
Abstract
Studies of internet-delivered cognitive behavioral therapy (ICBT) have documented its efficacy for pediatric Functional Abdominal Pain Disorders (FAPDs), but few have detailed how adolescents experience this. We investigated the lived symptom experiences of eight adolescents (age 13–17 years) with FAPDs, who had received ICBT. Semi-structured interviews were conducted using photo-elicitation, and analyzed using Interpretative Phenomenological Analysis, identifying three main themes; “Power of thoughts” describes the impact of thoughts on understanding symptoms and self. “Freedom in new behaviors” explores behavior changes in the adolescents and their families. “Mediators of change; why not give it a chance?” explores the helpful treatment-parts and the adolescents’ approach toward it. The findings support the positive effects of ICBT for pediatric FAPDs. Specific treatment elements motivated the adolescents, who experienced acquiring self-agency and improved symptom management. An encouraging secondary benefit was the experienced change of family-relationships, likely to further enhance the personal growth of the adolescent.
Keywords
Introduction
Functional Abdominal Pain Disorders (FAPDs) are a common subgroup of Functional Gastrointestinal Disorders (FGIDs) with a worldwide pediatric prevalence of around 10% (Korterink et al., 2015). The disorders are diagnosed and classified according to the Pediatric ROME-IV criteria, including prevalent subtypes, for example, Irritable Bowel Syndrome (IBS) and Functional Abdominal Pain – Not Otherwise Specified (FAP-NOS) (Hyams et al., 2016; Koppen et al., 2017) based on the presentation of characteristic clinical symptom pattern of long-lasting and disabling gastrointestinal symptoms, like abdominal pain and discomfort, which cannot be attributed to another medical condition (Hyams et al., 2016; Thapar et al., 2020). The etiology is unknown, but dysregulation of the brain-gut-axis, caused by interactions of biological and psychosocial factors, is suggested to play a significant role in the development and persistence of these disorders (Kozlowska et al., 2020; Thapar et al., 2020). The brain-gut-axis refers to the complex bidirectional communication system between the central nervous system (CNS), particularly the brain, and the gastrointestinal (GI) tract. Central mechanisms may involve visceral hypersensitivity with enhanced sensitivity to gut stimuli, leading to abdominal pain and discomfort, a hallmark of FAPDs, in combination with hypervigilance, that is, a heightened awareness of and thinking about gut symptoms amplifying the perception of discomfort and pain (Cole et al., 2020; Drossman, 2016).
Studies have shown how living with a FAPD can have a tremendous impact on daily functioning for adolescents, with reports of markedly reduced health-related quality of life (Varni et al., 2015; Youssef et al., 2006), high absence from school, more days spent in bed (Varni et al., 2015) and increased comorbid anxiety or depression (Newton et al., 2019). However, only a few qualitative studies have explored the more detailed perspectives of affected adolescents describing feelings of isolation (Brodwall and Brekke, 2021; Donovan et al., 2019), frustration in understanding their diagnosis (Woodham et al., 2022), and the use of different management strategies with limited effects (Brodwall and Brekke, 2021; Woodham et al., 2022).
The management of pediatric FAPDs may involve dietary advice and pharmacotherapy targeting specific symptoms (Thapar et al., 2020), as well as more effective treatments like psychological interventions, including cognitive behavioral therapy (CBT) (Gordon et al., 2022; Rutten et al., 2015). These interventions focus on empowering young people to manage their pain and other GI-symptoms by modifying maladaptive symptom perceptions and avoidance behavior through, for example, exposure (Thapar et al., 2020; Van Oudenhove et al., 2016). CBT has been shown to improve pain, reduce symptoms of anxiety and depression, and enhance the young person’s ability to participate in social life (Rutten et al., 2015; Thapar et al., 2020). Internet delivered exposure-based CBT (ICBT) has the potential to increase the availability of CBT (Vigerland et al., 2016). Such ICBT for FAPDs in children and adolescents has been developed and tested for efficacy in Swedish trials, demonstrating significant improvements in gastrointestinal symptoms, avoidance behaviors, quality of life, and school absenteeism (Bonnert et al., 2017; Lalouni et al., 2019), as well as reduced health-care costs (Lalouni et al., 2019; Sampaio et al., 2019).
However, engaging adolescents in psychological treatment, like ICBT, can be challenging (Bjønness et al., 2020; Gibson et al., 2016). Therefore, in order to understand how adolescents suffering from FAPDs may be engaged in and benefit from this type of promising treatment format, we conducted a qualitative study using semi-structured interviews to obtain more detailed information from the adolescents about their lived symptom experiences after having received ICBT. More specifically, we wanted to explore: (1) how the adolescents experienced the treatment overall, (2) if and how the treatment influenced their understanding of their disorder and their ability to cope with the symptoms in their daily life (i.e. their symptom understanding and symptom-related behavior), and (3) whether they experienced any changes in how their parents helped them manage their symptoms.
Method
The study was preregistered at Open Science Framework (OSF; https://doi.org/10.17605/OSF.IO/6BKJ8).
