
Abstract
Community-dwelling older people (CDOP) face important risks of falling, a leading cause of chronic pain and transitions into long-term disability. While exercise-based interventions are widely studied for fall prevention, psychoeducation may play an important preventive role. Nevertheless, psychoeducation for fall prevention remains underexplored. This study aimed to describe existing psychoeducation for fall prevention among CDOP, identify its key components, and derive recommendations to inform future interventions. Using a scoping review design, we selected 20 studies with focus on psychoeducation for fall prevention. Findings revealed that all selected studies incorporated at least one of the four psychoeducation elements described by Anderson et al. Key aspects including mode of delivery, intervention facilitator, and educational resources are described, but literature lacks convergence. Moreover, theory-based psychoeducation programs and integration of technology and interactive delivery methods are underexplored. Implications for the design of a psychoeducation program for fall prevention in CDOP are discussed.
Community-dwelling older people are older adults who independently reside in their own residence or within community environments, as opposed to those residing in care facilities such as hospitals or nursing homes (including dependant living facilities or long term care facilities). Remaining within one’s own home holds significant importance for older people. Després and Lord (2005) outline numerous reasons underlying older people’ preference for independently living instead of transitioning to long-term care facilities. These reasons include retaining a sense of autonomy and control, staying in close proximity to their relatives, fostering psychological and physical well-being, and preserving a self-perception that aligns with their personal identity. Due to various factors, including the often prohibitively expense of assisted living, spacial limitations within such facilities, and the projected surge in the older adult population by 2050 (Kisling-Rundgren et al., 2016), supporting older people to stay in their homes, as community-dwelling older people, has important implications for society and health care systems. When considering this population, according to Liu-Ambrose et al. (2019), falls in community-dwelling older people are the third most prevalent cause of chronic pain and transitions into long-term disability. Furthermore, in Europe alone, more than 35,000 adults aged 65 and above die each year due to fall-related injuries (Albornos-Muñoz et al., 2018). The financial burden associated with fall-related treatments is also noteworthy, with costs reaching up to 25 billion euros annually for the European population, and potentially rising to 45 billion euros in the absence of preventive measures (Albornos-Muñoz et al., 2018; Gallant et al., 2019).
Among the numerous systematic reviews published in the last years, Gillespie et al. (2012) and Sherrington et al. (2019) found that interventions incorporating exercise modalities are significantly more effective in preventing falls in comparison to usual care, typically no exercise intervention. However, these authors noted that certain exercises such as walking and balance may not provide advantages on their own compared to no intervention, and some exercises such as resistance training may even have some adverse effects. Further, Tricco et al. (2017) suggest that exercise may increase capacity and confidence in older people thus enabling them to increase their exposure to fall risk and that performing certain types of balance exercises potential increase an older people risk of falling. A recently published umbrella review concludes that fall prevention interventions should be based on exercise first and foremost, but when possible including a multifactorial approach, including psychoeducation, may improve outcomes (Meulenbroeks et al., 2024).
According to Hedman-Lagerlöf and Axelsson (2019), psychoeducation can be defined as interventions within healthcare services that provide patients with information about their specific disorders. The primary goal of such intervention is to empower patients by equipping them with the knowledge and resources they need to develop effective coping strategies. Ekhtiari et al. (2017) mention that psychoeducation is recognized as a crucial element of treatment for both medical and psychiatric disorders. Expanding on the findings of Bergland (2012), which highlight various risk factors for falls in older people associated with a lack of knowledge (such as choosing unsafe clothing or not securing the home), it is plausible to consider that psychoeducation could play a comparable role in preventing falls. Psychoeducation can have a positive impact throughout the entire course of an intervention, whether it is in the program introduction, providing a rationale for the program, finding productive ways to implement the program, and maximizing expected positive outcomes (Lavell et al., 2020).
