
Abstract
Cardiac Diseases (CD) have harmful devastating consequences for individuals. Their ill health may cause significant pain and suffering, psychological distress, social difficulties, reduced work capacity, and increased substantial economic strain. This study involved 120 self-employed individuals with CD, divided into lower and higher intolerance of uncertainty (IU) levels. Multi-group analysis was performed to examine differences between low and high IU groups. The study indicated a significant relationship among business profitability decline, IU, and high levels of demoralization in self-employed-individuals with CD. Self-employed-individuals with CD often encounter unique difficulties in performing their job roles appropriately, which affects their health. In addition, the results show that IU moderated the relationships between the study variables. Self-employed individuals with CD who were less tolerant of uncertainty had higher risk of psychological and work-related difficulties. Additionally, personal resources (such as self-efficacy and coping strategies) contribute to demoralization.
Introduction
Cardiac diseases and self-employed individuals
Cardiac diseases (CD), including coronary heart disease, stroke, heart failure, and artery disease, remain the leading cause of death in the United States and Europe (World Health Organization, 2023). CD have harmful devastating consequences for individuals. Their ill health may cause significant pain and suffering, psychological distress, social difficulties, reduced work capacity, and increased substantial economic strain, often forcing them out of employment and making them dependent on health care systems (Thornhill et al., 2008). Individuals with CD may often suffer from mood disturbances such depression (Kuhlmann et al., 2019) or demoralization (Rafanelli et al., 2005).
CD and demoralization
Demoralization is defined as a state of lowered morale and poor coping resulting in feelings of hopelessness, helplessness, and lost meaning and purpose in life (Bobevski et al., 2021). Unlike depression, symptoms of demoralization among individuals with CD have been scarcely examined (Liao et al., 2017; Tackmann and Dettmer, 2020). Demoralization following CD may have severe physiological, psychological, and social implications (Rzeszut and Assael, 2021). Individuals who have CD and experience demoralization report high levels of somatization symptoms, psychological suffering, and disease denial; significantly low levels of quality of life; and poorer psychosocial functioning (Tecuta et al., 2015). For example, study that examined factors associated with demoralization among patients before and after cardiac surgery revealed high levels of preoperative depression; that being retired predicted high levels of demoralization prior cardiac surgery; and that only high levels of postoperative depression predicted high levels of post-surgery demoralization (Liao et al., 2017). Additionally, demoralization often exacerbates chronically ill individuals’ sense of uncertainty, worsens their health conditions (Sajjadi et al., 2015), impairs family relationships (Behan, 2018; Clarke and Kissane, 2002), and harms overall quality of life (Sav et al., 2015). In a recent systematic review, involving adult heart-transplant recipients, high levels of demoralization were related to low levels of health-related quality of life (Tackmann Dettmer, 2020).
Uncertainty and coping
Intolerance of uncertainty (IU) is a dispositional tendency to react negatively to uncertain situations on cognitive, emotional, and behavioral levels due to negative beliefs about uncertainty and its implications (Buhr &and Dugas, 2009). Studies have demonstrated that individuals with higher self-reported levels of IU, relative to lower self-reported IU, tend to interpret (Cupid et al., 2021) and react to uncertainty negatively (see review by Morriss et al., 2021; also see Sahib et al., 2023). IU is normally distributed across the general population (see review by Carleton, 2016), and higher self-reported levels of IU are commonly observed among individuals presenting with anxiety (e.g. generalized anxiety, obsessive-compulsive disorder, posttraumatic stress), depression, and eating-related disorders (McEvoy et al., 2019). Studies also demonstrated IU regarding conditioned risk judgments was associated with lower engagement in exercise and eating a healthy diet to reduce the risk of CD (Orom et al., 2020). Furthermore, illness-related IU, which arises from the complexity of managing multiple diseases and lack of understanding regarding the course of an unpredictable CD, was negatively associated with recovery and compliance with self-care activity (Yu and Lee, 2024) and worse psychosocial adaptation to CD (Kim et al., 2019). Additionally, studies have shown a positive association between economic IU and deaths attributed to CD (Kawachi et al., 2023; Xia et al., 2022). Individuals with high levels of IU are prone to experience high levels of psychological distress when encountering uncertain or unpredictable situations (Carleton et al., 2007). High levels of IU among individuals with chronic diseases may have a significant negative impact on their emotional well-being and quality of life (Kurita et al., 2013; Sajjadi et al., 2015). Repeated and ongoing experiences of challenging circumstances typically lead to or exacerbate demoralization and exhaustion (Butler et al., 1991). Additionally, IU was found to be associated with avoidant coping related to diseases such as COVID-19 (Carnahan et al., 2022), cancer (Blom et al., 2023) and low levels of problem-focused coping in the case of the 2009 H1N1 pandemic (Taha et al., 2014).
