
Abstract
This study identified latent profiles of Asian American (AA) young adults based on family connectedness, interaction quality, and shared activities, and examined their associations with perceived influence on health behaviors (diet, exercise, sleep, stress management, social relationships, and risky substances). Using survey data from 500 AA young adults (ages 18–35), Latent Profile Analysis identified three profiles: fragmented (11.2%), ambivalent (33%), and strongly bonded (55.8%). Strongly bonded individuals reported greater family influence on health behaviors—especially sleep, stress management, and social relationships, and stronger personal influence on family members’ diet and exercise compared to the fragmented group. The ambivalent group showed limited influence, with most effects insubstantially different from the fragmented group. Findings underscore the importance of tailoring health interventions to distinct family profiles—leveraging strong bonds through culturally grounded programs, enhancing interaction in ambivalent families, and providing external support for those with strained family ties.
Keywords
Introduction
Family relationships play a central role in shaping health across the life course (Ho et al., 2022; Ramos et al., 2022; Thomas et al., 2017). Much of this influence often operates through behavioral pathways—supportive, cohesive families tend to foster healthier behaviors, while strained or conflictual family ties are often linked to maladaptive health practices (Ramos et al., 2022; Thomas et al., 2017; Umberson et al., 2010). However, most research adopts a unidirectional perspective, examining how family relationships affect health behaviors (Ailshire and Burgard, 2012; Hahm and Keum, 2025; Ng and Jeffery, 2003; Ramos et al., 2022).
Guided by Family Systems Theory (FST) and Social Control Theory (SCT), this study views families as interdependent systems in which members mutually shape one another’s behaviors (Del Vecchio and Rhoades, 2010; Gadhoke et al., 2015). FST highlights how relational dynamics operate, and SCT explains how norms and role expectations channel those dynamics into influence (Lewis et al., 2004; Umberson, 1987). Dyadic research leveraging Actor-Partner Interdependence Models (APIM) has captured these reciprocal processes, particularly in romantic partnerships (e.g., Kiecolt-Glaser and Wilson, 2017), but has rarely been applied to young adults.
Young adults are often portrayed as recipients of parental guidance, yet evidence shows they also exert upward and lateral influence on parents, siblings, and extended kin (Reczek et al., 2014; Sleddens et al., 2017). This calls for reconceptualizing social control, a key mechanism linking family relationships and health, as communal and multidirectional rather than strictly top-down (Lewis et al., 2004; Wilson et al., 2024). While parent–child and spousal ties remain central, most studies give limited attention to young adults, whose meaningful family interactions often extend to siblings and extended kin (Hahm and Keum, 2025; Kwon et al., 2025). Prioritizing the family members with whom participants interact most frequently, rather than predefined family ties, provides a more ecologically valid and inclusive understanding of how families influence health behaviors.
This study centers on perceived family influence—the extent to which individuals believe their family affects their health behaviors and vice versa. This construct is distinct from observed behavioral concordance (behavioral similarities or co-engagement) and directly observed influence (explicit acts of encouragement, monitoring, or modeling). Perceived influence reflects internalized norms, expectations, and emotional dynamics that may shape behavior even in the absence of direct interaction. Importantly, these subjective perceptions can be as—if not more—impactful than observable actions, as they guide how individuals interpret family relationships and internalize health-related norms (Vautero et al., 2021). Assessing perceived influence, therefore, helps illuminate the psychological mechanisms through which family ties shape health behaviors, while distinguishing these effects from external or observable drivers.
Rather than treating family-related factors like family support or conflict in isolation, this study employs a person-centered strategy—Latent Profile Analysis (LPA)—to identify subgroups defined by connectedness, interaction quality, and shared activities (Lindstedt et al., 2024). This approach aligns with FST’s focus on relational patterns and SCT’s emphasis on normative regulation, linking family configurations to health behaviors in a way that moves beyond isolated indicators of support or conflict.
LPA is particularly well-suited to Asian American (AA) families, where collectivism, intergenerational responsibilities, and internalized cultural expectations shape multiple dimensions of family life (e.g., Choi et al., 2021). The indicators used in LPA map onto these cultural constructs: connectedness reflects collectivist orientations and filial piety; interaction quality—spanning appreciative, positive, and negative interactions—captures norms of emotional harmony, face-saving, and conflict management; and shared activities represent interdependence in practice.
In AA families, emotional closeness often intertwines with hierarchical roles and shared obligations, producing both cohesion and potential tension (e.g., intergenerational conflict, acculturation differences). Traditional variable-centered approaches might overlook such constellations, whereas LPA uncovers culturally embedded patterns where emotional closeness, appreciation, and shared activity may co-occur—or diverge—in meaningful ways. This resonates with FST and SCT’s view of health behaviors as shaped by interdependent, culturally embedded relational systems.
AA families serve as powerful sources of support but also potential sources of tension and strain, especially as young adults navigate autonomy within cultural contexts that emphasize relational interdependence. These dynamics are not uniform—cultural values, migration histories, and family structures vary across East Asian, South Asian, Southeast Asian, and mixed-heritage groups (Paik et al., 2017). This heterogeneity underscores the value of a person-centered approach, which can identify distinct relational patterns rather than assuming a single model of AA family life.
Using survey data from 500 AA young adults (ages 18–35), this study (1) identifies distinct family relationship profiles and (2) examines how these profiles relate to perceived familial and personal influence on six domains of health behavior: diet, exercise, sleep, stress management, social relationships, and risky substance use.
Health and health behaviors in Asian American young adults
Young AA adults face unique cultural and developmental contexts that affect health behaviors. Despite the “model minority” stereotype, they face notable challenges in lifestyle-related domains—including obesity, sedentary behavior, and substance use—often at higher rates than their immigrant parents (Chan et al., 2024; Choi et al., 2023; Gong et al., 2019). These risks are further compounded by acculturation stress (Unger et al., 2004). Families may co-manage health behaviors across generations, transmit expectations, and reinforce health norms. Exploring family dynamics as reciprocal systems in which young adults may shape health practices can highlight culturally grounded leverage points for health intervention within the AA community.
Family system theory and social control theory
Our conceptual framework draws on Family Systems Theory (FST) and Social Control Theory (SCT). FST emphasizes families as dynamic, interdependent systems in which relational patterns—such as engagement frequency, interaction quality, and emotional closeness—shape how health norms and practices are transmitted, resisted, or co-constructed (Bowen, 1966; Ho et al., 2022; Lucas-Thompson and Goldberg, 2011). Within these systems, young adults are not only recipients of family influence but also active contributors who introduce and reinforce health practices. Complementing this, SCT explains the mechanisms through which influence occurs (Lewis et al., 2004; Umberson, 1987). It specifies how influence is enacted through direct strategies (e.g., encouragement, monitoring) and indirect processes (e.g., internalized values, role obligations, emotional accountability; Reczek et al., 2014; Tucker et al., 2004). Together, these frameworks help clarify why perceived family influence can manifest differently across profiles—for example, a profile characterized by high connectedness, but low co-engagement may, from an FST perspective, reflect relational involvement sustained by enduring emotional ties, while SCT highlights how internalized family norms and expectations can continue to guide behavior even in the absence of frequent shared activities. This integration motivates our use of Latent Profile Analysis (LPA) to identify configurations of family connectedness, interaction quality, and shared activity, and to interpret how these relational profiles channel family influence on health behaviors.