Psychoeducation serves as a versatile tool that can be utilized in various ways within fall prevention programs. In some cases, it could be employed as an introductory method to convey important information regarding the program, as a means to provide a rationale for fall prevention through relevant statistics, and as a valuable resource to effectively communicate exercises through illustrations and detailed explanations. Indeed, psychoeducation is commonly integrated into numerous fall prevention programs, frequently as a method to provide resources such as exercise guides or risk factors (Gallant et al., 2019; Katrancha and Bonachea, 2020; Liu-Ambrose et al., 2019; Logan et al., 2021). In fact, these materials regularly play an important role in effectively communicating knowledge and empowering individuals with the necessary information to mitigate fall risk and enhance safety. Moreover, in fall prevention, psychoeducation can play an influential role in helping participants reduce fears related to falling by providing them with the necessary knowledge to avoid falls. Psychoeducation can indeed play a large role in fall prevention through motivating older people to exercise more, highlighting its importance in preventing falls. It can also equip them with knowledge about high-risk situations and strategies to avoid them, further helping to reduce fear of falling. This approach can subsequently complement exercises, which equips participants with the physical capabilities needed to prevent falls. While psychoeducation is often incorporated into interventions, there appears to be a lack of studies that specifically evaluate key components to include, as well as the best delivery methods, to provide effective use of psychoeducation with aim to prevent falling among community dwelling older people. Consequently, this review aims to map peer reviewed literature to document the extent of existing knowledge and identify the gaps to inform future research and intervention.
Methods
While systematic reviews characteristically review the literature based on study design to identify effective interventions, scoping reviews methodology is used when the purpose is to map relevant literature in a field of interest, especially if the topic area is emerging or complex (Colquhoun et al., 2014; Levac et al., 2010). We conducted a preliminary search of the Cochrane Database of Systematic Reviews and no current systematic reviews or scoping reviews on psychoeducation for fall prevention among community dwellings older people were identified. Thus, we decided to use a scoping review design in this study. Based on Arksey and O’Malley’s (2005) recommendations, we led a five stages scoping review process, including: (a) determine the purpose; (b) identify potential studies; (c) screen and select relevant studies; (d) extract data into charts; and (e) collate and summarize the results.
Determining the purpose
For the purpose of this review, the terms “community dwelling older people” refers to individuals who are 65 years of age or older and are living in independent housing and are not living in a long-term care institution. The guiding question for this scoping review was: How to design an evidence-based psychoeducation program for fall prevention among community dwelling older people? The overarching goal of this scoping review is twofold. First, it aims to describe the main structure and key elements to include when it is time to design a psychoeducation program for fall prevention among community dwelling older people. Second, it aims to derive recommendations to inform future research.
Identifying potential studies
The eligibility criteria for this scoping review were determined based on the PICO tool, which includes the participant characteristics, the description of the psychoeducation intervention, and the prevention of falls as a principal outcome. The study design was also considered as an inclusion/exclusion criteria.
Participants
The inclusion criteria for this scoping review encompassed studies that met the following participant characteristics: at least 50% of the participants were aged 65 years or older, OR the mean age of the participants was at least 65 years, OR the study explicitly referred to older people as the target population, even if the specific age cutoff was not mentioned; and; study participants were exclusively community dwelling older people OR the study provided findings description for community-dwelling older people separately from older people living in institutional settings. Furthermore, while we did include studies with older people living with chronic conditions, we did not include studies concentrating solely on specific diseases causing falls among older people. This approach was adopted to ensure that the review informs best practices for psychoeducation for fall prevention in the general population of community dwelling older people, rather than specific subgroups.
Intervention(s)
The inclusion criteria for this scoping review consisted of studies in which interventions for fall prevention were solely based on psychoeducation, OR a combination of exercise-based program and psychoeducation OR an exercise-based intervention was compared with a control group who benefited from psychoeducation. We excluded studies in which exercise-based interventions were the main and only focus.
The term psychoeducation was initially introduced by Anderson et al. (1980) to encapsulate a comprehensive behavioral therapeutic concept comprising four key components: (1) providing patients with a comprehensive understanding of their illness, (2) equipping individuals with skills in order to solve their problems, (3) enhancing communication abilities, and (4) fostering a sense of self-assertiveness when facing their problems (Bäuml et al., 2006). These four components were employed to assess the extent to which interventions utilized psychoeducation techniques allowing for inclusion in this review. Consequently, the interventions included in the study featured at least one of the specified components in their programs.
Types of sources
This scoping review considered both experimental and quasi-experimental study designs including randomized controlled trials, non-randomized controlled trials, before and after studies, and interrupted time-series studies. Also, analytical observational studies including prospective and retrospective cohort studies, case-control studies, and analytical cross-sectional studies were considered for inclusion. This review also considered descriptive observational study designs, including case series, individual case reports, and descriptive cross-sectional studies for inclusion. Qualitative studies were also considered including, but not limited to, designs such as phenomenology, grounded theory, ethnography, qualitative description, action research, and feminist research.
