
Abstract
Neonatal hypoglycaemia can cause substantial morbidity and mortality. Pēpi Māori (Indigenous infants from Aotearoa New Zealand) are at increased risk. This study explored the lived experience of whānau (extended family kinship groups) Māori having a pēpi at risk of hypoglycaemia. Whānau Māori collectives were interviewed, and transcripts analysed using NVivo software and the Reflexive Thematic Analysis. There were 11 participants (10 whānau collectives; 10 Māmā (mothers) and one Pāpā (father)). The overarching concept of Pā Harakeke (flax bush) framed three superordinate themes, each with subordinate themes. Themes were Whānau, (desire to do the best for pēpi, whakapapa (geneology), collective decision making and whānau led solutions), Shifting the narrative (whānau as part of the team, communication, mana motuhake (self-determination), fully informed) and Health system (colonial health structures, navigation, racism and tikanga (customs)). Whānau Māori narratives provided insight into opportunities for optimising care for those with pēpi at risk of neonatal hypoglycaemia.
Introduction
Globally, neonatal hypoglycaemia affects up to 15% of pēpi (infants). Although the rate of neonatal hypoglycaemia affecting pēpi Māori (Indigenous Māori infants) is unknown, given the higher rates of diabetes in pregnancy and occurrence of lower birthweight in whānau Māori (pregnant people with Indigenous Māori ethnicity; Jowitt, 2016), it is reasonable to postulate that a number of pēpi Māori would be affected. Morbidity and mortality can occur following neonatal hypoglycaemia if untreated and therefore timely diagnosis, identification, and treatment is necessary to help reduce adverse events. There are potential opportunities to improve health outcomes in a pro-equity approach for whānau Māori in the perinatal period by screening pēpi at risk of hypoglycaemia.
In preterm infants, pēpi Māori experience inequitable health outcomes, including higher rates of early neonatal death compared to non-Māori (Edmonds et al., 2021). Edmonds et al. (2021) concluded that “the Aotearoa New Zealand maternity system privileges whiteness, suggesting that clinical care pathways for evidence-based medical care are not delivered systemically and equitably for all”. Reasons contributing to health inequities are multifactorial and intergenerational. The time course starts with colonisation, and the perpetual effects of racist practices, policies, and legislation that has established institutions and health sectors which benefit the majority, Pākehā (non-Indigenous people of Aotearoa; Smith, 2021; Walker, 2004). In 1840, Aotearoa’s founding document, Te Tiriti o Waitangi, was signed and established the relationship between the Crown and Māori. This agreement is for Māori and British citizens to have equal rights. However, there have been ongoing breaches in this legally binding agreement. Over 200 claims have been heard by the Waitangi Tribunal; the permanent commission of inquiry established to address legal claims regarding Te Tiriti o Waitangi breaches. The Health Services and Outcomes enquiry (WAI2575) was heard by the Waitangi Tribunal, which made a series of recommendations for primary healthcare, accountability, and a legislative and policy framework (Came et al., 2020; Clark, 2019). Recommendations included addressing underfunding of Māori health initiatives and the inclusion of Tiriti references in all policy documents in an attempt to address the health inequities caused through colonisation (Came et al., 2020; Clark, 2019). The Waitangi tribunal continues to receive submissions on Crown breaches.
Although the WAI2575 recommendations included improving health outcomes which included pēpi Māori, to the best of our knowledge there is no published literature investigating whānau Māori experience of being informed about risks, diagnosis, prevention, treatment, and follow up for their pēpi at risk of developing neonatal hypoglycaemia. Several Māori models of health care and wellbeing exist including Te Whare Tapu Wha (Durie, 1994), Te Wheke (Pere, 1991) and Pā Harakeke (Metge, 1995; Pihama et al., 2015). The strengths of these models include Te Ao Māori (Māori world views) perspectives and include acknowledgement of other aspects of health and wellbeing not included in westernised biomedical health care models. Given the current health outcomes for whānau Māori and the WAI2575 outcomes it is timely to consider how such models might also apply to whānau Māori with pēpi at risk of hypoglycaemia.
This research aims to explore whānau Māori experiences of having a pēpi at risk of hypoglycaemia. Through this research whānau Māori were invited to lead the kōrero (conversation) for solutions, and to enact their tino rangatiratanga (leadership, authority) and mana motuhake (self-determination). Understanding whānau Māori experiences of having an pēpi at risk of developing hypoglycaemia provides opportunities to support improved outcomes and subsequent lifelong health and wellbeing.
Methods
Participants, hui, and researchers
Using qualitative methodologies this study exploring the lived experience of whānau Māori who have had a pēpi at risk of developing hypoglycaemia. Participants met the eligibility criteria if they were the whānau of a pēpi of Māori ethnicity (self-identified), born at risk of developing hypoglycaemia soon after birth, were over 16 years of age, and had English or Te Reo Māori fluency. Pēpi at risk of developing hypoglycaemia included those whose birthing parent had diabetes, were large (>90th centile or >4.5 kg) or small (<10th centile or <2.5 kg) birthweight, or preterm (<37 weeks gestation) and required blood glucose monitoring in the perinatal period. Exclusion criteria included those not at risk of hypoglycaemia and non-Māori whānau. Based on the research team’s prior experience with whānau Māori and published literature guidance on sample size, 10 whānau collectives were included (Guest et al., 2006; Malterud et al., 2016).