Methods
Data
Data were collected via an online Qualtrics survey in March 2021, with participants recruited through social media and Asian American community organizations. Eligible individuals were 18–35 years old, self-identified as Asian American, and had at least one U.S.-based family member. This study received approval from the Institutional Review Board (Ali et al., 2022), and all participants provided informed online consent prior to data collection in the study. Although not nationally representative, this large and diverse sample offers valuable insights into family interactions and health behaviors among young Asian American adults.
Some variables, particularly those on family influence and connectedness, had higher missingness because they appeared later in the survey. Examination of Qualtrics’ progress indicator—a percentage reflecting how much of the survey a respondent completed—revealed that participants missing these items typically had scores below 63%, suggesting they exited the survey before reaching those questions. Thus, missingness primarily reflected attrition rather than item-level nonresponse.
Measures
Participants were asked to rank family members based on frequency of interaction—from 1 (most frequent) to 8 (least)—allowing the study to focus on the most influential relationship while avoiding dilution from less influential ties.
Next, participants reported the extent to which this family member influenced their own health behaviors and vice versa across six domains: diet, exercise, sleep, stress management, social relationships, and substance use. These domains were adapted from established lifestyle health indicators (American College Health Association, 2018) and reflect both behavioral practices and psychosocial functioning. Although social relationships are not behaviors per se, they shape and are shaped by health practices (e.g., social support for exercise, peer influence on substance use; Umberson et al., 2010), justifying their inclusion. To capture this broader scope, we use the term “health behaviors” rather than “healthy lifestyle behaviors.”
Perceived influence was rated on a 6-point scale (1 = no influence, 6 = extremely strong influence), with “don’t know” coded as zero. For analyses, scores were dichotomized into low (1–3) and high (4–6) influence. This cutoff was guided by both conceptual considerations—distinguishing minimal/moderate influence from strong guidance or support—and empirical patterns: medians fell between 3 and 4, the 75th percentile was ⩾ 4, and the distribution showed slight leptokurtosis (kurtosis > 2), indicating concentration toward scale endpoints. Although dichotomization entails some loss of variability, sensitivity analyses using the original continuous scale yielded substantively similar results, supporting the robustness of the binary categorization.
An overall perceived influence composite score was calculated by summing responses across the six domains (range: 0–36), which was included in the analyses.
The family connectedness scale was measured using a five-item Likert scale assessing emotional closeness and support, with items like “They care about your feelings” (Cronbach’s alpha = 0.88).
Interaction quality was assessed using a 28-item questionnaire that measured the frequency of positive, negative, and appreciative interactions (e.g. “I feel respected”). Participants rated each item on a six-point scale ranging from 1 (never) to 6 (always). The scale demonstrated excellent internal consistency (Cronbach’s alpha = 0.95–0.96; Ali et al., 2025).
Recognizing that shared experiences strengthen relational bonds and contribute to emotional and behavioral outcomes, the study also measured the types and frequency of shared activities with participants’ most frequently interacted-with family members. This was assessed using the 30-item Shared Activities with Family (SAF) Index, a newly developed instrument tailored for Asian American young adults through expert consultation and qualitative research (Ali et al., 2025). The measure was refined through an iterative process involving cognitive interviews and expert review to ensure content and face validity. A confirmatory factor analysis and correlations with related constructs (e.g. family connectedness) provided partial support for construct validity. However, the breadth of survey indicators limited more extensive psychometric testing (e.g. criterion or discriminant validity), which we acknowledge as a limitation. Participants reported the frequency of engagement in routine and shared activities using a six-point scale (1 = never, 6 = many times a day). Responses were averaged to create a shared activities index, with higher scores indicating greater involvement in shared family activities.
Covariates in the regression models included age (in years), gender (1 = female, 0 = male), relationship status (1 = married/partners, 0 = widowed/divorced/separated), educational attainment (some college or less, bachelor’s, master’s or more), specific Asian American ethnic subgroup (East Asian, South Asian, Southeast Asian, Mixed), religion, household size (1, 2–3, 4 or more), work status (currently working), nativity (being born in the U.S.), and acculturation (measured by a four-item Short Acculturation Scale).
Analytic strategy
We used Latent Profile Analysis (LPA) to identify subgroups of participants based on reported family connectedness, interaction quality, and shared activities. LPA models were estimated iteratively with increasing numbers of profiles, using 10 random seed starts. Model selection was guided by fit indices—log-likelihood, AIC, BIC, ABIC, entropy—and the Lo-Mendell-Rubin test (LMRT). Lower AIC/BIC and higher entropy (closer to 1) indicated better fit (Killian et al., 2019; Lo et al., 2001; Nylund et al., 2007). To avoid spurious solutions, we excluded models with profiles under 5% of the sample (Elliott et al., 2020)
Once the optimal model was identified, participants were assigned to profiles based on posterior probabilities. We then performed multiple regression analyses to assess whether perceived influence on health behaviors varied across profiles. To facilitate interpretation, logistic regression models were estimated using dichotomized influence ratings (low = 1–3, high = 4–6), consistent with the categorization described in the Measures section. As a robustness check, we also ran parallel models using the original continuous scores; results were substantively unchanged. All analyses were conducted in Stata 18.0 (StataCorp, 2023) using maximum likelihood estimation with robust standard errors.
Results
Descriptive characteristics
Sample characteristics are presented in Table 1. The final sample included 500 Asian American young adults (ages 18–35; M = 24.14, SD = 4.89) from diverse ethnic backgrounds: 48% East Asian, 21% South Asian, 23% Southeast Asian, and 8% mixed ethnicity. Most were U.S.-born (77%), with 41.6% holding a bachelor’s degree and 25.8% a master’s or higher. Participants reported moderate perceived familial influence on their own health-related behaviors (M = 19.19, SD = 7.98), especially regarding diet (58%), exercise (51%), substance use (47%), and stress management (42%). Similarly, they perceived influence on family members’ behaviors (M = 16.62, SD = 7.85), again mostly in diet (49%) and exercise (42%). Family connectedness scores were high (M = 4.13, SD = 0.89), and positive interaction quality was similarly strong (positive: M = 4.79, SD = 1.08; appreciative: M = 4.72, SD = 1.17), while negative interaction remained low (M = 2.48, SD = 1.10).
Descriptive statistics of the variables included in the analysis (N = 500).