Design
A qualitative study design with semi-structured interviews was applied, enabling participants to share their experience in a deep and meaningful way, while being guided by questions and probes (Cole et al., 2020). The methodological approach chosen was Interpretative Phenomenological Analysis (IPA) (Smith et al., 2021), which is useful as it seeks to explore and understand subjective lived experiences, meaning and sense-making of certain psychological phenomena, like, in our case, the symptom experience of adolescents with FAPDs (Brocki and Wearden, 2006; Smith and Osborn, 2015). This is sought through reflectively managing any preconceptions of the interviewer while creating theories based on in-depth descriptions and analysis of the participants’ own expressed understanding of the phenomenon (Brocki and Wearden, 2006; Cole et al., 2020).
Settings
The study is embedded in the larger ongoing research project “The Danish FGID Treatment Study,” which investigates the feasibility and effect of the Swedish-developed ICBT for patients with FGIDs, including FAPDs in adolescents, in a Danish clinical context (Skovslund Nielsen et al., 2025). Participants were recruited from pediatric departments in Central Denmark Region, Denmark, and diagnosed according to the ROME-IV criteria with either IBS or FAP-NOS, (see further inclusion criteria online (Skovslund Nielsen et al., 2025)). Together with their parents, the included adolescents participated in the ICBT-program throughout a 10-week treatment period.
Content of treatment
During the 10-week treatment period, adolescents and their parents worked separately on the modules they gained access to. Adolescents accessed a new online module each week, while their parents accessed one every other week. Each module required about 4 hours of work throughout the week, including time spent on home exercises, and could be completed at the participants’ own pace at home. A therapist from the Department of Child and Adolescents Psychiatry, Aarhus University Hospital Psychiatry provided weekly written online therapist support by either commenting on and encouraging the participants to perform various exercises or answering any written questions the participants might have had during the last week. The treatment content consisted of education about FAPDs, fictive case stories (fictive adolescents with FAPDs describing their symptoms and their thoughts about symptom management, as well as about the exercises presented in the ICBT) and reflective tools like the short mindfulness exercise SOL (“Stop, Observe, Let go”) (Lalouni et al., 2017). SOL is intended to help the participants acknowledge and label their symptoms, without ruminating or being controlled by them. Participants are instructed to stop what they are doing, observe and label the symptom, and then let go of the thought about the symptom and continue to do what they were doing before using the tool. Further, the treatment consists of identification of unhelpful avoidance behavior followed by individually designed exposure exercises. The adolescents expose themselves to previously avoided stimuli, for example, foods, situations or activities. In parallel parental exercises focus on spending more quality time with their adolescent without paying attention to the symptoms (Bonnert et al., 2017, 2019; Skovslund Nielsen et al., 2025).
Recruitment
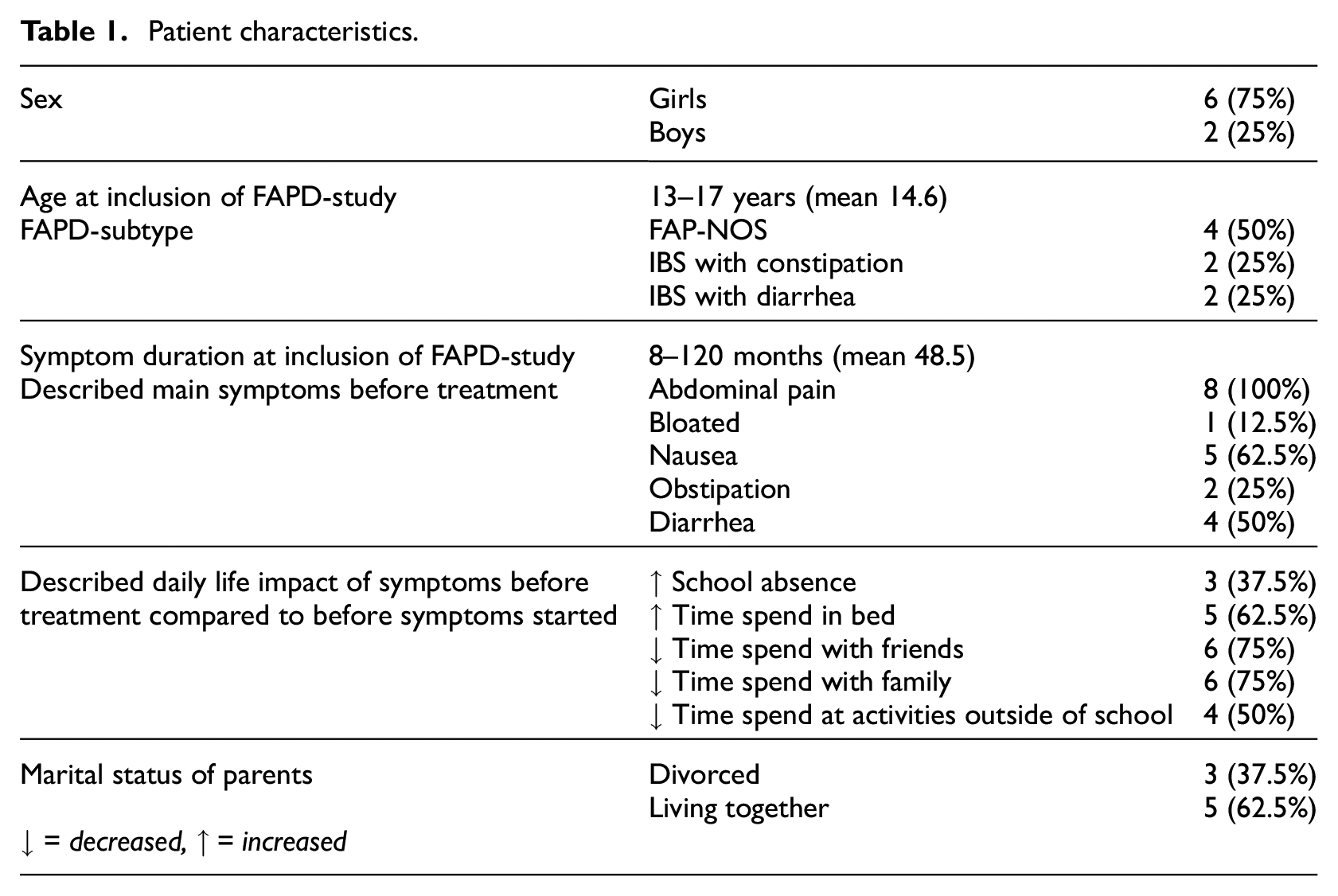
Parents of the adolescents, who had completed the ICBT program, were contacted by phone by the first author after the treatment-study’s 3-month follow-up. Those interested received further oral and written information about the study, and a date for the interview was planned. Written consent was obtained before commencement of the interviews from adolescents ≥ 15 years or from the parents of adolescents < 15 years. Guided by the concept of information power, the suggested sample size was proposed to five to ten adolescents (Malterud et al., 2016). Sampling aimed for variation in sex and age of the adolescents as well as variation in duration and severity of symptoms. The sample size was continuously evaluated and considered adequate when saturation of theory occurred. Eleven adolescents were invited, of which two declined to participate and one was a pilot interview. Therefore, the final sample consisted of eight adolescents (see characteristics in Table 1).