Tāmaki Makaurau (Auckland), Whangarei and Waikato based participants were recruited through previous participation in the hPOD trial (the hypoglycaemia Prevention with Oral Dextrose study); a multicentre, double-blind randomised controlled trial to determine the clinical utility of buccal dextrose gel for the prevention of neonatal hypoglycaemia, and subsequent follow-up studies (Edwards et al., 2022; Harding et al., 2021). Whānau Māori based in Otepoti (Dunedin), were recruited by a consent to approach process by staff located within each Neonatal Intensive Care Unit (NICU), or by self-referral (advertising fliers in whānau areas on maternity and neonatal wards, diabetes clinics). Participants were recruited from several different regions to capture the potential diversity of lived experiences between different hospital sites and regions. Participants were either approached by or introduced to a member of the research team (JR, LK) who followed the consenting process. Hui (meetings) occurred kanohi ki te kanohi (face-to-face) or by zoom and with a Te Ao Māori approach (tikanga (customs), including karakia (blessings), kai (food), whanaungatanga (connections)) in keeping with tikanga processes (Lacey et al., 2011).
Both interviewers are Māori, female, and with diverse qualitative research and clinical experience: an early career health researcher and pharmacist with NICU experience, and a registered nurse with extensive experience in qualitative research.
Data analysis
Audio recorded hui were transcribed verbatim by LR and two Māori researchers (LK, JR) checked for transcript correctness and independently coded the transcripts which were entered into NVivo (version 1.7.1, QSR International 2021). The Reflexive Thematic Analysis was used to identify and report patterns within an interpretive framework using the phases of data familiarisation, data coding, recognition, and rechecking of themes (Braun and Clarke, 2006). An