
Abstract
Chronic skin conditions can have psychosocial and somatic implications, influencing well-being and quality of life. This systematic review and meta-analysis aimed to synthesise evidence on the prevalence of comorbid mental health difficulties in 0–25-year-olds with chronic skin conditions. A secondary aim included identifying factors associated with resilience. The narrative synthesis included 45 studies. Four meta-analyses were performed with moderate-high quality studies, one for each outcome: diagnosed mental disorders; mental health symptoms; suicidal behaviour; socio-emotional and behavioural difficulties. The pooled prevalence of diagnosed mental disorders was 1.2% (95% CI = 0.2–6.1); of mental health symptoms was 22.6% (95% CI = 18.9–26.7); of suicidal behaviour was 7.8% (95% CI = 1.4–3.1); of socio-emotional and behavioural difficulties was 20.9% (95% CI = 14.7–28.8). Findings demonstrate the pooled prevalence of comorbid mental health difficulties in youth with chronic skin conditions.
Keywords
Introduction
Chronic skin conditions (CSCs) are common in youth. Acne vulgaris (acne) affects 85% of 12–25-year-olds (Seattle, 2013). Eczema affects 12% of 2–8 year-olds (Shi et al., 2021). CSCs can have wide-reaching implications for young patients. For example, they can greatly affect the quality of life of young patients and their caregivers, as well as incurring high financial costs (Finlay, 2009). Furthermore, CSCs can have adverse social and psychological implications for young patients. In terms of social effects, childhood, adolescence and young adulthood are impacted by differences in cutaneous physical appearance (Vivar and Kruse, 2018). From 2 to 10-years-old, children’s relationships with peers become more important and many experience bullying (Chernyshov, 2016). Individuals are most critical of their bodies during adolescence (12–17-years-old) and young adulthood (18–25-years-old) (Gestsdottir et al., 2018). Cosmetically disfiguring CSCs can result in increased self-consciousness and social disapproval or exclusion, sometimes leading to serious mental health problems (Gupta and Gupta, 2001). Conspicuous CSCs can provoke embarrassment and worry about body image in 12–18-year-olds, negatively impacting self-esteem and social engagement (Golics et al., 2009). With the societal and cultural importance of outward appearance, it is unsurprising that youth with visible CSCs especially may be concerned about their cutaneous physical appearance.
Psychodermatology concentrates on interactions between the mind and skin (Jafferany, 2007). Psychodermatologic conditions can require dermatological and psychological treatments. Psychophysiological conditions (e.g. eczema or psoriasis) can be exacerbated by emotional stress (Koo and Lebwohl, 2001). Stress contributes to the ‘itch-scratch cycle’ (Koo and Lebwohl, 2001) wherein itch is associated with stress, and stress can worsen itch (Sanders and Akiyama, 2018). This can lead to a cycle, negatively affecting patient behaviour (itching) and worsening disease prognosis and quality of life (QoL) (Sanders and Akiyama, 2018). Emotional stress is an aggravating factor for many CSCs including atopic dermatitis (AD) (Senra and Wollenberg, 2014), acne and urticaria (Gupta and Gupta, 2003).
It is well-evidenced that CSCs can have consequences on psychological well-being and QoL. Depression, anxiety and loneliness have been reported in adults with acne, AD and psoriasis (Yew et al., 2021). In a sample of 18-year-olds, those with acne had more depressive symptoms, feelings of uselessness and fewer feelings of pride, than their counterparts without acne (Dalgard et al., 2008). In interviews with adult hidradenitis suppurativa (HS) patients, participants reported that their sadness and depression began during adolescence and coincided with HS onset (Esmann and Jemec, 2011). Psychological comorbidities in combination with chronic health conditions can undermine medical treatment through poor adherence (DiMatteo et al., 2000), subsequently impacting disease outcomes. This has been reported for conditions including psoriasis (Bewley et al., 2014) and acne (Alghofaili et al., 2021).