Patient characteristics.
Ethics
The study was conducted according to the guidelines of the Danish Health Research Ethics Committee and registered there as part of “The Danish FGID Treatment Study” (registration numbers 1-10-72-80-22 and 1-10-72-277-21) without the need for further individual registration (request with journal no. 1-10-7210%-124-22). It is further regustrered as part of “The Danish FGID Treatment Study” under the Central Denmark Region’s records of research projects (reference numbers: 701921 and 769029). Participants were each assigned a pseudonym to ensure anonymity. Female aliases were used for female participants, and male aliases were used for male participants.
Data collection
In depth semi-structured, face-to-face interviews were conducted by the first author using an interview guide with open-ended questions developed by the research team. The interview guide was discussed and adjusted after the first pilot interview by DH, CR and HS. Interview-questions focused upon the following domains (1) the overall experience of the treatment and (2) the lived symptom experience of the participants before and after the treatment (e.g. how did you understand and manage your symptoms before and what has changed in your life after the treatment). A translated version of the full interview guide is available in the preregistration at OSF (https://doi.org/10.17605/OSF.IO/6BKJ8). Interviews were conducted approximately 3 months after ending the ICBT treatment, between April and October 2023. The adolescents chose the interview setting: their private home (n = 5) or the Department of Child and Adolescent Psychiatry (n = 3). Interview duration was 59–92 minutes (mean: 73 minutes). Photo-elicitation was used during the semi-structured interviews to facilitate these as it is a helpful tool for enabling communication and for illustrating the potential change experienced by the adolescents (Glegg, 2019). Participants were instructed to take two photos that could support them in sharing their experiences (1) of a situation in which they still felt bothered by their symptoms, and (2) a situation in which they no longer felt bothered by their symptoms. However, taking photos was optional as these were only used as a potential facilitating tool. Therefore, they were not included in the later data analysis. Four participants chose to take photos prior to the interview.
Data analysis
Interviews were recorded and subsequently transcribed verbatim by the first author with the use of a transcription guide. Transcripts were analyzed in their original language (Danish), but quotations have been translated for publication. Stepwise analysis was performed according to the principles of IPA and assisted by NVivo 12 (QSR International, 2018). Researcher audit was used throughout the entire research process (Smith et al., 2021). Both CR and DH audited the interview technique and analysis, and DH co-coded to check consistency. In step one, interviews were read thoroughly while noting initial thoughts for each. In step two, interviews were coded individually and then across interviews in several rounds. In step three, the emerging main themes and subthemes were determined in several discussion rounds by the entire research team.
Findings
The adolescents expressed an overall positive experience, with an emphasis on specific elements in the ICBT-program, for example, exposure exercises, SOL and the fictive case stories. The majority described how the treatment had led to a decrease in symptoms and/or in symptom-related impairment. As illustrated in Figure 1, analysis identified three main themes with two subthemes each, all of which seem to be interrelated, reflecting the experience of receiving treatment and living with a FAPD after ICBT.