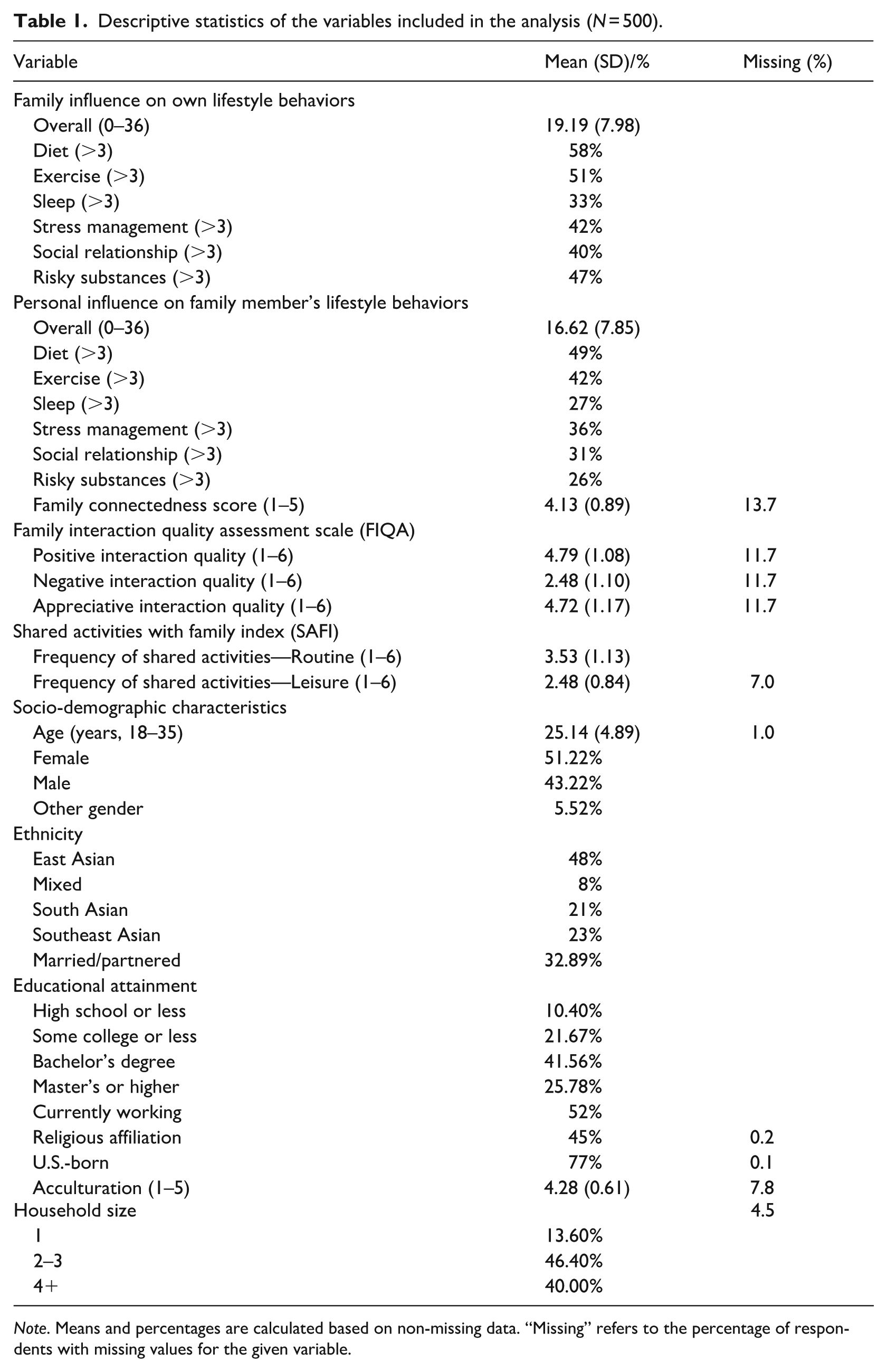
Note. Means and percentages are calculated based on non-missing data. “Missing” refers to the percentage of respondents with missing values for the given variable.
Latent profile analysis and profile characteristics
Table 2 presents model fit indices for two- to five-profile solutions. Fit improved with additional profiles, as indicated by decreasing AIC, BIC, and ABIC values and significant LMR LRT p-values (p < 0.001). However, improvements diminished beyond three profiles. The three-profile model showed the highest entropy (0.97), and met the minimum class size guideline, unlike the four-profile model, which had a group with less than 5% (Elliott et al., 2020; Sinha et al., 2021). Thus, the three-profile model was selected for its optimal balance of fit, class separation, and interpretability.
Latent profile analysis model fit indices for two to four profiles.
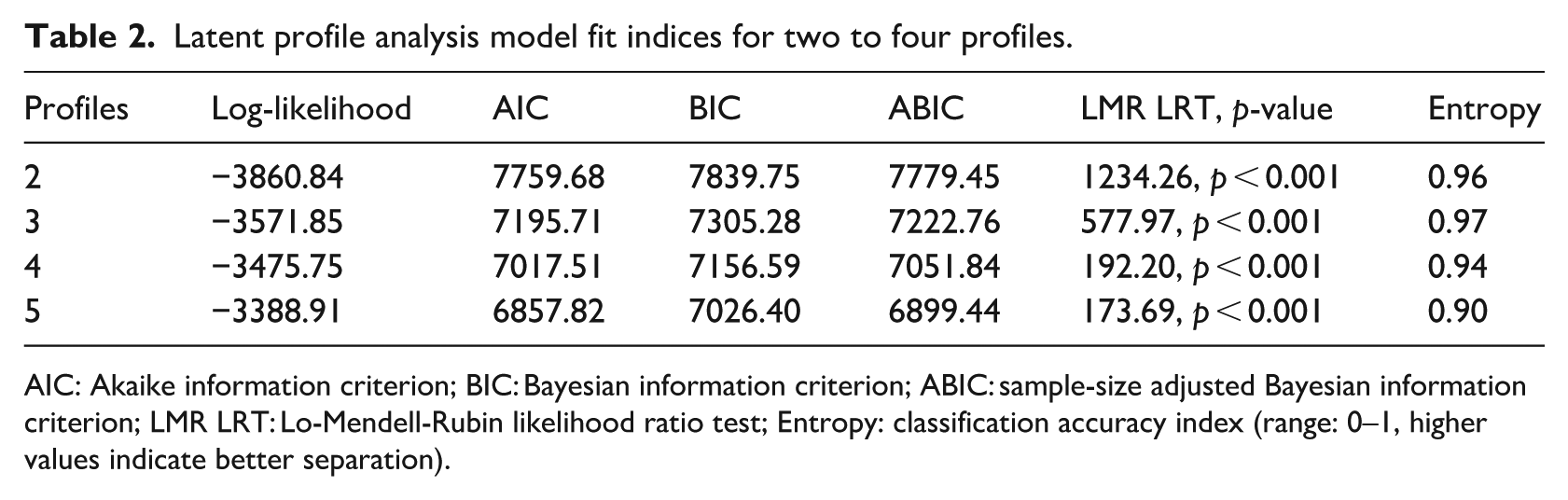
AIC: Akaike information criterion; BIC: Bayesian information criterion; ABIC: sample-size adjusted Bayesian information criterion; LMR LRT: Lo-Mendell-Rubin likelihood ratio test; Entropy: classification accuracy index (range: 0–1, higher values indicate better separation).
