
Abstract
Couples navigating medically assisted reproduction (MAR) may respond to relationship stressors by catastrophizing. Catastrophizers may be more likely to seek support indirectly; partners may miss these cues such that their responses are seen as unsupportive, which may impact sexual desire and distress. We investigated whether relationship catastrophizing predicted lower sexual desire and greater sexual distress, via lower perceived partner support, across 1 year. Couples (N = 314) seeking/undergoing MAR completed surveys at baseline, 6, and 12 months. Catastrophizing predicted decreases in both partners’ perceived support, and lower perceived support predicted decreases in one’s own downstream sexual distress, but there were no effects for sexual desire. Although we found no evidence of longitudinal mediation, at baseline, greater catastrophizing was associated with lower perceived support, which was in turn linked to lower desire and greater distress. Interventions targeting relationship catastrophizing and improving partner support may help couples navigate the challenges of MAR.
Keywords
Medically assisted reproduction (MAR; medical interventions to facilitate pregnancy; Péloquin et al., 2024), is a necessary step toward starting a family for up to 16% of couples (Bushnik et al., 2013), yet it places physical and psychological stress on both partners that can disrupt their sexual relationship. MAR may interfere with sexual desire (i.e. interest in sexual activity; Spector et al., 1996) and heighten sexual distress (i.e. concerns about one’s sex life; Derogatis et al., 2008), with implications for health and quality of life (Péloquin et al., 2024).
Intimate relationships are a key source of support when faced with life stressors, such as MAR (Pietromonaco et al., 2022). Indeed, individuals who perceived more support from their partners during MAR reported improved infertility-related quality of life (Joseph et al., 2025). However, the degree of support perceived from their partners may be impeded by certain patterns of coping. One such pattern involves catastrophizing about their relationship (Wang et al., 2024). In general, while relationship catastrophizing may reflect individuals’ attempts to elicit partner support, it can also heighten attentional focus on relational stressors such as sexual difficulties (Petrini and Arendt-Nielsen, 2020), and can thus be linked to lower sexual desire and greater sexual distress for both partners (Wang et al., 2024). Research has yet to explore factors such as relationship catastrophizing that might hinder couples’ perceived support during MAR, and in turn, their sexual relationship over time. Exploring relationship catastrophizing and perceived support can further our understanding of why couples vary in the extent to which their sexual relationship is affected while seeking or undergoing MAR.
How medically assisted reproduction can disrupt sexual relationships
A growing body of evidence illustrates how couples’ sexual experiences are negatively colored by MAR; up to 90% of cisgender women and 58% of men seeking MAR report problems with sexual function (Starc et al., 2019). Some sexual changes may be directly linked to MAR procedures, such as decreased desire as a side effect from hormonal medications (Marci et al., 2012), or lower sexual frequency from engaging in MAR-related treatments (e.g. fatigue from frequent medical visits; Repokari et al., 2007). Further, financial stress (Allsop et al., 2023), hopelessness about the success of MAR (i.e. approximately 50%; McLernon et al., 2016) may interfere with sexual desire and satisfaction and heighten sexual distress. MAR may also shape how couples view or experience sex: some couples might be directed to have sex at specific times to increase their chance of pregnancy, even in the absence of sexual interest (Luk and Loke, 2019), and as such, report that sex becomes “mechanical” over time (Repokari et al., 2007). Indeed, men and women seeking MAR for infertility report lower sexual satisfaction and function compared to fertile controls (Ozkan et al., 2015; Ozturk et al., 2019), which may further curb desire or amplify sexual concerns. While research involving same gender/sex couples is limited, requiring MAR encapsulates unique stressors (e.g. a lack of tailored services; Benoit et al., 2024) that may hinder sexual intimacy (Goldberg et al., 2010) for these couples. Studies that have examined sexual outcomes in the context of MAR have primarily focused on global sexual function, and despite the potential for couples’ feelings and cognitions about sexuality—including desire and distress—to shape overall health, these experiences have largely been neglected in prior research.
Relationship catastrophizing and sexual desire and distress
A key determinant of couples’ adjustment to MAR may be how they respond when faced with relationship challenges, which could be critical for sexual well-being above and beyond the stressors themselves. Relationship catastrophizing, a construct adapted from pain catastrophizing (Sullivan et al., 2001), represents one way in which couples seeking or undergoing MAR may respond to new or ongoing relationship stressors that may instigate detrimental outcomes. Relationship catastrophizing involves magnifying negative feelings and cognitions about the relationship (e.g. Sex will become even less pleasurable over time), ruminating about challenges or problems in the relationship (e.g. I can’t stop thinking about how “mechanical” our sex life has become), and adopting a helpless orientation toward these challenges (e.g. There’s nothing I can do to improve our sexual relationship). Given that MAR typically engenders increased stress and disrupted relational functioning (Luk and Loke, 2019), relationship catastrophizing may be a salient risk factor for couple’s sexual adjustment when seeking or undergoing MAR.
Theoretical models of pain catastrophizing conceptualize it as a maladaptive cognitive emotion regulation strategy that heightens one’s own negative emotions (Sullivan et al., 2001), such that individuals who catastrophize in response to relationship stressors during MAR could also be more likely to fixate on negative aspects of their relationship (Petrini and Arendt-Nielsen, 2020). In turn, doing so can ultimately reinforce catastrophic cognitions that result in their own and their partners’ disrupted sexual desire and amplified sexual distress. In the only study examining links between relationship catastrophizing and sexual outcomes, relationship catastrophizing predicted lower sexual desire and greater sexual distress during the transition to parenthood (i.e. another time fraught with novel challenges; Wang et al., 2024). The authors suggested that heightened relationship catastrophizing could elicit one’s own worry, stress, or anxiety, which may interfere with their ability to provide support. Accordingly, the interpersonal emotion regulation model of sexual dysfunction (Rosen and Bergeron, 2019) has implicated relationship catastrophizing as a maladaptive emotion regulation strategy that can hinder sexual well-being for both couple members—particularly when navigating disruptions to relationship or sexual well-being.
Perceived partner support
Given the interpersonal context inherent in the association between relationship catastrophizing and sexual outcomes, one important mechanism may be perceived partner support. Romantic partners are often the primary source of support for one another during MAR (Walen and Lachman, 2000), and Barry et al. (2009) identified four types of perceived support among romantic couples: esteem/emotional (i.e. validation, affection), informational (i.e. information, advice), physical comfort (i.e. support via physical acts), and tangible (i.e. actual or offered assistance). Although these forms of support are conceptually distinct (Barry et al., 2009), all types of perceived support may facilitate couples’ adjustment when faced with MAR-related challenges (Joseph et al., 2025). Reassurance and physical comfort may enhance intimacy, while offering advice or tangible support can help couples overcome stress as a team (Joseph et al., 2025). In turn, experiencing less subjective stress could alleviate worries or concerns about sex while enhancing partner-focused desire. Research has indeed identified partner support as a predictor of higher sexual desire (van Lankveld et al., 2021) and lower sexual distress (Rosen et al., 2020).
