
Abstract
Endometriosis is a devastating chronic condition with significant physical and social implications. This research focused on two questions: 1) how do endometriosis patients experience healthcare in Canada, and 2) how can the healthcare encounter effectively address the psychosocial burden of disease that patients bear? This study examines the psychosocial implications of endometriosis diagnosis and treatment. Data was obtained through semi-structured interviews with nine people diagnosed with endometriosis. Interview questions centering patient perceptions of care were thematically analyzed utilizing reflexive thematic analysis. Analyzing participant narratives and drawing upon Kleinman’s concepts of illness experiences and slow medicine, this article underlines the urgency of moving toward a deeper ethics of care for endometriosis patients, wherein the patient is understood and advocated for within the Canadian healthcare system. Drawing upon participant experiences, the present research calls for the widespread availability of a comprehensive healthcare model for the treatment of endometriosis.
Introduction
Approximately one million Canadian women and gender diverse peoples are diagnosed with endometriosis (Wahl et al., 2021), a devastating estrogen-dependant inflammatory condition (Singh et al., 2020); although diagnostic delay is thought to lead to an underestimate of its prevalence (Agarwal et al., 2018). The medical community has long recognized that the delay between the onset of symptoms and diagnosis of endometriosis is widespread, with an average diagnostic delay estimated to be approximately 11.7 years in the United States (Lukas et al., 2018). This diagnostic delay is often characterized by practitioners’ dismissal of patients’ symptoms (Markovic et al., 2008; Mikesell and Bontempo, 2023). As such, endometriosis is a disease that has long been misunderstood and underrepresented within the medical literature (Seear, 2014; Singh et al., 2020; Wahl et al., 2021).
Endometriosis is thought to be one of the most prevalent gynecological diseases in the world, as well as one of the most difficult to diagnose and treat (Wang et al., 2022). Pathologically, endometriosis is characterized by the existence of tissue similar to that of the endometrium found within parts of the body other than the uterus (Vercellini et al., 2013). This tissue bleeds throughout the patient’s menstrual cycle and causes widespread inflammation throughout the body (Jiang et al., 2016). The symptomatic burden of endometriosis is significant (Singh et al., 2020) and is often detrimental to the wellbeing of sufferers (Denny and Mann, 2007; Jones, 2016), with both pain and psychological burden lowering reported Quality of Life (QoL; Oehmke et al., 2009) and Health Related Quality of Life (HRQoL; Szypłowska et al., 2023).
Symptoms associated with endometriosis include intense pain and cramping during menstruation (dysmenorrhea); pain and cramping outside of the menstrual cycle (across the follicular, ovulatory, and luteal phases of the menstrual cycle); pelvic pain and pressure; dyspareunia (painful sexual intercourse); and infertility (Singh et al., 2020). Moreover, endometriosis diagnosis is further associated with diagnoses of other chronic pain conditions such as interstitial cystitis (painful bladder syndrome; Chung et al., 2005; Paulson and Delgado, 2007), irritable bowel syndrome (Schomacker et al., 2018), and central sensitization syndrome (Zheng et al., 2019).
Alongside the physical symptoms of endometriosis pain, patients also report several psychological consequences of the chronic illness. Endometriosis patients commonly suffer with reduced QoL, self-esteem concerns, feelings of failing one’s gender, anxiety, and depression (Moore et al., 2023; Moradi et al., 2014; Oehmke et al., 2009; Szypłowska et al., 2023). In their systematic review, Szypłowska et al. (2023) found that endometriosis patients experience significantly lower QoL and HRQoL (when compared to other chronic conditions, such as rheumatoid arthritis), and higher rates of anxiety and depression. As such, psychological interventions in the form of psychotherapy or counseling are often recommended for those who suffer from this chronic pelvic pain condition (Brooks et al., 2020).
In a study examining clinicians’ perceptions of endometriosis patients, Young et al. (2017) identified that medical professionals viewed endometriosis patients as often a “difficult patient” to treat, due to their “hysterical” tendencies. The psychological consequences of being deemed hysterical are presented by Cole et al. (2021), finding that women with endometriosis frequently experienced depersonalization, and derealization of one’s own identity after routinely being dismissed through their healthcare encounters. The negative consequences of such care extends beyond the clinician’s office; participants further expressed that their illness experiences (Kleinman, 1989) caused them to feel isolated not only from their care providers, but from their family, friends, and partners. This embodied disempowerment experienced by patients necessitates a reimagined model of care.
Literature review
Qualitative women’s health research supports the theory that feminine emotionality stereotypes have perpetuated a reality in which women struggle to receive adequate healthcare for chronic pain conditions, including endometriosis (Hamberg, 2008; Lloyd et al., 2020). Jones (2015) identifies that endometriosis is not merely a physical condition, and that it encompasses both social and physical consequences. Jones positions the social consequences of endometriosis diagnosis as being entrenched within hysteria discourse. This hysteria discourse—that female patients elaborate or fabricate pain experiences—remains a prominent concern associated with endometriosis care (Jones, 2015, 2016; Young et al., 2020), wherein patients are routinely dismissed through the medical encounter.