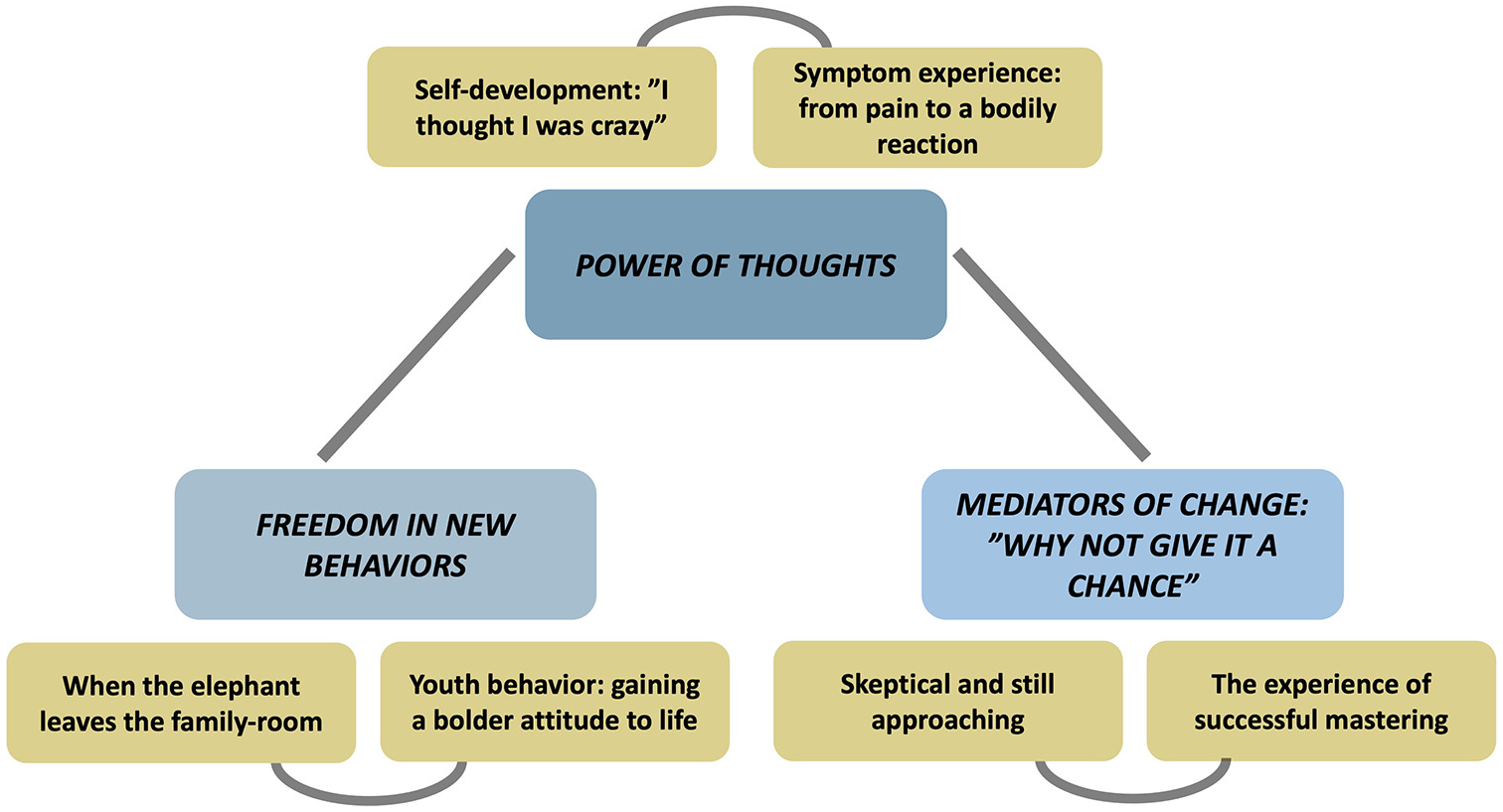
Analysis revealed three main themes (blue boxes) and six subthemes (yellow boxes).
Power of thoughts
This theme describes the adolescents’ reflections on how the treatment helped them realize the importance of the influence of their personal thoughts and changes in thought processes in regard to symptom- and self-understanding.
Symptom experience; from pain to a bodily reaction
Several adolescents recalled having a primarily biomedical symptom-understanding before receiving ICBT, expressing “do I have cancer” or “I thought I had an allergy or something.”
Rose had dealt with abdominal pain and nausea for almost a year. She remembered thinking: “it could not possibly be something in my head!”, when included in the program, thereby implying that she didn’t believe the pain could be affected by psychological factors as well. After finishing the program, her way of understanding her symptoms had changed:
“The only time I noticed the nausea … that’s when I had to go to an exam, then I became nervous.”
Rose had experienced a significant reduction in symptoms as they were no longer present on a daily basis. She now attributed symptoms to being nervous in relation to an exam. Rose continued describing her changed symptom-understanding:
“my body just said stop, and now I had to start working on myself.”
Rose now attributes symptoms to the body “saying stop,” thus correlating symptoms to her general wellbeing. Similar correlations were made by other participants, describing “I was very sad, and it became a physical feeling in my stomach” (Sam). Further, this understanding enabled a different symptom approach. Roses’ words “working on myself” indicate a form of attained self-agency, which was also described by other participants.