Individual and relational processes (e.g. relationship catastrophizing) may interfere with romantic partners’ ability to support one another in MAR, and in turn their sexual well-being (Wang et al., 2024). For couples seeking MAR, responding to stressors via catastrophizing may intensify unpleasant emotional experiences (Petrini and Arendt-Nielsen, 2020), which could hinder one’s ability to notice support provided by their partner. Indeed, individuals who engage in frequent catastrophizing may be more prone to seeking support indirectly (e.g. reassurance-seeking; Petrini and Arendt-Nielsen, 2020), increasing the likelihood that their partners will feel frustrated by or miss these cues entirely, and thus, that their responses are perceived as unsupportive. Individuals who catastrophize may also be less likely to interpret stressors—or their relational context—accurately, and may be less attuned to their partners’ feelings, which could result in their partners perceiving less support. Consequently, couples could report more difficulty withstanding stressors and establishing an interpersonal context that diminishes sexual distress and promotes desire (Rosen and Bergeron, 2019). Existing research points to less perceived support as a potential mechanism through which relationship catastrophizing may engender poorer sexual outcomes; yet these links have not been directly tested, including in the context of MAR. Investigating perceived support could elucidate one pathway by which catastrophic thoughts about relationship challenges might worsen couples’ sexual lives as they navigate MAR, and may implicate promising intervention targets.
Current study
In a dyadic longitudinal study of couples seeking or undergoing MAR, we investigated the mediating role of perceived partner support in the associations between relationship catastrophizing and sexual desire and sexual distress across a 12-month period. Given that many contextual factors interact with individual and interpersonal characteristics over a 12-month period, we also tested cross-sectional indirect links between the study variables at baseline. Informed by the actor-partner interdependence model (Cook and Kenny, 2005), we examined both actor (e.g. how relationship catastrophizing relates to one’s own outcomes) and partner (e.g. how catastrophizing relates to a partner’s outcomes) effects. To determine whether perceived partner support mediated the links between relationship catastrophizing and sexual desire or distress, we examined direct longitudinal associations between our variables of interest at the within-person level. Within-person longitudinal associations capture crucial fluctuations in our study variables across time, which is relevant because MAR is often experienced as a “roller-coaster” of emotions (Péloquin et al., 2024). We tested whether deviations from an individuals’ own average relationship catastrophizing at a given timepoint predicted deviations from their own, or their partner’s, average perceived partner support 6 months later. We also examined effects of relationship catastrophizing and perceived partner support on the sexual desire and sexual distress of both partners. Finally, we tested whether deviations from one’s own average relationship catastrophizing at baseline predicted their own or their partner’s sexual desire or sexual distress at the 12-month timepoint via perceived partner support at the 6-month timepoint.
We hypothesized that individuals who reported more catastrophizing about their relationship, relative to their average, at a given timepoint would report decreased support from their partner at a later timepoint (path a). Given that seeking MAR holds implications for both partners (Péloquin et al., 2024), we expected that partners would also report decreases in perceived support. We also expected that higher-than-average relationship catastrophizing would predict decreases in sexual desire and increases in sexual distress for both partners at the following timepoint (path c′). Next, we predicted that individuals who endorsed lower-than-average levels of perceived support at one timepoint would report decreases in sexual desire and increases in sexual distress at the next timepoint (path b), as would their partners. In sum, we expected that, the link between higher relationship catastrophizing at baseline and decreases in sexual desire or increases in sexual distress at 12-months would be mediated by decreases in perceived partner support at 6-months (path c). We expected the same pattern of effects when examining cross-sectional indirect paths at baseline. To gain understanding of the directionality of links between our variables of interest, we tested both directions of expected associations (e.g. whether changes in perceived support predicted changes in relationship catastrophizing).
Method
Participants
As part of a larger study examining treatment burden and well-being, couples requiring MAR completed three longitudinal surveys (i.e. baseline, 6 and 12 months). There have been five published manuscripts utilizing data from the larger study (i.e. Allsop et al., 2023; Benoit et al., 2024; El Amiri et al., 2021, 2023; Rossi et al., 2023); no studies have examined relationship catastrophizing nor perceived support.
Eligible couples were required to be seeking MAR and to have had their first visit to a MAR clinic within the past 6 months. 1 We aimed to recruit couples who were starting the treatment process (or restarting after a significant break, i.e. >12 months) to allow us to follow couples over the course of MAR. Both members of eligible couples were required to be (1) at least 18 years old, (2) fluent in English or French, (3) living in Canada or the United States. Exclusion criteria included self-reported unmanaged major medical or psychiatric illness that was significantly impacting daily functioning. Because sex- and gender-diverse couples report unique MAR-related challenges (Benoit et al., 2024), some recruitment specifically targeted the 2SLGBTQ+ community to enhance sample diversity. The final sample consisted of 314 couples who were seeking or undergoing MAR. See Supplemental Table S1 on the OSF for participant demographics.
Procedure
This study received approval from the Research Ethics Boards at Dalhousie University and l’Université de Montréal. Couples seeking MAR were recruited via an assisted reproductive therapies (ART) clinic in Halifax, Nova Scotia, Canada, online via social media, or via print advertisement from November 2019 to 2021. For in-person recruitment, researchers identified potentially eligible participants via review of medical records, who were then informed about the study by clinic staff upon check-in. 2 Couples underwent a brief screening procedure in-person or by phone to confirm eligibility before completing validated questionnaires online at baseline and 6, 12, 18, and 24 months later. The 6-month interval was implemented to capture the length of MAR treatment phases and reduce participant burden. Because missing data tends to increase over time in longitudinal studies (Asendorpf et al., 2014), and given the complexity of our analyses, this study utilized data from the baseline, 6-month, and 12-month surveys only. Of the 314 couples who completed the baseline survey, the completion rate was 88.4% at 6-months and 81.5% at 12-months. Couples were compensated up to $144 CAD for participation in the study.
Measures
Sociodemographics
At baseline, participants reported their age, sex, gender, sexual orientation, relationship status and duration, shared annual income, and ethnicity. At each timepoint, participants also reported on infertility diagnosis, treatment status, and reason for seeking MAR.
