
Abstract
Systemic family interventions of Latino families with a cancer patient have been suggested as effective and necessary, but few studies have focused on evaluating systemic functioning to design culturally relevant interventions. The purpose of study was to assess systemic functioning in Puerto Rican families with a cancer patient using the Spanish translated version of the Family Genogram Interview (FGI) that measures Bowen’s four emotional processes in nuclear family and family of origin. Fifty-one Puerto Rican participants related to a cancer patient were interviewed. Results suggested an acceptable reliability for the FGI-Spanish and higher presence of symptoms in a spouse or partner, symptoms in family of origin, focus on a child and emotional cutoff in family of origin. Qualitative findings suggested that main concerns for participants were related to family changes surrounding illness and familial roles, consistent with Bowen’s theory and clinical implications for designing systemic interventions for Puerto Rican families.
Cancer is the second most common cause of death in the United States (American Cancer Society, 2022) and a leading cause of death in Puerto Rico (Torres-Cintron et al., 2023). The number of Puerto Ricans living with cancer from 2016 to 2020 was estimated to be 71,769 persons (Torres-Cintron et al., 2023). Puerto Ricans are part of marginalized communities that are impacted by health disparities, such as lifestyles, health behaviors and access to care (Simmons et al., 2011). Not much is known about cancer health services in Puerto Rico, including effective psychosocial interventions that can mitigate these health disparities.
Psychosocial effects of cancer include depression, anxiety, deteriorating marital satisfaction, sexual complications, body image problems, cognitive decline, and even post-traumatic stress reactions, among others (Hodgson et al., 2011). In children, parental cancer can increase the risk for developing behavioral and emotional problems (Inhestern et al., 2016). Among the psychological dimensions associated with patients and their families is adjustment to the disease of the cancer patient (Romero and Cruzado, 2016). Family, as a whole, experiences cancer (Hodgson et al., 2011). Family is both a stressor for the cancer patient, as well as his/her first line of support and is also gravely impacted by cancer (Hodgson et al., 2011; Lewis, 2010; Sherman and Simonton, 1999). Cancer is a family illness, not a patient’s disease (Lewis, 2010).
Responses to cancer are shaped by the cultural, economic, and political contexts in which families are embedded, but few researchers have focused on the role of cultural factors in family adjustment to cancer (Llave et al., 2024). Marginalized communities, including Latino families are also affected by social determinants of health. Latino families experience significant health disparities, such as increased poverty rate in comparison with non-Hispanic whites and barriers to access better treatment due to lack of health insurance and language (American Cancer Society, 2021).
Family interventions with cancer patients
Psychosocial interventions have been proven effective with cancer patients and their families (Hodgson et al., 2012; Inhestern, et al., 2016; Llave et al., 2024; Lövgren et al., 2022; Shields et al., 2012). In a review of Randomized Control Trials (RCTs) of family interventions with health problems conducted by Shields et al. (2012), slightly more than half of the studies suggested positive results for couple or spouse interventions versus individual interventions. Despite this, among efforts to design and test psychosocial interventions for patients with cancer and their families, family therapy has largely not been included (Hodgson et al., 2011; Niemela et al., 2016). Most interventions which have been designated as family-based or family-centered, but they are designed for individuals, couples, or are group-based interventions for family members of patients with cancer (Hodgson et al., 2011).
Most studies about family interventions have been conducted with non-Hispanic White middle-class families and have not been tailored to the culturally diverse patient populations in the USA (Davey et al., 2013). A systematic review conducted by Guan et al. (2023), identified five effective psychosocial interventions intended for Latino families conducted in the U.S. and Brazil. All interventions included culture, by either including cultural values and beliefs and adapted to their populations and proved to be effective. One limitation of the studies was that outcomes were at the individual level, versus dyadic or at the healthcare systems levels (Guan et al., 2023).
Theoretical frameworks of family interventions
Family functioning with cancer patients has been conceptualized differently among studies. Researchers define behavioral reactions to cancer, or as adjustment, adaptation or reorganization of the family. Most conceptualization stems from a systems theory perspective (Lewis, 2010; Sherman and Simonton, 1999; Steinglass et al., 2011). Theoretical common lines among models emphasize a restructuring of the family following a diagnosis, treatment and survivorship of cancer.
Systemic perspectives focus on family’s structural and functional changes and life cycle transitions when a serious, chronic or terminal illness is involved. They also emphasize communication patterns, contextual aspects and family narratives. Adaptation to cancer is a dynamic process, affected by family structure, life-cycle tasks, and family schemata and where some families may be most vulnerable or more resilient to distress. Lewis (2010) characterizes cancer not as a single stressor event for families but as a series of multiple, interwoven, and layered psychosocial transitions. A family experiencing cancer attempts to reconfigure itself around the cancer and, in the process, there is destabilization, even in high resource and well-adjusted households. This destabilization occurs in both patient–spouse dyads and in the parent–child dyad and goes through “stuck points” or cross-cutting issues on which families get “stuck,” and with which they struggle, often with few or no resources (Lewis, 2010).
