
Abstract
This study examined the experiences of stigmatising language among adults living with type 1 or type 2 diabetes in Ireland, and its associations with psychological outcomes using a cross-sectional design. Multiple regression analyses revealed significant associations between stigmatising language from family, friends, healthcare providers, the media and colleagues and higher anxious symptoms (β’s = 0.27–0.47, p’s < .001), depressive symptoms (β’s = 0.25–0.42, p’s ≤ 0.002), and diabetes distress (β’s = 0.34–0.57, p’s < 0.001). Lower diabetes treatment satisfaction was significantly associated with stigmatising language from healthcare providers (β = −0.47, p < 0.001). Additionally, there were no significant associations between wellbeing and stigmatising language from any source (p’s > 0.002). These findings emphasise the importance of respectful communication to enhance psychosocial outcomes for people living with diabetes.
Introduction
It is estimated that 537 million adults (aged 18–79 years) lived with diabetes in 2021, and the prevalence is expected to rise to 783 million by 2045 (Sun et al., 2021). In Ireland, it is estimated that over 260,000 people live with diabetes (Diabetes Ireland, 2023). Type 1 diabetes is an autoimmune disorder in which the immune system destroys insulin-producing beta cells in the pancreas, resulting in insulin deficiency (Roep et al., 2020), whereas type 2 diabetes, accounting for approximately 90% of all diabetes cases, develops when the body becomes resistant to insulin, impairing its effective use (Goodarzi, 2014). Individuals living with diabetes may face not only daily management challenges, such as regular glucose monitoring and dietary restrictions, but also potential stigma and mental health challenges (Guo et al., 2023; Kalra et al., 2018; Lin et al., 2020).
Diabetes stigma refers to negative attitudes and judgements about diabetes, often stemming from public misconceptions and stereotypes (Beverly et al., 2019; Speight and Holmes-Truscott, 2023). Approximately 80% of individuals with type 1 or type 2 diabetes face some level of stigma, and about 20% self-report discrimination because of their condition (Speight et al., 2024). Individuals who have experienced stigma report increased feelings of shame, guilt and social isolation (Inagaki et al., 2022; Liu et al., 2017). People living with diabetes have identified five main sources of diabetes stigma: media, healthcare providers, colleagues, family and friends (Browne et al., 2013b).
The language used when speaking to or about a person living with diabetes, whether in healthcare settings, the media or personal relationships, has the potential to propagate diabetes stigma (Beverly et al., 2022; Browne et al., 2013a). In the context of diabetes, stigmatising language encompasses the use of words, phrases, or expressions that reinforce negative stereotypes or prejudices against individuals or groups. The Diabetes ‘Language Matters’ movement is a response to this issue, advocating for a shift towards more respectful and empowering language when discussing diabetes or communicating with a person living with diabetes (Litterbach et al., 2024; Speight et al., 2021). The global movement has seen position statements released from diabetes associations worldwide (e.g. Diabetes Ireland, 2024; Speight et al., 2021). These position statements underscore the importance of language in influencing the thoughts, feelings and behaviours of individuals with diabetes, and recommend the use of language that is neutral, non-judgemental, and emphasises the person, not the condition. Evidence suggests that higher perceived quality of provider-patient communication is associated with better self-management, improved wellbeing, perceived self-efficacy and lower diabetes distress (Peimani et al., 2018).
Despite the growing body of Diabetes ‘Language Matters’ reports and position statements advocating for more sensitive communication (Dickinson et al., 2017), there is a knowledge gap in quantitative research related to the potential impact of stigmatising language in the context of diabetes, particularly with regards to language used by the media, colleagues, family and friends. While qualitative data suggests a link between stigmatising language and psychosocial wellbeing, quantitative research examining the relationship between diabetes-related stigmatising language from the media, social relationships and healthcare providers and an individual’s psychosocial health, is needed.
The present study aimed to investigate associations between the frequency of stigmatising language related to diabetes on psychosocial outcomes, including depressive and anxious symptoms, diabetes distress, satisfaction with diabetes treatment and wellbeing, among people living with type 1 or type 2 diabetes in Ireland. We hypothesised that there would be positive associations between the frequency of stigmatising language and (1) depressive symptoms; (2) anxious symptoms; and (3) diabetes distress; and that there would be negative associations between the frequency of stigmatising language and wellbeing and diabetes treatment satisfaction.
Methods
Sample
A cross-sectional online study was conducted. The criteria for inclusion in the study were self-reporting being over the age of 18 and under the age of 70, having type 1 or type 2 diabetes and residing in the Republic of Ireland. Participants were recruited through social media advertisements by a charity (Diabetes Ireland) and through a diabetes-specific Facebook group. The sample consisted of 148 (80.9%) participants who self-reported living with type 1 diabetes and 35 (19.1%) participants living with type 2 diabetes. Survey items, developed by researchers and in consultation with a group of people living with diabetes and a patient advocacy organisation, assessed the frequency of diabetes-related stigmatising language encountered by participants across various settings. Diabetes-specific data and psychosocial data were collected using various questions and measures (described below). Ethical approval for the study was granted by the University College Dublin Taught Masters Research Ethics Committee – Psychology.
Measures and materials
Sociodemographic characteristics
Self-reported sociodemographic data collected in the survey included gender, age, marital status, employment status, ethnicity and education level. Diabetes-specific characteristics were also collected including type of diabetes and age of diagnosis (see Supplemental Table 1).
Diabetes-related stigmatising language
Respondents were asked to indicate how often in the past month they had encountered language considered to be stigmatising by (1) the media, (2) family, (3) friends, (4) colleagues and (5) healthcare providers on a 5-point Likert scale from 0 (never) to 4 (very often). These categories were selected as previous literature identifies them as five sources of potential stigma (Browne et al., 2013b).
