
Abstract
To meet the priority healthcare needs of any population there must be a consistently available blood supply donated by willing donors. Due to this universal need for blood, retaining blood donors remains an ongoing challenge for blood services internationally. Encouraging psychological ownership, or the feeling of ownership one experiences over a possession, provides a potential novel solution to donor retention. This study, based on semi-structured interviews with blood donors, investigates how donors perceive and develop psychological ownership in the context of blood donation. Interviews were conducted in Australia with 20 current blood donors (10 men, 10 women; Mage = 41.95). Through thematic analysis, six themes were identified based primarily on the theoretical framework of psychological ownership. This research offers a novel perspective on donor retention, suggesting that donors’ ownership over their individual donation practices, and not the blood service, may contribute to maintaining a stable blood supply.
Keywords
The World Health Organization (2023) lists blood and blood components as essential medicines. This means blood must be consistently available to fulfil the priority healthcare needs of any population. As consistent demand for blood requires the ongoing availability of willing donors, a key challenge for any healthcare system is sustaining a sufficient pool of blood donors to meet transfusion demands.
Alongside providing a consistent blood supply, retained donors offer multiple benefits to blood services as they are less likely to transmit infections, more motivated to recruit new blood donors and are more cost-effective compared to new donors (Devine et al., 2007). However, internationally between 16.5% and 64.7% of first-time blood donors will not return to donate again, with large variations in donor return observed across countries (Masser et al., 2020). Enhancing donor retention thus provides a key opportunity to increase the blood supply.
Most interventions to enhance donor retention have focused on reducing donor anxiety or encouraging donors to undertake additional planning around donation (Van Dongen, 2015). However, from a theoretical perspective blood donation becoming part of a donor’s self-identity (I am a blood donor) is considered a core motivational mechanism for sustaining donation behaviour (Callero, 1985; Ferguson et al., 2020; Piliavin and Callero, 1991). Formative research revealed a direct relationship between a blood donor self-identity and stronger intentions to donate blood amongst American blood donors (Callero, 1985). Likewise, research from Australia has shown that a specific blood donor self-identity is a stronger predictor of intention to donate blood in the future than a general altruist role-identity (White et al., 2017). However, despite donor identity being related to both future intentions to donate blood and blood donation behaviour (Masser et al., 2012), interventions to encourage this donor identity in the absence of donating blood are scarce. To our knowledge, the only research which has sought to build a blood donor identity in the absence of behaviour has leveraged already existing group identities. For example, research by Bryant et al. (2024) found support that using rivalry and competition based on Australian students’ university identities was effective in encouraging donation behaviour among students. In the absence of effective interventions to build a donor identity, we turn to psychological ownership as a construct with the potential to both strengthen this identity and encourage donor retention (Edwards et al., 2023).
Psychological ownership is a perceived sense of ownership of both material (e.g. the blood service) and abstract immaterial (e.g. blood donation behaviour) possessions (Pierce and Jussila, 2010). This ownership can be experienced over possessions not legally owned. There are multiple theoretical motivational reasons why someone may want to experience feelings of ownership. These are wanting to alter a potential environmental outcome (effectance), wanting to express identity through a possession (self-identity) and wanting familiarity (home; Pierce et al., 2001). Critically, ownership is theorised to bolster self-identity as identity can be established and maintained through possessions (Pierce et al., 2001). However, others have argued that identity provides the foundation for experiencing ownership (Peck and Luangrath, 2023). We suggest that bolstering ownership may increase self-identity but recognise that self-identity is likely a force that both creates and results from feelings of ownership.
The concept of psychological ownership originated in the organisational management literature, with research demonstrating that the more ownership employees feel over an organisation, the more likely they are to support the organisation (Van Dyne and Pierce, 2004). However, the utility of psychological ownership extends beyond for-profit organisations. In the first study to apply psychological ownership to a nonprofit service, Ainsworth (2020) demonstrated that the more time spent volunteering, the greater the sense of ownership volunteers had for their nonprofit organisation, and the more likely they were to keep volunteering.
In our previous research (Edwards et al., 2023), we tested whether psychological ownership was related to blood donation. We found that ownership experienced towards a blood service was positively related to past donation experience and was positively associated with future intentions to donate blood. Based on these findings, interventions which encourage ownership in blood donors could theoretically improve donor retention. However, most research on psychological ownership has measured, as opposed to manipulated, the construct (Peck et al., 2021). Further, there is a general lack of consensus on how psychological ownership is conceptualised and measured (Dawkins et al., 2017). As ownership-based interventions are a potential route to enhance blood donor retention, we need to understand how psychological ownership is experienced by blood donors.
This research focuses on how blood donors understand psychological ownership. First, we aim to explore whether blood donors experience ownership over their blood service or their blood donation experience (what is the target of ownership?). Most research on psychological ownership has focused on organisations as the target of ownership feelings (e.g. volunteers’ perceptions of ownership over a non-profit organisation; Ainsworth, 2020). Likewise, our previous research focused on the extent to which blood donors experience ownership over a blood service. In Australia, blood can only be donated through a single organisation (Australian Red Cross Lifeblood [Lifeblood]) and so it is possible that ownership of the organisation is synonymous with ownership of the act. However, given the multiple diverse donation systems that exist internationally (e.g. countries with more than one operating blood service), it is necessary to understand whether blood donors perceive ownership over the blood service (organisation) or towards the experience of donating blood (behaviour).