in-person hui occurred with Māori members of the research team (JR, LK, LE) to discuss the coded themes and to finalise thematic analysis. Given the importance of the Indigenous data collected, three Māori researchers reviewed the data and undertook thematic analysis incorporating Kaupapa Māori methodology and the Pā Harakeke model (Cram, 2019; Metge, 1995; Pihama et al., 2015). Data collected during the hui were handled as a taonga (treasure) and in accordance with The Māori Data Governance Model (Kukutai et al., 2023).
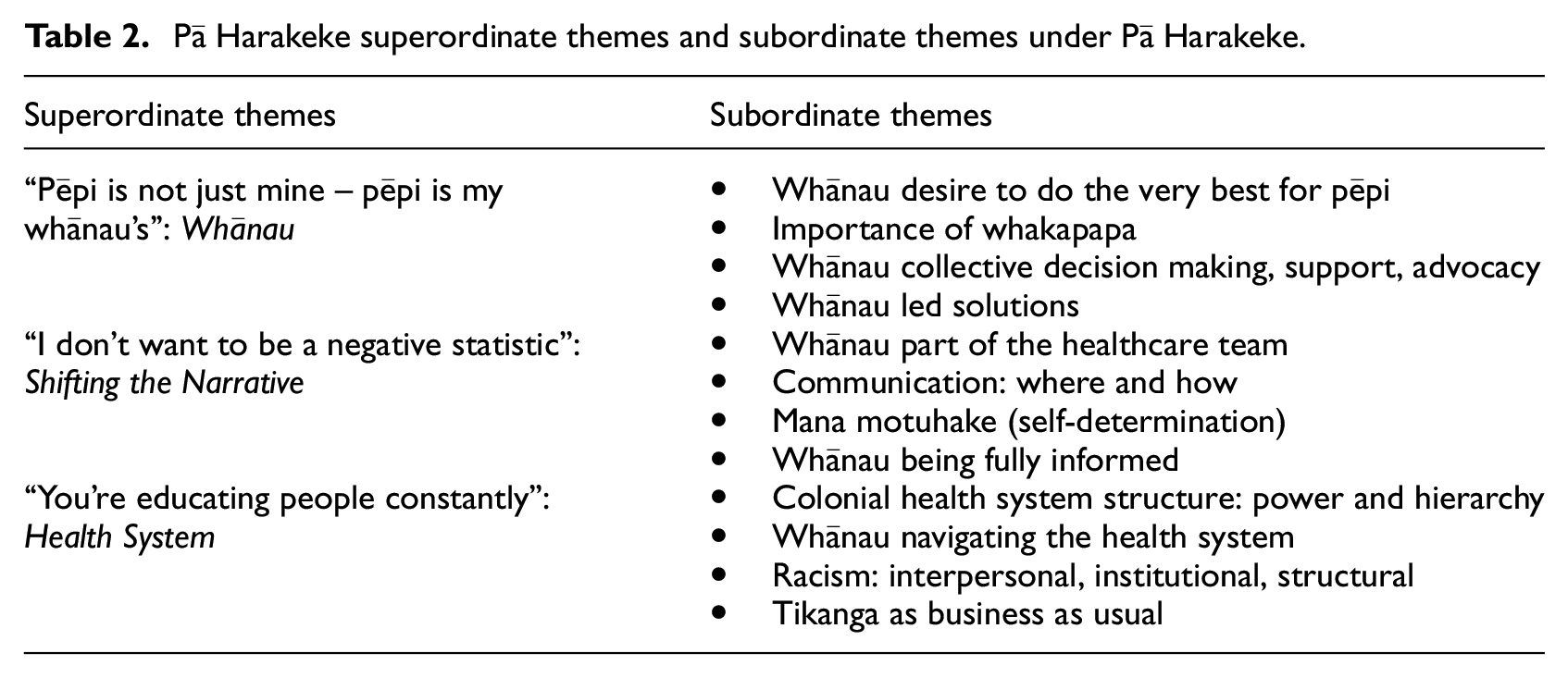
Pā Harakeke has been utilised as a metaphor for whānau and a model of protection for children, and whānau structure and well-being (Metge, 1995; Pihama et al., 2015). At the centre of the plant is the rito representing the baby or child, surrounding the rito are the awhi rito parent fronds or Mātua, then surrounding the awhi rito are the tūpuna and these are the grandparent and ancestor leaves. Analysis of the superordinate themes and subordinate themes were framed around the Pā Harakeke model. Researchers agreed that data saturation had been reached after 10 whānau groups had been interviewed on the basis of consistent themes and agreement between recruiting sites.
Ethics was approved by the Auckland Health Research Ethics Committee (25449). Māori consultation included Ngāi Tahu Research Consultation Committee and advice from the Liggins Māori Advisory Group.
Results
There were 11 participants (10 whānau collectives; 10 Māmā and one Pāpā) who shared their experiences of hypoglycaemia with researcher for up to an hour (Table 1). These whānau lived in five different locations and had pēpi cared for in four different hospitals. The narrative themes identified included three superordinate themes, each with four subordinate themes (Table 2).
Demographic information.
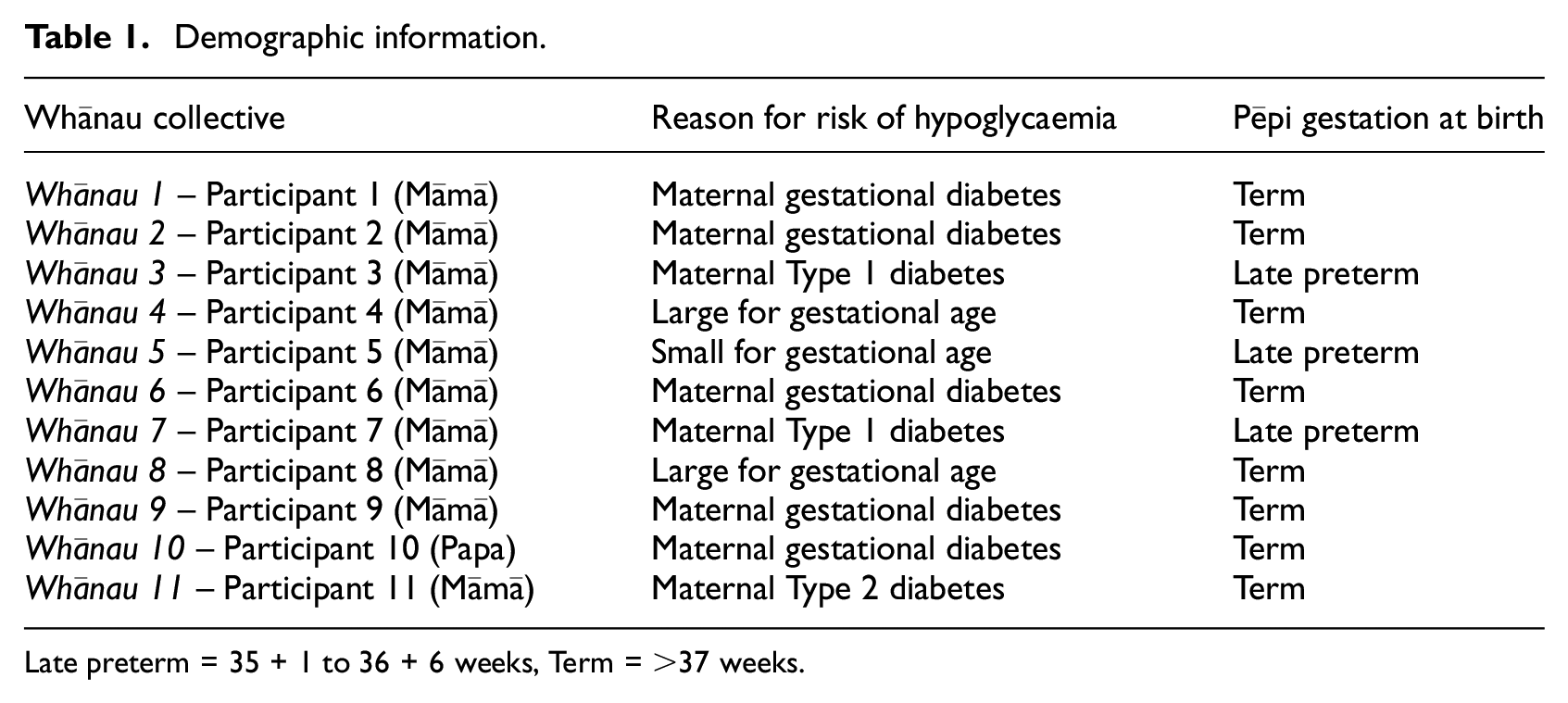
Late preterm = 35 + 1 to 36 + 6 weeks, Term = >37 weeks.