Depressive symptomatology
To assess the severity of depressive symptoms, the Patient Health Questionnaire-9 (PHQ-9) was administered (Kroenke et al., 2001). The PHQ-9, a widely used tool in diabetes research, was administered to assess depressive symptoms (Nouwen et al., 2021). Participants indicate the frequency of each symptom over the past 2 weeks on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The total score is obtained by summing the scores for all nine items, resulting in a range from 0 to 27. The PHQ-9 demonstrated a high internal consistency (α = 0.90) in this sample.
Anxious symptomatology
The Generalised Anxiety Disorder Assessment (GAD-7) measured generalised anxiety symptom severity among participants (Spitzer et al., 2006). The GAD-7 is a widely used, validated tool comprising seven items that evaluate the frequency of anxious symptoms experienced over the past 2 weeks. Participants rate each item on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). The total score is calculated by summing the scores for the seven items, resulting in a score ranging from 0 to 21. The GAD-7 demonstrated high internal consistency (α = 0.92) in this sample.
Diabetes distress
The Problem Areas in Diabetes (PAID-11) scale assessed diabetes-related distress (Stanulewicz et al., 2019). The PAID-11 is a validated and psychometrically robust shorter version of the PAID-20 questionnaire, designed to measure emotional distress related to living with diabetes. Respondents indicate the degree to which each of the 11 items is currently a problem for them, on a scale from 0 (not a problem) to 4 (serious problem). The scores for each item are summed to generate a total score. The PAID-11 scale demonstrated high internal consistency (α = 0.94) in this sample.
Wellbeing
To assess overall psychological wellbeing, the WHO-5 Wellbeing Index was administered (Bech, 2004). The scale consists of five items that assess positive mood, vitality and general interest over the past 2 weeks. Participants rate each item on a 6-point Likert scale ranging from 0 (not present) to 5 (constantly present). The total raw score ranges from 0 to 25, which is then multiplied by 4 to produce a final score ranging from 0 to 100, with higher scores indicating better wellbeing. The WHO-5 scale demonstrated high internal consistency (α = 0.89) in this sample.
Diabetes treatment satisfaction
The Diabetes Treatment Satisfaction Questionnaire (DTSQs) was administered to assess respondent satisfaction with their current diabetes treatment over the past few weeks (Bradley, 2013). The DTSQ consists of eight items, each rated on a Likert scale from 1 to 7, summed to create a total score ranging from 8 to 56. A higher score is indicative of higher diabetes treatment satisfaction. The items address various aspects of treatment satisfaction, including overall satisfaction, perceptions of blood glucose management, convenience and flexibility of the treatment, understanding of diabetes, willingness to recommend the treatment, and satisfaction with continuing the current treatment. The DTSQ scale demonstrated moderate internal consistency (α = 0.74) in this sample.
Diabetes stigma
Diabetes stigma was assessed using the Type 1 or the Type 2 Diabetes Stigma Assessment Scales (DSAS-1 and DSAS-2, respectively). Both are 19-item self-report measures designed to assess stigma related to living with diabetes, each focusing on either type 1 or type 2 diabetes (Browne et al., 2016, 2017). Each scale consists of three subscales: Treated Differently, Blame and Judgement, and Identity Concerns. Participants respond to statements on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). A total score is calculated by summing the responses to all 19 items, with scores ranging from 19 to 95. Higher scores indicate higher levels of stigma related to type 1 or type 2 diabetes. The DSAS-1 and DSAS-2 demonstrated very high internal consistency in this sample, with Cronbach’s alpha values of 0.95 and 0.93, respectively.
Experiences of diabetes-related stigmatising language
To gain a deeper understanding of participants’ experiences with stigmatising language, open-ended survey questions were also included. The questions included (1) What impact did your most recent healthcare appointment language have on you or your experience? (2) What words or phrases do you consider to be stigmatising, hurtful, or frustrating about diabetes? (3) What words or phrases do you prefer in reference to diabetes? Content analysis was conducted using an inductive approach to identify patterns and themes emerging from participants’ responses.
Analysis
Descriptive and frequency statistics were calculated to examine the bivariate associations between the predictor variables; the frequency of stigmatising language from the media, family, friends, colleagues and healthcare providers and outcome variables; diabetes stigma, diabetes distress, depressive and anxious symptoms, wellbeing, and diabetes treatment satisfaction. Multiple linear regression analyses were conducted to examine the associations between the frequency of stigmatising language from (1) the media, (2) family, (3) friends, (4) colleagues and (5) healthcare providers, and psychosocial outcomes variables with adjustments for ethnicity, gender, and education. Exploratory regression analyses examining Diabetes Stigma Assessment Scale (DSAS) scores as a predictor of psychosocial outcomes are provided in the Supplemental Materials (see Supplemental Material A).
Although multicollinearity diagnostics (e.g. VIF and tolerance) indicated no severe collinearity, inspection of full models revealed a high degree of shared variance (R2 > 0.28) without significant individual predictors, suggesting suppression effects. Following guidance from O’Brien (2007) and Dormann et al. (2012), we therefore analysed predictors separately to isolate their unique associations with psychosocial outcomes. Therefore, this study consisted of 25 planned analyses, as there were five predictor, and five outcome variables examined separately. As such, to minimise the risk of type I error, an alpha level of 0.002 was used to determine statistical significance (0.05/25). Finally, content analyses of free-text responses to open-ended questions were conducted using the software package NVivo (Release 1.7.2). Missing data were handled using pairwise deletion.