It is pertinent to note that dismissal poses a significant impact on quality of care for patients. Mikesell and Bontempo (2023) conducted a cross-sectional survey of patient experiences of endometriosis diagnosis and misdiagnosis, finding that endometriosis patients consistently experienced symptom dismissal. This dismissal causes patients to feel “invalidated,” “dismissed,” “ignored,” and “disbelieved” (p. 5). Here, it again becomes critical to note the inseparability between diagnosis and self that so many chronic illness patients are burdened with; the symptomology of the disease is attributed by the patient as a deeply intrenched facet of the self. Such feminine emotionality stereotypes suggest that women “dramatize, overemphasize, or even fabricate their experiences of pain” (Lloyd et al., 2020: 198). Denying the truth of women’s experiences exacerbates pain dismissal and diagnostic delay (Lloyd et al., 2020).
Throughout their extensive study, Mikesell and Bontempo (2023) revealed that feelings of dismissal were commonplace throughout the research findings, which in turn contributed to feelings of mistrust of medical practitioners amongst participants. The authors note that their data unveiled a unidirectional relationship between competence and fidelity; participants attributed health care providers’ poor understanding and education regarding endometriosis to be the cause of the dismissal imparted upon their patients. Similarly, Young et al. (2020) suggest that the dismissal that endometriosis patients face is often attributed to a lack of knowledge surrounding the disease itself on part of practitioners.
While many of the study participants discussed the hardships associated with dismissal, the value of an empathetic, informed health care provider was well regarded throughout the study population (Mikesell and Bontempo, 2023). Thus, while the shortcomings of care providers are indeed well reported amongst endometriosis patients, this is not indicative of the perceived value of empathetic healthcare providers. Participants express that they place tremendous value upon their relationship with their healthcare provider when the patient-practitioner relationship is mediated by informed, compassionate care.
Emotionality stereotypes, hysteria discourse, and lack of patient satisfaction with care pose dire consequences for patients. Bullo (2018 examined the consequences of disempowerment and endometriosis in a comprehensive multi-faceted research study. Bullo used a corpus of online data analysis and in-depth interviews to address: (1) What discourses of disempowerment are identified by women with endometriosis, (2) how do women present themselves as either empowered or disempowered in light of such discourses, and (3) how can understanding the discourses utilized by women with endometriosis advance medical practices and diagnostic delay of endometriosis? This research began with an analysis of online endometriosis self-help forums which were cross-referenced with medical and sociological scholarly articles on endometriosis. Bullo (2018) identified three themes of disempowerment experienced by participants: disempowerment caused by endometriosis, such as failing to perform gender roles; disempowerment caused by pain normalization and misdiagnosis; and the need to demonstrate self-advocacy to receive care. The shortcomings in medical care experienced by endometriosis patients illustrated by previous research underlines the urgency of the proposed research as patients routinely experience neglect and unnecessary pain.
However, due to the existing literature on emotionality stereotypes and endometriosis pain, it is critical that the provision of psychotherapeutic care (as proposed herein) does not psychologize pain, but that it empathetically addresses the psychological burden associated with this chronic illness. Alongside disempowerment from patient dismissal, endometriosis patients commonly experience reduced QoL as a result of the symptomology and comorbid illnesses associated with the disease. In a meta-analysis conducted by Wang et al. (2021) containing 44 articles spanning 13 countries, results unveiled that depression and anxiety symptoms were more prominent in endometriosis patients compared to controls, and as such, that endometriosis decreases mental and physical HRQoL for patients.
As illustrated, this psychological burden may be a culmination of dismissal within the healthcare encounter, and a result of the significant loss of QoL and autonomy that is a consequence of the symptoms, related infertility, or comorbid illnesses associated with endometriosis. Further, in a study conducted by Vannuccini et al. (2018), the authors found that of the participants in the study (n = 134), 59% of patients met the diagnostic criteria for one or more psychiatric illnesses, and that patients with higher prevalence of pelvic pain reported more severe psychiatric illness.
Taken together, the chronicity of endometriosis pain and the dismissal of illness experiences cause significant psychological burden for patients (Dowding et al., 2024); thus, psychotherapy is a commonly recommended treatment plan for this patient population (Dunselman et al., 2014). However, patients often go without accessing this psychological care as the emotional consequences of endometriosis pain, and reduction of QoL are often dismissed by care providers (Dowding et al., 2024). As a part of the Biopsychological Impact of Pelvic Pain cohort study, Dowding and colleagues sought to examine endometriosis patients’ perspectives on receiving psychological care for their chronic illness. The findings of the survey indicated that all the participants (n = 200) were interested in engaging in at least one form of psychotherapy for the management of their pain and QoL improvement, but that only 85 (42.5%) of the participants were actively enrolled in psychotherapy at the time of the study. These results indicate a significant lack of accessibility to mental health care amongst this population. Those who were engaged in psychotherapy for their chronic pain noted that psychotherapeutic methods such as Cognitive Behavioral Therapy (CBT), Dialectical Behavior Therapy (DBT), Acceptance Commitment Therapy (ACT), and mindfulness practice to be integral to their ability to cope with their chronic illness.
