
Abstract
Emerging adults may look for sexual healthcare services less frequently than other age groups. This study constructed the Seeking Sexual Healthcare Services Scale to assess behaviors toward seeking sexual healthcare services among emerging adults. In Study 1 (n = 350), 24 items were developed, and an exploratory factor analysis revealed a 17-item 4-factor model. In Study 2 (n = 280), two experts in sex-related research reviewed the identified factors and provided feedback on the results from Study 1. Subsequently, 23 items were tested and an exploratory factor analysis revealed a 20-item 4-factor structure, where factors were identified as Sexual and Reproductive Healthcare Importance, Perceived Barriers, Perceived Trust and Support, and Stigma. These factors demonstrated adequate internal reliability and convergent and discriminant validity. This scale may be a reliable and valid tool to assess access to sexual healthcare services and may facilitate continued research efforts to improve access to sexual healthcare services.
Keywords
Introduction
There is greater engagement in sexual risk behaviors within the U.S. compared to most other industrialized countries (World Population Review, 2022). Sexual risk behaviors (e.g. condomless sex, multiple sex partners) are sexual acts that contribute to adverse health outcomes for one or more persons (Senn, 2013) and can be detrimental to one’s well-being (Alonso-Martinez et al., 2021). Specifically, these sexual behaviors may lead to sexually transmitted infections (STIs), which if left untreated, may result in cancer, infertility, increased risk of HIV, and pelvic inflammatory disease (Office of Infectious Disease and HIV/AIDS Policy (OIDP), 2024). Individuals between 18 and 25 years of age, or emerging adults (Arnett, 2007), may be at increased risk for adverse sexual health outcomes as they are more likely to engage in sexual risk behaviors compared to older aged adults (Arnett, 2000; Ertl et al., 2022). Furthermore, people between 15 and 24 years of age account for a quarter of those who are sexually active, yet account for one-half of all new yearly STI cases (Centers for Disease Control and Prevention (CDC) , 2018). These disparate rates of STI contraction among emerging adults may be attributed to multiple factors such as a lack of education, lack of resources, and barriers when seeking sexual healthcare services. Sexual healthcare services may include preventative, diagnostic, and treatment for health issues such as pregnancy, STIs, HIV, and health guidance and counseling (CDC, 2024). As such, these factors elucidate a need for quantitative measurements to assess access to sexual healthcare services.
There have been generational shifts in the acceptability of sexual experimentation (Twenge et al., 2015), signaling decreases in taboo. This normalization of sexual experimentation may contribute to increased sexual satisfaction. That said, positive sexual satisfaction may contribute to future engagement in certain sexual risk behaviors (e.g. casual sex; Hawkins et al., 2023). Emerging adults in the U.S. may be more vulnerable to adverse sexual health outcomes than emerging adults in other countries due to a lack of fundamental sexual health education (Hall et al., 2016; Sekhar et al., 2024). While sex education is mandated in other industrialized countries (Ketting and Ivanova, 2018), only 17 out of 50 states in the U.S. mandate medically accurate sexual health education for young people (Guttmacher Institute, 2020). Furthermore, the sexual health information provided may still differ across states in which some states may focus extensively on abstinence and exclude pertinent information for sexual safety (CDC, 2019). States with abstinence-only education programs have higher teen pregnancy rates than states with comprehensive sexual education (Atkins and Bradford, 2021; Cheedalla et al., 2020; Fox et al., 2019). These differences in sexual health information may leave adolescents with insufficient knowledge in how to address their sexual health concerns and where to obtain information when seeking sexual healthcare services as they transition into emerging adulthood.
Indeed, emerging adults may seek services less frequently than other age groups (Adams et al., 2018; Caal et al., 2013) which may be due to an inability to confide in others with sexual health concerns (Jones et al., 2019). Specifically, emerging adults may desire sexual health information from family and friends but may encounter barriers such as confidentiality, stigma (Jones et al., 2019), or lack of support systems where they can obtain information (Bender and Fulbright, 2013; Jones et al., 2019; Scheinfeld, 2021). When disclosing sensitive information, emerging adults may feel stigmatized or judged by family and peers for asking questions about sexual health (Jones et al., 2019). This stigmatization may enhance the appeal of obtaining sexual health information from internet sources which may not always be reliable and can contribute to increased sexual risk (Fuxman et al., 2015). Adequately measuring potential barriers and facilitators to sexual healthcare access that emerging adults may experience is essential in order to promote sexual wellbeing and reduce sexual risk among this population.
Despite the proliferation of general sexual health research conducted in a wide array of modalities, most research on sexual healthcare seeking utilizes qualitative measures (e.g. focus groups, interviews; Decker et al., 2021). For example, Decker et al. (2021) state that qualitative assessments of sexual healthcare seeking are typically focused on obtaining information from specific interest groups rather than broader populations. While qualitative research is informative and essential for the development of quantitative measures, assessments using only qualitative methodology is not intended to generalize results to representative samples, so there is a lack of research leading to generalization. Specifically, the information obtained from in-depth interviews and focus groups provides invaluable information on how to best proceed in creating a quantitative measure for assessing intentions and behaviors for seeking sexual health services.
Present study
The primary aim of this study was to advance much-needed sexual health research by developing and testing a scale that measures behaviors in seeking sexual healthcare services in a sample of emerging adults. Given the above literature in which emerging adults may encounter difficulties in accessing such services (Caal et al., 2013; Jones et al., 2019), we developed a scale that was expected to reflect the following three themes: (1) sexual healthcare service seeking, (2) perceived barriers in seeking sexual healthcare services, and (3) perceived social support in seeking sexual healthcare services. The secondary aim of the present study were to assess convergent validity with Sexual Health Practices Self-Efficacy Scale (Barthalow Koch et al., 2011) and discriminant validity with the Right-Wing Authoritarianism Scale (Study 1; Zakrisson, 2005) and Need for Cognition Scale (Study 2; Cacioppo et al., 1984).
