
Abstract
People are exposed to misinformation about dieting practices every day on social media which can influence their health and wellbeing. While misinformation research has largely focused on general vulnerabilities to misinformation and strategies to counteract its spread, limited work has examined how specific harmful content, such as dietary misinformation, influences vulnerable groups, particularly those at risk of eating disorders (EDs). This study investigated whether individuals at risk of an ED were more likely to endorse Dietary Misinformation. After completing measures of dietary intentions, health conscientiousness and weight concern, 215 participants completed a behavioural measure of belief rigidity (i.e. Bias Against Disconfirmatory Evidence; BADE), and measures of general and diet-specific misinformation susceptibility. The findings suggest that participants who score highly on weight concern (ie, potentially at risk for an ED), were less likely to show belief flexibility and integrate new evidence and are more inclined to endorse diet-specific misinformation. This research highlights the broader importance of drawing attention to how particular misinformation online can affect the wellbeing of those potentially in vulnerable groups, in this case those at ED risk.
Introduction
The advent of social media has seen an increase in access to mass content and information about health, wellness and nutrition. This widespread access has also created opportunities for inaccurate dietary information to spread (Suarez-Lledo and Alvarez-Galvez, 2021). Dietary misinformation (DM) refers to false, misleading or unverified information about nutrition and dietary practices, which can lead to misconceptions and potentially harmful behaviours among vulnerable groups (Lofft, 2020; Sidhu, 2018). The rise of social media influencers focusing on diet and exercise has exacerbated this issue, as users are increasingly exposed to harmful messages from ‘authority figures’ with no scientific credibility (Lofft, 2020; Vasconcelos et al., 2021). For example, Topham and Smith (2023) conducted a discourse analysis revealing that popular social media trends, such as ‘What I Eat in A Day’ videos, often present misleading content as credible and scientific, illustrating how easily people can be exposed to potentially harmful information. While there has been extensive research on the semantics and spread of DM, less attention has been given to identifying who is more likely to endorse DM. This limitation also extends to our understanding of how individuals at risk of diet-related health concerns (e.g. eating disorders) interact with and process dietary misinformation.
People at risk of or those who have eating disorders (EDs) have been shown to demonstrate several cognitive biases in attention and when interpreting new information, which have relevance for interpreting information concerning body image and weight. The seminal work of Williamson et al. (2004) suggested attentional bias – the act of favouring or selectively processing information that is focused on body weight, dieting and control of food intake – was central to the development and maintenance of an ED. Indeed, Stott et al. (2021) and Rowlands et al. (2020) have highlighted that people at risk for an ED risk held a particular salience toward information focused on weight when faced with a multitude of other forms of information, regardless of its credibility and relevance. In other words, people at risk of an ED are more likely to fixate on information related to their specific weight concerns, rather than evaluating its credibility and relevance (Iceta et al., 2021; Ioannidis et al., 2021; Keegan et al., 2021; Matheson et al., 2019). This could suggest that DM is appealing based on a person’s fixated interest for the topic. This is like the trend more generally observed, that misinformation is often shared by individuals who prefer to draw attention to content that challenges the status quo or presents an alternative narrative about how the world works (e.g. conspiracy theories; Georgiou et al., 2021a, 2021b).
In addition to attention and information processes biases, people at risk of ED show similar cognitive biases when challenging their held beliefs to those who endorse misinformation and conspiracy theories. According to Tenconi et al. (2023), individuals at risk of an ED often exhibit a rigid adherence to incorrect beliefs about their worldview, resulting in a selective focus or ‘cherry-picking’ of information that supports their pre-existing beliefs and the rejection of counterevidence, regardless of its credibility (Balzan et al., 2022; Dent and Martin, 2023). Indeed, Tenconi et al. have emphasized that research into belief integration bias could enable us to shed light on hidden dimensional aspects of ED risk. This suggests that the Bias Against Disconfirmatory Evidence (BADE; Sanford et al., 2014), present in people who endorse misinformation and conspiracy theories, and those unwilling to challenge misinformed views on alternative health information (Bronstein et al., 2019), could also be present in people at risk of an ED. Further, Balzan et al. (2022) have shown that people with increased ED risk (a) draw attention toward information on body weight or diet, (b) may be more susceptible to endorse such content and (c) are then likely to remain in agreement with such content in the face of counterevidence. Yet, research has not examined whether the same biases make those with ED risk more susceptible to DM.
Considering the pervasiveness of false dietary and nutritional content available in abundance online, this raises the question of how widely accepted DM is among those at ED risk, and, more importantly, how prevalent are both DM endorsement and the associated cognitive biases. By understanding the potential prevalence, it could be further detailed whether DM is having an adverse impact on the health and wellbeing of potential vulnerable groups. More than 45% of dietary advice and nutritional information presented on social media is considered inaccurate, with many fad-diet approaches widely accepted within the general population (Denniss et al., 2024).
The present study will investigate the relationship of ED risk as a continuum across the general population and the susceptibility to endorse DM. Specifically, building on the work of Tenconi et al. (2023), we will explore the relationship between cognitive biases associated with ED risk, and their relation to the weight concern, dietary intention and level of health conscientiousness amongst the general population, and to whether this may predict engagement with DM. We will also examine whether ED risk is predictive solely of DM, or whether it may also lead to a higher susceptibility to more general misinformation shared online. The following investigations will enable us to assess whether exposure to DM is an issue for the wellbeing of those in more vulnerable groups.
