
Abstract
Binge eating is associated with a range of negative health outcomes and may be influenced by early life adversity. While childhood trauma is a known risk factor for disordered eating, the mechanisms underlying this relationship are not fully understood. This study examined whether perceived stress mediates the association between childhood trauma and trait binge eating in adults. A community sample of 391 participants (82% women; aged 17–76) completed the Childhood Trauma Questionnaire-Short Form, the Perceived Stress Scale, and the Binge Eating Scale. Mediation analyses revealed perceived stress partially mediated the relationship between childhood trauma and binge eating symptoms. Furthermore perceived helplessness and low self-efficacy as sub-components of perceived stress were mediators in relation to emotional abuse and physical neglect. These findings support the role of cognitive-affective stress appraisals as mechanisms linking early adversity to disordered eating behaviours and highlight targets for prevention and intervention efforts.
Introduction
Childhood trauma (CT) refers to distressing experiences during childhood or adolescence, including physical, emotional, or sexual abuse, neglect, and domestic violence. CT is a well-established risk factor for psychological issues including substance abuse (Zhang et al., 2020), depression (Dunn et al., 2013), and suicidal behaviour (Grattan et al., 2019), with effects that often persist into adulthood (Norman et al., 2012). CT has also been linked to eating psychopathology. In a systematic review, Palmisano et al. (2016) found that 87% of studies identified adverse life experiences as risk factors for obesity and binge eating disorder (BED). Binge eating carries metabolic risk, psychological distress, impaired functioning, and reduced quality of life, underscoring its public health relevance. Caslini et al. (2016) found associations between childhood abuse and various eating disorders, including links between emotional and sexual abuse and BED. Similarly, Pignatelli et al. (2017) reported higher prevalence of emotional and physical neglect in individuals with eating disorders. In obese women, CT was positively associated with binge eating severity (Imperatori et al., 2016), and binge eating has been linked to more severe CT, psychopathology, and higher BMI.
Efforts have sought mechanisms linking CT to disordered eating to inform interventions. A review by Rabito-Alcón et al. (2021) highlighted mediators including self-criticism (Dunkley et al., 2010) and dissociation (Waller et al., 2001). PTSD symptoms have also been identified as a mediator (Malinauskiene and Malinauskas, 2018). PTSD symptoms (re-experiencing, hyperarousal, avoidance) may promote dysregulated eating by heightening negative affect and threat vigilance, increasing urges to numb internal states, and narrowing coping repertoires, elevating risk for loss-of-control eating. However, most research has focused on non-childhood trauma or clinical eating disorders rather than binge eating behaviours. Few studies have examined stress as a mediator between CT and binge eating, despite theoretical and empirical links.
Stress influences food choice and intake (Chao et al., 2017). Acute stress can suppress appetite (Charmandari et al., 2005), whereas chronic stress often increases intake of highly palatable foods via hypothalamic–pituitary–adrenal (HPA) activation and cortisol release (Torres and Nowson, 2007). Sustained cortisol enhances mesolimbic reward processing in the insula and striatum (Zerbes et al., 2020), increasing incentive salience for sweet/fat foods and cue-elicited craving (Wonderlich et al., 2017). Peripherally, glucocorticoids act with insulin to up-regulate lipoprotein lipase and promote triglyceride storage and adipocyte differentiation, favouring visceral fat (Stice and Yokum, 2016; Torres and Nowson, 2007). Cortisol also increases ghrelin secretion, amplifying appetite and meal size, and may blunt leptin signalling (Spencer, 2014). Together, these pathways may explain how chronic stress elevates cravings and promotes fat gain, increasing vulnerability to binge eating.
Beyond physiological mechanisms, there is growing interest in how individuals appraise and respond to stress. The Perceived Stress Scale (PSS-10; Cohen et al., 1983) captures these cognitive-affective dimensions, particularly helplessness and self-efficacy. Perceived stress indexes appraisals of uncontrollability and coping (helplessness/low self-efficacy), which are proximal, modifiable mechanisms linked to loss-of-control eating; individuals who appraise stressors as overwhelming and feel unable to cope may be more likely to binge to down-regulate affect. Evidence shows that individuals with a history of CT tend to report elevated perceived stress in adulthood (Krause et al., 2003; Reiser et al., 2014), which can exacerbate vulnerability to psychopathology. Trauma can impair emotion regulation and coping, increasing sensitivity to later stressors (Michopoulos et al., 2015). From this perspective, perceived stress may represent a critical psychological mechanism linking CT to maladaptive behaviours such as binge eating.
The multidimensional nature of stress including physiological, emotional, and cognitive domains, warrants careful operationalisation in research. The PSS-10 offers strong validity in assessing how individuals experience and manage stress cognitively. This is relevant to binge eating, which has been associated with emotion regulation difficulties and a sense of loss of control (Heatherton and Baumeister, 1991). Emotional eating is often discussed as a coping strategy for stress (Adam and Epel, 2007), but it differs from binge eating, which involves consuming large amounts of food with a sense of loss of control and distress. Importantly, perceived stress has been shown to be associated with binge eating even after controlling for emotional eating (Michopoulos et al., 2015), and predicts binge frequency (Turner et al., 2018). Emotional eating reflects affect-driven intake without the quantity/loss-of-control that define binges; the association between perceived stress and binge eating after controlling for emotional eating suggests stress appraisals relate specifically to loss-of-control eating rather than affect-linked snacking alone.