Participation in the ICBT-program specifically supported the understanding of a brain-gut-connection, which the adolescents had not necessarily considered a role-player for their symptoms before. Consequently, they had developed a more nuanced understanding of how their bodies and minds respond in various situations, recognizing the significance of this interaction in influencing their wellbeing.
Self-development: “I thought I was crazy”
Before the treatment, some adolescents recalled a sense of loss of self, explaining how “I had no idea of where I was. … Yes, who I was?” (Olivia) and even thinking “I am crazy” (Mia). Jack had suffered from abdominal symptoms for years and used to spend most of his days in bed due to his symptoms. Following the treatment, the symptoms still affected him, but to a lesser degree.
“I think I ’ve gained another mentality towards it. I think in another way now… Yeah, that they (the symptoms) should disappear again… It ’s easier to ignore them, cause now I have those techniques to help me to ignore them.”
The treatment supported a change in thoughts, which allowed Jack to take charge of the way he dealt with the symptoms. Using the words “another mentality” and “think in another way” indicates a deeper understanding of the process he had gone through, expressing a change in the way he thought about himself and his symptoms.
In line with Jack’s experience, Sam, who had been struggling with abdominal symptoms for a long time, leading to a high absenteeism from school, recalled:
“I guess I have learned more about myself. … You know, I have learned that I could actually do it myself.”
Sam’s description of how he understood more about himself and his own abilities illustrates a changed self-perception. He gained greater confidence and self-perspective regarding his own role in life, as he was empowered to and realized that he could be the one taking control over how to deal with his symptoms as expressed with “I could actually do it myself.”
Amelia was still dealing with her abdominal symptoms after the treatment, yet she described a new awareness, that the more she thought about the symptoms, the worse they got.
“So I think that if you never thought about having pain in your stomach, then you also wouldn ’t have it.”
She learned that, when giving her thoughts about the symptoms less attention, they would eventually disappear. This illustrates a nuanced and complex illness understanding with emphasis on the importance of thoughts for symptom experiences, which other adolescents likewise acquired; “Now I don’t think so much about it (the pain), I just think that it’s not really something special … and there’s probably other things to think about instead.” (Ava).
Self-development occurred as the adolescents became more aware of the power of their own thoughts and as they realized they could better control their symptoms.
Freedom in new behaviors
The second main theme concerns some of the changes that the adolescents experienced in both their own and in their parents’ behavior after receiving the treatment.
Youth behavior: Gaining a bolder attitude to life
Many adolescents described how they learned to manage their symptoms better, which led to a change in their approach to life in general. They shared stories of being able to go to concerts, school, shopping, scout camp, parties and much more, which before was seen as a tremendous challenge for them.
Mia experienced abdominal pain that impeded her ability to carry out everyday activities. She contemplates on the changes she underwent:
“I do what I want to do and my stomach doesn ’t hurt, when I go for long walks now or when I play handball. So my daily life has become much better. I ’m a bit more free.”
As the symptoms were no longer a dictating factor and hindrance in Mia’s life, she felt like she was more free to do what she wanted, indicating increased self-agency and braveness as expressed in “I do what I want to do.” Ava still suffered from abdominal pain after the treatment, but described how she had changed the way she thought about her symptoms. She expressed, like Mia, a braveness with the words “Just do the things you wanted to do anyway”, indicating a will to not let the symptoms affect her choices.
By being empowered to deal with their own symptoms, the adolescents gained greater freedom to live a more normal teenage life.
When the elephant leaves the family-room
Before treatment, the symptoms typically took up a lot of time in many of the adolescents’ families. As Rose described “it became this topic at home… we often talked about it,” indicating how the symptoms occupied the family room, overshadowing normal family life. As part of the program, parents engaged in exercises, where they practiced paying less attention to their child’s symptoms by asking fewer questions about them. Jane describes a change in her father’s behavior, which aligned the proposed goal of these parent exercises:
“He doesn ’t talk so much about it. When I tell him, I ’m in pain, then he doesn ’t ask about where I ’m in pain and how much I ’m in pain. Instead he just says‘shouldn ’t we try to get you to school.’”
Compared to before, when the symptoms got a lot of attention from Jane’s father, she now describes how he tries to focus on something else, like school. Other adolescents described a similar change, further expressing how they themselves stopped sharing about their symptoms to their parents, as they gained more symptom control. This altogether led to less focus on the symptoms within the family.
Further, many adolescents also described how they perceived a change in their relationship with their parents. Sam said “I might have become a bit closer to my mum” as a result of them spending more time together and sharing more things. In line with this, Olivia, who had dealt with abdominal pain and nausea for almost 3 years, used to isolate herself in her room daily, but now expressed “I’ve started to talk much much more with them (parents) now than before”. Likewise, Rose described how her and her mum now talked about all sorts of things together, making the comparison of getting an extra friend through her mum; “It’s actually really nice to just have an extra kind of girlfriend.”
The symptoms used to hinder the families in just being together, but as a result of the changed behavior of both the adolescents and their parents, many adolescents now had closer relationships and a more normal family life.
Mediators of change; “why not give it a chance?”
The third main theme reflects the adolescents’ perceived mediators of change, including tools of the program, their experience of success with these and their attitude toward the program.