Screening and selecting relevant studies
Search strategy
An academic librarian was consulted throughout the creation of this search strategy. The search ranged from January 1st 2018 to September 8th 2024, which allowed for the inclusion of the most recent evidence over the past 5 years pertaining to the association between psychoeducation and fall prevention. By limiting the search to this frame, we aimed to provide a summary of the most recent evidence in the field. Studies published in French and English were included. The databases that were explored included APA PsycINFO, CINAHL, and PubMed. The search strategy, including all identified keywords and index terms, was developed in collaboration with an academic librarian. The search term is presented in the Supplemental Material.
Study selection
Titles and abstracts for all identified citations were each screened by two reviewers for assessment against the inclusion/exclusion criteria. The first author acted as a referee when inter-judge disagreement was observed. Selected articles were retrieved, and imported into Mendeley Software. The full text of selected citations was assessed in detail against inclusion criteria by two independent reviewers. Reasons for exclusion of sources of evidence that do not meet the inclusion criteria were recorded and reported in the scoping review. Any disagreements that arose between the reviewers at each stage of the selection process were resolved with discussion, or with an additional reviewer. The selection process is presented in Figure 1, using the PRISMA-ScR flow diagram (Tricco et al., 2018).
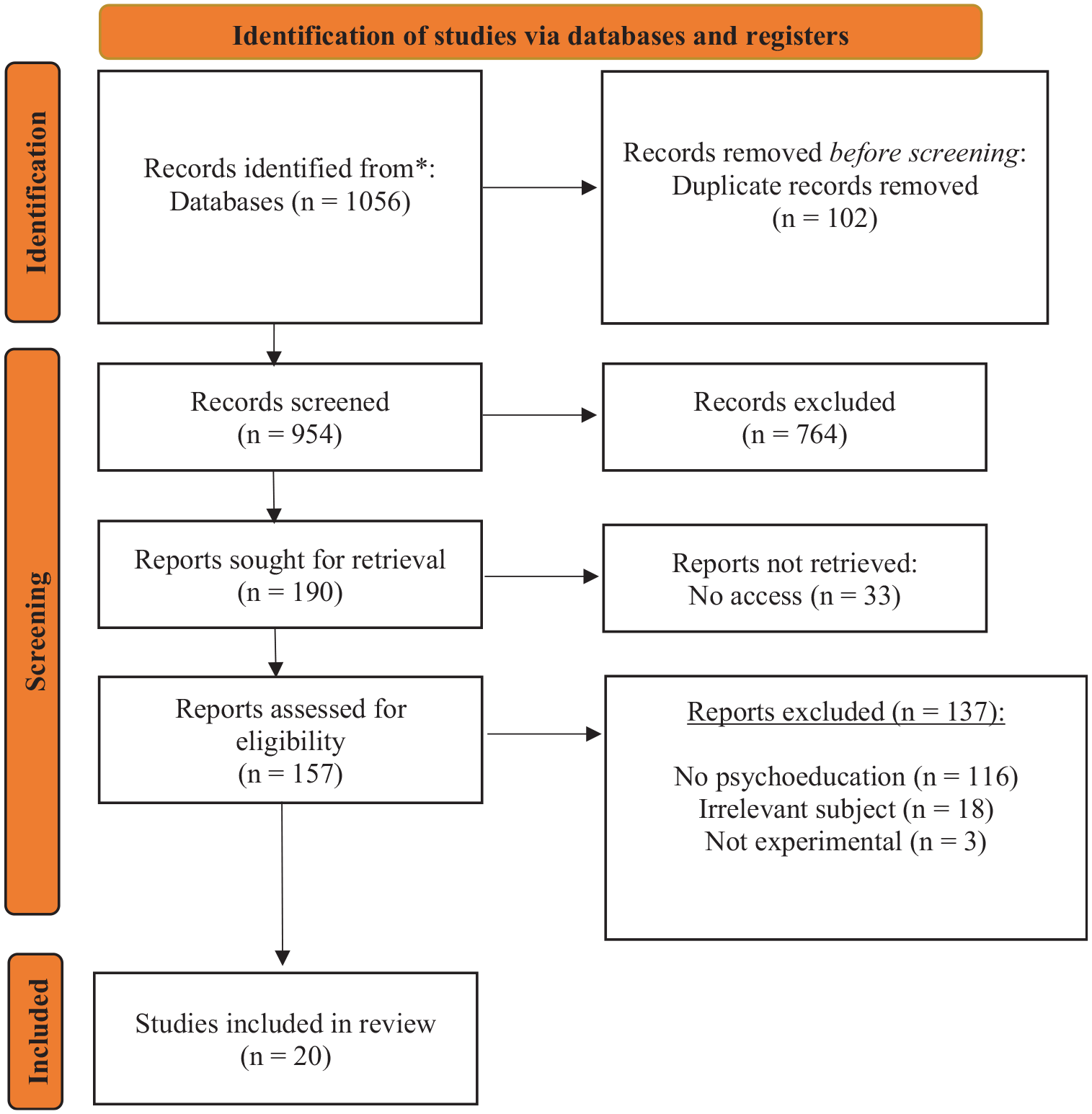
Flow chart.