The present study focuses on trait binge eating (TBE) measured using the Binge Eating Scale (BES). The BES is a widely used instrument suitable for non-clinical populations (Greeno et al., 1995). Here, ‘TBE’ denotes a dimensional propensity towards binge-like episodes and associated cognitions/emotions, as captured by the BES, rather than a categorical BED diagnosis. Using a dimensional outcome has clear advantages in this context: it captures the broader continuum of risk-relevant symptoms (including subclinical presentations), increases variance and statistical power in community samples where full BED is rare, and aligns with our appraisal-based mediation focus (perceived stress, helplessness, self-efficacy) that is theorised to operate on cognitions/emotions linked to loss of control. Accordingly, we interpret our outcome as trait binge-eating severity rather than discrete episode frequency.
The theoretical basis for this study draws on the affect regulation model and the diathesis–stress model. The affect regulation model posits that binge eating can serve as a maladaptive coping strategy for managing negative affect (Heatherton and Baumeister, 1991). From this view, perceived stress may trigger binge eating in individuals with poor emotion regulation, especially those with trauma histories. The diathesis–stress model suggests that psychopathology arises from an interaction between predisposing vulnerabilities (e.g. CT) and stress exposure (Monroe and Simons, 1991). CT may sensitise individuals to later stress, making them more vulnerable to disordered eating in the face of current perceived stress. These models jointly support a mediation framework, in which perceived stress plays a key role in linking CT to binge eating.
The current study aimed to test whether perceived stress mediates the relationship between CT and TBE in a non-clinical adult sample. It was hypothesised that higher perceived stress would partially mediate this relationship. In addition to the primary model, we explored specific pathways involving different types of CT (e.g. physical, emotional, and sexual abuse; neglect) and perceived stress subcomponents (helplessness and self-efficacy). We anticipated that trauma subtypes might differentially relate to stress appraisals (e.g. neglect and helplessness; abuse and low self-efficacy), consistent with reports that trauma timing and type shape binge-eating trajectories (Quilliot et al., 2019).
Methods
Participants
391 participants were recruited via the university participant pool (course credit) and social media posts (no incentive). Recruitment materials stated the study examined ‘stress and eating’. On completion, all participants received a debrief with links to support resources (e.g. BEAT Eating Disorders, NHS IAPT services, Samaritans). Those who had not finished the survey and therefore left more than 5 answers blank were removed from the data set, this meant analysis was conducted on 338 adults. The attrition rate for this study (those who started but did not complete the survey) was 13.55%. No specific fidelity/attention checks were implemented beyond excluding incomplete responses. We were unable to compare completers to non-completers because demographics were not consistently captured prior to withdrawal. Participants were aged between 18 and 76 (M = 25.91, SD = 13.14) with the majority being female (82.5%), furthermore most respondents were from a white ethnic background (85.8%). For a full break down of demographics please see Table 1. Those who were recruited on the University participant pool, had an incentive of course credits. There were no other rewards for participation other than the valuable contribution to research in this field. Participants were required to be of or over the age of 18, there were no other inclusion or exclusion criteria.
Participant characteristics, sex and ethnicity.
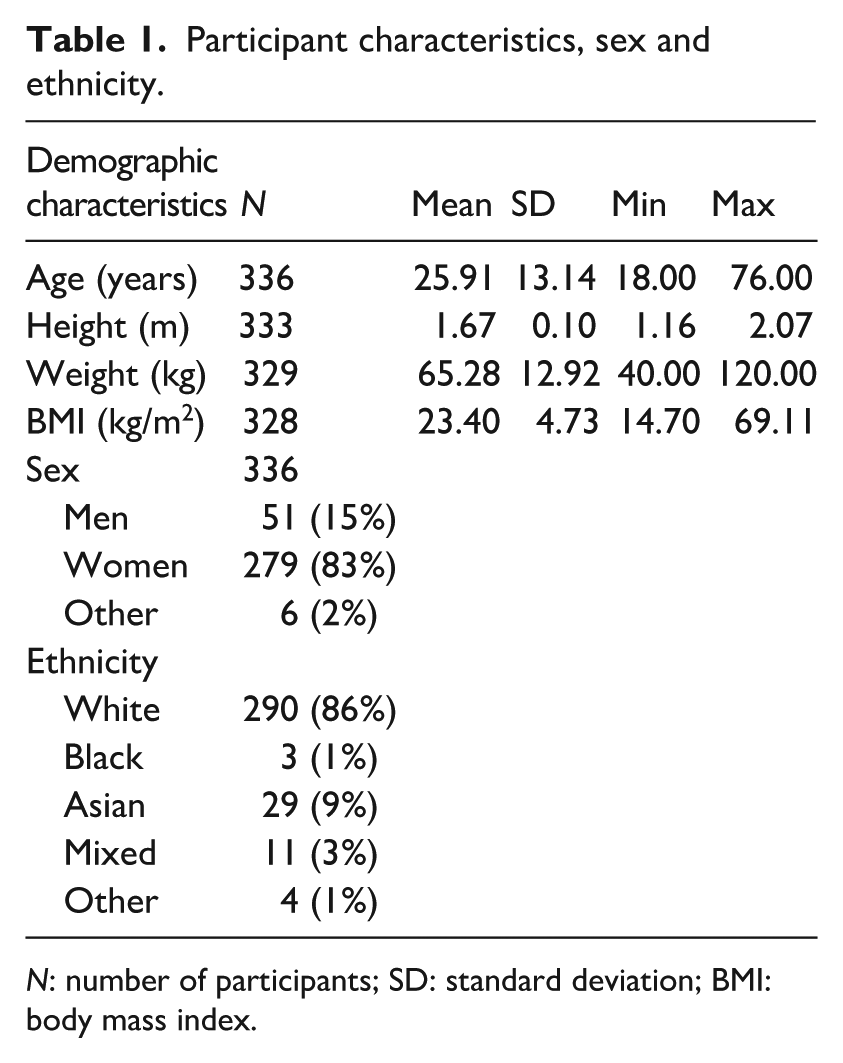
N: number of participants; SD: standard deviation; BMI: body mass index.