Pā Harakeke superordinate themes and subordinate themes under Pā Harakeke.
Theme 1: Whānau
Throughout all the interviews the importance of whānau was highlighted and discussed by all participants. Different aspects of the theme whānau were highlighted in the subordinate themes identified.
Whānau desire to do the very best for pēpi
After whānau found out that their pēpi was at risk of hypoglycaemia, the response was one of aroha (love) and a desire to do the very best for their pēpi. There were strong responses from whānau wanting good health for themselves and pēpi.
I think it’s important for whānau to, not to put a negative tone on it, but not… but to understand that knowledge is power. So it’s not about understanding the risk in a negative way but it’s how, as whānau we have… we have that knowledge of things that that can take place if our child has this, you know, like I guess it’s all about that prevention space, really, for me as a whānau member too, and that that engagement of so many parts of our health sector for te reo Māori whānau that we are not always ambulance at the bottom of the cliff, and I think that the more that whānau have knowledge and I guess more… knowledge that’s probably even shared on the hapū wānanga space, too, of this could be your journey with your pēpi and… what we can do to have better outcomes, I guess, for Māori…
When being informed about hypoglycaemia risk, some whānau found this difficult, especially those who had challenges becoming hapū (pregnant) and with other medical conditions.
My pēpi is a miracle pēpi. So I was told I wouldn’t get pregnant at all. And so when I was pregnant with pēpi that was firstly a big journey for our whānau to go through because we’ve already done our grieving process, and I had already frozen embryos for a different journey. You know I can say to be told that you are pregnant with this pēpi was one thing, and then also to have that level also that we had at the time of whether or not I would carry her, you know, like whether or not this would be a viable pregnancy. I also had pre-eclampsia. So they had wanted to make sure that she was okay. We tried to keep her baking as long as possible. Yeah. So there was a lot of things going on, and but that was one of my main concerns - didn’t bother me the things that were going on with myself. I just wanted to make sure that she was gonna come out safely.
Whānau felt a sense of responsibility and guilt for causing the need for hypoglycaemia testing, and reflected if there was anything that they could have done differently to prevent their pēpi from needing hypoglycaemia testing (via blood glucose heel prick testing) or treatment (dextrose oral gel or intravenous).
So it is really hard to not feel some level of guilt about that so I think that that when you’re actually visibly seeing um the blood being drawn and at times certainly for my babies it was every two hours, you know their toes were massacred, their heels were massacred there was like there was no spaces left to take that blood and it’s very hard to not feel a little, at least or a lot of guilt and um blame yourself that they’re in that position.
Some Māmā who had Type 1 diabetes, had medical knowledge themselves or a whānau member had medical knowledge, and this knowledge was seen by whānau as an advantage when receiving and asking questions about infant hypoglycaemia. Whānau felt a responsibility to become more knowledgeable about hypoglycaemia.
So I googled it, and got myself educated in that area. And so that’s how we first found out. And so the normal feelings would be around. Now in terms of what does it mean? If it is the case, if she is born, and then she does have hypoglycaemia. Now what are what are the consequences, and then follow on?
Importance of whakapapa
Whānau have described having a deep connection to whakapapa; tīpuna, pēpi, and whānau. There were reflections on the connectedness of whānau and a collective sense of being hapū and belonging to pēpi via whakapapa. For example, when pēpi were needing testing or treatment for hypoglycaemia, whānau used karakia as a way to connect to tīpuna.
Yeah we create this, we can create this bubble. I try… that’s how I try and explain it. So I’m creating this special bubble right now through this karakia in that my belief is that my tīpuna will come when I call this karakia and, you know, it’s the same as our waiata and yeah, and why we why we do that. Because we, you know, we believe in that space of calling our tīpuna to come and be those guides through that time. Absolutely. What do you do on that end of the spectrum when that’s like they are the newest part to your whakapapa, how do we nurture that conversation in ways that makes cultural embedded sense to us, as well as the practical stuff like I think it’s always a balance but if there’s a tikanga led process then we totally understand the practical need to do the heel prick tests because we know that oh that’s just about protecting your whakapapa, all good, let’s do it.
