
Abstract
Elimination of burnout and work-related mental illness in hospital doctors, at least in the short term, is unrealistic. Supporting doctors’ recovery continues to be important. Despite this, the aftermath of work-related mental illness and burnout, is not well understood. Using a descriptive phenomenological method, we describe the experience of coming to terms with mental crisis perceived to be caused or exacerbated by work stress for six senior consultant hospital doctors. Findings show that, in the aftermath of crisis, doctors engaged in two types of reflection: ‘situational sense-making’ to make sense of their experiences and ‘transformative self-reflection’, reflection in a deeper way on the experience, themselves and their lives. Transformative self-reflection led to change and in some cases growth. Not all doctors engaged in transformative self-reflection, and the process of recovery was complicated by contextual factors and when support from employers was perceived as absent, poor or acrimonious.
Keywords
Introduction
Over half of practising physicians experience work-related mental illness or symptoms of burnout (Rotenstein et al., 2018). A doctor is more likely to take their own life than a member of the general public (Gerada, 2018) and work-related stressors are more frequently associated with physician than non-physician suicide (Ye et al., 2021). In Ireland burnout, as conceptualised by Christina Maslach, may be present in almost 30% of hospital doctors (Haire et al., 2024; Hayes et al., 2019). Maslach’s conceptualisation defines burnout as a three-dimensional syndrome: emotional exhaustion (feeling drained and unable to cope), depersonalisation (cynicism and detachment from work or people) and reduced personal accomplishment (feeling ineffective or unproductive; Maslach and Jackson, 1981).
Extensive research into burnout among doctors has identified systemic factors like extreme work demands (West et al., 2016) lack of opportunities for adequate rest (Walsh et al., 2019), individual factors like perfectionism (Montgomery, 2014; Patel et al., 2018; Stehman et al., 2019) and cultural factors including expectations of high performance, blame culture and management-doctor conflict (Montgomery, 2014; Walsh et al., 2019). Research into the impact of burnout has highlighted a potential knock-on negative effect on patient care including increased medical errors and adverse events and poorer clinical outcomes (De Hert, 2020; Patel et al., 2018; Stehman et al., 2019).
While prevalence, antecedents of burnout (Kumar, 2016; Rotenstein et al., 2018) and prevention (Ahola et al., 2017; Panagioti et al., 2017; West et al., 2016) of burnout have been the subject of much research its elimination in the short term, is unrealistic. Burnout has been consistently identified in medical populations since 1978 (Sweileh, 2020) with systemic antecedents not easily resolved (West et al., 2018). Supporting doctors’ recovery is therefore crucial, yet the aftermath of work-related mental illness and burnout, including the recovery and return-to-work phase, remains poorly understood (de Vente et al., 2008; Korczak et al., 2012).
Interventions combining workplace modifications with treatment show promise (Ahola et al., 2017). Cognitive behavioural therapy effectively reduces emotional exhaustion but does not consistently facilitate return-to-work (Korczak et al., 2012). Recovery from fatigue, including time for rest, predicts return-to-work (Ekstedt et al., 2009; Sonnenschein et al., 2008) but personal recovery processes have received limited attention (Korczak et al., 2012).
Qualitative research on burnout in doctors highlights organisational factors and group dynamics as antecedents and protective factors of burnout showing that doctors identify numerous organisational factors as originators of burnout but envision protecting themselves individually (Sibeoni et al., 2019). A phenomenological study of general practitioner (GP) partners in distress identified conflicted doctor identity and workplace relationships as key contributing factors (Spiers et al., 2020). Despite extensive qualitative research on risk factors and interventions, personal experiences and aftermath are not explored (Sibeoni et al., 2019). One study that included recovery, focusing on hospital doctors in training, found that recovery involved nurturing personal lives, reframing unrealistic self-expectations and setting boundaries with patients (Abedini et al., 2018). Many trainee doctors in Abedini’s study attributed recovery to nurturing their personal lives, reframing unrealistic expectations they had of themselves to perform to their internalised ideal of the ‘good doctor’ and learning how to set boundaries with patients. Building on this, our study examines specific recovery processes in a more senior cohort of doctors.
To date, no phenomenological studies have explored the role of reflection in burnout recovery, particularly among senior consultant hospital doctors. We propose that mid- to late-career consultants, without prior mental illness, experience work-related mental crises as uniquely significant, negative life events, warranting focused study.
The aim of the current study is to provide an in-depth, descriptive, phenomenological analysis of the reflective processes used by senior hospital doctors, in recovery from burnout or mental health crisis perceived to be caused or exacerbated by work stress. A descriptive phenomenological method is adopted to achieve these aims, as such methods, which capture participants’ voices and personal narratives, are lacking and are critical for understanding their experiences and guiding the relevant support interventions in recovery (Malpert et al., 2017; Riessman, 2002).