Design and procedure
A cross sectional research design was used. The survey was launched on the 10/01/2023. The online survey consisted of three questionnaires; the perceived stress scale (PSS-10; Cohen et al., 1983), the binge eating scale (BES; Gormally et al., 1982), and the childhood trauma questionnaire-short form (CTQ-SF; Bernstein et al., 2003). Participants were also required to answer demographic questions before taking part in the questionnaires. Once the survey had been completed, the respondent was debriefed. The aims of the study were reiterated to the participant and support materials were provided. Qualtrics facilitated data collection and storage, this data was then exported to SPSS when the questionnaire closed. Data collection finished on 16.02.23.
Ethical approval
This study was approved by the University of Leeds Ethics Committee (#PSYC-705, date of approval 19/12/2022). Before agreeing to take part in the survey participants were provided with an information sheet explaining what was being asked of them. This explained about the potentially distressing material and that support was available for those who felt it was needed. Participants were also made aware that their responses were anonymous and confidential, furthermore that they did not have to answer a question if they did not wish to do so.
Measures
Childhood trauma questionnaire-short form (CTQ-SF)
Childhood trauma was assessed using the CTQ-SF (Bernstein et al., 2003), a 28-item self-report measure that retrospectively assesses five domains of maltreatment: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. It also includes three questions with a minimisation/denial scale for detecting those who may be underreporting traumatic events. Items are rated on a 5-point Likert scale (1 = never true to 5 = very often true). The CTQ has demonstrated strong psychometric properties across clinical and non-clinical populations, with good convergent validity, test-retest reliability, and discriminant validity in relation to interviewer-based assessments of trauma (Scher et al., 2001). The original CTQ-SF had a moderate to high Cronbach’s alpha value of 0.85 (Bernstein et al., 2003). In the present study, Cronbach’s alpha values for the subscales were: emotional abuse (α = 0.85), physical abuse (α = 0.82), sexual abuse (α = 0.94), emotional neglect (α = 0.89), and physical neglect (α = 0.67).
Perceived stress scale
The PSS-10 is a 10-item questionnaire developed by Cohen and Williamson (1988) used to evaluate perceived stress levels over the past month. The questions ask about thoughts and feelings, assessing the degree to which an individual has perceived life as uncontrollable, unpredictable, and overloading. The questions have a general nature instead of focusing on specific stressful events. Respondents are asked to indicate how often they felt a certain way in the previous month on a five-point scale from ‘never’ to ‘very often’, coded 0–4, respectively. There are two subscales within the PSS-10; perceived helplessness and lack of self-efficacy. The PSS-10 is widely used in health psychology and has demonstrated good construct validity, factorial stability, and predictive validity across diverse populations (Lee, 2012). In the current sample, Cronbach’s alpha was 0.89 for the total scale, with subscale alphas of 0.87 (helplessness) and 0.74 (self-efficacy).
Binge eating scale
Trait Binge Eating (TBE) was assessed using the BES, devised by Gormally et al. (1982. This is a 16-item scale used to evaluate the presence of binge eating behaviour that may be indicative of an eating disorder. Eight questions are designed to capture the behavioural aspects of binge eating traits, for example large amounts of food consumed. The remaining eight questions assess the cognitive and emotional aspects, for example feeling out of control around food. Participants scores are summed resulting in a score range from 0 to 46. BES items include 3–4 response options where participants choose which of several sentences within an item fits them best. For example Q2i) I don’t have any difficulty eating slowly in the proper manner; ii) Although I seem to ‘gobble down’ foods, I don’t end up feeling stuffed because of eating too much.; iii) At times, I tend to eat quickly and then, I feel uncomfortably full afterwards, or; iv) I have the habit of bolting down my food, without really chewing it. When this happens I usually feel uncomfortably stuffed because I’ve eaten too much. Marcus et al. (1988) defined the scores from the binge eating scale as non-bingeing; 17 or less, moderate; 18–26, and severe binge eating; 27 and greater. The BES scale has a moderate to high internal reliability with a Cronbach’s alpha value of 0.88 (Duarte et al., 2015). In this study, Cronbach’s alpha for the BES total score was 0.88.
Statistical analyses
A formal a priori power analysis was not conducted for this study. However, the final sample size (N = 338) is consistent with or exceeds those used in previous mediation studies examining psychosocial mechanisms between childhood trauma and disordered eating (e.g. Michopoulos et al., 2015; Reiser et al., 2014). According to MacKinnon et al. (2007), detecting a small to medium indirect effect in a simple mediation model with 80% power requires approximately 350 participants. Therefore, the current sample is likely to have sufficient power to detect effects of similar magnitude. Effect sizes for indirect effects are reported in the Results to aid interpretation.
Analyses of the data were carried out using IBM SPSS Statistics Version 28.0.1.1. For the mediation analysis 18 models were analysed. These were created using the total CTQ-SF and its subscales, the total PSS-10 and its subscales, and the BES. All mediation models were carried out separately. The perceived stress scale was split into its subscales; perceived helplessness and lack of self-efficacy to examine them as conceptually different pathways that may mediate the relationship between childhood trauma and TBE.
Normality of data was checked before the correlation and mediation analysis were performed. The Shapiro-Wilk and Kolmogorov-Smirnov tests were disregarded as the sample size is considered too large (n > 300), for these sensitive tests. In this case the histograms were relied on to visually analyse the normality and distribution of the data. The histograms showed that height, PSS-10 total, perceived helplessness, lack of self-efficacy were all normally distributed, representing a bell-shaped curve. Weight appeared to be normally distributed with a slight positive skew, as was similar for BMI. The histograms for the BES, CTQ-SF and its subscales did not show normal distribution, these were all positively skewed. However, this was to be expected for the variables being measured, the sample aimed to gather results from a range of participants on experiences that are adverse. Therefore, the data does reflect the prevalence of TBE and CT in a wider population. For these variables, non-parametric analyses were used. Statistical outliers falling within the valid range of the scales were retained.