Extracting data
Data extraction from the included studies in the scoping review was conducted by two independent reviewers using a specifically designed data extraction tool created in Excel sheets by reviewers. The extracted data included author’s name, publication year, study goals, study type, participant details (age, sample size), and intervention details (name, exercise type, psychoeducation type, delivery method, duration). This comprehensive data extraction process ensured that relevant information was systematically collected and enabled analysis of the included studies. A draft data extraction tool was modified and revised as necessary during the process of extracting data from each included evidence source. All modifications were detailed in the scoping review.
Summarizing data
The data extracted was organized and organized regarding three distinct subgroups: interventions focusing on educative material, interventions focusing on exercise, and interventions combining both educative material and exercise. We then analyzed and categorized pertinent data from all the studies included. This process allowed us to uncover potential trends and patterns, facilitating a deeper comprehension of the fundamental mechanisms involved in fall prevention through psychoeducation.
Ethics approval
This review did not involve human participants. Thus, ethical approval and informed consent were not required.
Results
Results of the search
After conducting a preliminary search across all three bibliometric databases, we identified 1056 articles. After eliminating duplicates (n = 102), we screened titles and abstracts of 954 records, resulting in the exclusion of 764 records deemed irrelevant to this scoping review. The majority of the excluded records during screening were related to reasons such as participants not being healthy or community-dwelling, and records being irrelevant to fall prevention. Out of the 157 accessed studies, 33 reports were not retrieved due to a lack of access (electronic or paper format not available). After reviewing the full reports of the remaining studies, 20 peer-reviewed articles were deemed relevant to this scoping review.
Characteristics of included reports
Descriptive characteristics
Of the 20 reports identified in our search, the distribution across study types is as follows: nine (45%) randomized controlled trials, five (25%) before-and-after studies, three (15%) quasi-experimental studies, one (5%) mixed-methods studies, one (5%) observational study, and one (5%) qualitative study. The interventions spanned across multiple countries, including 10 (47.6%) from the USA, three (14.3%) from Australia, two from Thailand, and one from each of the following countries Egypt, the Netherlands, China, Korea, and the Czech Republic. The included studies had an average of 133 participants, ranging from a minimum of 17 participants to a maximum of 503 participants. All the studies that were identified focused on community dwelling older people. The descriptive characteristics are shown in Supplemental Table 1.
Interventions characteristics
A diverse array of interventions were employed to address fall prevention and alleviate the fear of falling across the 20 identified reports. Among these interventions, three (15%) studies utilized a combination of psychoeducation sessions and the Otago Exercise Program, which is a personalized strength and balance regimen typically offered by physical therapists (Mohammed et al., 2019; Olij et al., 2019; Suttanon et al., 2018). Three (15%) additional studies tested the Matter of Balance program for fall prevention (Geyer and Thompson, 2021; Katrancha and Bonachea, 2020; Mielenz et al., 2019). This program focuses partially on cognitive strategies to initiate lifestyle changes before incorporating exercises aimed at enhancing individual strength. Moreover, three (15%) studies employed fall prevention education without adhering to any intervention model (Chidume, 2021; Lee, 2023; Tiefenbachová and Zeleníková, 2019). Three studies used the StrollSafe program, designed to offer outdoor safety information (Chippendale, 2019; Chippendale et al., 2023; Chippendale and Chen, 2023). The remaining eight (40%) studies implemented varied interventions, using psychoeducation alone or in combination with exercise program. Regarding psychoeducation-based interventions, Lim et al. (2023) employed the myCompass program, an online cognitive behavioral therapy tool. Within the realm of multifactorial interventions, incorporating both psychoeducation and exercise to prevent falls, the remaining studies employed several different programs: Muniak et al. (2019) utilized the SAIL program, Lukaszyk et al. (2018) used the Ironbark program, Areeudomwong et al. (2019) adopted the Thai Boxing Dance program, Ye et al. (2022) used the Teach-back health education program, and Delbaere et al. (2021) implemented the StandingTall program.