Results
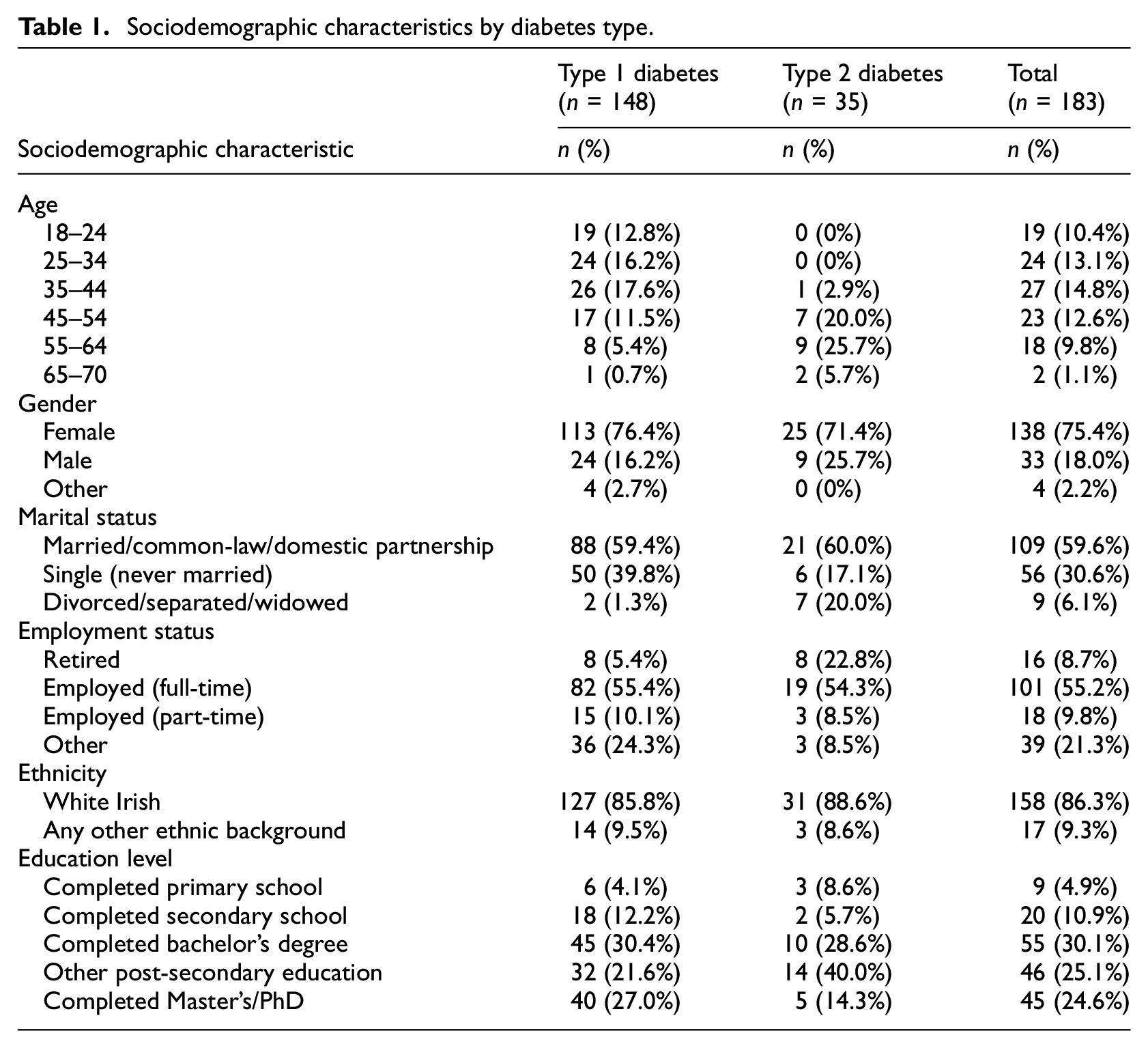
The sample consisted of 183 participants, with 80.9% living with type 1 diabetes and 19.1% living with type 2 diabetes. Most participants were female (75.4%), White Irish (86.3%), and employed full-time (55.2%). Participants ranged in age from 18 to 70 years (see Table 1). Bivariate correlations and means (SD) of each predictor and outcome variable are presented in Table 2. The results of the multiple linear regression models are presented in a summary table (Table 3). The frequencies of encounters with stigmatising language from each source are reported in Table 4.
Sociodemographic characteristics by diabetes type.
Bivariate associations of frequency of stigmatising language using Pearson’s correlation (R).
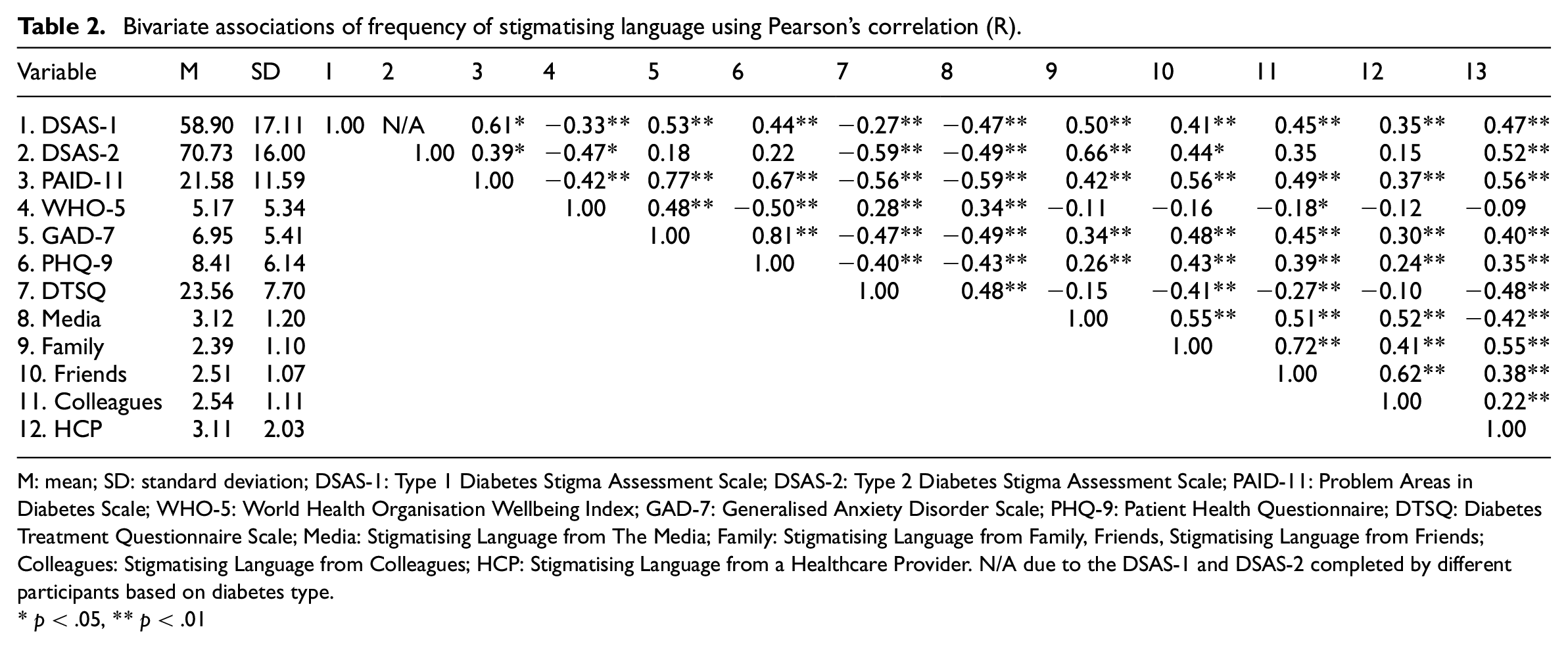
M: mean; SD: standard deviation; DSAS-1: Type 1 Diabetes Stigma Assessment Scale; DSAS-2: Type 2 Diabetes Stigma Assessment Scale; PAID-11: Problem Areas in Diabetes Scale; WHO-5: World Health Organisation