
Abstract
Depression is often described as likely associated with engagement and risk of disengagement (i.e. non-usage attrition) in digital behavior change interventions, but is rarely studied in-depth outside of mental health-specific programs; thus, we sought to quantify its influence on disengagement risk. Data come from 363 adults (mean age = 51.86, SD = 10.86; 70.3% female) randomized to the intervention groups of the LoseNowPA eHealth weight management intervention. Kaplan-Meier and Cox proportional-hazards modeling were applied on the outcome of cessation of logins before program end at 12 months. Overall, mild to moderate depression symptoms were associated with an increased risk of early disengagement from this eHealth intervention, controlling for sociodemographic covariates (p < 0.0001). Subclinical levels of depression can still exert meaningful influence on participant risk of disengagement in digital weight loss interventions, which can limit their effectiveness. Future interventions may wish to consider tailoring on depression symptoms to possibly preserve engagement.
Introduction
Over 70% of U.S. adults live with overweight or obesity, which significantly contributes to lifetime risk of preventable mortality and morbidities including diabetes, cardiovascular disease, and certain types of cancers (Lega and Lipscombe, 2020; NIDDK, 2021; Pati et al., 2023; National Center for Health Statistics, 2021). Digital behavior change interventions (DBCIs) can address a variety of health outcomes including weight management, often eliciting equal or greater effect sizes than traditional in-person interventions (Flores Mateo et al., 2015; Mangieri et al., 2019; Rivera et al., 2016; Shaw et al., 2013; Vandelanotte et al., 2016). DBCIs feature increased scalability to reach numerous participants without significantly increasing costs relative to in-person formats (Fryar et al., 2018). Engaging with these programs is an instrumental step for their effectiveness, with engagement defined from Perski et al. as the degree of participant usage and interactivity with the digital interface of an intervention, including responsiveness and attention to program messages and lessons, as well as accessing of program tools and resources (Perski et al., 2016).
Generally, the longer participants are engaged with a DBCI, the more effective the intervention is, as this prolonged engagement increases the dose received of intervention materials delivered via messages, lessons, resources, self-monitoring, and other components which may be objectively measured (Eysenbach, 2005; Funk et al., 2010; Hurley et al., 2025; Perski et al., 2016; Richardson et al., 2013; Short et al., 2018). However, there is a known tendency for DBCI engagement to sharply decline within the first few months of interventions (Eysenbach, 2005; Yeager and Benight, 2018). As such, there has been interest in researching how to preserve engagement and reducing the likelihood of early disengagement (also referred to as non-usage attrition), defined here as a point in time when participants stop interacting with a DBCI and all engagement indicators reach zero, but that participant is not lost to intervention follow-up (Eysenbach, 2005).
Research has found associations between some sociodemographic characteristics and risk of disengagement with DBCIs. Generally, age has been found to be positively related with DBCI engagement until around age 65, although some studies report younger adults aged 18–35 may show high levels of early program engagement before disengaging sooner in time (Borghouts et al., 2021; Glasgow et al., 2007; Gokee-LaRose et al., 2009; Perski et al., 2016). Additionally, higher educational levels tend to be positively associated with participant engagement and reduced risk of disengagement in DBCIs (Geraghty et al., 2012; Perski et al., 2016; Richardson et al., 2013; Strecher et al., 2008). Some studies have reported that females show lower risks of disengagement or dropout with online interventions (Funk et al., 2010; Geraghty et al., 2012). Additionally, participants who report dissatisfaction with programs, lower readiness to change, time constraints, or perceived lacking of mastery of key behaviors have an increased risk of early DBCI disengagement or dropout (Al-Asadi et al., 2014; Habibović et al., 2014; Neve et al., 2010; Postel et al., 2011).
Depression has been previously acknowledged as probable contributor to reduced DBCI engagement and overall adherence to DBCI program recommendations, but is rarely quantitatively examined in-depth outside of interventions directly targeting mental health issues (Perski et al., 2016; Wing et al., 2002; Yeager and Benight, 2018). As depression symptoms and weight status are positively correlated and tend to exhibit reciprocal relationships such that higher bodyweight is associated with higher depressive symptoms and vice versa (not including severely underweight individuals); this is a pertinent issue for DBCIs related to weight management to consider (Breymeyer et al., 2016; Jung et al., 2017; Noh et al., 2015).