Second, we ask: how is psychological ownership developed? Before ownership-based interventions can be created to enhance donor retention, it is necessary to understand how blood donors may experience ownership. When Pierce et al. (2001) defined psychological ownership, they identified three potentially interrelated theoretical routes (antecedents) to experiencing psychological ownership: controlling a possession (control), coming to intimately know a possession (intimate knowledge), and investing the self into the possession (investment of the self). These antecedents are proposed to act as levers that can either increase or decrease perceived psychological ownership (Peck and Luangrath, 2023). Given that the application of psychological ownership as a theoretical framework to blood donation is novel, below we provide a summary of how each antecedent may be conceptualised in relation to blood donation.
Control
Pierce et al. (2001) proposed that controlling an object was key to experiencing ownership. Giordano et al. (2020) later defined control as personally using, shaping, or influencing an object, as well as controlling its use by others. Within an organisational context, individuals will feel more ownership towards the element of an organisation they can control (Pierce and Jussila, 2011). Donors may exercise control over their blood donation by practicing autonomy in their individual donation experiences and establishing donation-based habits and routines.
Intimate knowledge
Pierce et al. (2001) proposed that individuals can experience ownership through both association and familiarity. Intimate knowledge thus refers to both the depth and breadth of knowing an object (Brown et al., 2014). However, what this means practically in a blood donation context is unclear. Verkuyten and Martinovic (2017) argued that unlike forming an attachment to an entity, ownership is established and maintained in relation to others (this is my blood service, not yours). As such, blood donors may perceive intimate knowledge as specific donation knowledge that they hold relative to other donors. Conversely, donors may establish intimate knowledge through a more generalised familiarity with the blood donation process.
Investment of the self
Pierce et al. (2001) proposed that in the same way one owns their self and their labour, one owns the objects they invest themselves into. Investment of the self thus refers to an individual’s personal investment of time, energy and any other aspect of themselves into an object (Brown et al., 2014). As one cannot donate blood without investing both time and a physical resource (blood), self-investment is likely indistinguishable in practice from past blood donation behaviour and as such is not a core focus of this research.
In this research, we explore if Australian blood donors perceive and develop psychological ownership. Specifically, we explore what the target of ownership is for blood donors (organisation or behaviour), and how ownership is developed in blood donors through exploring the theoretical antecedents of psychological ownership: control and intimate knowledge.
Methods
Materials and methods were preregistered on the Open Science Framework prior to data collection (https://osf.io/bkpe3).
Sampling and recruitment
We sought to recruit 20 current blood donor participants based on Braun and Clarke’s (2013) recommendation of 15–20 interviews when the study forms part of a larger program of research.
Eligible participants were over 18 years of age (the minimum age for blood donation in Australia). We defined current donors as those who successfully donated whole-blood, plasma and/or platelets at least once in Australia within the past 2 years.
Between September and October 2022, we conducted semi-structured interviews with 21 participants. Due to an audio failure only 20 transcripts were useable. As mentioned on all recruitment materials, participants were offered a $AUD30 gift card for their participation; 20 of 21 participants accepted.
Ten participants were recruited through an online blood donation community page (Donor Community) and were thus considered highly motivated donors. These participants had also previously participated in an initial survey on psychological ownership and blood donation (Edwards et al., 2023) where they consented to be contacted again by the research team. Ten additional participants were recruited through university networks.
Data collection
The interview guide was primarily created by the first author with support from all co-authors. The authorship team has collective research expertise in blood donation and psychological ownership, as well as conducting qualitative research. The primary focus of interviews was whether participants perceive ownership over their blood service or their blood donation, and if ownership is fostered through donation habits and routines. As such, interviews broadly comprised questions and prompts to understand whether participants created routines around their blood donation and how these routines may change with donation experience. Specifically, participants were asked to provide an in-depth account of their last donation experience and were further prompted to provide information on their donation preparation and recovery. Further questions were asked to understand what knowledge is meaningful to participants (e.g. ‘Was there anything that you were particularly curious about when you started donating?’), how participants viewed themselves in relation to other donors (e.g. ‘Do you ever communicate with other blood donors?’) and how participants perceive the blood service (e.g. ‘When you think of the blood service, what do you think of?’). Finally, participants were asked direct questions to gauge their perceptions of ownership towards the blood service (e.g. ‘Do you feel personal ownership over the blood service?’). Additional prompting questions were used throughout the interviews.
