
Abstract
Women who complain of bladder pain and urinary urgency and frequency wait years to receive the label of interstitial cystitis (IC), an “orphan disease” which has no known cause or cure. The current research used phenomenological research methods to understand the experiences of women who have IC as they affect their sexualities. Ten women with IC participated in individual, semi-structured interviews. Nine themes emerged from the interviews. Findings indicated that women who have IC experienced severely limited sexual relationships, negative physician-patient interactions, the necessity for self-management of symptoms and diminished quality of life. Their accounts underscore the profound impact IC has on sexuality, revealing how sexual experiences are deeply intertwined with the emotional, physical and medical challenges of the condition. These findings contribute to a deepened understanding of the experiences of women who have IC and help to increase physicians’ understanding and awareness of the sexual effects that accompany IC.
Introduction
Sexuality is a fundamental component of human life, which can affect individuals’ emotional and physical well-being and their overall quality of life (La Rosa et al., 2020). According to a systematic review by Macleod and McCabe (2020), sexuality has been defined inconsistently in the literature. However, a commonly cited definition by the World Health Organization (WHO) considers sexuality to be “a central aspect of being human throughout life [that] encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction” (WHO, 2017, para. 5). The way people experience and express their sexuality is “different for each individual and can be influenced by biologic, psychological, social, cultural and religious factors” (Southard and Keller, 2009: 213).
Individuals who have chronic pain report adverse effects on their sexuality, including sexual dysfunction (Flegge et al., 2023). Interstitial cystitis (IC) is a chronic bladder pain condition unfamiliar to many people and is a condition that has no known cause and no known cure. Current studies suggest that 3–8 million American women have symptoms consistent with a diagnosis of IC (Berry et al., 2010; Konkle et al., 2012). Women diagnosed with IC report symptoms including pelvic pain, pain in the genitals and genital area, urinary urgency and frequency and pressure in the bladder (Hanno et al., 2015; Payne et al., 2007). Despite research and treatment advances, the specific impact of IC on the sexual experiences of women remains poorly understood.
Quantitative studies demonstrate that women who have IC experience dyspareunia (i.e. pain on vaginal penetration), altered sexual desire and orgasm frequency and insufficient lubrication (Agrawal et al., 2020; Gardella et al., 2011; Lee et al., 2015). Most studies examining the sexual functioning of women with IC have demonstrated a higher prevalence of sexual dysfunction among women with IC compared to women in the general population (Tonyali and Yilmaz, 2017). Quantitative studies of sexual functioning through self-report measures or with unvalidated measures typically focus on quantifying symptoms or general patterns, which might not capture accurately the complexities associated with IC nor how IC affects women’s subjective experiences of their sexuality. Qualitative research, in contrast, allows for a more nuanced exploration of these experiences. Speaking directly with women about their experiences can reveal the subjective aspects of living with IC, providing deeper insight into how IC affects their sexuality.
Qualitative studies of women with IC
Only four qualitative studies to date have investigated the general experiences of women with IC. Linton (2007), in an unpublished master’s thesis, explored the general lived experiences of women with IC. Five women were interviewed using an unstructured approach and were asked “What is it like to live with IC?.” Their descriptions revealed eight themes. Women described a life marked by physical torment, including unrelenting bladder and pelvic pain, unpredictable flares and the frustration of trial-and-error treatments. Women said that IC disrupted their sense of self, strained relationships and led to job loss, isolation, and emotional suffering. Despite being dismissed frequently by others, participants also found moments of empowerment, often through support groups and meaningful connections that helped them navigate the challenges of IC (Linton, 2007).
Kirkham and Swainston (2022) conducted a phenomenological research study exploring the lived experiences of women with IC/painful bladder syndrome (PBS). Twenty women with IC were asked to e-mail in a written account of their experiences of living with IC. The transcripts were analyzed using thematic analysis and revealed four themes: diagnostic uncertainty, restrictions and limitations on life, self-management and interpersonal relationships and social support. Women in their study reported difficulties obtaining an IC diagnosis, often undergoing numerous tests and referrals. After trying multiple treatments with limited success, many turned to alternative sources for information and management. Participants also reported negative effects on their sexual and social relationships (Kirkham and Swainston, 2022).
Chien et al. (2023) conducted a descriptive phenomenological study examining women’s life experiences with IC. Four major themes were identified: torment, restriction, acceptance and empowerment. Women in this study endured physical and psychological distress and loneliness and experienced obstacles and limitations in daily living because of their symptoms. Eventually, women accepted their condition, considered their symptoms as a part of everyday life and developed coping strategies for IC (Chien et al., 2023).