Taken together, previous literature demonstrates that individuals at risk for EDs exhibit cognitive biases that may increase their susceptibility to endorsing misinformation. These biases include selective attention to shape and weight-related information (Rowlands et al., 2020; Williamson et al., 2004) and a rigid adherence to incorrect beliefs despite counterevidence (Tenconi et al., 2023). Therefore, we hypothesize that individuals with higher ED risk will be more likely to endorse dieting-related misinformation (which focuses on weight change) compared to neutral misinformation.
Furthermore, in line with the attention bias model of ED risk, we expect that the relationships between health consciousness and dieting intentions with dieting misinformation susceptibility will depend on ED risk. Specifically, as ED risk increases, the associations between health consciousness, dieting intentions and misinformation susceptibility may reflect maladaptive patterns – where heightened concern for health and diet does not necessarily serve as a protective factor but instead amplifies susceptibility to misinformation. Thus, we predict that ED risk will mediate the relationship between health consciousness, dieting intentions and susceptibility to dieting misinformation. In other words, individuals with higher ED risk may engage with health-related and dietary content in a way that makes them more vulnerable to endorsing misinformation rather than critically evaluating it.
Method
Participants
The study involved a total of 215 participants (110 female, 105 male). This was a general population sample gathered from the international panel Cloud Research aged between 18 and 70 (M = 27.99, SD = 9.77). Participants were predominantly sampled from US, UK, Canada, Australia and South Africa (85%), and the remainder mostly from continental Europe. The demographics of the sample are described in Table 1. Forty-two participants disclosed receiving a previous clinical diagnosis from a health professional, with 11 indicating a diagnosis of an ED at some stage during their childhood or adulthood. Importantly, regardless of disclosed prior diagnosis, 56 (26.0%) participants scored above the potential risk of eating disorders according to the weight concern scale (≥47), which is well above the average rates amongst the general population (Alhaj et al., 2022). Gpower analysis indicated at least 150 cases would be sufficient to achieve a power of 0.80 for multiple regression with six predictors and anticipated R2 = 0.30 and an alpha level of 0.05.
Demographic characteristics of the sample (N = 215).

Sampling procedure
The study used an international sample and was advertised as an investigation into how people view the world and their opinion on common health claims. All participants received monetary compensation for their time and effort ($9US per hour). The data retrieved was made anonymous and only presented in group form. The study was approved by the Human Research Ethics Subcommittee at Flinders University as a low-risk study.
Study measures
Demographic background
Participants were asked to provide demographic information, including gender, age, country of residence, highest education level, current employment status and prior history of clinical diagnosis.
Weight-Concerns Scale
The Weight Concern Scale (WCS; Killen et al., 1994), designed to measure an individual’s preoccupation with weight and fear of weight gain, is frequently used in research related to EDs, body image and related psychological concerns (Jenkins et al., 2020; Ross and Wade, 2004; Shagar et al., 2017). Consistent with prior research (Jacobi et al., 2004; Killen et al., 1994) the WCS is most often used to indicate risk for ED development. The WCS is a one-factor scale consisting of five questions rated on 4-point (item 4), 5-point (items 1, 2 and 5) and 7-point (item 3) Likert-type response scales. The McDonald’s Omega was 0.81, which is above the typical 0.70 indicator of a robust level of internal reliability (Hayes and Coutts, 2020).
Diet Intentions Scale
The Diet Intentions Scale (DIS; Cruwys et al., 2013) is designed to measure an individual’s intentions and motivations regarding dieting. This scale is particularly useful in understanding the psychological factors that influence dieting behaviour and the likelihood of engaging in dieting practices. The DIS particularly contributes a focus on naturalistic dieting behaviour and future-oriented beliefs regarding dieting behaviour. Each item on the DIS is scored from a range of 1 (Strongly Disagree) to 5 (Strongly Agreed), with the final question across a 5-point Likert range using specific valence-phrasing. The McDonald’s Omega was 0.78, which again, is above the typical 0.70 indicator of a robust level of internal reliability (Hayes and Coutts, 2020).
The Health Consciousness Scale
The Health Consciousness Scale (HCS; Gould, 1990) is a self-report instrument that assesses an individual’s level of attention to general health and health behaviours. It measures the level of knowledge about the body, the importance placed on health and the impact of lifestyle on health (Remr, 2023). The HCS is comprised of nine items, each assessed on a 5-point Likert-type scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). The total score ranges from 9 to 45, with a higher score indicating greater health consciousness. Health consciousness has been shown to act both as a barrier to weight concerns in populations with lower levels of eating disorder symptomatology, but it may also be considered a risk factor when combined with higher levels of eating disorder symptoms (Ellickson-Larew et al., 2013). The McDonald’s Omega was 0.88.
The Brief Misinformation Susceptibility Test
The Misinformation Susceptibility Test (MIST; Maertens et al., 2024) is a validated measure of misinformation susceptibility with an emphasis on discernment between true and false items. The MIST-8 was designed as the briefest form of the assessment and has been cross-validated against other MIST iterations and convergent measures of misinformation (Maertens et al., 2024). Participants are asked to rate whether a piece of information is ‘True’ or ‘Fake’, with each correct response corresponding to a score of 1 (0 for incorrect), with a range of 0–8. This measure has been shown as a valid measure of misinformation in the general population across a range of age, nationality and clinical contexts (Maertens et al., 2024; Roozenbeek et al., 2022). The McDonald’s Omega was 0.78.
