
Abstract
Second-generation antipsychotics are highly effective in controlling symptoms if taken as prescribed. However, poor medication adherence results in patients continuing to experience psychotic episodes and metabolic disturbances that can cause them to develop abnormal lipid levels, weight gain, and diabetes. Understanding the underlying modulators that impact follow-up appointments and metabolic monitoring is critical. Semi-structured interviews were conducted with patients and their treating psychiatrists across four sites in South India. Narrative data were thematically analyzed, informed by an inductive approach. Patient-reported barriers included medication side effects, lack of awareness about metabolic monitoring, and financial constraints. Psychiatrists reported both patient and resource barriers that impact their provision of care. This study has shed light on key barriers impacting the provision of care and subsequently health outcomes for patients living with severe mental illness to inform strategies that target barriers for both patients and psychiatrists.
Introduction
Severe mental illness (SMI) is associated with a threefold increased risk of premature mortality when compared to the general population and is estimated to shorten the life expectancy of those impacted by approximately 10–20 years (Padmavati, 2016). Antipsychotics are a core component of effective management for individuals who experience psychosis, both for relieving acute symptoms and for preventing relapse (Cooper et al., 2019). Psychosis is indeed a relatively rare and distinctive feature within the spectrum of SMIs and often necessitates a stronger reliance on antipsychotic medications compared to other SMIs. Second-generation antipsychotics (SGAs) are highly effective and appear to have better safety profile when compared to their earlier counterparts (American Diabetes Association, 2004).
While SGAs are a critical component of effective management, research indicates that a high percentage of people prescribed SGAs do not adhere to therapy, which includes deviations from the prescribed dose or frequency or both, or stopping treatment altogether (Lacro et al., 2002). Studies show that the adherence rates for SGAs after a year of treatment range from 50% (Dolder et al., 2002; Sajatovic et al., 2006) to 60% (Ascher-Svanum et al., 2008; Gilmer et al., 2004).
Further, SGAs have a high level of associated risks, particularly with the development of metabolic syndrome (Thompson et al., 2011). Specifically, the use of SGAs has been linked to an atherogenic lipid profile, dramatic weight gain, and obesity and diabetes (Thompson et al., 2011). Fluctuating blood glucose levels, hypercholesterolemia, and obesity are well-established risk factors for the development of cardiovascular disease, stroke, and death (Rofail et al., 2009). For people prescribed SGAs, monitoring of metabolic changes is fundamental for preventing these long-term negative outcomes. According to the American Diabetic Association/American Psychiatric Association (ADA/APA) guidelines, body weight (BW) should be monitored monthly for the first 3 months after commencing or changing SGAs and quarterly thereafter (ADA, 2004). Fasting blood sugar, lipid levels, and blood pressure (BP) should be monitored at 3 months after starting SGAs. Subsequently, BP and glucose levels should be checked annually, and for patients with abnormal lipid levels, repeat testing should be conducted once every 5 years thereafter (ADA, 2004). The guidelines also emphasize the need for clinicians to incorporate frequent discussions about potential medication-related side effects with their patients, lifestyle advice that supports the maintenance of physical health, in addition to emphasizing the ongoing need for metabolic monitoring (Padmavati, 2016; Rofail et al., 2009). Metabolic monitoring is also critical throughout the treatment continuum, for example, while switching of antipsychotics, especially when patients have existing metabolic disturbances (Cohn and Sernyak, 2006). Lifestyle advice should incorporate information about healthy eating, and exercise, as well as relaxation techniques such as yoga (Padmavati, 2016). These recommendations are supported by a growing body of evidence that highlight the ascribed benefits of non-pharmacological interventions for people with SMI (Rofail et al., 2009). However, anecdotal and research evidence suggests that the guidelines have been poorly implemented in clinical practice, particularly with regards to recommendations for metabolic monitoring (Cunningham et al., 2018; Hasnain et al., 2009).
While the lack of adherence to SGAs and to metabolic monitoring alongside the negative clinical outcomes of one or both has been reported, there is scarcity of research that focuses on understanding factors underpinning these observations. To date, there is only a limited number of studies that have focused attention on understanding psychiatrists’ knowledge and attitudes towards metabolic issues related to SGAs. Understanding the lived experiences of both patients (in some cases, their carers), and their psychiatrists will provide valuable insights into the modulators that impact on medication adherence and metabolic monitoring uptake, critical for informing strategies that target barriers, and ultimately, improve outcomes for people who are prescribed SGAs.
Aim and objectives
The aim of this study is to explore the perspectives of people living with SMI who have been prescribed SGAs and their psychiatrists, to identify factors that contribute to suboptimal adherence to SGAs and to metabolic monitoring. Young and experienced psychiatrists were included to capture their insights on the challenges of metabolic monitoring, drawing on their varying levels of professional experience – an aspect that has not been extensively explored in this population. Patients on antipsychotics for 1 year, as well as those on long-term treatment, were included to provide a comprehensive understanding of adverse effects, barriers to adherence, and monitoring needs, taking into account the influence of treatment duration.