Psychological factors can affect the management of CSCs in over one-third of dermatology patients, making it essential to consider such factors in their treatment (Picardi et al., 2006; Ponarovsky et al., 2011). Despite evidence highlighting comorbid mental health problems in adults with CSCs, evidence in youth with CSCs is more limited. Existing estimates in younger populations are inconsistent, ranging from 8% (Gilaberte et al., 2020) to 70% (Kara et al., 2019). It is important to synthesise evidence that holistically describes comorbid mental health difficulties in youth with CSCs. The primary aim of this review was to comprehensively synthesise evidence on the prevalence of comorbid mental health difficulties in young people with CSCs. Resilience is a dynamic process that promotes adaptation in individuals exposed to adversities and protective factors associated with resilience may result in functional outcomes in the context of diagnosable illness (Stainton et al., 2019). Identifying protective factors associated with resilience in the context of CSCs will add to our knowledge and contribute to the improvement of young people’s lives. A secondary aim of this review was to identify factors associated with better quality of life and/or resilience.
In this review, ‘diagnosed mental disorders’ refers to measures appropriate for diagnosis (e.g. formal diagnosis or diagnostic interview conducted by a psychologist). ‘Mental health symptoms’ refers to measures of symptoms of mental disorders but without meeting clinical diagnosis criteria, or tools not appropriate for diagnosis (e.g. depressive symptoms measured using the Hospital Anxiety and Depression Scale [HADS]).
Methods
A systematic review and meta-analysis were conducted adhering to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Liberati et al., 2009). The protocol was registered with the International Prospective Register of Systematic Reviews (ID: CRD42021258813).
Eligibility
Inclusion criteria were participants aged 0–25-years-old with CSCs; report of co-morbid mental health difficulty; cross-sectional or other study designs where the prevalence of interest is reported; published in English; peer-reviewed. Exclusion criteria were participants aged >25-years-old; acute/short-term skin conditions; case reports/series; reviews; grey literature; conference proceedings; editorials.
Search strategy
The Joanna Briggs Institute (JBI, 2020b) Manual for Evidence Synthesis guidelines were followed. Initial searches were conducted using keywords associated with the population, conditions and comorbidity of interest. Titles and abstracts were examined for keywords and database-specific index terms. A specialist librarian was consulted. Electronic searches were then conducted using keywords, index terms and other relevant terms retrieved using a thesaurus. A systematic search of the literature was conducted up to October 16, 2023. Searches were conducted in four electronic databases (PubMed, CINAHL PLUS, PsycINFO, EMBASE). Search strings are included in the Supplemental Material S1. Last, reference lists of included articles were searched.
Screening and data extraction
Titles and abstracts were screened by two authors independently. Inter-reviewer agreement was 99% (Cohen’s k = 0.88). Full text review was conducted by two authors independently. Inter-reviewer reliability was 96% (Cohen’s k = 0.79). Disagreements were resolved via discussion. References of included studies were reviewed by one author. Two authors extracted data using the JBI (2014) Data Extraction Form for Prevalence and Incidence Studies, adapted for this review. Figure 1 depicts the PRISMA flow diagram.