Methods
Research design
In this research, the experience of recovering from and coming to terms with a mental illness perceived to be caused, or exacerbated by work stress, as a senior consultant hospital doctor, was studied. Amadeo Giorgi’s descriptive phenomenological analysis (DPA) methodology (Giorgi, 2009) was chosen to examine the phenomenon of ‘coming to terms with’ a mental illness perceived to be caused or exacerbated by work stress. On preliminary analysis, the phenomenon of reflection was strongly evident as a key component of the experience and the DPA method was used to examine, in-depth, the phenomenon of reflection in this context. The decision to narrow the focus of the DPA to the phenomenon of reflection was taken for three reasons. Firstly, describing specific internal processes applied by doctors in coming to terms with mental illness was considered more valuable than providing a broad description of experience, as it was deemed to have greater practical potential for recovery. Secondly, understanding processes of recovery was deemed to add new insight to the research already conducted by Abedini et al. which looked more generally at the experience of recovery. Finally, phenomenological designs, and in particular the DPA method, are known to produce more powerful results with a narrow focus due to the detail-oriented method and essence-seeking approach which necessitates a clear and focused phenomenon to study (Cresswell, 2013; Giorgi, 2009; Tindall, 2009; Van Manen, 1997). A further rationale in selecting the DPA method was to give precedence to the physician’s voice and subjective experience. Two key methodological elements amplify its effectiveness in representing experience closely, ‘phenomenological epoché’ or ‘bracketing’ and ‘free imaginative variation’ described in the Supplemental Material.
During the phenomenological analysis of the data, two distinctive forms of reflection were identified, and data was sufficiently rich to determine an essential structure of both forms of reflection. A deductive content analysis was conducted to provide participant-specific information relevant to the phenomenon such as their illness and help seeking experiences and the context within which they were working.
Participants and recruitment
A sample of 20 consultant doctors was purposefully selected, to include a mix of genders, specialties, hospital locations and sizes, from 53 doctors who volunteered to participate in qualitative research following completion of a wellbeing survey (Hayes et al., 2017). From the 16 interviewed (4 dropped out due to work commitments), six were selected for analysis based on inclusion criteria: (1) burnout and/or mental illness experienced, (2) burnout and/or mental illness perceived to be caused or exacerbated by work stress and (3) professional help availed of. Two of the six interviewees were female born and female identifying, the remaining four were male born and male identifying. Interviewees’ career stage was mid to late consultant level (approximate age 45–65 years). Specialties represented in the sample include four acute, front-line specialties and two diagnostic hospital specialties.
Data collection
Ethical approval for the study was obtained from the Royal College of Physicians of Ireland (RCPI) ethics committee and the study was overseen by a stakeholder group with medical representatives from various specialties and grades who gave guidance from a participant perspective. Face-to-face interviews were chosen due to the potentially sensitive nature of the topic at a location chosen by the participants from the following options: their place of work, their home or a private meeting room at the RCPI. Due to the sensitive nature of the topic and the small numbers of doctors within in some specialties in Ireland, confidentiality and anonymity were considered of high importance to participants and were key components of the study design. All potentially identifiable data including references to people, places or very specific events were anonymised in transcripts before analysis. Written, informed consent was obtained. Participants were advised of their right to opt out at any stage. Participants were interviewed in person about their experiences of work stress, mental illness, help-seeking and recovery according to phenomenological interview guidelines (Giorgi, 2009). Following three pilot interviews, conducted by GW with volunteer hospital doctors who were not participants in the study sample, the research team met to review the interview process and ensure adherence to phenomenological guidelines. Interview questions were open and focused on participants’ experience of ill health related to work stress. The two questions which generated the most discussion were: ‘tell me about your personal experience of work stress?’ and ‘Did you ever feel your work stress was impacting your health? If so, tell me about this time’. The interviewer continued to draw out the details of the experience of coming to terms with work-related ill health according to the specifics of each participant’s experience in an open and conversational manner. Interviews were conducted by the first author. Interview transcripts were returned to interviewees for comment if requested. Two were requested, provided and returned to researchers with minor amendments to clarify points made or request details which may have identified people or hospitals discussed within their narratives to be anonymised.
Analysis
The transformation from raw data to the essence of the phenomenon was performed according to Giorgi’s DPA methodology (Giorgi, 2009). The key steps of the analysis method including the process of bracketing and free imaginative variation and examples of the analysis are provided in Supplemental Material. Analysis of one interview was conducted by GW and SD who then met twice to discuss their analysis and ensure adherence to the method. The remaining five interviews were analysed by GW in regular consultation with the full research group (YF, SD, BH) as required for challenging cases or sections of raw data. All authors cross-analysed two interviews. GW developed the preliminary structures of the phenomena which were reviewed and finalised by the full research group. The final findings consist of the essential structure of the phenomena and a description of key elements of the phenomena, known in Giorgi’s method as the key constituents.
A deductive content analysis was conducted by GW and reviewed by YF, SD and BH to provide a description of the sample in terms of work context, illness experienced, help-seeking attempts, social support available to participants at the time of illness and a snapshot of where participants were with respect to their recovery at the time of interviewing. This analysis is intended to provide a backdrop within which to interpret the descriptive phenomenological analysis only and is not the primary focus of the study.
Findings
Our findings are presented in two parts: results of the content analysis and the results of the DPA on reflection.