Methods
Participants
This phenomenological study was conducted across four sites in South India that included tertiary care psychiatry facilities, rural health centres and community clinics. Ethical approval was granted by the Institutional Ethics Committee for interviewing the participants. All methods were performed in accordance with the Declaration of Helsinki and Good Clinical Practice (International Council for Harmonisation, 2021; World Medical Association, 2024). Patient participants were those aged 18 years or above; diagnosed with one or more severe psychiatric conditions including schizophrenia, schizoaffective, bipolar disorders; and who had been prescribed SGAs for a minimum duration of 6 months. Patient participants were excluded if they were bedridden, had pre-existing metabolic comorbidities such as diabetes, hypertension, and dyslipidemia before diagnosis of psychiatric conditions, or had ongoing medico-legal issues or both. Psychiatrist participants were those directly involved in the provision of clinical care of patient-prescribed SGAs. These participants were purposively sampled to provide maximum variation (e.g. leadership roles and years of clinical practice). All participants were provided with information about the research and informed that their participation in the study was completely voluntary. Participants’ written informed consent also included consent for the interview to be audio recorded. During the interview process, some participants were accompanied by family or friends who were acting in the capacity as their support or carer).
Data collection and handling
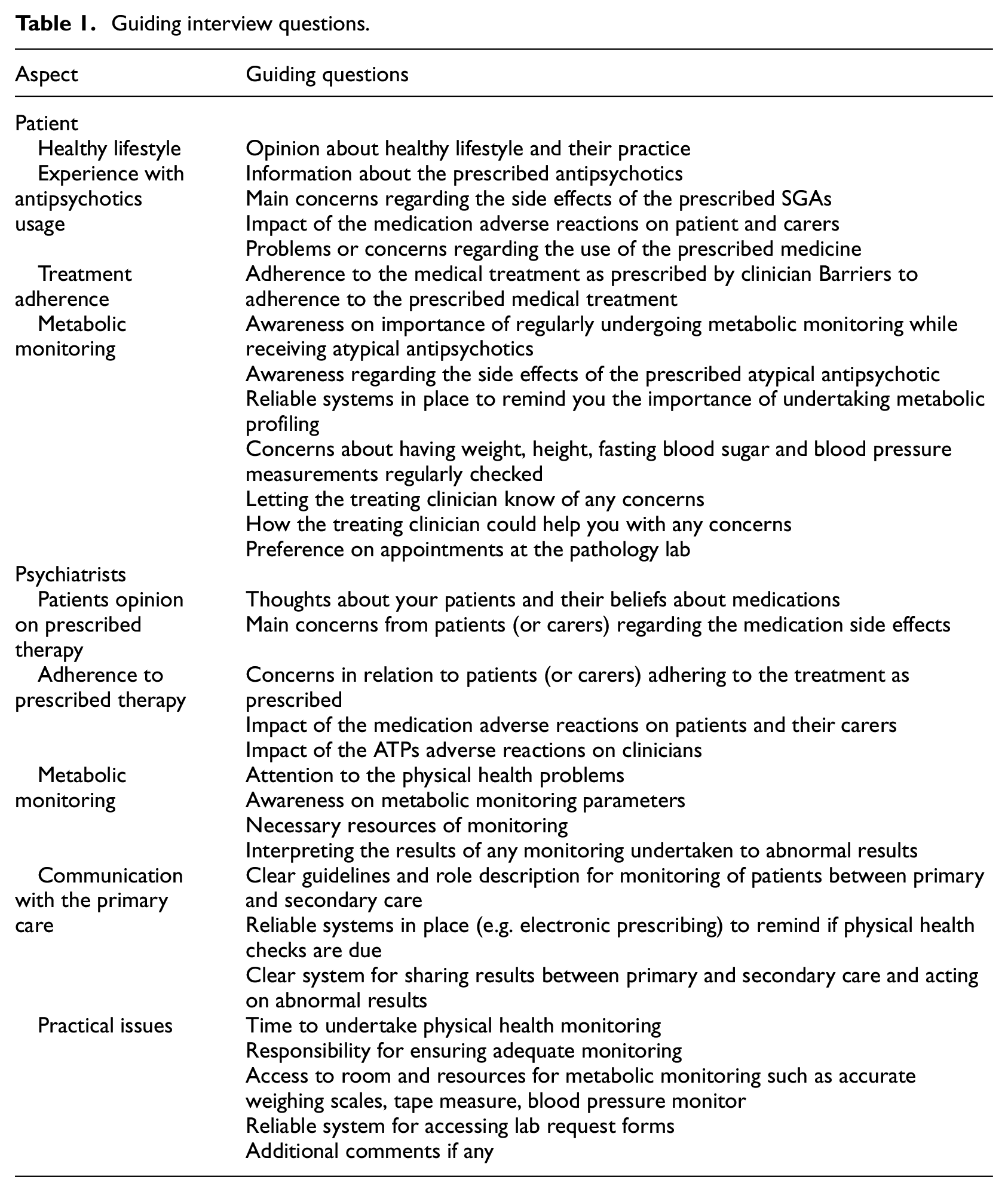
Interviews were conducted on a one-on-one basis in a private room at a healthcare facility. The interviews were conducted by the principal investigator (PI) who has completed her post-graduation in clinical pharmacy. She undertook specialized training to develop the skills necessary for conducting interviews with target participants during her doctoral program. Two interview guides (one for patient participants and one for psychiatrist participants), consisting of broad and open-ended questions were used to encourage conversation between interviewer and interviewee. Development of the interview guides was based on information gained through (i) a review of the literature, (Ronsley et al., 2011) and (ii) consultation with research and clinical experts including practicing psychiatrists, senior mental health researchers, and hospital policymakers. Examples of guiding questions for each participant group are presented in Table 1. Each interview took between 20 and 30 minutes to complete.