Whānau collective decision making, support, advocacy
The whānau interviewed reported that when whānau were in any health setting, whānau would like to know who the staff are that are present, and what their role and contribution is to the healthcare team and their whānau. They described in the narratives that when whānau are engaged with what is occurring they want to ensure that they are actively part of the health journey, and that healthcare is not something that is done to whānau but with whānau. A whānau member who has medical knowledge is often present at various stages of the healthcare journey and is there for support and advocacy.
We didn’t have that sense of oh, holy shit the world is going to fall in, type thing. It was basically like, it is what it is, and this is the potential of what could happen. And this is what we can do about it and then make a decision. I can’t do this alone, because pēpi is not just mine –pēpi is my whānau’s.
Whānau often discussed health decisions as a collective. Although not all whānau were able to attend clinic and hospital visits, the whole whānau share the childbirth journey, supporting and being there for each other. Whānau also shared experiences of advocating for their pēpi, and in some situations feeling judged for doing so.
Well, I feel that there’s like a bias that, yeah, you’re a big mum and you have a big baby. There’s going to be issues. And that’s not always the case. I just grow massive, healthy, healthy babies.
Whānau led solutions
Whānau requested that they be fully informed of what to expect following hypoglycaemia testing of pēpi, when and what follow up they should receive, and what both the short term, medium term, and long-term best practice monitoring plan is. Whānau thought about the future, and any involvement in providing feedback was from the perspective of benefit for future generations. Whānau led solutions were highlighted throughout their narratives.
I want to be included and wanted my whānau voice to be there is that we need more research for Māori whānau as we navigate through the colonised health system that we deal with. And so I wanted us to have that research data there. It might be better next time. This might help someone else. It’s just that support for the whānau and also, yeah, the idea of having our doctors and also midwives clarifying some things around the tamariki and what they might be. You know what’s going on with them internally, I think that those things could be probably better. It can be photo or video showing the baby’s heel. Because I imagine a lot of parents probably wouldn’t be expecting their child to have holes in their feet for quite a while after.
Theme 2: Shifting the narrative
Whānau highlighted that “I don’t want to be a statistic” and discussed the need to shift the narrative. As part of the narratives whānau shared their lived experience of Māori health inequities and are aware of the unjust colonial healthcare system they access. Alongside these experiences they also emphasised the need to shift the narratives towards where they wanted to be in the healthcare experience.
I want to be included and wanted my whānau voice to be there is that we need more research for Māori whānau as we navigate through the colonised health system that we deal with. And so I wanted us to have that research data there. And so you know, I knew when I was due for testing, it was probably going to come back that we were quite high, if not that we would be a hapū diabetic pregnancy. I still was gutted. I’ll be honest. You know like it did change a lot for us on that day when they rang us. Like ahhh just… I had done everything in my power I felt to try and not be that statistic. I think that some of us as Māori whānau do that a lot, you know, like we worry that that’s another negative statistic actually for our people.
Several subordinate themes are described below.
Whānau as part of the healthcare team
When whānau had the opportunity for whanaungatanga with members of the healthcare team this led to whānau feeling a sense of safety. However, whānau were also highly tuned to notice when healthcare professionals appeared to be desensitised when providing care vs caring for their pēpi. Opportunities for whānau to be part of the healthcare team supporting pēpi and whānau during this process were identified.
It was about getting the blood out more easily and things like filling up a glove with hot water and resting their heel in it and things like that, just to make the flow um… better. And so just those little things that made you feel like this person cares about your poor little baby’s foot, you know? But I think absolutely having nurses and carers that really understand and really um try to connect with you because you are kind of just a number in the system and often you’d be there for many, many shift changeovers and you’d have nurses going home and then coming back for two weeks you know or longer. So I wonder if it’s a little bit like that where they might do that every day so they might do those heel pricks every day to lots of other babies, but she was our first baby that was our first experience so it’s sort of to honour that’s a whānau first experience.
Communication between whānau and healthcare team: Where and how
Whānau articulated the wish to have information about hypoglycaemia, especially risk and testing, communicated to them in a way that considers them as the receiver of information, and delivered in a way that creates opportunities for whānau to ask the questions they need to. One whānau mentioned that they received information about hypoglycaemia risk and the need for testing during their caesarean section and another by a phone call.
Oh, yeah, low blood sugar and she had to have a feeding tube. Yeah, but my husband, because I had a C section [caesarean section] and they took her off me straight away. Pretty much so, my husband and Mum were with her. They stayed down there because I was quite sick. I had lost a lot of blood with her. So yeah, I didn’t get to see her till the night, so I had her like around midday 12, ish? But I didn’t get to see her until late. Maybe 8 o’clock at night. Yeah, that was hard. My midwife was like “why did they tell you over the phone, they should have told you to make an appointment with me.” You know, and because she goes, “I’ve got that through an email.” But she yeah, she at the time she was like, “why were you told over the phone?” and I was like, you know, I don’t know. But we need to deal with this.… . I was like, why am I getting told this [risk of hypoglycaemia] over the phone, why am I getting told to make an appointment? You know that this should be a back-office thing where my midwife is reaching out and saying “could you come in to see us?”