Gonzalez et al. (2023) conducted a digital ethnography study examining women’s experiences with IC. The following themes emerged from their qualitative analysis: online community engagement, triggers and disease etiologies, medical comorbidities, effects on quality of life, patient experience with medical care and alternative therapies and self-management strategies (Gonzalez et al., 2023). Women turned to online communities to share their experiences, validate their symptoms and exchange information on IC triggers, comorbidities and self-management strategies. They highlighted the physical, psychological and social impacts of IC and reported dissatisfaction with medical care, financial strain and a reliance on peer support and alternative therapies due to limited clinical guidance (Gonzalez et al., 2023).
Taken together, these qualitative findings illustrate the complex nature of women’s experiences and the physical and psychological effects of IC and other bladder conditions (Hatchett et al., 2009; Kinsey et al., 2016) on women’s daily lives. Although previous studies have illuminated the emotional, physical and social tolls associated with IC, they have largely overlooked one key area of women’s lives: sexuality. One qualitative study (Kirkham and Swainston, 2022) mentioned women’s painful experiences during sexual intercourse and loss of intimacy within sexual relationships. No qualitative study, to our knowledge, has set out to focus on the sexual experiences of women who have IC. This was the focus of the current study, which aimed to explore women’s experiences through detailed, open-ended inquiry.
Current study
This qualitative research study aimed to explicate the experiences of women who have IC and its effects on sexuality. To accomplish this, our research team spoke to women directly about this topic. The central question investigated in this study was: What are the experiences of women who have interstitial cystitis as they affect women’s lives in general and their sexualities in particular?
Methods
Research design
Descriptive phenomenology
We used descriptive phenomenology, informed by Husserl (1970), as our methodological framework because our aim was to understand individuals’ experiences (Polkinghorne, 1989). This approach is particularly valuable for exploring subjective phenomena, traditionally through conducting in-depth interviews. By focusing on women’s experiences with IC and its impact on their sexuality, as described in their own words, descriptive phenomenology allows for a rich, nuanced understanding that goes beyond surface-level symptom reporting. Supporters of descriptive phenomenology hold that there are common essences among all the individuals who experience a particular phenomenon, which are generally presented as themes (Lopez and Willis, 2004). The “essence” refers to the fundamental nature or core meaning of the experience, while the “structure” refers to the way in which these elements are organized or related to one another within the experience (Lopez and Willis, 2004).
Descriptive phenomenologists believe that it is essential to try to achieve “transcendental subjectivity” or remain as unbiased as possible throughout the research process (Laverty, 2003; Lopez and Willis, 2004). This process is referred to as bracketing or epoché. In bracketing, the researchers’ previous thoughts, biases, presuppositions, assumptions, judgments and beliefs about a phenomenon are set aside in the hopes of approaching the phenomenon from a fresh and naïve perspective (Husserl, 1970; Laverty, 2003). The purpose of this is to allow the essence or structure of the participants’ experience to emerge with minimal influence from the researcher (Laverty, 2003; Lopez and Willis, 2004).
To check and reduce biases in this study, the researchers collaborated to identify emerging themes as outlined by Van Kaam (1966). Biases were identified, discussed and limited during discussions at team meetings – a technique that underlies the desire for scientific rigor when doing descriptive phenomenology (Laverty, 2003). The composition of the research team deliberately included individuals with a diversity of academic, clinical and life experiences to further check one another’s possible preconceptions. Multiple research team members from the Optimal Sexual Experiences Research Team of the University of Ottawa utilized an iterative process of discussion and returning to the data; that is, researchers revisited and re-read the interview transcripts repeatedly to assess how the emerging themes aligned with participants’ interview responses. This iterative process of moving back and forth between the interviews and emerging themes helped ensure that the themes were grounded in the participants’ actual words, rather than in researchers’ preconceived notions.
Participants
In descriptive phenomenological research (Laverty, 2003; Lopez and Willis, 2004), the recruitment of a random sample of participants is neither desired nor advised. Rather, key informants who have expert knowledge regarding the phenomenon under study were invited to participate (Moustakas, 1994; Polkinghorne, 1992). To participate in this research study, participants needed to (1) be able to read, write and speak English, (2) have a diagnosis of IC or symptoms consistent with a diagnosis of IC, (3) be willing to have their interview audio-recorded for data analysis purposes and (4) have access to a telephone or a computer with an Internet connection. Ten women who had IC were recruited to participate in the study through online advertising. Participants were selected on a first-come, first-served basis. We distributed information about the study via email to online support groups and posts on social media groups (e.g. Reddit) for individuals diagnosed with IC.
Ten women from Canada and the United States who were diagnosed with IC or who had symptoms consistent with a diagnosis of IC agreed to participate. The age range of participants was 23–40 years, with an average age of 29. All 10 participants were in relationships. Five participants were married and one participant was engaged. The onset of symptoms ranged from adolescence to mid-twenties and women had symptoms for a period ranging from 1 to 10 years.