Guiding interview questions.
Interviews were conducted until data saturation, and no more participants were recruited. No repeat interviews were carried out. Interview recordings were anonymized and transcribed and translated verbatim into English language by a qualified interpreter. The transcriber adopted a three-pass per tape policy and a random selection of transcripts was proofread by the research team from India and Australia to review the accuracy of the transcripts. Recordings and transcripts were stored in a secure location accessible only to the members of the research team.
Data analysis
Interview transcripts were read and re-read by two of the authors, while listening to the recordings. This process was undertaken to ensure the accuracy of transcription and to gain a basic understanding of emerging themes related to the key research questions.
The themes were then reviewed and discussed by the research team to establish relevance. To ensure reliability, the two researchers agreed on a coding framework to summarise key emerging ideas. Codes were progressively refined and sorted into emerging themes and sub-themes (Naeem, 2023). Reflections and field notes from the investigator who facilitated the interviews were also reviewed in conjunction with the analytical process. This step was undertaken to facilitate understanding of the messages being conveyed by the research participants. This inductive approach allowed for understanding to be derived from the data and therefore reflected the perspectives of the participants. NVivo (NVIVO, 2019) software (QSR International Pty Ltd., trial version 12 for Windows) was used to manage the data and to facilitate analysis.
COREQ (Consolidated Criteria for Reporting Qualitative Studies) was used to report the methods and findings of the study provided in Supplemental File 1 (Tong et al., 2007).
Results
Background of participants
A total of 29 participants (n = 20 patients, n = 9 psychiatrists) provided written informed consent and shared their experiences and perspectives through one-on-one interviews. A summary of their characteristics is provided in Table 2.
Participant characteristics.
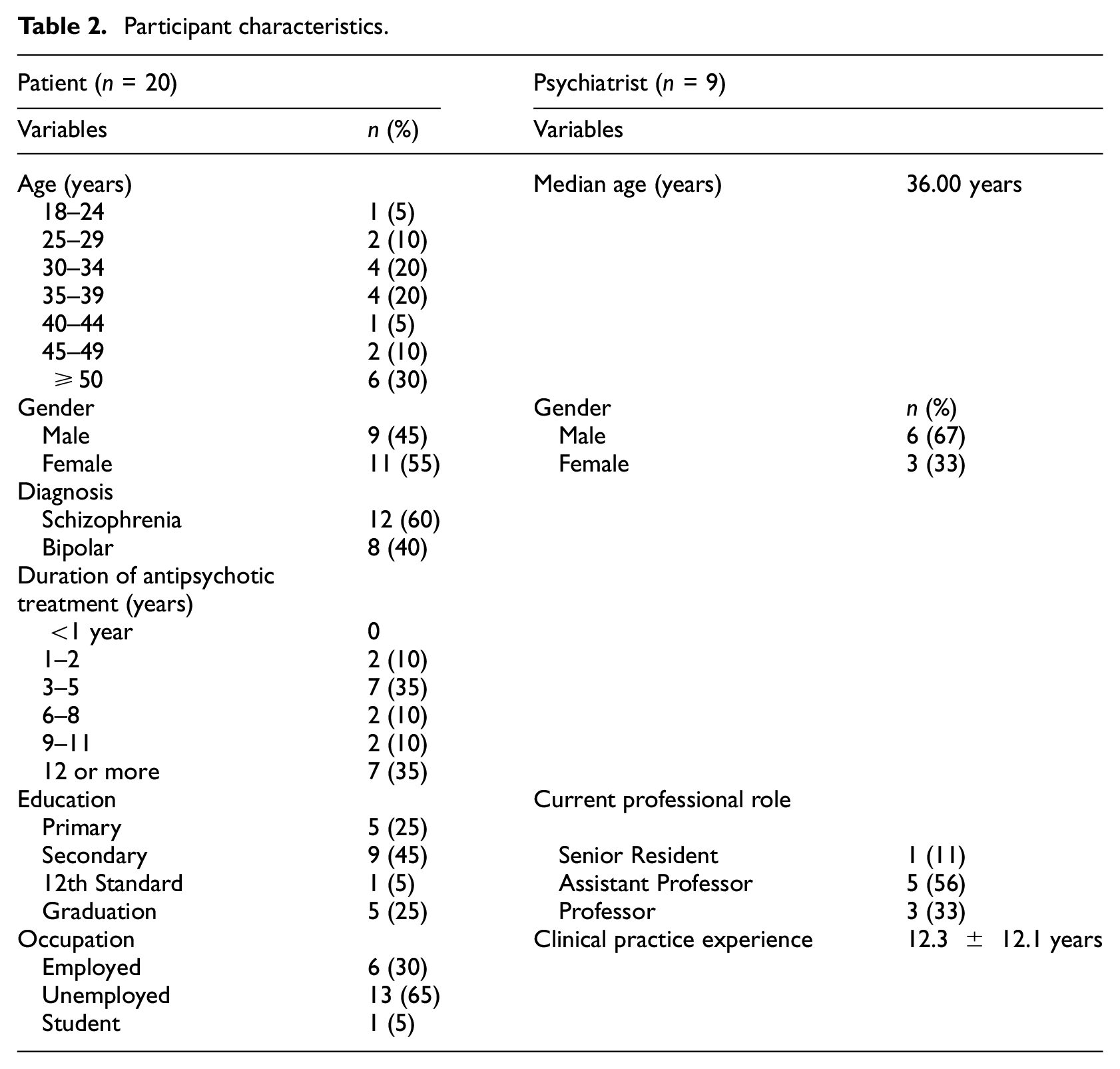
Patient participants comprised 11 females and nine males, the youngest was 24 years, and the oldest was 65 years (median age: 37.50 years). About 60% of the patients were schizophrenic. Approximately 65% were unemployed. Psychiatrist participants comprised three females and six males, they ranged in age from 30 to 69 years. The median age of psychiatrists was 36.00 years and the mean years of their experience were 12.3 ± 12.1 years. Majority (n = 3), had professional practice experience of 5–9 years.