Bowen’s family systems theory
One of the main systems family theoretical frameworks is Murray Bowen’s. From Bowen’s perspective family system theory is considered a theoretical-therapy system (Titelman, 1998), meaning, family therapy refers to the way the therapist thinks about the family and the efforts to modify the family relationship system. Therefore, the goal of family therapy is to facilitate the ability of one or more members to adapt to the vicissitudes of life, focusing more on the process of symptom management and less on the content (Titelman, 1998). From Bowen’s theory, symptoms in families arise after non-resolved conflicts in the family of origin were transmitted through generations (Bowen, 1978). He named fusion and differentiation as two extremes in a dimensional continuum to describe the functioning of the families. Differentiation means the level of emotional independence from the family of origin and fusion means being non-differentiated from it. Families who are emotionally fused are a non-differentiated mass. Bowen’s Systemic theory offers a conceptualization about how families deal with illness and death. Illness and death are considered extreme nodal events, and just like unemployment, and emigration, can modify a functioning position in the family. Bowen stated that death in a family can creates a wave effect that can last through generations (Bowen, 1991). It alters the family’s emotional equilibrium, and the effects are not necessary grief, but other symptoms. Death can also be a taboo subject in families and create close systems at multiple levels- in the patient, in the family and in the doctors and other professionals (Bowen, 1991). He recommended that family therapists should assess the structure and functioning of the family, as well as the level of adaptation to illness and anticipation of death.
Although few research has focused on Bowen systems theory on Latino families, it’s widely utilized clinically in many Spanish-speaking countries (Rodríguez-González et al., 2016). Bowen argued that his theory holds “universal relevance,” but empirical evidence is needed to confirm it’s fit with Latino family culture (Taylor et al., 2006). For example, Latinos differ from Anglo culture in the US with respect to family values. The concept of differentiation -an ideal goal for the family in Bowen’s perspective- leans toward individualism as a goal, which is not typical in mainly collectivist Latino culture.
Systemic evaluation of families using genograms
The present study adopts an integrative theoretical framework consisting of Bowen’s systems theory and a micro-cultural perspective to Bronfenbrenner’s ecological approach (Vélez-Agosto et al., 2017). A family unit is defined as persons who may or may not reside with the patient and whom the patient recognizes play an important and meaningful role in his or her cancer care experience (Hodgson et al., 2011) and includes persons who define themselves as members of families, demonstrate commitment to one another, and share a personal history (Niemela et al., 2016). There is diversity in family compositions that may include other generations, such as parents and children or extended family members as in the case of Latino families. The cultural micro-system model is a revision of Bronfenbrenner’s ecological model, where culture is not situated in the macro sphere, but relocated in the micro system. This conceptual change implies that family members participate in practices shaped by cultural-context specificity and interact with communities and social institutions, both proximal and distal, where culture is embedded (Vélez-Agosto et al., 2017). Assessment of family functioning should consider how culture shapes or defines the family system from the micro system perspective.
The use of genograms is recommended for this assessment of functioning in both systemic and qualitative dimensions (Platt, 2009). A genogram is a kind of family tree which usually contains some basic information on three or more generations (McGoldrick et al., 2008). Assessment using genograms may vary across disciplines, but recollection of family stories is done by using symbols and narratives. Much genogram development has focused on expanding the symbols used in them (Platt, 2009). Very few research has focused on developing structured interviews to formalize the process to facilitate replicating studies and confer more validity and reliability to this form of assessment (Platt, 2009; Puhlman et al., 2023).
The genogram is a flexible technique that aligns with other therapeutic models-such as narrative therapy- because it creates a unique occasion to explore and re-tell family stories (Chrzastowski, 2011; Sherman and Simonton, 2001). The re-telling process enables a person to look at their life from a certain distance; it strengthens the semantic and reflective processes and facilitates people’s analysis of their different feelings toward family members (Chrzastowski, 2011). Although family therapists have debates in respect to the difference between systemic and narrative paradigms, some family therapists have argued in favor of integrating them (McGoldrick et al., 2008). The genogram harmonizes both dimensions, the narrative and the systemic, and gives a more comprehensive in-depth description of family functioning.
Research on genograms
Bowen was the first to establish an interview protocol for using genograms, then Michael Kerr (Kerr and Bowen, 1988). McGoldrick et al. (2008) standardized the format for symbolizing family patterns and thus creating the “family genogram.” Although widely used in a variety of clinical settings, limited agreement exists about a specific format for the genogram (Platt, 2009) and not much research has focused on the reliability of genogram interviewing or it’s use beyond clinical settings (Alexander et al., 2022; Puhlman et al., 2023). Studies such as Coupland et al. (1995), Rohrbaugh et al. (1992), and Rogers and Holloway (1990) suggest limitations regarding genogram interviewing because of lack of agreement in interview protocols. Because of its flexibility, genograms may prevent researchers from rigorously testing theoretical and clinical assumptions about the family genogram’s utility (Platt, 2009). Genograms present an opportunity to test and extend theoretical frameworks, examine clinical assumptions and provide complex explanations for family interactions (Puhlman et al., 2023).