Interview prompts
Semi-structured interviews were conducted by the first author or by the first two authors. The interview protocol, developed by the first two authors, consisted of five open-ended questions with two specific prompts designed to invite women to talk about their experiences with IC and its effect on their sexuality. The questions were based on a thorough review of the literature on the phenomenon being studied. Throughout the interview process, we adhered to the principles of descriptive phenomenology, ensuring that the questions remained open-ended and focused on understanding participants’ subjective experiences. The questions were: What prompted you to seek health care treatment that led to a diagnosis of interstitial cystitis (IC)/symptoms consistent with a diagnosis of IC? How long have you been wrestling with these symptoms/feeling pain? How has this condition affected you and your life? How would you describe your current sex life? How has interstitial cystitis affected your sex life? Additional prompts were used as needed to help participants clarify or elaborate on their experiences or to reflect more deeply.
Procedure
The study was approved by the Research Ethics Board of the University of Ottawa in July, 2022. All participants provided written informed consent prior to enrollment in the study. The interviews were conducted from September to October, 2022 using a Personal Health Information Protection Act (PHIPA) compliant online platform and were audio-recorded with informed consent. Interviews ranged from 23 to 63 minutes in duration (average = 33 minutes).
Process of uncovering emerging themes
There were eight researchers involved in this study. Seven researchers from the Optimal Sexual Experiences Research Team of the University of Ottawa who had been trained previously in this descriptive phenomenological method met weekly to uncover themes. Uncovering themes in descriptive phenomenology involves focusing on what is explicitly present in the participants’ descriptions rather than reading between the lines or inferring meanings that are not directly stated by participants. This collaborative approach ensures that themes are identified through a careful, collective reflection on the interview transcripts, with each team member contributing insights to ensure the findings remain as close as possible to the participants’ descriptions.
Having multiple researchers from diverse multidisciplinary backgrounds (i.e. counseling, psychology, medicine, education), clinical and life experiences allowed us to approach the data from different perspectives and identify potential biases, particularly regarding how we understood experiences related to sexuality and chronic illness (Hill et al., 2005). Our decision to involve a larger team builds on our successful use of this approach in previously published studies (Kleinplatz et al., 2009; Ménard et al., 2015; Rice et al., 2025). By including multiple team members, we might also increase the dependability and credibility of the research findings through “analyst triangulation,” that is, using multiple researchers to independently review the interviews and compare findings.
Each interview was transcribed verbatim and all identifying information was removed. We utilized the procedure outlined by Van Kaam (1966) in which the research team members (1) read each transcript repeatedly and identified emerging themes (2) reviewed each other’s preliminary themes collaboratively, (3) discussed emerging themes until consensus was reached, (4) wrote out the description or an initial list of emerging themes (5) applied the themes to other transcripts and (6) revised again collaboratively until consensus was reached about the final list of themes that fully, accurately and faithfully captured participants’ experiences. In this process, “emerging themes” refer to preliminary or evolving patterns identified during the process, which were refined and finalized as “themes” as consensus was reached. In an attempt to establish confirmability, the eighth team member, who had not been involved thus far in weekly meetings, then conducted an external, reviewer check to help revise the themes at the final stage of the process. During the process of theme refinement, team members referred back to the themes and direct quotations from the transcripts to ensure that the themes were qualitatively different from one another. Descriptions of each theme are highlighted by direct quotations from the interview transcripts.
In order to build consensus while minimizing the influence of hierarchy or dominant voices within the group (Asch, 1951), researchers shared their initial themes during weekly meetings in sequence from the least to most experienced member in descriptive phenomenology. This approach was designed to encourage active participation from all team members, particularly those with less academic experience, to speak candidly. The sequence also aimed to reduce social pressures for unanimity, ensuring that all viewpoints were considered before reaching consensus. Team members had a total of 19 collaborative meetings (35.5 hours).
Results
Themes: women’s experiences of IC
In the interviews, participants described their experiences with IC and how IC affected their lives in general and their sexuality in particular. In this study, nine themes emerged (Figure 1). The arrows in the figure highlight the direction of the themes and the impact of one theme on another. The directional arrows underscore how sexual, psychological and relational factors interact over time. During the process of uncovering the themes, it became clear that no single theme stood out as more prominent than the others. Rather, the nine themes identified in this study represent interconnected, yet distinct, aspects of the participants’ experiences. Each theme was equally important in capturing the richness of the phenomenon. Taking all of the themes together, key informants stated that they experienced significant sexual difficulties and losses in their romantic relationships which were exacerbated by their interactions with physicians.