The experience of successful mastering
The adolescents expressed how the use of tools and exercises were helpful for mastering their symptoms. Many explained that they continued using SOL after they stopped the treatment, including Mia, who expressed “I still use it (SOL), if there is something… because it helps”, and Olivia, who described how it was helpful both in gaining control over the symptoms, but also within other situations of life.
“Yeah SOL exactly. Yes, I thought that was difficult. Actually, I think that was the most difficult thing about it (the program), but it also ended up being that which helped me the most.”
As Olivia describes, using SOL was difficult, possibly because it challenged the adolescents to change the way they reacted to their symptoms. Despite this, Olivia realized that it helped her succeed in dealing with her abdominal symptoms. Similar was expressed by Jane, who pointed out “I used that (SOL) a lot,” and Amelia described how when using SOL the symptoms could disappear fast “Cause then you observe and so, and then you think about “where does it actually hurt”, and then you can feel that it hurts somewhere, and then you just leave it (let go of the thought about the pain)”.
The fictive case stories from the program were also highlighted as encouraging and motivating. Rose explained how it was for her to read them:
“I thought it was really nice to get the examples from other young people as well … Because I was thinking “okay, I ’ve never heard about this and everyone who I talked with had also never heard about it.” So I thought “Okay, I ’m just all alone in the world- kind of.” But then it turned out I wasn ’t.”
Rose recalls how she felt like she was the only one dealing with a FAPD-diagnosis. But as she went on with the program, she was relieved when she realized that she wasn’t alone with these symptoms. As expressed by other adolescents, the cases resembled their own situation and depicted adolescents, who had succeeded in the exercises, which further motivated them to continue the treatment.
Skeptical and still approaching
Before referral to the ICBT-program the majority of the adolescents had gone through a long diagnostic process, trying out several other strategies and medications, which created skepticism toward new treatments. Olivia described this; “I obviously hoped that it would help, but I didn’t expect anything of it, because I had tried a hundred other things before … which didn’t help at all.” Likewise, Rose expressed this skepticism toward the program, but also described why she approached it.
“I thought “yeah yeah, let us just try it.” I mean, I was willing to do anything.”
“Willing to do anything” may describe a certain desperation and hopelessness to get rid of the symptoms. Possibly, this led Rose to give the treatment a chance, and choose a “just-do it”-attitude toward the program. Several adolescents expressed this attitude with words like “ …do it anyways” (Jack) and “Then I was like “you know what, we’ll try it”, because I didn’t want this anymore. I just wanted to get over this” (Mia). Further, this attitude seemed to be enhanced as they experienced success with the program. Rose was asked to give advice to others like her, and encouraged them to do the program:
“And it actually works, so just keep on doing it. Even if it gets annoying as you ’re in it.”
For Rose, the success of the exercises, expressed with “it actually works”, was a key motivating factor for continuing the program, even when it was “annoying”.
Rather than giving up when exercises became difficult and despite their initial skepticism, the adolescents persisted with the attitude of “doing it anyways”, because they found it to be worth the reward of learning how to manage their own symptoms.
Discussion
This study aimed to explore how adolescents with FAPDs engaged with and potentially benefited from ICBT. Specifically, it investigated whether the treatment influenced their understanding of symptoms and symptom-related behavior, and whether they experienced any changes in how their parents assisted them in managing their symptoms. Our analyses identified three main themes: Power of thoughts, Freedom in new behaviors and Mediators of change; “why not give it a chance?”. The findings provide insight into and elaborate on the specific effects of the treatment program as well as the wider aspects of its effects. This includes how the adolescents experienced the changes they went through in understanding their symptoms and themselves, as well as the perceived positive changes within their families. The adolescents described how they learned, not only to manage their symptoms, but also how to be in unprecedented charge of their own lives, as they acquired self-agency and were empowered. Despite some initial skepticism, they expressed how they approached the program with a “just do it”-attitude, possibly further enhanced by their experience of success with the program as they went along.
The adolescents described how they became aware of the importance of recognizing and acknowledging the role of their own thoughts in regard to both symptom- and self-understanding. The initial biomedical symptom-understanding is common among patients with functional disorders, as explored in other qualitative studies, where adolescents expressed uncertainty about their diagnosis and fear of a serious disease (Brodwall and Brekke, 2021; Woodham et al., 2022). During this ICBT-program the adolescents described a change in their symptom-understanding, which now resembled the nuanced understanding of a dysregulation of the complex interactions within the brain-gut-axis, including the impact of mental health on the experience of pain (Thapar et al., 2020). As the adolescents received the treatment, they also expressed a change in their self-understanding, and acquired self-agency leading to greater symptom-management. These experiences are similar to that of the adolescents in Woodham et al. (2022), who after having been taught about their FGID-diagnosis, including FAPD-diagnosis, developed an awareness of the brain-gut-axis, leading to greater symptom-management, personal growth and increased grasp of the role of self (Woodham et al., 2022). Moreover, the adolescents in our study expressed a new awareness of the role of thoughts in regard to symptom-severity, which they learned to control by focusing less on their symptoms. These findings are supported by literature regarding catastrophizing thoughts, which are known to increase the experienced pain and maintain symptoms (Rogers and Farris, 2022; Van Oudenhove et al., 2016), and therefore have been suggested to be an important target when treating patients with FAPD (Van Oudenhove et al., 2016).