Mediation analyses
Mediation analysis was performed using the SPSS add on PROCESS v4.3. via bootstrapping effect (Hayes, 2009). Bootstrapping has been used as opposed to Sobel’s test (Sobel, 1982) to determine if the relationship between the independent variable and the dependent variable has been reduced after inclusion of the mediator. This is because bootstrapping does not require assumptions of normality to be met within the data, it also provides an increase in power over Sobel’s test.
Path a is the relationship between the predictor variable and the mediator, path b is the relationship between the mediator and the outcome variable. The direct effect is the relationship between the predictor variable and the outcome variable when the role of the mediator is accounted for. The indirect effect is the effect of the predictor variable on the outcome variable that operates through the mediator. The total effect is the overall effect of the predictor variable on the outcome variable, without controlling for the mediator. If the indirect effect is significant this suggests that there is mediation. If the direct effect is significant then this suggests that there is partial mediation, if the direct effect is non-significant then this suggests full mediation. The primary mediation model consisted of CT, which was the predictor variable, TBE, was the outcome variable, and stress as the mediator. Other secondary mediation models using the subscales of the PSS-10 and the CTQ-SF were performed. For a breakdown of all models refer to Table 2. BMI was not included as a covariate because it may lie on the causal pathway between stress/trauma and eating, and adjusting for potential mediators can bias indirect-effect estimates. Moreover, bivariate correlations with CT were negligible and with TBE modest; we therefore report unadjusted models and highlight BMI as a target for future sensitivity analyses.
Mediation analysis for study variables and their subscales.
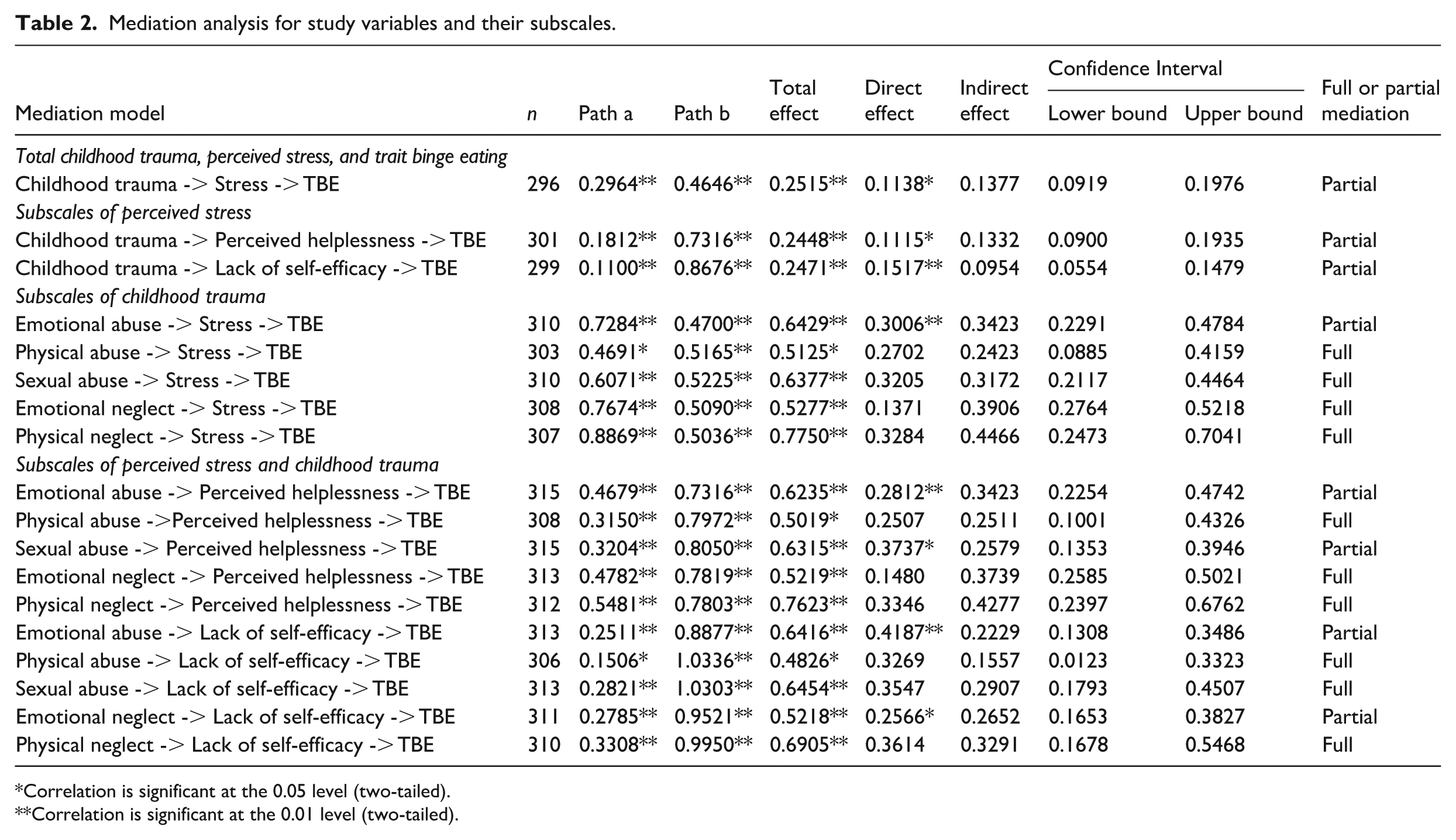
Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
Results
Descriptive statistics and correlations
Descriptive statistics for the study variables, and their subscales, are presented in Supplemental Table S1.