Wellbeing Index; GAD-7: Generalised Anxiety Disorder Scale; PHQ-9: Patient Health Questionnaire; DTSQ: Diabetes Treatment Questionnaire Scale; Media: Stigmatising Language from The Media; Family: Stigmatising Language from Family, Friends, Stigmatising Language from Friends; Colleagues: Stigmatising Language from Colleagues; HCP: Stigmatising Language from a Healthcare Provider. N/A due to the DSAS-1 and DSAS-2 completed by different participants based on diabetes type.
p < .05, **p < .01
Summary of individual multiple regression analyses testing the associations between the frequency of stigmatising language and psychosocial outcomes.
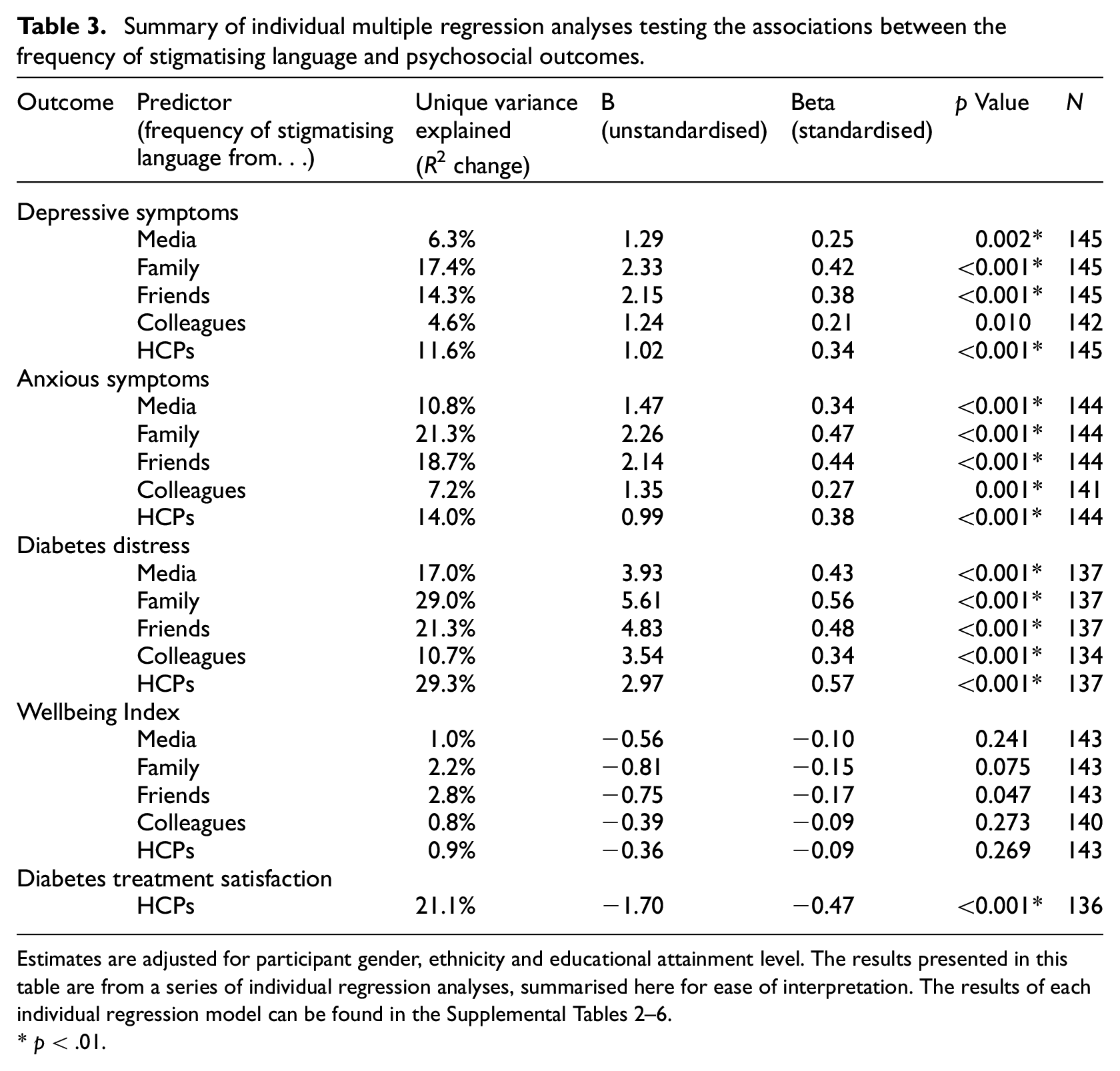
Estimates are adjusted for participant gender, ethnicity and educational attainment level. The results presented in this table are from a series of individual regression analyses, summarised here for ease of interpretation. The results of each individual regression model can be found in the Supplemental Tables 2–6.
p < .01.
