
Abstract
Non-adherence is common in people with rheumatoid arthritis (RA). According to the ‘necessity-concerns framework’, beliefs about the necessity and concerns about prescribed medications influence adherence. The present study’s objective was to investigate whether depression moderates associations between beliefs about medicines and adherence among people with physician-diagnosed RA in a longitudinal study (N = 361; 31% male, mean age [SD] 60.2 [13.4]). Adherence (adherent vs non-adherent; MARS), beliefs about medicines (BMQ), and depression (HADS) were assessed at baseline, 3- and 12-month follow-up. Multivariate logistic regression models were calculated (predictors: necessity/concerns, depression; outcome: adherence). Two-thirds of patients were non-adherent. No significant interactions were found between necessity/concerns and depression. Contrary to previous cross-sectional research, we did not find evidence for a moderating role of depression in associations between beliefs about medicines and adherence. Possible moderating effects of depression might be less robust than previously thought and therefore harder to detect in longitudinal analyses.
Keywords
Background
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by an often progressive course. Patients with RA suffer from pain, joint swelling, limited mobility, associated disability and reduced health-related quality of life (Di Matteo et al., 2023; Smolen et al., 2018). Although pharmacological treatment is effective, non-adherence is prevalent in patients with RA. Estimates of the extent of non-adherence vary between 10% and 90% (Anghel et al., 2018; Scheiman-Elazary et al., 2016; van Den Bemt et al., 2012).
The ‘necessity-concerns framework’ (Horne and Weinman, 1999) explains non-adherence in terms of beliefs about medicines, that is, patients’ beliefs about (a) the necessity of their prescribed medications to maintain their health and (b) their concerns about potential side effects. This association between beliefs about ones’ prescribed medication and adherence is empirically well established: Several reviews on the causes of non-adherence in the treatment of RA have identified patients’ beliefs about the necessity of medication as well as patients’ concerns consistently as relevant patient-centred factors associated with non-adherence (Chowdhury et al., 2022; Horne et al., 2013; Pasma et al., 2013).
An important area of research is the investigation of the way in which the association between beliefs about medicines and adherence behaviour may be influenced by patient characteristics, such as the presence of co-morbidities. This way, interventions to improve adherence in RA patients can be better tailored towards patients’ needs.
A common co-morbidity in RA patients is depression (Cheng et al., 2023; Matcham et al., 2013). In a cross-sectional analysis, Brandstetter et al. (2016) found that depression moderates the relationship between beliefs about medicines and adherence in a sample of RA patients, with different effects depending on the specific beliefs in question (necessity beliefs vs concerns). Specifically, patients with elevated depressive symptoms showed a stronger association between necessity beliefs and adherence, whereas higher depressive symptoms attenuated the associations between concern and adherence. This study was limited by its cross-sectional study design. Cross-sectional findings may overestimate the actual effect size, for example, as a methodological artefact due to co-occurrence of predictor and outcome measures. Therefore, longitudinal studies of patient cohorts are needed to establish the robustness of results from cross-sectional analyses (and also strengthen causal assumptions). Our research question therefore is whether depression moderates the association between beliefs about medications and medication adherence in patients with RA in a longitudinal setting using the same cohort as Brandstetter et al. (2016).
Methods
Study design and sample
The study was conducted at the Department of Rheumatology, Asklepios Medical Center Bad Abbach, a tertiary care centre for patients with autoimmune and rheumatic diseases, located in the south of Germany (Brandstetter et al., 2016, 2017). At the initial study visit (baseline [T0]), participants were asked to complete self-report questionnaires. In addition, information was extracted from electronic health records. Patients were eligible for participation if they were aged 18 years or older, had physician-diagnosed RA and were currently under medical treatment for RA. Baseline data were collected in 2012 and 2013 (T0, N = 361). At baseline, participants provided their postal address and received self-report questionnaires by mail 3 (T1, N = 292) and 12 (T2, N = 245) months later as follow-ups. The study has been approved by the ethics committee of University of Regensburg (file-number: 12-101-0126).
Measures
Medication adherence, beliefs about medicines, and depression were assessed at all three measurement points.