The present study
The purpose of this study was to translate and culturally adapt a genogram interview protocol, the Family Genogram Interview (FGI) (Platt, 2009), to a Puerto Rican sample and explore systemic family functioning when a family member experiences cancer. The Family Genogram Interview is informed by Bowen’s systems theoretical framework, operationalizing four family emotional processes: marital conflict, symptoms of a spouse, emotional cutoff and focus on a child. Gathering empirical data guided by a family theoretical lens with the use of genograms can lead to a furtive dialog where theory can be further refined or challenged with cultural sensitivity.
The present study answered the following research questions:
a. How does cancer affect the systemic functioning of Puerto Rican families with a cancer patient?
a. What themes emerged from the narratives consistent with Bowen’s four emotional core processes?
b. What is the reliability of the Family Genogram Interview in Spanish?
Quantitative Goals:
Translate the Family Genogram Interview (FGI) to Spanish.
Test the reliability of the FGI in a Hispanic sample of individuals from families with a cancer patient.
Assess the systemic functioning of Hispanic individuals from families with a cancer patient using the translated FGI.
Qualitative Goal:
Explore the narratives surrounding the systemic functioning of individuals from families having a member with cancer.
Methods
The research design was a qualitative oriented mixed-methods approach or a mixed world-views approach defined by the interplay of different methods and approaches that are in dialogue between them (Creswell and Clark, 2007; Mason, 2006).
Participants
Purpose sampling of the deductive theoretical construct type (Patton, 2015) was used to recruit 51 Puerto Rican (98%; n = 50) adult participants (21 years old or older) who were either a spouse, a partner, a brother or sister, a mother, father, a son or daughter, or a primary caretaker of a cancer patient that had at least 1 month after being diagnosed. Deductive theoretical construct sampling involves finding case manifestations of a theoretical construct of interest to examine and elaborate the construct, its variation and implications; and deepening or verifying theory in new contexts, periods or situations (Patton, 2015). Settings for recruitment were an oncology hospital and a hospice center in the Metropolitan Area of Puerto Rico. Formal authorization was solicited via an endorsement letter to recruit participants. Recruiting was done by the principal investigator and interviewers. Informative sheets were given to possible participants who solicited services in the hospital’s social work offices and posted in the social work office. Before the interview, informed consent procedures were followed. Participants gave written consent for conducting the study and the publishing of anonymized results. Then, they were given a sociodemographic sheet to fill out. After the interview, participants received an incentive of ten dollars. Appropriate procedures were taken to ensure participants’ confidentiality and a stand in protocol was placed in case of adverse situations.
The sample size for the quantitative component was 51 participants. For the qualitative component, only nine of the participants were selected for analysis following Robinson (2014) and Smithet al. (2009) epistemological and practical guidelines. The researcher determined after the ninth interview that definitions provided thick descriptions of the theoretical constructs. In qualitative studies, fewer participants are suggested for providing scope for developing cross-case generalities, while preventing the researcher being bogged down in data (Robinson, 2014). Data collection was done between March through May of 2018.
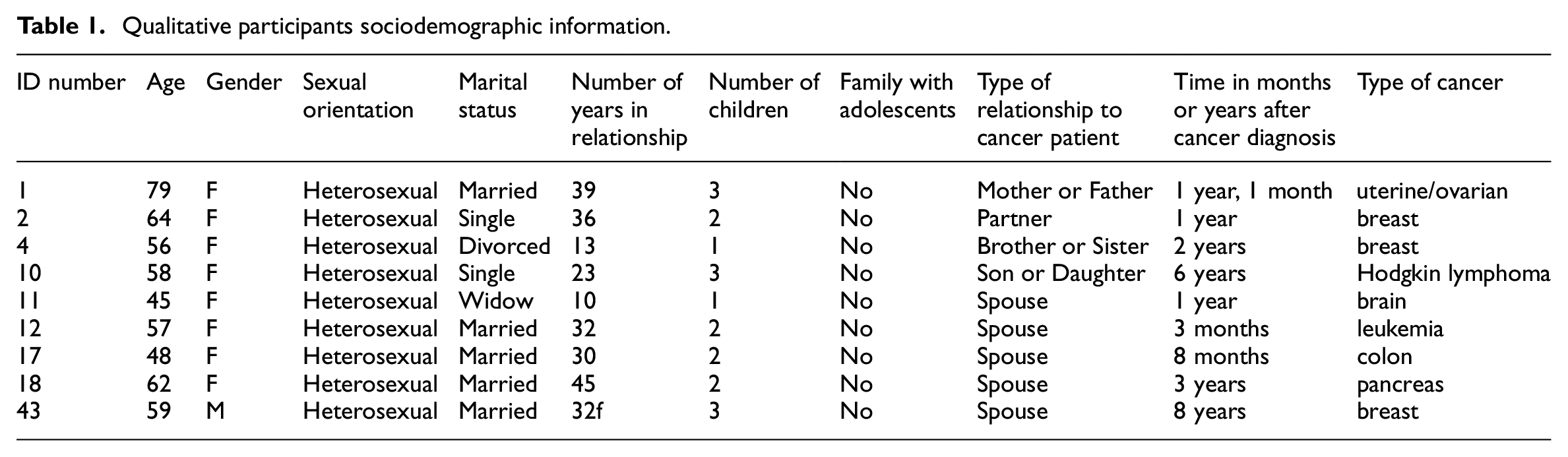