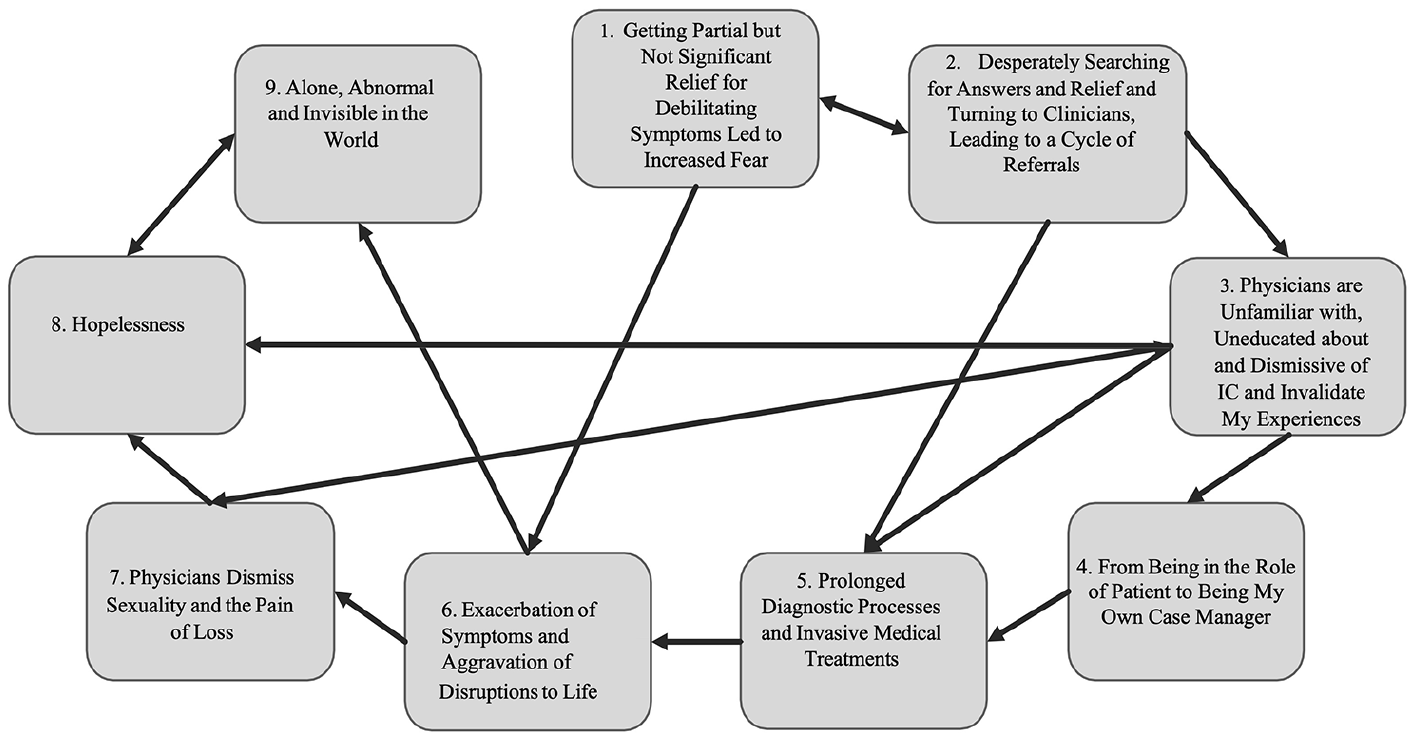
Themes of women’s experiences of IC.
Ideally, in descriptive phenomenological studies, pseudonyms are used to assist the reader in following the detailed and individual stories of each participant involved in a study. In the case of the current study, women’s voices were quite distinctive and their information quite identifying even when using pseudonyms. In consultation with the research team and the Research Ethics Board of the University of Ottawa the determination was made to err on the side of caution and to protect the identity of participants by using their words without pseudonyms. This approach aligns with recent ethical considerations in qualitative research, such as those discussed by Gore-Gorszewska (2024), who highlights the challenges of maintaining confidentiality in studies dealing with sensitive topics and strongly voiced identities. Representative quotes from each participant are distributed throughout the results section in equal proportion.
Getting partial but not significant relief for debilitating symptoms led to increased fear
Participants described debilitating symptoms, including vaginal pain and sexual difficulties that began between adolescence and their mid-twenties. All of the participants tried to get relief from their symptoms, unsuccessfully, which led them to question and fear what was happening to them. Symptoms were intermittent in nature, showed up in “flares” (i.e. symptom exacerbations) and were triggered by a variety of factors, most especially intercourse, exercise and diet. The symptoms included: vaginal tension and pain during and after sexual intercourse, masturbation and orgasm; urinary urgency and frequency; nocturia (i.e. awakening to urinate); burning, irritation and pain with urination; pelvic pain and discomfort; and abdominal pain and discomfort. Almost all of the women in this study felt pain during intercourse. One stated: “Pain during sex was definitely a thing. Um … just, um, shooting pains during sex.” One participant stated that the association of sex with pain diminished her desire for solo sex: Yeah, um… with… solo sessions I guess, um…– I mean I – it’s also just like impacted like me even feeling in the mood to be sexual at all. Um… cause at this point… I like associate sex with pain.