Relationship catastrophizing
Relationship catastrophizing was measured using the 13-item Relationship Catastrophizing Scale (RCS), which assesses three facets of catastrophizing about relationship challenges (i.e. magnification, rumination, and helplessness). The RCS was previously adapted from the Pain Catastrophizing Scale (PCS; Sullivan et al., 1995) and scores were validated across three studies (see Wang et al., 2024). Because a 3-factor model and a 1-factor model of the RCS both demonstrated good fit in past research and we did not have hypotheses that differentiated between the three facets of catastrophizing, we computed a total score of relationship catastrophizing. At each timepoint, participants rated the degree to which they experienced certain thoughts when experiencing relationship challenges over the past month on a five-point Likert scale from 0 (not at all) to 4 (all the time), with total scores that could range from 0 to 52 and higher scores indicating greater catastrophizing. The RCS demonstrated strong internal consistency across study timepoints (α = 0.93 at baseline, 0.94 at 6-months, 0.95 at 12-months).
Perceived partner support
Using the 25-item Support in Intimate Relationships Rating Scale (SIRRS; Barry et al., 2009), participants reported the degree to which they felt their partner provided them with four types of support over the past 4 weeks on a scale from 0 (never) to 4 (almost always). Research has often utilized a total score indicating the overall extent to which individuals felt they received support from their partner (e.g. Brock et al., 2023; Dewar et al., 2023). Thus, because we were interested in overall perceptions of received support, did not have unique theoretically-based hypotheses for each type of support, and given the complexity of statistical models, items were summed for a total score that could range from 0 to 100, with higher scores indicating greater perceptions of partner support. The SIRRS has shown strong psychometric properties (Barry et al., 2009) and had excellent internal consistency in the current sample (α = 0.94 at baseline, 0.95 at 6-months, and 0.95 at 12-months).
Sexual desire
Participants reported their sexual desire over the past month utilizing two equivalent sexual desire items (i.e. Over the past 4 weeks, how often have you felt sexual desire? and Over the past 4 weeks, how would you rate your level of sexual desire?) from the International Index of Erectile Function (IIEF; Rosen et al., 1997) and the Female Sexual Functioning Index (FSFI; Rosen et al., 2000), similar to previous studies (e.g. Allsop et al., 2023; Rossi et al., 2023). Items were rated on a five-point Likert scale and summed, and total scores could range from 2 to 10, with higher scores representing higher desire. The IIEF and FSFI have shown strong psychometric properties among couples seeking MAR (El Amiri et al., 2021). In the current study, the two items from the IIEF (α = 0.83 at baseline, 0.85 at 6-months, and 0.84 at 12-months) and the FSFI (α = 0.89 at baseline, 0.91 at 6-months, and 0.86 at 12-months) displayed good internal consistency.
Sexual Distress
Sexual distress over the past 4 weeks was measured using the five-item Sexual Distress Scale-Short Form (SDS-SF; Santos-Iglesias et al., 2018). Items are measured on a five-point Likert scale from 0 (never) to 4 (always) and summed for a total score ranging from 0 to 20, with higher scores representing greater sexual distress. The SDS-SF has shown strong reliability and validity in past research (Santos-Iglesias et al., 2018). Reliability in the current study was excellent (α = 0.91 at baseline, 0.93 at 6-months, and 0.92 at 12-months).
Data Analysis
Descriptive statistics were analyzed using SPSS Version 28; all other analyses were computed using MPlus (Version 8.8; Muthén and Muthén, 1998–2017). To promote transparency and replicability of analyses, de-identified data and syntax are available on the OSF repository site: https://osf.io/3wbzr/?view_only=b4907fdb437246049d4e89019902fec5. Analyses, informed by the actor-partner interdependence model (Cook and Kenny, 2005), examined actor and partner effects while accounting for couple interdependence. Our sample was comprised of same-gender/sex and mixed-gender/sex couples at varying stages of MAR; in some cases, both members of the couple were involved in medical procedures either at the same or different timepoints. Thus, there were no variables that consistently distinguished members of a couple across all dyads and timepoints, so dyads were treated as indistinguishable (Kashy et al., 2008). Random role assignment was used within dyads to designate one partner as “Partner 1” and the other as “Partner 2” (Ledermann and Kenny, 2017). Model paths, variances, and intercepts were also constrained to be equal between members of a couple (Kashy et al., 2008). Couples whose relationship ended during the study were excluded. To handle item-level missing data, if a participant missed less than 50% of the items in a scale, a total score was computed using the means of the completed items. Missing data were handled using full information maximum likelihood if one or both members of a couple did not complete a follow-up survey.
Random-intercept cross-lagged panel models
Associations at the within-person level (i.e. co-occurring changes across time) and the between-person level (i.e. averaged across timepoints) were simultaneously assessed using dyadic random intercept cross-lagged panel models (RI-CLPM) within a structural equation modeling (SEM) framework, in line with recommendations by Mulder and Hamaker (2021). The RI-CLPM is an extension of traditional cross-lagged panel models (CLPM) via disaggregation of within- and between-person variances, thereby providing information about the temporal relationships among study variables. To increase statistical power, two separate models (i.e. one for sexual desire and one for sexual distress) were constructed to examine associations between relationship catastrophizing, perceived partner support, and sexual well-being, including variables for both partners simultaneously. Each model allowed us to investigate whether deviations from one’s own average relationship catastrophizing at a given timepoint predicted increases or decreases in perceived partner support (path a) or sexual desire/sexual distress (path c’) for either member of the couple at a later timepoint, whether deviations from one’s own average perceived support predicted changes in either partner’s sexual well-being at the next timepoint (path b), and whether deviations from one’s own average relationship catastrophizing predicted deviations in sexual outcomes via changes in perceived partner support (path c). Informed by the APIM, we tested four distinct indirect paths examining associations between: (1) relationship catastrophizing and one’s own sexual outcomes via one’s own perceived partner support; (2) relationship catastrophizing and one’s own outcomes via one’s partner’s perceived support; (3) relationship catastrophizing and one’s partners’ outcomes via one’s own perceived support; and (4) relationship catastrophizing and one’s partner’s outcomes via one’s partner’s perceived support.
Within-person effects in each RI-CLPM include cross-lagged paths (i.e. the extent to which increases or decreases in a given score is explained by deviations from their own or their partner’s average score of another construct from the previous timepoint), autoregressive paths (i.e. the extent to which deviations in a given score can be explained by deviations in one’s own score or their partner’s score on the same construct at the previous timepoint), as well as concurrent associations (i.e. associations among partners’ scores on study variables within the same timepoint). In computing cross-lagged and autoregressive paths, we controlled for all deviations from average scores at previous timepoints. Only results for cross-lagged paths were central to our hypotheses and are reported in text. While we were primarily interested in examining within-person associations, each model also evaluated between-person associations (e.g. scores averaged across timepoints).