Results of content analysis
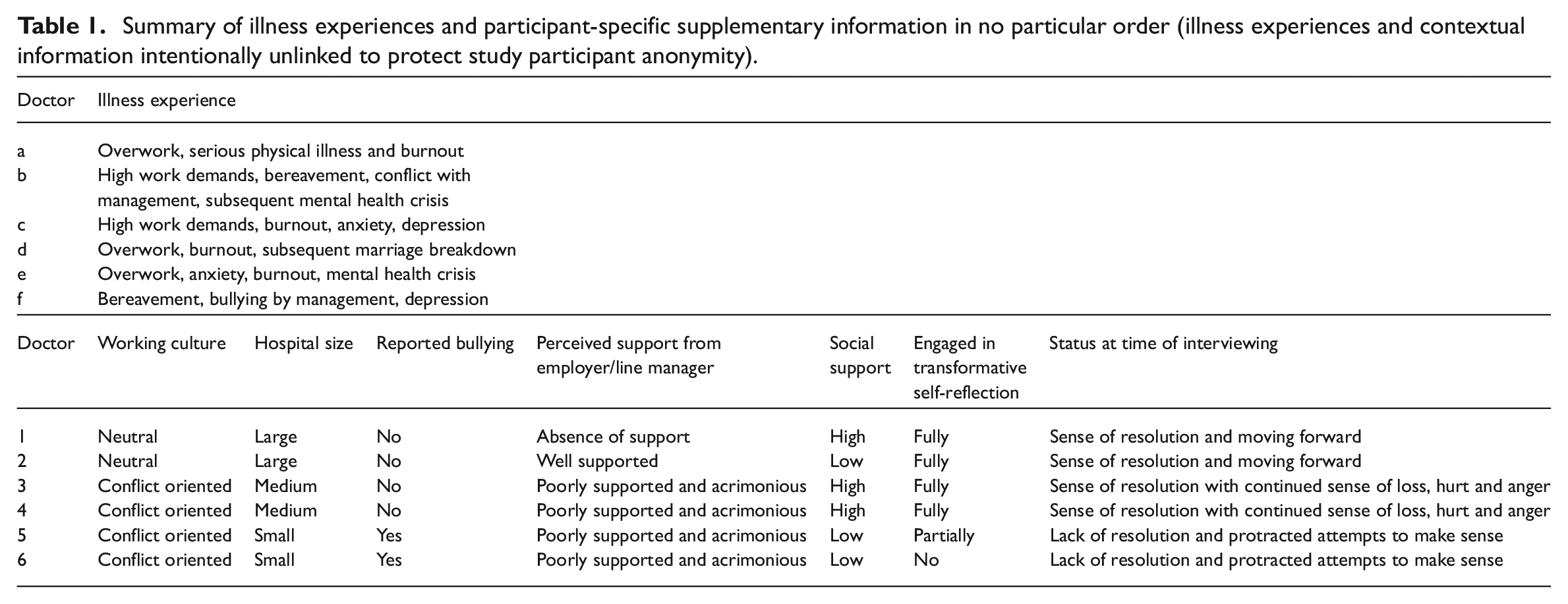
A summary of the results of the content analysis is provided in Table 1.
Summary of illness experiences and participant-specific supplementary information in no particular order (illness experiences and contextual information intentionally unlinked to protect study participant anonymity).
Illness experience
Participants’ illness experiences included burnout, anxiety and depression and were perceived by participants to be caused or exacerbated by work stress.
Perceived quality of the help-seeking experience
The quality of the help-seeking experience was perceived as positive or neutral by two of the doctors but perceived very negatively by the remaining four doctors and dominated by a lack of support from, and acrimony with, their employer. Generally positive experiences with primary care physicians, private healthcare, occupational health and employee assistance programmes were overshadowed by lack of support and acrimony from the employer which persisted in some cases throughout recovery and return-to-work.
Context: Working conditions, culture, hospital size
All participants described working conditions involving excessive hours and inadequate staffing to meet patient needs. Four participants worked in environments characterised as conflict-oriented, with delays in staff replacement and instances of bullying by management. In contrast, two participants, although also facing extreme workloads, felt supported by colleagues and worked in larger departments where workloads were managed collaboratively, and recruitment challenges were less severe.
Social support
The level of social support varied among participants. Three participants reported high social support, which included having a supportive spouse, friends or family with whom they could share their stresses and mental health struggles. The remaining three participants had low social support, with no supportive spouse and limited or no help from friends or family during their illness.
Psychological status with respect to experience at time of interviewing
At the time of interviewing, in two cases there was a clear sense of resolution and moving forward from the experience of mental illness and associated help-seeking. For two of the doctors there was some resolution and a sense of moving forward, however, feelings of loss, hurt and anger remained. For two of the doctors, there was a lack of resolution, and they appeared to be still in a process of protracted sense-making and rumination.
Results of the descriptive phenomenological analysis
In the analysis it was identified that doctors engaged in two different types of reflection to come to terms with their experience. The first is a process of reflection, which helps individuals to understand and make sense of their experience. We refer to this process as ‘situational sense-making’. The second is a deeper process of reflection and contextualisation of the experience that is accompanied by transformative change in the lives of participants. We refer to this process as ‘transformative self-reflection’. Using the methodological steps of the DPA, it was possible to define a fundamental structure for the phenomenon of situational sense-making and a fundamental structure for the phenomenon of transformative self-reflection. Each structure is built on essential themes, known in Giorgi’s method as key constituents. For clarity, we first present a brief overview of the distinction between situational sense-making and transformative self-reflection as determined by our analysis. This is followed by the essential structure of each phenomenon and key constituents of each structure.