Presence of psychoeducation within the programs
The presence of psychoeducation interventions was assessed based on the number of components included, which ranged from 1 to 4. The studies included within our analysis all had a minimum of 1 element of psychoeducation as described by Anderson et al. (1980) and had on average 2.24 elements pertaining to psychoeducation. Specifically, three studies had one, eleven studies had two, six studies had three, and only one study had all four elements of psychoeducation. Among the 20 studies examined, all of them included methods to prevent falls. However, six of these studies did not include the element of informing the participants about falls and their associated risks, sixteen of the studies did not include a component for facilitating communication, and fifteen of them did not include elements designed to cultivate a proactive desire in participants to take action in preventing falls.
Regarding the theoretical foundations of the psychoeducation provided, five studies followed a specific theoretical framework, while fifteen studies did not report any theoretical basis. The frameworks used were the Ecological and Health Belief Model (Becker, 1974; Bronfenbrenner, 1977; in Chippendale, 2019; Chippendale et al., 2023; Chippendale and Chen, 2023), the Lifestyle Redesign Program Model (Clark et al., 2012), the Nursing as Caring Model (Chidume, 2021; Smith and Parker, 2019), and the Multifactorial Fall Risk (Feldman and Chaudhury, 2008; in Tiefenbachová and Zeleníková, 2019).
Characteristics of psychoeducation for fall prevention
Mode of delivery
Among the 20 included studies, 17 were delivered within a structured fall prevention program. Among these, four programs were available free (Chidume, 2021; Lim et al., 2023; Szanton et al., 2021; Tiefenbachová and Zeleníková, 2019). The other studies either did not report whether their programs were available for free or did not offer their programs for free. Out of the included studies, only three did not provide programs in person (Delbaere et al., 2021; Lim et al., 2023; Ye et al., 2022). Alternatively, one program offered their sessions through a hybrid format (Lee, 2023). Furthermore, 11 programs were delivered in group settings (i.e. Chippendale et al., 2023; Katrancha and Bonachea, 2020; Mielenz et al., 2019). Among those who chose to deliver their interventions in groups, they enrolled 15 participants on average (33 participants being the maximum, 8 participants being the minimum). Additionally, one study had a total of six groups who took part in their program across six different locations (Lukaszyk et al., 2018). The remaining included studies had participants take part in their program individually.
Format
The included studies had diverse program formats. Specifically, six studies focused exclusively on fall prevention education (i.e. Chippendale, 2019; Lim et al., 2023). Alternatively, six studies focused on exercise to allow fall prevention, but also had some forms of included psychoeducation (i.e. Mohammed et al., 2019). The other nine studies concentrated on both educative and exercise elements in their programs (Geyer and Thompson, 2021; Muniak et al., 2019). To transmit the information found in their programs, some studies chose to include self-guided components (Areeudomwong et al., 2019; Delbaere et al., 2021; Lee, 2023; Lim et al., 2023; Olij et al., 2019; Szanton et al., 2021; Ye et al., 2022). Furthermore, seven studies had some forms of group discussions within their programs (i.e. Chippendale, 2019; Chippendale et al., 2023; Katrancha and Bonachea, 2020). Additionally, only five studies did not include any forms of exercise within their programs for falls (Chippendale, 2019; Chippendale et al., 2023; Chippendale and Chen, 2023; Lim et al., 2023; Tiefenbachová and Zeleníková, 2019). Among the included studies, one chose to provide quizzes to their participants to better capture their understandings of the program (Ye et al., 2022), and one study included simulations to prevent falls (Lee, 2023). Finally, 13 of the included studies incorporated elements that were meant to be dynamic and interactive, thus allowing for more active participation from participants (i.e. Areeudomwong et al., 2019; Lee, 2023). Several studies had a lecture-style format, where only one person (often a facilitator) communicated information to the participants (Chippendale et al., 2023; Lee, 2023).
Duration of programs
The included studies varied in terms of duration of the program. While only one study did not report its program duration, the remaining 19 studies had interventions lasting an average of 64.85 days, with a maximum of 168 days and a minimum of 1 day. Notably, only two studies had interventions that were conducted over a single day (Chidume, 2021; Tiefenbachová and Zeleníková, 2019). Furthermore, while three studies did not report the duration of one session, the other eighteen studies lasted 63.44 minutes on average (maximum being 120 minutes and minimum being 10 minutes). Among these, one study reported having varying durations between 20 and 90 minutes (Ye et al., 2022). Additionally, seven studies did not conduct follow-ups with their participants. For those that did, follow-ups occurred on average 9 months after the programs ended, with a maximum of 24 months and a minimum of 1.5 months. Notably, only one study included a booster session to reinforce new knowledge 12 weeks after the intervention concluded (Szanton et al., 2021).