Participants were on average 54.10 years of age (SD = 13.28, range 23–79); 76.5% (n = 39) were female and 23.5% (n = 12) were male. Participants were 96.1% (n = 49) heterosexual and 51% (n = 26) reported being married, while 29.4% (n = 15) reported being single or living with their partners. The rest of participants reported being divorced or widowed (19.6%; n = 10). Married or partnered participants reported an average of 20.36 years in a relationship and participants with children reported an average of 2.02 children. Only 15.7% (n = 8) of participants reported having an adolescent in their nuclear family. Participants were primarily low income (66.7% reported an annual income of $ 0–20,000, 15.7% reported $20,001–30,000 and 17.7% reported $30,001 and up). The majority reported having an education of a high school diploma or less (41.2%; n = 21), followed by 31.4% (n = 16) reporting a bachelor’s degree and 25.5% (n = 13) reporting a technical or associate’s degree. Only one participant reported a higher degree. Cancer patients had an average of 3.20 years after being diagnosed (SD = 5.64; range from 1 month to 30 years). Highly reported cancers were colon (15.7%; n = 8), prostate (11.8%; n = 6) and breast (11.8%; n = 6) followed by leukemia (9.8%; n = 5) and lung (7.8%; n = 4). Only one (n = 1) participant didn’t complete the interview, and data was not used in final analysis.
The qualitative sample consisted of participants: 1, 2, 4, 10, 11, 12, 17, 18, and 43. See Table 1 for sociodemographic information.
Qualitative participants sociodemographic information.
Instruments
Sociodemographic questionnaire
The sociodemographic questionnaire consisted of age, ethnicity, socioeconomic status, marital status, level of education, number of years married or in a relationship, number and age of children, time in months or years after cancer diagnosis of family member, type of cancer, type of relationship to cancer patient (spouse, partner, mother or father, brother or sister, son/daughter or caretaker).
Family genogram interview (FGI)
This study used a translated version of the Family Genogram Interview (FGI) by Platt (2009). Authorization to use the FGI was solicited from Dr. Platt and granted via email. The FGI has quantitative questions that provide means of assessing family functioning and qualitative questions, intended to gather more rich and complex information from participants to give context or elaborate on family processes (Platt and Skowron, 2013). The FGI is designed to assess the nuclear family (e.g. partner and children) or family of origin (parents and siblings). The proposed study evaluated either the nuclear family section or the family of origin section, depending on the relationship with the cancer patient.
The FGI consists of four subscales evaluating the four core emotional processes in Bowen’s Systems Theory: Marital conflict (FGI-MC), Emotional Cutoff (FGI-EC), Symptoms in a Spouse (FGI-SS) and Focus on a child (FGI-focus on a child). Each family process in the FGI is operationalized based on Kerr and Bowen’s (1988) description. Each scale consists of quantitative Likert-type scale items (5-point scale) and categorical items (Yes/No); and qualitative questions assessing both nuclear family and family of origin. The FGI-MC consists of a total of 9 quantitative and 31 qualitative questions; the FGI-EC scale consists of a total of 20 quantitative and 14 qualitative questions; the FGI-SS scale consists of a total of 31 quantitative and 23 qualitative questions; and the FGI-FC scale consisted of a total of 8 quantitative and 16 qualitative questions. Higher scores on the FGI-MC, EC, and SS-Total subscales indicate greater levels of marital conflict, emotional cutoff, and symptoms in a spouse, respectively. The FGI has good interviewer reliability, 100% percent agreement regarding asking all the questions and 0.95 reliability on essential identical participant responses across two interviewers. Consistency reliability of the FGI subscale scores was mixed. Three of its subscale scores demonstrated good internal consistency reliability, however, one subscale scores did not (Cronbach’s alpha = 0.51) (Platt and Skowron, 2013). Construct validity assessments yielded mixed results, where the FGI-MC and the FGI-SS were the only ones found with significant results compared to their respective external measures, The Marital Satisfaction Inventory–Revised (MSI-R), Differentiation of self Inventory-revised (DSI-R), Outcome Questionnaire-45 (OQ-45) and the Parent Protection Scale (PPS) (Platt and Skowron, 2013).