Data was collected through semi-structured interviews conducted via online video calls (Zoom) and phone calls, based on participant choice. All interviews were conducted by the first author who has experience in conducting research with blood donors. Interview duration was between 20 and 90 minutes, with the average interview lasting approximately 40 minutes. Participants provided written consent prior to the interview, and verbally re-confirmed consent at the beginning of their interview. All participants were informed both in writing and verbally that interviews would be recorded and would later be transcribed and analysed by the research team. Further, participants were informed of the voluntary nature of their participation and that they could cease participating at any time.
Ethical statement
The study was approved by The University of Queensland’s Human Research Ethics Committee (2022/HE001220) and ratified by the Lifeblood Ethics Committee (2022#34).
Analysis
Data analysis was informed by Braun and Clarke’s (2006) six-phase thematic analysis process. The application of our theoretical framework (psychological ownership) to a blood donation context is novel. As such, thematic analysis allowed for themes to be informed deductively based on the broader psychological ownership literature, as well as inductively to capture novel interpretations based on the unique blood donation context.
Interviews were transcribed verbatim and de-identified. Only transcripts of audio recordings informed analysis. The first author read the transcripts thoroughly to check for accuracy, while simultaneously gaining familiarity with the interviews and making initial annotations. Coding was then conducted on the complete dataset. NVivo (1.6.1) was used throughout the analysis process. The first and second authors, one of whom is an experienced qualitative researcher, co-coded three transcripts and then came together to compare and discuss codes and higher-level themes. The remaining interviews were coded by the first author. Transcripts were coded with the view to identify topics related to psychological ownership and its antecedents as well as inductive coding to identify other topics commonly discussed by participants.
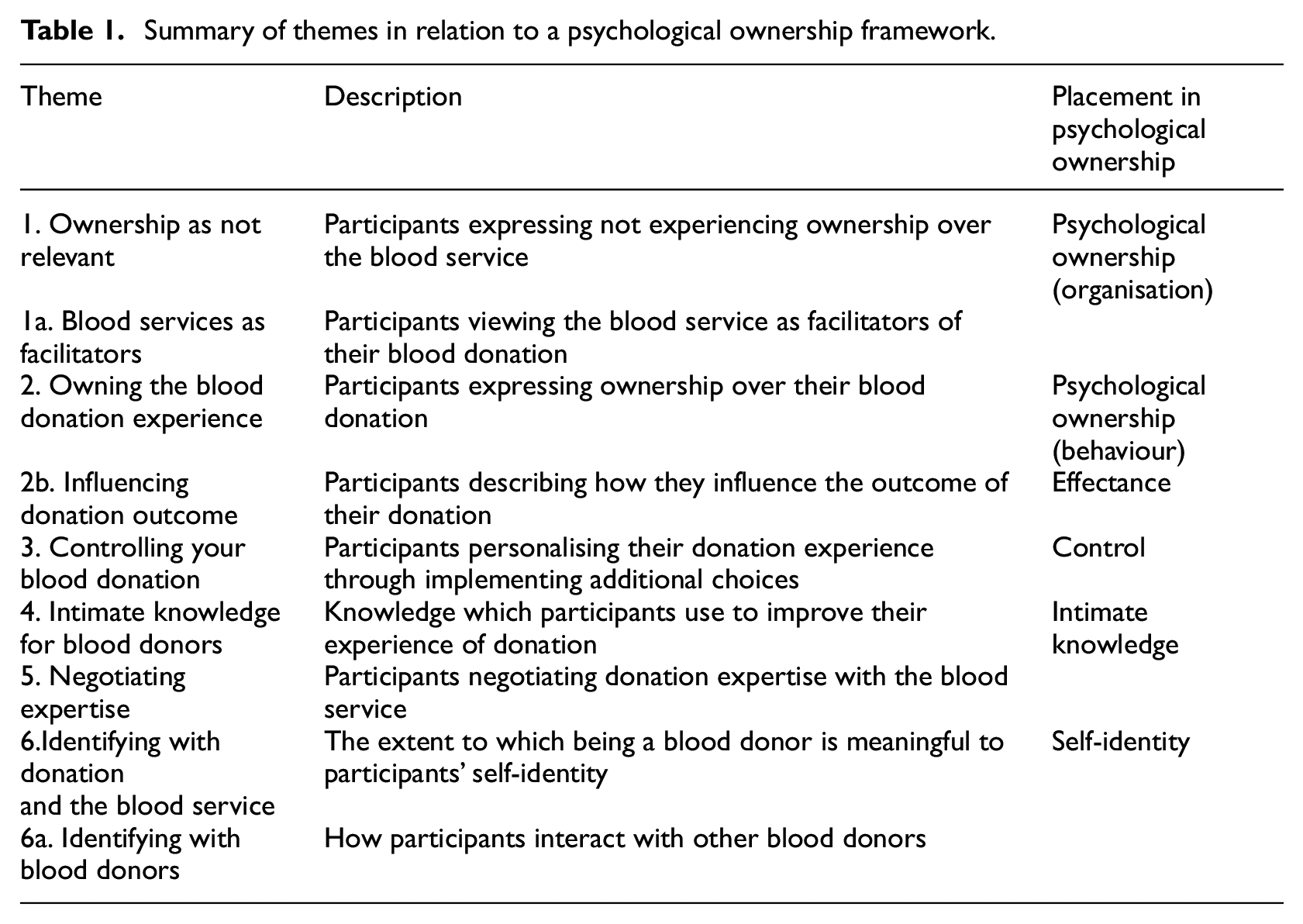
Themes were initially constructed based on our theoretical framework: psychological ownership, with its theoretical antecedents (control and intimate knowledge) and motivational factors (effectance and self-identity; see Table 1 for a summary of themes in relation to this framework). We had originally intended to only focus on psychological ownership and its antecedents. While most themes were derived from psychological ownership as a theory, the theme Negotiating expertise and sub themes Blood Services as facilitators and Identifying with blood donors were based on inductive coding. Themes were refined by the research team.
