in sedentary behaviors than younger groups (Bauman et al., 2018). Second, our study used three validated measures of cognitive health. Third, we adjusted for several covariates, including low-intensity, moderate-intensity, and high-intensity physical activity. This approach ensures that results are not biased by extraneous factors, reduces the chances of incorrect conclusions about causal relationships, and increases precision and statistical power. This approach also improves comparability of groups, more accurately isolates the effect of the independent variable on the dependent variable, and increases generalizability of the findings to different populations and contexts (Andrade, 2024; Van Lancker et al., 2024). Fourth, our findings are based on questionnaires completed by interviews, which overcome challenges that older adults may have with paper-based and digital questionnaires (Kutschar and Weichbold, 2019; Reichstadt et al., 2010). For example, the personal interview provided greater insights into older adults’ subjective experiences and views on successful aging than surveys and focus groups (Reichstadt et al., 2010). Also, the use of survey research explicitly faces unique methodological challenges in older adult populations (Quinn, 2010). Fifth, we disaggregated overall sitting time into conceptually or analytically determined categories of behavior, consistent with previous research (Compernolle et al., 2020; Kikuchi et al., 2014; Russell and Chase, 2019; Wingood et al., 2024).
Our study has limitations. First, sedentary behaviors were self-reported and may be inaccurate due to self-presentation bias, comprehension, uncertainty, recall errors, misestimates, social-desirability bias, influences of mood and depression, and other factors. Indeed, objective measures revealed more sedentary behaviors than self-reports (Harvey et al., 2015). Second, the posture during each sedentary behavior was unknown. Older adults may have stood, walked, or completed upper body exercises while engaging in behaviors classified as sedentary (e.g. standing while using the computer; Olanrewaju et al., 2020). However, sitting is the most prevalent posture for behaviors classified as sedentary in our study (Compernolle et al., 2020; Mitsutake et al., 2020), and older adults reported that performing habitual sedentary behaviors in a standing position is extremely difficult (Compernolle et al., 2020). Third, the full context of each sedentary behavior (e.g. alone or with others) was not provided. This context is needed to precisely and accurately rate the four domains of the Taylor taxonomy of sedentary behaviors. However, even without the full context, we identified three distinct categories of sedentary behaviors with different mean ratings. Finally, although we included a range of covariates, unmeasured confounders (e.g. snacking and drinking) may have affected our results.
Our study informs future work. First, future studies can use more precise and accurate survey questions. The following question stems are recommended: “while sitting” or “how often do you perform the following activities while sitting or lying down?” or “about how much time do you spend sitting” (Kurita et al., 2022; León-Muñoz et al., 2013; Major et al., 2023). Second, future studies should include objective measures of sedentary behaviors (e.g. inclinometers, accelerometers, sensors, activPAL monitors; Heesch et al., 2018; Leask et al., 2015; Mañas et al., 2017; Webster et al., 2021; Zou et al., 2024). These objective measures, when combined with self-reports and pictures (e.g. wearable camera), can provide a full context of sedentary behaviors (Leask et al., 2015). Third, future studies can include a comprehensive list of sedentary behaviors (e.g. writing, transportation in a vehicle as a driver or passenger) for more robust analyses. Fourth, future studies can address the direction of causality by including reverse and bidirectional causation. Reverse causation occurs when healthier individuals engage in more health-promoting sedentary behaviors versus individuals becoming healthier from participating in health-promoting behaviors. Bidirectional causality occurs when both conditions are true (Pedisic et al., 2014; Rebar et al., 2014). To evaluate causality, changes in sitting time during longitudinal studies, intervention studies, or randomized controlled trials are needed. Also, Mendelian randomization (i.e. a statistical method using genetic variation) can assist in examining potential causal effects on different outcomes, minimizing confounding, and addressing reverse causation (Pinto et al., 2023; Zou et al., 2024). Fifth, future research can replicate and extend our findings with other datasets (e.g. National Health and Aging Trends Study) that include different measures of cognitive health and a broader range of health outcomes (e.g. mental health, brain health, psychological health, physical function). Finally, future work can consider a global perspective among various countries representing diverse cultures, income levels, and perspectives of aging.
Conclusions
In our study, specific categories of sedentary behaviors were positively associated with cognitive health in older adults. These findings support efforts to encourage health-promoting sedentary behaviors and discourage health-compromising sedentary behaviors in this population. These findings also support that the Taylor taxonomy of sedentary behaviors can reduce complexity, promote understanding, and clarify relationships among sedentary behaviors and cognitive health. Thus, the Taylor taxonomy is a useful, practical, and valuable framework for understanding sedentary behaviors and informing interventions that improve the health and quality of life for older adults.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261419219 – Supplemental material for Associations between sedentary behaviors and cognitive health in older adults based on the Taylor taxonomy of sedentary behaviors
Supplemental material, sj-docx-1-hpq-10.1177_13591053261419219 for Associations between sedentary behaviors and cognitive health in older adults based on the Taylor taxonomy of sedentary behaviors by Wendell C. Taylor and Chuong Bui in Journal of Health Psychology
Footnotes
Acknowledgements
We thank Kelly Schrank of Bookworm Editing Services, LLC and Crystal Herron, PhD, ELS(D), CMPP, of Redwood Ink for editing the manuscript. Also, we thank Kelly Schrank for creating the Taylor taxonomy image.
Ethical considerations
The Health and Retirement Study is a longitudinal project sponsored and approved by the National Institute on Aging (NIA U01AG009740) and the Social Security Administration.
Informed consent
There are no human participants in this article and informed consent was not required.
Consent to participate
For The Health and Retirement Study, participation in the study is completely voluntary. Prior to each interview and collection of biomarkers and physical measures, participants are provided with a written informed consent information document. At the start of each interview and collection of biomarkers and physical measures, all respondents are read a confidentiality statement, and give oral consent by agreeing to do the interview and collection of biomarkers and physical measures.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Author contributions
WCT: Conceptualization, Supervision, Writing - original draft, Writing - review & editing. CB: Data curation, Writing - original draft, Writing - review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.