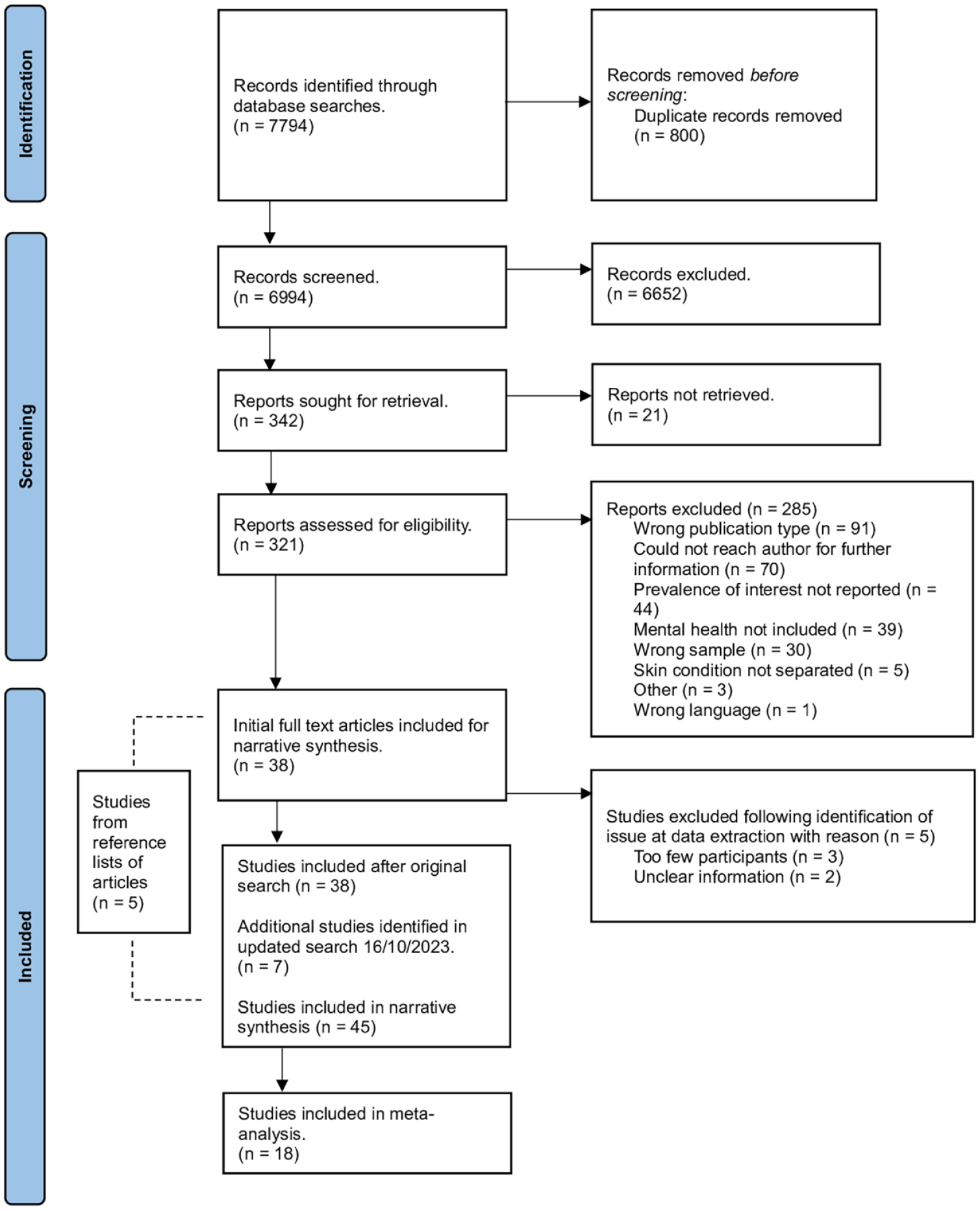
PRISMA flow chart to illustrate the process by which articles were selected or rejected for inclusion in the study.
Quality
Two authors performed quality assessment using the JBI (2020a) Critical Appraisal Checklist for Prevalence Studies. Nine criteria are represented with an item rated on a four-point response (Yes, No, Unclear, Not Applicable). There is variability regarding which domains to assess in prevalence studies (Migliavaca et al., 2020b). This tool is superior due to its high methodological rigour and ability to capture the most important domains (Migliavaca et al., 2020b). Applicable quality scores were calculated according to Glasgow et al. (2020). The score has a value range from −100% to 100% (where higher scores indicate higher quality) Glasgow et al. (2020) categorise scores into five ranges: from −100 to −60; −59 to −20; −19 to 20; 21 to 60; and 61 to 100. In order to improve interpretability of results, we assigned nominal labels to the score ranges (Very Low; Low; Moderate; High; and Very High respectively). Studies meeting 50% quality score thresholds were retained for meta-analyses.