In a qualitative study of adolescents with FAPDs, who received an online psychological intervention, changes in pain-perceptions and coping strategies after psychological treatment led to positive changes in behavior (e.g. spending more time with friends) (Nieto et al., 2020). This supports that the experienced freedom of the adolescents in our study was possibly due to their changed symptom- and self-understanding. The adolescents also described that the changes in their parents’ behavior led to a change in family relationships and a more normal family life. Quantitative studies in relation to ICBT have previously found that managing parental catastrophizing leads to a decrease in the child’s symptoms (Lalouni et al., 2022; Levy et al., 2014), but not whether this would also lead to inter-relational changes within the family as found in our study. This seems to be a secondary benefit of the treatment, and the improved parent-adolescent relationship can potentially contribute to strengthening the personal growth and resilience of the adolescent (Morris et al., 2021). In McGurgan et al. (2022), parents of children with FAPDs received psychological interventions for their child’s FAPD, and expressed that learning to contain their child’s pain and acknowledging the role of their own impact led to an improved relationship with their child (McGurgan et al., 2022). Further research concerning the parental experience of receiving this specific ICBT for a child’s FAPD would be beneficial to learn more about its inter-relational effects within the family.
The adolescents expressed appreciation for the exposure exercises and SOL within the ICBT- program. When succeeding with these, they grew in symptom-management, which is in line with prior quantitative studies showing how reduced avoidance and fear of symptoms, learned through the exposure exercises, led to reduction in abdominal symptoms. (Bonnert et al., 2018; Lalouni et al., 2021). Furthermore, the fictive cases were highlighted as encouraging, which is compatible with findings of a systematic review of peer-to-peer support for adolescents with chronic illness that showed that such support improved pain self-management and emotional symptoms of the adolescents (Ahola Kohut et al., 2014). A qualitative study of adolescents with IBS also described that the adolescents felt connected in a special way with other adolescents struggling with similar symptoms (Donovan et al., 2019). Even though the cases in the ICBT-program were indeed fictive compared to specific peer-to-peer support, it seems that they still provided the adolescents with the assurance of not being alone with their diagnosis, which further motivated them to continue the treatment.
The initial skepticism some of the adolescents showed toward the program seemed to facilitate a “just do it”-attitude, which was enhanced during their work with the program. Prior literature regarding adolescents’ investment in psychological treatment showed that adolescents tend to invest more in treatment forms that allow them a sense of autonomy and control over the treatment (Gibson et al., 2016). Spencer (2014) defined empowerment as to give someone the power to control decisions regarding their own health and life, and further suggests that for treatments to be effective for adolescents, they need to resonate with the adolescent’s lived experiences (Spencer, 2014). Bjønness et al. (2020), likewise states that one of the challenges of engaging adolescents to participate in their treatment is their need for autonomy, and therefore suggest a broad understanding of shared decision-making as a treatment approach with increased user involvement that empowers the adolescents in their decisions (Bjønness et al., 2020). Our study indicates that participants grew in self-agency as a result of the various exercises they were encouraged to do. Giving the adolescents a sense of autonomy over their own treatment (e.g. coming up with exposure-exercises themselves) and increasing their self-understanding, might have empowered them to take control over their symptoms, and further engage in the treatment program. Therefore, the initial skepticism of the adolescents seemed to be countered by the empowerment they received in the treatment. Further, an initial skepticism and potential unwillingness toward psychotherapy among adolescents might be explained by their desire for independence from adult authorities, as therapy implies trusting and acknowledging an adult clinician (Lavik et al., 2018). Here it might be beneficial that the ICBT-program is online with only written therapist contact, thereby increasing the independence of the adolescents as well as giving them freedom in how and when to use the program. This leads to a form of individualization of the treatment, which seems preferable when targeting treatment like this toward adolescents (Gibson et al., 2016).
Strength and limitations
The consolidated criteria for reporting qualitative research (COREQ) statement (Tong et al., 2007) were widely met, for example, with regard to a thorough description of the research team, the chosen methodology, the settings and the data-collection. Further, the sampling of participants was transparently described in both text and Table 1. Likewise, regarding data-analysis, a presentation was made of the applied software, number of data coders and of the derivation of themes following the steps of IPA.
Qualitative research rigor was kept in mind throughout the entire research process as described in the methods section, which is a strength of the study. The first author is a medical student, who previously worked as a research assistant on “The Danish FGID Treatment Study,” one of the co-authors is a MD and PhD-student working on “The Danish FGID Treatment Study,” and five of the co-authors are experienced researchers within the field of child and adolescent psychiatry (three MDs and two psychologists), of which four have experience in the development and evaluation of the ICBT-program and one has experience in IPA. This wide composition of the team enhanced the analytic breadth and expert knowledge of the study. The sample of participants widely met the aimed variation in sex, age and symptom-severity and -duration, leading to a heterogeneous group of adolescents. Data saturation was achieved with the final sample size of eight adolescents.