This secondary analysis assesses whether depression symptoms are associated with the likelihood of participants disengaging with the website of a 12-month eHealth intervention for weight loss in a primary care setting. The guiding hypothesis for this analysis is that higher levels of depression symptoms are associated with increased risk of early disengagement from this DBCI, controlling for sociodemographic characteristics.
Materials and methods
Study design and participants
Data for this analysis come from LoseNow PA (LNPA), a 12-month cluster-randomized controlled trial using an eHealth website to promote weight management for patients in a primary care setting (Tate et al., 2022). In this program, 31 primary care providers (PCPs) and 550 patients were randomly assigned to one of three intervention groups: (1) enhanced usual care (EUC, n = 187); (2) internet weight loss intervention (IWL, n = 181); or (3) internet weight loss intervention plus automated physician-tailored feedback (IWL + PCP, n = 182). Participants were enrolled if they were between 21 and 70 years old, had a body mass index (BMI) of 25–50 kg/m2, had reliable internet access, and had plans to visit their PCP within the same year (Tate et al., 2022).
Participants in both IWL intervention arms had access to the LNPA study website requiring a username and password to log in. The study website included instructional lessons; self-monitoring pages for calories, physical activity, and weight; computer-tailored feedback; personal goal setting tools; problem solving tools; a progress summary page; resource pages; a message board with other participants; and opt-in reminder text messages containing updates, encouragement, and motivational content. The primary difference between the intervention arms was that the IWL + PCP condition also received biweekly emails containing computer-generated tailored messages addressed from their PCP related to weight loss progress, frequency of website log-ins, time in the program, and other factors such as patient-reported motivation. PCPs could view and edit these messages for each patient before sending, although end results showed that only 1.2% of all provider messages sent were edited (Tate et al., 2022). Briefly summarizing primary outcomes of the trial, both the IWL and IWL + PCP arms exhibited significantly greater weight loss than EUC; however, there were no significant differences between IWL and IWL + PCP on any outcomes. As the study website was functionally identical across both intervention arms and no significant influence of the automated physician advice messaging was detected, participants from both arms are pooled to maximize statistical power for this secondary analysis. For further details of the LNPA trial, see Tate et al. (2022).
Ethical statement
The parent LNPA study was approved by Institutional Review Boards (IRB) at the University of North Carolina at Chapel Hill (#12-1661) and Penn State College of Medicine (#39237), and was pre-registered on ClinicalTrials.gov (NCT01606813). All participants provided written informed consent prior to enrollment and randomization into the study, and all research was ethically conducted in accordance with the World Medical Association Declaration of Helsinki. This secondary analysis uses de-identified data from the LNPA study and was exempt from IRB approval, as the identities of human subjects cannot be ascertained directly or through identifiers linked to the subjects.
Measures
LNPA participants completed clinical anthropometrics and survey assessments at baseline, 3, 6, and 12 months. The Center for Epidemiological Studies-Depression (CES-D) scale was administered as part of these packets at baseline, and is applied here as a validated indicator for depression symptoms as the primary independent variable of analysis (Herrero and Meneses, 2006). CES-D score values range from 0 to 60, with higher values indicating greater depressive symptomatology, and scores ≥ 16 typically referenced to indicate risk of clinical depression, although the scale itself is non-diagnostic (Herrero and Meneses, 2006). Additional covariates applied in this analysis include self-identified age, baseline bodyweight, sex, race/ethnicity, and highest educational attainment. Age and bodyweight are mean-centered relative to the full (n = 363) sample to promote interpretability.
Engagement and, by extension, disengagement are indicated via user logins to the IWL website. Each website login was timestamped and program day was calculated relative to a given participant’s start date. To be considered for this secondary analysis, participants must have logged onto the IWL website at least once during the 12-month program must have 12-month clinical measurements. Disengagement is operationalized as the dependent variable (DV) of analysis as the program day of a participant’s last login to the IWL website, but they were not lost to follow-up at the 12-month study assessment (to distinguish disengagement from other types of attrition). Logins after this 12-month date were right-censored. Sensitivity analyses using the full sample of those who disengaged or dropped out without 12-month follow-up measures were also conducted for comprehensiveness.