Situational sense-making versus transformative self-reflection
Situational sense-making is concerned with working through and making sense of specific events. In the process of transformative self-reflection, individuals reflect in a deeper way, on themselves, their lives, their history and the experience, and this deeper reflection leads to change (see Figure 1 for a schematic representation of the two phenomena and how they differ). The data suggest this distinction; however, it is important to note that the processes are closely linked and a clear boundary between where situational sense-making ends, and transformative self-reflection begins does not exist. Although it is likely that some situational sense-making occurs first, as events unfold and individuals begin to process what is happening, there is no linear relationship in time between situational sense-making and transformative self-reflection. Individuals can engage in both in parallel and iteratively. Both types of reflection occurred during all stages of the experience from mental health crisis, through help-seeking, recovery and long after. It is not possible, from our data, to say definitively that situational sense-making did not lead to some transformation in the lives of study participants, it likely did. However, in our dataset, those who engaged in deeper reflection experienced greater transformation in their lives.
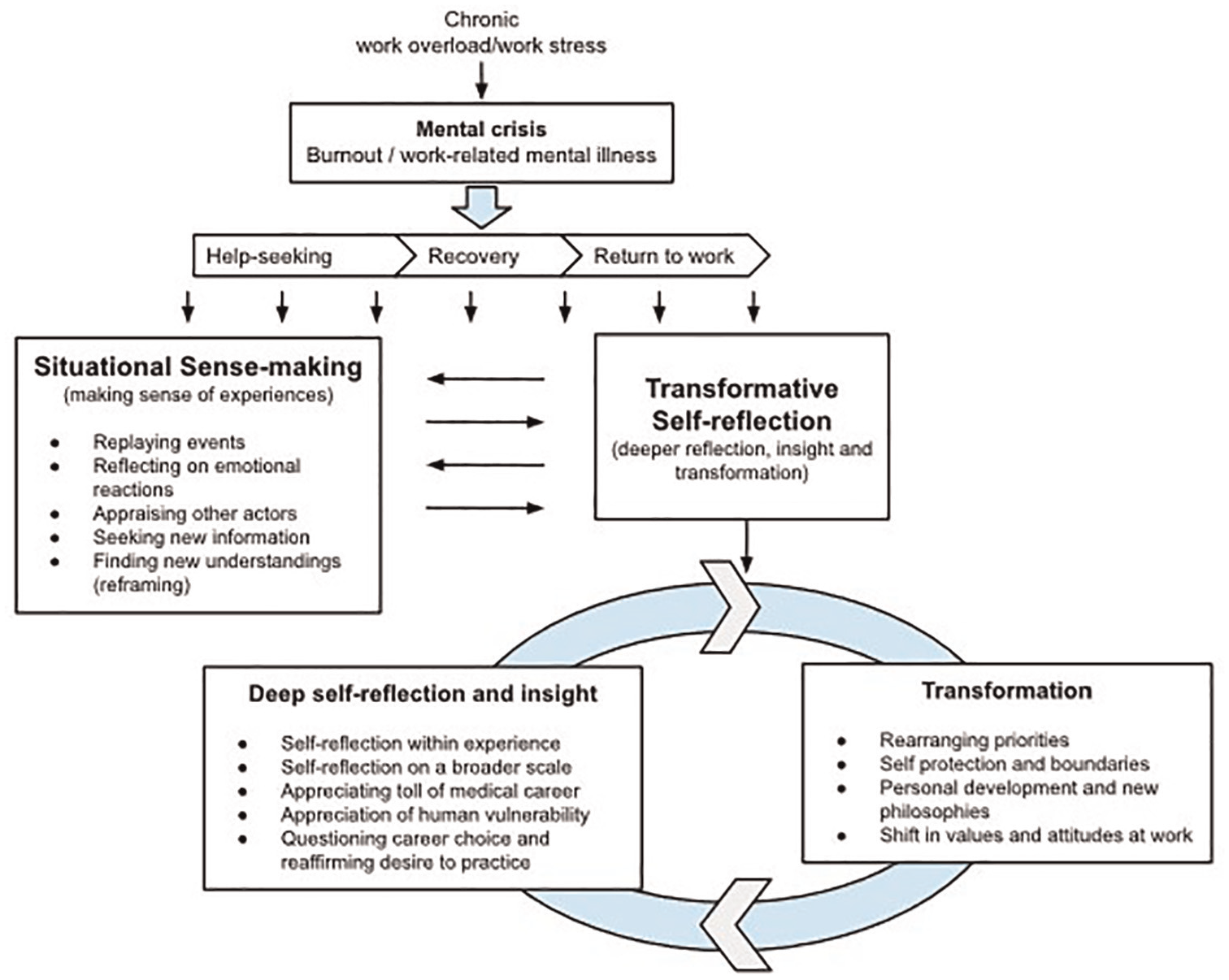
Schematic overview of the reflective processes of situational sense-making and transformative self-reflection which occur for a senior hospital doctor in response to a mental health crisis perceived to be caused or exacerbated by work stress.