Summary of themes in relation to a psychological ownership framework.
Participant demographics
The analysed sample comprised 20 participants (10 men, 10 women) ranging in age from 21 to 71 years (Mage = 42.0). Participants self-reported to have successfully completed between 2 and 443 donations. Donor community participants were on average more experienced donors (Mdonations = 152.8) than university network participants (Mdonations = 21.5).
Results
Themes are presented and discussed in order of their relevance to the theory of psychological ownership (see Table 1 for summary of themes).
1. Ownership as not relevant
When asked about their perceptions of the blood service, most participants responded positively, commenting on the necessity of having a blood service, the friendliness of staff and the generosity of blood donors. However, despite having positive attitudes towards the blood service, participants did not express feeling ownership of the blood service. Ownership is not an easily articulated construct (Peck and Luangrath, 2023), and even participants who were highly experienced donors only spoke about ownership when directly prompted to do so through questions such as, ‘do you feel like the blood service is your organisation’ and ‘do you feel any ownership towards the blood service’.
Most discussions around ownership occurred at the end of these interviews after psychological ownership was explained to participants. Within these discussions only two participants described feeling a sense of ownership over the blood service. Of these two, one participant described feeling ownership over their local donor centre due to the amount of time they had invested donating blood at that specific location. In discussing how they interpreted ownership prior to the psychological ownership framework being explained, participants commented on having difficulty applying the concept of ownership, which often felt tied to objects or constrained by legal definitions, to a non-profit organisation: I do feel that sense of like… [donor centre], that’s my centre. So I do feel like the ownership in that sense. It’s a place that I go to, often, regularly for years… It’s just like saying [place name] is my city. So yeah, I feel the ownership, in that sense. It’s a place that I go to often. I enjoy going there. And a part of me is intertwined in that. So I do feel that kind of ownership. (Donor Community 9, 175 donations)
One participant who was both a blood donor and employed as a phlebotomist at the blood service described not feeling ownership over the blood service. They explained that this was due to the limited influence they had over the donation process relative to the influence they experienced as a staff member. When asked why they didn’t feel like the blood service was their organisation, another participant explained, ‘It just doesn’t feel incredibly personalised. It seems like it’s very big, very large system that does something relatively generic’ (University Networks 10, 9 donations).
1a. Blood services as facilitators
On reflecting on why they did not perceive ownership over the blood service, participants spoke about how they viewed their role as a donor compared to the role of a blood service as an organisation within a broader blood collection system. One participant spoke about not feeling ownership over the blood service as they did not have legal ownership over the donation facilities (the role of the blood service): …I don’t own the building…. I don’t have any ownership of the staff or the building or what they’re doing in there. So I don’t really have any ownership of that… I trust that they’re doing the right thing with my blood… I just figured that they own it now so they can do whatever they want with it. (University Networks 2, 15 donations)
This participant accepted their role as a donor and as such did not need to know or control the procedures and policies of the blood service. Other participants expressed various degrees of interest in the blood service and what happens to their blood post-donation.