Frequency of stigmatising language.
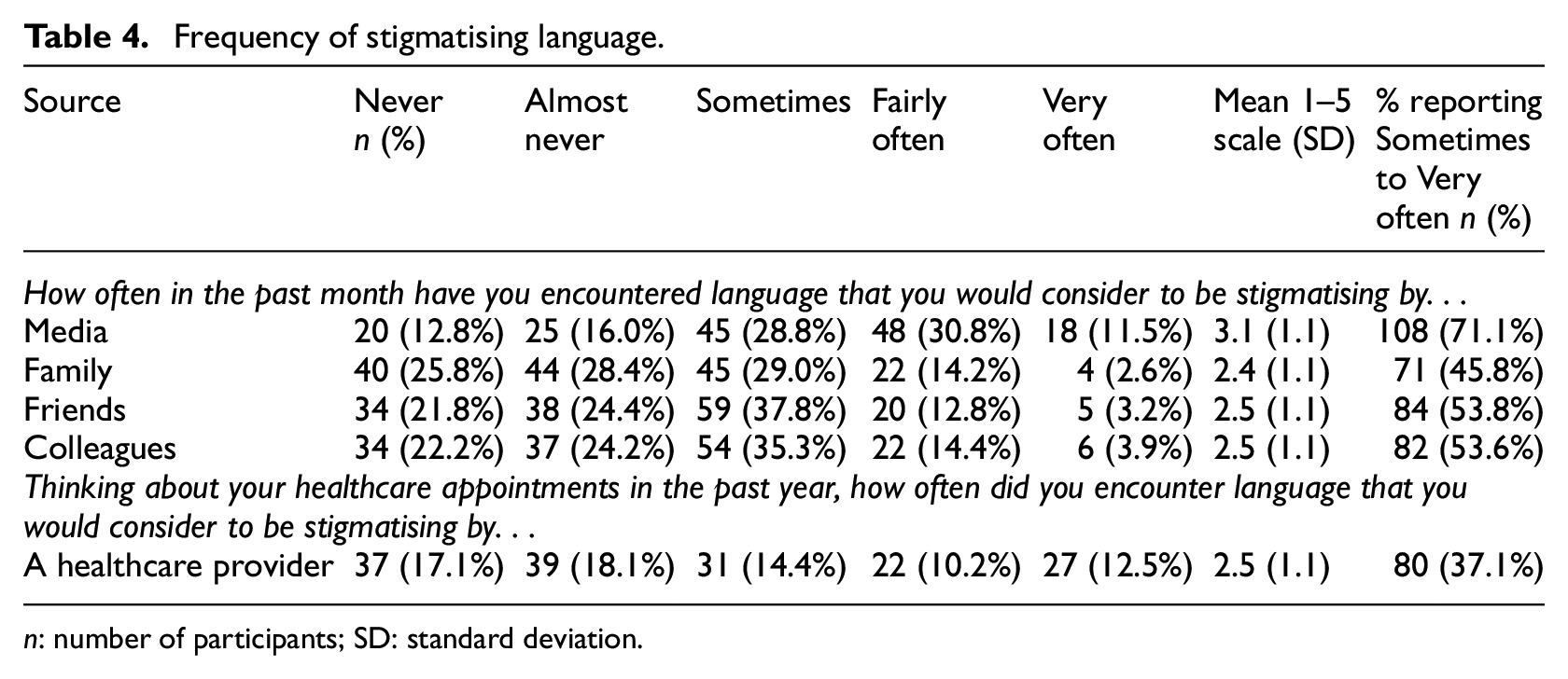
n: number of participants; SD: standard deviation.
Depressive symptomatology
The regression models revealed a significant positive association (p’s < 0.002) between the frequency of stigmatising language from family, friends, colleagues and healthcare providers and elevated depressive symptomatology, with moderate effect sizes. Stigmatising language encountered from family was the strongest predictor, accounting for 17.4% of the variance in depressive symptomatology (β = 0.42, p < 0.001). Stigmatising language from friends accounted for 14.3% of the unique variance (β = 0.38, p < 0.001). Healthcare providers’ stigmatising language explained 11.6% of the unique variance (β = 0.34, p < 0.001). Stigmatising language experiences through the media accounted for 6.3% of the unique variance (β = 0.25, p = 0.002). However, the association between frequency of stigmatising language from colleagues (
Anxious symptomatology
Moderate significant positive associations (p’s < 0.002) were found between the frequency of stigmatising language from media, family, friends, colleagues and healthcare providers with elevated anxious symptomatology. Stigmatising language encountered from family was the strongest predictor, uniquely accounting for 21.3% of the variance in anxious symptomatology (β = 0.47, p < 0.001) after adjusting for sociodemographic covariates. Stigmatising language from friends accounted for 18.7% of the variance (β = 0.44, p < 0.001); stigmatising language from healthcare providers explained 14.0% of the unique variance (β = 0.38, p < 0.001); stigmatising language from the media accounted for 10.8% of the variance (β = 0.34, p < 0.001) and stigmatising language from colleagues explained 7.2% of the variance in anxious symptomatology (β = 0.27, p = 0.001).
Diabetes distress
Significant positive associations were found between the frequency of stigmatising language and diabetes distress. Stigmatising language encountered from family was the strongest predictor, accounting for 29.0% of the unique variance in diabetes distress (β = 0.56, p < 0.001). Stigmatising language from friends accounted for 21.3% of the variance (β = 0.48, p < 0.001). Healthcare providers’ stigmatising language explained 29.3% of the variance (β = 0.57, p < 0.001). Stigmatising language through the media accounted for 17.0% of the variance (β = 0.43, p < 0.001). Colleagues’ stigmatising language explained 10.7% of the variance in diabetes distress (β = 0.34, p < 0.001).