Themes and sub-themes
Analysis of the interview data revealed themes and sub-themes that provide unique insights from participants’ perspectives as illustrated in Figure 1. These themes and sub-themes, ground in barriers that include medication side effects, inaccurate beliefs about mental illness and about medications, lack of resources, and lack of clear treatment guidelines, provide insights into major barriers impacting on medication adherence and uptake of metabolic monitoring. Exemplar quotes are accompanied by codes to indicate whether that participant was a patient (P), a carer (C) or clinician (Cl), their gender male (M) or female(F), and their age (two numerical values). Additional participant quotes are provided in Supplemental File 2.
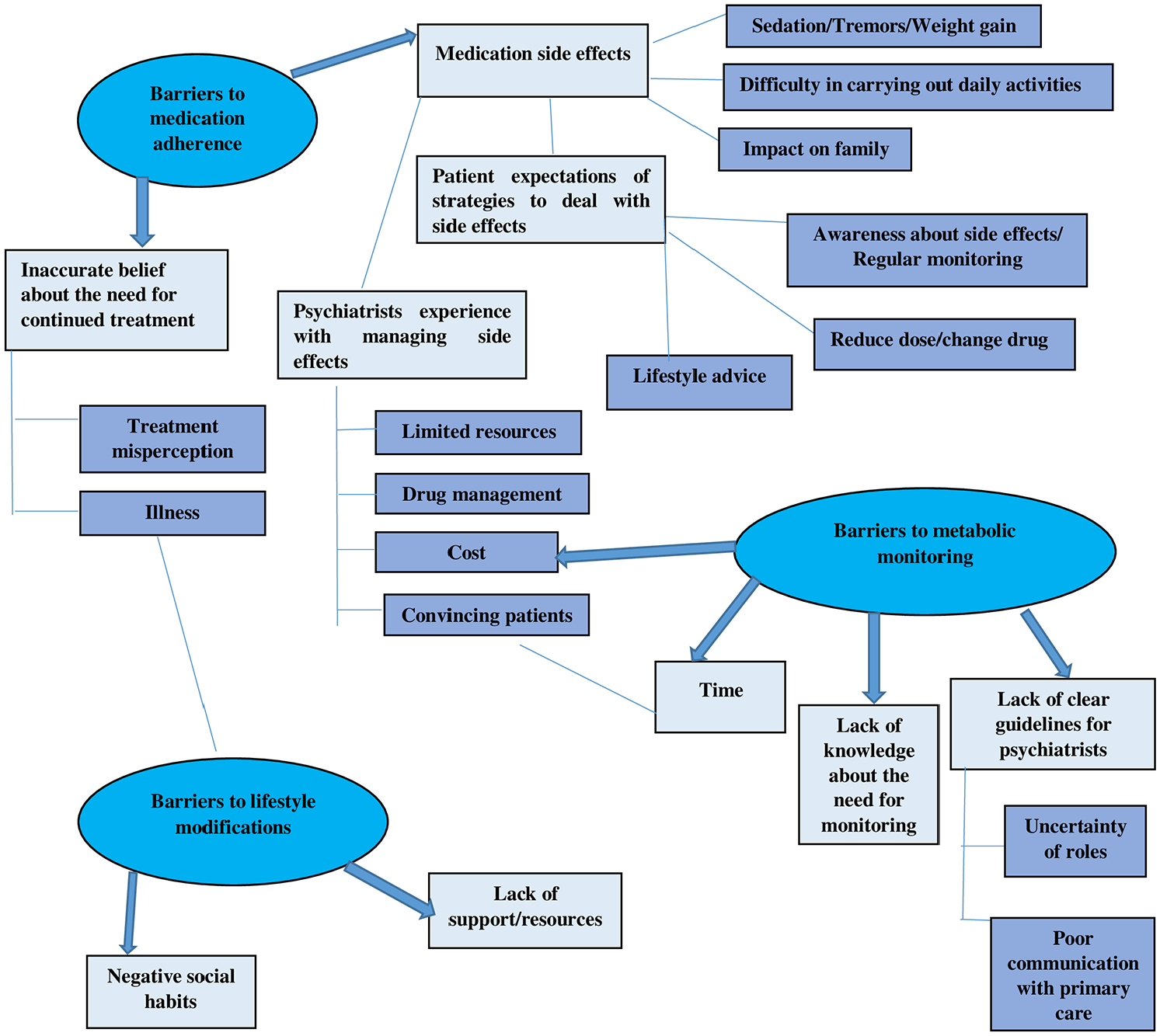
Themes and subthemes arising from interviews.