Procedures
The Committee for Research Ethics (IRB) at Carlos Albizu University approved our interviews (approval: Fall 17–24) on February 1st, 2018. The translation and cultural adaptation of the FGI in Spanish was done following a modified version of Erkutt et al. (1999) dual-focus approach to creating bilingual measures. First, a bilingual/bicultural research team that includes researchers indigenous to cultures being studied was constituted to lead the project. The principal investigator (PI) is Puerto Rican and indigenous to the culture being studied and was part of the team along with the Dissertation Mentor, who is bicultural and experienced with the translation method, and a Puerto Rican psychologist, expert in family therapy and Bowen’s constructs. The second step consisted of operationalizing the content area of the construct(s) being studied by deciding on concepts that provide equally valid definitions of the constructs in both cultures. The third step was translating the FGI into Spanish by a professional translator. Then the team discussed the wording for each subscale item simultaneously in English and Spanish. The last step was to evaluate the measure’s psychometric properties, in this case, the internal consistency of the subscales.
Five master’s level clinical psychology graduate students and one doctorate level clinical psychologist were recruited to do the interviews with the principal investigator (PI). All participated in an interview training about conducting structured interviews and qualitative interviews conducted by the PI- which has experience in training graduate students in research methods. The interviewers also helped recruit participants. Interviews were scheduled in the clinical offices used by graduate students located at the hospital to practice therapy, as well as in a closed library room provided by the hospice lodge. The clinical offices had good lighting and closed doors for privacy. Interviews had a duration of approximately 30 minutes to 1 hour. Ten of the interviews were conducted by the PI and audiotaped. Later they were transcribed for further qualitative analysis. All identifying information was eliminated from the transcripts. These interviews were done from a qualitative-oriented stance, where open-ended questions were further explored.
Data analysis
The quantitative component of the study tested for reliability of the newly translated and cancer adapted FGI. Internal consistency reliability of the participants scores on the FGI subscales was assessed with Cronbach’s alpha. Second, a descriptive analysis was done to examine systemic functioning of individuals from families with a cancer patient. Sociodemographic data was presented in frequencies and percentages. The four subscales were described with means, standard deviation, and ranges. Quantitative data was analyzed using IBM SPSS Statistics (Version 25).
The qualitative component analysis used a hybrid approach (Swain, 2018) where deductive thematic analysis principles were used to enhance descriptions of Bowen’s core processes, while also following an inductive approach such as Smith et al. (2009) Interpretative Phenomenological principles for analyzing the open-ended questions of the FGI-Spanish. Smith et al. (2009) suggest that IPA is not a prescriptive methodology, and every researcher can adapt it. Nine interviews were analyzed by the PI and a graduate master’s level clinical psychology student trained in qualitative analysis and with prior experience in qualitative research. Each transcription was read two times separately by the analysts. Each analyst wrote annotations of comments, possible themes, and a preliminary analysis about what is significant was written on the left margin of the transcription until the whole end. On the right margin, they wrote theme titles or concise phrases that capture the essential quality of the text which was continued through the whole transcript. The analysts met to discuss agreements on the themes of each interview and further discuss alignment and distance between emergent themes and Bowen’s constructs. The themes were then listed to see connections among them and clustering by the PI. Some themes were dropped if they didn’t fit well with the emergent structure and did not provided further enhancement of Bowen’s constructs. In the next stage, the themes were ordered coherently in a table to identify some clusters which captured most strongly the participants’ concerns on the topic. In the final stage, the PI translated the themes to a narrative account where participant’s quotes were used to describe the overall experience. The final themes were described under Bowen’s constructs.