Figure 1 displays the profile means of each indicator, with three profiles identified based on patterns of interaction and connectedness. The first profile, “the fragmented” (n = 56, 11.20%), was marked by low family connectedness (2.40), high negative interaction (4.68), low positive interaction (3.37), and infrequent shared activities (1.78), reflecting strained or distant family ties. Although the smallest class, its size exceeded the commonly recommended 5% threshold for interpretability in LPA (Elliott et al., 2020; Sinha et al., 2021). Its distinct pattern of limited engagement and strained interactions supports retaining it as a conceptually meaningful group. The second, “the ambivalent” (n = 165, 33%), reflected a mix of moderate positive and negative interactions, representing a middle ground between fragmentation and strong bonding. The third, “the strongly bonded” (n = 279, 55.80%), showed high connectedness (4.75), high positive interaction (6.49), low negative interaction (2.26), and the most frequent participation in shared activities (leisure: 2.83; routine:3.93).
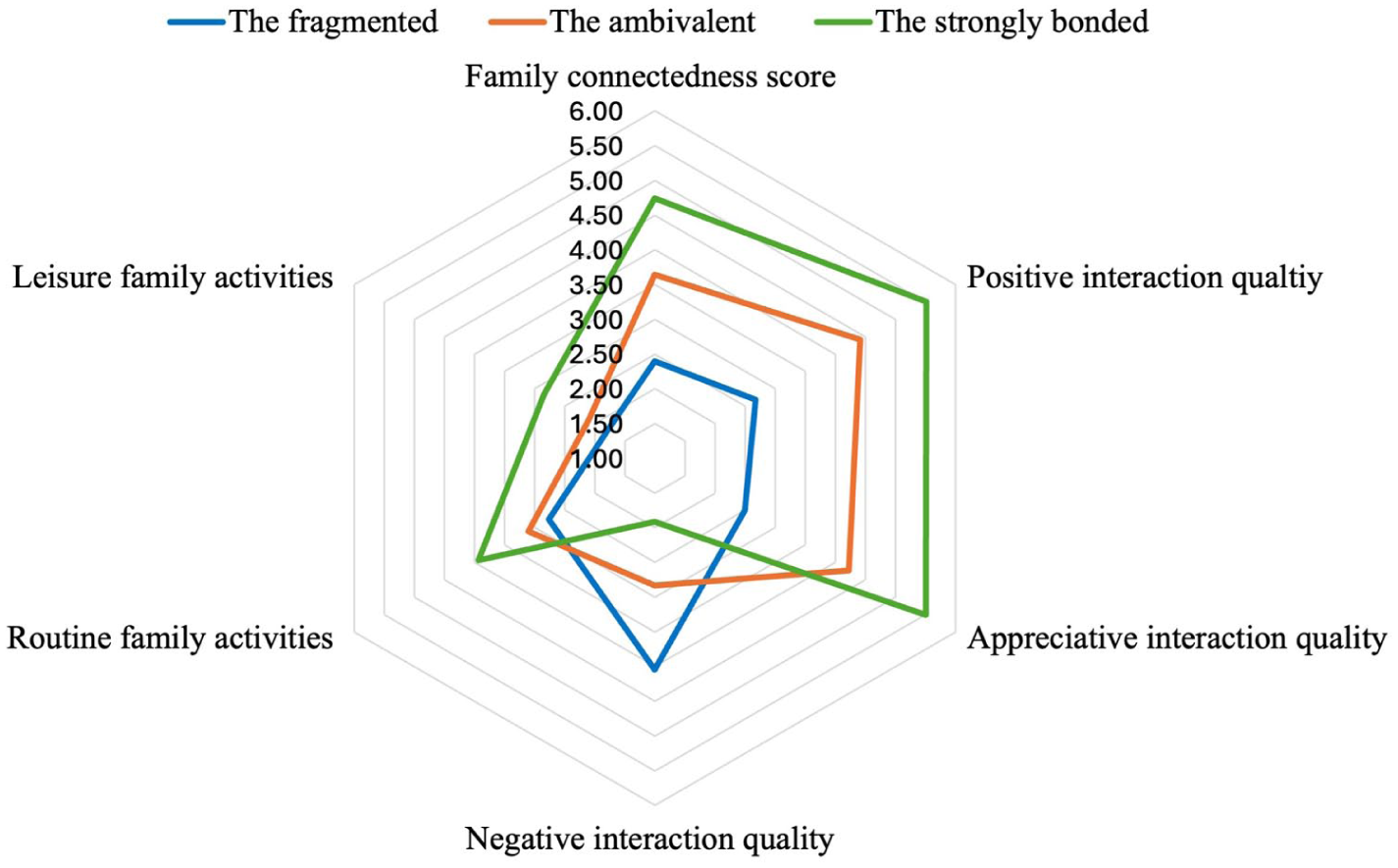
Profile stratified average latent profile analysis indicator variable scores. The fragmented (Profile 1): Low connectedness, low shared activity, high negative interactions. The ambivalent (Profile 2): Moderate connectedness, moderate shared activity, mixed interaction quality (positive and negative). The strongly bonded (Profile 3): High connectedness, high shared activity, high positive interactions.
Association between family interaction profiles and perceived influence on health behaviors
Table 3 presents multivariate regression results using the fragmented profile as the reference group. The first two columns display associations between profiles and familial influence on health behaviors, while the last two reflect personal influence on family members’ health behaviors. Compared to the fragmented group, the strongly bonded reported significantly higher perceived family (b = 5.36, p < 0.001) and personal influence (b = 6.82, p < 0.001) on health behaviors. The ambivalent also showed stronger perceived influence (family influence: b = 2.06, p < 0.10; personal influence: b = 2.67, p < 0.05), though the effects were weaker.
Regression estimates predicting perceived family and personal influence health behaviors, Abridged.