Rather than expressing ownership, participants saw the blood service as the facilitator of their blood donation in that the organisation provided the infrastructure and opportunity to support their individual donation practice. In response to whether they felt like the blood service was their organisation, one participant noted that while they saw themselves as part of the organisation due to their regular donation schedule, the blood service was primarily a service provider for their blood donation: I mean, I think of them in that, almost that like I’m part of them as like a regular donor. And they kind of facilitate me being able to do what I want in terms of donating. Like, they have the facility there. They’ve got the staff who are capable and knowledgeable. And they make it easy for me to do what I want to do, which is show up once a month and donate. (Donor Community 5, 18 donations)
2. Owning the blood donation experience
Within the discussions of ownership that occurred at the end of the interviews, participants spoke about having ownership over their donation experience. Although donors are unable to control or influence the blood service, they can control aspects of their donation. When asked if they felt ownership over the donation process, one participant described that while their donation was facilitated by the blood service, they were able to have ownership of their donation: So I guess there is definitely like some ownership over donation. Because if you can go in and [the blood service staff] say… ‘which arm’ and you go, ‘oh, this one’s the only good vein’ or like, ‘I prefer this one.’ So that’s sort of you being like, ‘yeah, this is my donation. You’re sort of the conduit to get the blood out of me. Absolutely. But like… I know how this donation is supposed to go’. (Donor Community 3, 28 donations)
Another participant when asked if they felt ownership over the donation process described owning the small part that their individual donation experience played within a much larger blood collection system: …I do take absolute ownership of my experience and getting ready for my experience, but in terms of the whole organization… I’m just a little corner piece… in the bottom row of the whole mega thing. And I go there, I play my part, I do what I want [donating blood], what I’m there to do, because I believe in [blood donation] and it’s important. And it motivates me massively as an individual. But when I walk out the door, that bag of fluid is going into… somebody else’s hands now. (Donor Community 6, 443 donations)
2b. Influencing donation outcome
Ownership allows individuals to modify and adapt their environment. The process of causing an outcome is proposed to fulfil an innate need to be efficacious or to have the ability to produce a desired outcome (Pierce et al., 2001). Participants spoke about implementing new practices into their donation preparation to influence their desired donation outcome. For example, when describing their last blood donation one participant who had multiple previous unsuccessful donation attempts described how they used preparation to optimise their chance of successfully donating: I remember I was optimistic because I felt pretty relaxed. I had a mate with me and I had done all the drinking water and having some food and all the things that I could possibly do to make it work well. I talked to them about getting some heat packs on my arms so that my circulation was really good, stuff like that. (University Network 10, 9 donations)
Although not the primary focus of the interviews, participants expressed wanting to influence outcomes of their donation beyond just successfully donating. These outcomes included donating in a way that was fast and efficient to them, gaining purposeful downtime, and feeling healthy both during and after donating. For example, one participant described choosing to donate in the evening on their way home in order to have a relaxing donation experience: …I usually do the 7 o’clock in the evening appointments or around about, because it makes it easier to get there, there’s no traffic… and then I just go home when I’ve finished… I find that makes it less stressful because basically, once I get to the blood donation place, that’s it. I can just relax and sit there and wait for them to stab me… So that makes the actual donation process a lot more relaxed… (University Networks 7, 25+ donations)
3. Controlling your blood donation
Most participants expressed having stable blood donation routines. Such routines were based around donating at the same location, donating at a consistent time, donating the same product in regular intervals, and in some instances scheduling other activities (e.g. grocery shopping, physical activity) around blood donation.
These interviews provided insights on what components of a donation experience offer participants additional choices outside of the standard donation procedure. Participants could choose if they donate, what substance they donate, and at which location they will give their donation. While some participants preferred to choose the substance they donated (e.g. whole blood or plasma), others relinquished this choice to the blood service based on supply demands: …I always booked… fortnightly appointments [to donate plasma] unless [the blood service] needed whole blood. (Donor Community 1, 222 donations)
In Australia, donors can donate at either a fixed donation centre (allowing for blood, plasma and platelet donations), or a mobile blood collection van (allowing for only blood donations). Some participants expressed consciously choosing the site in which they donate based on the substance they wanted to donate, as well as the environmental aspects of the donation site. While some participants valued the convenience and atmosphere of the donation vans, others preferred the additional space offered in centres: I think some of the best experiences I’ve had have just been in the mobile vans… One time I went to a mobile van and they had just a whiteboard, and people had written up why they were blood donors and what got them started and stuff like that…Things like that are a really positive experience for me. (University Network 10, 9 donations)
Participants also expressed controlling elements of how they prepare for and recover from blood donation. Within this Australian context, donors are given standard preparation and recovery instructions to drink 8–10 glasses of fluids the day before a donation, and to drink 750 mL of fluids, eat something savoury and avoid strenuous exercise three hours before a donation. Participants used these instructions to inform their preparation for a donation. However, while some participants chose to strictly adhere to these instructions, others chose to deviate and engage in a preparation schedule which was more intuitive to them: With the rehydration protocol I’m not measuring my water. I know the first few times I [donated blood] I was really conscious of how many mLs I was putting in, and following everything to a T. I think now I have a bit more of an intuitive sense of my hydration. So that’s now more ad hoc. (University Network 9, 9 donations)
Although participants indicated that they focused more on preparing for donation than recovering, participants still exerted control through making choices post-donation. These choices extend to waiting the recommended recovery time at the donor centre, taking additional post-donation supplements such as iron tablets, adhering to recommendations to refrain from physical activity and sharing their donation experience with others.
4. Intimate knowledge for blood donors
Originally, we proposed that donors may establish intimate knowledge through becoming familiar with the blood donation process. When asked if anything had changed about how they donate blood since becoming a donor, one participant commented that the only notable change in the 2 years since they started donating was an increasing sense of comfort with each donation. ‘I think the first time I ever [donated blood] I was probably a bit nervous. Like now, it doesn’t make me nervous at all… just more comfortable each time I suppose…’ (University Network 3, 4-6 donations). Although gaining a general familiarity with both the donation centre and donation process was important for novice donor participants, given the standardised nature of the blood donation process general familiarity may not be inherently meaningful to more experienced donors.