Because of the pain, most participants felt fearful when they engaged in sexual activity. Some women described challenges with masturbation. One said: It was fear. I got to the point where, I wouldn’t even, um, masturbate anymore because I was so scared … At the time I was like, ‘All I know is I’m just scared to do anything.’… . I was very scared of it.
One woman used the following metaphor to describe painful sensations in her pelvic floor area: I would get these – what I described as a ‘crack of lightning’ through just my . . . pelvic floor more in the front area now . . . . You’re just . . . like, ‘Oh my God, what’s happening?’
Desperately searching for answers and relief and turning to clinicians, leading to a cycle of referrals
Because participants had partial but not significant relief from their symptoms, including sexual problems, they felt desperate. In desperation, women first turned to the medical system for relief of their symptoms. They were willing to try anything to get relief. As one stated: I tried acupuncture on my bladder and, um, one of those TENS (transcutaneous electrical nerve stimulation) machines. I would sit with it on my abdomen and in hopes that that would help and, um, yeah, you get kind of desperate . . . And then I did – my acupuncturist sold me Chinese medication pills. You’ll try anything really, yeah.
To try to find relief, one woman visited the emergency department repeatedly: But then after a while the symptoms would persist and I – they would do urinalysis and nothing would come up but they would keep giving me antibiotics anyways … . And I kept going to urgent care, um, and trying to get an answer but they would just send me home with antibiotics.
Ten participants saw three clinicians on average including emergency room physicians, family physicians, urologists, gynecologists, urogynecologists (i.e. specialists in both urology and gynecology), nurse practitioners, physician assistants and physiotherapists. The majority of participants felt frustrated and disappointed that urology and gynecology specialists did not have answers or helpful insights and sometimes, gave referrals to other clinicians. This cycle of referrals meant that most participants in the study had to wait for months or years for answers and relief. Many participants reported that they saw multiple physicians over several years. One said: “So, I had probably seen in the span of five years, uh, I want to say probably seven different doctors, um, who just had no answers.”
Physicians are unfamiliar with, uneducated about and dismissive of IC and invalidate my experiences
The majority of women in the current study indicated that most of their interactions with physicians resulted in negative experiences. Specifically, participants reported that physicians were unfamiliar with and uneducated about the diagnostic processes and treatment for IC. One participant felt frustrated because physicians told her they did not know what to do: The reason why I’ve seen so many different doctors is because it feels like if you do not have the most basic of problems . . . they’re kind of done with you at that point . . . I’ve literally had doctors tell me, ‘Well I don’t know what to tell you […]’ . . . . It feels like they just give up on you.
Another woman expressed anger with the medical system’s limited scope, particularly when physicians admitted their lack of knowledge directly to her: So, it just makes me mad that these doctors really only know about the general stuff and not everything else that can happen in the body. So, I don’t really know who to blame that on but I just know that… it’s… is very stressful when you are the patient and the doctor literally tells you, “I don’t know what to tell you”
One participant indicated that her physicians dismissed the possibility of her having IC: “So, they were like, ‘Well you’re too young you can’t have IC because you’re too young. You can’t have IC because you never had kids.’” Participants wanted relief but the messages they received were: Your symptoms are not significant, your symptoms are “in your head” or are impossible, your symptoms will diminish and your functioning is unimportant. One said: “He wouldn’t say whether or not he believed it’s IC. His physician’s assistant (PA) believes I have it but he’s just convinced that a lot of this is in my head.”
From being in the role of patient to being my own case manager
Participants reported that their experiences and symptoms were being dismissed and invalidated by physicians. Therefore, women had to rely on themselves to try to manage their symptoms and to look for relief. Women were compelled to take matters into their own hands, navigating their treatment options without the support they needed from the medical system. Participants devoted time and energy to assessing their needs and to monitoring, adjusting and evaluating information about IC and its treatment. As one reported: I’ve tried so many things and whatnot. The Internet led me to things, like, um, D-Mannose, um, supplements. Um, led me to Prelief, which is also a supplement of sorts. Um, I took a lot of baths . . . . Um, as far as sex – lube and things like that – I learned things to avoid.
Most said they conducted online searches about treatments and made changes to their lifestyles. One woman stated: I just started researching, uh, treatment options . . . . So, I was able to see a pelvic floor specialist … I changed my diet. Um, uh, stopped drinking coffee and tea . . . I drank nothing but water.
Many participants recounted an all-consuming process of trying multiple treatments to get relief. One indicated: Um, the aloe vera I’ve done off and on …. I guess another thing I’ve tried is diet …. Um, hydroxyzine I think … Physical therapy … but that’s not been consistent …. and then the Zyrtec and the Hiprex I’ve been on since [2020s] so about three-ish months there too.