Study 1: Item development
Items for our scale assessing seeking sexual healthcare services were developed from previous sexual health scales, theory, and qualitative research. Specifically, items from the Health Belief Model Scale for Cervical Cancer and Pap Smear Test developed by Guvenc et al. (2011) informed item development as the current measure assessed seeking sexual health services beyond cervical cancer screening. Moreover, similar to previous scale development work (e.g. Champion et al., 2013), the Health Belief Model (Rosenstock et al., 1988) was also referred to for item development such that we examined the perceived barriers and benefits of seeking sexual healthcare services. Third, previous qualitative research revealing themes related to barriers, social support, and other facilitators for seeking sexual healthcare services was also referred to for item development (Caal et al., 2013; Scheinfeld, 2021).
Method
Participants
Monte Carlo simulations were used to determine sample size. Assuming items had standardized factor loadings of 0.30, standardized residual error variances of 0.91, and inter-factor correlations of 0.375 among the three hypothesized factors for a 24-item measure, all factor loadings had power that exceeded 0.90, and all inter-factor correlations had power that exceeded 0.80 with a sample size of 300. An additional 20% of the sample size (n = 60) was added to account for attrition and incomplete data, resulting in a desired sample size of 360.
To participate in the study, participants had to reside in the U.S. and be between 18 and 25 years of age. Three-hundred and sixty participants were ultimately recruited. However, 10 participants were excluded from analysis for not passing at least three out of four attention checks, resulting in a final analyzable sample size of 350 emerging adults (Mage = 22.32, SD = 1.99; 48.0% women).
Materials
Sociodemographic survey
This 10-item demographic survey assesses age, sex, gender, ethnicity, race, sexual orientation, highest level of education completed, and current romantic relationship status.
Seeking Sexual Healthcare Services Scale (SSHSS)
The SSHSS is a 24-item scale that assesses intentions and behaviors toward seeking sexual healthcare services. The SSHSS contained items reflecting the following three themes: (1) Service Seeking, (2) Perceived Barriers, and (3) Perceived Social Support. Items utilize a 7-point Likert scale (1-Strongly Disagree – 7-Strongly Agree), and an average score is computed for each factor. Items assess views toward seeking sexual and reproductive healthcare services such as contraceptive use, STI screenings, and reproductive cancer screenings (e.g. cervical, ovarian, testicular, prostate), and potential deterrents and sources of support in seeking sexual and reproductive healthcare services. Higher scores indicate a greater likelihood of seeking sexual healthcare services.
Sexual Health Practices Self-Efficacy Scale (SHPSES)
This 20-item scale measures the confidence and knowledge of engaging in safe sexual practices (Barthalow Koch et al., 2011). Items utilize a 5-point scale (1-Not at all Confident – 5-Extremely Confident), and a mean score is computed with higher scores indicating greater levels of the scale construct (α = 0.91). This scale was used to assess convergent validity with the SSHSS as the SSHSS assesses theoretically related concepts to the SHPSES (e.g. perceptions regarding sexual service acquisition), and albeit having distinct dimensions, these scales were expected to be strongly correlated.
Right Wing Authoritarianism Scale
This 15-item scale measures authoritarian aggression, authoritarian submission, and conventionalism (Zakrisson, 2005). Items utilize a 7-point Likert scale (1-Very Negative – 7-Very Positive), and a mean score is computed with higher scores indicating greater attitudes toward authoritarianism (α = 0.85). This scale was used to assess discriminant validity with the SSHSS as the Right-Wing Authoritarianism Scale focuses on broad attitudes relating to authoritarianism and was expected to differ conceptually from the SSHSS which assesses sexual health service seeking. Based on these conceptual differences, the Right-Wing Authoritarianism Scale was expected to be uncorrelated with the SSHSS.
Procedure
Prior to study implementation, IRB approval was obtained. Data were collected on April 17, 2023. Participants were recruited via Prolific, an online crowd-sourcing platform for research, then were directed to the Qualtrics platform to first read and electronically sign a consent form. Once consent was obtained, participants completed a series of questionnaires in randomized order to protect against order effects. Following the measures, participants were asked to answer an open-ended question to summarize their thoughts on the survey which served as a captcha to remove potential automated responses (“bots”) in the present sample. Participants were then debriefed, offered sexual health resources (e.g. telephone numbers for STI/HIV testing), and received $3.00 as compensation.
Approach to analyses
Descriptive statistics revealed participant characteristics. Parallel analysis was conducted to determine the number of retained factors; factor extraction stops at the last factor in which the data eigenvalue is greater than the random eigenvalue. Exploratory factor analysis assessed the factor structure of the SSHSS using Mplus 8.11 (Muthén and Muthén, 1998–2025) in which maximum likelihood estimation was used for factor extraction and Geomin (oblique) rotation was used as the rotation method. To analyze model fit and factorial validity, indices of fit including the Satorra-Bentler chi-square (SB χ2) and its associated p-value, comparative fit index (CFI) ⩾ 0.95, root mean square error of approximation (RMSEA) ⩽ 0.06, and standardized root mean square residual (SRMR) ⩽ 0.08 (Hu and Bentler, 1999) were used. Slightly more liberal thresholds were also accepted, including CFI ⩾ 0.90 (Blackburn et al., 2004) and RMSEA ⩽ 0.08 (MacCallum et al., 1996). To assess internal reliability, Cronbach’s alpha (α) was used. The SHPSES and Right-Wing Authoritarianism Scale were used to assess convergent and discriminant validity with the SSHSS, respectively, using Pearson’s correlation coefficient.
One hierarchical multiple linear regression was performed to assess if the subscales of the SSHSS predicted SHPSES scores. Participant sex, age, and ethnicity were controlled for and entered in Step 1 given that past research has observed links between these variables and this study’s variables of interest (e.g. Caal et al., 2013), and the factors of the SSHSS were entered in Step 2. Gender was not controlled for, given that too few participants identified as a gender other than man or woman (i.e. 2.9%–3.6%) to make meaningful comparisons.
Results
Descriptive statistics and participant characteristics are reported in Table 1.
Descriptive statistics and participant characteristics for Study 1.