Of the 338 respondents, 17 did not answer all BES questions and therefore a TBE score was not calculated for them. 243 (75.7%) individuals were classed as non-binge eaters, 59 (18.4%) individuals were classed as moderate binge eaters, and 19 (5.9%) individuals were classed as severe binge eaters. The CTQ-SF was broken down into its subtypes to analyse the how many participants fell into each category; none, low, moderate, and severe. The cut off point for the low (to moderate) category was used to assess whether someone had experienced CT. Therefore, 195 (58.3%) participants experienced childhood emotional abuse, 35 (10.7%) participants experienced childhood physical abuse, 36 (10.7%) participants experienced childhood sexual abuse, 115 (34.5%) participants experienced childhood emotional neglect, and 82 (24.8%) participants experienced childhood physical neglect. For the perceived stress scale, 10 individuals did not provide answers for all questions, therefore 110 (33.5%) participants were classified as highly stressed. The remaining 218 (66.6%) were classified as having low stress levels.
A bivariate correlation using Spearman’s Rho was conducted to examine the associations between CT, stress, TBE, and BMI. For the correlation analysis the PSS-10 and the CTQ-SF were further broken down into their subscales. CT was found to be significantly positively correlated with stress r(308) = 0.408, p < 0.001, perceived helplessness r(313) = 0.374, p < 0.001, lack of self-efficacy r(312) = 0.375, p < 0.001, and TBE r(302) = 0.251, p < 0.001, it was not correlated with BMI. For further correlations between the subscales please refer to Supplemental Table S2.
Mediation analyses
All mediation models performed in the study are summarised in Table 2.
Total childhood trauma, stress, and binge eating
Path a indicated that CT had a significant, positive effect on stress (b = 0.2964, 95% BCa CI [0.2152, 0.3775] t = 7.1914, p < 0.001). The R2 for this model was 14.9%. Path b indicated that stress had a significant positive effect on TBE (b = 0.4646, 95% BCa CI [0.3465, 0.5827], t = 7.7425, p < 0.001). When the role of stress was accounted for, the direct effect of CT on TBE was significant (b = 0.1138, 95% BCa CI [0.0233, 0.2043], t = 2.4757, p = 0.0139). The R2 for this model was 24.5%. The total effect of CT on TBE, without controlling for stress, was significant (b = 0.2515, 95% BCa CI [0.1601, 0.3429], t = 5.414, p < 0.001). The R2 for this model was 9%. The indirect effect of CT on TBE through stress was significant (b = 0.1377, 95% BCa CI [0.0919, 0.1976]). Therefore, stress partially mediates the relationship between CT and TBE. For a visualisation of this model, please refer to Figure 1.
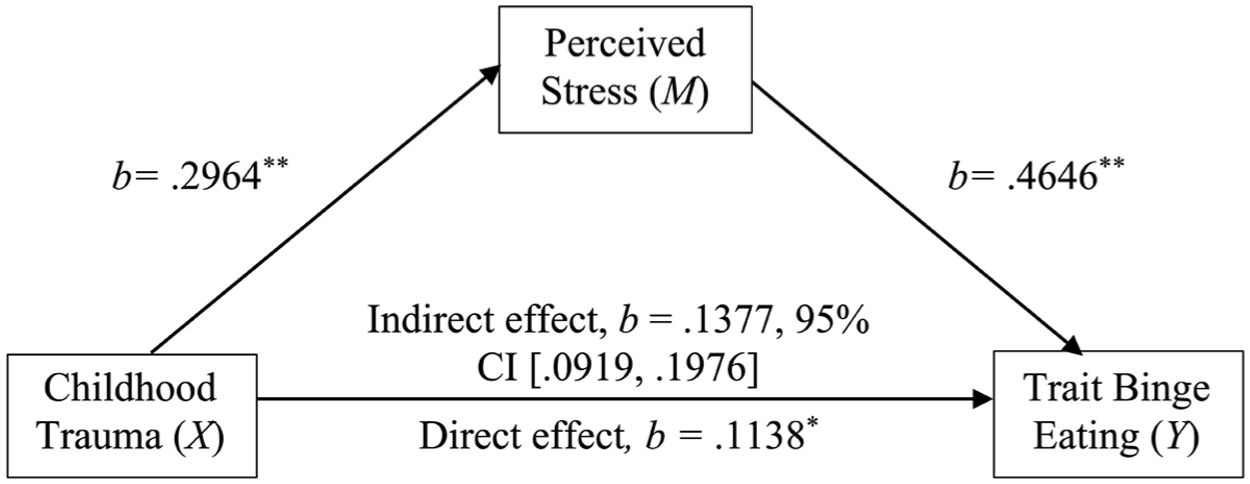
Mediation model of CT, Perceived stress, TBE.
Emotional abuse
Path a suggested that emotional abuse had a significant, positive effect on stress (b = 0.7284, 95% BCa CI [0.5420, 0.9147], t = 7.6911, p < 0.001). The R2 for this model was 16.1%. Path b suggests that stress had a significant positive effect on TBE (b = 0.4700, 95% BCa CI [0.3544, 0.5855], t = 8.0029, p < 0.001). When the role of stress was accounted for, the direct effect of emotional abuse on TBE was significant (b = 0.3006, 95% BCa CI [0.0909, 0.5103], t = 2.8204, p = 0.0051). The R2 for this model was 25.9%. The total effect of emotional abuse on TBE, without controlling for stress, was significant (b = 0.6429, 95% BCa CI [0.4321, 0.8537], t = 6.0010, p < 0.001). The R2 for this model was 10.5%. The indirect effect of emotional abuse on TBE through stress was significant (b = 0.3423, 95% BCa CI [0.2291, 0.4784]). Therefore, stress partially mediated the relationship between childhood emotional abuse and TBE.