When being informed about pēpi hypoglycaemia risk, whānau felt responsible for being part of the cause for the risk of hypoglycaemia and concerned about the health journey ahead of them and their pēpi. Communication was highlighted as important given the significance of the diagnosis and the interventions then required to keep pēpi well.
But I yeah again, you know, just those Mama guilts, especially in the last kind of like home stretch finding these [hypoglycaemia risk] things out. And because I don’t think we’ve ever dealt with …like high blood sugars or anything like that in our whānau. It wasn’t until about… I was over 35 weeks along, and then I was told that I had GD [gestational diabetes]. And so then they of course told me about like the risk factors [of hypoglycaemia], mostly around baby, so that’s sort of how I was told, but more in a scaremongering way, so I was really frightened. So it really coloured, I think, my whole experience of pregnancy. That it had been fine and good up until that point. And then the language that was used carried a form of that I’m negligent, right?
Mana motuhake (self-determination)
Whānau described both feeling empowered and then experienced disempowerment by the healthcare team, and the health system, when health provision happened to them, rather than with them. Whānau shared experiences of healthcare delivery that occurred without explanation, resulting in disempowerment, and others asked questions to enable enactment of mana motuhake, especially around tikanga.
So maybe we get written off a little bit like they wouldn’t understand or they didn’t ask so we won’t tell them… I’m pretty lucky in the sense that I can go and process things, and I also had…I’m quite happy to ask questions at the time, so no the people that did deal with me were pretty good. I am lucky that I can hold that space, and that I will say things like I want karakia that I… that I want whānau support, you know. yeah, cause it’s a very it’s a very special space as, as you know, you know. And that’s, I guess, why there is that mamae and that grief when you get told that you have to birth in a hospital, because you just feel at times that it’s such a sterile non space where things could happen.
Whānau being fully informed
Whānau reflected how they were informed about decisions and also how they often were not fully informed of hypoglycaemia test results and the lack of follow up, and support following provision of information. Whānau were also highly perceptive of healthcare professionals being unable to notice when whānau were needing more support and facilitating access to support. The sharing of information, as part of being fully informed, was noted by whānau as having an impact on their experiences.
I would have loved to have been, I guess more informed, because I didn’t really understand exactly what was going on. It was more like this info was just thrown at me and deal with it how you will. And I’m very, very aware of when … . that doesn’t feel right, and for me I think it’s really just making sure there are lots of questions asked and reading whether the person feels comfortable or not because if they don’t seem to be feeling comfortable then they’re not going to really have the ability to listen and take in everything they need to, and feel comfortable enough to question…
Theme 3: Health system
The third theme identified by whānau were their interactions with the health system “you’re educating people constantly.” Whānau discussed their experiences of both challenges and also solutions to meet these challenges within the health system. Whānau articulated their need to interact with the health system along with the challenges and the benefits of these interactions.
I think that [hospital] was obviously the best place for her and I, and then she ended up in NICU, so I’m grateful that actually I had that place where, I was like you are the medical professionals and I trust you with this, so I will challenge you on some things, and especially around my tikanga, and how, you know, I can ensure that my whānau can still be part of this journey, but I will not challenge you if I know and trust you, that you want the best for myself and for my pēpi, yeah.
Colonial health system structure: Power and hierarchy
Whānau discussed how they were aware of the power and hierarchical health system, and how this influenced communication between themselves and healthcare professionals. Whānau reported that they felt disempowered to ask questions in certain situations, and how other whānau members got push-back when they did ask questions. When whānau were exerting their tino rangatiratanga and mana motuhake, the response from some healthcare professionals included a lack of support and withdrawal of care.
But certainly, for me, whenever I look at medical intervention or medical experiences, it’s that’s very much about a perceived power imbalance. One would always think that the person that’s communicating to you has all the knowledge and because of that generally holds the power, so it’s often not, it might not feel appropriate to question or to or you might feel like, it’s not… like it wouldn’t be right to question some of the things they were saying or, or be inquisitive about it. So, I guess being aware that when you’re communicating … that there might be a perceived power imbalance well that you might not feel your dominance. like dominance in that relationship for most receivers, but fear you are. I said to him but my GD [gestational diabetes] is managed, my blood pressure’s fine, and he just said, well, this is just what I recommend for all mums that have GD. And then when I questioned him some more, with some literature, he said, oh well, if you want to do it your way, you’ll have to sign a waiver and I won’t help you, right? Yeah. And, like, let’s just book in a date and get it done, like an induction. And, yeah, and then it was framed further in the discussion as, you’d be totally negligent if you chose to do anything else but what I want you to do.
Whānau felt distressed and disempowered to change things in certain situations, especially if pēpi were removed from them for the healthcare professionals to provide care. Also, whānau who had unmet health needs, discussed that this resulted in a late diagnosis and a negative health impact on pēpi. When these health needs were brought to the attention of healthcare professionals, māmā and pēpi were often not viewed as a collective, and rather treated as individuals despite them being whānau.