Wellbeing
No significant associations were found between the frequency of stigmatising language and wellbeing across all sources (media, family, friends, colleagues, and healthcare providers; Table 3).
Diabetes treatment satisfaction
We found a significant negative association of medium magnitude between the frequency of stigmatising language from healthcare providers with diabetes treatment satisfaction, after controlling for gender, ethnicity and education levels. Stigmatising language from healthcare providers’ explained 21.1% of the variance in diabetes treatment satisfaction (β = −0.47, p < 0.001).
All findings remained consistent when diabetes type was included as a covariate in the model, suggesting that the overall pattern and interpretation of results were not meaningfully altered after adjusting for diabetes type.
Content analysis of open-ended responses
Table 5 describes example responses from each of the three open-ended questions asked during the survey.
Quotes from participants on their perceived impact of diabetes-related language.
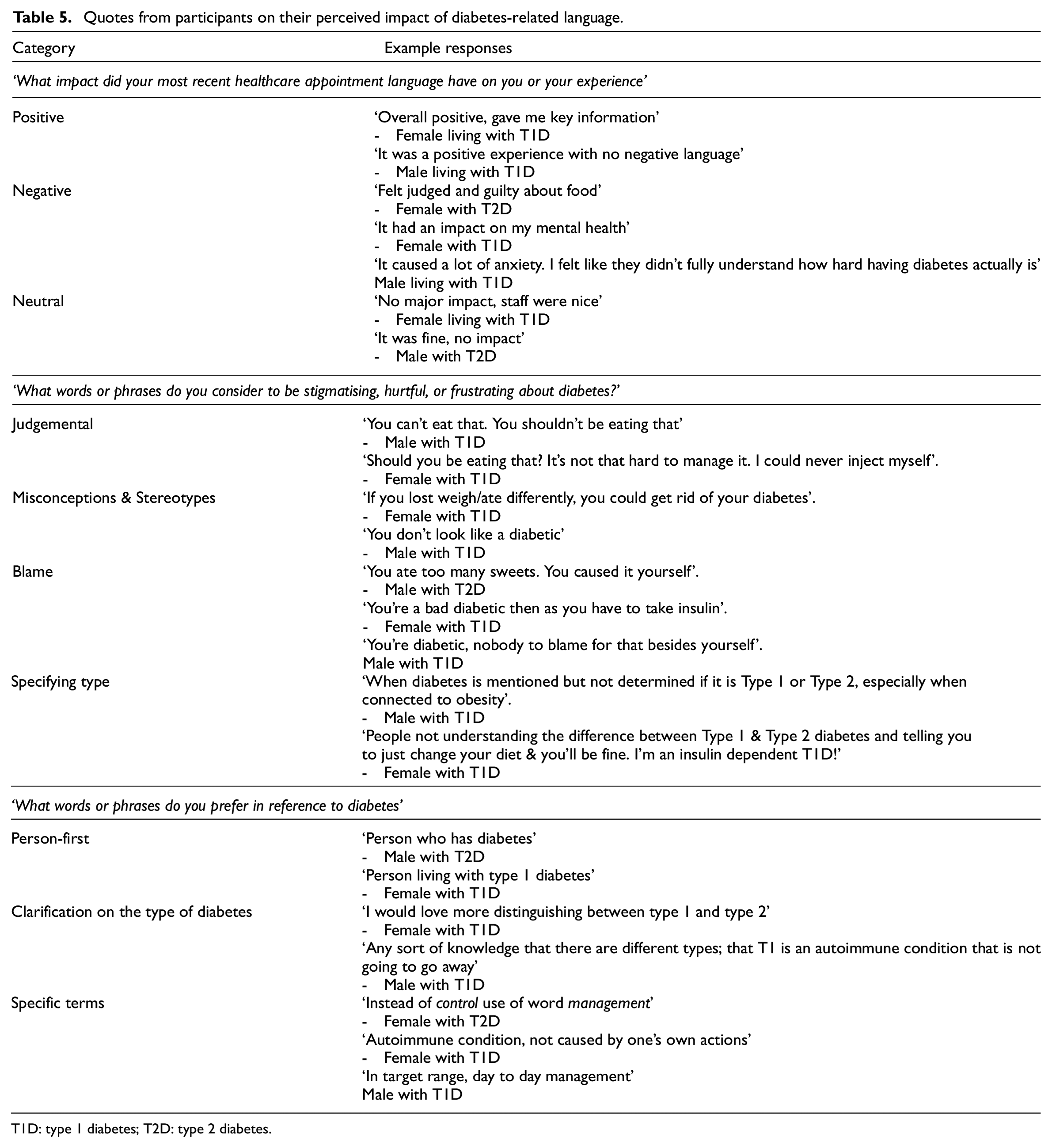
T1D: type 1 diabetes; T2D: type 2 diabetes.
Impact of recent healthcare appointment language
A content analysis of free text responses to an open-ended question asking ‘What impact did your most recent healthcare appointment language have on you or your experience’ was conducted by categorising responses as either positive, negative, or neutral. A total of 106 participants (58% of total sample) responded to the question, with 68% (n = 72) living type 1 diabetes and 32% (n = 34) of respondents living with type 2 diabetes. Fifty-four percent (54%; n = 57) of participants reported experiencing negative impacts from the language used during their last healthcare appointment. Some of the negative responses mentioned heightened anxiety and stress following exposure to language at a recent healthcare appointment, and many individuals (17%) described feeling judged or guilty because of the language used by their healthcare providers. On the other hand, 24 respondents (23%) described the language used in their appointment as positive and informative, suggesting that language choice can be perceived as constructive. A neutral experience was reported by 25 respondents (24%).