Situational sense-making
Structure of the phenomenon of situational sense-making
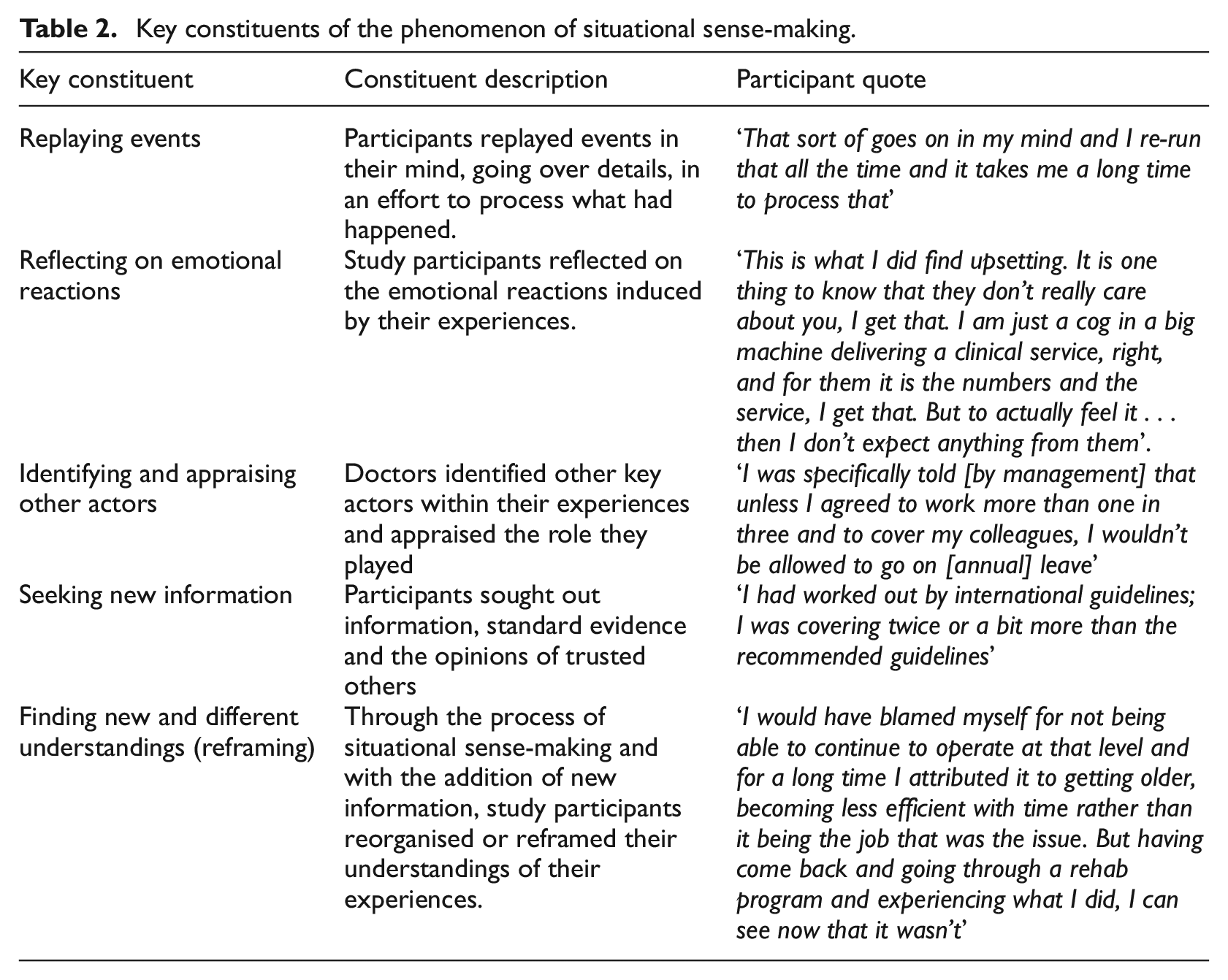
In trying to understand and come to terms with their experiences of mental illness and associated help-seeking in the context of intense work stress, senior doctors engaged in a process of situational sense-making in which they reflected on their experiences and sorted through them. They replayed events in their minds and revisited details of the experience. They recalled the emotional states aroused by the experience, both at the time of the experience and on reflection. In recounting their experiences, their most vivid descriptions were of memories relating to difficult parts of the experience.
They reflected on specific other actors within the experience, the role these individuals played and whether they had a positive or negative impact within the experience. To help work through their experiences, they sought out new information, evidence or outside opinion and, through the process of situational sense-making, they found new or different understandings of their experiences than they had at the time the events occurred, reframing and reorganising them. In this way, they attempted to find an understanding of events that made sense to them.
Constituents of situational sense-making
The key constituents of the phenomenon of situational sense-making are presented in Table 2.
Key constituents of the phenomenon of situational sense-making.
Transformative self-reflection
Structure of the phenomenon of transformative self-reflection
During and following their experiences of mental illness and help seeking in the context of intense work stress, hospital doctors engaged in a process of transformative self-reflection, which can be understood to occur in two ways: through deep reflection and associated transformation. Individuals engaged in deep reflection and transformation in parallel and iteratively. Transformative self-reflection was characterised by periods of active or passive deep reflection, significant, impactful moments of insight and associated conscious and unconscious change.
Within the process of deep reflection, participants engaged in a close examination of their experiences, of themselves and the ways they acted within the context of their experiences. They engaged in self-reflection with respect to the ways in which they live on a broader scale and entered into an examination of their personal history, life choices and career choices. They developed an appreciation of their human vulnerability and the toll a career in medicine had taken in terms of their physical, emotional, mental health and personal relationships.
In parallel with this process of deep reflection, the doctors began to make changes in their lives, which amounted to significant transformation. They began to practise self-protection and establish strong boundaries at work. Through the process of transformative self-reflection, and as a result of their experiences, a change in the type of doctor they were took place on a fundamental level.