Physical abuse
Path a indicates that physical abuse had a significant, positive effect on stress (b = 0.4691, 95% BCa CI [0.0997, 0.8385], t = 2.4989, p = 0.0130). The R2 for this model was 2%. Path b indicates that stress had a significant positive effect on TBE (b = 0.5165, 95% BCa CI [0.4071, 0.6258], t = 9.2950, p < 0.001). When the role of stress was accounted for, the direct effect of physical abuse on TBE was non-significant (b = 0.2702, 95% BCa CI [−0.0896, 0.6300], t = 1.4779, p = 0.1405). The R2 for this model was 23.9%. The total effect of physical abuse on TBE, without controlling for stress, was significant (b = 0.5125, 95% BCa CI [0.1090, 0.9160], t = 2.4995, p = 0.0130). The R2 for this model was 2%. The indirect effect of physical abuse on TBE through stress was significant (b = 0.2423, 95% BCa CI [0.0885, 0.4159]). Therefore, stress fully mediated the relationship between childhood physical abuse and TBE.
Sexual abuse
Path a suggests that sexual abuse had a significant, positive effect on stress (b = 0.6071, 95% BCa CI [0.2672, 0.9470], t = 3.5143, p = 0.0005). The R2 for this model was 3.9%. Path b suggested that stress had a significant impact on TBE (b = 0.5225, 95% BCa CI [0.4135, 0.6316], t = 9.4262, p < 0.001). When the role of stress was accounted for, the direct effect of sexual abuse on TBE was non-significant (b = 0.3205, 95% BCa CI [−0.0167, 0.6578], t = 1.8700, p = 0.0624). The R2 for this model was 25.2%. The total effect of sexual abuse on TBE, without controlling for stress, was significant (b = 0.6377, 95% BCa CI [0.2628, 1.0126], t = 3.3472, p = 0.0009). The R2 for this model was 3.5%. The indirect effect of sexual abuse on TBE through stress was significant (b = 0.3172, 95% BCa CI [0.2117, 0.4464]). Therefore, stress was a full mediator for the relationship between childhood sexual abuse and TBE.
Emotional neglect
Path a demonstrates that emotional neglect had a significant, positive effect on stress (b = 0.7674, 95% BCa CI [0.5868, 0.9480], t = 8.3616, p < 0.001). The R2 for this model is 18.6%. Path b suggests that stress had a significant effect on TBE (b = 0.5090, 95% BCa CI [0.3898, 0.6283], t = 8.3984, p < 0.001). When the role of stress was accounted for, the direct effect of emotional neglect on TBE was non-significant (b = 0.1371, 95% BCa CI [−0.0751, 0.3493], t = 1.2714, p = 2046). The R2 for this model was 24.7%. The total effect of emotional neglect on TBE, without controlling for stress, was significant (b = 0.5277, 95% BCa CI [0.3156, 0.7398], t = 4.8958, p < 0.001). The R2 for this model was 7.3%. The indirect effect of emotional neglect on TBE through stress was significant (b = 0.3906, 95% BCa CI [0.2764, 0.5218]). Therefore, this suggests that stress fully mediated the relationship between childhood emotional neglect and TBE.
Physical neglect
Path a suggests that physical neglect had a significant, positive effect on stress (b = 0.8869, 95% BCa CI [0.5314, 1.2425], t = 4.9083, p < 0.001). The R2 for this model was 7.3%. Path b suggests that stress had a significant effect on TBE (b = 0.5036, 95% BCa CI [0.3921, 0.6150], t = 8.8916, p < 0.001). When the role of stress was accounted for, the direct effect of physical neglect on TBE was non-significant (b = 0.3284, 95% BCa CI [−0.0369, 0.6937], t = 1.7689, p = 0.0779). The R2 for this model was 24.4%. The total effect of physical neglect on TBE, without controlling for stress, was significant (b = 0.7750, 95% BCa CI [0.3809, 1.1691], t = 3.8694, p < 0.001). The R2 for this model was 4.7%. The indirect effect of physical neglect on TBE, through stress, was significant (b = 0.4466, 95% BCa CI [0.2473, 7041]). Therefore, stress fully mediated the relationship between childhood physical neglect and TBE.
Perceived helplessness and lack of self-efficacy
Analyses using the PSS-10 subscales perceived helplessness and lack of self-efficacy mirrored total-scale findings. Helplessness and low self-efficacy each transmitted CT effects to TBE, with patterns varying by trauma subtype (Table 2). Helplessness showed robust indirect paths for neglect; low self-efficacy showed robust paths for abuse.
Discussion
Summary of findings
The present study examined whether perceived stress mediates the relationship between childhood trauma (CT) and trait binge eating (TBE) in adulthood. Among participants, 24.3% showed moderate to severe TBE, and 33.5% reported high perceived stress. Emotional abuse and neglect were the most commonly reported traumas, while physical and sexual abuse were less frequent. Perceived stress partially mediated the relationship between overall CT and TBE, as well as between emotional abuse and TBE. It fully mediated the relationships between physical abuse, sexual abuse, emotional neglect, and physical neglect with TBE. Further analysis showed that perceived helplessness and low self-efficacy sub-components of perceived stress also acted as full or partial mediators across all trauma subtypes. These findings highlight perceived stress as a key psychological mechanism linking childhood trauma to adult binge eating traits.