Data analysis
A null model of logins over time is initially examined using Kaplan-Meier estimates to create a survival curve displaying the probability of users having >0 logins at each interval (Goel et al., 2010). After establishing the null model, the login DV was regressed onto CES-D scores and sociodemographic covariates using a Cox proportional-hazards regression analysis (Borgan et al., 1995; Fox and Weisberg, 2002; Schober and Vetter, 2018).
Conditional Cox proportional-hazards models regressed disengagement onto the CES-D and sociodemographic covariates to calculate a hazard ratio (HR) indicating higher or lower risk of disengagement occurring relative to a reference group, conditional on time (Schober and Vetter, 2018). In this analysis, the comparison group comprises white, female participants with a high school education of average age, baseline bodyweight, and CES-D scores for the sample. HRs > 1 indicate an increased risk of early disengagement relative to this group, while HRs < 1 indicate a reduced risk of early disengagement relative to this group, following a 1-unit increase in predictor covariates. All analyses were conducted using R statistical software (Therneau and Grambsch, 2022).
Results
Descriptive statistics
LNPA participants randomized to the IWL and IWL + Advice groups were mostly white (82.3%) and female (70.3%) with a mean age of 51.86 and mean baseline weight of 97.99 kg (216.03 lbs). Less than half of the sample (38.3%) reported completing a Bachelor’s degree equivalent or greater. Baseline CES-D scores had a mean of 13.13 (SD = 9.96) with a range of 0–41. Approximately 112 (30.9%) of the sample reported CES-D scores ≥ 16, which would indicate a risk for clinical depression (Eaton et al., 2004). A summary of baseline characteristics is displayed in Table 1.
Participant characteristics of full LNPA sample (N = 363).
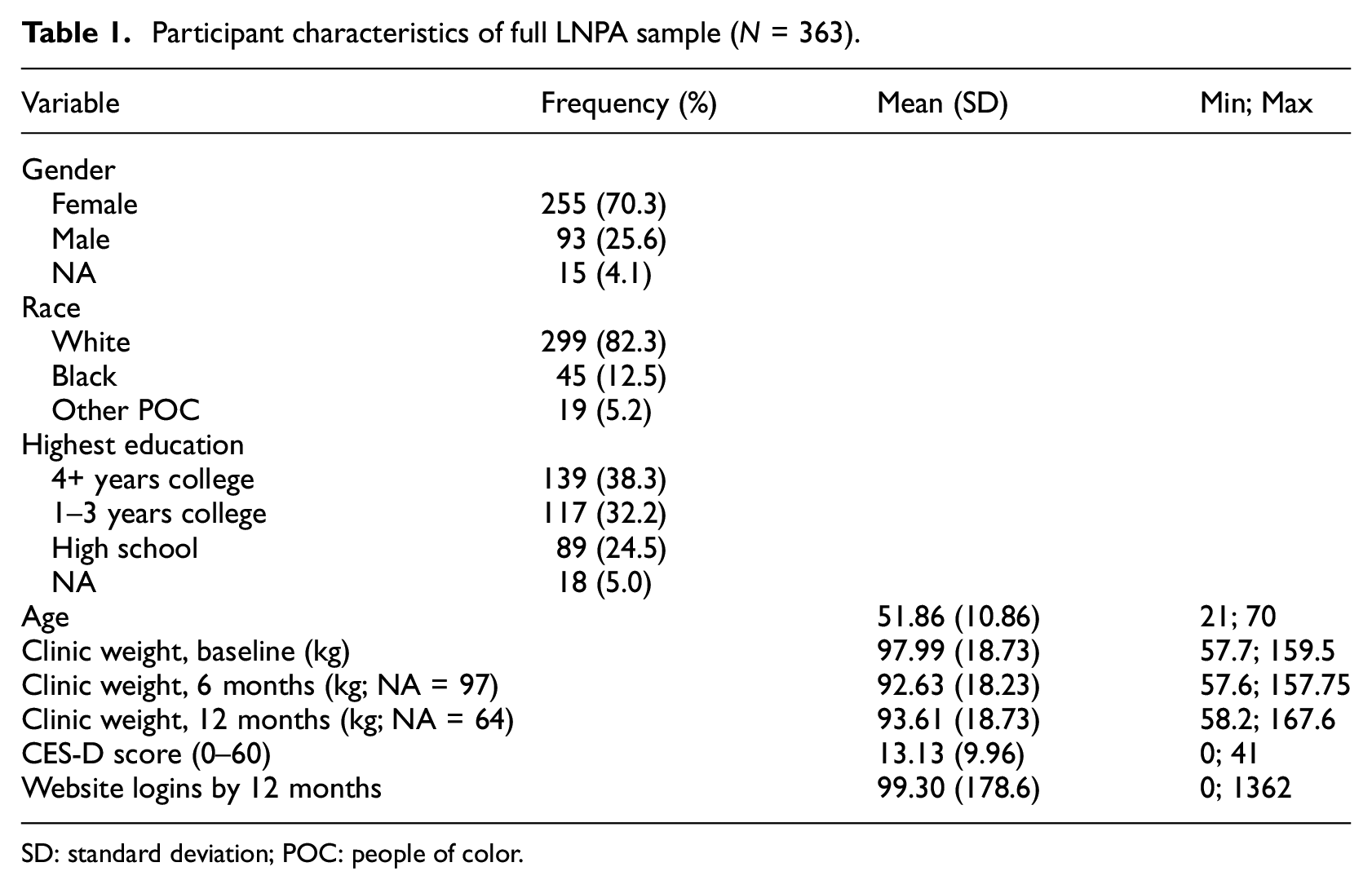
SD: standard deviation; POC: people of color.