In a systematic review of the mind-body interventions utilized to improve patient QoL including psychotherapy, counseling, and mindfulness practices such as yoga, Evans et al. (2019) identified that of the 12 reviewed publications, 89% of the studies reported improvement in pain with the use of psychological care alongside biomedical intervention. Similarly to Evans et al., Samami et al. (2023) conducted a systematic review of pain-focused psychological interventions for endometriosis patients. The findings of the review demonstrated that all of the interventions (CBT, mindfulness, yoga, psychoeducation, and progressive muscle relaxation (PMR) therapy were all found to moderate reductions in patient pain and improvement in QoL. In a RCT examining the effect of psychological interventions for improvement of endometriosis patient QoL, Hansen et al. (2023) found that patients who received the intervention experienced significantly improved QoL, demonstrating greater senses of control and emotional well-being.
The present research
Due to the noted disparities in care and the disease prevalence, I conducted patient-centered endometriosis research, grounded within a focus on patient experiences of care. Throughout the present research meaningful care is defined as accessible, empathetic, and empirically-based care. These pillars of care are informed by Arthur Kleinman’s seminal contributions to the study of chronic illness care. Kleinman’s (1989) concept of illness experiences and their distinction from disease features throughout this analysis. Differently than disease, which is a distinct set of signs and symptoms with assigned nosology and nomenclature, illness narratives explain the unique individual experience of chronic illness that each patient has. When the clinician considers the patient’s illness experience, rather than their disease alone, we are able to better understand how to care—this intimate caring relationship between clinician(s) and patient is what Kleinman refers to as slow medicine.
This research focuses on the experiences of women and gender diverse individuals diagnosed with endometriosis in Canada, and was guided by the research questions, (1) how do endometriosis patients experience healthcare in Canada, and (2) how can this experience be improved? By asking participants about their healthcare experiences, this research proposes the implementation of a comprehensive model of care for endometriosis patients. As it applies to the present research, comprehensive care is operationalized as a model that includes a team of providers concerned with the somatic (physicians, physiotherapists) and the psychic (psychologists, counselors) experiences of the patient. The corporal and psychological implications of inadequate care as presented herein evidence the need for such a comprehensive model. Here, the tenants of slow medicine (Kleinman, 1989) are applied to practice.
Guided by the experiences of the research participants, the present analysis seeks to articulate the ways in which identity and illness intersect when care is inadequate, in many cases becoming inextricably linked. That is, patients identify with their chronic illness, so much so that it becomes the very essence through which they understand their own personhood—this experience is exacerbated by shortcomings in care. The experiences of the research participants then culminate with a discussion of future care participants desire, bookended by a call for a comprehensive care model comprised of care for the body (biomedical care) and mental health care.
Method
The present research was approved by the Thompson Rivers University research ethics board (approval #103060) and was further endorsed by The Endometriosis Network Canada (TENC), a not-for-profit organization engaged in facilitating support for endometriosis patients and spreading awareness of endometriosis drawn from top medical experts internationally (The Endometriosis Network Canada, n.d.).
Participants and recruitment
The invitation to participate in research was disseminated by TENC to their membership, by the World Endometriosis Research Foundation (WERF), a global not-for-profit supporting the conduction of international endometriosis research (World Endometriosis Research Foundation, n.d.), and through online endometriosis support groups. The recruitment materials included an infographic containing details about the research, as well as the document containing the invitation to participate in research. The infographic explained inclusion criteria, inviting Canadian citizens 19 years of age or older surgically diagnosed with endometriosis to participate in an online semi-structured interview to discuss their endometriosis experiences. Participants without a surgical diagnosis of endometriosis were ineligible to participate, these prospective participants were excluded as it was a primary objective of the study to investigate the trajectory of care from suspected endometriosis to a confirmed diagnosis. As laparoscopic surgery is the only means to definitively diagnose endometriosis, all the research participants experienced this surgery to confirm their disease.