Medication adherence
Medication adherence was assessed using the German version of the Medication Adherence Report Scale (MARS; Mahler et al., 2010). The scale consists of five items on intentional and non-intentional adherence behaviours (e.g. forgetting to take medication, or intentionally taking less dosage than prescribed). Items are answered on a five-point Likert-scale ranging from 1 (never) to 5 (always). A sum score was calculated (Cronbach’s α = 0.769, 0.773 and 0.791 for baseline, 3 and 12 months follow-up). Due to the highly skewed distribution, we dichotomized the MARS score with the value of 25 indicating complete adherence (vs 24 or less indicating non-adherence). Additionally, sensitivity analyses were performed with cut-off values of ≤24 and ≤23 to ensure the robustness of the results (data not shown). As there is no agreement in the literature on a specific cut-off value, we applied sensitivity analyses to confirm the main results of the analyses by repeating the analyses with varying cut-off points (i.e. 23, 24 and 25). This approach also encapsulates a median split (Md = 24 [IQR = 22–25]) as a statistical method for dichotomization for all MARS scores at baseline, and 3 and 12 months follow-up.
Beliefs about medicines
Patients’ beliefs about medicines were measured using two scales of the Beliefs about Medicines Questionnaire (BMQ; Horne et al., 1999; Mahler et al., 2012). The ‘necessity’ scale assesses patients’ perceived necessity regarding their prescribed medicines and consists of five items (e.g. ‘I could not live without my medicines’). The scale ‘concern’ assesses patients’ concerns about their medicines and consists of six items (e.g. ‘Sometimes, I worry about my medicines’). Items are answered on a five point Likert-Scale from 1 (fully disagree) to 5 (fully agree). The scale scores were calculated as a mean with higher values indicating stronger beliefs. Cronbach’s alpha were α = 0.766, 0.858 and 0.856 (necessity) and α = 0.758, 0.770 and 0.798 (concerns), for baseline, 3 and 12 months, respectively.
Depression
The depression scale of the Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith, 1983) was used to assess patients’ depressiveness. The total sum score ranges from 0 to 21, with higher values indicating the presence of more depressive symptoms (Cronbach’s α = 0.861, 0.886 and 0.870, for baseline, 3 and 12 months, respectively).
Statistics
For continuous variables, either median (Md) or interquartile range (IQR), or mean (M) and standard deviation (SD) are reported. For categorical variables, counts and percentages are used. Group differences were determined by t-tests.
Multivariate logistic regression models were calculated to test the moderating role of depression. To ensure comparability with Brandstetter et al. (2016), analyses were replicated from that study: Necessity/concerns and depression are predictor variables, and were transformed by grand mean centring before inclusion into the regression model. Sex (for necessity only), the number of prescribed RA medications and self-rated pain were included as confounders; in the original study, the included confounders were selected from a larger set of theoretically devised confounders, based on univariate analyses. Results of the logistic regression analyses are given as odds ratios (OR) and 95% confidence intervals (CI). Model fit is reported as Nagelkerke’s R2. p-Values <0.05 were interpreted as statistically significant. All analyses were performed using SPSS.29. To assess the robustness of the association between the multivariable predictors and non-adherence, the performance of the non-adherence model was tested with a less conservative definition (MARS values ≤ 24 and ≤23; data not shown).
For the regression models, beliefs about medicines (necessity, concerns) at T0 predict adherence at T1 and T2. The stability of beliefs about medicines is then assessed (T0–T1). If beliefs about medicines are not sufficiently stable (i.e. low reliability), regression models are calculated with beliefs about medicines at T1 predicting adherence at T2. If reliability is high (T0–T1: r ≥ 0.7), this step is omitted.
Results
Sample characteristics
Characteristics of study participants are presented in Table 1. Variables include socio-demographic and medical characteristics. About 30% of participants were male with a mean age of approximately 60 years (SD = 13.4, range: 19–92 years). The reported duration of RA was M = 11 years (SD = 9.2, range: <1–43 years), and about 40% of participants reported having experienced severe side effects from their medication at some point in time (‘Have you ever experienced serious side effects from the medication you take to treat your rheumatic disease?’).