Some limitations should also be considered. As stated, several researchers in the team had been and were still actively involved in the ICBT-program, which may have led to a bias toward finding positive themes regarding the program. However, this was continuously sought to be countered by being conscious of the potential biases through reflective discussion. Finally, two eligible adolescents declined to participate in this study, and it is unknown whether they would have added a different perspective on the lived symptoms experiences of FAPDs after ICBT.
Perspectives and future research
The findings suggest that ICBT in general is a beneficial method for treating adolescents with FAPDs. The experiences of the adolescents can potentially be used to further optimize the treatment by for example, adding illustrative quotes to the existing case stories, to further encourage and motivate new young patients receiving the treatment. Similar research on the parental experience of ICBT could further improve the understanding of its effects for adolescents with FAPDs, and of how to also refine the parental parts of the intervention. In line with this, it could be of interest to investigate how the additional positive effects of improved family-life and -relationships can potentially further support the personal growth, empowerment and acquired self-agency of the adolescent. We would also suggest that for future research, similar studies could seek to include “drop-outs,” that is, participants who have not finalized the treatment program, and therefore might have a less positive experience with ICBT, to understand their perspectives as well. Additionally, exploring if adolescents suffering from other functional disorders could benefit from a similar ICBT should be considered for future research.
Conclusion
To our knowledge, this is the first study exploring the lived symptom experiences of adolescents after they had received ICBT with exposure-based methods for their FAPDs. Overall, the findings support the positive effects of ICBT with exposure-based methods in adolescents with FAPDs, underlining this to be a successful treatment choice for young patients with these disorders. Specific treatment elements such as the short mindfulness exercise SOL and the fictive case stories especially seemed to motivate and engage the adolescents in the treatment with an overall experience of acquired self-agency and improved symptom management through being empowered and provided a sense of autonomy. Finally, an encouraging secondary benefit of the treatment was the experienced change and improvement of relationships in the family, which is likely to further enhance the personal growth of the adolescent.
Supplemental Material
sj-pdf-1-hpq-10.1177_13591053251320600 – Supplemental material for “I’m a bit more free”: Lived symptom experiences in adolescents with functional abdominal pain disorders after internet-delivered psychological treatment
Supplemental material, sj-pdf-1-hpq-10.1177_13591053251320600 for “I’m a bit more free”: Lived symptom experiences in adolescents with functional abdominal pain disorders after internet-delivered psychological treatment by Helene Søgaard-Singh, Ditte Roth Hulgaard, Eva Skovslund Nielsen, Karen Hansen Kallesøe, Marianne Bonnert, Maria Lalouni and Charlotte Ulrikka Rask in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053251320600 – Supplemental material for “I’m a bit more free”: Lived symptom experiences in adolescents with functional abdominal pain disorders after internet-delivered psychological treatment
Supplemental material, sj-pdf-2-hpq-10.1177_13591053251320600 for “I’m a bit more free”: Lived symptom experiences in adolescents with functional abdominal pain disorders after internet-delivered psychological treatment by Helene Søgaard-Singh, Ditte Roth Hulgaard, Eva Skovslund Nielsen, Karen Hansen Kallesøe, Marianne Bonnert, Maria Lalouni and Charlotte Ulrikka Rask in Journal of Health Psychology
Footnotes
Acknowledgements
We want to show our gratitude to all the adolescents in this study, who willingly participated and honestly shared their stories.
Authors contribution
▪ HS contributed to the design of the study, wrote the interview guide, carried out the interviews and data analysis, and wrote this article.
▪ DH contributed to the design of the study and interview guide, to the interview-technique, data analysis and to the article by giving substantial feedback on several drafts.
▪ EN contributed to the design of the interview guide, the discussion and decision about themes and to the article by giving substantial feedback on several drafts.
▪ KK contributed to the design of the interview guide, the discussion and decision about themes and to the article by giving substantial feedback on several drafts.
▪ MB contributed to the design of the interview guide, the discussion and decision about themes and to the article by giving substantial feedback on several drafts.
▪ ML contributed to the design of the interview guide, the discussion and decision about themes and to the article by giving substantial feedback on several drafts.
▪ CR contributed to the design of the study and interview guide, to the interview-technique, data analysis and to the article by giving substantial feedback on several drafts.
Data sharing statement
This qualitative study is based on transcripts of interviews and photo-elicitation. In order to protect the anonymity of the participants, the raw data and material are not freely available.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was funded by Lundbeckfonden (nr. R377-2021-340). No other funding was received for conducting this study.
Ethics approval
The study was performed in line with the principles of the Declaration of Helsinki. The study was conducted according to the guidelines of the Danish Health Research Ethics Committee and registered there as part of “The Danish FGID Treatment Study” (registration numbers 1-10-72-80-22 and 1-10-72-277-21) without the need for further individual registration (request with journal no. 1-10-72-124-22). It is further registered as part of “The Danish FGID Treatment Study” under the Central Denmark Region’s records of research projects (reference numbers: 701921 and 769029).
Informed consent
Written informed consent was obtained from all individual participants ≥ 15 years, and informed consent was obtained from their parents. Informed consent was obtained from all individual participants < 15 years, and written informed consent was obtained from their parents.
Consent for publication
Not applicable.
Preregistration
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.