Beyond the work sphere of their lives and following feelings of regret at what they had lost personally and in personal relationships, they rearranged their life priorities. They placed their personal health and wellbeing, as well as their personal relationships, at a higher priority than their work, recognising that they previously had given work the highest priority. They undertook personal development outside of work, learning new skills, expanding their social circles, experiencing growth and embracing or deepening alternative life philosophies. On reflection, and despite challenges with working conditions, which they accepted were likely to continue, they reaffirmed their love of medicine and their desire to continue to practise. This realisation led to further transformation in that it led them to refocus their energy on the positives within their work.
Constituents of transformative self-reflection
The phenomenon of transformative self-reflection is conceptualised in our findings in two (nonlinear) phases; ‘deep reflection leading to insight’ and associated ‘transformation’ (see Table 3).
Key constituents of transformative self-reflection – deep reflection and insight phase and transformation phase.
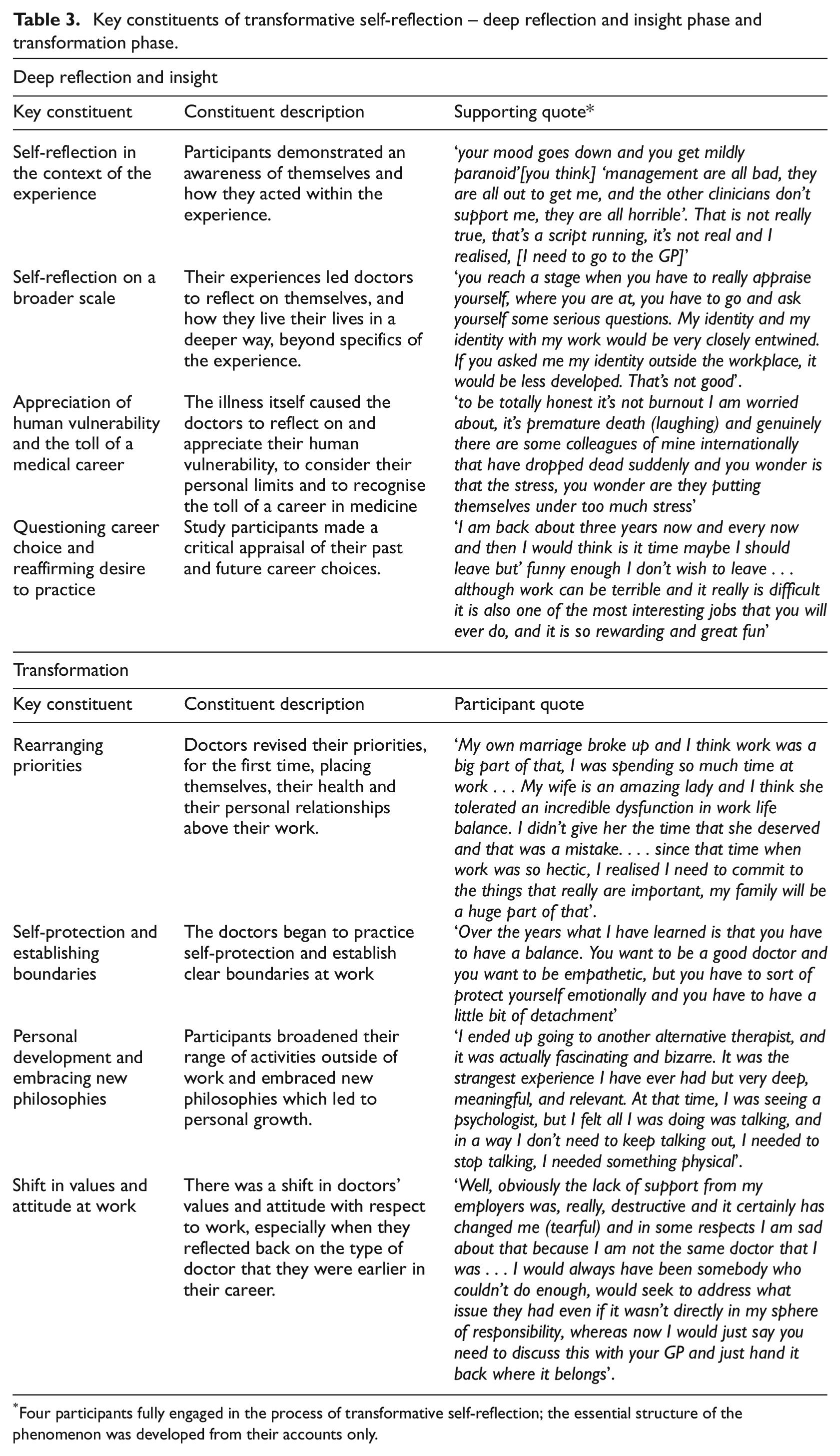
Four participants fully engaged in the process of transformative self-reflection; the essential structure of the phenomenon was developed from their accounts only.
Engagement in transformative self-reflection
All participants in our study engaged in situational sense-making but only four engaged fully in the deeper process of transformative self-reflection. Those who engaged in transformative self-reflection had reached a sense of resolution at the time of interviewing. Those who engaged only in situational sense-making, and who seemed to get stuck attempting to make sense of their experiences without entering a process of deeper self-reflection and change, were less resolved and remained distressed about some aspects of their experiences. Other factors within our data which may be important in achieving a sense of resolution and coming to terms with this experience are working culture, social support and support received from employer or line manager. See Table 1 for a summary of these factors in relation to which participants engaged in transformative self-reflection.