Sociodemographic and medical characteristics of study participants at Baseline (T0, N = 361).
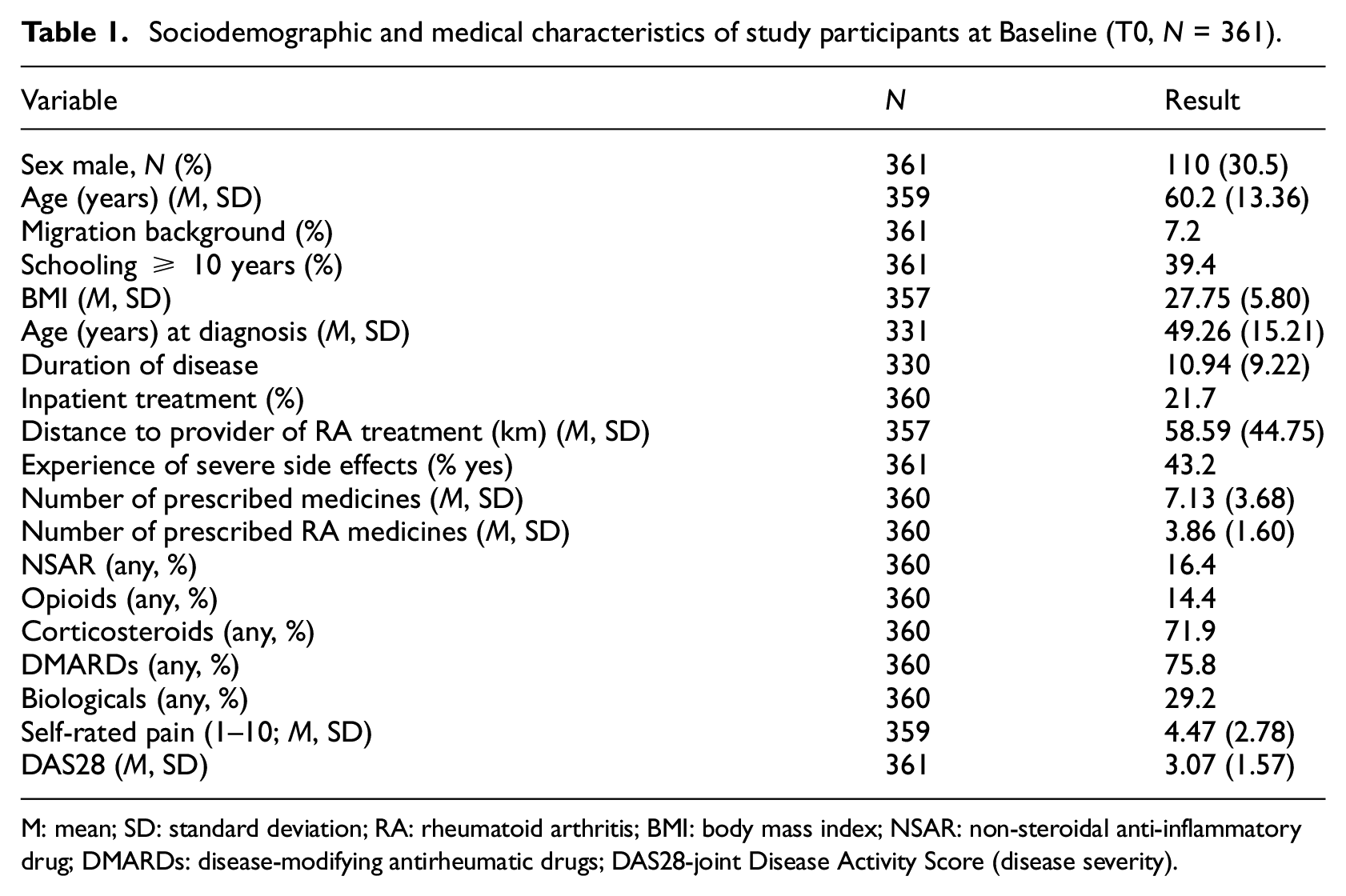
M: mean; SD: standard deviation; RA: rheumatoid arthritis; BMI: body mass index; NSAR: non-steroidal anti-inflammatory drug; DMARDs: disease-modifying antirheumatic drugs; DAS28-joint Disease Activity Score (disease severity).