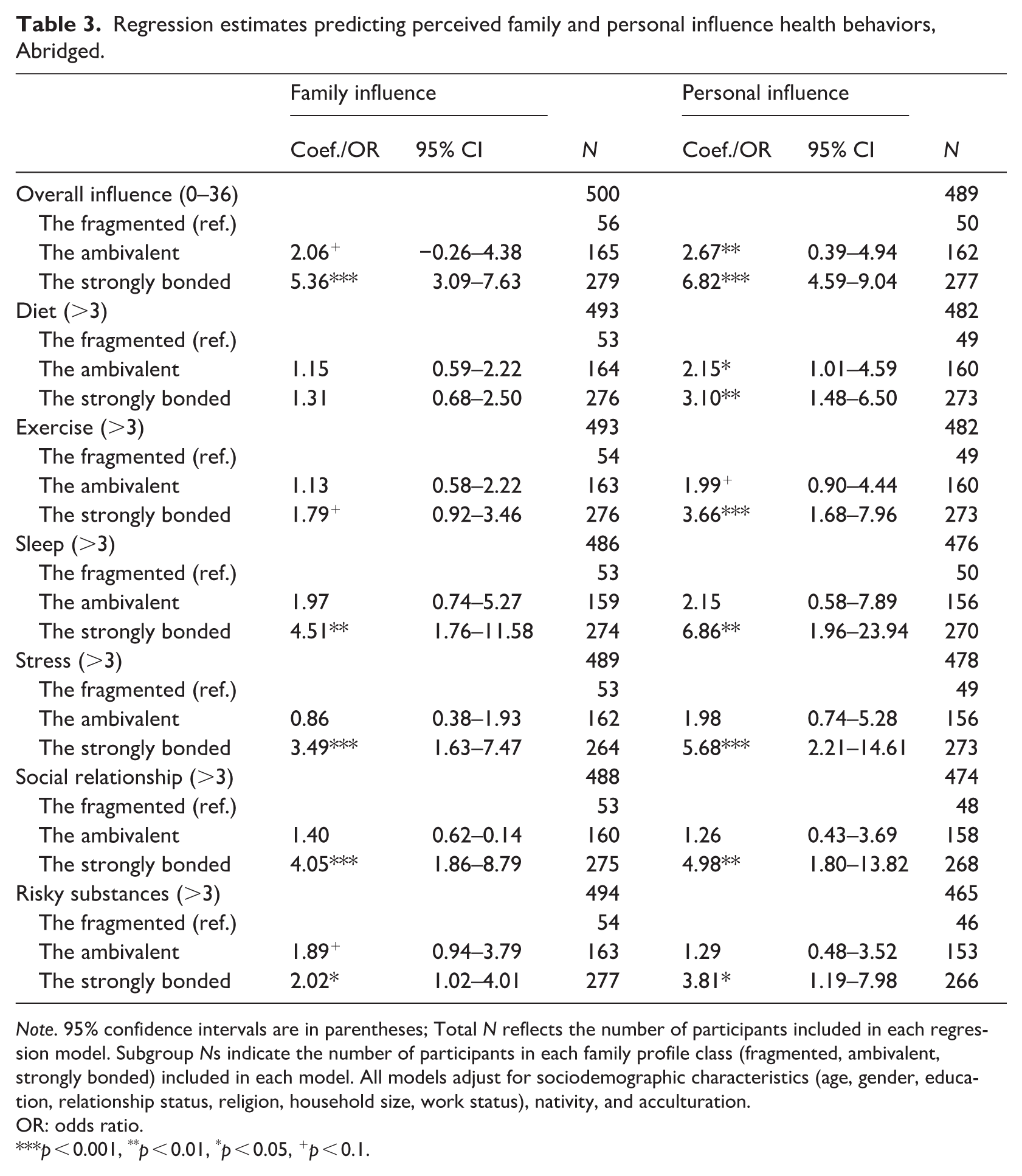
Note. 95% confidence intervals are in parentheses; Total N reflects the number of participants included in each regression model. Subgroup Ns indicate the number of participants in each family profile class (fragmented, ambivalent, strongly bonded) included in each model. All models adjust for sociodemographic characteristics (age, gender, education, relationship status, religion, household size, work status), nativity, and acculturation.
OR: odds ratio.
p < 0.001, **p < 0.01, *p < 0.05, +p < 0.1.
Multivariate regression analyzes examining associations between sociodemographic covariates and perceived influence are presented in Supplemental Table S1. South Asian participants reported significantly greater family (b = 2.29, p < 0.01) and personal (b = 2.37, p < 0.01) influence compared to East Asians (reference group), while no differences were observed for Southeast Asian or mixed-ethnicity participants. Domain-specific analyses showed this pattern held across diet, exercise, sleep, and stress management, but not risky substance use. Neither nativity (U.S.-born) nor acculturation emerged as significant predictors. Greater family and personal influence were also observed among married participants and those with a religious affiliation, while gender, age, and education showed no consistent associations.
In domain-specific analyses, both the strongly bonded and ambivalent groups had significantly higher personal (but not family) influence on diet and exercise. For sleep, the strongly bonded group showed significantly greater both family (OR = 4.51, 95% CI: 1.76–11.58) and personal influence (OR = 6.86, 95% CI: 1.96–23.94), while the ambivalent group did not. Similar patterns were observed for stress management, social relationships, and risky substance use, with only the strongly bonded showing significant associations. Overall, these findings indicate that the strongly bonded profile was consistently more likely than the fragmented profile to both influence and be influenced by family members across all six domains, whereas the ambivalent group’s influence patterns more closely resembled those of the fragmented group.
Figures 2 and 3 illustrate the predicted probabilities of high perceived influence across multiple domains, with full numeric values provided in Supplemental Table S2. For example, in the sleep domain, there was a 55% predicted probability of reporting high perceived family influence in the strongly bonded group, whereas the probabilities were 22% for the ambivalent group and 25% for the fragmented group. In terms of personal influence on exercise, there was a 49.7% predicted probability of reporting high influence in the strongly bonded group, compared to 21.2% for the ambivalent group and 35.1% for the fragmented group.