Evaluating cross-sectional indirect associations
As with our longitudinal models, the cross-sectional models were in line with the APIM and followed a SEM framework. Using the baseline survey data, we constructed two models (i.e. for sexual desire and distress) that evaluated indirect links between relationship catastrophizing and sexual outcomes via perceived support. We examined whether individuals’ relationship catastrophizing was associated with their own or their partners’ perceived support (path a) or sexual desire or distress (path c′), and in turn, whether perceived support was associated with sexual desire or distress (path b).
All longitudinal and cross-sectional models met appropriate fit criterion, as demonstrated by CFI > 0.90, SRMR < 0.10, and RMSEA < 0.08 (see Supplemental Table S2 on OSF; Hair et al., 2010).
Results
Means and standard deviations for all predictor and outcome variables are reported in Supplemental Table S3 on OSF. Within- and between-person correlations between study variables across all timepoints are displayed in Supplemental Tables S4 to S7. Results of the longitudinal mediation analysis are presented in Table 1, and cross-sectional indirect results are presented in Table 2. Results for all other hypothesized effects are reported in Tables 3 and 4 (within-person longitudinal effects), and Table 5 (between-person cross-sectional associations). For completeness, autoregressive effects are displayed in Supplemental Table S8 and between-person longitudinal associations are reported in Supplemental Table S9.
Longitudinal indirect associations between relationship catastrophizing at baseline, perceived partner support at 6-months, and sexual desire or sexual distress at 12-months (n = 314 couples).
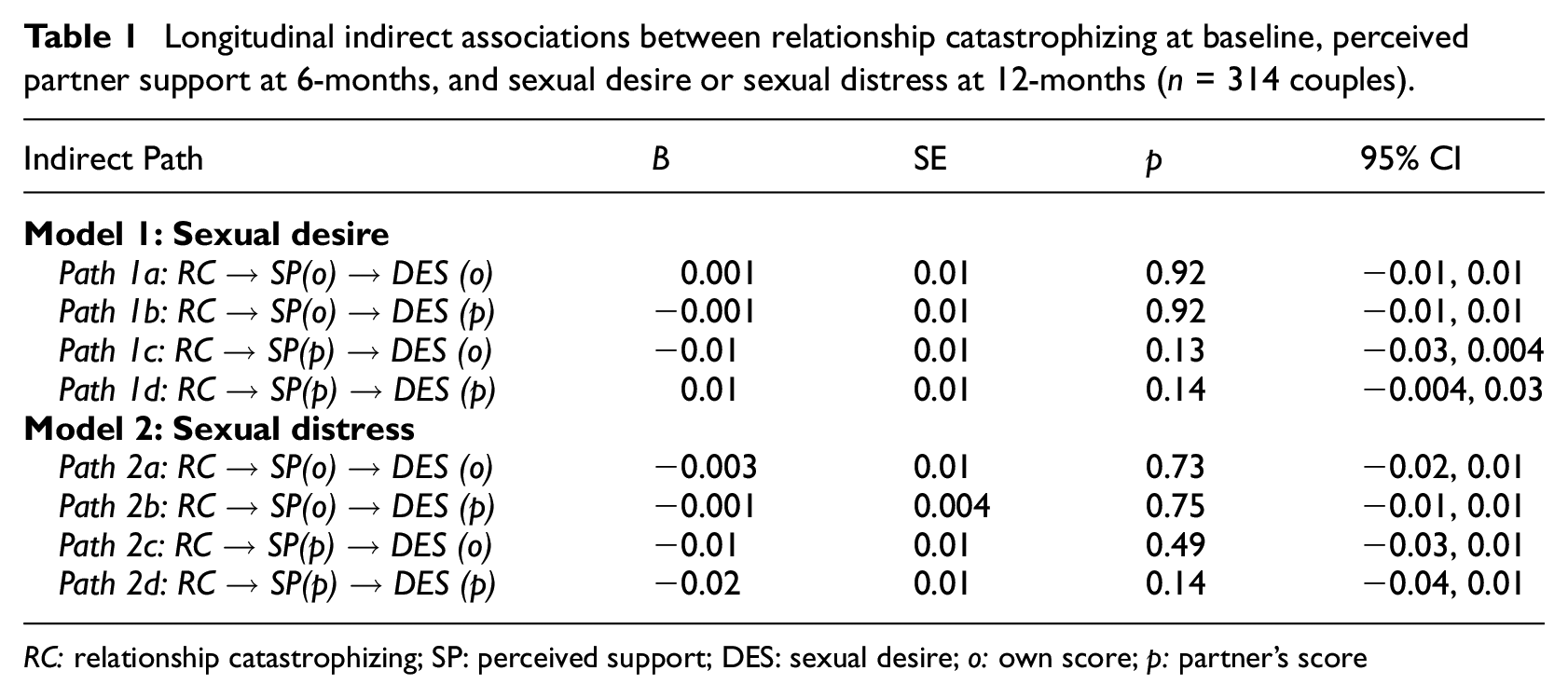
RC: relationship catastrophizing; SP: perceived support; DES: sexual desire; o: own score; p: partner’s score
Cross-sectional indirect associations between relationship catastrophizing, perceived partner support, and sexual desire or sexual distress (n = 314 couples).