Main outcomes
Descriptive results for BMQ, HADS Depression and MARS are presented in Table 2. Results are displayed for the complete sample as well as differentiated by adherence (adherent vs non-adherent). At all measurement points, 66%–68% of patients were non-adherent. Necessity beliefs, concerns and depression scores are also stable for the complete sample across measurement points (necessity: M = 4.2–4.3 [SD = 0.6–0.8]); concerns: M = 2.7–2.9 [SD = 0.8]; depression: M = 6.0–6.2 [SD = 3.8–4.0]). No group differences for necessity beliefs were found (all ps > 0.05). For concerns and depression, scores were significantly higher in non-adherent participants (Concerns: T0: t(341) = −3.71, p < 0.001, Cohen’s d = 0.43; T1: t(274) = −3.03, p < 0.01, Cohen’s d = 39; T2: t(236) = −2.58, p < 0.05, Cohen’s d = 0.36); Depression: T0: t(343) = −3.25, Cohen’s d = 0.38, p < 0.001; T1: t(279) = −3.65, p < 0.01, Cohen’s d = 0.47; T2: t(237) = −2.24, p < 0.05, Cohen’s d = 0.31).
Descriptive results of main variables: Beliefs about medicines, depression and adherence.
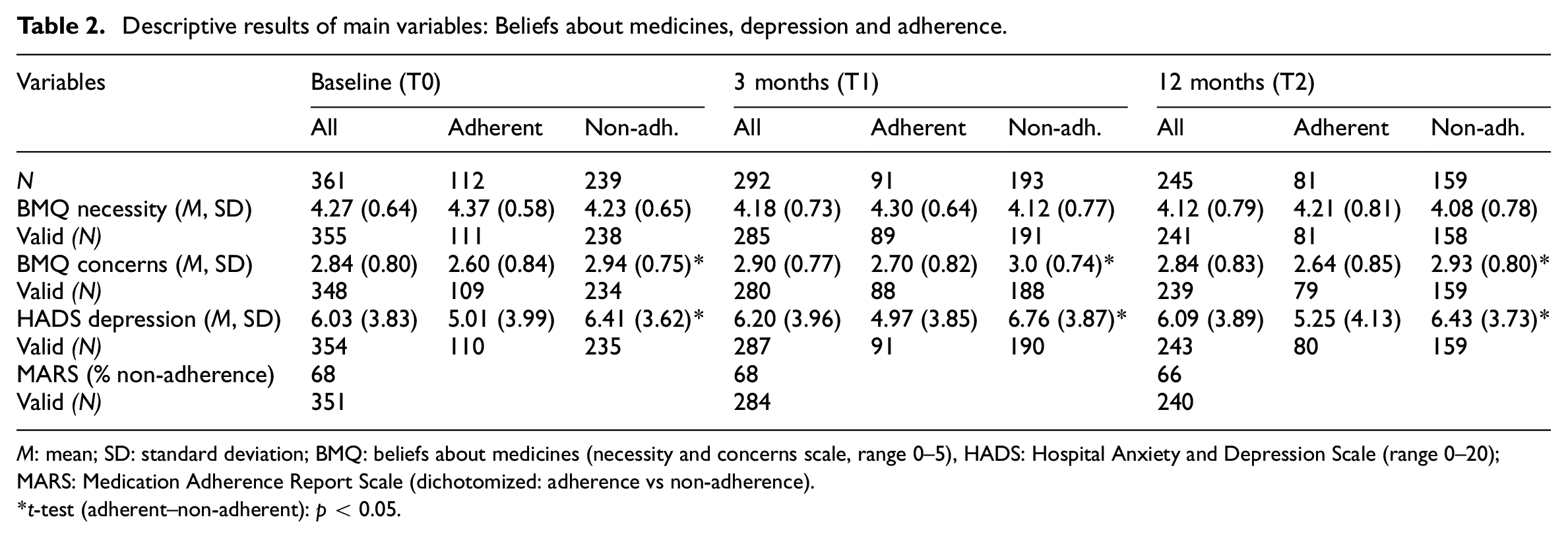
M: mean; SD: standard deviation; BMQ: beliefs about medicines (necessity and concerns scale, range 0–5), HADS: Hospital Anxiety and Depression Scale (range 0–20); MARS: Medication Adherence Report Scale (dichotomized: adherence vs non-adherence).
t-test (adherent–non-adherent): p < 0.05.