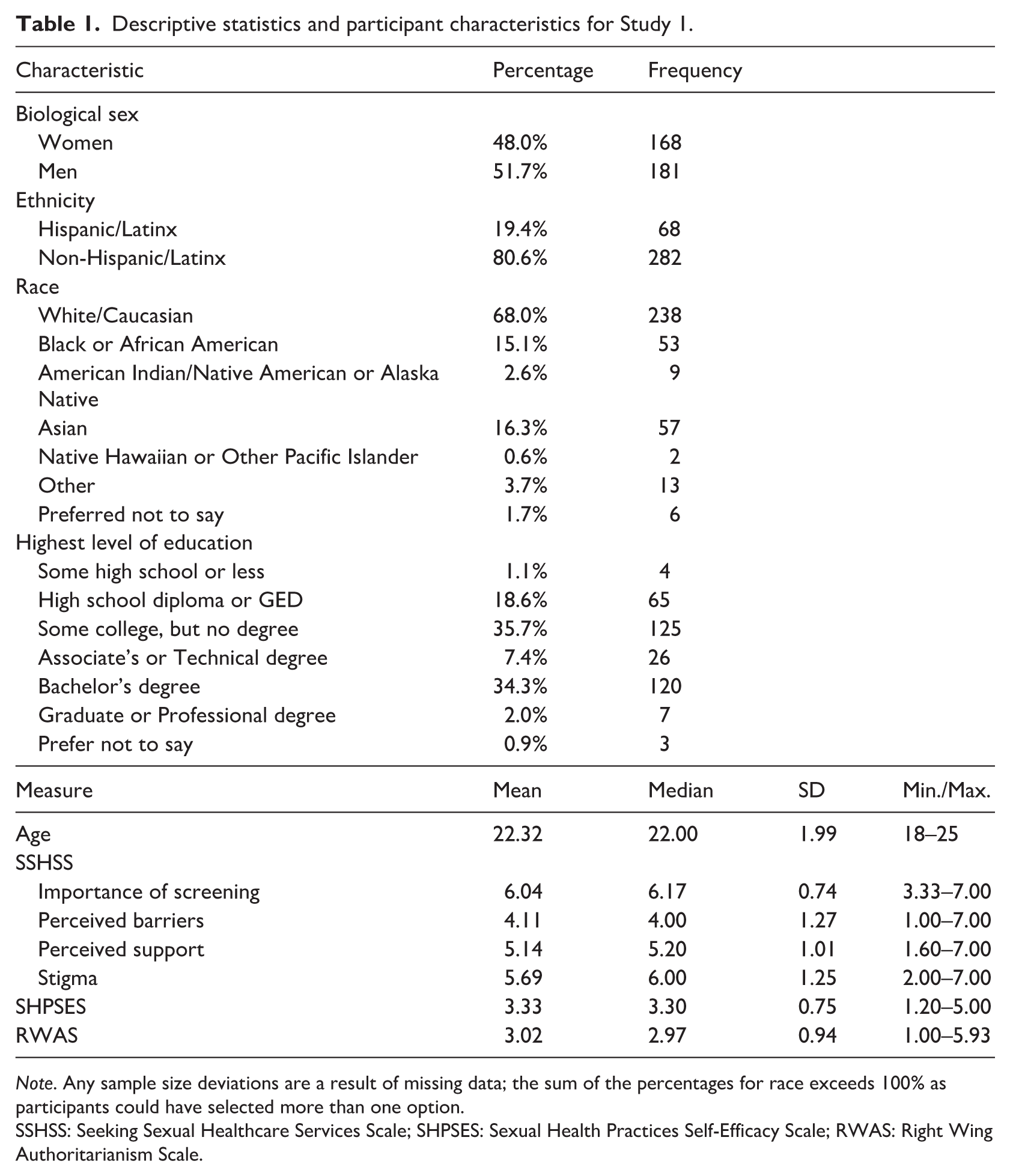
Note. Any sample size deviations are a result of missing data; the sum of the percentages for race exceeds 100% as participants could have selected more than one option.
SSHSS: Seeking Sexual Healthcare Services Scale; SHPSES: Sexual Health Practices Self-Efficacy Scale; RWAS: Right Wing Authoritarianism Scale.
Exploratory factor analysis
Parallel analysis suggested that four factors be retained. Exploratory factor analysis revealed that the fit of the four-factor dimensionality of the SSHSS was: SB χ2 (186, N = 350) = 379.056, p < 0.001, CFI = 0.921, RMSEA = 0.054 (90% CI: 0.047, 0.062), SRMR = 0.036. Geomin rotated factor loadings were examined to assess how the 24-items loaded on these four factors. Using recommendations from past literature (Costello and Osborne, 2005; Tabachnick and Fidell, 2001), an item was considered to demonstrate fidelity to a factor (dimension) if that item had a factor loading of 0.32 or above on that factor and did not crossload (i.e. the item loaded at 0.32 or above on two or more factors). If an item did not meet these criteria, then dimensional fidelity was not established and that item was removed. Using these guidelines, rotated factor loadings within each dimension showed six items loading on factor one (λ’s = 0.377–0.852), three items loading on factor two (λ’s = 0.342–0.665), five items loading on factor three (λ’s = 0.324–0.767), and three items loading on factor four (λ’s = 0.503–0.561). By assessing these retained items, the four factors were titled as: (1) Screening Importance (variance explained = 37.35%), (2) Perceived Barriers (variance explained = 11.74%), (3) Perceived Support (variance explained = 10.53%), and (4) Stigma (variance explained = 8.42%; Table 2).
Exploratory factor analysis of significant geomin rotated factor loadings for the seeking sexual healthcare services scale in Study 1.