Prolonged diagnostic processes and invasive medical treatments
Most participants reported that they did not find lasting relief from their symptoms after taking matters into their own hands. Women said that they continued to seek help from the medical system. The majority of participants reported significant delays in and obstacles to obtaining a diagnosis of IC. Nine of the 10 participants received a formal diagnosis of IC from physicians. The average time from onset of initial symptoms to receiving a diagnosis was 3 years. One participant reported: They didn’t really give me an official diagnosis . . . . But then it took I think, at least six months if not longer than that to actually speak with a urologist. So, um, yeah, it was probably I’d say at least six to eight months before I got the diagnosis.
Participants reported that physicians recommended invasive treatments. Most women stated that their physicians’ recommendations included antibiotics, tricyclics for modulating pain, antihistamines (i.e. allergy pills), antispasmodics (i.e. medications that are used to suppress muscle spasms), anticonvulsants, Botox, vitamin supplements, bladder instillations, physiotherapy and suggested that women make changes to their diets and lifestyles. One woman recounted her experience with bladder instillation treatment: So, they would basically put a catheter into my urethra, um, and then fill up my bladder with this solution. I believe it was some sort of baking soda solution, um, and there were other medications, I think . . . . Um, ultimately, I think just the insertion of the catheter was too painful for me to continue with that treatment.
Women reported that physicians offered treatments simultaneously or one after another with minimal or no relief. As one woman stated: It started with the bacterial vaginosis (BV) medicine and then . . . the anti-fungals . . . But then when the BV treatment wouldn’t work, they gave me antibiotic gel to insert in there and then for the urea plasma I was given doxycycline . . . . But for the IC they . . . he gave me, um, . . . . a lot of medicines throughout my life, no matter what it is . . . don’t really work on me.
Exacerbation of symptoms and aggravation of disruptions to life
Participants reported that invasive medical treatments, delays in diagnosis and the majority of treatments led to increased pain and aggravated their symptoms. This, in turn, had adverse effects on participants’ sexual functioning. Participants reported aggravated disruptions and changes to their partnered and solo sex lives, romantic relationships, daily functioning and to their physical and mental states. Women used phrases such as “non-existent sex life,”“broad effects,”“long journey,”“change,”“cannot do it anymore,”“scared,”“suicidal thoughts,”“horrendous,” and “deter my life” to describe their physical or mental states. The majority of women in this study reported increased pain during and after intercourse and masturbation, the loss of sexual intimacy in their relationships and feeling isolated in their sexual relationships. One woman stated that her symptoms “robbed” her of the ability to enjoy her sex life with her current partner: I’m upset that I can’t enjoy my full sex life from what I used to be able to do with previous partners . . . . I feel robbed of the fact that I can’t fully enjoy it with my [current partner] . . . . and it makes me pretty upset because this is the person that I want to be able to give myself to and yet I can’t . . . . I just want to emphasize that I guess the combination of the physical pain and the mental inability to have sex has drastically decreased my libido.
The majority of participants said that pain during and after intercourse led to adverse effects on their daily functioning. As one stated: Um, it’s affected pretty much everything. Um, the first thing it started affecting was my sex life because it’s – [sighs] first is just the burning. But then there’s the after sex where you can’t sleep because all you feel is pressure on your bladder and you’re just laying awake all night and you gotta put a heating pad on and sometimes even take pain medicine … I can’t really … do it at the moment and if I do choose to do it I’m basically choosing – I know I’m gonna be in pain after. So, it’s – you want to do it but you know it’s gonna be painful.
One woman emphasized the unpredictable and risky nature of engaging in sexual activity: Um, so it’s just – I don’t really know how I am going to resume intercourse at this point. Either way it’s – I am playing Russian roulette and I’m going to have some kind of pain after this. So, is it worth it? There’s always that question.
Another participant described the need to adapt during partnered and solo sexual activity because of the sudden and unpredictable onset of pain: Uh… yes. Cause I think it’s more like – like I can even be doing like one thing and it’s fine and then all of a sudden it starts feeling painful and so I just kind of have to like readjust in that moment.
Physicians dismiss sexuality and the pain of loss
As their sexual difficulties worsened, women reflected more deeply on the suffering and losses in their romantic relationships and their interactions with physicians while seeking help. Participants did not believe that physicians understood – or cared about—the effects that IC had on women’s sex lives and sexual functioning. As a result, women emphasized the need for physicians to prioritize the management of the sexual difficulties that accompany IC. Most participants stated that their physicians dismissed their sexual symptoms. One woman said: I would say one of the frustrations of it is going to a provider like a urogynecologist or a urologist you’re told all the time that . . . these are the professionals you can talk to about these kind of issues that you’re having and I feel like I’ve just been totally dismissed and like they don’t want to talk to me about these things.