Moderation analyses
Table 3 shows the results for the moderation analyses (multivariate logistic regressions). Main effects were significant only for depression (HADS) at T1 (ORs = 0.9, ps ≤ 0.02), whereas no other main effects or interactions (depression × necessity/concerns) were significant (all ps > 0.15).
Moderation analysis of medication adherence on depression and necessity/concerns.
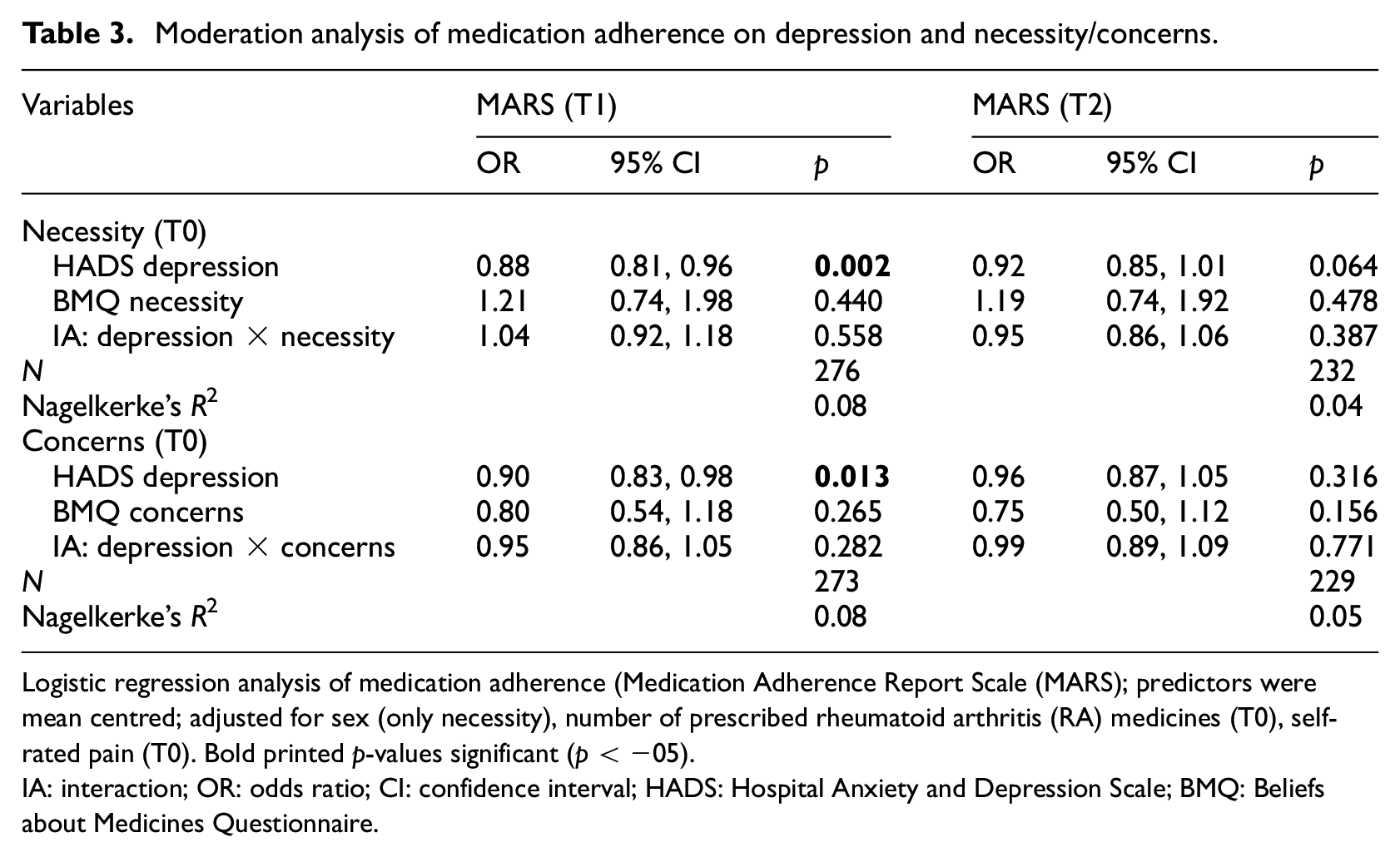
Logistic regression analysis of medication adherence (Medication Adherence Report Scale (MARS); predictors were mean centred; adjusted for sex (only necessity), number of prescribed rheumatoid arthritis (RA) medicines (T0), self-rated pain (T0). Bold printed p-values significant (p < −05).