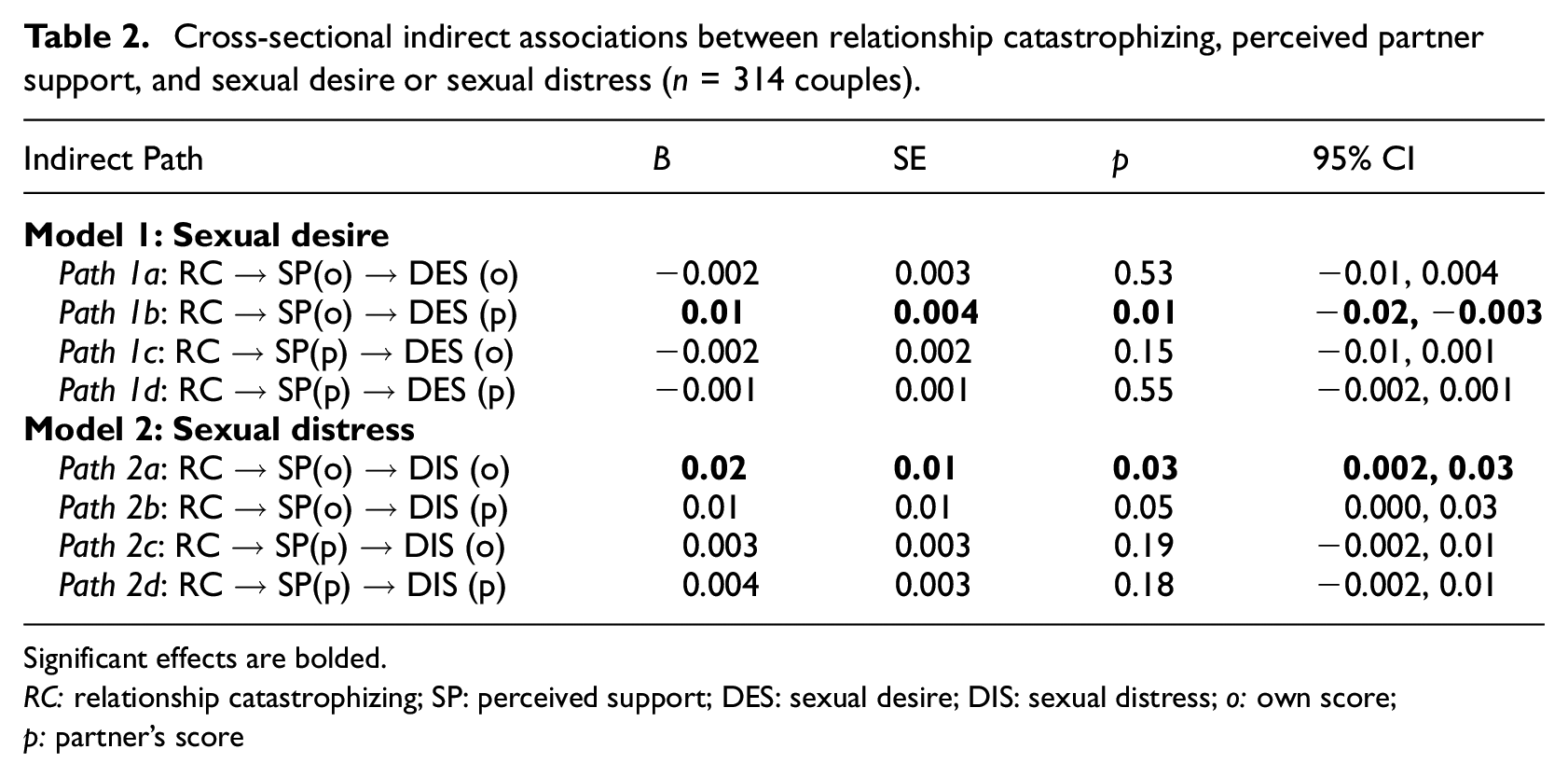
Significant effects are bolded.
RC: relationship catastrophizing; SP: perceived support; DES: sexual desire; DIS: sexual distress; o: own score; p: partner’s score
Longitudinal within-person associations between relationship catastrophizing, perceived partner support, and sexual desire across 12 months (Model 1; n = 314 couples).
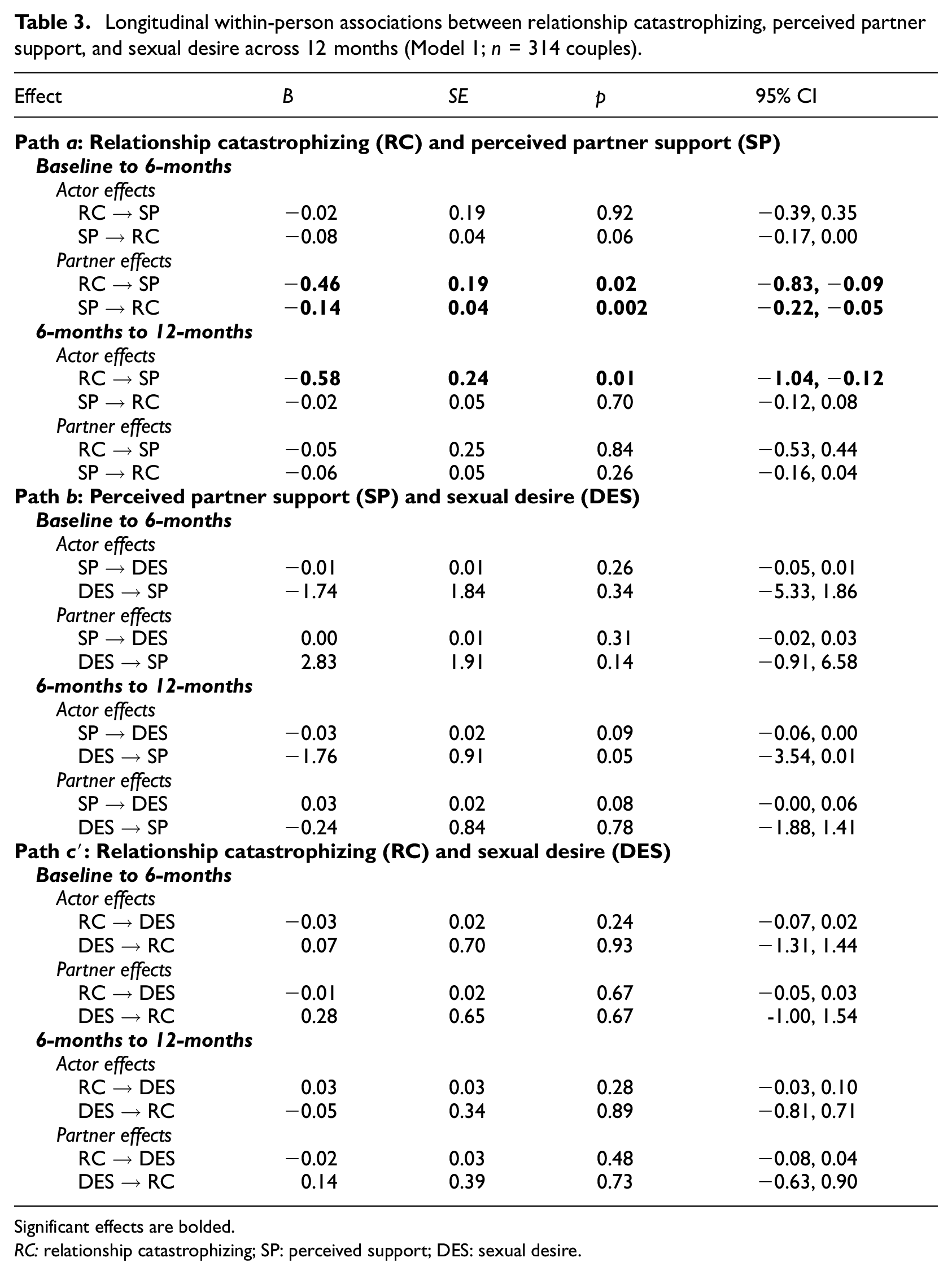
Significant effects are bolded.
RC: relationship catastrophizing; SP: perceived support; DES: sexual desire.
Longitudinal within-person associations between relationship catastrophizing, perceived partner support, and sexual distress across 12 months (Model 2; n = 314 couples).