Notably, while blood donor staff were not actively recruited, two donor community participants were also phlebotomists (one currently employed by Lifeblood [Donor Community 2], and one previously employed by Lifeblood [Donor Community 3]). An additional two participants (Donor Community 6, Donor Community 5) worked in health services and thus commonly used blood products in their work. The responses these participants provided reflected a general greater familiarity with blood donation and the use of blood products compared to other participants.
Throughout the interviews, participants expressed gaining various types of knowledge through their donation experiences. This included learning about the physical process of how a blood donation works, such as how blood is drawn and how a plasmapheresis machines operates. Participants also spoke about learning how blood donation felt within their body and how they could best prepare for and recuperate from donation. Finally, participants had gained a degree of organisational knowledge about how the blood service operates. However, participants still indicated substantial gaps in their knowledge of the blood service, and a want to learn more. When asked if there was anything about blood donation which they were still curious about, multiple participants responded with questions about blood service processes and procedures. Specifically, participants described wanting to know more about how blood is distributed, how plasma is and is not commodified, and generally what happens to their blood post-donation: I would love to know, like, much more about like, what happens after you donate. Like how… [the blood] actually reaches the hospitals and what the processes are … like do they get stored? Or do they like go to the hospital immediately, or stuff like that. I think would be cool to know. (University Network 1, 4-5 donations)
We initially proposed that intimate knowledge within this blood donation context would be knowledge donors held above that of their fellow donors. While one participant spoke about having more procedural knowledge than other donors due to their rare blood type, participants gave far more examples of actively sharing knowledge with other donors. Some participants even incorporated sharing their donation experience on social media as a part of their regular donation routine. When asked if there was anything about donation which they found particularly interesting, one participant described valuing learning about plasma donation as it was information which could be shared with others: …whenever I say I donate plasma, people are like, ….‘what’s plasma?’ …It’s not so known about compared to like a blood donation. So when I saw that, having learned about what …plasma can be used for that was handy in terms of when I started talking about it with other people. (Donor Community 9, 175 donations)
From these interviews, useable knowledge appears to be most meaningful to participants. For example, participants reported valuing knowledge which they could share with others (e.g. their experience and understanding of the donation process), use to monitor their own health (e.g. haemoglobin levels and blood pressure), and implement to improve their donation experience (e.g. using a blanket for additional heat). Participants combined information provided by the blood service and information learned through donating to optimise their donation experience. One participant described combining their understanding of their individual donation experience with more technical process-based knowledge to have a comfortable and efficient donation: I take my own blanket, because I just get really cold. I also know that my body, I need a heat pack to just help. Because I do get cold and when you get cold your blood, your vessels constrict, and then your blood flow’s not high enough. So I have a heat pack. (Donor Community 6, 443 donations)
Participants also valued knowing what they could do ‘ …outside of the structured stuff…’ (Donor Community 5, 18 donations). Examples of participants discovering additional ways to customise aspects of their donation included learning they could ask for different bandages and alcohol swabs.
5. Negotiating expertise
Through this process of applying knowledge gained from their own experiences, some participants engaged in a process of negotiating who is the expert and which body of knowledge to rely on when making sense of donation experiences. While participants acknowledged that they had both limited control over the in-centre donation process and limited phlebotomy knowledge compared to blood service staff, they had expertise of the experience of donating gained through often extensive donor histories. These negotiations of expertise often centred around phlebotomy incidents, where participants felt unsure of whether to rely on their own experiential expertise or the expertise of the phlebotomist at the blood service. For example, when recounting their last experience donating plasma, one participant commented on how the donation had taken longer than usual. In making sense of why this was the case, the participant was unsure whether to rely on their understanding of which veins they can donate from or the expertise of the phlebotomist: …the fact that the donation was slow was surprising because I’m not usually a slow donor, which I just attributed to the fact that they were using a vein that they don’t usually. Because normally… I’ve got quite big ones right in the middle of my forearms, which is normally where they go. So I wasn’t quite sure why they picked one on the side. But you know… they’re professionals. It’s their job. (Donor Community 5, 18 donations)
One participant and former staff member experienced an adverse donation event where during the apheresis process of plasma donation the red blood cells were not able to be successfully returned. This participant expressed frustration that the phlebotomist had not listened to their original request to stop the donation when they felt that the needle had been poorly inserted, ‘…I feel like if we had stopped earlier we could have returned it, but we had just jacked up so much pressure into that vein that I couldn’t get it back. So I think that’s what made it unpleasant to me that I have sort of said, ‘I think we should stop.’ And they’d sort of gone, ‘no, it’s okay’ ’ (Donor 3, 28 donations). For this donor, not having their expertise acknowledged led to both a physically unpleasant donation and the feeling of a loss of control over their donation experience.