Comparison with hypotheses and previous research
The finding that perceived stress partially mediates the relationship between childhood trauma (CT) and trait binge eating (TBE) suggests it plays an important, but not exclusive, role in the development of binge eating among trauma-exposed individuals. This aligns with prior research showing multiple mediators such as depression and dissociation link trauma to disordered eating (Rabito-Alcón et al., 2021). Emotional abuse was the only CT subtype partially mediated by stress, indicating that other psychological mechanisms may be at play. Partial mediation for emotional abuse may reflect additional pathways (e.g. shame, interpersonal sensitivity, body image disturbance), whereas neglect-related pathways may be more tightly coupled to chronic uncontrollability (helplessness) and diminished coping capacity. Emotional abuse is particularly developmentally harmful, often undermining a child’s emotional security and self-worth (Trickett et al., 2009). Resulting difficulties in emotion regulation, self-esteem, and psychological distress (Kilpatrick et al., 2003) may increase vulnerability to maladaptive coping strategies such as binge eating. These findings reinforce the importance of considering different trauma subtypes and their unique psychological consequences when examining pathways to disordered eating.
Stress as a full mediator between physical neglect and TBE had the largest effect size for the indirect effect, compared to the other mediation models. Physical neglect may involve inadequate access to food and a chronically unstable home environment, leading to both physical deprivation and psychological stress (Ekern, 2020). Prior research has linked childhood food insecurity to later binge eating, driven by early experiences of starvation and related stress (Coffino et al., 2020; Grilo et al., 2001). The finding that perceived helplessness and low self-efficacy mediated this relationship suggests that the consequences of physical neglect extend beyond food deprivation. Neglect may impair a child’s developing sense of control and agency (Hildyard and Wolfe, 2002), fostering beliefs that they cannot influence or manage their environment. These cognitive vulnerabilities may persist into adulthood, increasing susceptibility to maladaptive coping behaviours like binge eating in times of stress or emotional dysregulation. The observed mediation pathway may therefore reflect how early neglect undermines self-regulatory capacity, shaping long-term stress responses and increasing vulnerability to disordered eating patterns.
Mediation is a theoretical construct, and it is likely that other unmeasured variables contribute to the observed relationships. The finding that perceived helplessness and low self-efficacy mediate the link between childhood trauma and binge eating symptoms supports psychological models highlighting impaired emotion regulation and coping as consequences of early adversity. Childhood maltreatment can undermine beliefs about control, competence, and distress tolerance (McLaughlin et al., 2014), leading to a lasting sense of helplessness. This may prompt maladaptive coping strategies like binge eating as a means of emotional escape (Heatherton and Baumeister, 1991). Low self-efficacy is associated with diminished perceived control over behaviour and emotion regulation (Bandura, 1997), which may increase vulnerability to loss-of-control eating. Patterns in the sub-components of perceived stress were consistent with theory: neglect related more strongly to helplessness (enduring appraisals of uncontrollability), while abuse related to low self-efficacy (reduced confidence in regulating emotions/behaviour). These findings suggest that cognitive-affective stress appraisals shaped by trauma may act as mechanisms linking early adversity to disordered eating. Targeting these beliefs in treatment through cognitive restructuring or skills-based approaches may be valuable for individuals with trauma histories and binge eating symptoms.
Correlational analysis showed that physical abuse was not significantly associated with perceived stress, self-efficacy, helplessness, or TBE, contrary to previous findings (Caslini et al., 2016). However, mediation analysis revealed that physical abuse significantly predicted TBE, with stress, perceived helplessness, and low self-efficacy acting as mediators. This discrepancy may be explained by a suppressor effect, in which a variable enhances the predictive validity of another in regression analysis (Krus and Wilkinson, 1986). The true relationship between physical abuse and TBE may have been masked in simple correlations and became apparent only when controlling for other mediators in the regression model.
Not everyone who experiences (traumatic) stress will develop an eating disorder. The diathesis–stress model posits that psychological disorders arise from an interaction between genetic vulnerability and environmental stress (Broerman, 2017). This explains why some individuals with a predisposition remain healthy in the absence of stress, and others exposed to stress do not develop disorders due to lack of genetic risk. Additionally, protective factors can buffer against the negative impact of stress. These include individual traits like resilience and external conditions such as parental and social support (Sussman, 2023). Such factors reduce the likelihood of psychopathology, even in the presence of both diathesis and stress. In the context of childhood trauma, this suggests that children exposed to adverse experiences may not go on to develop binge eating behaviours if they also benefit from strong protective factors. Enhancing these buffers could be key in preventing disordered eating in vulnerable populations.
Implications
This study has important implications for individuals experiencing binge eating, particularly those with a history of CT. While CT should be prevented wherever possible, its long-term effects must be addressed when prevention is not possible. Positive childhood experiences (PCEs) are protective and associated with fewer mental health problems, better diet, and improved sleep (Bethell et al., 2019; Crandall et al., 2019). Our findings suggest that perceived stress and especially helplessness and low self-efficacy, may link CT, particularly physical neglect, to trait binge eating in adulthood. Assessing perceived stress in those with early adversity, even without a clinical diagnosis, may help identify individuals at risk. Screening for stress appraisals in trauma-exposed adults can guide stress-focused CBT (reframing uncontrollability beliefs), skills to enhance coping self-efficacy, and trauma-informed interventions (e.g. grounding, distress-tolerance). For maltreated youth, caregiver-focused programmes stabilising routines may prevent consolidation of helplessness. Trauma-informed care models that incorporate stress management may be particularly effective. These findings also support prevention strategies aimed at strengthening perceived coping capacity to buffer the long-term impact of early trauma on eating behaviour.