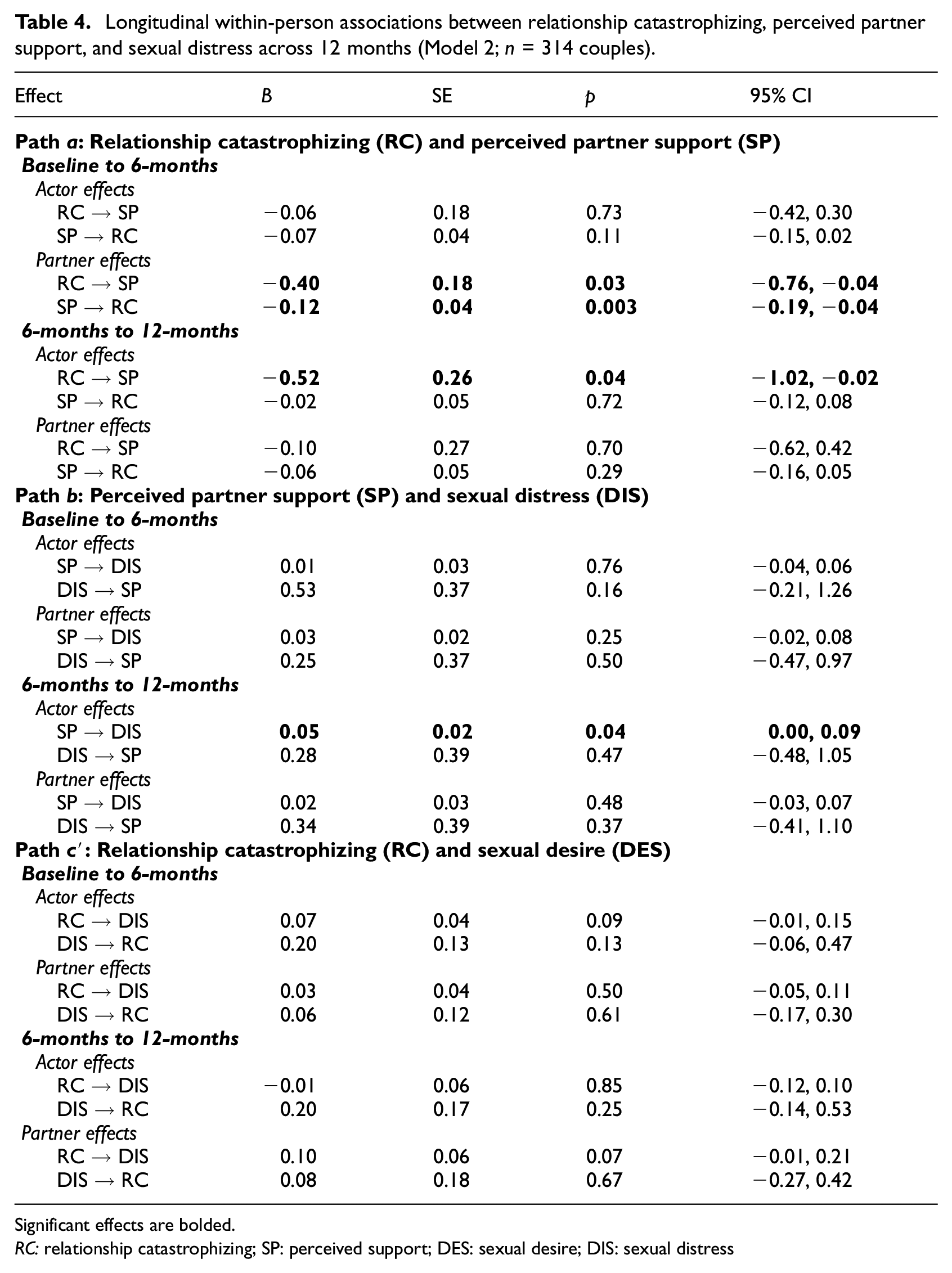
Significant effects are bolded.
RC: relationship catastrophizing; SP: perceived support; DES: sexual desire; DIS: sexual distress
Cross-sectional associations between relationship catastrophizing, perceived partner support, and sexual desire or sexual distress.
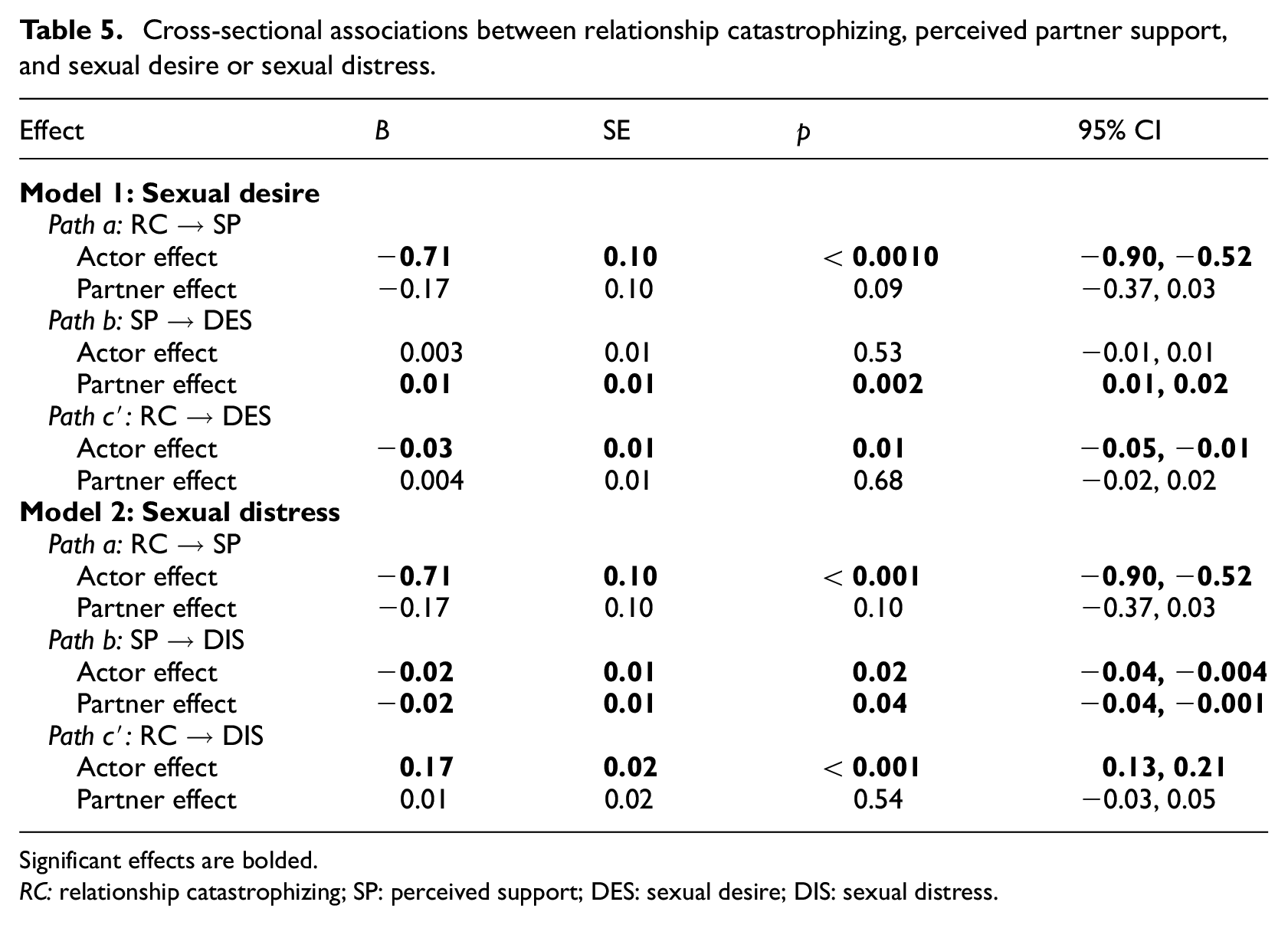
Significant effects are bolded.