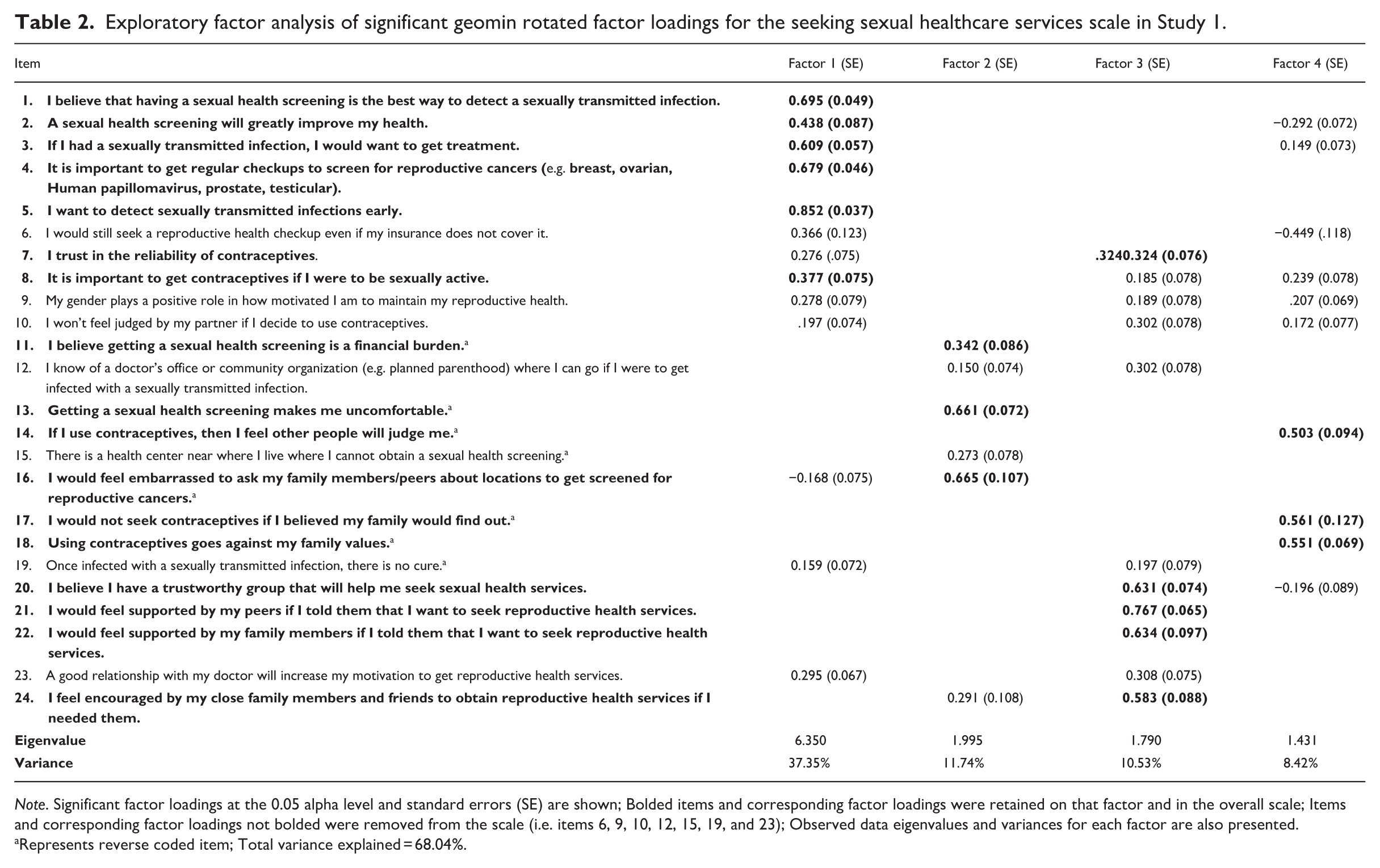
Note. Significant factor loadings at the 0.05 alpha level and standard errors (SE) are shown; Bolded items and corresponding factor loadings were retained on that factor and in the overall scale; Items and corresponding factor loadings not bolded were removed from the scale (i.e. items 6, 9, 10, 12, 15, 19, and 23); Observed data eigenvalues and variances for each factor are also presented.
Represents reverse coded item; Total variance explained = 68.04%.
Coefficient alpha for the four factors of the SSHSS were adequate except for Perceived Barriers: Screening Importance, α = 0.76; Perceived Barriers, α = 0.55; Perceived Social Support, α = 0.78; Stigma, α = 0.76. Screening Importance was positively correlated with Perceived Barriers (r = 0.170, p = 0.001), Perceived Social Support (r = 0.493, p < 0.001), and Stigma (r = 0.455, p < 0.001). Perceived Barriers was positively correlated with Perceived Social Support (r = 0.322, p < 0.001) and Stigma (r = 0.378, p < 0.001). Perceived Social Support was positively correlated with Stigma (r = 0.418, p < 0.001).
The four factors of the SSHSS demonstrated acceptable convergent validity with the SHPSES. SHPSES was positively correlated with Screening Importance (r = 0.331, p < 0.001), Perceived Barriers (r = 0.382, p < 0.001), Perceived Social Support (r = 0.446, p < 0.001), and Stigma (r = 0.296, p < 0.001). The four factors of the SSHSS demonstrated low-to-adequate discriminant validity with the Right-Wing Authoritarianism Scale. Right wing authoritarianism was negatively correlated with Screening Importance (r = −0.319, p < 0.001), Perceived Social Support (r = −0.316, p < 0.001), and Stigma (r = −0.402, p < 0.001), but not correlated with Perceived Barriers (r = −0.020, p = 0.706).
Regression analysis
The full regression model predicting SHPSES from the four factors of the SSHSS was statistically significant (F(7,339) = 20.160, R2 = 0.294 (Adjusted R2 = 0.279), p < 0.001). Participants who reported greater sexual health practices self-efficacy also reported greater levels of recognizing the importance of screening (β = 0.127, p = 0.024), fewer perceived barriers of seeking sexual healthcare services (β = 0.260, p < 0.001), and greater perceived social support in seeking sexual healthcare services (β = 0.315, p < 0.001; Supplemental Table 1). Participant age, sex, and ethnicity were controlled for and not associated with SHPSES scores in the full model (β’s = −0.031 to 0.047, p’s > 0.05).
Study 2: Item refinement
Study 1 revealed that the SSHSS was best explained by a 17-item four-factor structure including Screening Importance, Perceived Barriers, Perceived Social Support, and Stigma in which retained items demonstrated strong fidelity by dimension. However, internal reliability was low for the Perceived Barriers factor, and Right-Wing Authoritarianism did not exhibit adequate discriminant validity with the Screening Importance, Perceived Support, and Stigma factors. Thus, for Study 2, two experts in sex-related research reviewed the items of the SSHSS and provided feedback in improving item structure by increasing the clarity of items and adding four items to the Perceived Barriers factor and two items to the Stigma factor. Furthermore, to establish discriminant validity with the SSHSS, the Need for Cognition scale (Cacioppo et al., 1984) was used.