Coping strategies have been suggested as a main factor that mediates the effect of stressors on mental health (Ben-Zur, 2002; Cohen, 2014; Folkman et al., 1986). Coping strategies are defined as attempts to render a perceived stressor more tolerable and minimize the distress induced by the situation (Folkman et al., 1986). Coping strategies can be classified into two main domains: engaged and disengaged coping (Carver and Connor-Smith, 2010). Engaged coping involves active coping strategies directed toward dealing with the stressor or vigorously changing the context or meaning of the stressful situation (e.g. support seeking, acceptance, planning, cognitive restructuring). Disengaged coping is aimed at escaping the threat or related emotions (e.g. denial, wishful thinking, excessive use of alcohol; Carver and Connor-Smith, 2010). Unlike engaged coping, disengaged coping among individuals with CD has been associated with high levels of psychological distress and poor adjustment (Allman et al., 2009; Hallas et al., 2009; Nahlén and Saboonchi, 2010). Personal resources are defined as individual characteristics that promote effective coping in the face of stressful situations, resulting in reduced psychological distress and enhanced well-being (Cohen, 2014; Levkovich et al., 2015). In the present study, we focused on self-efficacy—defined as the ability to respond effectively to life’s demands and challenges (Bandura, 1977). Previous findings indicated a positive association between self-efficacy, health literacy, and self-care, with medication adherence among CD patients (Chen et al., 2020; Cousin et al., 2020; Liu et al., 2023). For example, previous studies showed a positive association between self-efficacy and engagement with physical activity among patients with CD (Shajrawi et al., 2020). Higher self-efficacy was found to be associated with more healthy eating and smoking cessation (Wang et al., 2016). Additionally, findings of previous studies suggest that self-efficacy is positively related to aspects of psychological well-being and quality of life among cardiac patients (Banik et al., 2018; Krok and Zarzycka, 2020). To the best of our knowledge, no studies to date have examined the relationships among demoralization, IU, disengaged coping, and self-efficacy among self-employed individuals with CD.
Self-employed individuals and study variables
The British Heart Foundation estimates that approximately 260 million men and 290 million women suffer from CD across the world (Go et al., 2014). Studies also have shown that about 45% of people with CD are of working age and employed (Gupta et al., 2014). Self-employment is a highly demanding type of work that may significantly increase rates of uncertainty (Schonfeld and Mazzola, 2015; Smedegaard et al., 2017) due to unique challenges, such as maintenance of business profitability, work-related stress, and unstable work schedules (Krittanawong et al., 2020; Smedegaard et al., 2017). A recent systematic review noted high levels of depression, anxiety, exhaustion, and fatigue among self-employed individuals from Europe and Asia (Willeke et al., 2021). Self-employed individuals with CD need to cope with not only reduced work capacity, increased substantial economic strain, and uncertainty about maintaining their business profitability (Thornhill et al., 2008), but also the physical, psychological, family, and social implications of the disease for their daily lives, which can exacerbate feelings of uncertainty (Yagil and Cohen, 2024). This was the first study to identify demoralization among self-employed individuals with CD and associated psychological and work-related factors. To the best of our knowledge, no study to date has assessed the role of IU in psychological reactions among self-employed individuals with chronic health conditions, particularly CD. In addition, no previous studies were found regarding demoralization among self-employed individuals with CD. Finally, because of their unique characteristics, studying self-employed individuals will enable us to gain a better understanding of the relation between demoralization, disengaged coping, and personal resources (self-efficacy), business profitability decline, and uncertainty for those with chronic health conditions, particularly CD. To address these research gaps, this study aimed to investigate the psychological and work-related challenges faced by self-employed individuals with cardiac diseases (CD). Specifically, the study focused on:
1. Examining the relationships among physical symptoms, self-efficacy, and demoralization.
2. Examining the mediating role of disengaged coping and business profitability decline in the relationships among physical symptoms, self-efficacy, and demoralization.