This sentiment was echoed in participants’ broader reflections on the effects of IC on sexuality being ignored routinely in clinical care. One participant noted: “So, I don’t know… maybe it’s just like in general I felt like that aspect of having this has been neglected by providers like in terms of advice… in terms of like being proactive and wanting to try things.” Several participants highlighted that sexuality was rarely a focus of treatment, despite its importance in their lives. One woman recounted feeling dismissed by her urologist: Not really… and there hasn’t really been a lot of like – like… like that’s never something that’s a focus of treatment, I find. Like, if I bring it up with my urologist he’s kind of like, “Oh, well, like sex is sex” like – but it’s never – yeah, it’s not something that he seems particularly concerned about treating . . . .
Another participant said that her provider not only failed to address the sexual impact of her condition but also contributed to her feelings of isolation: My provider has even told me he’s at the end of his rope with me . . . . So, feeling like I’m on my own in all of this and also feeling like a really bad partner because I haven’t been able to have intercourse for over a year because my flares have been so bad . . . . I wish providers would pay attention to that aspect of it a little bit more, because it is important and it’s something that’s not easy to talk about or bring up with a provider.
Hopelessness
As a result of the invasive diagnostic procedures and medical intervention, delays in diagnosis, exacerbation of symptoms, aggravated effects on their lives and lack of consistent and significant relief, women felt hopeless about their sex lives and their situations. One participant bemoaned that her lack of relief from pain led to hopelessness. She relayed that she had been close to thoughts of suicide: Uh – [sighs] I mean you can’t – you’re in pain all the time. So, you can’t really do anything . . . it’s frustrating because there’s no relief really . . . . I don’t want to say that I had suicidal thoughts but it wasn’t – it was probably close, to be honest.
Another woman said that getting better did not feel possible and expressed concern that her romantic partner would leave her: I want to get better. I feel, like, even though my [partner] has never made me feel this way I feel like I’m on a clock of trying to get this figured out before being left . . . I don’t know how long it’s acceptable for this sort of thing to be happening . . . . But I don’t think I’m going to get it figured out.
Most participants felt hopeless because they could not find relief and because of their interactions with physicians. One reported: It can just get really – feel just really hopeless I guess cause it feels like nothing’s working still at this point and . . . they’ll act like nothing’s even wrong with me and so I just have to deal with it . . . and not a lot of people know about it and so you don’t really know what to do . . . It’s just been very stressful overall.
Alone, abnormal and invisible in the world
As a result of the delays in diagnosis, exacerbation of symptoms, aggravated effects on their lives, a lack of consistent and significant relief, and hopelessness, women felt alone in the world, that they were abnormal and that their experiences of suffering in their sexual lives were invisible. One participant recounted the loneliness she felt after she asked a physician for support in improving her sex life: Um, but I was just tearing up and saying, ‘I just want to be able to have sex with my [partner]’ and . . . the provider just looked uncomfortable and looked away and was just, like, ‘Yeah, I know’ and then that was it [chuckles]. There was no advice . . . or support or anything there and that’s one of the loneliest parts of all of it.
Another woman described the adverse impact of IC on her sex life and that it made her feel abnormal in comparison to peers: It makes me feel abnormal and also just jealous every single day of normal people with normal bodies. I see people on social media and they’re out with their boyfriends and I just know, like, ‘Oh, I bet you have sex every single night and your life is perfect’ . . . . So, it makes me very insecure, very jealous, very mad.
Many women spoke of “invisible illness,” to describe their experience with IC. One said: “With it being kind of an invisible illness, you’re sometimes not sure whether people actually take you seriously or whether people will believe you.”
Discussion
This is the first published qualitative study that has focused on the sexual experiences of women who have IC, as described in their own words. The findings highlight the devastating effects this condition has on women’s sexual lives. In their interview responses, women emphasized that their healthcare journeys, emotional struggles and day-to-day challenges were intertwined with their sexual experiences. Many of the participants expressed themselves with vivid, poignant imagery; ordinary language alone could not capture their suffering.
For many participants, their symptoms of vaginismus (i.e. the tension or spasm of muscles at the vaginal opening which can lead to painful penetration)—a condition distinct from interstitial cystitis—and pain during and after masturbation and intercourse, introduced a cascade of emotional and relational challenges. Participants noted that as these symptoms continued, they reduced the frequency of their sexual activity significantly in both partnered and solo sex. These findings are consistent with previous quantitative research (Agrawal et al., 2020; Gardella et al., 2011; Lee et al., 2015). However, we present novel findings around the impact of IC on the frequency of solo sex, in particular, challenges related to masturbation. Most quantitative studies have focused on the impact of IC on partnered sexual activity (Agrawal et al., 2020; Gardella et al., 2011; Lee et al., 2015). Currently, no studies have explored how this condition affects masturbation. This reduction in solo sexual activity can be particularly worrisome, as it may signal a deeper level of sexual distress and disengagement from one’s sexual self.