Facilitators
Most of the included studies featured a human facilitator for their programs. Notably, only 4 out of the 20 studies did not involve a facilitator (Areeudomwong et al., 2019; Delbaere et al., 2021; Lee, 2023; Lim et al., 2023). These facilitators were mostly involved in providing instruction to participants on various aspects of the program, including homeworks and educational material. Only 4 among the 16 studies that considered psychoeducation interventions delivered by a facilitator reported the sex of the facilitator and all four were females (Chippendale, 2019; Chippendale et al., 2023; Chippendale and Chen, 2023; Ye et al., 2022). Included studies assured various qualifications for their facilitators. Among these, four studies had facilitators who were educated as occupational therapists (Chippendale, 2019; Chippendale et al., 2023; Chippendale and Chen, 2023; Szanton et al., 2021), four interventions had facilitators who were educated as nurses (Chidume, 2021; Mohammed et al., 2019; Tiefenbachová and Zeleníková, 2019; Ye et al., 2022), three studies provided training to the facilitators (Geyer and Thompson, 2021; Katrancha and Bonachea, 2020; Muniak et al., 2019), two studies had members of their research teams handle facilitating (Mielenz et al., 2019; Olij et al., 2019), one study had individuals educated as physical therapists (Suttanon et al., 2018), and one study had individuals with experiences with a specific culture as facilitators (aboriginal; Lukaszyk et al., 2018). Among studies with facilitators, four had some forms of communications outside of the interventions. For example, Suttanon et al. (2018) had two follow-up calls with their participants by phone, and Mohammed et al. (2019) had monthly phone calls. None of the included studies who had facilitators reported their attitudes toward participants.
Resources
The included studies provided various types of resources for their participants to participate in their fall prevention programs. Among the included studies, 14 chose to provide manuals to their participants to help them navigate the program (i.e. Chippendale, 2019; Chippendale et al., 2023; Lim et al., 2023). Alternatively, some studies chose to include websites in their programs as a supportive source of information (Delbaere et al., 2021; Lee, 2023; Lim et al., 2023; Ye et al., 2022). Many studies also utilized handouts delivered to participants, at the beginning of the program or at the end of each session (Chidume, 2021; Chippendale, 2019; Geyer and Thompson, 2021; Tiefenbachová and Zeleníková, 2019). These manuals and handouts often aimed to aid participants with their understanding of key exercises and concepts within their programs. Alternatively, the studies that included websites utilized these as the main source of education for their participants (i.e. interactive online modules). The other extracted variables (presence of podcasts, forums, or Q&A sessions) were not utilized by any of the included studies.
Discussion
In this scoping review, we identified scientific reports that concentrate on fall prevention programs for community-dwelling older people, in which psychoeducation material is utilized in order to enhance effects. Afterward, the results of this scoping review were to be utilized in order to determine the most beneficial methods to include psychoeducation in a fall prevention program targeting community-dwelling older people. In order to optimize the creation of this program, this study aimed specifically to (1) understand how psychoeducation for fall prevention is delivered to community-dwelling older people and (2) to identify the key components of these programs. Results of this scoping review highlight a limited body of research on psychoeducation for fall prevention in community-dwelling older people, with a need for more theoretical foundation and standardized intervention components. Common practices relevant to delivery methods are also discussed.
Scope of the existing literature and theoretical foundations
Our results revealed a rather scarce literature on psychoeducation interventions for fall prevention amongst community-dwelling older people. In effect, while many studies during our search strategy studied fall prevention, most of them focused on non-healthy subjects and exercise based approaches without a psychoeducational component. Out of an initial search yielding over a thousand articles, only 20 met the criteria for psychoeducation interventions for fall prevention among community-dwelling older people, reflecting the narrow scope of focused studies in this area. This limited yield may suggest that psychoeducation is an underexplored or underreported component in fall prevention research, despite evidence supporting its role in other health settings (Burke et al., 2024; Ong et al., 2023).