3. Examining the moderating role of IU in the relationships between the study variables (physical symptoms, self-efficacy, disengaged coping, business profitability decline, and demoralization). Based on these objectives, the study tested the following hypotheses
Hypothesis 1. Higher physical symptoms will be associated with higher profitability decline and demoralization levels, whereas higher self-efficacy will be associated with lower profitability decline and demoralization levels among self-employed individuals with CD.
Hypothesis 2. The relationships between the study variables—physical symptoms, self-efficacy, business profitability decline, disengaged coping, and demoralization—will differ among self-employed individuals with CD by low and high IU groups.
Hypothesis 3. The relationships between physical symptoms, self-efficacy, and demoralization among self-employed individuals with CD will be mediated by business profitability decline and disengaged coping strategies. H3a: Physical symptoms will be associated with higher business profitability decline, greater use of disengaged coping, and increased demoralization levels. H3b: Self-efficacy will be associated with lower business profitability decline, lower disengaged coping, and decreased demoralization levels.
Method
Participants and procedure
The ethics review board of the affiliated University of Haifa approved this research. The study involved 120 self-employed people with CD.
Participants worked in their own company (as single owners or in a partnership), ranging from small to medium enterprises (0–20 employees). Inclusion criteria were as follows: aged 18 or older, diagnosis of a CD in the prior 2 years, and employed before and after the diagnosis. Individuals were included if they were diagnosed in the last 2 years with angina, suffered a cardiac event (heart attack), experienced cardiac-related symptoms, or received cardiac medications.
Two years was chosen to ensure respondents had not experienced a significant duration of time since their diagnosis, which might have masked the impact of CD. For recruitment, we relied on a survey company with a panel of more than 10,000 individuals who recovered from chronic health problems. Participants complete demographic questionnaires on their education, marital status, and income, among other variables. We randomly identified 120 participants through the company after initial filtering of the panel. We then reached out to potential participants by text message or email with an explanation of the research and an invitation to participate. People who expressed interest received more information about the goals and format of the study and were assured they would remain anonymous. During this process, they completed a consent form and settled on a time and place to complete the study questionnaire. The survey took 30–55 minutes to complete. This time reflects the entire process of participation in the study. This process began with a research assistant contacting participants, explaining the study’s purpose and procedures, addressing any questions, and obtaining informed consent after participants had an opportunity to read the consent form carefully. Only then did participants proceed to complete the questionnaire. Participants had the option to complete it in Hebrew or Arabic, Israel’s two main languages, and they received a $30 incentive.
Measures
Background variables were gender, age, education level, marital status, and income. We assessed physical symptoms via a six-item scale based on the EORTC QLQ-C30 (Aaronson et al., 1993). This scale is similar to a seven-item scale adapted from the WHOQOL-BREF (Skevington et al., 2004), which focused on CD patients (Areias et al., 2013). Respondents were asked: “To what extent have you experienced each of the following situations during the past month? For example, pain, fatigue (not related to strenuous activity) or sleep disturbances.” They answered using a 5-point Likert scale (0 = not at all to 4 = a great amount), and we calculated mean scores. Translated versions in Arabic and Hebrew were used (Koller et al., 2007). Scale reliability was α = 0.81.
IU was assessed via the short form of the Intolerance of Uncertainty Scale (Carleton et al., 2007). We only used the seven-item subscale measuring prospective anxiety (fear and anxiety about future events), which features a 5-point Likert scale (1 = not at all characteristic of me to 5 = entirely characteristic of me). Example items are: “Unforeseen events upset me greatly” and “It frustrates me not having all the information I need.” We calculated mean scores. Prior research found this instrument has high reliability (Cronbach’s α = 0.96). We used the translated and validated Hebrew version (Cohen et al., 2022) and translated it to Arabic using the back-translation method. Internal consistency in this study was good (Cronbach’s α = 0.83).