Method
Participants
Monte Carlo simulations were used to determine sample size in which values were based on values observed in Study 1. Assuming the items had standardized factor loadings of 0.40, standardized residual error variances of 0.84, and inter-factor correlations of 0.40 among the four factors for a 23-item measure, all factor loadings had power that exceeded 0.90 and all inter-factor correlations had power that exceeded 0.80 with a sample size of 210. An additional 20% of the sample size (n = 42) was added to account for attrition and incomplete data, resulting in a desired sample size of 252.
Three hundred and eighteen participants were recruited for Study 2. However, 33 participants were excluded from analysis for not passing at least three of four attention checks and five duplicate entries were removed, resulting in a final analyzable sample size of 280 emerging adults (Mage = 19.87, SD = 1.70 86.1% women).
Materials
Sociodemographic survey
This 19-item sociodemographic survey assesses typical demographic information such as age, sex, ethnicity, household income, and parents’ highest level of education.
SSHSS – Refined
After analyzing the SSHSS in Study 1 and consultation with two experts in sex-related research, the SSHSS became a 23-item four-factor scale that assesses participants’ intentions and behaviors toward seeking sexual healthcare services. The SSHSS reflects four themes: (1) SRH (Sexual and Reproductive Healthcare) Importance, (2) Perceived Barriers, (3) Perceived Trust and Support, and (4) Stigma. Items utilize a 7-point Likert scale (1-Strongly Disagree – 7-Strongly Agree), an average score is computed with higher scores indicating greater likelihood of seeking sexual healthcare services.
SHPSES
The SHPSES was again used to assess the confidence and knowledge one has to engage in safe sexual practices (Barthalow Koch et al., 2011) as described in Study 1. This scale was again used in Study 2 (α = 0.88), given that item refinement of the SSHSS was not expected to impact previously observed convergent validity.
Need for cognition
The Need for Cognition scale was used to assess discriminant validity; this 18-item scale measures one’s ability to organize and evaluate information provided (Cacioppo et al., 1984). Items utilize a 9-point scale (−4-Very strong disagreement – 4-Very strong agreement), and a mean score is computed with higher scores indicating greater need for cognition (α = 0.82). The Need for Cognition scale was used to assess discriminant validity given that this scale measures unrelated concepts (e.g. information processes) to the SSHSS and may not be influenced by confounding relationships exhibited by the Right-Wing Authoritarianism Scale (e.g. conservatism) as observed in Study 1.
Procedure
IRB approval was obtained prior to study implementation; data were collected between August 2024 and October 2024. Participants were recruited via SONA, a secure web-based recruitment website. Participants first read and signed a consent form indicating that they agreed to participate in the survey. After, participants completed a separate series of questionnaires via Qualtrics, were debriefed, and were offered course credit for their participation.
Approach to analyses