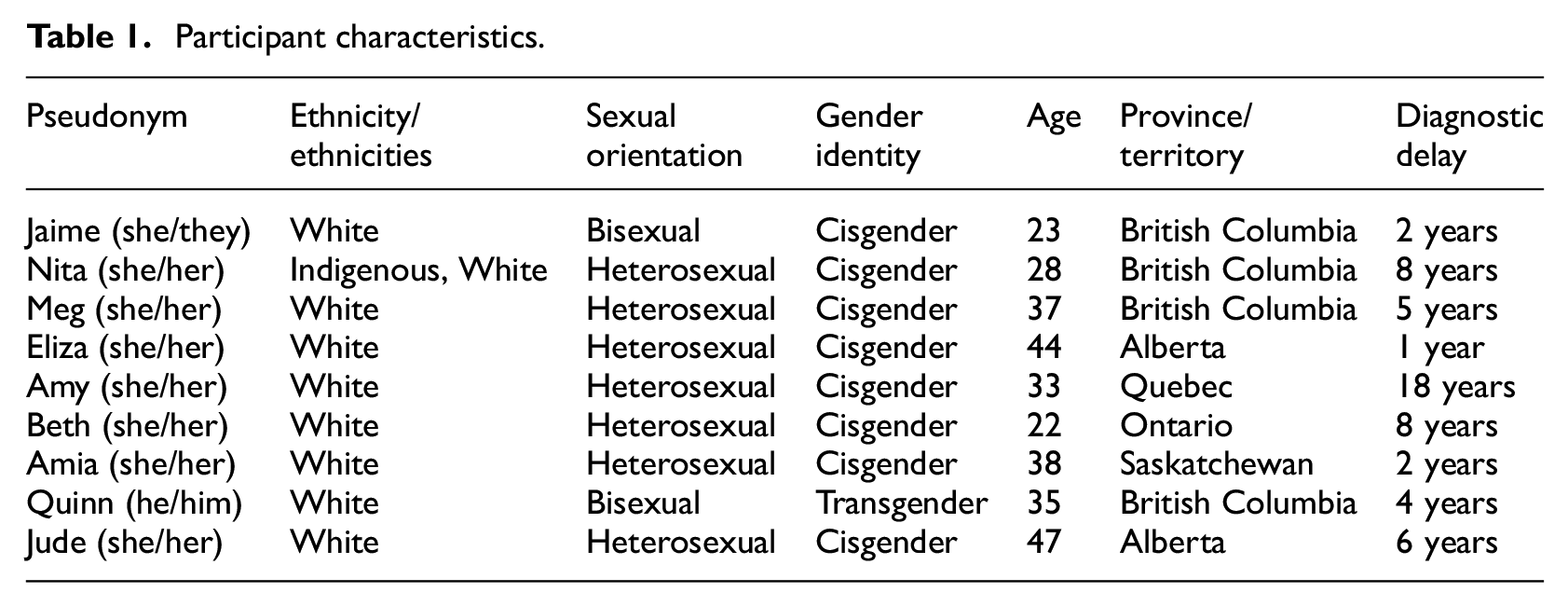
Through the three recruitment streams, nine women and gender-diverse individuals self-reporting a surgical endometriosis diagnosis volunteered to participate in the semi-structured interview. Of the nine participants, eight (89%) identified their ethnicity as being white, and one (11%) as Indigenous and white. Further, eight (89%) identified their gender identity as cisgender, and one (11%) as transgender. As there are significant disparities of inclusion between Black, Indigenous, people of color (BIPOC) and gender diverse endometriosis sufferers, the recruitment methodology involved the specific invitation of BIPOC and gender diverse individuals for participation. However, as the sample suggests, the population for the study is not entirely representative of the intersecting identities and illness experiences of the diverse population of endometriosis patients in Canada. The ages of the participants were between 22 and 47 years of age (M = 34 years of age). The participants self-reported a mean diagnostic delay of 6 years.
Data collection
Participants were sent the interview questions and signed the written informed consent form prior to the interview. Interview questions were focused on quantitative data about symptom duration and diagnostic delay (Table 1), and qualitative data pertaining to the biopsychosocial illness experiences (Kleinman, 1989) of participants. Topics addressed included perceptions of care, perceptions of practitioner bias, symptom dismissal, and participant’s ideas for improved care. The length of the interviews was between 26 and 48 minutes (M = 39 minutes). Participants were provided with a $20 gift card in appreciation for their time and participation upon the completion of their interview. Data was manually transcribed through online transcriptional services and manually checked for accuracy. The transcripts were deidentified, and pseudonyms were assigned for each participant. Streamlined transcription style was used, however, significant pauses and silences were noted as they occurred. Following transcription, data was imported to AtlasTI Qualitative Data Analysis Software.
Participant characteristics.
Data analysis method
Data was coded and analyzed inductively, utilizing reflexive thematic analysis (Braun and Clarke, 2020). Thematic analysis is a broad approach to analyzing qualitative data, first introduced by Braun and Clarke in 2006. As it is described by Braun and Clarke (2020), reflexive thematic analysis is characterized as a distinct form of traditional six-phases thematic analysis that places significant emphasis on the positionality and subjective reality of the researcher as a part of the analysis itself. Due to the focus on how the researcher uniquely interprets the data, bias cannot be avoided throughout analysis. Rather, the focus on the researcher positionality denotes the researcher as a resource and a creator of knowledge within the research process. Braun and Clarke (2020) describe reflexive thematic analysis as a guiding methodology that aligns with various theoretical orientations and analytic processes, spanning from experiential to critical epistemologies, and from deductive to inductive analyses. As it applies to the present study, reflexive thematic analysis was chosen as the guiding analytical methodology given its focus on open and organic coding methods, the generation of themes as the summation of codes generated throughout analysis, researcher positionality, and single-researcher analysis.