Three interrelated themes from the patient and psychiatrist interviews (oval) namely barriers to medication adherence, barriers to metabolic monitoring and barriers to lifestyle modifications were identified in relation to the study objective. These themes are reported along with their respective sub-themes (rectangular).
Theme 1: Barriers to medication adherence
Sub-theme 1.1: Negative impact of medication side effects
In general, patients reported positive orientation towards their treatment and stated that medication benefitted them by controlling their symptoms.
It calms you down, at any extreme point in your life if nothing is working out, you take antipsychotic drug it will calm you that’s all. PM26
However, participants described an extensive range of side effects that they had experienced, many of which caused them significant concern. Almost all reported that due to the sedative effects of their medication, they had trouble waking up in the morning: I cannot get up after sleeping, even after keeping alarm I cannot wake up. Mother has to wake me up nowadays, before I used to wake up at 4. Now I cannot wake up till 11-11·30. PM34
Another major side effect that patients were particularly concerned about was the tremors in their legs, arms and hands. They reported that their tremors were generally misinterpreted by members of the public and negatively impacted on how they are perceived: Even if I am normal people feel that I am drunken. PM39
Weight gain was a major concern.
Before I was 55 kg, 45-50 kg, when I came here first time, I was 28kg, then after taking medications I was above 60 kg. Now I am 74 kg. PF36
To a lesser extent patient also experienced blurred vision which made it difficult to see and to coordinate their movement. Experiences of side effects were not singular, instead, the vast majority of participants reported experiencing them in combination, the impact of which was profound. For example, some participants reported that taking their medication made them dull and inactive and they were not able to carry out daily activities of living, causing them to eat a lot of food due to increased, uncontrollable appetite and caused them to behave aggressively towards family and members of the public. As a result, family members endured increased workload, and were subject to stigma from members of the public.
If I don’t walk correctly people feel why is he like this, he may have some disease. PM39
Participants reported that to try and mitigate some of the medication side effects, they asked for their medications to be changed or they stopped taking their medication. Stopping medication was also commonly reported to occur when participants believed that their medication was not working, irrespective of whether they had experienced side effects or not.
… sometimes he gives me less power medications, last time he had given. PF30
Some also reported that they asked for a new medication when they felt the one that were taking was ineffective. Most of the patients also expressed a desire for more information about medication side effects and for regular check-ups so that they can be supported to manage medication side effects. Unanimously, participants agreed that having information and advice that incorporated lifestyle measures, particularly in the early stages after commencing SGAs, would help them anticipate and subsequently, the impact of medication side effects: Yes, of course, awareness regarding side effects if the doctors don’t tell you obviously you would not know what the impact has happened. PM35
However, some participants highlighted that often, if medication side effects became unbearable, they were more likely to stop taking their medications.
Psychiatrist participants also expressed concerns about the negative impact of medication side effects. They mentioned that raising awareness about potential side effects was a key priority.
… if we give them awareness that these things might happen they will be ready they may know that this can happen and they may not stop it in their own and they will come back with their concerns. ClF36
Unanimously, they articulated their observation that patients who had experienced significant weight gain, excessive sedation, and or metabolic syndrome, particularly in combination, would not likely keep taking their medication as prescribed, even when counselling is provided early in the treatment journey: I always explain to them about the side effects and till they are aware but there are people who have had weight gain and so they had stopped medications there had few people and we had people who knew the side effects and they were not willing to start treatment specially weight gain and infertility. ClF36
Psychiatrist participants also highlighted that the burden of increased appetite not only impacts the patient, for example, by causing weight gain, but often places financial burden on families who may then struggle to find enough money to feed the patient. Financial constraints were reported across many aspects of the care continuum, are discussed later.
few of them have reported a problem with that specially if the appetite becomes too much they reported that they find it difficult for looking after the family members because they get up at night and start eating food at night and they would have stored certain things for next day morning and its already empty. So a couple of patients have reported that and in fact sometimes this has been the reason why family members stop the medications also they say that it increases appetite so much so we can’t manage it so we want to stop. ClM35
Trialing different medications to minimize side effects and at the same time, maximize symptom control is challenging. Citing a lack of clear guidelines, psychiatrists described the process as a series of trial and error. With each new medication trialed, additional monitoring was needed which also placed a greater burden on limited hospital resources. While these aspects of changing medication were identified as challenging, they highlighted that the most challenging part was trying to convince the patient to try the new medication, keeping in mind the general health and comorbidities of the patient: So, for me also it is difficult to prescribe what I want then I have to make some adjustments mostly it’s like I have to convince, and I have to spend some time with them so it’s time-consuming. ClF36
One participant reported that some patients are reluctant to change their medication even if they are experiencing symptoms of metabolic syndrome: these drugs can cause diabetes that is they don’t take it seriously, there are some patients whom I explain okay still they want the same drug because they say they improve with that they say you put the treatment for diabetes or change the drug, these are the barriers patients’ beliefs. ClM47
Sub-theme 1.2: Inaccurate beliefs about the need for continued treatment
Some patient participants expressed a belief that once their symptoms had improved, it was unnecessary to continue to take their medications despite being advised by their psychiatrist to continue taking their medication as prescribed: I feel medications are not necessary since I am fine now, but Doctor says I cannot leave the medications now. PF42
Psychiatrists expressed the view that some patients lacked knowledge about medications and held erroneous beliefs about their illness: Second thing is this lack of knowledge that these drugs can cause diabetes that is they don’t take it seriously, there are some patients whom I explain okay still they want the same drug because they say they improve with that they say you put the treatment for diabetes or change the drug. ClM47
Their comments also align with the view expressed by psychiatrists that when symptom control is achieved, medications are believed to be no longer necessary. In addition, psychiatrists highlighted that for some patients, their illness may render them incapable of adhering to the prescribed medication regimen. For these patients, psychiatrists’ comments appear to transfer the responsibility of ensuring adherence to the patient’s carer or family members.