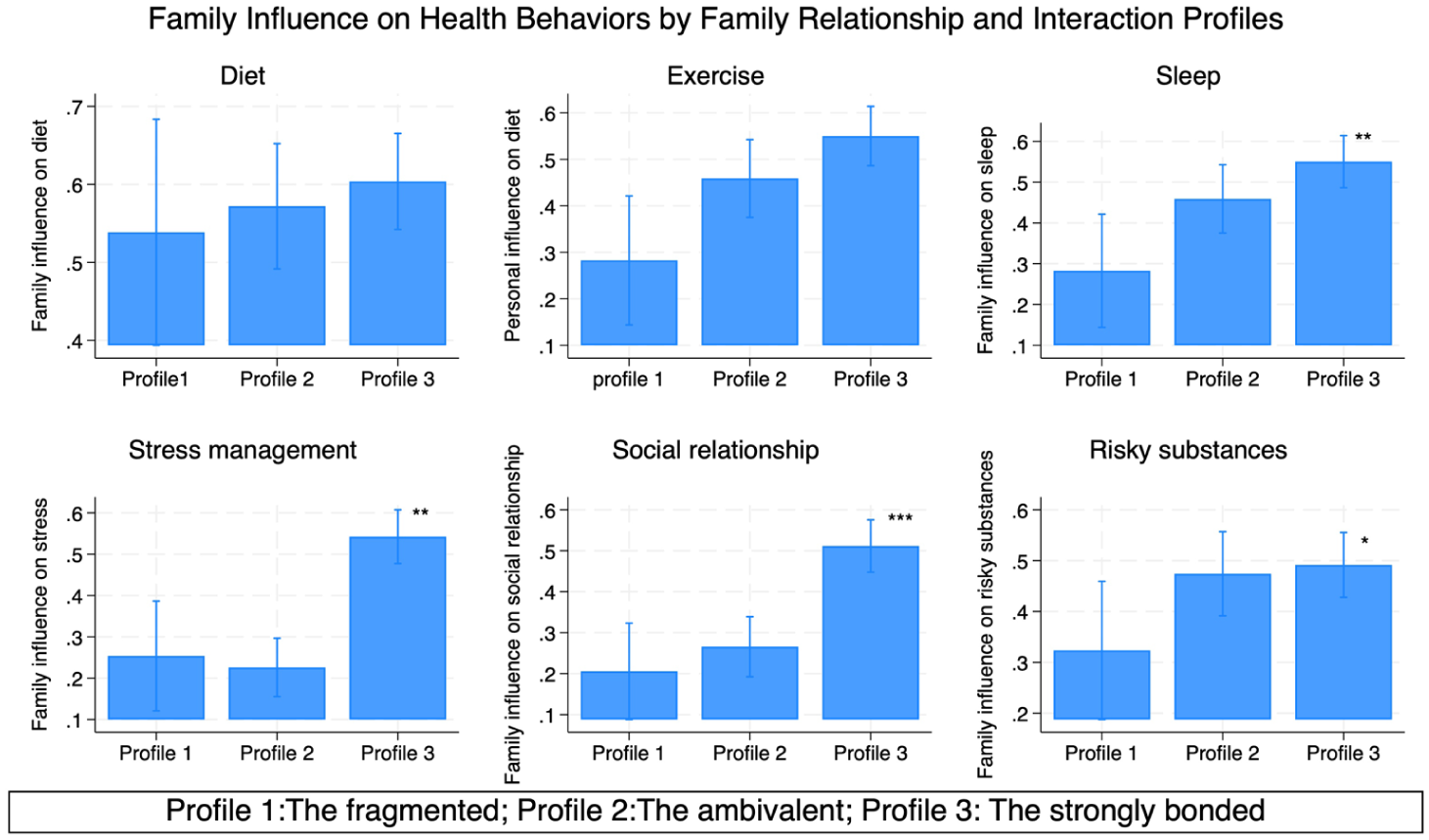
Predicted probability of high family influence on health behaviors by family interaction and relationship profiles.
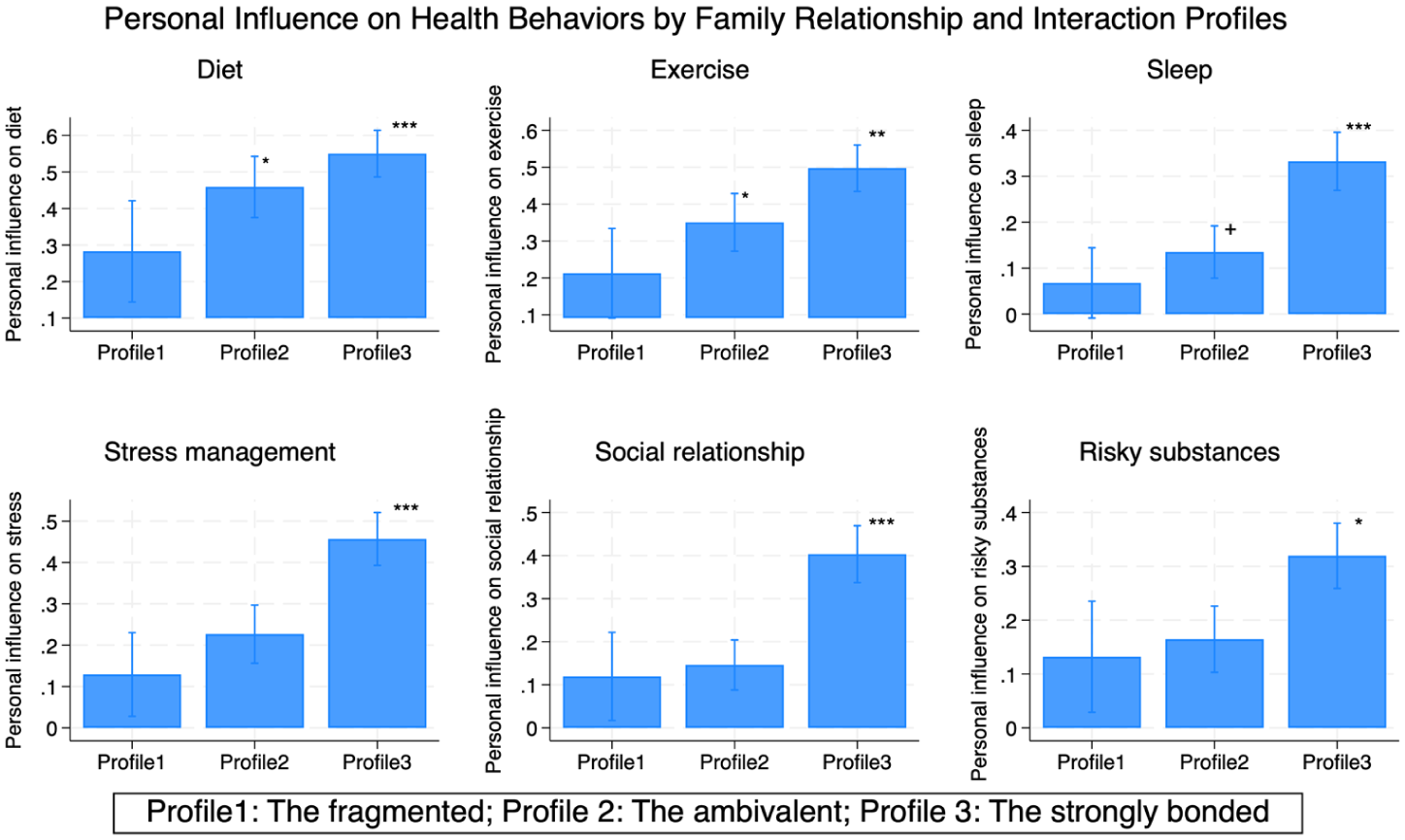
Predicted the probability of high personal influence on family members’ health behaviors by family interaction and relationship profiles.
Although Profile 1 met the recommended 5% minimum size for inclusion in LPA models and was conceptually distinct from the other profiles, its relatively small sample size resulted in wider confidence intervals (Figures 2 and 3), which may limit the power to detect associations. Replication with larger samples will be important to confirm these findings.
Discussion
In light of growing public health concerns surrounding Asian American (AA) young adults (Gong et al., 2019), this study examined how family dynamics shape their health behaviors by analyzing the links between family interaction profiles, relationship patterns, and perceived influence. Using Latent Profile Analysis (LPA), we identified three distinct family profiles—fragmented, ambivalent, and strongly bonded—with the strongly bonded profile being the most prevalent.