6. Identifying with donation and the blood service
Participants varied in the extent to which they spoke about blood donation being an important part of who they were (donor self-identity). This was primarily reflected in participants responses to whether they spoke to others about being a donor. While most participants would mention donation to others around the time of their donation appointment, few participants spoke about donation outside of their appointment schedule. When asked if they spoke to others about being a blood donor one participant described only having conversations about donation when prompted by having a bandage on their arm: …the way they bandage you after you’ve given a donation people are like, “Oh, is something wrong with your arm”, and that’s a perfect opportunity to say, “No, I’ve actually just given blood” … it kind of – perhaps has prompted conversations… But, yeah, not otherwise. I don’t think there’s – you know, start the conversation out of nowhere… (University Network 8, 2 donations)
Perhaps as a product of being active members of a donor community, more participants recruited from the blood donor community page mentioned having conversations about blood donation outside of their appointment schedule and encouraging others to donate blood compared to participants recruited through university networks. For example, when asked if they talk to others about being a blood donor one donor community participants responded, ‘Yeah, all the time. Every opportunity I have, I try and encourage …people to donate blood…’ (Donor Community 6, 443 donations).
While some participants expressed an overlap between their identity as a blood donor and the blood service other participants saw themselves as separate from the blood service. When describing why they didn’t feel ownership over the blood service, one participant expressed that they did not see themselves as part the blood service ‘ …If there’s a Venn diagram I would be like way over on the left and the blood service will be way over on the right. And there will be no, no interaction’ (University Networks 2, 15 donations).
6a. Identifying with blood donors
Most participants did not see themselves as forming a coherent group with other donors, with only a handful of participants regularly interacting with other donors during and after their donations. One potential explanation for this lack of interaction during donations was the physical layout of donor centres with one participant commenting on how the donation chairs being placed far apart from each-other hindered socialising with other donors. However, multiple participants commented on actively choosing not to interact with other donors as they perceived blood donation to be synonymous with a medical procedure. For example, when asked if they interact with other donors one participant commented ‘No. I might have had a very brief nod of the head or something to somebody, but personally I feel like – you know like in some sense it’s quite personal. And it’s a pseudo-medical procedure, so perhaps rightly or wrongly I kind of want to give people their space and not impose upon them’ (University Network 9, 9 donations).
While for the majority of participants blood donation was an individual activity, the exception to this was the value placed on the interactions with blood service staff. Although not the key focus of these interviews, participants frequently spoke of their interactions with staff which ranged from pleasant small talk to staff actively facilitating a sense of community.
Discussion
This research provides a novel contribution to the blood donation literature through exploring how blood donors understand psychological ownership, and how ownership is developed and experienced by donors within an Australian context. While participants did not express ownership of the blood service, they did express ownership of donating blood. Theoretically, ownership is gained through controlling a possession, intimately knowing that possession and investing oneself into the possession (Pierce et al., 2003). Although donors can invest themselves into their local donor centre, blood donation is a highly structured procedure which offers donors limited opportunities to control or intimately know the blood service. Instead of expressing that they felt as though they owned the blood service, participants positioned the blood service as the facilitator of their individual donation practice.
Participants primarily expressed ownership over what they could control and know: their individual donation experience. Within controlling your blood donation participants expressed being able to choose which substance they donate, where they donate and how they prepare for and recover from donation. Further, through additional donation preparation, participants felt able to influence their individual donation outcome. Theoretically, being efficacious of having the ability to influence a desired outcome is an underlying motivation to experience psychological ownership (Pierce et al., 2001; Peck and Luangrath, 2023). We thus propose that donors are motivated to experience ownership as a means to influence the outcome of their donation.
Within intimate knowledge for blood donors, participants expressed gaining various types of knowledge through donating blood. This knowledge concerned the physical process of donation as well as how blood donation felt within the body. Within psychological ownership, intimate knowledge is the depth and breadth of knowledge one has of an object (Brown et al., 2014). Originally, we proposed that donors might establish intimate knowledge through gaining generalised familiarity with the donation process. However, while becoming familiar with the donation process was important for novice participants, it was not meaningful to experienced donors. Participants expressed valuing knowledge which could be applied. Specifically, participants appear to use what they learn from the blood service and through donating to share with others, monitor their own health, and to enhance their donation experience. We thus propose that the intimate knowledge which theoretically precedes ownership for blood donors is applicable knowledge.
Our finding that participants did not perceive ownership over the blood service contrasts with survey research in which blood donation history was positively associated with greater psychological ownership over a blood service (Edwards et al., 2023). One potential explanation for this contrast is that in survey research donors’ general positivity towards the blood service may have led participants to respond positively to items about ownership of the organisation. This alternative explanation has a basis in the literature as blood donors have generally positive perceptions of blood services, with donors internationally reporting a high level of quality, satisfaction and trust with their blood service (Melián-Alzola and Martín-Santana, 2020). Alternatively, interviews compared to surveys may have allowed donors to discuss ownership in their own words rather than simply responding to set questions focused on ownership of the organisation. Given that both previous survey research and the current study took place in an Australian single blood service context, questions on organisational ownership may have instead captured ownership of the donation experience. This speculation would be consistent with our findings that donors in the current study expressed ownership of their donation experience.