RC: relationship catastrophizing; SP: perceived support; DES: sexual desire; DIS: sexual distress.
Within-person longitudinal associations
Relationship catastrophizing and perceived support (Models 1 and 2, path a)
From baseline to 6-months, an individual’s own relationship catastrophizing at baseline was not significantly associated with their own perceived support at 6-months, and perceived support at baseline also did not predict their own relationship catastrophizing at 6-months. However, in both Model 1 (sexual desire) and Model 2 (sexual distress), and in line with hypotheses, individuals’ higher scores of relationship catastrophizing at baseline compared to their own average predicted decreases in their partners’ perceived support 6 months later. Individuals’ higher-than-average perceived partner support at baseline also predicted decreases in their partners’ relationship catastrophizing at 6-months, suggesting a bidirectional link between individuals’ greater relationship catastrophizing and their partners’ decreased perceived partner support within this timeframe. Higher-than-average relationship catastrophizing at the 6-month timepoint was also associated with decreases in one’s own perceived partner support at 12-months, consistent with our prediction, but not with a partner’s perceived support at 12-months. Perceived partner support at 6-months was also not significantly associated with one’s own or one’s partner’s relationship catastrophizing at 12-months.
Perceived support and sexual outcomes (path b)
Relationship catastrophizing and sexual outcomes (path c′)
Longitudinal mediation (path c)
There were no significant indirect within-person effects observed in our longitudinal analyses. Although several significant cross-lagged effects indicated partial support of the hypothesized indirect paths, as described above, perceived partner support did not mediate the association between relationship catastrophizing and sexual desire or distress over time.
Indirect cross-sectional (between-person) associations
At baseline, relationship catastrophizing was significantly associated with one’s own, but not a partner’s, lower perceived support (path a) as well as sexual desire and greater sexual distress (path c′). Moreover, perceiving more partner support was linked to partners’ greater sexual desire, as well as lower sexual distress for both members of the couple (path b).
We found one significant indirect path between relationship catastrophizing and sexual desire, and two for sexual distress. Specifically, individuals’ greater relationship catastrophizing was associated with their own lower perceived support, which in turn was linked to their partners’ lower sexual desire and both their own and their partners’ greater sexual distress. There were no other significant cross-sectional indirect effects.
Discussion
In a dyadic study of couples seeking and receiving MAR, we examined longitudinal associations between relationship catastrophizing, perceived partner support, and sexual desire and distress across 12 months. Individuals’ greater relationship catastrophizing was associated with their own lower perceived partner support within the same timepoint and predicted decreases in their own perceived support 6 months later. However, results indicated a more nuanced relationship between perceived partner support and sexual outcomes. Higher-than-average perceived support at one timepoint was largely unassociated with sexual desire and distress at the next timepoint, with the exception of one significant path between lower levels of perceived support at 6 months and one’s own decreased sexual distress at 12 months. Perceived support did not mediate within-person associations between relationship catastrophizing and sexual desire and distress over time; yet, cross-sectional results provided evidence of these indirect associations occurring proximally. Within the same timepoint, individuals’ greater relationship catastrophizing was associated with their partners’ lower sexual desire, and both their own and their partners’ greater sexual distress, via their own lower perceived support. Our significant findings are consistent with theory and research positing catastrophizing as a strategy that individuals may use to seek partner support, but one that can backfire such that people who catastrophize more may perceive their partners as less supportive, which can have adverse short-term consequences (Sullivan et al., 2001). Proximally, less perceived support indirectly explained the links to lower sexual desire and higher sexual distress for both partners, but consequences did not persist over time, which may be an encouraging message for couples seeking MAR.
Evidence of cross-sectional indirect associations
By demonstrating that greater relationship catastrophizing was linked to lower sexual desire and greater sexual distress—by way of perceiving less partner support—within a given timepoint, we extend models that specify catastrophizing as a maladaptive strategy for seeking support (Petrini and Arendt-Nielsen, 2020) to the context of MAR. Individuals who were seeking or receiving MAR who catastrophized more about their relationship challenges also perceived less partner support, and in turn, they reported lower sexual desire and both partners reported greater sexual distress. Indirect cross-sectional results extend the interpersonal emotion regulation model of sexual dysfunction to couples navigating MAR, positing relationship catastrophizing as a maladaptive emotion regulation strategy (Rosen and Bergeron, 2019) that may be implicated in partners’ tendencies to respond in less supportive ways (Martire et al., 2019), with consequences for sexual outcomes. Relationship catastrophizing might heighten negative emotions or attentional focus toward negative aspects of their relationship (Petrini and Arendt-Nielsen, 2020), such as concerns of sex feeling “mechanical” rather than pleasurable, which could impede an individual’s ability to notice support provided by their partner. Moreover, individuals who catastrophize more about pain are more likely to seek support indirectly (e.g. reassurance-seeking) than to use direct communication (Cano, 2004), which may also extend to relationship catastrophizing. Given that coping with MAR-related stressors is a dyadic experience, having to decipher what is intended by their partners’ indirect communication can be an additional burden that reduces their capacity for supportive behaviors (Overall et al., 2009) As a result, catastrophizing may be less likely to motivate action or problem-solving (e.g. scheduling times to engage in sexual activity for connection) within the couple. By catastrophizing, individuals may inadvertently reduce the likelihood of receiving their desired support (Petrini and Arendt-Nielsen, 2020), which may interfere with intimacy, amplify concerns about sex, and reduce sexual interest, at least in the short-term.