IA: interaction; OR: odds ratio; CI: confidence interval; HADS: Hospital Anxiety and Depression Scale; BMQ: Beliefs about Medicines Questionnaire.
Reliability of BMQ measures and HADS depression from T0 to T1 is high (necessity: r = 0.758, p < 0.001; concern: r = 0.694, p < 0.001, HADS depression: r = 0.798, r < 0.001) and therefore no additional moderation analyses (BMQ, HADS depression T1 to MARS T2) were computed. Furthermore, the interaction term remains non-significant in all sensitivity analyses (all ps > 0.16).
Discussion
Key findings
We did not find a moderating role of depression for the association between beliefs about medicine and adherence behaviour in a sample of people with RA. Thus, the key finding of the cross-sectional moderation analysis conducted by Brandstetter et al. (2016) could not be replicated in a longitudinal approach utilizing the same cohort study sample.
Strengths and limitations
Main strengths of the present study include a well characterized cohort with little missing data and the prospective design, with a relatively low dropout rate (68% of patients at 1-year follow-up) and a corresponding longitudinal analyses of the relationship between beliefs and behaviour across measurement points. This approach is essential for validating findings from cross-sectional analyses and investigate causal assumptions. A further strength of the present study is the relatively representative socioeconomic (i.e. educational) status of the sample: 60% of sample reported to have 10 or less years of schooling, compared to 66% of the German general population (Bundeszentrale für politische Bildung, 2024). A representative sample with regard to SES is especially important since SES, or education respectively and medication use in RA patients are associated in (e.g. Russell et al., 2023).
One of the main limitations of the study is the use of self-report to assess adherence. Self-reporting of medication adherence can be biased, for instance due to recall bias or social desirability, which could lead to an overestimation of true adherence (Stirratt et al., 2015). In addition, the dichotomization of our adherence measure could result in more subtle influences remaining undetected (Pasma et al., 2013).
Interpretation, in relation to literature
The study by Brandstetter et al. (2016) was the first to examine the potential role of depression as a moderator within the ‘necessity-concerns’ framework. We followed up on their study, but with different results. Our non-significant findings may indicate that the moderating effect of depression may be more elusive than initially expected. To the best of our knowledge, no other studies have yet investigated this research question in patients with RA.
Conversely, there is a body of literature examining the direct influence of depression on non-adherence in RA patients. This literature predominantly indicates an association between depression and non-adherence (Chowdhury et al., 2022; Goh et al., 2017; Vangeli et al., 2015) For instance, in their systematic review of factors associated with non-adherence to treatment for immune-mediated inflammatory diseases, Vangeli et al. (2015) conclude that treatment concerns, necessity beliefs and depression are among the psychological factors with the strongest evidence for an impact on adherence. In this regard, it is noteworthy, that the only significant effects identified in our study were observed for depression predicting adherence at the 3-month follow-up. Consequently, depression may be modelled as a direct influence on adherence rather than a moderator (Chowdhury et al., 2022; Dagli et al., 2024; Vangeli et al., 2015). Moreover, recent studies suggest a bidirectional relationship between depression and rheumatoid arthritis (Lwin et al., 2020; Ng et al., 2022) highlighting a dynamic interplay between adherence and depression that encompasses both biological and psychological factors.