The Diet-related Misinformation Susceptibility Test
The Dietary-related Misinformation Susceptibility Test (D-MIST) was developed for the present study to mirror the format of the MIST (Maertens et al., 2024). It targets popular misinformation about fad-diets prevalent on social media (Statistica.com; Anderson, 2023). The D-MIST consists of six items, each designed to assess an individual’s susceptibility to dietary-related misinformation. Participants are asked to rate a piece of information on a 5-point Likert scale from ‘Highly Fictitious’ to ‘Highly Credible’. In total, there are four false-diet items and two true items for participants to assess. To further examine cognitive biases in individuals at risk of EDs, the ‘false’ items in the D-MIST were designed to suggest either a weight-focused ‘fact’ or a non-weight-focused fact, with two of the four ‘false’ items randomly assigned to either the weight focused or neutral formulation of the item (see Appendix A).
Participants were given an overall engagement with false diet content score for the four items they were exposed to, with each item scored from 1 (highly unlikely) to 5 (highly likely). Participants received a total score for the false items ranging from 4 to 20, as well as separate scores for ‘False-Neutral’ and ‘False-Weight Focused’ items. Scores for the two items in each of these categories ranged from 2 to 10. Participants were also presented with weight-focused and neutral forms of real diet information across two items (i.e. one of each). The McDonald’s Omega was 0.77, indicating adequate reliability.
Belief Inflexibility: The Bias Against Disconfirmatory Evidence Task
The Belief Inflexibility: The Bias Against Disconfirmatory Evidence Task (BADE; Woodward, Moritz, Chen, 2006; Woodward, Moritz, Cuttler, and Whitman, 2006) consists of several delusion-neutral scenarios which can assess an individual’s persistence to hold certain beliefs in the face of disconfirmatory evidence. The BADE assessment involves participant ratings of the plausibility of four statements for their fit to a specified scenario, which is based on a single piece of information (i.e. ‘Jenny can’t fall asleep’). Each scenario had one true interpretation, two lure interpretations and one absurd interpretation from the four statements. The plausibility of the four interpretations is rated for each scenario from a scale of 0 (Poor) to 100 (Excellent).
Each scenario starts with the statement (e.g. ‘Jenny can’t fall asleep’) and participants rate the four statements provided. After this initial round of ratings, a second piece of information is displayed (i.e. ‘Jenny can’t wait until it is finally morning’). The participants then rate the four statements again. This is repeated with a third and final piece of information (i.e. ‘Jenny wonders how many presents she will find under the tree’). The true interpretation (‘Jenny is excited about Christmas morning’) appears uncertain initially but becomes clearer as additional information is revealed (e.g. ‘Jenny is nervous about her exam the next day’), which should prompt the participant to update their choices. Meanwhile, the lure interpretations appear plausible initially but become increasingly less implausible as additional information is revealed (e.g. ‘Jenny loves her bed’).
Statistical analysis
Pearson’s correlation coefficients were first used to gauge the relationships between each measure in the present study. As presented in the aims of this study, ED risk will be measured across a continuum to gauge its influence within the general population on dietary misinformation, and for exploratory analysis also be used as a dichotomous variable according to cut-off score for eating disorder risk. In accordance with the methods of Jacobi et al. (2004), scores of ≥47 on the Weight Concern Scale (WCS) were used to form comparative groups between those ‘at-risk’ of eating disorders and a normative subsection of the current sample. These groups were then compared across all dependent variables, and on their scores from the Bias Against Disconfirmatory Evidence (BADE) task, as per the findings of Tenconi et al. (2023). To gauge whether ED risk may predict dietary misinformation, a series of hierarchical linear regression models were used to gauge significance, followed by a mediation analysis to explore whether ED risk mediated other covariates and their relationship to BADE performance or misinformation endorsement.
Results
Preliminary analysis
Prior to the commencement of analysis, all data were confirmed to be suitable for parametric assessment. To ensure the appropriateness of ANOVA, we assessed the normality of the data using the Shapiro-Wilk test, which indicated that the residuals were normally distributed (p > 0.05). Additionally, Levene’s test confirmed the assumption of homogeneity of variances (p > 0.05). Given that both assumptions were met, a parametric ANOVA was deemed appropriate for this analysis. A one-way ANOVA revealed no significant differences in Dietary Intentions, Health Conscientiousness, Weight Concern or either misinformation measures (e.g. MIST, D-MIST) based on demographic variables of level of education. There were trend-level differences according to age groups according to Weight Concern with those aged 18–25 showing the highest scores, F(4, 212) = 2.25, p = 0.09.
Participants were categorized based on whether DM items were weight-focused or neutral to ensure that observed differences were not a result of demand characteristics (i.e. variations due to item content rather than the manipulation). A linear mixed-effects model was conducted to assess whether randomization into weight-focused or neutral items affected participant responses on the D-MIST. No significant differences were found due to this variation (t = 1.20, p = 0.24; AIC = 148.15, BIC = 155.45). These results suggest that the randomization of item valence (neutral vs weight-focused) did not systematically influence participant responses, supporting the validity of the randomization process.