Results
Quantitative findings
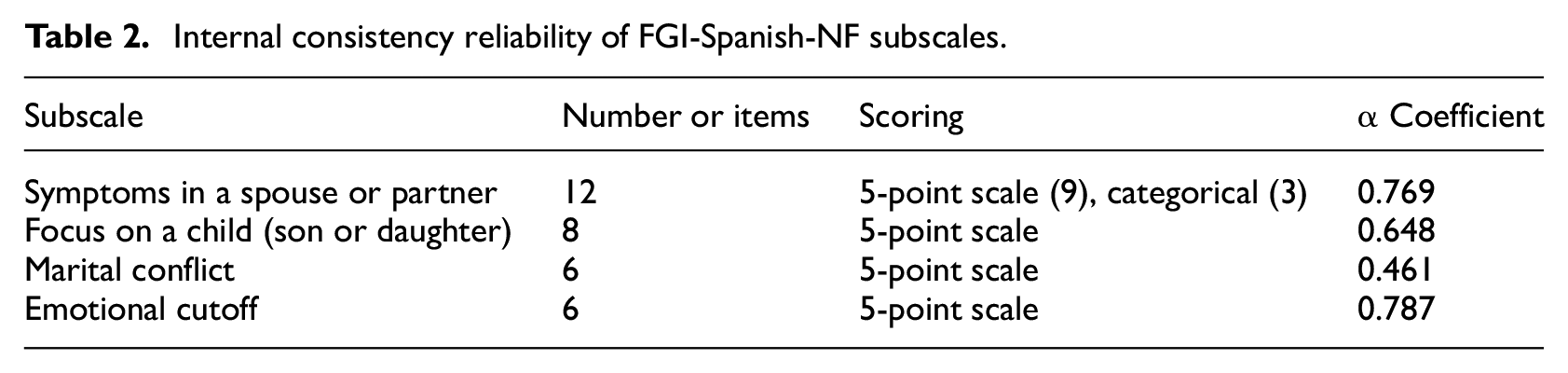
The sub-sample assessed with the Nuclear Family part of the interview were twenty-nine participants (n = 29). Overall, only Symptoms in a spouse or partner and Emotional Cutoff subscales reported an accepted reliability (α > 0.7). See Table 2 for Cronbach’s α coefficients, and the number and type of items in the FGI-Spanish Nuclear Family subscales.
Internal consistency reliability of FGI-Spanish-NF subscales.
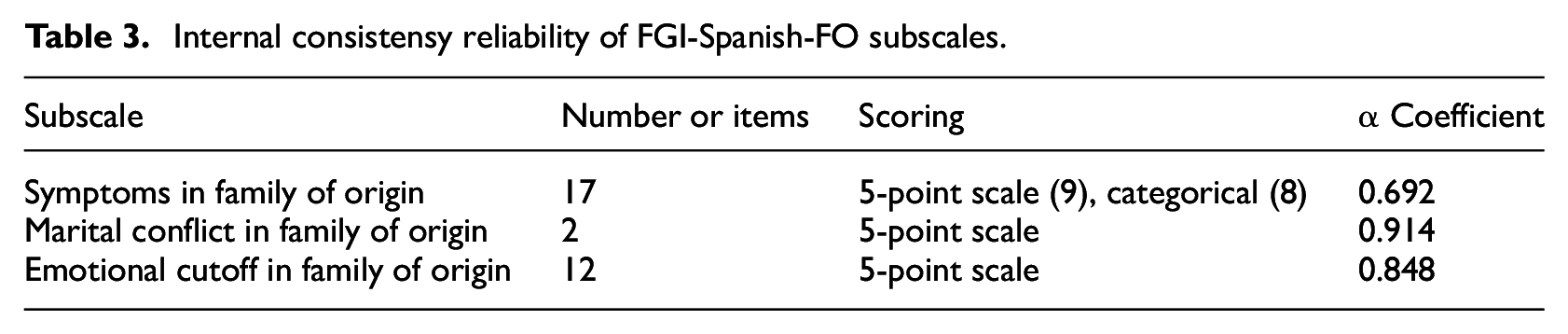
The sub-sample assessed with the Family of Origin part of the interview consisted of nineteen participants (n = 21). Missing data in questions about parental health in symptoms of Family of Origin were excluded on two of the interviews in final analysis. All scales reported an accepted reliability. In the Symptoms in Family of Origin subscale, most items appeared worthy of retention, with exception of item 17. Most items appeared worthy of retention in the Emotional Cutoff in Family of Origin subscale, except for items 3 and 4. In the See Table 3 for Cronbach’s α coefficients, and the number and type of items in the FGI-Spanish Family of Origin subscales.
Internal consistensy reliability of FGI-Spanish-FO subscales.
Participants that completed the Nuclear Family part of the interview reported an average of 23.24 (SD = 7.48) in Symptoms of a Spouse or Partner, an average of 14.79 (SD = 5.58) in focus on a child, an average of 12.02 (SD = 2.94) in Marital Conflict and an average of 8.10 (SD = 4.57) on Emotional Cutoff.
Participants that completed the Family of Origin part of the interview reported an average of 25.52 (SD = 6.67) on Symptoms of Family of Origin, an average of 3.88 (SD = 2.44) on Marital Conflict of Family of Origin and an average of 25.7 (SD = 9.04) of Emotional Cutoff in Family of Origin.
Higher scores on the FGI-Spanish Total subscales indicate greater levels of the family process in nuclear family or family of origin.
Qualitative findings
Qualitative themes were theoretically organized into three of Bowen’s family emotional processes assessed in the FGI-Spanish and themes surrounding the cancer experience. The following themes emerged from each core process: “cancer as a family illness,” “children as the priority,” “conflict versus support during illness management.”