The same approach to analyses was conducted for Study 2 as was done in Study 1. In short, descriptive statistics revealed participant characteristics, and parallel and exploratory factor analysis were performed to assess factor structure using maximum likelihood estimation and Geomin (oblique) rotation. To analyze model fit and factorial validity, indices of model fit included the SB χ2 and its associated p-value, CFI ⩾ 0.95, RMSEA ⩽ 0.06, and SRMR ⩽ 0.08 (Hu and Bentler, 1999). A CFI ⩾ 0.90 (Blackburn et al., 2004) and RMSEA ⩽ 0.08 (MacCallum et al., 1996) were also accepted. Cronbach’s alpha was computed for internal reliability, and the SHPSES and Need for Cognition Scale were used to assess convergent and discriminant validity with the SSHSS, respectively, using Pearson’s correlation coefficient. Further, one hierarchical multiple linear regression was performed to assess if the subscales of the SSHSS predicted SHPSES scores while controlling for sex, age, and ethnicity.
Results
Descriptive statistics and participant characteristics are reported in Table 3. Interestingly, for one question included in the demographic survey (“How likely are you to seek sexual health services (e.g. cervical or testicular cancer screenings, sexually transmitted infection screenings, contraceptive care) if you needed them?”), participants reported moderate-to-high levels of seeking sexual health services (M = 5.65, SD = 1.62; Range = 1-Very Unlikely – 7-Very Likely).
Descriptive statistics and participant characteristics for Study 2.
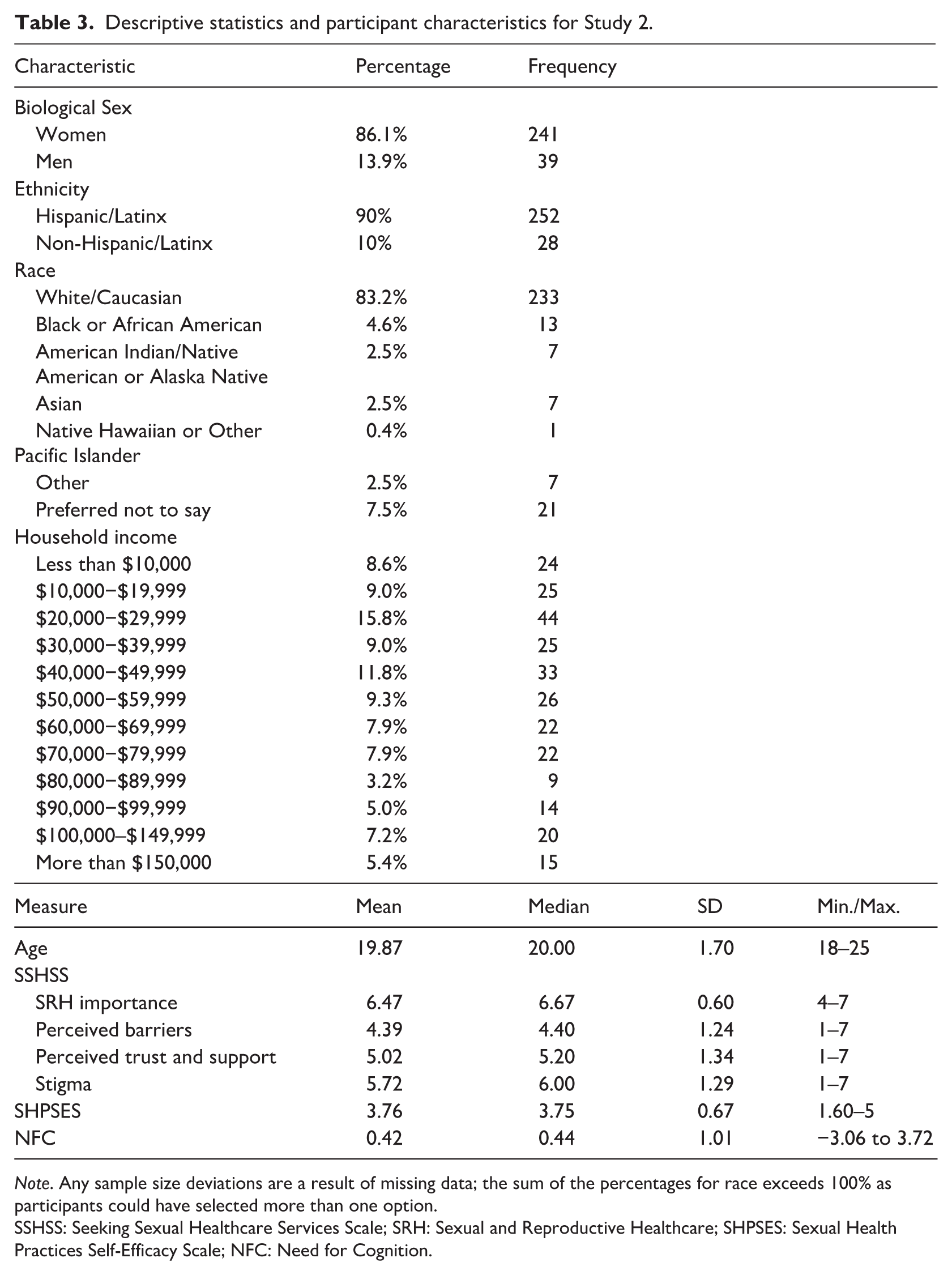
Note. Any sample size deviations are a result of missing data; the sum of the percentages for race exceeds 100% as participants could have selected more than one option.
SSHSS: Seeking Sexual Healthcare Services Scale; SRH: Sexual and Reproductive Healthcare; SHPSES: Sexual Health Practices Self-Efficacy Scale; NFC: Need for Cognition.
Exploratory factor analysis
Parallel analysis suggested that four factors be retained. Exploratory factor analysis revealed that the fit of the four-factor dimensionality of the refined SSHSS items was: SB χ2 (167, N = 280) = 427.882, p < 0.001, CFI = 0.890, RMSEA = 0.075 (90% CI: 0.066, 0.083), SRMR = 0.041. Geomin rotated factor loadings were examined to assess how the 23-items loaded on these four factors. Similar to Study 1, an item was considered to demonstrate fidelity to a given factor (dimension) if that item had a factor loading of 0.32 or above on that factor and did not crossload (i.e. the item loaded at 0.32 or above on two or more factors). If an item did not meet these criteria, then that item was removed from the scale. Using these guidelines, rotated factor loadings showed six items loading on factor one (SRH Importance; λ’s = 0.480–0.757; variance explained = 30.66%), five items loading on factor two (Perceived Barriers; λ’s = 0.474–0.668; variance explained = 12.16%), five items loading on factor three (Perceived Trust and Support; λ’s = 0.433–0.854; variance explained = 11%), and four items loading on factor four (Stigma; λ’s = 0.431–0.786; variance explained = 6.89%; Table 4).
Exploratory factor analysis of significant geomin rotated factor loadings for the seeking sexual healthcare services scale in Study 2.
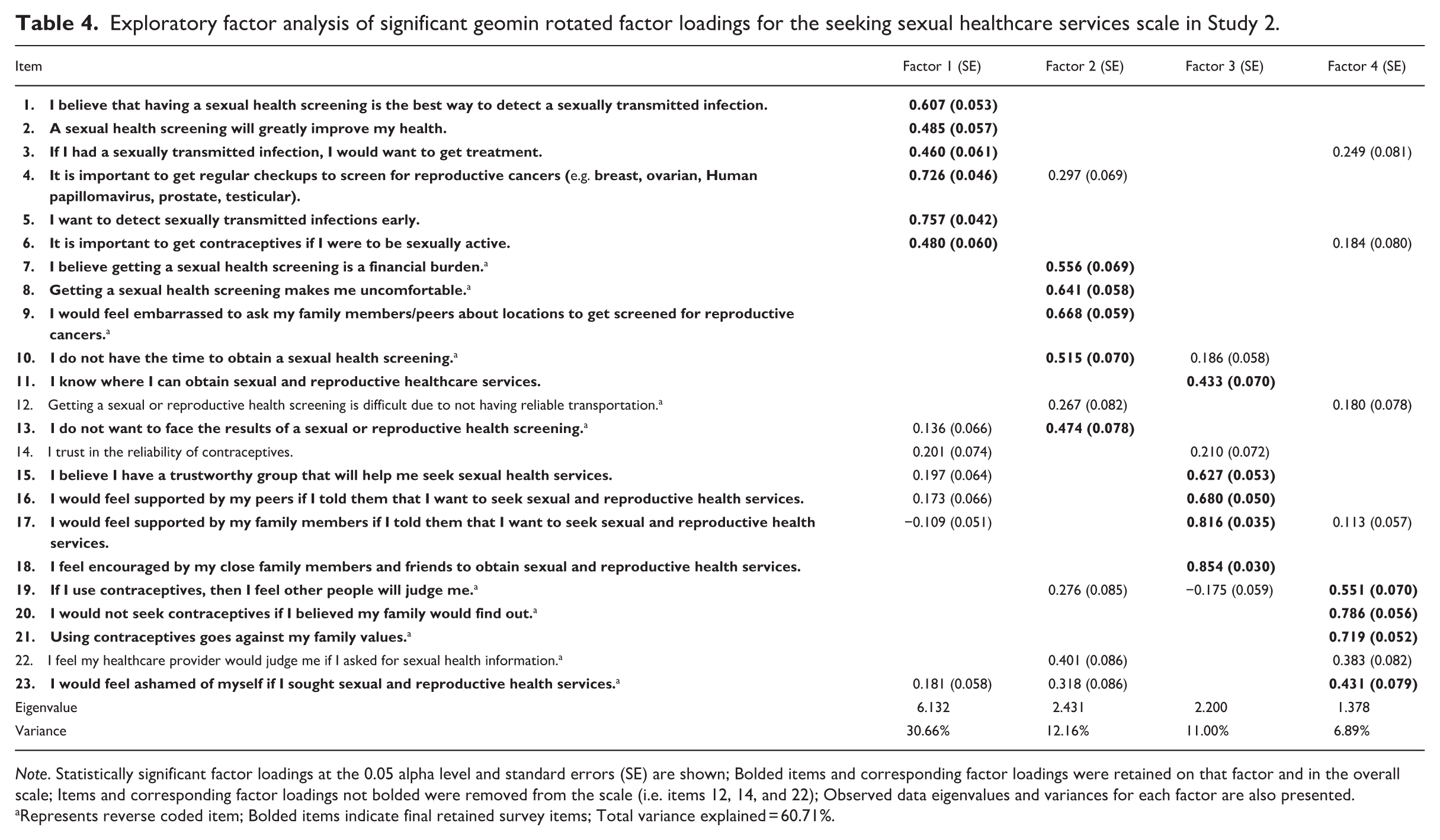
Note. Statistically significant factor loadings at the 0.05 alpha level and standard errors (SE) are shown; Bolded items and corresponding factor loadings were retained on that factor and in the overall scale; Items and corresponding factor loadings not bolded were removed from the scale (i.e. items 12, 14, and 22); Observed data eigenvalues and variances for each factor are also presented.