Psychometric and demographic measures
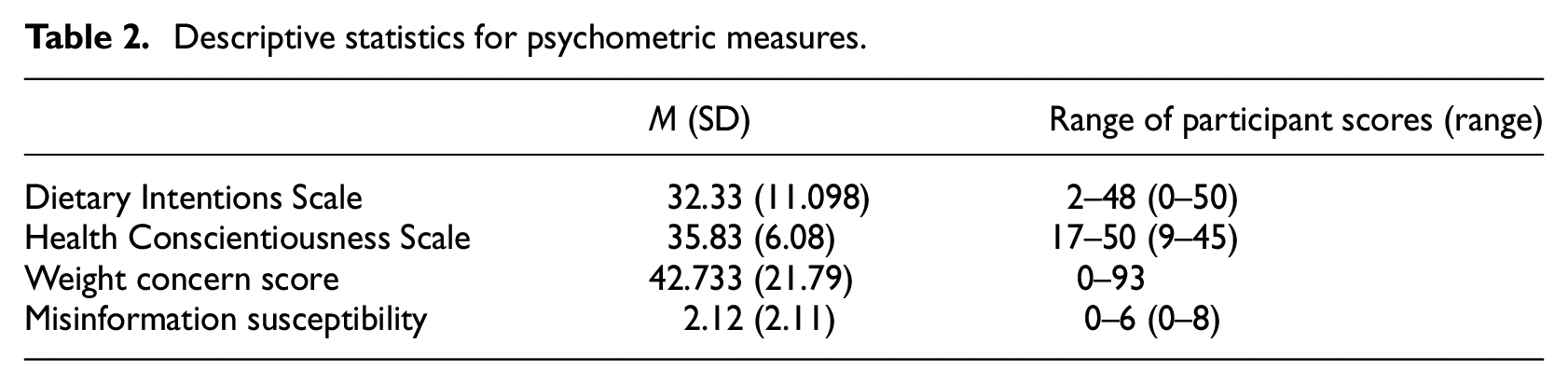
Table 2 summarizes the descriptive results for the various psychometric variables of this study. As indicated, a considerable number of Weight Concern Scale (WCS) scores were above the cutoff for ED risk, while the sample generally fell just below this cutoff. Regarding diet intentions and health conscientiousness, participants’ scores were generally above the midpoint of the scale. These results suggest that the convenience sample drawn for this study contains a sizable proportion of participants who place significant focus on their health and nutrition. Misinformation susceptibility scores were similar to results found in other research concerned with the general population (Roozenbeek et al., 2023).
Descriptive statistics for psychometric measures.
Correlation analysis
Pearson correlations are presented in Table 3. Consistent with our hypotheses, there were moderate positive correlations between weight concern scores and dietary intentions, which were also positively associated with dietary misinformation endorsement. Health conscientiousness showed an almost significant negative association with D-MIST scores (r = −0.135, p = 0.060) and a significant negative association with general misinformation endorsement (r = −0.217, p = 0.004). This suggests that individuals who are more conscientious about their health may be more attentive to the content presented across both measures and less likely to endorse incorrect dietary information.
Pearson’s correlation between covariates and task performance indices of the present study (N = 201).
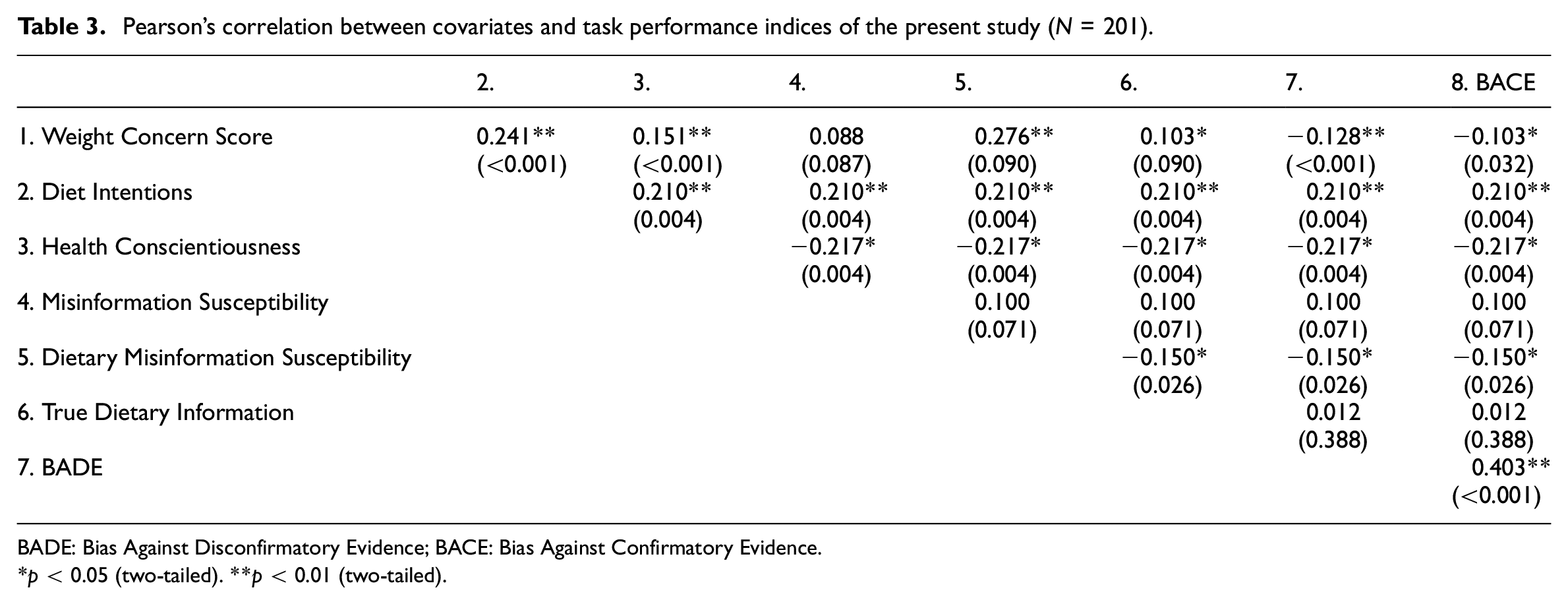
BADE: Bias Against Disconfirmatory Evidence; BACE: Bias Against Confirmatory Evidence.