Ainsworth (2020) found support that people who regularly volunteered experienced psychological ownership over their nonprofit organisation. As such, participants perceiving ownership of the donation experience, and not the blood service, may highlight key differences in how blood services operate compared to other nonprofit organisations. Volunteers often act as partial employees of their nonprofit and are given opportunities to exert control or gain exclusive knowledge about how their nonprofit operates (Ainsworth, 2020). In contrast, blood donors are unable to control many of the processes and procedures put in place by the blood service, and do not gain exclusive knowledge of how a blood service operates. As such, donors may be unable to directly experience the feeling of ownership over a blood service. However, donors can control and know their donation practice and thus feel ownership over their individual donation experience.
Psychological ownership and its antecedents of control and intimate knowledge provide theoretical extensions of established constructs associated with donation behaviour. Specifically, within self-determination theory, autonomy is defined as having control over one’s behaviour (Ryan and Deci, 2000). Within blood donation, autonomy has been conceptualised as the sense of control donors have over the decision to donate blood. Interventions which build autonomy have been linked to increased motivation to donate blood (France et al., 2021). However, while research on autonomy has focused specifically on the decision to donate blood, our research supports the idea that donors also seek to control aspects of their donation experience. Through recognising that donors seek control beyond the initial decision to donate blood, blood services might focus on how to facilitate donors’ ability to personalise and control their donations within safe limits. This could be achieved through allowing donors to customise certain aspects of the donation process such as their individual donation schedules (Thorpe et al., 2020).
Curiosity, or the want to gather novel information, has been previously proposed to motivate donation behaviour (Bednall et al., 2013). Our findings fit with this idea, suggesting that donors want to use the knowledge gained from donating. Blood services may be able to leverage these findings through providing donors with useable education materials. Although blood services often provide such materials to decrease anxiety (France et al., 2010) or negative reactions (Thijsen et al., 2020), these education materials may have the additional benefit of providing donors with useable knowledge. This potential link between donor education and psychological ownership should be further examined in research.
A key limitation of this study is the dual sources of participant recruitment. Specifically, half of participants were recruited through an online blood donor community page and half were recruited through university networks. Donor community participants had on average more extensive donation histories and had previously participated in survey research on psychological ownership towards a blood service. Further, donor community participants had chosen to join a community group specifically focused on blood donation. While participants in both groups spoke about not experiencing ownership over the blood service, donor community participants primarily expressed ownership over the act of blood donation. This difference could reflect the importance of ownership in promoting donation behaviour (as donor community participants were on average more experienced donors), however it may also be a function of donor community participants being familiar with the psychological ownership framework due to their participation in our previous study. However, given the brief nature of the survey and the 8 months between participation, it is unlikely that interviewed participants retained key information from the survey. Future research should aim to look at naturally occurring ownership in groups of donors who have not been previously exposed to psychological ownership. Another limitation of the current study is that interviews were primarily coded in relation to the theme of psychological ownership. By focusing on a single theory, we may have limited our findings and missed capturing themes outside of psychological ownership that were important to participants. However, to mitigate this risk we included a combination of both theory driven and inductive coding in the analysis process. A final limitation of this study is that all participants came from an Australian single blood service context that is a Red Cross organisation, and thus findings from these interviews may not generalise to other institutional contexts or contexts where multiple blood collection agencies operate.
Maintaining a sufficient pool of blood donors is crucial for meeting predicted transfusion demands. Using psychological ownership as a theoretical framework represents a novel approach for enhancing donation behaviour. This study serves as a foundation for understanding how blood donors interpret psychological ownership and how ownership might be used to enhance donor retention. Psychological ownership appears to be closely linked to the donor’s individual sense of control and personalisation over their donation experience, not the blood service. An avenue for future research thus lies in empirically testing this notion. This could be achieved by using a simple ownership intervention, such as the ‘welcome to YOUR park’ messaging used by Peck et al. (2021) to enhance prosocial behaviour and manipulating the target of ownership to be donating blood. Such a study would be a first step to leveraging psychological ownership to potentially enhance donor retention.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241254581 – Supplemental material for ‘Yeah, this is my donation’: An application of psychological ownership in blood donation
Supplemental material, sj-docx-1-hpq-10.1177_13591053241254581 for ‘Yeah, this is my donation’: An application of psychological ownership in blood donation by Abigail R-A. Edwards, Rachel Thorpe, Barbara M. Masser and Fiona Kate Barlow in Journal of Health Psychology
Footnotes
Acknowledgements
We thank the participants for generously donating their time to this research.
Data sharing statement
The data generated and analysed during the current study are not publicly available as transcripts include personal health information relating to participants blood donor histories. Further, given the extensive donor histories of some participants we are hesitant to release additional information which may risk participants being identified. An extended codebook with additional example quotes is provided in supplementary materials.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by research funds allocated to the first author as part of their PhD and an award made from The University of Queensland Vice Chancellor’s Strategic Funds to the third author.
Ethics approval
The study was approved by The University of Queensland’s Human Research Ethics Committee (2022/HE001220) and ratified by the Australian Red Cross Lifeblood Ethics Committee (2022#34).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.