Ya I ensure that they adhere to the treatment … I usually tell the relative also to see them, sometimes patients may not be in a position to take medicines or may not be reliable so the relatives [unintelligible segment] give the medicines. ClM69
Theme 2: Barriers to lifestyle modifications
Sub-theme 2.1: Negative social habits
Some patients stated that social habits such as alcohol, smoking were the barriers to treatment adherence and were planning to quit their social habits since it doesn’t go well with antipsychotics.
I used to smoke, recently I am planning of quitting, because it’s not going well with my medications. PM27 Apart from that alcohol use also is negligible. Well actually, I am an occasional drinker, so alcohol is also negligible but there is some restrictions on that too. PM35
Sub-theme 2.2: Lack of support/resources
Psychiatrists also stated that they find it difficult to assess the lifestyle modifications suggested to the patients due to their illness or lack of personal motivation.
Barriers that we face are like we will not be able to monitor patient’s lifestyle modifications, so certain things that we are recommending them are now after use witness bands and let them come and show us. ClM35
Some of the patients experienced difficulty incorporating their medication into their daily lifestyle and undergoing regular monitoring and suggested that strategies like reminders along with awareness on lifestyle changes would help them.
Yes, reminders will be useful, it will help us understand if any improvement is there or is required. CF48
Theme 3: Barriers to metabolic monitoring
Sub-theme 3.1: Lack of knowledge about the need for monitoring
Patient responses indicate while they had experienced a range of medication effects, they had limited knowledge about how to manage the side effects and about the need for metabolic monitoring. Many disclosed that they only undertook monitoring when they were sick, during their follow-up appointment or when the medications got over: Whenever I am not well only that time had done this test. Once I got a fever before 2 years so that time BP had been checked. PF42
Sub-theme 3.2: Time and financial constraints
Some patients highlighted that due to a lack of time and travel expenses and cost of the test itself, they could not afford to undergo regular monitoring. They expressed a desire for greater access to testing so that they can minimize some of the associated costs: It is a lot of expenses and not only expenses only thing is the travel takes time and roadways and motorways you can’t just trust them when accidents can turn out to take place [cross talk]. Rather if you just give us a prescription of what needs to be tested then I can get it done it near my house. PM35
Their comments indicate an understanding that monitoring is beneficial to their health and are ready to undergo the tests if provided information and awareness regarding the tests nearby their homes.
Whenever asked if I have time, I will do but I make a point to do it, because it’s for my good only you are asking then why I wouldn’t do. PM26
The majority of psychiatrists agreed that monitoring the patient’s health, both in terms of treatment outcomes and metabolic impact, was their responsibility and that they should direct adequate attention to patients based on family history, guidelines, and when medications linked to metabolic syndrome are prescribed. Abnormal results are communicated to the general practitioners and necessary adjustments are done in the treatment.
Yes obviously it is before we start the medications it is our responsibility to evaluate them properly at the baseline only for eg, we take the consideration of even the family history of diabetes or any other problems before starting any antipsychotics so we consider it as our responsibility. ClM35 For eg, if there is any abnormal response immediately they are conveyed and we contact Physician and seek the opinion(…) and if necessary adjustments will be made in antipsychotics either shifting to some other antipsychotics or reducing the dosage. ClM35
One of the major concerns faced by the psychiatrists was patient’s unwillingness to undergo testing due to financial issues.
One of the barriers that we face is anybody that we ask to get blood tests done sometimes they become hesitant as to why it is required, because this is a mental illness and you tell about monitoring of the side effects then how much does it cost, should we do it so frequently, so if we want to look at the guidelines and want to strictly follow most of them we will do it at 6 months, few people will refuse and say they will do at next visit and they will never do. As a policy atleast I look once a year to make them mandatory do it. ClM35
As a strategy, they scheduled laboratory tests on the same day as their appointment date to help patients avoid transportation and consultation costs. However, as depicted by the comment above, the strategy in not always effective and many patients opt for testing near their house or do not undergo testing at all.
Sub-theme 3.3: Lack of clear guidelines for Psychiatrists
While some psychiatrists reported having a clear understanding of their responsibility for the monitoring of patients and having systems in place for communicating with primary care providers, many commented on a lack of standardized guideline that clearly define roles and responsibilities for the various health professional in the care continuum. Thus, there are discrepancies among health professionals as to their responsibilities which can result in miscommunication and subsequently, have a negative impact on the patient. A lack of guidelines for addressing medication side effects was also identified to compound difficulties experienced by psychiatrists. As described below, often they recognize that the medication should be changed for particular patients due to the metabolic side effects observed.