*p < 0.05 (two-tailed). **p < 0.01 (two-tailed).
Weight concern was associated with a higher susceptibility to a bias against disconfirmatory evidence (BADE; r = −0.128) and a bias against confirmatory evidence (BACE; r = −0.103), consistent with Tenconi et al. (2023). A noteworthy finding is the association between health conscientiousness and a higher BADE effect, alongside a lower susceptibility to both misinformation measures. This could be interpreted as individuals who are more conscientious may be less likely to alter their beliefs but are not necessarily more prone to misbeliefs.
Comparison of cognitive flexibility and misinformation endorsement according to eating disorder risk
To assess whether individuals at risk of eating disorders (ED) show a greater association with cognitive biases and beliefs associated with general and dietary misinformation, the WCS was used as a dichotomous variable in Table 4 (i.e. a cutoff score for ED risk). According to an independent samples t-test, participants who scored above the cutoff for ED risk were significantly more likely to engage in misinformation, t(213) = 4.25, p < 0.001, d = 0.15. There were also non-significant trends suggesting at-risk individuals were more likely to demonstrate a BADE effect, t(213) = 1.92, p = 0.067, d = 0.11, and lower levels of evidence integration, t(213) = 1.78, p = 0.078, d = 0.10. These results suggest preliminary evidence that individuals at risk of an ED may process evidence differently compared to the general population, particularly in relation to deciphering misinformation content.
Comparison of those above and below the Weight Concern Cut-off for Eating Disorder Risk.
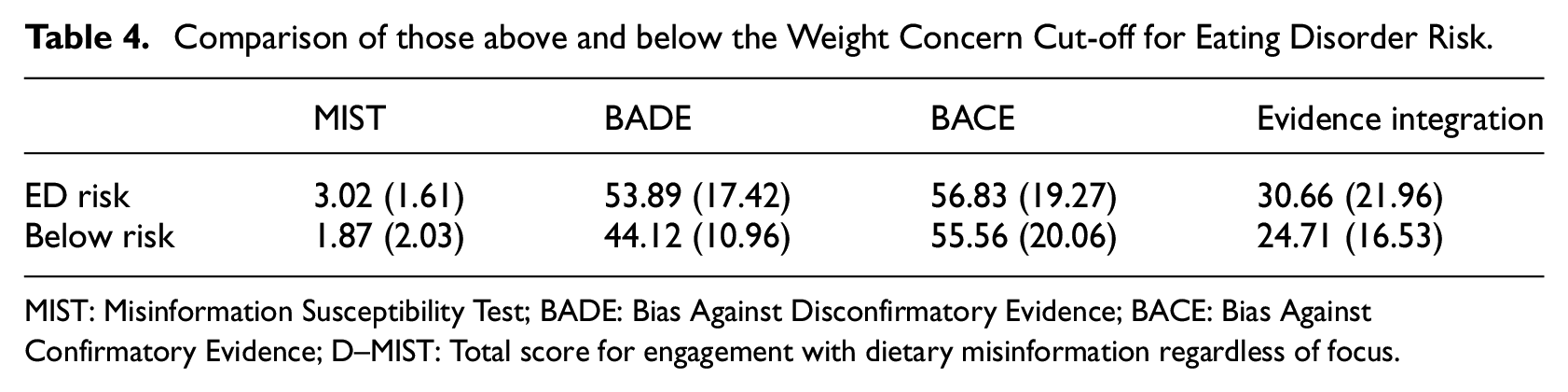
MIST: Misinformation Susceptibility Test; BADE: Bias Against Disconfirmatory Evidence; BACE: Bias Against Confirmatory Evidence; D–MIST: Total score for engagement with dietary misinformation regardless of focus.
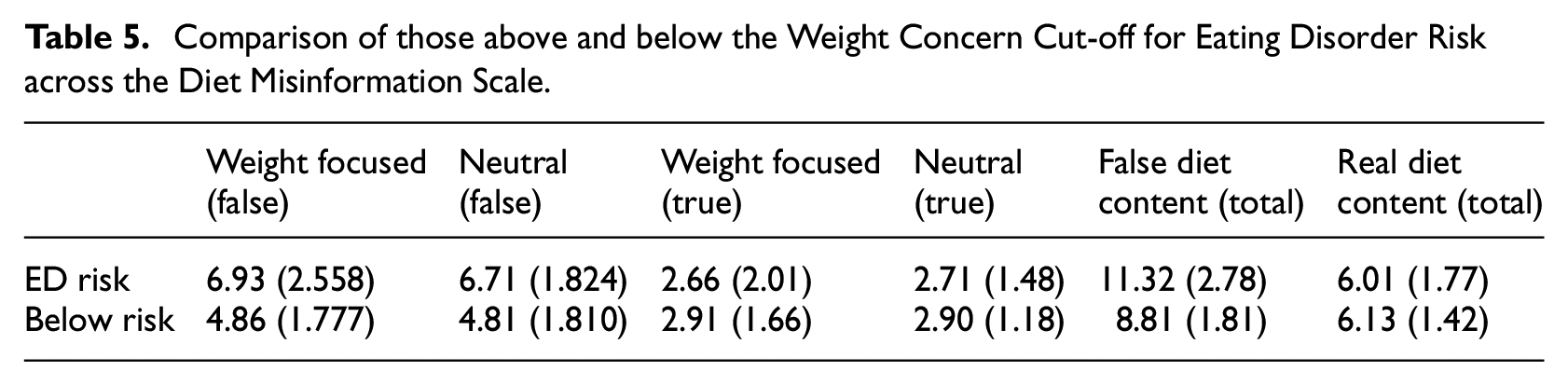
As shown in Table 5, comparisons were also made across each domain of the dietary misinformation assessment. An independent sample t-test revealed that participants above the cutoff for ED risk were more likely to endorse false dietary misinformation overall t(213) = 3.76, p < 0.001, d = 0.13. This increased likelihood was observed for both weight-focused misinformation t(213) = 2.98, p = 0.003, d = 0.16 and neutral false content t(213) = 2.45, p = 0.015, d = 0.10.