Guided by the research questions, data was initially coded inductively by highlighting features of the interviews pertinent to research questions and that were participant-driven (Braun and Clarke, 2020). Codes were then organized into themes according to frequency or repetition across the data set and keyness or importance in relation to the research questions (Braun and Clarke, 2020). Themes were then reviewed and mapped to ensure comprehensiveness in capturing the data and coherence altogether (Braun and Clarke, 2020). These themes include: (1) experiences of dismissal, (2) experiences of disempowerment, and (3) calls for comprehensive care. This analysis was informed by employing a social constructivist epistemological viewpoint, through which the structural conditions that have shaped the participant accounts were centered.
Data availability statement
The data generated and or analyzed during the current study are not publicly available nor are they available upon request due to the qualitative and interview-based nature of the study whereby details in the interview are inseparable from one’s identity and experiences. Thus, making such data available may compromise the confidentiality of participants.
Analysis
The themes of dismissal, disempowerment, and calls for comprehensive care are derived inductively from the answers of the participants to questions about diagnostic delay, quality of care, and the emotional impact of their illness and the care that they have received. The following themes underline disparities associated with disempowerment and discredit, which cause patients to feel misunderstood and dismissed within the healthcare encounter. Throughout the present analysis, I suggest that dismissal and disempowerment act both separately and simultaneously, contributing to the disparities and barriers that those with endometriosis face within the healthcare encounter.
For analytic purposes, I find it important to distinguish how disempowerment and dismissal act separately. Dismissal is operationally defined as pain or symptom dismissal from clinicians, and disempowerment is operationally defined as the resulting feelings of dismissal, including shame, sorrow, anger, or exhaustion. As I will refer to the concepts throughout the present analysis, dismissal is first introduced and is a catalyst of subsequently experienced disempowerment. That is, disempowerment is a product of dismissal. When endometriosis patients are dismissed, as the forthcoming analysis will present, this results in feelings of disempowerment and loss of trust in the practitioners who are meant to care for them. The themes presented discuss dismissal, where participants describe care shortcomings; disempowerment, where participants divulge the biopsychosocial consequences of dismissal; and finally, a comprehensive care model, where participant suggestions for future care are illuminated.
Care experiences: On patient dismissal
The present theme focuses particularly on the participant’s experiences of pain normalization and pain dismissal. A commonly shared sentiment amongst research participants was that they were not taken seriously for their pain; each one of the research participants spoke of plentiful examples of pain normalization and dismissal, experiences that could span the length of this report in its entirety.
Contending with pain dismissal, Eliza described a conversation that took place between her and her surgeon following one of her excision surgeries. She informed the surgeon that she was still in pain, as she recounts:
“Well, you know, you could have cancer, it could be worse, I did the best I could, you‘re just [going to] have to live with it.”
Of this, Eliza remarked: [this] was awful, but I accepted that because what else can you do?
Eliza sheds light upon the dismissal and comparison that endometriosis patients often face. The comparison of endometriosis and cancer as noted by Eliza’s surgeon suggests that the lack of terminal illness associated with endometriosis negates the need for further care. Here, the focus becomes survival, rather than an improved QoL. While this comparison of suffering is awful, as Eliza described, it is pertinent to note that the severity of individual cases of endometriosis must not be overlooked. As it has been noted throughout the medical literature, deep infiltrating (DI) endometriosis may result in the need for severe, life-altering treatments such as bowel resection and re-anastomosis (Meuleman et al., 2014), oophorectomy (the removal of one or both ovaries; Gosset et al., 2022), and salpingectomy (the removal of one or both fallopian tubes; Prodromidou et al., 2022). The various complications that necessitate such surgical intervention further exemplify the complexities of endometriosis prognosis.
Moreover, many of the present research participants noted that they were dismissed based upon a normalization of menstrual pain. As endometriosis is associated with dysmenorrhea, there is a significant amount of dismissal based upon what it means to have “normal” menstrual pain, something that is misunderstood within medical literature. As it is differentiated from proposed normal menstrual cramps, dysmenorrhea refers to “the need for medication and the inability to function normally” during menstruation (Grandi et al., 2012: 169). The research participants of the present study described the concerns that they expressed to their healthcare providers regarding menstrual pain, which were met with pain normalization and dismissal.