There was high variability in IWL website logins. Of the N = 363 participants assigned to the IWL and IWL + PCP groups, 24 (6.6%) participants never logged in to the LNPA website, and 53 (14.6%) participants logged in ≤5 times over 12 months. In contrast, there were several users with very high engagement indicators (e.g. one user had 977 website logins within 6 months, relative to the sample mean of approximately 99 logins at the time). This high variance in logins persisted after outlier assessment and removal, so these observations remained in the dataset.
After restricting the dataset to the n = 339 participants who had logged into the IWL website at least once, a further 51 participants were missing 12-month clinical weight measurements and marked as lost to follow-up; rendering the effective sample size for this secondary survival analysis n = 288. There were no significant differences in study variables between the full and subset samples. Considering disengagers only (i.e. not attritors lost to follow-up), there were approximately 48 (16.7%) website disengagements by 3 months, and 35 (12.1%) new disengagements at 6 months; leaving the remaining ~205 (71.1%) participants to disengage at some point between program months 6 and 12.
Survival analysis
Kaplan-Meier plots display the longitudinal probability that an event (i.e. cessation of logins) had not occurred by a given time point, without involving any predictor variables or applying assumptions that can be violated (i.e. nonparametric distributions; Goel et al., 2010). The plot displayed in Figure 1 shows the proportion of participants logging in to the LNPA website over time, measured in days on the x-axis. The dotted lines represent a 95% confidence band. Median survival time for this sample, when approximately 50% of users had disengaged, is approximately 278 days (slightly over 9 months) with 182 participants still logging in to the program after this time (SE = 0.0262; 95% CI = 0.45, 0.53).
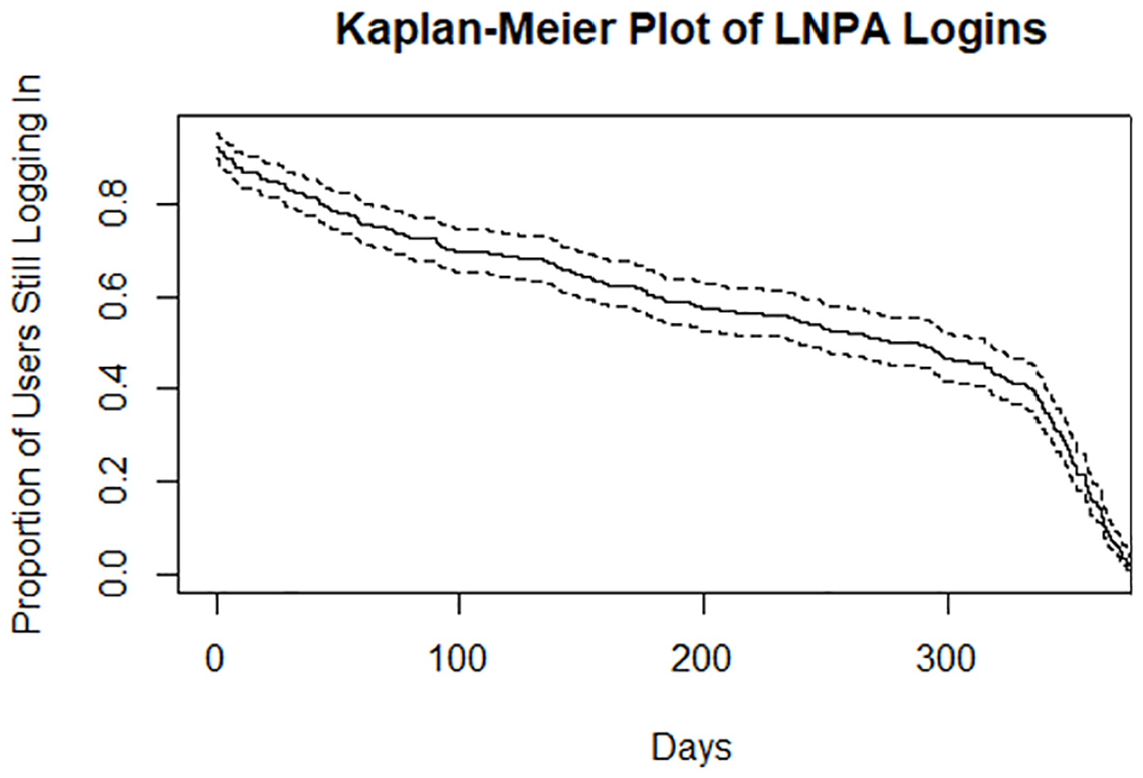
Kaplan-Meier plot of LNPA disengagement over 12 months.
Results from the Cox proportional-hazards model are summarized in Table 2, with HR coefficients exponentiated for interpretability. When modeled in isolation (not shown in table), a 1-unit increase in baseline CES-D scores above the sample mean (13.13) multiplicatively increased the hazard of disengagement by a factor of 1.056, which was significant (SE = 0.007; p < 0.0001). Controlling for participant age, sex, race, education, and baseline bodyweight a 1-unit increase in baseline CES-D scores above the sample mean increased the HR of disengagement by a factor of 1.047, which remained statistically significant (SE = 0.007; p < 0.001). Concordance for this model was 0.736 (SE = 0.027).
Cox proportional-hazards of early disengagement over 12 months.
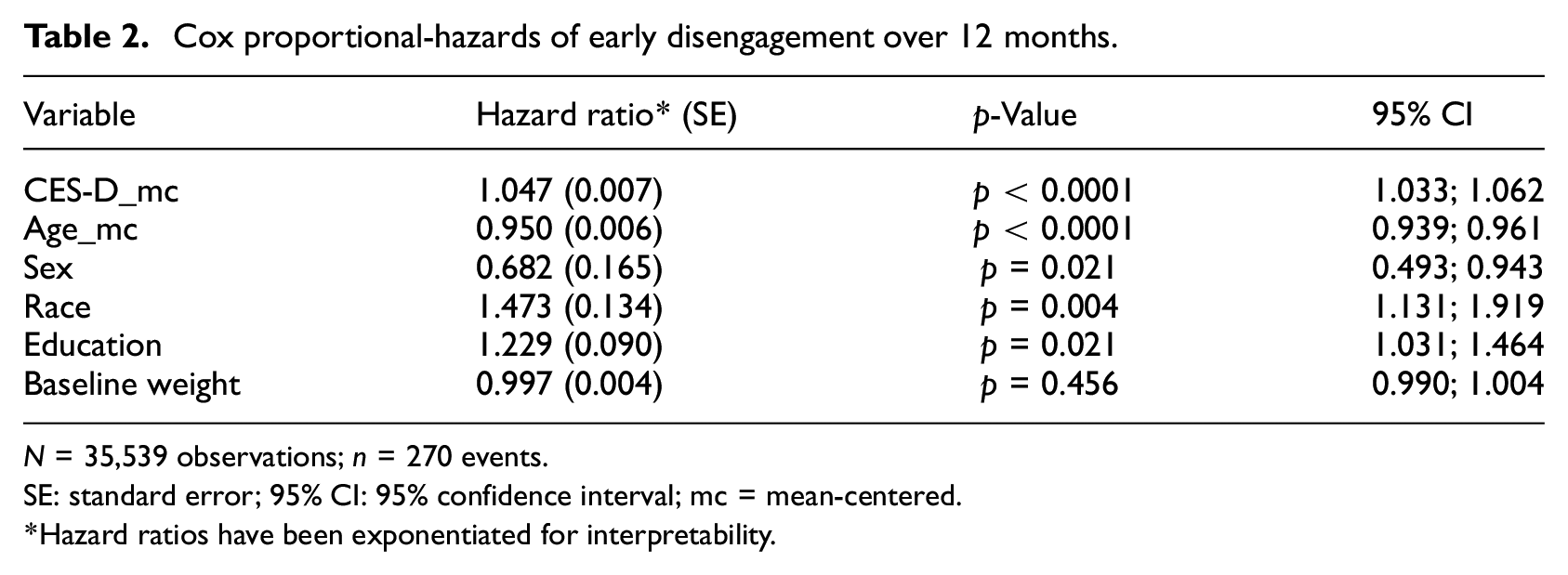
N = 35,539 observations; n = 270 events.