Those who achieved a sense of resolution and moving forward at the time of interviewing had engaged in transformative self-reflection but were also working in a large hospital with a non-conflict-oriented working culture at the time of illness, reported no bullying and received support either from their employer or a spouse, friend or family member throughout recovery.
Those who achieved a sense of resolution with a continued sense of loss, hurt and anger at the time of interviewing did engage in transformative self-reflection and had high social support. However, at the time of illness they were working in a medium sized hospital with a conflict-oriented working culture and were poorly supported by their employer through help seeking and recovery.
Those who had a lack of resolution at the time of interviewing and who were stuck in protracted attempts to make sense of their illness and help seeking experience had not engaged in a process of transformative self-reflection. They also experienced the most negative set of circumstances throughout illness and recovery in that they were working in a small hospital with a conflict-oriented working culture at the time of illness and reported bullying by management. They reported being poorly supported by management throughout help seeking and recovery and also did not have good social support at that time.
Discussion and implications
To our knowledge, there are no studies of senior hospital doctor burnout that include recovery, aftermath and return-to-work. We identified essential descriptions of two types of reflective processes doctors engaged in during the aftermath of crisis: situational sense-making, and transformative self-reflection. Situational sense-making is concerned with working through and making sense of specific events. In contrast, in transformative self-reflection, individuals reflect in a deeper way on their experience, their history, themselves and their lives and this deeper reflection leads to change. This happens in a non-linear, iterative way.
Our findings highlight reflective processes as a key component in recovering from burnout and work-related mental health crises. Existing literature emphasises resilience-building, coping strategies, job changes, social support, professional self-efficacy, vocational maturity and self-understanding as central to recovery (Cherniss, 1990; Maslach and Leiter, 2016; Pines and Aronson, 1988). However, our research identifies reflective processes as more critical for this cohort than factors like job changes (often unfeasible), resilience, self-efficacy or vocational maturity, already well-developed in this group. Specifically, recovery was supported by reflections on human vulnerability, the toll of a prolonged medical career, and an honest re-evaluation of past career choices.
Our findings build on Abedini et al.’s (2018) phenomenological analysis of internal medicine trainees (median age 30, 1–3 years post-graduation, practising in the US), which identified factors contributing to recovery. Our study extends these findings by focusing on a senior cohort and exploring the mechanisms of recovery, particularly the role of reflective processes.
Common recovery practices across both studies included adopting self-protective practices, establishing workplace boundaries, focusing on the positives of a medical career and nurturing life outside medicine. However, consultants in our study could not rely on recovery strategies available to trainees, such as rotating to a new hospital, increasing clinical competency or finding senior role models. Instead, recovery for consultants was driven by deep reflection, long-term career review, reprioritisation, strengthening self-protective practices and recognising the personal toll of a medical career.
The findings align with phenomenological research conducted in 2024 on the lived experiences of palliative care physicians in cultivating mindfulness (Lai et al., 2024). Both this study and our findings highlight the transformative impact of reflective practices which enabled participants to recognise their vulnerability, reassess personal values and priorities, and foster significant personal growth and self-care amid the challenges of their professions. Within our study, those who engaged only in situational sense-making, without entering a process of deeper self-reflection and change, were less resolved, and remained distressed about some aspects of their experiences. This aligns with meaning-making theorists (Park, 2010), who suggest that only transforming one’s beliefs, goals and operating systems, as distinct from efforts to make sense of a specific negative event, can lead to growth.
Although this DPA focused on individual experiences, the significant impact of the working environment on recovery cannot be ignored. All participants experienced extreme overwork before illness and described situations where optimal care could not be delivered, conditions linked to moral distress in doctors (Kherbache et al., 2022). Participants working in conflict-oriented cultures or receiving poor employer support during recovery reported unresolved psychological distress at the time of the interviews.
Our findings suggest that while deep reflection and personal changes are vital for post-adversity adjustment, working conditions, culture and employer support may be equally important in cases of work-related adversity. Existing research aligns with this, showing that the working environment is a key factor in burnout development among trainees (Prins et al., 2007) and reasonable workloads, management support and positive organisational culture reduce burnout (Kumar, 2016; Wallace et al., 2009). Additionally, quality social sharing of emotions at work, particularly support from supervisors, has been shown to alleviate burnout (Delroisse et al., 2023).
In our study, participants’ generally positive experiences with GPs, private healthcare, occupational health and employee assistance programmes were overshadowed by a lack of support and conflict with employers. Our findings support previous research which highlights the influential role of consultant doctors’ line managers, for example, senior hospital managers or CEOs, in doctors’ help-seeking, recovery and return-to-work processes (Putnik et al., 2011; Walsh et al., 2019). Our findings further highlight that poor or absent support, and in some cases conflict instead of support, from hospital management may hamper recovery, causing further distress at a vulnerable time.
Additionally, our study contributes to post-adversity growth theory (Linley and Joseph, 2004) by providing essential, phenomenologically developed descriptions of a post adversity experience and by highlighting a unique emphasis for this cohort. Participants reported a newfound appreciation of their personal vulnerability, contrasting with broader studies where post-adversity growth is more often associated with an appreciation of personal strength and resilience (Linley and Joseph, 2004). Given that doctors typically hold high expectations of their own capabilities (Montgomery, 2014) and have been found to be more resilient than the general population (West et al., 2020), this shift in perspective may be equally valuable in supporting recovery and preventing relapse in this cohort.