I was separated from her and so I think that was really distressing to me that like you can have a brand new baby and I remember I was crying because I couldn’t remember what her face looked like right like because I wanted her yeah so I was like I just I think it’s weird that she’s just through that door and she should be with me. Yeah, and so that felt like, I think it probably took like less than an hour, but it felt like it was forever.
Whānau shared experiences of being in an unwanted position of educating healthcare professionals on tikanga due to their lack of knowledge and acknowledged the added responsibility that came with this.
It’s also like you feel sometimes that you’re educating people constantly. I’m like, you know, it’s not a karakia to God. Or you know, this is a karakia for us to have this space so that it’s a safe space for us.
Whānau navigating the health system
Whānau repeatedly highlighted a lack of information provided about follow up, and/or that follow up after hypoglycaemia testing did not occur, despite whānau being engaged and aware of what should happen during their care and wanting to have good health outcomes.
No, but it [follow up] would have been nice, they’re healthy. But it would have been nice to know if I needed to have a follow up. Or if there was anything that I could have keep an eye out for like, like, my kids are always on the 90th percentile for everything. …. But it would be good to know, especially because we’ve got a family, a whānau history of diabetes.
Racism: Interpersonal, institutional, structural
Whānau shared experiences of interpersonal, institutional, and structural racism (in all its forms) through their narratives. Stereotyping of whānau alongside racism were also experienced and described. The potential impact on their care was highlighted alongside lived experiences of bias and assumptions described in the narratives.
I just grow, and our family grow big babies. It’s not to do with me having gestational diabetes or anything. And that’s I, I believe that that there was the assumption made that I was cos I’m a big mum that that and yeah, but there was no discussion - this is why we’re doing it. Hey, are you okay? Are you happy for us to do it? It was just basically this is what we have to this is what we’re doing. Oh, she’s a Māori baby and I hate to say like that. And then, yeah, then they were like, oh, your baby’s jaundiced, and her levels are very, very high. So, we need to put her in NICU, and we need to put her in a bilibed and I was like ahh that process was again. I think, you know, you’re emotional, anyway. Had a bit of a cry about that. But then, yeah, within the 24 hours, it’s like this is the best place for her. Or before that nurse has walked on the ward nurse said big mum, Māori, big baby, it’s got to be something wrong. That’s that. And I just I hate that assumption. Because you get it everywhere, wherever you go. And as soon as you say, how do you What’s your nationality? You know, I’m a New Zealand Māori. Oh. It is and it’s such a bias that people…And then as soon as they see your other factors. Oh, big, oh yeah. They don’t take care of themselves. They won’t take care of the baby.
Tikanga as business as usual
Whānau carried out tikanga as business as usual for them and reflected on how this can occur within the provision of healthcare, including clinical care and communication. The importance of tikanga and how this should and can be business as usual were highlighted by whānau as part of healthcare provision and examples of this discussed.
We prayed before my birth. My husband did a little prayer. Just me, my husband and baby. There wasn’t really much people around, cause I was fine. To be honest I liked it liked with just me and my kids and my husband. My whānau when we present to a Pākehā world health thing seems that we are not Māori so, therefore we are a bit of a shock to them when we also all kōrero Māori and then also we’ll say, you know, um, and you know I did say to them too that there would be waiata and there would be karakia, and that was a bit of a shock, I think, to the teams. I would just hope that they would understand that it should be an offering for all people actually, that Te Ao Māori space and offering of what makes you culturally feel safe should be offered to all. It’s whakawhanaungatanga it’s being able to connect and getting to know someone deeper than just…this is the update for you. It’s really just showing that care and really committing to a relationship. Even if you’re never gonna see them again you’ve got them for those 12-hour shifts, you know? So, it’s really being able to feel that you’re not alone up there.
Discussion
This study highlights and explores the lived experience of whānau Māori who had a pēpi at risk of developing hypoglycaemia and is the first of its kind to outline their lived experiences of these journeys. The sharing of the lived experiences provides learnings and opportunities for health professionals who are supporting whānau who have pēpi at risk of hypoglycaemia. These learnings can be integrated into the health system, and also into the development of national guidelines for Aotearoa. The depth of the kōrero provided by whānau participating is a taonga in itself and provides examples of Te Ao Māori learnings for a wider cohort than just whānau Māori. Pausing and reflecting on what has been shared by whānau provides the opportunities for future improvements in care.
The Pā Harakeke theme was used as part of the data analysis for this study and is a metaphor for supporting pēpi within the whānau collective has been described in other literature (Pihama et al., 2015; Watson, 2020). The first theme, Whānau, highlighted the concept of pēpi being nurtured within a wider collective is a narrative likely to resonate with many whānau in their hopes and aspirations for pēpi being well and thriving. Health care professionals are well placed to recognize and support whānau in their positioning as a resource and support for pēpi. These findings are in keeping with other models that support pēpi to grow and thrive including the work on attachment which highlights whānau as a resource throughout the generations (Mikahere-Hall, 2020).