Words or phrases considered to be stigmatising
A total of 95 participants responded to the question ‘What words or phrases do you consider to be stigmatising, hurtful, or frustrating about diabetes?’, with 67% (n = 64) of respondents living with type 1 diabetes and 33% (n = 31) living with type 2 diabetes. Nineteen participants (20%) reported they often experienced confusion between the different types of diabetes and prefer when the full name of the condition is used. Additionally, 46 participants (48%) referred to comments insinuating blame or judgement on the individual with diabetes, with specific references to jokes about diabetes and misinformation being particularly hurtful and frustrating. Ten participants (10%) felt neutral about the language used, and 35 individuals (37%) specifically reported disliking the terms ‘control’, ‘diabetic’, and ‘non-compliant’.
Preferred language in reference to Diabetes
When asked, ‘What words or phrases do you prefer in reference to diabetes?’, 111 participants responded (69% (n = 77) with type 1 diabetes; 31% (n = 34) with type 2 diabetes). Twenty-four participants (21.6%) highlighted the importance of using person-first terminology and 35 (31.5%) wrote that they prefer when individuals clarify the type of diabetes when referring to someone with the condition. These respondents advocated for terms like ‘management’ instead of ‘control’. Additionally, 32 participants (29%) expressed a preference for non-judgemental and informed language, emphasising the value of genuine curiosity and understanding. They also indicated that jokes about diabetes are often offensive. Nine respondents (8%) were neutral, indicating that the language used to discuss their diabetes did not significantly affect them.
Discussion
This study examined the associations between the frequency of diabetes-related stigmatising language and psychosocial outcomes among adults living with type 1 and type 2 diabetes in Ireland. Greater exposure to stigmatising language, particularly from family members, healthcare providers and friends, was associated with higher levels of diabetes distress, depressive symptoms, and anxious symptoms, with moderate effect sizes. Similarly, stigmatising language from healthcare providers was significantly associated with decreased diabetes treatment satisfaction. There were no significant associations between the frequency of stigmatising language and wellbeing. We also found positive correlations between diabetes stigma and several psychosocial outcomes, including depressive symptoms, anxious symptoms and diabetes distress, as well as a negative association with diabetes treatment satisfaction. Open-ended responses suggested that participants frequently reported feeling judged and blamed due to the language used by healthcare providers, family members and friends. Many participants also expressed a preference for more person-centred, non-judgemental language that acknowledges the differences between types of diabetes.
Frequency of stigmatising language and psychological outcomes
Stigmatising language from family members showed strong associations across psychological outcomes, accounting for up to 29% of the variance in diabetes distress. These findings align with prior research that emphasises the potential role of family members in perpetuating stigma and the significant influence family dynamics may have on the mental health of individuals with chronic illnesses (Adu et al., 2022; Aldersey and Whitley, 2014). Studies have demonstrated that negative comments and discrimination from family can undermine self-esteem and exacerbate feelings of shame and guilt, which are particularly impactful due to the close nature of these relationships (Major and O’Brien, 2005). Furthermore, we found a similar association for friends and colleagues, where more frequent exposure to stigmatising language was positively associated with more elevated depressive symptoms, anxious symptoms, and diabetes distress, with small to moderate effect sizes.
Stigmatising language from healthcare providers was significantly associated with elevated levels of diabetes distress, and depressive and anxious symptoms. These findings are congruent with the qualitative work of Beverly et al. (2022) and Dickinson (2018), who found that diabetes-related stigmatising language is prevalent in healthcare settings and can lead to feelings of judgement, blame and shame, thereby adversely affecting mental health and treatment regimens. Our results are in line with the broader literature on the impact of stigmatising language in healthcare, which demonstrates that respectful, person-first language is crucial for fostering positive healthcare experiences and outcomes (Lloyd et al., 2018; Speight et al., 2021).
The significant association between the frequency of stigmatising language from the media and elevated levels of diabetes distress, depressive symptoms and anxious symptoms may be understood through the pervasive influence of media on public perceptions and self-image (Blackwood et al., 2022). Media representations can reinforce negative stereotypes and misconceptions about diabetes (Hunt et al., 2022), which are associated with feelings of shame, guilt and worthlessness, which in turn may lead to increased psychological distress. Previous empirical research has demonstrated that negative media messages about diabetes can contribute to misconceptions and lower perceived seriousness of the condition (Holmes-Truscott et al., 2024). This may lead to lower motivation for general health behaviours and greater diabetes-related distress, which correlates with negative mental health outcomes. Our findings support the notion that stigmatising language and negative media portrayals is related to individuals’ mental health, potentially by reinforcing harmful stereotypes and diminishing the seriousness of diabetes in the public eye.
Interestingly, our analysis did not find frequency of stigmatising language to be significantly associated with lower wellbeing. This finding may reflect the notion that negative mental health outcomes, such as depression and anxiety, are conceptually and empirically distinct from positive dimensions of mental health, like happiness and life satisfaction. As such, stigmatising language may be more strongly associated with negative mental health outcomes without necessarily being associated with positive aspects of wellbeing. It is also possible that the wellbeing measure used in this study was not sensitive enough to detect associations between language exposure and positive mental health. Future research should explore this further using different measures of wellbeing to capture the potentially nuanced relationship between language and mental health and wellbeing.
Diabetes treatment satisfaction
Our study also found negative associations between the frequency of stigmatising language from healthcare providers and diabetes treatment satisfaction. Stigmatising language from healthcare providers accounted for 21.1% of the variance in treatment satisfaction, highlighting the important role of provider-patient communication. These findings align with existing literature that emphasises the importance of respectful and supportive communication in healthcare settings (Peimani et al., 2018; Riedl and Schüßler, 2017). Enhanced physician-patient communication skills have been linked with improved health outcomes, including increased treatment satisfaction and improved diabetes self-management practice (Riedl and Schüßler, 2017). As such, implementing language sensitivity training for healthcare providers, perhaps embedded into educational curriculums, could be a vital step towards improving diabetes care and patient outcomes.