When examining the theoretical foundations of psychoeducation interventions for fall prevention among community-dwelling older people, it is notable that only a minority of studies included a specific theoretical basis. While the physical activity portion of some programs followed a specific structure and framework, many studies did not mention the theory that helped structured their psychoeducational content. In the five studies that explicitly mentioned a theoretical framework guiding their psychoeducation intervention design, these included framework addressing intrapersonal, interpersonal, and community-level influences on fall prevention (Ecological and Health Belief Model; Bronfenbrenner, 1977) or by exploring the interactions of mobility, behavioral, and physical environment factors in fall prevention (Multifactorial falls risk model; Feldman and Chaudhury, 2008). The presence of a theoretical background of some sort could help structure interventions to better address different needs (Furr, 2000), such as psychoeducational components (see Anderson et al., 1980).
Key components in the design of psychoeducation interventions
Furthermore, a key observation is the inconsistency in how psychoeducation components are integrated into fall prevention interventions. Our results revealed that many studies lacked comprehensive elements essential to psychoeducation (Anderson et al., 1980; Bäuml et al., 2006), such as enhancing communication abilities and fostering a sense of self-assertiveness when facing the problems. This inconsistency may point to a need for standardized frameworks within psychoeducation for fall prevention to ensure that critical elements, which can encourage motivation and proactive behavioral change, are included. For example, the study included in this review that had the highest psychoeducation presence (Lukaszyk et al., 2018), suggested a decrease of fall risk for community dwelling older people, and remained 12 weeks post-intervention. Thus, similarly to the lack of a consistent theoretical framework for psychoeducation for fall prevention, a closer look at the quality of the psychoeducation delivered according to their key components should be considered in future programs.
In effect, some of the gaps noted in psychoeducational components could be attributable to the diversity of the delivery format in some studies. In the studies reviewed, there was a variation in delivery styles: while some interventions employed a dynamic approach that actively engaged participants through interactive components (e.g. group discussions, Chippendale, 2019), relied on a more traditional, magistral delivery, where information was primarily conveyed by a single facilitator, or through the use of self-guided modules (e.g. Ye et al., 2022). Indeed, dynamic approaches that stimulate discussion and active participation tend to be recommended in clinical guidelines relative to psychoeducation delivery (e.g. Lucksted et al., 2012; Sarkhel et al., 2020). Dynamic interactions also foster collaboration, offering older people valuable social reinforcement and a sense of belonging (Lu and Churchill, 2014). By comparison, magistral formats, where the facilitator primarily lectures, may limit opportunities for active learning and engagement. While these sessions can efficiently convey information, they may not be as effective in supporting sustained behavioral change, thus not reinforcing components 3 (enhancing communication abilities) and 4 (fostering a sense of self-assertiveness) of Anderson et al.’s (1980) model. This interactive component should thus be considered when designing psychoeducational programs for community-dwelling older people, or in any psychoeducation program.
In addition, regular follow-ups and booster sessions could play a key role in bridging this gap, especially for those who received magistral instruction. Studies including follow-ups, typically months after the intervention, can offer an opportunity to refresh knowledge and address any challenges participants may face while applying what they learned (i.e. Szanton et al., 2021). However, many studies in our review (n = 7) did not include this support, and fewer administrated booster sessions (n = 1). In line with current recommendations on the administration of psychoeducation, the presence of such support could be beneficial to include (Sarkhel et al., 2020).
Key aspects for a preliminary program structure
Based on our findings, a preliminary structure for a psychoeducation intervention aimed at fall prevention among community-dwelling older people can be suggested. First, the objectives of the intervention should be multifactorial (see Muniak et al., 2019; Ye et al., 2022, for examples). In this sense, psychoeducation used should aim to reach the following objectives: (1) to increase older people awareness of fall risks and related injuries; (2) to enhance self-efficacy and motivation for adopting preventive behaviors; (3) to improve physical strength and balance through structured exercises; (4) to reduce fear of falling by providing coping strategies and relevant education; and (5) to foster proactive engagement in lifestyle changes that reduce the likelihood of falls. This structure would also follow closely the psychoeducation elements suggested by Anderson et al. (1980). Such an approach would aim the goals to be aligned to help older people confidently and effectively manage their fall risk.
Furthermore, the presence of a theoretical foundation plays a key role in structuring effective interventions (Furr, 2000). Although many existing studies lack a strong theoretical foundation, some theories could be recommended such as the Ecological and Health Belief Model (Bronfenbrenner, 1977), to address perceptions of fall risk and motivate behavior change and multiple levels of influence. This perspective could also be supported through the use of a multifactorial fall risk model (Feldman and Chaudhury, 2008). In line with the objectives, this theoretical framework could support some key intervention components, such as the educational sessions on fall risk awareness and preventive practices, alongside strength and balance exercises (i.e. a multifactorial approach).