One potential explanation for the lack of significance in our findings is that empirical effect sizes are reduced to the longitudinal design, whereby the predictor and outcome variables are not measured at the same time. For instance, the ORs for the interaction effects are slightly lower in comparison to those reported by Brandstetter et al. (2016): ORs: 1.08–1.15 versus 0.95–1.04. In addition to this methodological issues, publication bias may also be a contributing factor in explaining the discrepancy between our findings and those of the majority of existing studies with regard to the main effects of necessity/concerns.
Furthermore, it is possible that the results are influenced by selective dropout. For example, patients with lower levels of adherence or higher scores on depression may be more likely to drop out. However, dropout analyses showed that there were no statistically significant differences between study sample and drop-out sample with regard to beliefs (necessity, concerns) and non-adherence at baseline (t-tests and chi-squared tests, all ps > 0.05). Also, no baseline difference was identified for the 3-month dropout sample in terms of depression (p > 0.05). However, at the 12-month mark, the dropout sample exhibited slightly elevated depression scores at baseline in comparison to the study sample (HADS depression = 6.8 vs 5.7, t = 2.4, p = 0.019). We then repeated the interaction analyses of Brandstetter et al. (2016) with only the subset of participants who remained at the 12-month follow-up (N = 245). In this analysis, the interaction term did not reach statistical significance (OR = 1.17, p = 0.057). This suggests that selective dropout of patients with higher depressive symptoms could contribute to the non-significant findings we observed in the long term.
Future research
Further prospective cohort studies are needed. These studies should ideally use more direct measures of adherence, in conjunction with self-report data. For example, measurement of blood drug levels or measurement methods based on regular, daily or event-based monitoring could be utilized, such as diaries or medication event monitoring systems (MEMS; Michaud et al., 2019). Other psychological comorbidities, such as anxiety, could also be investigated as potential moderators of the relationship between beliefs and adherence behaviour. Furthermore, the association between disease activity and adherence might also play a role in explaining adherence, as adherence impacts disease activity, and possibly vice versa (Hope et al., 2016; Kelly et al., 2020; Li et al., 2017).
As RA is a chronic disease, a cohort study of patients should be conducted over several years, ideally from the start of therapy. In this way, influences of factors such as comorbidities, treatment outcomes (e.g. remission), discontinuation or change of therapy, etc. can be studied in their interaction with changes in beliefs, and corresponding changes in behaviour can be evaluated together in their ‘true’ (long-term) dynamics. In this way, the actual impact of various potentially influential factors (such as depression) can be identified in a more realistic setting.
Conclusions
Contrary to previous research, we did not find evidence for a moderating role of depression in the association between beliefs about necessity or patients’ concerns and adherence behaviour in a longitudinal setting. Thus, possible moderating effects of depression might be less robust than previously thought and therefore harder to detect in longitudinal analyses. Further longitudinal studies are warranted to evaluate the robustness of cross-sectional findings, including different populations and settings.
Footnotes
Author contributions
Conceptualization: SB, HS, BE, MS, CA; Data curation: SB, BE, CA; Formal analysis: HS, CA, SB; Funding acquisition: CA; Investigation: SB, BE, MS, CA; Methodology: SB, HS, BE, MS, CA; Project administration: SB, CA; Resources and Software: HS, CA Supervision: CA, SB; Validation: SB, HS, BE, MS, CA; Visualization: HS; Writing – original draft: HS, CA; Writing – review & editing: SB, HS, BE, MS, CA.
Data sharing statement
The datasets used and/or analysed during the current study are available from CA on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study has been approved by the ethics committee of University of Regensburg (file-number: 12-101-0126).
Informed consent
Written informed consent to participate was obtained from 361 participants.
Consent for publication
All authors give consent for the manuscript to be published in its current form.
Declaration of generative AI in scientific writing
During the preparation of this work, the authors used ChatGPT and DeepL Write to improve the language and readability of their paper. After using these tools, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.