Perceived family influence followed a clear gradient: lowest in fragmented families, intermediate in ambivalent families, and highest in strongly bonded families. This pattern held across nearly all domains, suggesting that the profiles capture degrees of closeness and interaction rather than qualitatively distinct family types. Notably, young adults in the strongly bonded group reported not only being influenced by their families but also exerting influence in return, consistent with Family Systems Theory (FST; Bowen, 1993), which emphasizes the co-construction of health norms and behaviors through reciprocal interaction. Conceptually, Social Control Theory (SCT) provides one lens for interpreting these patterns, as it outlines how influence can occur through direct strategies (reminders, modeling) and indirect processes (internalized expectations, obligations). Although our data did not distinguish between these mechanisms, SCT helps illustrate how perceived influence may operate in strongly bonded families—where frequent interaction and emotional closeness could facilitate both forms of social control. In this sense, young adults’ mutual influence within their families may reflect both internalized expectations and relational modeling of healthy practices. A caveat should be acknowledged that this interpretation represents a theoretical explanation rather than a direct empirical finding, offering a conceptual framework for understanding how relational contexts might channel family influence on health behaviors.
Building on this theoretical framing, our model integrates Family Systems Theory (FST) and SCT to link relational structures with perceived influence. FST specifies the relational configurations that define profile membership (connectedness, interaction quality, shared activities), while SCT describes how norms and role obligations within those configurations are enacted as perceived influence. Strongly bonded families provide fertile conditions for both direct and indirect social control, fostering robust bidirectional influence. Ambivalent and fragmented families, by contrast, offer weaker contexts for these mechanisms, with fewer opportunities to reinforce norms and expectations consistently.
These findings echo previous research showing that children can influence parents’ health behaviors (Backett-Milburn and Harden, 2004; Backett-Milburn and Jackson, 2012; Gadhoke et al., 2015; Reczek et al., 2014; Thomas et al., 2019). They also align with SCT’s emphasis on the role of supportive, indirect strategies—such as reminders, shared expectations, and emotional accountability—which are especially effective in emotionally close relationships (Lewis et al., 2004; Lewis and Butterfield, 2005; Umberson, 1992). These forms of influence are often viewed as more legitimate and acceptable than overt or coercive approaches, which may explain why strongly bonded families demonstrated the most significant influence (Craddock et al., 2015; Lewis and Butterfield, 2005; Reczek et al., 2014). While SCT provides a useful interpretive framework for understanding these dynamics, the present study did not include measures that directly capture distinct forms or modalities of social control (e.g., direct vs indirect, verbal vs nonverbal). As such, our ability to empirically evaluate specific SCT-driven processes was limited. Future work should incorporate more fine-grained measures to capture how these mechanisms operate across culturally diverse family contexts. In Asian American families, for example, norms of filial piety and interdependence may amplify these supportive forms of control, making the cultural grounding of SCT processes especially important to examine.
As this study centered on participants’ most frequently engaged family members, we did not distinguish among specific relational roles. To provide context, we examined the type of primary family member with whom participants reported the most frequent interaction. As shown in Supplemental Table S3, the most common were mothers (37%), spouses or partners (29%), and siblings (21%), suggesting that our results primarily reflect close nuclear family relationships. This contextualization is important, as these ties have been identified in prior research as key sites of reciprocal health influence. For example, within couples, greater relationship satisfaction has been linked to greater alignment in health behaviors (Homish and Leonard, 2005; Jackson et al., 2015; Kiecolt-Glaser and Wilson, 2017; Lewis and Butterfield, 2007).
In contrast, the ambivalent group—those reporting moderate emotional closeness but inconsistent or limited engagement—showed weaker, often nonsignificant, associations with perceived health influence, in many cases resembling those observed in the fragmented group. This pattern suggests that emotional connectedness alone may not translate into reciprocal health-related influence without consistent, positive engagement (Lewis and Butterfield, 2007; Umberson et al., 2010). For example, ambivalent participants often described feeling close to family but reported infrequent involvement in shared activities such as eating meals together, watching TV or movies, participating in religious or cultural events, or collaborating on household tasks—activities that typically reinforce influence.
Auxiliary analyses reinforce this gap: 52% reported high family connectedness (scores ⩾ 4), yet only 18% endorsed high positive interaction quality (scores > 4), 14% reported high appreciative interactions (scores > 4), and fewer than 5% engaged in frequent shared activities. This disconnect may reflect cultural norms that value cohesion without consistent behavioral expression. Moreover, mixed interactions—those involving both positive and negative interactions—may dilute perceived influence by undermining the stability of health norms (Gaydosh and Harris, 2018; Theiss, 2017). Although negative interactions were rare (2%, vs 26% in the fragmented group), the lack of regular engagement appeared equally limiting. As such, ambivalence may signal a form of latent closeness—emotionally anchored but behaviorally muted—that constrains the translation of family bonds into actionable health influence.
The degree of family influence varied across health behavior domains. Strongly bonded families exerted the greatest impact on sleep, stress management, and social relationships that are tightly embedded in daily routines and emotional dynamics. For instance, family expectations around bedtime or productivity can directly affect sleep patterns (Ailshire and Burgard, 2012; El-Sheikh and Kelly, 2017; Punamäki et al., 2023). Likewise, stress coping often occurs through shared problem-solving or emotional reassurance, particularly in culturally collectivist settings like many AA households (Juang and Alvarez, 2010; Lucas-Thompson and Goldberg, 2011). Families also shape social relationships by guiding friendships and reinforcing intergenerational norms (Flynn et al., 2017; Rubin et al., 2004), with support or conflict within core ties spilling over into other relational domains (Sentse and Laird, 2010).
On the other hand, perceived family influence was notably weaker for diet and exercise, likely reflecting greater personal autonomy and stronger external influences from school, work, peers, and social media. As young adults transition out of parental and family oversight, they gradually gain increased independence in health-related decision-making, shifting the primary sources of influence away from the family (Beasley et al., 2004; Pelletier et al., 2014; Reczek et al., 2014; Umberson et al., 2010). Yet, an interesting reversal pattern emerged: young adults exerted greater influence on their family members’ diet and exercise than vice versa. This bottom-up influence reflects a shift from traditional parent-to-child dynamics to more reciprocal—and at times youth-initiated—forms of change (Reczek et al., 2014). Prior research demonstrates that even young children influence parents’ health behaviors through encouragement and reminders (Del Vecchio and Rhoades, 2010; Gadhoke et al., 2015; Reczek et al., 2014). Young adults may amplify this effect by introducing new dietary habits, fitness routines, and digital health trends (Kelly et al., 2020; Thomas et al., 2019).