The second theme identified was Shifting the narrative. Often the narrative described in literature is one of deficit and comparison to the “norm” which all too often is non-Māori and negative in the description and potential expectation (Reweti, 2022). The recognition of the whānau as a resource and team members in the care of their pēpi empowers both the whānau and the clinical teams to optimise outcomes and contribute to the flourishing of the pēpi (Reweti, 2023). It could be suggested that Family Integrated Care (used commonly in Neonatal Intensive Care Units) could be Whānau Integrated Care, with a shift to empowerment and a change in the narrative and discourse for whānau (Parai, 2020). Literature supports the use of relational models of health to improve wellbeing (Wilson et al., 2021). Whānau within this research provided solutions through the suggestion of shift the narrative and its impact on care.
The third theme highlighted by whānau included their lived experience of the health systems. This included racism in all its forms, which had a direct impact on whānau and pēpi. Harris et al. (2024) reported that racism within general practice settings can lead to negative experiences of healthcare with resulting lower satisfaction, which aligns with our findings. Racism has also been shown to be a social determinant of health, with an association with inequitable health outcomes (Talamaivao et al., 2020). Cultural safety education for health professionals, both in training and practising, is a mechanism for helping dismantle institutional racism and will contribute to eliminating health inequity associated with this social determinant of health (Curtis et al., 2019).
Also within the third theme were the challenges associated with navigating the health system and the potential opportunities to improve this journey, as has been highlighted elsewhere (Brown, 2018; Goodyear-Smith and Ashton, 2019). This included the potential prospects of tikanga becoming business as usual so improving whānau experiences and cultural safety within a universal and individual focused care system, opening the prospect of improved experiences of care and engagement of the system to meet whānau needs. The benefits of Kaupapa Māori intervention in health have been demonstrated and our study is in keeping with this evidence (Rolleston et al., 2020).
The sample size could be considered a limitation of the study, although given the qualitative approach of this research and the in depth kōrero and perspectives offered the sample size is in keeping with other research (Vasileiou et al., 2018). In addition, similar themes emerged throughout all the narratives suggesting consistency within the analysis. Given that the whānau largely self-selected or had existing relationships with the researchers, there is the potential that there are other unheard lived experiences of whānau Māori and future mahi especially involving Pāpā is needed. The use of whanaungatanga for recruitment into this study is in keeping with other Māori research methodologies and supports the connectedness within this research given the challenges recalled by many whānau. Exploring these themes with intergenerational whānau groups highlighted other aspects of the harakeke model and these narratives and whānau experiences of the system to developed themes in keeping with collective approaches for whānau. The important of whānau voice has been highlighted by others and this study contributes to this body of evidence (Palmer et al., 2019). Having Māori researchers involved as principal investigators, interviewers and with data analysis has provided the opportunity to use a strength based non deficit lens to the study kaupapa and provided support both for the researchers, the kaupapa and whānau involved.
The lived experiences of whānau Māori who have a pēpi at risk of developing hypoglycaemia offers solutions to optimise care and outcomes. These include the importance of whānau led solutions, shifting the narrative and health systems and tikanga as business as usual. This is the start of influencing health care service provision for whānau in the future for the benefit of all pēpi and their whānau.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251330098 – Supplemental material for Experiences of whānau Māori with pēpi at risk of neonatal hypoglycaemia: A qualitative study
Supplemental material, sj-docx-1-hpq-10.1177_13591053251330098 for Experiences of whānau Māori with pēpi at risk of neonatal hypoglycaemia: A qualitative study by Jenny Rogers, Lisa J Kremer, Jane Harding, Orla Walsh, Lily Roberts and Liza Edmonds in Journal of Health Psychology
Footnotes
Appendix 1. Glossary
Disclaimer: Many of the descriptions used in this glossary are specific interpretations for this publication, and do not denote the fullness of meaning normally associated with the word or term. All efforts have been made to uphold the taonga of each kupu within the writing of this publication.
Acknowledgements
The authors wish to acknowledge the taonga that was gifted to them through the sharing of lived experience by whānau. For their guidance on the design of this study we would like to acknowledge the Neonatal Hypoglycaemia Guideline Governance Group.
Author contributions
Study concept: LK. Study design: JR, LK. Drafting study protocol: LR, OW, LK, LE, JR, JH. Funding application and ethics: JH, OW. Data collection: JR, LK. Data analysis: JR, LK, LE. Reviewing of manuscript for intellectual content: All authors. All authors agreed on the final paper for publication. All authors read and approved the final manuscript.
Data sharing statement
Full transcripts of interviews from participants will not be made available under Māori data governance protocol Te Mana Rauranga. All material that can be shared is included in the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Ministry for Business, Innovation and Employment and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health (NIH; grant R01HD091075). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NICHD or the NIH.
Ethics approval
This study was approved by the Auckland Health Research Ethics Committee (reference number 25449).
Informed Consent
All participants gave written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.