Strengths, limitations and future research
The study’s strengths, based on Sousa’s quality criteria for descriptive phenomenological research, include effective phenomenological reduction, eidetic analysis and identification of invariant elements across participants despite varied work contexts and illness presentations (Sousa, 2014). Specifics were transformed to general where doing so did not impact the essence of the phenomenon. For example, ‘impactful moments of insight’ occurred in many different ways for individual doctors. For one doctor a moment of insight came while watching a film. Integration of diverse accounts into a unified understanding of situational-sense making and transformative self-reflection in this context has been another strength of the research. Further details of the method and sample analysis are provided in Supplemental Materials.
In this study, we employed a descriptive phenomenological analysis (DPA) as our primary research method, complemented by content analysis to provide contextual and background information and enrich our understanding of the primary findings. This methodological approach was chosen to capture the essence of participants’ lived experiences and to situate these experiences within a specific context and is a further strength of the study. The study’s credibility is strengthened by the diverse perspectives of the research team, which included an occupational health physician (female) with expertise in doctors’ wellbeing and three experienced researchers (two female, one male) with backgrounds in human resources, organisational psychology, health psychology and health services (Graneheim and Lundman, 2004). However, a limitation is the exclusion of senior, non-consultant hospital doctors not in training, who should be included in future research.
Follow-up research should explore why some individuals engage in transformative self-reflection while others do not and examine how it can be encouraged. Factors affecting recovery, such as the conflict-oriented cultures and bullying experiences described by participants, also warrant attention. These behaviours, which may contribute to illness and hinder recovery, should be studied to determine their prevalence, contributing factors and potential solutions.
Practical implications
Our study highlights the deep existential impact of work-related mental illness for hospital doctors, particularly in later career stages, and emphasises the importance of fostering critical reflection during recovery. Supporting doctors in exploring positive transformation and guiding them towards growth may enhance recovery. Our findings also align with findings of Shaw et al. who stress the importance of reflective practices for healthcare professionals to process difficult experiences and foster personal growth and who emphasise the importance of support and recognition from management as well as civility in the workplace (Butcher et al., 2022; Shaw et al., 2024; Yeter et al., 2024).
Therapeutic interventions based on models of meaning-making and post-adversity growth may be especially beneficial. Techniques such as ‘meaning constructs’ and ‘meaning-oriented techniques’, as summarised by Dezelic (2017), can help doctors explore and reestablish meaning in their lives. Additionally, our study underscores the need for health organisations to address the line management void in medicine, particularly for senior doctors.
Conclusions
Doctors are regularly faced with difficult working conditions in which optimum care cannot always be delivered and which can precipitate or exacerbate mental health crisis. In recovering from mental health crisis, senior hospital doctors can engage in two processes of reflection, situational sense-making, and transformative self-reflection. Doctors reflect on their experiences to make sense of them and may reflect in a deeper way on themselves, their experiences, their history and their lives on a broader scale. This deeper reflection may lead to changes in their priorities, values and ways of living which allow them to recover and move forward. Engaging in this deeper transformative self-reflection may lead to better outcomes and post adversity growth. Following an initial period of making sense of the specifics of their experience, it may be helpful to guide doctors in crisis towards transformative self-reflection and to encourage them, with kindness, to make positive and self-protective changes in their lives. With time they should be further supported to explore positive revisions of their views of self, their goals, priorities and sense of meaning in life. If doctors are not well supported through this vulnerable time, particularly by their employer, recovery, adjustment and positive outcomes may be more difficult to attain.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251328455 – Supplemental material for ‘I would have blamed myself, but coming back, I can see that it wasn’t me’: A qualitative, descriptive phenomenological analysis of doctors’ reflective processes in recovery from burnout and mental crisis
Supplemental material, sj-docx-1-hpq-10.1177_13591053251328455 for ‘I would have blamed myself, but coming back, I can see that it wasn’t me’: A qualitative, descriptive phenomenological analysis of doctors’ reflective processes in recovery from burnout and mental crisis by Gillian N Walsh, Yseult Freeney, Simon Dunne and Blánaid Háyes in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to express gratitude to all the doctors who took part in these interviews and shared with us their insight and experience. We would also like to thank our study Steering Group for their input into the design of this study and the doctors who participated in the pilot phase of the study.
Author contributions
GW led the study design process. All authors were involved in review and refinement of study design. GW conducted all the interviews and the majority of the analysis. YF, SD and BH reviewed pilot interviews and cross analysed two interviews. All authors were involved in finalising analysis. GW wrote the first draft of the manuscript. YF, SD and BH contributed to subsequent drafts.
Data sharing statement
The qualitative interview transcripts are not publicly available to protect participant confidentiality and comply with ethical guidelines. However, de-identified excerpts may be provided upon reasonable request, subject to ethical approval.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We wish to acknowledge the generous financial support provided by the Human Resources National Directorate of the Health Service Executive (HSE) as well as that provided by the Royal College of Physicians of Ireland, the Royal College of Surgeons in Ireland and the College of Anaesthetists.
Ethics approval
The study protocol was approved by the Royal College of Physicians of Ireland’s (RCPI) Research Ethics Committee in December 2013 (RCPI RECSAF 20).
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide licence the Publishers and its licensees in perpetuity.
Informed consent
Written informed consent was attained from participants prior to commencement of interviews.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.