We used the short version of the Cardiac Self-Efficacy Scale to assess the confidence of participants regarding their ability to follow medical recommendations (Sullivan et al., 1998). The scale consists of 13 items categorized based on two factors. Control symptoms were measured with eight items and refer to confidence in the ability to control the symptoms (e.g. “How confident are you that you know how to take your cardiac medication?”). The second factor was function maintenance, measured by five items that captured the participants’ confidence in maintaining their functioning (e.g. “How confident are you that you can maintain your usual social activities?” Respondents used a 7-point Likert scale (0 = not at all confident to 6 = totally confident). A previous study found both factors had adequate reliability (α = 0.83 and 0.70, respectively; Tabernero et al., 2019).
To assess business profitability, we used a single item that measured any change in estimated business profitability before and after the CD diagnosis. Respondents rated their profitability change on a 5-point Likert scale (1 = much higher today to 5 = much lower today).
Sixteen items from the Brief COPE (Carver et al., 1989) were used to measure coping strategies in the workplace. Twelve items assessed engaged coping strategies (e.g. “trying to get advice on how to act”) and four items measured disengaged coping (e.g. “giving up and stop trying to deal with the situation”). Participants responded on a 4-point scale (0 = not at all to 3 = very much). Higher scores indicated more use of the coping approach. Scholars previously translated the questionnaire into Hebrew and Arabic and validated it (Ben-Zur, 2002; Khalaila and Cohen, 2016). Its internal consistency was acceptable in previous studies (Carver et al., 1989) and in the present study was α = 0.84 for engaged coping and α = 0.83 for disengaged coping.
We used the Demoralization Scale II to assess demoralization, which is the short version of the Demoralization Scale-24, a widely validated tool used to measure demoralization among people with chronic health conditions (Clarke and Kissane, 2002). The 3-point self-report scale (0 = never to 2 = often) has 16 items spread among two subscales—(a) meaning and purpose and (b) distress and coping ability. Based on its revalidation, psychometric strength, and simplification, the short version is an improved and practical assessment of demoralization for clinical and research purposes (Robinson et al., 2016a, 2016b). Example statements are: “I do not cope well with life” and “I feel that I cannot help myself.” Previous studies used this scale with individuals with CD and found it to be reliable (α = 0.86–0.92; Liao et al., 2017; Wu et al., 2019).
Data analysis
We calculated means, standard deviations, and Pearson correlations, then tested the research model with structural equation modeling in AMOS 27. Multi-group analysis was used to examine differences between low IU (coded 0) and high IU (coded 1) groups, with a mean cutoff score of 3.55. Multi-group analyses used here to identify potential moderating effects of IU on the relationships between the variables of interest by comparing model relationships across groups (low and high IU). To ensure the validity of the analysis, we assessed measurement invariance to confirm that variables were measured similarly across groups. Five indexes were used to assess model fit: chi-square and normed chi-square tests for overall fit and parsimony (good fit is indicated by normed chi-square values of 2.0 or less); the comparative fit index (CFI), Tucker-Lewis index (TLI), and normed fit index (NFI), which are incremental fit indexes; and root mean square error of approximation (RMSEA) and its corresponding confidence interval (CI), which indicates discrepancy per degree of freedom and the model’s absolute fit. In addition, we explored the statistical significance of indirect effects using 5000 bootstrap samples and 95% bias-corrected CIs.
Results
Demographic details of the participants (groups based on low and high IU levels) are shown in Table 1. No differences in background characteristics were found between participants who reported low or high IU. Participants ranged in age from 21 to 70 years. Men comprised about 80% of the sample. The range of years of education was 10–25. About two-thirds of the participants were married. The means, standard deviations, and ranges of the study variables are presented in Table 2. Significant differences emerged between the two groups. The high IU group experienced higher levels of demoralization, used more disengaged coping, and had more physical symptoms compared to the low IU group. Business profitability decline was higher in the low IU group.
Demographic characteristics of participants by low and high IU.

Low IU group coded 0 and high IU group coded 1.