Cancer as a family illness
Symptoms in Spouse or Partner showed the following themes: (1) family gets sick with the ill, (2) the tumbling relationship between illness and work, (3) functioning within illness. Participants discussed how family roles were altered by the illness of the cancer patient and the emotional impact on the family. The roles of adult children were considered important for support of cancer patients in caregiving and economic stability. As one participant (4) stated: “children should be the 99% of everything” when caring for cancer is concerned. They also consider the role of the spouse or partner as essential, in caregiving and emotional support. A participant (7) described it as “the health of a partner is one’s own.” Another participant (10) described the emotional impact of his wife’s cancer leading to her being the one cheering him and saying: “don’t worry, everything will be fine.” This meant that cancer patients were also key in supporting other members in the family. Most spouses or partners assumed the main caregiving role, supporting with daily activities, managing the health condition, providing emotional support and providing cancer care, such as nursing and helping with personal hygiene. Emotional support sometimes meant not crying in front of the patient and not discussing cancer with them or, in contrast, joining in “the battle” and maintaining positivity. A participant (10) stated: “emotional support is very important; you tell your partner: it (cancer) does not matter.”
Emotional impact on spouses or partners was expressed in many ways by participants. Some participants indicated that the partners or spouses felt “depression” or “anxiety.” A participant (2) indicated that her spouse was affected only when he “thought about it.” Emotional impact on cancer patients was described more positive in some families, while in others, more deteriorated. Regarding children, cancer was described as having a significant impact on their emotional health. A participant (10) described how his wife’s cancer led to his son’s drug addiction. Another (8), how her son “suffers his father’s illness” and “calls every day.”
Work was described by participants as a major stressor. They described how cancer impacted participating in job tasks or how little support they received from their employers during illness. One participant (9) described how her husband did not received support from his agency after being diagnosed and soliciting sick leave: “he tells me, it’s a shame, that I ask for permission to take care of my health, the agency denies me… seeing how my body was deteriorating.” Not being able to work was also seen as a cause of economic hardships during illness, where sometimes adult children had to contribute financially.
Participants described restrictions in everyday activities because of illness. Among them, they mentioned: cancer patients not being able to work or participate in hobbies because of physical limitations. Also, caregivers were limited because of caregiving responsibilities. Participant (7) mentioned: “it affects me, in a sense, because I have to spend a lot of time, that is, I have to dedicate time to him, but between that time, I take time to follow my daily routine, do you understand?” Participants indicated also that socializing was limited, but described participating in some family and religious activities, and helping in their communities. They mentioned communication and “giving to others” as evidence of social functioning after illness.
Children as a priority
Regarding focus on a child, both in nuclear family and family of origin, the following themes emerged: (1) worries about their children, (2) support from adult children in illness, and (3) relationship conflicts because of their children. Adult children were described generally in a favorable way, alluding to their morals, character and working habits as main descriptors. Participants expressed positively how children affected their relationships. They described it as “bringing more love to the relationship” or changing their lives in a good way.
Participants expressed worries about their children’s physical and emotional health, marital conflicts and divorce, or about going out. Adult children play a great role in managing parental illness. Participants expressed their adult children as principal emotional and financial support during illness. A participant (10) indicated about his daughters: “they help me every time my wife has had to be hospitalized; they prepare an agenda to be with their mom in the hospital, they cook… they help us financially.” Support is mostly expressed by calling parents regularly and being “pendiente,” which means the state of actively asking and being available for their needs. Parents also express concern with their adult children through being “pendiente” despite illness.
Conflict versus support during illness management
Marital conflict reflected the following themes: worries about adult children’s relationships, illness management and changes in roles (the role of the sick and the role of the partner as caregiver), work and everyday activities. A participant (10) described his opposition to his wife’s radiotherapy and how this caused a rift, not only with his wife, but with his daughter: “when they wanted to give my wife radiation therapy, I did not agree… and both insisted, and we had an argument at home.” Participants also expressed concerns about the patient “assimilating” the cancer. A participant (9) indicated that her husband sometimes questioned her about his cancer. For example, “he would ask: when is it going to leave?”. This example illustrated the difficulty of the partner being the caregiver and listening to the cancer patient’s concerns. Another participant (7) reported disagreements about what her husband could or could not do because of cancer. In both cases, “assimilating the cancer” became the main motive of arguments between partners in a relationship, because usually the caregiver served as the boundary enforcer and “the reality check” for the patient. Some participants admitted to not talking about illness or its consequences with the patient. In contrast, participants described attachment between the couple as being communicative and close, having warmth and being supportive.
Emotional cutoff was denied in most participants, but some admitted not talking to their spouses about certain topics to avoid conflict and stressing the partner.
Discussion
This study assessed the systemic functioning of fifty-one Puerto Rican families with a cancer patient and evaluated the psychometric properties of the newly translated FGI- Spanish, an innovative genogram research tool. Psychometric evaluation suggested an accepted reliability of the FGI-Spanish, but caution should be taken in the subscales of marital conflict and focus on a child in the Nuclear Family part of the interview. Further studies with a homogenous sample will be needed to have a better estimation of reliability of the translated version.