SE: standard error; 95% CI: 95% confidence interval; mc = mean-centered.
Hazard ratios have been exponentiated for interpretability.
These raw effect size estimates may appear small because CES-D scores fall on a scale of 0–60; thus, a 1-unit increase in CES-D score represents a minute change in reality. To assist with interpretation of effects, this model was re-run using standardized CES-D scores such that a one standard deviation increase in scores (approximately 10) above the sample mean (13.13) was associated with a 1.58 factor increase in the hazard of disengaging from the IWL website early, controlling for covariates (SE = 0.063; p < 0.0001). To interpret this effect, a participant who scores approximately 23 on the CES-D and would be considered at risk of developing clinical depression has 1.58 times the hazard of disengaging from an eHealth intervention earlier than others, controlling for sociodemographic covariates.
Interpreting control covariates, each year increase in baseline age above the sample mean (~51.86) was associated with 0.95 times the hazard of disengagement, controlling for covariates (SE = 0.006; p < 0.0001). Males had approximately 0.65 times the hazard of early disengagement, compared to the reference group of female participants, which was significant (SE = 0.15; p = 0.004). Participants identifying as Black and other POC had approximately 1.5 times the hazard of disengagement in this sample, controlling for covariates (SE = 0.132; p = 0.002). Increased educational status of at least some college also significantly increased the hazard of disengagement by a factor of approximately 1.23, controlling for covariates (SE = 0.09; p = 0.02). These results remained consistent when examined at 6 months via right-censoring, and when compared to the full sample including attritors. Increases in baseline bodyweight above the sample average were not found to be associated with risk of disengagement over time.
Discussion
This analysis confirms the hypothesized association between depression and disengagement risk such that CES-D scores indicating mild to moderate depression symptoms, but below the threshold indicating clinical depression (i.e. CES-D ≥ 16), were associated with an increased risk of earlier disengagement from an eHealth intervention, controlling for sociodemographic covariates.
Other studies examining DBCIs for various health behaviors have identified factors contributing to risk of early disengagement or dropout such as program dissatisfaction, readiness to change, time constraints, or perceived behavior mastery (Al-Asadi et al., 2014; Habibović et al., 2014; Neve et al., 2010; Postel et al., 2011); however, we are aware of only one study that has only reports clinically-diagnosed depression as a significant contributor to disengagement risk (Hebert et al., 2010). It is known that depression may negatively influence one’s self-efficacy to perform behavioral tasks necessary to achieve program goals and contribute to stronger negative emotions when those goals are failed, which could lead users to give up on a program (Bandura and Locke, 2003; Perski et al., 2016). However, it is beyond the scope of the present analysis to examine these postulations in meaningful depth.
This secondary analysis revealed significant associations between sociodemographic control covariates and risk of disengagement. Participants aged above the sample mean (m = 51.86) were slightly less likely to disengage with the DBCI before its end date. This aligns with previous findings that age can be positively associated with engagement in digital interventions (Borghouts et al., 2021; Glasgow et al., 2007; Gokee-LaRose et al., 2009; Perski et al., 2016). Conversely, education was found to be associated with an increased risk of disengagement over time in this study, compared to participants with a high school education. This was unexpected, and goes against common consensus in DBCI literature where education tends to be positively associated with engagement (Geraghty et al., 2012; Perski et al., 2016; Richardson et al., 2013; Strecher et al., 2008); however, Couper et al. (2010) also reported higher levels of education being negatively associated with engagement in an online nutrition promotion intervention. It is possible the LNPA IWL contents may have had more appeal for those with high school education levels.