This bottom-up influence highlights underutilized opportunities for public health practice. Interventions could mobilize young adults as initiators of health-promoting routines at home (e.g., family meal preparation, intergenerational fitness challenges). In Asian American households, culturally tailored strategies could draw on young adults’ unique roles as cultural and technological bridges, such as helping families interpret health information, navigate digital platforms, or adapt culturally familiar recipes in healthier ways. Emerging evidence supports the promise of youth-initiated strategies (SAMHSA, 2025), showing that when young adults share health knowledge, facilitate family health conversations, and promote intergenerational engagement, the benefits extend beyond the individual. Similarly, youth-led digital campaigns that showcase culturally resonant practices or success stories could strengthen family involvement across generations (e.g., Chen and Wang, 2021). By leveraging their relational credibility, young adults can serve not only as recipients of health influence but also as active change agents, particularly in collectivist contexts where they bridge tradition and innovation.
Finally, influence on risky substance use was modest across all profiles. This may partly reflect the relatively low exposure to substance use among AA young adults, with family bonds reinforcing protective cultural norms (Kim et al., 2002). Still, the direction of influence warrants further attention. Future research should investigate whether fragmented families convey risk by permitting or modeling unhealthy behaviors, thereby inadvertently promoting negative habits rather than offering protective or neutral influence. Clarifying this distinction would help determine whether low levels of perceived influence reflect a genuine absence of influence or the coexistence of protective and risk-enhancing processes that counterbalance each other.
Beyond family profile differences, certain sociodemographic factors were also associated with perceived family influence. South Asian participants, as well as married and religiously affiliated individuals, reported greater perceived family influence. These patterns align with prior evidence that cultural values and relational commitments heighten the salience of family ties in shaping health behaviors (Jahangir et al., 2025; Umberson et al., 2010). While beyond the scope of our main analyses, they suggest that cultural and relational contexts may condition how family influence is perceived and enacted, pointing to important directions for future research.
Reciprocal family influence may emerge most strongly where close family ties are culturally valued, yet its salience and meaning are deeply context-dependent. In Asian American families, collectivist orientations that emphasize interdependence, filial obligation, and hierarchical roles may amplify both the expectation and the perceived responsibility to align health behaviors with family values. For young adults, health practices may thus function not only as personal choices but also as expressions of family respect and harmony. This distinguishes the AA context from more individualistic cultural settings, where autonomy and self-direction are prioritized over family alignment. In individualistic contexts, health influence within families may be seen as supportive but optional. In AA families, by contrast, influence frequently carries moral or relational weight. Filial piety may heighten the obligation to adopt behaviors consistent with parental or elder expectations, while interdependence fosters reciprocal monitoring and caregiving across generations. At the same time, younger AA adults often act as cultural and technological brokers—translating health information, navigating Western health systems, and introducing digital health practices into the family—further shaping family influence in ways less pronounced in other cultural contexts.
There are several limitations. Recruitment via social media and Asian American community organizations may have introduced selection bias, potentially overrepresenting individuals with stronger family or community ties. As a result, findings may not fully generalize to less socially connected individuals. While this limits generalizability, focusing on families with ongoing contact remains aligned with our aims. Future work should also include individuals with weaker social connections to capture a broader spectrum of family influence. Self-reported data may also be subject to recall error, social desirability bias, and shared method variance, with perceived influence reflecting subjective interpretations rather than observed behaviors or mutual reports from multiple family members. Future research would benefit from dyadic or family-level data to capture mutual influence, compare perspectives across members, and assess how perceived influence corresponds to actual health behaviors.
The cross-sectional design precludes causal inference; it is possible that healthier behaviors strengthen family relationships rather than the reverse. Nonetheless, prior longitudinal evidence suggests that changes in relationship quality influence health behaviors (Josefsson et al., 2018), supporting the significance of these associations. While this study sought to capture culturally salient family dynamics among AA young adults, it did not directly measure constructs such as collectivism, filial obligation, or cultural value. Accordingly, the latent profiles should be interpreted as proxies for culturally shaped family dynamics rather than direct measures of cultural constructs. Future research should incorporate validated measures of cultural orientation and family cultural conflict to better contextualize these profiles and clarify whether the observed patterns reflect broader cultural dynamics or more general family processes.
Additionally, the Shared Activities with Family (SAF) Index demonstrated content validity through expert consultation and cognitive interviews; it has not yet undergone full psychometric validation, highlighting the need for further testing. Finally, the modest sample size restricted the ability to meaningfully disaggregate findings by both family relationship ties and Asian subethnic groups, constraining the reliability and validity of subgroup analyses. Larger, more diverse samples are needed to examine variability across family structures and subethnic groups and to strengthen the generalizability of the findings.
Conclusion
Distinct family relationship profiles among AA young adults meaningfully shape perceived influence on health behaviors. Our person-centered approach revealed that strongly bonded families experience reciprocal influence, while ambivalent and fragmented families exhibit weaker or absent patterns. These findings carry practical implications. For strongly bonded families, culturally relevant interventions that build on shared routines and emotional support may be especially effective. For ambivalent families, strategies that strengthen communication and create opportunities for joint activities—such as cooking or exercising together—may help translate emotional closeness into tangible health influence. For fragmented families, external supports and peer networks may serve as essential anchors.
Importantly, empowering young adults as proactive health influencers—particularly in diet and physical activity—offers a viable path for intergenerational health promotion within AA communities. In short, tailoring interventions to family relational profiles—by leveraging strong bonds, activating latent engagement, or providing external supports—holds potential for health promotion efforts in both community and clinical settings.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251399061 – Supplemental material for Family profiles and perceived family influence on healthy lifestyle behaviors: A person-centered approach in young Asian American adults
Supplemental material, sj-docx-1-hpq-10.1177_13591053251399061 for Family profiles and perceived family influence on healthy lifestyle behaviors: A person-centered approach in young Asian American adults by Soyoung Kwon, Kristine J. Hahm, Ralph J. DiClemente and Shahmir H. Ali in Journal of Health Psychology
Footnotes
Acknowledgements
The project described in this paper relies on data from survey(s) administered by the New York University South Asian Health and Research Group (SAHARA). The content of this paper is solely the responsibility of the author and does not necessarily represent the official views of NYU-SAHARA.
Ethical considerations
The NYU IRB approved the parent study protocol.
Consent to participate
All participants provided informed consent prior to participating in NYU EMBRACE (
Consent for publication
The authors affirm that all data were de-identified and participants consented to the publication of anonymized responses.
Author contributions
S.K. conceptualized the study, conducted data analysis, interpreted the findings, and drafted and finalized the manuscript.
K.J.H. contributed to the literature review, assisted with manuscript preparation, and reviewed and edited sections of the paper.
R.J.D. served as the principal investigator of the original data collection project, provided access to the dataset, and offered critical feedback on study design and interpretation.
S.H.A. assisted with variable preparation and data analysis, contributed to reviewing the manuscript, and provided feedback to strengthen the theoretical framing and discussion.
All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.