Represents reverse coded item; Bolded items indicate final retained survey items; Total variance explained = 60.71%.
Coefficient alpha for the four factors of the SSHSS were acceptable: SRH Importance, α = 0.76; Perceived Barriers, α = 0.73; Perceived Trust and Support, α = 0.82; Stigma, α = 0.79. SRH Importance was positively correlated with Perceived Barriers (r = 0.242, p < 0.001), Perceived Trust and Support (r = 0.305, p < 0.001), and Stigma (r = 0.338, p < 0.001). Perceived Barriers was positively correlated with Perceived Trust and Support (r = 0.341, p < 0.001) and Stigma (r = 0.495, p < 0.001). Perceived Trust and Support was positively correlated with Stigma (r = 0.268, p < 0.001).
The four factors of the SSHSS demonstrated acceptable convergent validity with the SHPSES. SHPSES was positively correlated with SRH Importance (r = 0.394, p < 0.001), Perceived Barriers (r = 0.368, p < 0.001), Perceived Trust and Support (r = 0.370, p < 0.001), and Stigma (r = 0.247, p < 0.001). Further, the single question assessing likelihood of seeking sexual health services stated above was positively correlated with SRH Importance (r = 0.313, p < 0.001), Perceived Barriers (r = 0.163, p = 0.001), Perceived Trust and Support (r = 0.204, p < 0.001), and Stigma (r = 0.164, p = 0.001). The new four factors of the SSHSS also demonstrated adequate discriminant validity with the Need for Cognition Scale. Need for cognition was not correlated with SRH Importance (r = 0.087, p = 0.147), Perceived Trust and Support (r = 0.103, p = 0.086), or Stigma (r = 0.074, p = 0.219); however, need for cognition was positively (weakly) associated with Perceived Barriers (r = 0.158, p = 0.008).
Regression analysis
The final regression model predicting sexual health practices self-efficacy from the new four factors of the SSHSS was statistically significant (F(7,272) = 15.10, R2 = 0.280 (Adjusted R2 = 0.261), p < 0.001). Participants who reported greater sexual health practices self-efficacy also reported greater levels of recognizing the importance of receiving sexual and reproductive health services (β = 0.289, p < 0.001), fewer perceived barriers of seeking sexual healthcare services (β = 0.249, p < 0.001), and greater perceived trust and support in seeking sexual healthcare services (β = 0.213, p < 0.001; Supplemental Table 2). Participant age, sex, and ethnicity were controlled for and not associated with SHPSES scores in the full model (β’s = −0.096 to 0.036, p’s > 0.05).
Discussion
The aim of the present study was to advance much needed sexual health research by developing and testing the Seeking Sexual Healthcare Services Scale in emerging adults. Hypotheses for the present study included that an exploratory factor analysis of the SSHSS would include factors reflecting the following themes: (1) sexual healthcare service seeking, (2) perceived barriers in seeking sexual healthcare services, and (3) perceived social support in seeking sexual healthcare services, and that factors revealed from the SSHSS would positively predict scores on the SHPSES. These hypotheses were partially supported such that the SSHSS revealed four factors reflecting the following themes: (1) SRH Importance, (2) Perceived Barriers, (3) Perceived Trust and Support, and (4) Stigma. Furthermore, the second hypothesis was partially supported such that three of the four factors (i.e. SRH Importance, Perceived Barriers, Perceived Trust and Support) in both studies predicted greater sexual health practices self-efficacy in the expected direction, demonstrating convergent validity.
The final 20-item scale (as demonstrated from Study 2) as well as the four factors showed adequate internal reliability and convergent validity. All factors were positively correlated with greater likelihood of seeking sexual and reproductive healthcare services. This shows that the SSHSS may be a useful tool for quantitatively assessing access to sexual healthcare services. Furthermore, the presence of these factors is congruent with past literature which suggests that perceived benefits, perceived barriers, social support, and stigma may be associated with access to sexual healthcare services (Newton-Levinson et al., 2016; Ramaswamy et al., 2018; Suanda et al., 2013). Indeed, greater perceived benefits and social support may facilitate access to sexual healthcare services by normalizing service utilization and emphasizing the importance of maintaining sexual well-being (Hall et al., 2018). Fewer perceived barriers and reduced stigma may also contribute to service utilization by facilitating accessibility of such services (Suanda et al., 2013).