Means and standard deviations of study variables by low and high IU.

p < 0.05. **p < 0.01.
Associations between study variables
Pearson correlation coefficients of the study variables for each group are presented in Table 3. In both groups, physical symptoms were positively associated with business profitability decline, and self-efficacy was negatively associated with demoralization. In the low IU group only, demoralization was positively associated with business profitability decline. In the high IU group only, demoralization was positively associated with disengaged coping and physical symptoms.
Associations among study variables by low and high IU.

p < 0.05. **p < 0.01.
Study model
First, the associations between the study variables and background characteristics were examined to determine which background variables should be controlled. Only education level was associated with the outcome variables and thus, was entered in the initial model. Therefore, the variables in the examined model were education level, physical symptoms, self-efficacy, and disengaged coping. Education level and engaged coping variables were omitted due to lack of associations. A multigroup analysis was performed to test and compare the model for the two groups: high and low IU. Significant differences were found in the associations of the model variables between the two groups (χ2 = 22.72, df = 8, p < 0.001). The final overall model for the two groups (Figure 1) showed good fit: χ2 = 1.624, df = 2, p = 0.44; χ2/df = 0.81; NFI = 0.98; TLI = 1.00; CFI = 1.00; RMSEA = 0.00, 90% CI (0.01, 0.07).
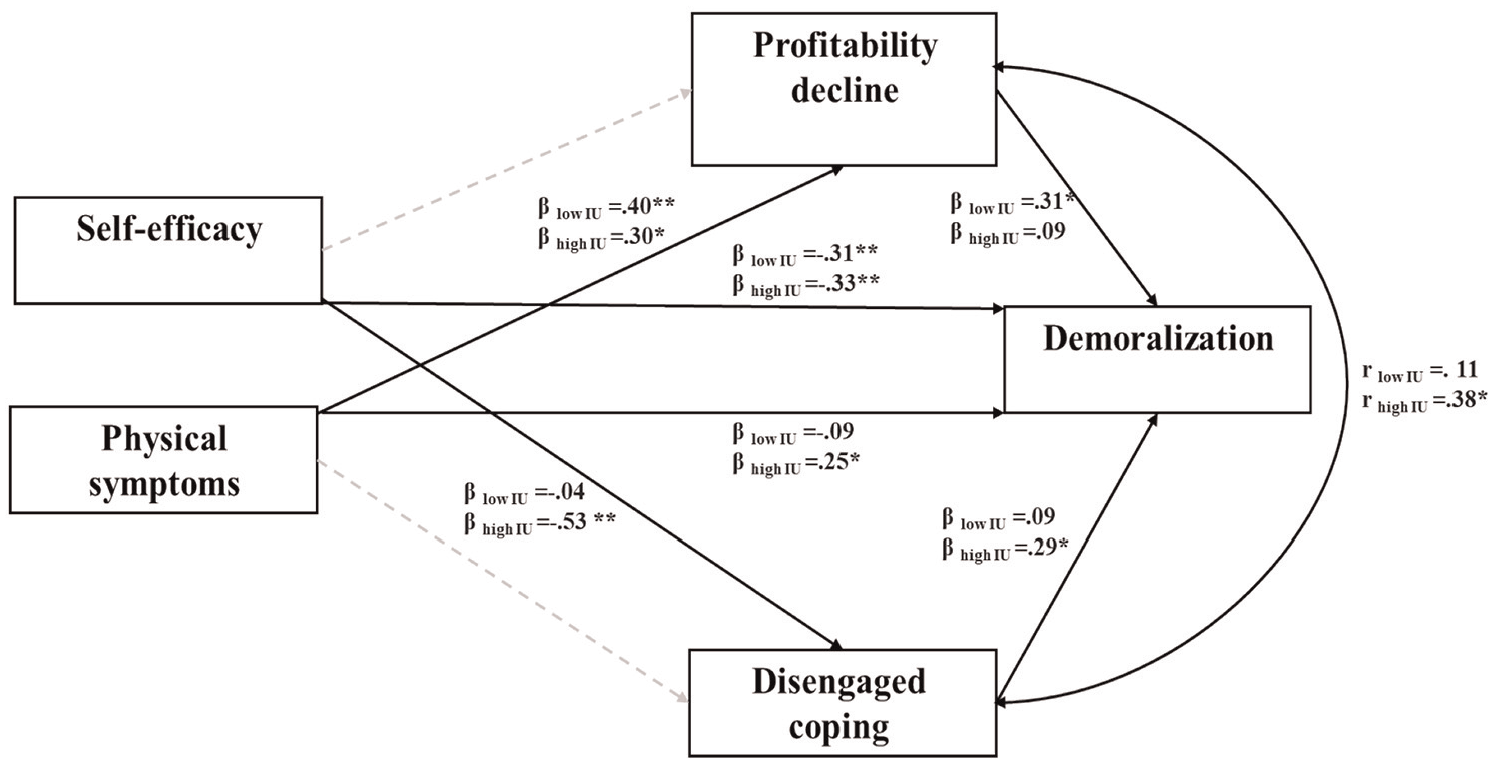
Direct and indirect associations among study variables.