Some of the participants felt that more training for psychiatrists in handling metabolic side effects would be helpful along with the team as the psychiatric patients don’t develop rapport with other doctors such as general practitioners.
Ya I think we psychiatrists should be trained more about it as I told you like handling diabetes, handling because especially in a country with shortage of what we say, health itself is a big issue here. ClM47
Discussion
We conducted an in-depth interview to explore the challenges in the metabolic monitoring of patients on SGA from the practitioners’ and consumer’s perspectives. Literature evidences indicate that non-adherence to therapy can be troublesome in patients prescribed with SGAs antipsychotic medications. In our study, the patient participants reported negative impact of medication side effects, inaccurate beliefs about the need for continued treatment, and personal barriers such as substance use, financial constraints and lack of awareness about monitoring contributed to non-compliance to both medication and metabolic monitoring. Such perceptions may reduce adherence to therapy and monitoring. Understanding their concerns, experiences with antipsychotic drugs, and barriers in undertaking monitoring may permit healthcare professionals to target aspects of treatment that affect patients, which may in this manner influence their satisfaction and adherence to treatment. Also, a qualitative study by Bourassa et al. (2017) stated that parents, adolescents, and clinicians identified several individual and environment-related obstacles to obesity control including psychiatric symptoms, drug side effects, and lack of access.
To date, there has been a lack of published qualitative research studies that assess the subjective experiences of patients with severe mental illness treated with antipsychotic drugs regarding challenges in metabolic monitoring (Bjornestad et al., 2019). The findings of this study indicate that although most patients found that their treatment helped them with their condition, they did not feel it to be beneficial all the time. They reported adverse events with these antipsychotic drugs such as weight gain, and increased sleep which in turn caused a negative impact on their daily lives, due to difficulty in working. The current findings support previous research conducted by Rofail et al. (2009) to explore the experiences of patients with schizophrenia taking antipsychotic medication, the results of the thematic analysis showed that patients with schizophrenia usually found their treatment to be somewhat acceptable, but they also reported some adverse events and inability to work due to which they wanted to stop taking antipsychotic drugs. Also, a recent systematic literature review and meta-analysis of qualitative studies by Bjornestad et al. (2019) reported similar various adverse effects with the antipsychotics such as sedation, weight gain, limiting daily activities.
The key challenges to metabolic monitoring identified by our study were patients’ lack of awareness about metabolic monitoring, time and financial issues to undergo monitoring and lack of clear guidelines for psychiatrists. This is consistent with findings by Peña et al. (2018) on overcoming the barriers related to monitoring in patients prescribed with SGAs which identified a lack of patient and provider awareness regarding the risk of metabolic syndrome with the SGA use and financial hardships affecting follow-up as the barriers for low monitoring rates. These findings should be considered to address the barriers related to metabolic monitoring. Tabvuma et al. conducted an integrative review to assess the perspectives of mental health patients on physical health interventions. As per the patients, unresponsive healthcare systems were due to the lack of information about the medication side effects, negative staff attitudes, lack of importance to physical health, and failure to address physical health concerns (Tabvuma et al., 2022).
Most of the patients suggested providing awareness about the side effects along with regular monitoring and lifestyle modifications such as healthy diet, physical activities and reminders for monitoring would be helpful in preventing the concerns of antipsychotic adverse effects. A study conducted by Kioko et al. (2016) on improving the metabolic syndrome screening of patients on SGAs also recommended that the mental health professionals should consider including automatic reminders of monitoring for metabolic syndrome which will help the clinician when the tests are due and enable them to stick to the recommended guidelines. Follow-up calls to patients by case managers to prompt them of the importance of undergoing blood tests can also improve the screening rate. Findings from a meta-analysis by Mohanty et al. (2024), concluded that psychosocial management integrated with lifestyle modifications can help to prevent/manage the antipsychotic-induced weight gain.
In our study the major concerns of the practitioners about antipsychotics were the adverse effects of the drugs and the treatment misperception that when symptom control is achieved, medication is believed to be no longer required by the patients were the major contributors to the non-compliance of the medications. Another challenge faced by the psychiatrists was managing medication side effects of the SGAs as they had to spend additional time in trialing different medications to minimize side effects, maximize symptom control, and additional monitoring which was also a burden due to limited time and hospital resources. One of the major concerns faced by the psychiatrists was patient’s unwillingness to undergo testing due to financial burden. While some psychiatrists reported having a clear understanding of their responsibility for the monitoring of patients and having systems in place for communicating with primary care providers, many commented on a lack of standardized guideline that clearly define roles and responsibilities for the various health professionals in the care continuum. This was similar to a focus group conducted by Cooper et al. to understand the views and experiences of mental health professionals on antipsychotic reduction which indicated that participants acknowledged antipsychotics can have major adverse effects and that they were generally supportive of trying to reduce these drugs to the lowest effective dose, although stopping antipsychotics was less acceptable. Lack of resources, pressure to discharge, and poor continuity of care were seen as organizational barriers (Cooper et al., 2019). These findings suggest that healthcare professionals should explore and understand patients’ concerns and experiences with antipsychotic medication along with the regular discussion of potential adverse events or dissemination of educational materials. This can have a positive impact on patient adherence to treatment and monitoring which may benefit in decreasing relapses, health care finance, and social impact.