Amy: I will receive comments like, “Oh, maybe you’ re a bit too sensitive.” Beth: “All women have bad periods.” Or “you’re just really anxious or stressed.” Jude: “All girls have bad periods.” Meg: I feel that especially in terms of menstrual pain and menstrual issues, it’s just written off […]. You’re just brushed under the table.
The dismissal of menstrual pain is pertinent to note, as it is a symptom so commonly associated with endometriosis diagnosis (Singh et al., 2020). While this is a common finding in the literature (Hamberg, 2008; Lloyd et al., 2020), it cannot be disregarded; if one of the primary symptoms of a disease is normalized, so too is the misdiagnosis of the disease itself. The pain that the participants of the present research speak of is simultaneously described as a debilitating occurrence and as a benign facet of the female anatomy by many practitioners. Here, it is pertinent to note that the complexity of endometriosis diagnosis is deeply entrenched within the clinical misunderstanding of menstrual pain. The complication regarding endometriosis diagnosis is inextricably linked to the shortcomings in understanding not only of the disease itself, but by misunderstanding of menstruation. As degrees of severity for menstrual pain are yet to be established and widely understood, the single most prevalent symptom of endometriosis is often misunderstood or missed entirely.
Care narratives: On disempowerment
Disempowerment featured prominently throughout the participant interviews. For many endometriosis patients, and for those of the present research, disempowerment is experienced as a loss of agency, a loss of bodily autonomy, and a loss of sense of self. Each of the participants of the present research experienced disempowerment through a denial of knowing and loss of bodily autonomy. For Nita, disempowerment occurred when she was denied the provision of a hysterectomy for the management of her endometriosis pain. Nita explained that she had always known that she did not want to carry her own children, and that she was adamant about this with her surgeon and the surgical fellow. However, Nita was required to attend a counseling program and to write a letter as to why she felt that she wanted, or needed, to have a hysterectomy preformed. Nita recalls how she felt when she couldn’t simply be believed and have her surgery performed:
I’m coming to you in tears with pages and pages of medical history and saying like, “I need this for my health. I will not be around long enough to have children— if that’s what you think I should be doing— if you don’t remove this organ.”
In this moment, Nita recognizes the loss of bodily autonomy that she is experiencing through the denial of her knowing. Nita spoke of the loneliness associated with navigating the healthcare encounter while feeling disempowered. In some of her concluding remarks, Nita explained:
[T]here’s only one instance in the world that makes me think I want a partner, and that’s when I’m lying flat on my back in some medical office, because it’s just really scary to do that alone.
The disempowerment that presents itself when women’s knowing is dismissed is a visceral, emotional experience. Concluding the analysis of the present theme, Jaime succinctly articulates how the simultaneous experience of pain and dismissal produce disempowerment:
And it was really frustrating and it was really hard for me to be positive and keep hope that I was going to get through this really long time period of constantly being in pain, and just having all of these doctors continue to be discouraging was not helping.
In the wake of dismissal and disempowerment: Towards a model of comprehensive care for endometriosis patients
Throughout the research interviews, each of the participants described their experiences of care, and how they may be improved. The participants articulated the following calls to action:
•For practitioners to listen to their experiences, and to hear their pain
•Improved individualized, comprehensive care
•Improved pre-emptive care and screening for endometriosis
•Increased political involvement, funding and policy making pertaining to endometriosis
As it applies to the use of reflexive thematic analysis (Braun and Clarke, 2020), it is important to note that this theme is central to the narratives of each of the participants. That is, it is not only the result of the answers to one specific interview question, such as, the questions, “what words would you use to describe your interactions with your healthcare provider when discussing your endometriosis symptoms/ diagnosis” and, “what, if any, suggestions would you make to improve your experience in the healthcare system pertaining to your endometriosis?.” Both questions certainly contributed to the present theme, but more broadly, the experiences and attitudes reflected in this theme can be found across the data set in terms of frequency and from a variety of the interview questions. Moreover, reflexive thematic analysis is suited to an inductive approach as seen in the present theme so long as this induction is grounded in the data (Braun and Clarke, 2020). As the overarching ideas that contribute to this theme appear in response to numerous interview questions, this theme is in alignment with the reflexive thematic analysis procedures set out by Braun and Clarke (2006, 2020).
Throughout the interview questions, the participants offered suggestions for more comprehensive care, and this was often unprompted by the interviewer. The various calls for change by the participants are a striking feature of the data and highlights the current need for participants to engage in self-advocacy to fight for the care that they deserve. Capturing the overarching suggestions of many of the participants, Jaime underlines the need for specialized care, considering the psychosocial impact of the disease:
I find if you don’t have access to specialized care right away, general healthcare does not do [much at all] for you.
Quinn further speaks to the lack that endometriosis patients experience in the absence of comprehensive care:
There was nothing else they could offer me, they didn’t look at nutrition, they didn’t look at exercises or lifestyle changes, there was no thought of maybe you can get … some form of assistance.