Experiences of stigmatising language
In open-ended text responses, participants reported positive and negative impacts of language used during healthcare appointments. This dichotomy reflects findings from previous qualitative research, emphasising the significant role that both positive and negative communication plays in healthcare experiences (Beverly et al., 2022; Dickinson, 2018). Notably, over half of the respondents reported negative impacts from stigmatising language used by healthcare providers, which often led to feelings of judgement, guilt, anxiety, and stress. This is consistent with the literature indicating that negative interactions with healthcare providers can exacerbate psychological distress in individuals with chronic illnesses (Peimani et al., 2018; Riedl and Schüßler, 2017). Positive experiences were also noted by just less than a quarter of the participants, underscoring the potential for constructive language to foster a supportive environment and improve patient outcomes.
Participants in the study identified specific words and phrases they found stigmatising. Many expressed dissatisfactions with the lack of distinction between the types of diabetes and indicated that comments insinuating blame were particularly hurtful. This aligns with previous literature indicating that non-specific references to diabetes can perpetuate stereotypes and misinformation, contributing to feelings of frustration and stigmatisation among individuals with diabetes (Dickinson et al., 2017). The preference for person-centred terminology and clarification of diabetes type highlights the importance of precise and respectful language in reducing stigma and improving communication. Although people may vary in their preference for person-first versus illness-first language, the majority preference for person-first language in diabetes is supported by qualitative studies advocating for the use of person-first language to promote dignity and respect in healthcare settings (Dickinson et al., 2017).
Strengths and limitations
The present study provides unique quantitative evidence of the associations between stigmatising language and various psychosocial outcomes in individuals with diabetes in Ireland. The integration of quantitative data with opportunities to expand qualitatively on stigmatising experiences provides a comprehensive understanding of the issue. However, several limitations should be noted. First, the cross-sectional design of this study allowed observations of potential relationships and associations, but it limits causal inferences. Future research could explore longitudinal designs to provide a deeper insight into the direction of relationships. Secondly, our sample did not reflect the population of people with diabetes in Ireland, particularly with a lower number of participants with type 2 diabetes compared to type 1 diabetes (148 participants with type 1 diabetes and 35 participants with type 2). This imbalance likely reflects a broader pattern of underrepresentation of people with type 2 diabetes in online research, potentially due to digital exclusion, lower community engagement or the impact of stigma (Browne et al., 2013b; Choi et al., 2014; Herrero et al., 2020; Jordan et al., 2025). The age spread across diabetes might also not be well reflected in our sample. Furthermore, other types of diabetes were not reflected in the study such as gestational diabetes. The low sample size of participants with type 2 diabetes prevented stratification of analyses by diabetes type and therefore, impacts generalisability of the results. Thirdly, there was a significant gender imbalance in the sample, with more female participants than male participants (138 females, 33 males and 4 non-binary participants). This gender bias could influence the generalisability of the results, as previous research has highlighted experiences of stigma may differ between genders (Kato et al., 2019). Finally, some participants responded to the open-ended questions on language by referring more broadly to their health experiences, and may not have referred to language specifically. Therefore, the content analysis results should be interpreted in light of this. Future research should aim to balance the representation of participants to reflect the general population trends by age, gender and diabetes type, to ensure the findings are generalisable to the true population of people living with diabetes in Ireland, with stratified analyses conducted.
Conclusions
The results of this study demonstrate the associations between stigmatising and psychological distress. It suggests a need for promoting positive and non-judgemental communication focused on the individual rather than the condition. In particular, our findings suggest that the role of family and friends may be an important one for supporting individuals with diabetes. While social support is important for managing diabetes, the use of stigmatising language by close social circles can undermine this support, leading to increased feelings of isolation and decreased motivation to engage in the recommended diabetes self-management practices (Browne et al., 2013b; Schabert et al., 2013). Therefore, educational interventions targeting family members and friends may be beneficial to improve their understanding of diabetes and the potential impact of their language on individuals’ mental health. Additionally, our findings highlight stigmatising language from healthcare providers is also significantly associated with negative psychosocial outcomes. This supports previous literature emphasising the importance of person-first language and respectful communication in healthcare (Peimani et al., 2018; Riedl and Schüßler, 2017), and reflects the need for language sensitivity training for healthcare providers. This implication echoes previous literature calling for increased language awareness around a multitude of chronic conditions (Volkow et al., 2021; Waters et al., 2023).
In conclusion, addressing stigmatising language in healthcare, media, and social contexts could help reduce the psychological burden of diabetes and enhance the quality of life of those affected, though future interventional research is needed. Fostering a more respectful and supportive communication environment may help improve psychosocial and overall health outcomes for people living with type 1 and type 2 diabetes. This work supports the ongoing efforts of the Diabetes ‘Language Matters’ movement and aligns with existing research into diabetes-related stigmatising language, emphasising the need for continued advocacy and education to combat stigma in all its forms.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251341796 – Supplemental material for Stigmatising language and its association with psychological outcomes among people living with type 1 or type 2 diabetes
Supplemental material, sj-docx-1-hpq-10.1177_13591053251341796 for Stigmatising language and its association with psychological outcomes among people living with type 1 or type 2 diabetes by Méabh Finnegan, Ellie Patterson, Eimear C Morrissey, Michelle Lowry, Tomás P Griffin, Ann-Marie Creaven and Sonya S Deschênes in Journal of Health Psychology
Footnotes
Acknowledgements
The authors wish to thank all the study participants for their time in completing the survey. We are also grateful for the support of the Irish Diabetes Language Matters working group, Diabetes Ireland and Thriveabetes, especially for their help in reviewing the survey items and assisting with recruitment.
Data sharing statement
Requests for data access can be sent to the Corresponding Author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study received funding from the University College Dublin Ad Astra Start-Up grant (PI Deschenes).
Ethics approval
The study received ethical approval from the University College Dublin Taught Masters Research Ethics Committee - Psychology.
Informed consent
All participants provided informed consent prior to study participation.
Consent to participate
All participants provided informed consent prior to study participation.
Consent to publication
All participants provided consent to have their data analysed and anonymously presented within academic publications.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.