The costs of relationship catastrophizing for sexual outcomes via less perceived support may not translate to long-term changes; perceived support did not mediate longitudinal associations between catastrophizing and sexual outcomes. These links might occur more proximally during MAR, with relevance for when couples are in the throes of relational stressors brought on by MAR. Even so, an analysis of direct longitudinal paths could help to delineate implications for couples during MAR, and is thus presented below.
Relationship catastrophizing predicted decreases in perceived support 6 months later
In line with theories of catastrophizing (Cano, 2004), higher-than-average relationship catastrophizing was linked to decreases in perceived partner support 6 months later. Our finding that individuals’ higher average relationship catastrophizing at 6-months predicted decreases in their own perceived partner support at 12-months demonstrates that engaging in greater catastrophizing about relationship challenges can indeed result in perceiving less partner support, even 6 months later. Patterns wherein catastrophizing may orient individuals’ attention toward MAR-related stressors (e.g. “mechanical” sex; Petrini and Arendt-Nielsen, 2020) may be self-reinforcing and can indeed intensify the salience of these stressors over time, with implications for noticing partner support. Catastrophizing also can have downstream implications for one’s partner, as evidenced by decreases in perceived support at 6-months for partners of individuals who catastrophized more at baseline. Given that individuals’ lower perceived support at baseline also predicted increases in their partners’ catastrophizing at 6-months, perceiving a partner as less supportive may provoke catastrophic thoughts about the relationship. For instance, perceiving less partner support may elicit worries (e.g. My partner is going to leave me if we don’t get pregnant) that may turn into catastrophizing (Cano, 2004), contributing to a bidirectional cycle of unhelpful positive reinforcement.
Associations between perceived support and sexual desire and distress 6 months later
Perceived support was largely unrelated to changes in downstream sexual desire or distress, contrary to significant cross-sectional associations between these variables. Predicting sexual outcomes over time is challenging given that many contextual factors interact with individual and interpersonal characteristics to impact sexuality across 6–12 months, especially when navigating MAR—which is often experienced as an emotional “roller-coaster” that changes as treatment cycles progress (Péloquin et al., 2024). Thus, we might expect variation in individuals’ responses depending on when they complete questionnaires relative to where they are in a MAR treatment cycle; it is difficult to conclude whether varying patterns of results between timeframes is empirically meaningful or whether it simply captures changes in participants’ feelings and cognitions that fluctuate with MAR procedures.
While opposite in direction to predictions, individuals who perceived lower-than-average levels of partner support at 6-months reported decreases in sexual distress at 12-months. It could be that individuals perceived less support from their partner because they were less distressed (i.e. have less support needs; Raposo et al., 2024), provided they have been coping together with MAR for an extended period of time, and less overall distress may translate to decreased sexual distress 6 months later. This finding was contrary to our hypotheses and warrants replication.
Relationship catastrophizing did not predict sexual desire and distress 6 months later
Although relationship catastrophizing was associated with both partners’ lower sexual desire and higher sexual distress cross-sectionally, we, unexpectedly, found no significant links between relationship catastrophizing and sexual outcomes 6 months later. However, it is fairly consistent with a prior study of new parents, which found that relationship catastrophizing predicted higher daily sexual desire and lower distress, but had minimal effects 4 months later (Wang et al., 2024). It is possible that the adverse impacts of catastrophizing on sexual relationships may not persist over time given the many other factors affecting desire and distress during MAR. Other research has implicated more robust short-term repercussions of pain catastrophizing, particularly given that catastrophizing about stressors may be most harmful when the stressors are novel or salient (Frumkin et al., 2023).
Strengths, limitations, and future directions
We recruited a large sample that was inclusive of sex- and gender-diverse and non-heterosexual individuals and couples, potentially extending generalizability. We shed light on the proximal versus enduring nature of these associations by comparing longitudinal and cross-sectional results, providing support for the state-dependent nature of catastrophizing applied to seeking MAR that has been evidenced in other contexts (e.g. pain; Day et al., 2021).
The current research also has important limitations. Given the nature of cross-sectional findings, indirect paths evaluated within a given timepoint should be interpreted cautiously, such that we cannot draw conclusions about directionality. Further, couples may be more prone to catastrophizing in response to specific stressors, such as reduced sexual satisfaction due to increased pressure to facilitate pregnancy (Repokari et al., 2007), and future research might consider utilizing a study design (e.g. daily diary) that can capture effects for perceived support, and subsequently, sexual outcomes closer in time to when the stressors occurred. Couples were asked to report on catastrophizing about relationship challenges, but instructions did not refer to MAR specifically; we cannot ascertain whether catastrophic thoughts pertained to MAR-related stress or to other relationship challenges. An observational study in which couples engage in a discussion about a MAR-related relationship stressor could further situate processes within the unique context of MAR. Lastly, although our sample exceeded recommendations for dyadic longitudinal studies (Ledermann et al., 2022), given the complexity of our statistical models and that RI-CLPM power analysis tools do not yet account for dyadic data, we may have been underpowered to detect all effects.
Conclusion and implications
While seeking or undergoing MAR, couples are vulnerable to unique relationship stressors that may increase the likelihood of catastrophizing about their relationship, and over time, repeated challenges can result in chronic stress that can further reinforce these patterns. Findings are consistent with models of catastrophizing (Sullivan et al., 2001) and dyadic processes in sexual relationships (Rosen and Bergeron, 2019), such that in the short-term—but not the long-term—perceiving less support from a partner indirectly accounted for the associations between relationship catastrophizing and sexual desire and distress in the context of MAR. Moreover, relationship catastrophizing may also contribute to perceiving a partner as less supportive over time. We extended the limited knowledge on relationship catastrophizing, conceptualizing it as a response to relational stress with adverse implications for sexual relationships—by way of constructing a more negative interpersonal environment surrounding sexuality (Rosen and Bergeron, 2019).
Findings point to potential psychoeducation and intervention targets aimed at helping couples maintain sexual well-being during MAR. For instance, couple-based cognitive-behavioral strategies might emphasize identifying and reducing catastrophic thought patterns, employing direct support-seeking strategies, and increasing both supportive behaviors and awareness of these behaviors when enacted by a partner (Bodenmann et al., 2020). As a result, couples may be better positioned to effectively manage stress to their relationships over the course of MAR, which in turn could support more satisfying sexual relationships.
Footnotes
Acknowledgements
We would like to thank our research team and study participants.
Data sharing statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
As of July 2019, this project has received Research Ethics Board approval from Dalhousie University (2019-4831) and l’Université de Montréal (19-070-P).
Informed consent
All participants provided written informed consent online prior to participation.
Consent for publication
Consent for publication is not applicable as it does not contain any identifiable data.