That the best fitting model was composed of four factors and included Stigma is consistent with past literature. Indeed, Jones et al. (2019) noted that there are prevalent stigmatized attitudes among emerging adults seeking sexual healthcare services, and these attitudes may promote an aversion to acquire such services. In Study 2, we expanded on this factor by soliciting expert consultation to improve the items in this factor and increase the predictive power of this construct in which items reflecting self-stigma were added. Expert consultations improved the SSHSS in Study 2, specifically the Stigma and Perceived Barriers factor, as internal reliability for both of these factors increased from Study 1 to Study 2. However, model fit was still slightly less than acceptable with regard to CFI (CFI = 0.890), so future studies should continue to assess the validity of this scale in similar age groups as well as other age groups such as adolescents given that 16% of individuals engage in sexual intercourse by the age of 15 (Finer and Philbin, 2013).
In Study 1, the Right-Wing Authoritarianism Scale was negatively correlated with three of the SSHSS factors, which demonstrated insufficient evidence for discriminant validity in our developed SSHSS. However, this may not be surprising given today’s volatile climate toward sexual health services (Pugh, 2019). The Right-Wing Authoritarian Scale measures the extent to which people adhere to established authority, display aggression toward outgroups, and support the traditional values that are endorsed by the authority (e.g. conservatism; Zakrisson, 2005). Therefore, participants may have political opinions about seeking healthcare services, specifically women’s healthcare. Due to this weak discriminant validity, the Need for Cognition Scale (Cacioppo et al., 1984) was used for Study 2. Need for cognition adequately displayed discriminant validity with the SRH Importance, Perceived Trust and Support, and Stigma factors. However, Need for Cognition Scale was positively correlated with the Perceived Barriers factor. This could indicate that those with higher cognitive abilities may be more perceptive and therefore more likely to recognize barriers to accessing sexual healthcare services; future studies may wish to further explore this relationship.
Furthermore, the ethnic composition of the samples differed from Study 1 to Study 2. Given that 90% of individuals in the second sample identified as Latinx, other cultural factors may have influenced exploratory factor analyses findings. Past studies have noted that cultural factors (e.g. marianismo, machismo) may impact how Latinos navigate sexual healthcare service acquisition (Ertl et al., 2018; Rivera et al., 2021). Thus, future studies may be warranted to continue validating this measure in different ethnocultural groups.
Limitations and strengths
Several limitations of our study are worth mentioning. First, the sample in Study 1 was comprised of predominantly non-Latinx (80.6%) individuals and had an even distribution of females to males (48.0% vs 51.7%). In contrast, Study 2 was comprised of predominantly Latinx (90%) and female (86.1%) participants. These differences in sample composition may have impacted the exploratory factor analysis given that past studies have noted differences in treatment-seeking by gender and ethnicity (Eastman-Mueller et al., 2022; Sutton et al., 2021). Second, no confirmatory factor analyses were conducted highlighting the need to confirm our observed 20-item four-factor model in future studies. Third, we did not conduct measurement invariance analyses across socioeconomic measures (e.g. highest level of education, household income) as our study reported on exploratory factor analyses. Fourth, the fit of the second exploratory factor analysis was a slightly less than acceptable fit given that CFI did not meet the 0.90 threshold, suggesting that future studies may be required to improve on model fit. Despite these limitations, this is the first study to create a quantitative measure to help facilitate the assessment of seeking sexual healthcare services among emerging adults by utilizing past qualitative research on sexual healthcare service acquisition.
Future directions and clinical implications
Future studies are warranted to continue exploring and validating the SSHSS. Specifically, studies should confirm the factor structure of the SSHSS and conduct measurement invariance analyses of the SSHSS across socioeconomic measures. Similarly, validating the SSHSS among other important groups such as adolescents and racial/ethnic and gender minorities is paramount given that these groups may also encounter additional cultural and age-specific difficulties when seeking sexual healthcare services (Decker et al., 2021; Sutton et al., 2021). Furthermore, translation to other languages may help increase the utility of this measure to non-English-speaking populations.
This measure contributes substantially to sexual health literature and clinical practice by serving as a tool to assess the likelihood of sexual healthcare service utilization and to help reduce potential barriers and stigma when accessing services. The brevity and standardization of this measure allows for practitioners to assess accessibility of sexual health resources in a cost-effective manner. Moreover, the present study builds a foundation for the future development of scales aiming to measure sexual healthcare seeking behaviors as this measure may facilitate continued research efforts to improve access to sexual healthcare services. This is paramount given recent funding cuts to sexual health research (Cohen, 2023) and sexual health disparities among emerging adults (CDC, 2022).
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251408560 – Supplemental material for Developing the Seeking Sexual Healthcare Services Scale among emerging adults
Supplemental material, sj-docx-1-hpq-10.1177_13591053251408560 for Developing the Seeking Sexual Healthcare Services Scale among emerging adults by Ariana Cervantes, Miguel A. Garcia, Andrea Rodriguez-Crespo, Miguel Urbina, Theodore V. Cooper and Osvaldo F. Morera in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would also like to thank Chelsea Queen and Grace Hanzelin for facilitating data collection for Study 1 and their invaluable feedback on this manuscript. We would also like to thank Mitchell Kirwan for his feedback on the refinement of scale items in Study 2.
Ethical considerations
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Institutional review board approval was obtained from the University of Texas at El Paso (Study 1 approval number: 2047002; Study 2 approval number: 2190063).
Consent to participate
All participants provided written consent to be included in the study prior to data collection.
Consent for publication
Participants provided consent for their anonymized data to be used in publications.
Author contributions
Cervantes: Conceptualization, Investigation, Data curation, Formal Analysis, Writing – original draft; Garcia: Conceptualization, Data Curation, Formal analysis, Writing – original draft; Rodriguez-Crespo: Conceptualization, Data curation, Writing – review and editing; Urbina: Conceptualization, Writing – review and editing; Cooper: Conceptualization, Supervision, Writing – review and editing; Morera: Conceptualization, Formal Analysis, Methodology, Investigation, Resources, Supervision, Funding Acquisition, Writing – review and editing.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Study 1 received funding from the last author’s overhead funds. Study 2 received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset generated during and/or analyzed during the present study are available in the Figshare repository: Study 1 is available at: https://doi.org/10.6084/m9.figshare.28764956.v1. Study 2 is available at: ![]() .
.
Supplemental material
Supplemental material for this article is available online.