In the next step, the total, direct and indirect effects (unstandardized and standardized) were further tested for size and statistical significance, using 5000 bootstrap samples. Figure 1 and Table 4 summarize the standardized direct and indirect effects and corresponding statistical significance values. The model depicted several direct effects: In both groups, in accordance with our first hypothesis, physical symptoms score was directly and positively associated with business profitability decline (high IU: β = 0.30, CI [0.02, 0.48], p = 0.02; low IU: β = 0.40, CI [0.16, 0.54], p = 0.03). In addition, in both groups, self-efficacy was directly and negatively associated with demoralization (high IU: β = −0.33, CI [−0.61, −0.02], p = 0.01; low IU: β = −0.31, CI [−0.59, −0.03], p = 0.02), such that the higher the self-efficacy, the lower the demoralization. Thus, our first hypothesis was partially supported.
Direct effects and 95% confidence intervals for final model by low and high IU.
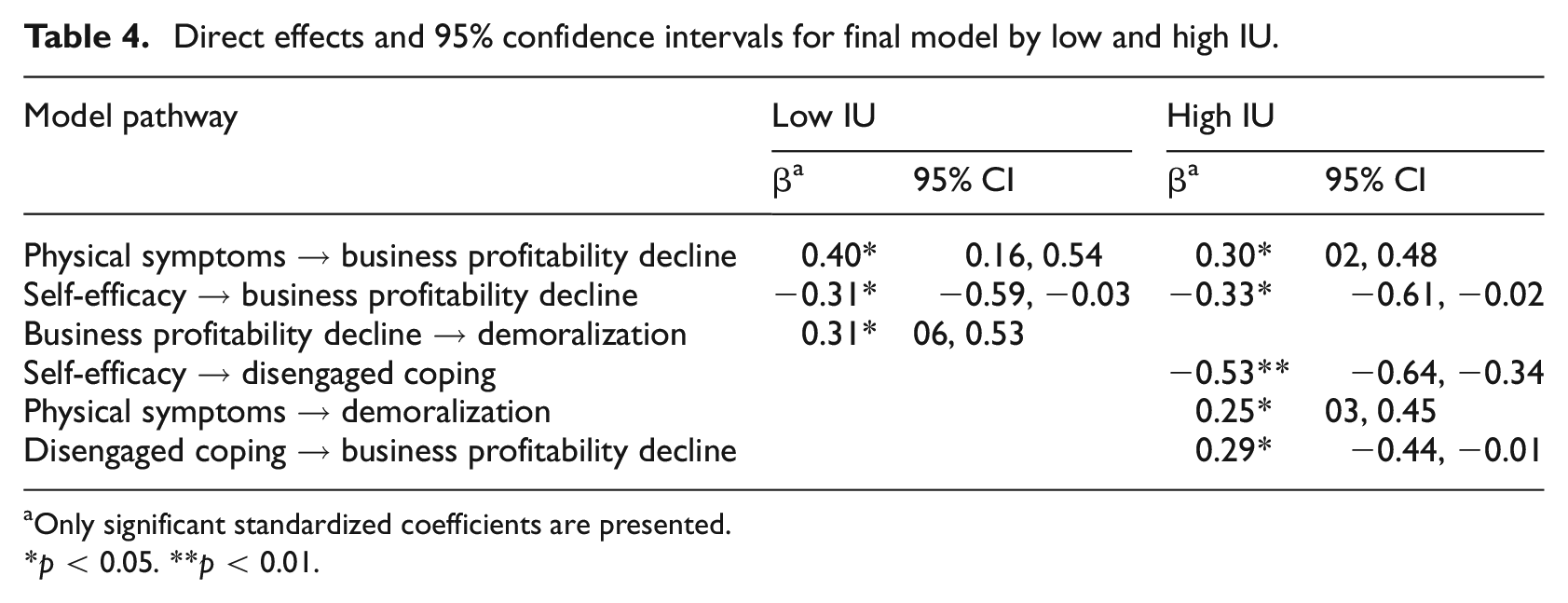
Only significant standardized coefficients are presented.