The culmination of participant experiences of shortcomings in care and their calls to action throughout inform the proposal of a reimagined model of care. This proposed model is defined as one that considers the diverse needs of endometriosis patients across Canada, including mental health and biomedical care. While patients are able to access mental health care privately, the inaccessibility of fee-for-service care and the separation between private care and the medical encounter does not adequately address the unique mental health consequences of chronic illness diagnosis.
Moreover, the research participants have conveyed that they did not feel that they were provided enough information about their diagnosis in general. While some participants described a lack of information about the disease itself, others presented concerns about information on treatment options. Taken together with the absence of mental health care, this lack of information provides further support for the introduction of a comprehensive care model, based upon empirical endometriosis research and participant experiences.
The accounts of the participants inform a model of biopsychosocial healthcare that places central emphasis on participant illness experiences. Here, it is pertinent to note that this is not an entirely new concept, as many researchers have called for the introduction of comprehensive care models for chronic illness populations. My participants offer their own subjective reasoning for these calls but also echo what others have articulated (Agarwal et al., 2019; Opoku-Anane et al., 2020). Just as reflexive thematic analysis methods suggest that frequency and repetition within studies are important, frequency and repetition across studies are also important in showing a patterned social and medical problem and in advocating for more equitable healthcare solutions. The present study expands understandings of the psychosocial implications of dismissal and mistrust within the care encounter while also affirming such calls that have come before (Agarwal et al., 2019; Opoku-Anane et al., 2020).
Discussion
This research has explored the experiences of participants obtaining healthcare for endometriosis in Canada, and has addressed two central research questions: 1) how do endometriosis patients experience healthcare in Canada, and 2) how can this experience be improved? Reflexive thematic analysis (Braun and Clarke, 2020) unveiled that patients often experience care in a multiplicity of ways, but most notably, that patients experience dismissal throughout their navigation of the healthcare system. Thus, this research has answered both research questions as follows: (1) healthcare is often experienced as an entirely complicated journey that dismisses patient concerns, and (2) this experience can be improved by implementing a comprehensive, empirically informed care model.
Kleinman’s (1989) concept of slow medicine and greater standards of medical care have informed each of the three themes presented; as this concept suggests, participants frequently emphasized the need for more empathetic, genuine patient-practitioner relations. Throughout the themes of dismissal and disempowerment, what Kleinman identifies as inauthentic, unempathetic care is frequently experienced by participants, where the illness experience of the patient is not recognized by the care provider. The proposed model of comprehensive care is grounded in Kleinman’s concept of slow medicine and illness experiences, wherein the patient-practitioner relationship is a caring environment, addressing all of the effects of disease on patient well-being.
The present research findings on dismissal and disempowerment were very similar to those of Bullo (2018). Bullo’s study was multifaceted and included an analysis of a corpus of online data, as well as semi-structured participant interviews. Within the semi-structured interviews, Bullo found that disempowerment existed throughout the medical encounter, suggesting that “disempowerment and vulnerability are […] consequences of obstacles encountered by women in the social and medical environment” (p. 577). In my analysis I found the same to be true; participants spoke of experiences of disempowerment and proclaimed that those feelings where in relation to the medical encounter and consequences of medical dismissal. Bullo’s findings were based on 21 research participants; thus, their findings bolster and support those of the present research with a larger sample of qualitative research participants.
Moreover, the importance of empathetic care is also emphasized within Krebs and Schoenbauer’s (2020) analysis of communication within the medical encounter. The authors draw the poignant distinction that while the healthcare encounter is an empirical, biomedical process, it is also “a social event” (p. 1014) as it relies upon productive communication between practitioner and patient. As noted throughout the literature, ascertaining a deeper understanding of communication between patients and healthcare providers is of critical importance (Kleinman, 1989; Krebs and Schoenbauer, 2022), but often devalued.
Addressing the second research question utilizing reflexive thematic analysis, participant narratives were inductively analyzed to present a model of comprehensive care to address the disparities experienced by participants. In alignment with Kleinman (1989), the recommendations for such a comprehensive care model center the illness experiences of patients, with a particular emphasis upon the chronicity of endometriosis and the improvement of patient QoL. The proposed comprehensive care model would include the integration of both biomedical and psychological care (psychotherapy, counseling) for patients, emphasizing that equitable care is both corporal and moral (Kleinman, 1989). With the integration of a care model that considers each of the biopsychosocial impacts of illness, the healing nature of the healthcare encounter itself may be realized.