Comparison of those above and below the Weight Concern Cut-off for Eating Disorder Risk across the Diet Misinformation Scale.
Multiple regression analysis of dietary misinformation endorsement
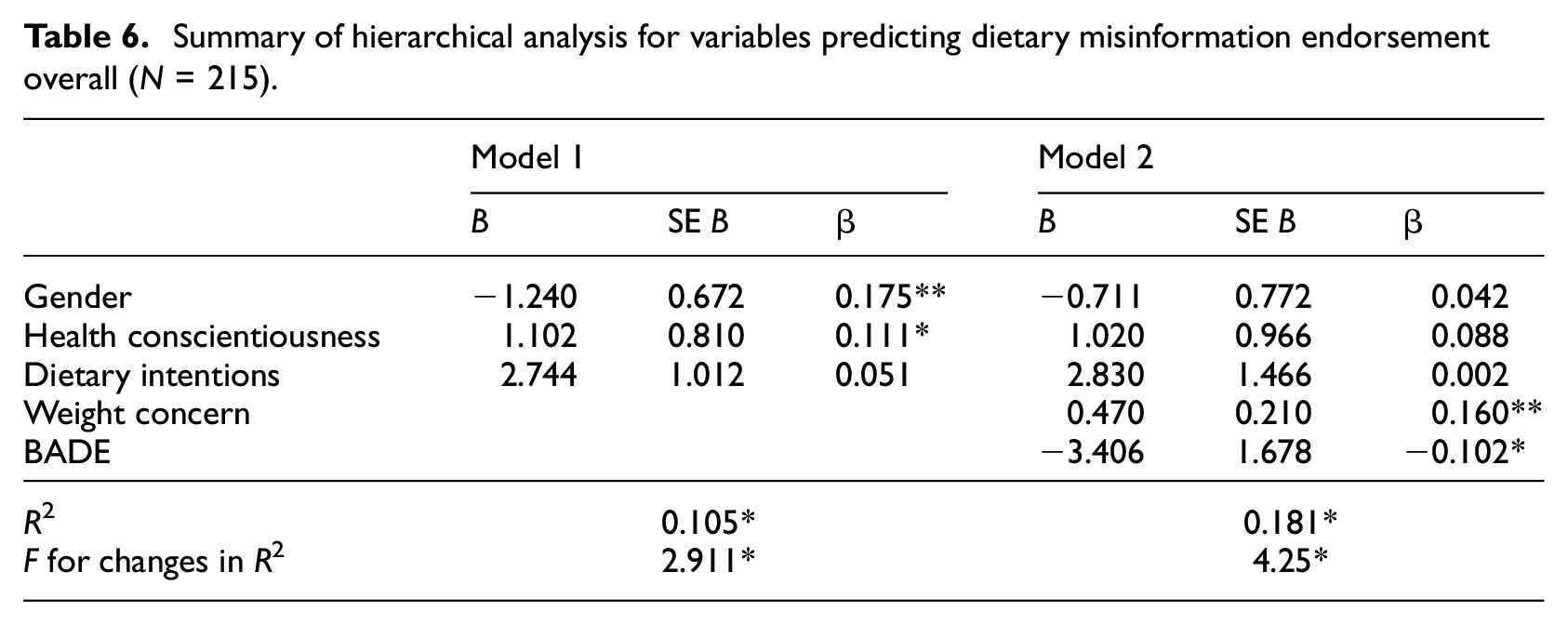
As dietary intentions, health conscientiousness and weight concern scores were associated with each other in Table 3, as well as with both cognitive biases (i.e. BADE) and misinformation susceptibility (i.e. MIST, D-MIST scores), it is important to examine whether these variables maintained their predictive value for dietary misinformation after controlling for each covariate. According to a hierarchical multiple regression (Table 6), gender and health conscientiousness were significant predictors of changes in dietary misinformation endorsement, while dietary intentions did not show predictive value. The addition of factors related to ED risk and cognitive bias (i.e. weight concern scores and BADE performance) increased the model’s explained variance to 18%, with only weight concern and BADE performance remaining as significant predictors of dietary misinformation endorsement. Overall, these results suggest that the associations found in Table 3 may not hold when controlled for in a predictive model but could still be explored in a mediation analysis.
Summary of hierarchical analysis for variables predicting dietary misinformation endorsement overall (N = 215).
Mediation analysis
The findings of the hierarchical multiple regression shown in Table 6 are further supported by examining the role of weight concern as a mediator on each performance measure. Considering the weak relationships found within previous models, the significance of indirect effects was tested using bootstrapping procedures suggested by Hayes and Scharkow (2013; n = 5000), with confidence intervals set at 95%.