p < 0.05. **p < 0.01.
In contrast, the following direct associations were obtained in only one group (see Table 4). In the low IU group, business profitability decline was directly and positively associated with demoralization, such that the more the business profitability decline, the higher the demoralization. In the high IU group, self-efficacy was negatively associated with disengaged coping, such that the higher the self-efficacy, the lower the disengaged coping. In addition, in the high IU group, physical symptoms were positively associated with demoralization, so the higher the physical symptoms, the higher the demoralization. Finally, for the high IU group, disengaged coping was positively associated with business profitability decline and demoralization, such that the higher the use of disengaged coping, the higher the business profitability decline and the higher the demoralization (Figure 1). Therefore, our second hypothesis was partially supported.
Finally, to examine the third hypothesis, we tested the mediating effects of business profitability decline and disengaged coping strategies on the relationships between physical symptoms, self-efficacy, and demoralization, with particular attention to the role of IU. Business profitability decline mediated the relationship between physical symptoms and demoralization only in the low IU group. The higher the physical symptoms, the greater the decline in business profitability, which was associated with higher demoralization levels. Disengaged coping mediated the association between self-efficacy and demoralization only in the high IU group (see Table 5). The higher the self-efficacy, the lower the use of disengaged coping, which was related to higher demoralization. Accordingly, the third hypothesis was partially supported.
Direct, indirect, and total effects and 95% confidence intervals for final model by low and high IU.

p < 0.05. **p < 0.01.
Discussion
The present study indicated a significant relationship among business profitability decline, IU, and high levels of demoralization in self-employed individuals with CD. Self-employed individuals with CD often encounter unique difficulties in performing their job roles appropriately, which affects their health. In addition, the results show that IU moderated the relationships between the study variables. Self-employed individuals with CD who were less tolerant of uncertainty had a higher risk of psychological and work-related difficulties.
This study was the first to examine the effects of business profitability, disengaged coping, and IU on the relationships of physical symptoms and self-efficacy with demoralization among self-employed individuals with CD. Our first hypothesis was partially supported. The results suggest that self-employed individuals with CD cope with not only uncertainties related to their illness (e.g. possibility of progression of their condition) but also unique uncertainties associated with being self-employed (maintaining business). Specifically, individuals in the high IU group experienced difficulties tolerating multiple uncertainties and experienced high demoralization compared with the low IU group. This supports previous studies that found a negative association between inability to tolerate uncertainty and emotional and overall well-being (Hong and Lee, 2015).
The present results partially support the second hypothesis. Our results stress that physical symptoms had a significant effect on business profitability decline among self-employed CD individuals, independently from the IU level. These results are in accordance with previous studies, which indicated that self-employed individuals with cancer reported a more significant decrease in their income, higher levels of financial concerns, higher economic uncertainty, and poorer self-rated health (Torp et al., 2019). Our research revealed no significant associations between self-efficacy and business profitability decline. Study findings show that the higher the use of disengaged coping, the higher the business profitability decline and the higher the demoralization in the high IU group. Additionally, for self-employed individuals with CD, negative relationships between self-efficacy and disengaged coping were partially moderated by high IU. Positive relationships between physical symptoms and demoralization were partially moderated by high IU. Positive relationships between disengaged coping and business profitability decline were partially moderated by high IU. No previous studies were found to compare them with the present results. Our study findings emphasize that self-employed individuals with CD who are less tolerant of uncertainty are at higher risk of using disengaged coping and experiencing demoralization. To summarize, self-employed individuals with high IU levels might be disproportionately affected by their CD situation. Therefore, it might be helpful to identify these individuals early in the treatment process because they might profit from interventions that modify their IU levels.