Universal mental healthcare as apart of chronic illness care is necessary to bridge the gap between the physical, and psychological pain associated with endometriosis. Research has demonstrated that the mental strain of being diagnosed with chronic pelvic illnesses is often comparable to the pain of the condition of itself; as patients are dismissed, misdiagnosed, and often await diagnosis and proper treatment for many years, mental exhaustion is widespread across this patient population (Cole et al., 2021; Jones, 2015, 2016; Seear, 2009; Young et al., 2020), these findings are replicated in the present research. Existing research on chronic pelvic pain conditions and the provision of psychotherapy demonstrates that the mental health of patients is significantly improved with such treatment (Dowding et al., 2024; Dunselman et al., 2014). Notably, therapeutic modalities such as CBT, ACT, mindfulness practices, and DBT have been successfully implemented amongst women with endometriosis (Donatti et al., 2022; Dowding et al., 2024; Hansen et al., 2023).
The proposed care model is also aligned with the calls to action presented within the Canadian Mental Health Association’s (CMHA) ACT for Mental Health (Canadian Mental Health Association (CMHA), 2022). Throughout the ACT, the CMHA argues that the universal healthcare system in Canada is not truly a universal healthcare system, as there is a lack of equitable mental health care accessible to all Canadians. The ACT recognizes that while mental healthcare is indeed available to everyone, this care is often offered based upon a fee-for-service model, which presents barriers to access. Due to this gap in healthcare policy, the CMHA calls upon the Canadian government to create a Universal Mental Health and Substance Use Health Act. Building upon the ACT for Mental Health, the present call to action focuses specifically on the implementation of integrated mental health care for patients suffering with endometriosis.
The recommendation of this reimagined care model is in alignment with the results of the Biopsychological Chronic Pelvic Pain cohort study conducted by Dowding et al. (2024), wherein participants reported a lack of multidisciplinary care access. The results of Dowding et al. (2024) are closely replicated by Omtvedt et al. (2022), who found that 89% of their research participants did not have proper access to the care of a psychologist, with 42.4% stating that they felt that they deeply needed this mental health care to improve their QoL. Such a model is further supported by scholars such as Young et al. (2017), who demonstrated that gynecologists and general practitioners recognized that patients would benefit from mental health care, but that they did not feel equipped to provide such care. This gap in scope of practice amongst clinicians further demonstrates the necessity of a reimagined care model, such as the one proposed herein.
Limitations and future research
While the present research has significant strengths, such as in-depth qualitative interviews, there are limitations that call attention to the importance of further inquiry on patient experiences with endometriosis and care provision. As the present research was conducted under the time constraints of the received funding, the representation in the sample is relatively limited; future research would benefit from a broader sample of a representative population of women and gender diverse peoples. The conduction of endometriosis research on the limited access to endometriosis care and the associated disparities for Northern, rural, and Indigenous Canadian communities is an area of research which requires further inquiry. Moreover, as proposed herein, the implementation of a comprehensive care model is arguably valuable for most all chronic conditions; the generalizability of these calls to action to other diseases means that it is critical that further research is conducted on the specific forms of biomedical care and psychotherapy that are most effective amongst the specific endometriosis patient population.
It must also be recognized that as endometriosis research has as relatively small prevalence within the literature, it is important to call attention to the continuation of this research, supported with adequate funding and policy implementation, such as that proposed by EndoAct, which seeks to implement policy regarding the funding and support of Canadian endometriosis research and to integrate visions for the future of endometriosis care into practice (Wahl et al., 2021).
Conclusion
As articulated herein, endometriosis is a severe chronic illness with significant implications on the patient’s life course. The present research identifies endometriosis patient dismissal and associated disempowerment, demonstrating the need to move toward a greater ethics of care for this patient population. Guided by participant illness experiences, this research concludes with a call to action for the Canadian healthcare system to integrate a comprehensive care model comprised of both biomedical and psychological care. The goal of this recommendation for care is to alleviate the psychological consequences associated with dismissal, disempowerment, and illness chronicity that endometriosis patients face – it is further supported by existing research as noted throughout this article. To better care, it is imperative that patients are treated with respect, and that they are believed for their pain. The proposed comprehensive care model fosters the tenants of slow, meaningful medicine, characterizing a kind of healthcare encounter that is healing in that of itself (Kleinman, 1989).
Footnotes
Acknowledgements
Thank you to my supervisors, Dr. Rochelle Stevenson, and Dr. Jennifer Shaw, for their support and guidance throughout the conduction of this research. Further, thank you to the research participants, who have provided their insight and shared their experiences.
Data sharing statement
The data generated and or analyzed during the current study are not publicly available nor are they available on request due to the qualitative and interview-based nature of the study whereby details in the interview are inseparable from one’s identity and experiences. Thus, making such data available may compromise the confidentiality of participants.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present research was financially supported via the Undergraduate Research Experience Award Program scholarship from Thompson Rivers University.
Ethical approval
The present research was approved by the Thompson Rivers University Human Research Ethics Review Board. Thompson Rivers University Human Research Ethics Board, Approval #103060
Informed consent
Written consent was obtained by the research participants prior to their participation in the research interviews. Before beginning the interview at the beginning of the meeting, each participant was given the opportunity to ask any outstanding questions about the informed consent form.