According to a mediation model shown in Figure 1, the relationship between Dietary Intentions and BADE performance showed a weak direct effect (R2 = 0.10, 95% CI [0.069, 0.198], p = 0.001). However, a statistically significant indirect effect through WCS scores (R2 = 0.17, 95% CI [0.109, 0.303], p = 0.001) suggests that the relationship between a person’s intentions to diet and certain cognitive biases is mediated by their level of weight concern. In other words, only when individuals express concerns about their body weight or are at risk of developing disordered eating behaviours (i.e. scoring high on the Weight Concern Scale) do their dieting intentions relate to a reduced ability to consider counterevidence. Furthermore, as shown in Figure 2, a similar relationship exists between Dietary Intentions and endorsement of DM.
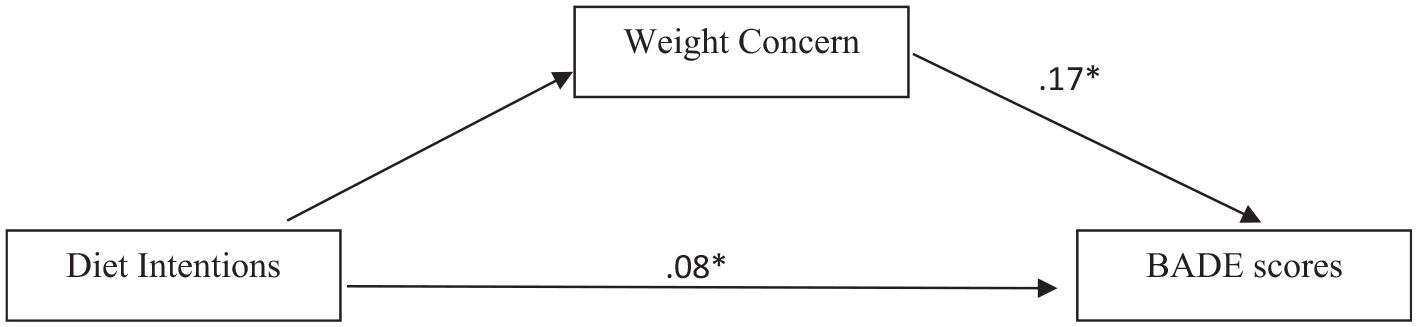
Weight Concern Score mediates the relationship between Dietary Intentions and BADE performance.
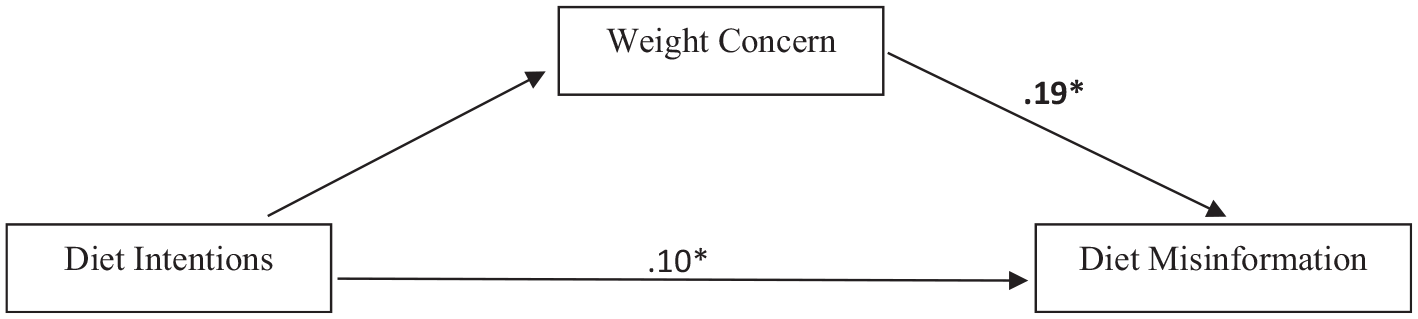
Weight Concern Score mediates the relationship between Dietary Intentions and Dietary Misinformation Endorsement.
A second mediation model was tested to examine the indirect effect of weight concern on the relationship between Dietary Intentions and dietary misinformation endorsement (i.e. D-MIST Total Score on False Items). Dietary Intentions had a weak significant, direct effect on misinformation endorsement (R2 = 0.10, 95% CI [0.085, 0.312], p = 0.038). However, a significant indirect effect was found through WCS scores (R2 = 0.19, 95% CI [0.120, 0.420], p = 0.001), suggesting that the connection between intentions to diet and susceptibility to dietary misinformation is mediated by an individual’s level of concern about their weight. This highlights that weight concerns may exacerbate a person’s likelihood of endorsing false dietary information.
Discussion
The present study aimed to investigate the relationship between eating disorder (ED) risk as a continuum across the general population and susceptibility to endorsing dietary misinformation (DM). Overall, the results suggest preliminary evidence that DM may pose a significant issue for individuals across the continuum of ED risk. Those who are less receptive to counterevidence (i.e. exhibit the BADE effect) are also more likely to endorse such misinformation. Additionally, our mediation analysis demonstrated that individuals with dieting intentions may be more prone to cognitive biases and show a preference for diet misinformation, particularly if they also show a heightened level of concern about their weight. Overall, the present study provides a case for how particular DM may pose an issue for the health and wellbeing of those of ED risk.
Implications for misinformation research
While most studies have focused on general engagement with misinformation, such as perceptions of credibility or consequences (Harris, 2024; Lu et al., 2023), few have examined how particular types of misinformation disproportionately affect specific populations. By focusing on DM, this study extends the field by highlighting its unique impact on individuals at risk for eating disorders, thus underscoring the importance of understanding content-specific influences on vulnerable groups.