Even though systemic literature on cancer provides theoretical descriptions of how cancer impacts families, there is a gap in literature with respects to studies of family therapy in cancer care settings (Hodgson et al., 2011). Qualitative findings of this study provided a description of how Bowen’s emotional processes were experienced in Puerto Rican families with a cancer patient while using a genogram interview as an innovative research tool.
Findings showed how in nuclear families, the experience of cancer inscribes new roles to spouses, partners, and adult children, such as those of caregivers and supporters. For example, adult children assumed financial and emotional support for parental cancer and consistent with Bowen’s system theory, they changed their functioning position (Titelman, 1998). Role structuring is considered evidence of family reorganization and adaptation to cancer and can lead to both positive and negative consequences (Lewis, 2010; Sherman and Simonton, 2001; Steinglass et al., 2011). One of the negative consequences is a change in family hierarchal structure, where the marital dyad is subsumed under the parental-child subsystem. Family systems theory conceptualizes subsystems as interdependent (Cox and Paley, 2003), and the role reversion introduced new conflicts in the marital sub-system creating distress that was reflected back into the parent-child sub-system.
This study was also consistent with systemic literature that in that cancer changes routines and the daily activities of families (Sherman and Simonton, 1999; Steinglass et al., 2011). For example, the patient or partner may no longer participate in work, adding financial concerns to cancer burdens. An area exception when it came changes in routine was socialization outside the family. Families participating in religious activities were considered part of a patient’s wellbeing. Therefore, some aspects of Puerto Rican culture and spirituality were more dominant than the cancer experience. A previous study of identifying cancer education needs in Puerto Rico showed how cultural beliefs about masculinity reduce colon cancer screening (Jiménez et al., 2018). Systemic literature emphasizes that chronic illness dominates family life and concerns (Steinglass et al., 2011), but this study showed that although it alters the family’s structure, other aspects of family life were also dominant. Cultural practices are at the center of how families reorganize their lives and merit greater attention (Rivero-Vergne et al., 2008).
Bowen’s concept of Symptom formation in a spouse was also present in the quantitative and qualitative findings and demonstrated similarities to other studies (Lewis, 2010; Manne and Ostroff, 2011). Descriptive statistics showed a major presence of Symptoms in the Spouse or partner, and Emotional Cutoff only in the Family of Origin. Qualitative data showed how spouses or partners struggled with similar worries as the patient regarding treatment side effects and illness management. Therefore, emotional cancer-related distress was shared and interdependent within couples (Martinez et al., 2020). Couples also had difficulties discussing cancer with the patient due to worrying about bringing more stress to the patient. This phenomenon of communication can be referred to as a state of paralysis or denial and can have undesirable effects on coping and psychosocial outcomes (Martinez et al., 2020; Rosenbaum et al., 2006).
When it came to marital conflicts, most issues expressed were related to the couple’s adult children’s wellbeing and relationships. Focus on a child, a core emotional process in families, might be a way to deal with the anxiety of the cancer experience by deflecting from the primary concern. A previous study showed that focus on a child was more evident in Puerto Rican mothers than in fathers when it came to pediatric cancer due to assuming the role of the main caretaker and receiving most of the emotional burden (Rivero-Vergne et al., 2008).
Implications for practice
Genogram interviews can be of value when assessing family functioning in other contexts, such as in different cultures or in marginalized populations, but further research is needed to establish them as a structured interview protocol (Platt, 2009). Latino families with a cancer patients would benefit systemic interventions that addressed their main concerns surrounding illness, such as the role restructuring of family members into caregivers and supporters, illness management and focus on children. Multi-family therapy interventions could be effective in addressing these concerns (Laqueur, 1972) and have proven effectiveness in anorexia (Salaminiou et al., 2017) and drug addiction (Garrido-Fernández et al., 2017).
Limitations
The proposed study had several limitations. Cross-sectional studies are limited in only measuring data at a single point. This study would have benefited from evaluating multiple points in time to assess further changes in family functioning. Also, the assessment of family functioning with only one member affects construct validity, due to rating only the perception of one member about the other as in the case of spouses. This could also lead to a desirability bias, where family members would then to portray their family with a more favorable view. The generalization of quantitative data was limited by the purpose sampling strategy used and the diverse compositions of families in the sample. Although the original reliability study of the FGI (Platt, 2009) considered 50 as an adequate number, it included a more homogenous sample of mainly Caucasian heterosexual mothers. This study included diversity in gender and members of the family, such as sisters and brothers, or sons and daughters. Further studies should be done with a larger, more homogeneous sample within Latino families and psychometric properties should be re-tested to improve the FGI-Spanish. Lastly, genograms were not analyzed visually, thus, missing adding another layer to grasp family relationships.
Footnotes
Data sharing statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
My study was approved by the Carlos Albizu University Institutional Review Board (approval no. Fall 17-24).
Informed consent
All participants provided written informed consent to conduct the study and publish anonymized results.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.