The majority of women in this study described a sense of fear, particularly surrounding sexual activity and the repercussions of sexual intimacy, which led to a sense of loss and hopelessness about their relationships and sexual futures. These findings align with the broader literature on other chronic pain conditions, where pain-related fear and anticipatory anxiety contribute to emotional distress (Boersma and Linton, 2006). None of the women in this study were referred to psychological support services to help them manage the losses within their sexual relationships. By sharing women’s experiences of this very real and debilitating condition, our hope is that psychologists, sexologists and therapists will understand the gravity of women’s sexual difficulties so that they might create empathic and compassionate spaces for these individuals. Therapists who are aware of IC and who have experience in helping women and couples with sexual dysfunction, pain, loss and trauma may be invaluable for people who have IC.
Sexuality is seen as a critical aspect of overall health (Quinn et al., 2011; Urry et al., 2019) however, the majority of women in the current study described that this importance was not reflected in their interactions with physicians and the medical system. When participants disclosed their sexual difficulties to physicians, women were told, “it’s not that big of a deal,”“this isn’t happening to you,”“we can’t do anything about it,”“what you’re experiencing is not possible” or “so what?.” Evidence from the literature demonstrates that physicians dismiss the experiences of their patients who have IC (Brown et al., 2024; Kanter et al., 2017; Kirkham and Swainston, 2022; Windgassen et al., 2022). In the current study, the majority of women reported that their physicians dismissed their sexual experiences and disregarded their sexual difficulties, which resulted in feelings of despair, hopelessness and isolation. Although gender dynamics were not a focus of this research, our findings align with literature on the marginalization of women’s sexuality in healthcare contexts (Kleinplatz et al., 2020). The majority of individuals diagnosed with IC are women, yet their sexual experiences are often overlooked—reflecting a broader, systemic pattern of silencing of women’s experiences in medicine and the persistent disparity in attention given to women’s healthcare compared to men’s (Betai et al., 2024; Khan et al., 2024). These findings point to the urgent need for a more comprehensive approach to sexual difficulties—one that centers and prioritizes women’s voices, acknowledging the mental, emotional and physical dimensions of sexuality in IC assessment and treatment.
Ultimately, women in the current study felt trapped in a cycle of sexual difficulties, painful symptoms, a lack of relief and despair. Participants’ sexual relationships with their partners were strained, and they despaired at messages from their physicians that their sexuality and sexual functioning were unimportant. Women were left grappling with not only the physical toll of their condition but also the emotional devastation of feeling unseen, unheard, and disconnected from their sexual selves. It is crucial that physicians and the wider healthcare community listen to the experiences of women who have IC in relation to their sexuality. This could not only help patients, but enable clinicians to gain a deeper understanding of the psychological and physical effects that IC has on women’s sex lives. It could also aid physicians in developing specific assessments and interventions for this population.
Strengths, limitations, and future research
The process of identifying emerging themes by eight researchers was iterative, rigorous and in line with descriptive phenomenological research. All eight experts had conducted sex research using a phenomenological lens previously. The distinct approach to phenomenology that was utilized in this study involved: an iterative and collaborative process of discussion; a continuous return to the data; and researchers checking each other’s possible biases on the participants’ experiences to establish dependability, confirmability and credibility of these findings (Lincoln and Guba, 1985).
Purposive sampling was utilized to recruit key informants who have expert knowledge regarding the phenomenon being studied and who could describe their experiences in depth. As it happened, the study sample skewed young in terms of age. All but one participant (n=10) were aged 23-39. As a result, the experiences of IC among older women or women who have experienced IC for longer periods may not be captured accurately in this study.
Future research should continue to investigate the experiences of women with this condition. Researchers should also examine the interactions between physicians and patients who have IC and the barriers faced when dealing with IC. In addition, future research should investigate the effectiveness of current IC treatments, how current treatments affect patients’ sexual response and psychological treatments to target the physical, psychological and sexual difficulties that accompany IC.
Conclusion
Findings from this study help to break the silence and stigma that surrounds IC and sexual difficulties and help to increase physicians’ understanding and awareness of the negative effects that accompany IC. This research focuses on the sexual, psychological and physical needs of women with IC, which are at best, underserved in current treatment approaches. By continuing to share the stories of individuals with IC, our hope is that the suffering and sexual effects that accompany this condition will be recognized, understood and treated better by mental health professionals, physicians and medical researchers.
Footnotes
Acknowledgements
The authors would like to thank the participants in this study. It was an honor to listen to your experiences.
Data sharing statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
Declaration of conflicting interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (Grant #N/A).
Ethics approval
Our study was approved by the Research Ethics Board of the University of Ottawa (approval no. S-06-22-7841).
Informed consent
All participants provided written informed consent for participation and anonymised publication.