Our third hypothesis was partially supported. Specifically, low use of disengaged coping mediated the relationship between high self-efficacy and low demoralization for self-employed individuals with CD only in the high IU group. Previous studies pointed to self-efficacy as a strong personal resource that enables efficient coping with various stress situations (Lazarus and Folkman, 1984), including physical illness (Jones et al., 2023; Mehawej et al., 2023) and psychological distress (Dymecka et al., 2021; D’Souza et al., 2023). To the best of our knowledge, this is the first study to examine the role of self-efficacy in modifying the harmful effects of demoralization in this population, especially in relation to coping as a mediator and IU as a moderator. Additionally, high physical symptoms were associated with more business profitability decline, which mediated the relationships with high demoralization only in the low IU group. A possible explanation is that individuals in the low IU group are initially more vulnerable than the high IU group to harmful physical effects; as a result, they might experience much more business profitability decline, which leads to high demoralization. This is in accordance with previous studies, which have shown that a high degree of uncertainty among individuals with chronic diseases can lead to worsening health conditions, increased anxiety and depressive symptoms (Kurita et al., 2013; Sajjadi et al., 2015), impaired ability to maintain daily life functions, and negative effects on quality of life (Sav et al., 2015).
The present results have relevant practical future implications. First, self-employed individuals with CD should be encouraged to engage in planned treatment programs. Second, it is advisable to provide them with detailed information on their health condition and interventions that promote self-confidence and self-efficacy. Because IU is a significant factor in prolonging worry and uncertainty, interventions that promote tolerance and acceptance are highly recommended after CD diagnosis. For example, a study of mindfulness-based interventions among undergraduate psychology students in the United States showed that higher levels of mindfulness may lead people to perceive internal experiences as less threatening, thereby increasing their ability to tolerate uncertainty and decreasing the need to worry and engage in behaviors that perpetuate health anxiety (Kraemer et al., 2016). A longitudinal study in Australia showed that emotion regulation (e.g. rumination and thought suppression) served as a significant mediator in the relationship between IU and both anxiety and depression in the general population (Sahib et al., 2024). Based on these examples involving the general population, providing mindfulness-based interventions and minimizing the use of maladaptive emotion regulation, such as rumination and thought suppression, could be potential approaches to alleviating emotional difficulties among self-employed individuals with CD.
Several limitations of the study should be highlighted. Our data were collected from a single source, which might have resulted in single-source bias. Further, because the study was cross-sectional, caution should be exercised regarding the direction of the relationships among the variables. However, this is the only study to have investigated demoralization among self-employed individuals with CD. We suggest that future investigation of this group and related policy activities should consider their mental state (demoralization) and personal traits (IU) as important factors that affect health-related quality of life, emotional well-being, and overall quality of life.
Conclusions
The present study extended the literature on self-employed individuals with CD, providing insight into the impact of business profitability decline, self-efficacy, and coping with demoralization. Moreover, IU is especially relevant to self-employed people because they must cope constantly with unpredictable work-related events (Rothausen and Henderson, 2019). As a result, it is important to identify people with CD who are prone to IU. Based on our preliminary findings, we also recommend extending research to examine the effect of other personal resources, such as self-compassion and personal resilience, on IU among self-employed individuals with CD.
Footnotes
Authors’ contribution
All authors contributed to the study conception and design. Material preparation was performed by all authors. The analysis was performed by WS.
Data sharing statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Approval was obtained from University of Haifa Committee for Ethical Research with Humans (permit no. 248/21).
Informed consent
Informed consent was obtained from all individual participants included in the study. In addition, all methods were performed in accordance with University of Haifa Committee for Ethical Research with Humans guidelines and regulations.
Consent for publication
Consent for publication is not applicable as it does not contain any identifiable data.