Strengths and limitations
The present findings indicate a correlational, not causal, relationship. In this context, correlational designs are ethically appropriate for examining mediators. While the sample size of 338 was adequate, the study did not focus on individuals with obesity. Only 7.4% were classified with obesity and 29.3% with overweight, both lower than national estimates for adults, yet nearly a quarter displayed moderate to severe binge eating traits. This supports the idea that binge eating can occur independently of weight status but may underrepresent patterns seen in obese populations, where the prevalence in England is 25.9% (NHS England, 2022). Furthermore, the sample was predominantly female, limiting analysis of sex differences. Although BED is more prevalent among women (2.8%) than men (1%) (Wick et al., 2020), the lack of male participants prevents examination of potentially important gender-specific experiences. The mostly female sample may also have led to the higher than expected estimates of binge eating prevalence. Future studies should prioritise more balanced sampling across sex and weight strata to improve generalisability and better capture sex-related differences in binge eating behaviours.
This study used the Childhood Trauma Questionnaire Short Form (CTQ-SF) to assess trauma experienced before age 18. This is a strength of the current research, as its 5-point Likert scale enables respondents to report the frequency of various trauma types (emotional, physical, and sexual abuse), as well as emotional and physical neglect, rather than forcing a simple yes/no answer. In contrast, the ACE Questionnaire (Felitti et al., 1998) uses dichotomous response options, which do not capture differences in severity or frequency. This could place individuals with vastly different trauma histories in the same category, limiting the measure’s sensitivity. However, the CTQ-SF also has limitations. Unlike the ACE Questionnaire, it does not assess household dysfunction such as parental separation, mental illness, substance abuse, or domestic violence. These factors are known to contribute to long-term health outcomes. As a result, some participants may have experienced adversity that was not captured by the CTQ-SF. Moreover, neither questionnaire accounts for other significant childhood stressors such as bullying, bereavement, medical trauma, natural disasters, or exposure to violence or terrorism (Oseldman, 2018). These limitations suggest that while the CTQ-SF provided useful data for this study, it may underestimate the full scope of adverse childhood experiences relevant to perceived stress and binge eating. Future studies should consider broader and more comprehensive trauma assessments.
Another limitation of this study concerns the interpretation of the psychological constructs measured by the PSS-10 and BES. The PSS-10 assesses perceived stress over the past month and is primarily focused on cognitive and affective appraisals of stress, rather than physiological symptoms or objective stress exposure. In contrast, the BES does not specify a time frame for participant responses and captures a combination of binge eating behaviours, thoughts, and emotional responses. This mismatch in temporal framing and construct specificity makes it difficult to draw conclusions about direct or causal relationships between stress and binge eating. Although the mediation model was statistically supported, the results should be interpreted cautiously, as they reflect associations between two subjective, self-reported constructs with potentially differing temporal anchors. Future research should consider using measures with aligned time frames and more precise behavioural or physiological assessments of both stress and eating pathology to enhance construct clarity and inferential validity.
Future research directions
Future research should address this study’s conceptual and methodological limitations. The Binge Eating Scale captures behavioural, cognitive, and emotional features and future work could separate these to examine whether perceived stress differentially predicts binge behaviours (e.g. food quantity) versus binge-related thoughts (e.g. guilt, loss of control). Future work should test additional mediators (e.g. shame, self-criticism, intolerance of uncertainty, dissociation) and integrate physiological stress indices (cortisol, HRV) alongside perceived stress to clarify multi-system pathways. As mentioned, the cross-sectional design limits causal interpretation therefore longitudinal designs are needed to establish temporal direction. Ecological momentary assessment (EMA) could also shed light on real-time associations between stress and eating. Finally, experimental or intervention studies should explore whether reducing perceived helplessness and enhancing self-efficacy might moderate the link between childhood trauma and binge eating, offering promising avenues for therapeutic development in trauma-exposed individuals.
Another direction for future research may include focusing more on disordered eating behaviours in men. Historically, eating disorders are the most gendered of psychiatric illnesses and this has consequences as the way they are treated and assessed is generally female orientated (Gorrell and Murray, 2019). Striegel-Moore et al. (2009) found that men with BED were more likely to report ‘overeating’, whilst women with BED were more likely to report ‘loss of control whilst eating’ and body check more than men. Eating disorders in men may be shown in different ways such as intense weightlifting, low fat/high protein diets, and taking supplements, but as these are not common features of an eating disorder, they often go unnoticed (Gorrell and Murray, 2019).
Conclusion
The results of this study demonstrate that perceived stress mediates the relationship between CT and TBE in adulthood. Despite certain study limitations that have been highlighted, the findings have particular importance for those engaging in binge eating behaviour. Stress interventions may be an effective treatment for some individuals, where CT has been experienced. It is crucial that successful therapies are designed and advised appropriately as binge eating can lead to numerous other physical and psychological health problems, such as obesity and depression (Özdin et al., 2021).
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251401296 – Supplemental material for Perceived stress appraisals mediate the association between childhood trauma and trait binge eating in adults
Supplemental material, sj-docx-1-hpq-10.1177_13591053251401296 for Perceived stress appraisals mediate the association between childhood trauma and trait binge eating in adults by Leah Harwood and Graham Finlayson in Journal of Health Psychology
Footnotes
Ethical considerations
The Research Ethics Review Committee at University of Leeds approved this study (approval: #PSYC-705) on December 19, 2022.
Consent to participate
Respondents gave written informed consent to participate and consent to publish before proceeding with the survey.
Author contributions
Graham Finlayson: Conceptualisation; Project administration; Supervision; Writing – review and editing. Leah Harwood: Conceptualisation; Data curation; Formal analysis; Investigation; Visualisation; Writing – original draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data will be made available upon reasonable request to the corresponding author at
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.