This qualitative study focuses on patient beliefs about illness, medication, and perceived side effects, alongside psychological factors such as the availability of support systems and socioeconomic factors like cost and access to services, contribute to barriers in medication adherence and monitoring which can help in the development of targeted interventions addressing the above factors.
Strength of the study – To our best knowledge this is the first study to specifically investigate the views of both patients and their treating practitioners on metabolic monitoring of patients on antipsychotics. This study included young and experienced psychiatrists in order to get their insights regarding the challenges faced in metabolic monitoring which has not been explored in this vulnerable population. Patients who were on antipsychotics for a year as well as those on long-term treatment were also included in the study. Another strength of this study was that despite the patient’s illness we could engage the participants in the conversation.
The limitations of this study were that due to the lack of insight in psychiatry patients and the busy working schedule of the psychiatrists, we were unable to do member checking or obtain feedback on our analysis from the participants. The interview guide questions could have been more directive and also the patient’s state of condition limited the richness of the conversation. The direct generalisability of this study may be limited as the availability and accessibility of resources differ among various countries but these findings can still provide valuable insights for regions with similar challenges and contextual understanding which can serve as a basis for comparative studies in future among diverse patient populations.
Conclusion
Improving patient awareness about SGAs and the benefits of metabolic monitoring may enhance adherence to both and contribute to better patient outcomes. Future research is important to decide the necessary strategies to increase the rate of metabolic monitoring in routine clinical practice. The clinical implications of these findings indicate that healthcare professionals should take time to address the barriers to metabolic monitoring which should include the development of relevant strategies such as education, metabolic monitoring tools,and reminders to improve the metabolic monitoring rate in patients on antipsychotic drugs.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251315263 – Supplemental material for Consumers’ and practitioners’ perspectives on the antipsychotic induced metabolic syndrome and challenges in metabolic monitoring to patient prescribed second generation antipsychotics in severe mental illness
Supplemental material, sj-docx-1-hpq-10.1177_13591053251315263 for Consumers’ and practitioners’ perspectives on the antipsychotic induced metabolic syndrome and challenges in metabolic monitoring to patient prescribed second generation antipsychotics in severe mental illness by Pooja Gopal Poojari, Amary Mey, Sohil A Khan, Sonia Shenoy, Keshava Pai, Sahana Shetty, Sripathy M Bhat, P Venkataraya Bhandary, Leelavathi D Acharya, Swarnali Bose and Girish Thunga in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053251315263 – Supplemental material for Consumers’ and practitioners’ perspectives on the antipsychotic induced metabolic syndrome and challenges in metabolic monitoring to patient prescribed second generation antipsychotics in severe mental illness
Supplemental material, sj-pdf-2-hpq-10.1177_13591053251315263 for Consumers’ and practitioners’ perspectives on the antipsychotic induced metabolic syndrome and challenges in metabolic monitoring to patient prescribed second generation antipsychotics in severe mental illness by Pooja Gopal Poojari, Amary Mey, Sohil A Khan, Sonia Shenoy, Keshava Pai, Sahana Shetty, Sripathy M Bhat, P Venkataraya Bhandary, Leelavathi D Acharya, Swarnali Bose and Girish Thunga in Journal of Health Psychology
Footnotes
Acknowledgements
Pooja Gopal Poojari would like to acknowledge Indian Council of Medical Research (ICMR), New Delhi for providing the fellowship for her PhD, Manipal Academy of Higher Education (MAHE), Manipal College of Pharmaceutical Sciences, Department of Psychiatry, Kasturba Medical College, Manipal, Kasturba Medical College, Attavar, Mangalore, Mitra Hospital, Udupi and Baliga Hospital, Udupi and Griffith University, Australia.
Author note
First author Pooja Gopal Poojari has moved to a new institution after the completion of her PhD. New affiliation: Pooja Gopal Poojari, Associate Professor, Department of Pharmacy Practice, Srinivas College of Pharmacy, Valachil, Farangipete Post, Mangalore – 574 143 Karnataka, India.
Author contributions
Pooja Gopal Poojari substantially contributed to literature search, conducting interviews, transcribing interviews and drafting the manuscript. She has access to all data. Girish Thunga, contributed to design, conception, analysis of the data and also has verified the data along with Pooja Gopal Poojari. Sohil A Khan contributed to conception, designing the questionnaire. Sonia Shenoy, Keshava Pai, P Venkataraya Bhandary, Sripathy M Bhat aided in data collection. Swarnali Bose, Amary Mey helped in interpretation of the data. Sahana Shetty, Sohil A Khan, Leelavathi D Acharya, Swarnali Bose, Sonia Shenoy, Keshava Pai, Girish Thunga contributed to revision of the manuscript. All authors gave final approval and are having access to the data. Amary Mey is an expert in qualitative research who provided her valuable feedback in revision of the manuscript.
Data sharing statement
Raw qualitative data cannot be shared due to ethical restrictions. Anonymised qualitative data will be shared on reasonable request to the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was granted by the Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee (IEC No-490/2018) for interviewing the participants and the study was registered with the Clinical trials registry of India (CTRI Registration Number: CTRI/2018/12/016610).
Informed consent
Written informed consent was taken from the participants before audio recording the interviews.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.