In terms of delivery, while the program could be delivered via a hybrid format, such as combining in-person group sessions with self-guided modules, group sessions would be beneficial to enhance engagement and support (Lucksted et al., 2012). To ensure continuity and reinforcement of learning, follow-ups or booster sessions could be included to maintain the engagement of participants. Furthermore, the program could consider qualified facilitators who have a background in psychoeducation, fall prevention, or any domain relative to health. Studies included in the review featured facilitators such as occupational and physical therapists or trained nurses (e.g. Chidume, 2021; Chippendale, 2019). Others opted for individuals who received specialized training in fall-prevention strategies to adequately deliver the program’s content (e.g. Gallant et al., 2019; Muniak et al., 2019). The use of trained facilitators could thus be useful in the development and implementation psychoeducation for fall prevention among community-dwelling older people.
Limitations and future directions
This scoping review did present some methodological limitations. First, our search term was limited toward peer-reviewed studies, thus excluding potentially important findings regarding the efficacy of psychoeducation (i.e. book chapters). Second, our search was limited toward studies written in English or French, which in turn potentially excluded relevant data. Third, the results of our study were highly dependent on the information that authors chose to deliver within their studies. As a result, it is conceivable that the studies included in this review may have contained more data relevant to the foundations and delivery of psychoeducation, but the authors did not see these findings as relevant.
Future studies should address gaps identified in this review regarding the implementation of psychoeducational programs for fall prevention. For instance, applying a theoretical framework and utilizing diverse core psychoeducation elements such as the enhancement of communication skills and self-assertiveness. Further investigation into delivery methods, such as hybrid and interactive formats, could improve participant engagement (Lucksted et al., 2012). Additionally, exploring the role of follow-up sessions or booster interventions in maintaining long-term behavioral change is crucial (Sarkhel et al., 2020). Examining the influence of facilitator training on program effectiveness could also inform best practices, enhancing the feasibility and credibility of the program. Collectively, these approaches would strengthen the integration of psychoeducation into fall prevention programs, facilitating their implementation.
Conclusion
In summary, the results of this scoping review highlight key components of programs designed to reduce falls among community-dwelling older people. Many elements were found to be common within included studies (i.e. facilitators, resources, in person programs). The results of this review are important as they can subsequently be used to better inform the inclusion of psychoeducation in programs designed to prevent falls among community-dwelling older people. They also highlight the need for future studies to develop more generalized theoretical foundations for the use of psychoeducation for fall prevention in this population, as this varied substantially between included studies. Nevertheless, exploring the key elements found in these interventions represents a significant step toward providing beneficial psychoeducational content allowing for community-dwelling older people to decrease fall risks through knowledge within such programs.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251326383 – Supplemental material for Psychoeducation for fall prevention among community-dwelling older people: A scoping review
Supplemental material, sj-docx-1-hpq-10.1177_13591053251326383 for Psychoeducation for fall prevention among community-dwelling older people: A scoping review by Jalila Jbilou, Joey Frenette, Marie-Pier Mazerolle, Chloé McLaughlin, Caroline Lovens, Grant Handrigan, Cornel Oros and Liliane Bonnal in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053251326383 – Supplemental material for Psychoeducation for fall prevention among community-dwelling older people: A scoping review
Supplemental material, sj-pdf-2-hpq-10.1177_13591053251326383 for Psychoeducation for fall prevention among community-dwelling older people: A scoping review by Jalila Jbilou, Joey Frenette, Marie-Pier Mazerolle, Chloé McLaughlin, Caroline Lovens, Grant Handrigan, Cornel Oros and Liliane Bonnal in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank Marc Harper, a health librarian at Université de Moncton, for his expertise and support elaborating the keywords chain and conducting the boolean searches. We also wish to thank Danica Maillet for the logistic support at the early stages of this project.
Data sharing statement
Data availability is not applicable to this review article as no datasets were generated or analyzed in conducting the review. Neverthless, the Excel spreadsheet containing information extracted from the selected articles, which supports the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant (CO102) from the Healthy Seniors Pilot Program. The Healthy Seniors Pilot program is a joint project between the Government of New Brunswick and the Public Health Agency of Canada.
Ethics approval
No ethical approval is needed for this review.
Informed consent
No informed consent was needed.
Pre-registration
The protocol is not registered with PROSPERO, as it currently does not accept scoping reviews. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) to prepare the protocol and the PRISMA-ScR extension for scoping reviews to present the results.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.