Additionally, these findings emphasize the need to consider cognitive performance and clinical factors alongside individual difference factors in misinformation research. Our regression analysis demonstrated that the predictive value of dieting intentions and health conscientiousness on dietary misinformation was significantly reduced when BADE performance and WCS scores were included in the model. Without incorporating cognitive performance and clinical measures, the relationship might appear confounded and misrepresent the antecedents of dietary misinformation engagement. Thus, this study provides a novel example of a more holistic approach to modelling misinformation engagement, as urged in recent literature (Peñas et al., 2023).
Implications for eating disorder research
Our results suggest that susceptibility to DM may contribute to the development and of EDs. Indeed, endorsing information that promotes weight loss, regardless of credibility, is of clear benefit to the ED symptom cycle, as it may provide suggestions for new dieting methods (e.g. ‘water fasting’) that serve to address the underlying psychological need (e.g. ‘to lose weight because my body is disgusting’). This idea raises a further consideration: is dietary misinformation shared unintentionally or deliberately within this context? For example, someone with ED symptoms may share diet information that they logically know to be harmful (e.g. eating ice cubes to stay full) because the goal is not to maintain health but instead to lose weight by any means possible. If this was the case, it might be more accurate to categorize this as disinformation, rather than misinformation. Future work should aim to disentangle the motivations for sharing dietary misinformation within online spaces.
Nevertheless, our results raise the possibility that techniques to improve the detection of misinformation could be incorporated into clinical treatment programmes for EDs to reduce the harmful impact of DM that may be encountered online. There is an increasing amount of research which has examined how metacognitive training (MCT) may assist how people with an ED reframe their understanding of their own body and weight, by targeting cognitive biases (Balzan et al., 2023; Grilo and Udo, 2021). Hence, future research may aim to assess whether the same MCT designed to reduce ED symptomology and been previously used in the context of misinformation (e.g. teaching participants how to engage with content; Salovich and Rapp, 2021), may also assist those at risk of an ED in how they engage with dietary misinformation. Moreover, examining if a similar susceptibility to misinformation applies to other ED related stimuli (e.g. exercise tips) could also be a promising avenue of future work.
Limitations and future directions
A limitation of this study relates to the measurement of weight concern and the potential gender bias in the conceptualization of eating disorder risk. The Weight Concern Scale (WCS) primarily conceptualizes weight risk in terms of a drive for thinness (Killen et al., 1994). While males do experience a desire to be thinner, many male body image concerns centre on a drive for muscularity (Murray and Touyz, 2012). As a result, the use of the WCS may have excluded some males with elevated weight and shape concerns related to a desire to increase muscularity rather than reduce weight. Future research should investigate how males with a drive for muscularity perceive weight concerns and explore whether the findings of this study regarding dietary misinformation apply across different weight concern contexts.
Another limitation is that people who have ED symptoms may experience a general cognitive impairment due to malnutrition or motivational factors (e.g. rigid thinking to cope with stress; Rodgers et al., 2023). Hence, future research could assess whether engagement with misinformation is due to a general susceptibility or due to cognitive impairment for those particularly high or at risk of an ED.
This study may also be limited by the influence of pre-existing beliefs. Since the DM content within the D-MIST measure was based on popular misinformation prevalent on social media, participants may have been exposed to this information prior to the study. This exposure could lead participants to respond based on prior beliefs rather than the randomized focus of the false items (i.e. weight-focused vs neutral). Hence, beyond addressing varying forms of weight concern (i.e. thinness vs muscularity), it is also essential that future research vary the level of familiarity with the misinformation content presented in the D-MIST measure. Moreover, as the D-MIST is essentially a replicated measure of the MIST put forward by Maertens et al. (2024), it also may be susceptible to the same limitations in measurement. For instance, as the method of measurement is based on the ability to demonstrate ‘discernment’ (i.e. to not endorse false information and endorse true information), future iterations of the D-MIST put forward may be improved via advancements in how discernment is measured. Higham et al. (2024) suggests that signal detection theory-based measures are less affected by response criteria shifts and may produce a more accurate representation of the true ability to distinguish information. Hence, moving forward, as with most research in the field of misinformation – the way in which diet-based misinformation measures are proposed should consider methods of measurement as well.
Another limitation of this study concerns the use of a convenience sample, which resulted in an age range of 18–70. This is broader than typical for ED populations, so the representativeness of these findings should be interpreted with caution. Also, the sample size of the present study whilst justified via a power analysis, could be considered as a hindrance for the generalizability of the findings. Therefore, a key consideration for the present findings is whether they would replicate in an adolescent population, and to what extent the same cognitive biases are observed from an early intervention perspective.
Conclusion
The results of the present study suggest that individuals who demonstrate a higher level of weight concern, or potentially are at risk of an ED, are more likely to engage in a bias against disconfirmatory evidence and are more likely to endorse dietary specific misinformation. It is evident that this research provides a novel representation for how particular misinformation can influence vulnerable groups, and how targeting DM may be a beneficial step in the ED symptom cycle. Future research should develop upon these findings by investigating whether these relationships can be replicated in other at-risk groups (e.g. adolescents with ED risk), or to whether these same cognitive tendencies represent a future direction for intervention research against misinforming content online.
Footnotes
Appendix A
Author contributions
Conceptualization: NG, MT, TW, VB, RB; Methodology: NG, MT; Formal Analysis: NG; Data Curation: NG; Writing – Original Draft: NG, MT, VB; Writing – Review & Editing: NG, MT, TW, VB, RB; Supervision: RB, TW.
Data sharing statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the School of Psychology, Flinders University.
Ethics approval
This study received ethics approval by the human ethics research committee of Flinders University.
Informed consent
Participants provided consent for data to be analysed, shared and published as part of the informed consent form provided before entering the study.