Participants who identified as Black or other PoC showed almost 1.5 times the risk of early disengagement from the LNPA website, net of other covariates. This effect was significant despite this group only accounting for <20% of the full intervention sample. It is known that mobile health apps and interventions in the U.S. often recruit high numbers of middle-aged white women with high education and moderate to high income, leading to concerns that studies may inadvertently lead to tailoring recommendations for, as Freudenberg alliterates, the “white, worried, and well” which could exacerbate existing health disparities (Freudenberg, 2017; Hutchesson et al., 2015; Sherrington et al., 2016). While this discovery is incidental and interpretations should be made with strong caution based on the small number of observations in this sample, it signals a need both to recruit more diverse samples in DBCIs, as well as for future research examining whether some DBCI aspects may be turning participants of color off or away.
Limitations and strengths
Our operationalization of disengagement as the last website login was not sensitive to gaps or lapses in engagement to the study site—only permanent disengagement. For example, if a hypothetical user logged into the study site daily in month 1, took a 6-month break, and logged in one last time in month 7, they would only be captured here as having disengaged in month 7 (though we did not observe such extreme gaps in this sample). Furthermore, the LNPA study sample lacked racial and gender diversity, with a large majority of study participants identifying as white (82.3%) and/or female (70.3%), which is unfortunately not uncommon among weight management DBCIs conducted around this time (Hutchesson et al., 2015; Sherrington et al., 2016). However, to identify some strengths, the LNPA study did include >50% of participants without a Bachelor’s degree or equivalent, included many older participants living with comorbidities including diabetes and hypertension from primary care settings, and applied objective indicators of study engagement logged from the program website.
While this analysis quantifies how individual characteristics were associated with early disengagement, it does not provide insight into mechanisms underlying these associations. As digital interventions continue growing in complexity, future studies could investigate time spent on various digital resources or reading program messages as metrics for attentiveness or absorption into program contents. Future studies might also consider using in-app assessments of participants’ perceptions of the program or behavior change processes prior to program end to provide further insight into mechanisms influencing disengagement from those who may later attrit (Short et al., 2018).
Conclusion
To quote Albert Bandura, “Those beset by self-doubts become the early quitters rather than the successful survivors” (Bandura, 1997). This analysis shows that participants reporting higher symptoms of depression were more likely to disengage from a weight management DBCI earlier than participants reporting lower symptoms. These findings could carry greater implications for DBCIs targeting health behaviors that have known associations with depression, that the people who may be at higher risk and need for assistance could also be at higher risk of disengaging from these programs if no considerations are made for them. Future digital interventions should examine if this relationship indeed holds for behaviors outside of weight management, and consider tailoring program content on depressive symptomatology and examining if this helps prolong affected users’ program engagement and subsequent benefits to health outcomes.
Footnotes
Acknowledgements
The authors would like to thank Karen Hatley, Molly Diamond, and Kristen Polzien for their invaluable assistance with the primary LNPA intervention.
Author contributions
DT and CS supervised the original study and provided data for analysis. LH conceptualized this secondary analysis, curated, and analyzed the data, and wrote the initial manuscript draft. NGO provided methodological supervision and validation. All authors were involved in the writing of this paper and had final approval of the submitted version.
Data sharing statement
De-identified data and R code from this analysis may be made available by request to the corresponding author, in compliance with applicable privacy laws, data protection, and requirements for consent and anonymization.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the T32 Cancer Health Disparities Training Grant from the National Cancer Institute of the National Institutes of Health [grant number T32CA128582]. Parent study funded by National Institute of Diabetes and Digestive and Kidney Diseases [grant number R01-DK095078].
Ethics approval
The parent LNPA study was approved by institutional review boards at the University of North Carolina at Chapel Hill (#12-1661) and Penn State College of Medicine (#39237). This secondary analysis was exempt from ethical approval as all data were de-identified such that the identities of human subjects could not be readily ascertained directly or through identifiers linked to the subjects.
Informed consent
Within the parent study, primary care providers and patients completed and returned informed consent forms prior to randomization and data collection.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Pre-registration
The parent study was pre-registered on ClinicalTrials.gov (NCT01606813).