Meta-analysis overview
Four meta-analyses were performed, one for each identified outcome: diagnosed mental disorders; mental health symptoms; suicidal behaviour; socio-emotional and behavioural difficulties. Only studies meeting 50% applicable quality scores were included. Random-effects models were used to account for heterogeneity. This assumes variance in effect sizes between studies leading to a more conservative null hypothesis model (Han and Eskin, 2011), and taking into consideration subject-specific effects (Laird and Ware, 1982). Outcomes were reported as dichotomous variables (presence/absence). Aggregated estimates, 95% confidence intervals (CI), Cochran’s Q-statistics and estimated effect sizes (tau2) were reported. Alpha was set at 5%. Heterogeneity was assessed using I2. Estimates were grouped by identified outcome, with separate meta-analyses performed for each. Four estimates were excluded because outcomes were not deemed appropriate for meta-analysis. Specifically, one estimate combined anxiety/depression, and three reported attendance at psychological services. Dependence, which can threaten the validity of meta-analytic results between-within studies, was addressed by conducting separate meta-analyses for each outcome (Van den Noortgate et al., 2015). Dependence may arise from multiple estimates spanning multiple outcome types but originating from one study. This method can result in the number of studies for some outcomes being too small to yield meaningful results. The Cochrane Collaboration state that two studies are sufficient, given they are meaningfully pooled and sufficiently similar (Ryan, 2016). There were four to eight studies for each outcome, therefore separate meta-analyses were possible.
Heterogeneity was explored using meta-regression testing the association between pooled estimates and type of mental health outcome, and CSC. Sub-analyses were performed where there were enough data.
Results
Table 1 summarises the included studies. Forty-five studies were included (n = 538,583 participants). Most studies were cross-sectional (n = 18) or retrospective reviews (n = 12). Most were conducted in the United States (U.S.; n = 8), Turkey (n = 6) and the United Kingdom (U.K.; n = 5). Sample sizes ranged from 7 to 409,431 participants. Where the sample’s age ranged above 25 years, only the relevant data were extracted, where possible.
Characteristics of the included studies. Time is in years unless otherwise stated.

Where (M; SD) is not reported in the table, it was not reported for our age group of interest.
Where male gender (%) is not reported in the table, it was not reported for the subgroup of interest.
International Classification of Diseases (ICD) 10th Revision code.
Schedule for Affective Disorders and Schizophrenia for School-Age Children.
Psoriasis; non-melanoma skin cancer; actinic keratosis; eczemas and contact allergy; acne; atopic dermatitis; Naevi and benign tumours; Rosacea, perioral dermatitis, facial erythema; Autoimmune diseases; Malignant melanoma; Hand eczema; Pustulosis palmoplantaris; Infections (not venereal); Urticaria; Pruritus and prurigo; ulcus cruris, stasis dermatitis and chronic venous insufficiency; Genital, not venereal; Monogenetic conditions; Other; Vitiligo; Seborrhoeic dermatitis; Hidradenitis suppurativa; Sarcoidosis and granuloma; Lichen planus; Alopecias; Pyoderma gangrenosum; Hyperhidrosis.
Hospital Anxiety and Depression Scale.
Patient Health Questionnaire-9.
International Classification of Diseases (ICD) 9th Revision code.
Treatment was considered effective, when improvement was observed on disease activity or quality of life. Children were characterised as ‘responders’ or ‘non-responders’.
Diagnostic and Statistical Manual of Mental Disorders.
Strength and Difficulties Questionnaire.
Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime version.
Joint initiative of the Dermatology Section of the European Academy of Allergology and Clinical Immunology (EAACI), the EU-founded network of excellence, the Global Allergy and Asthma European Network (GA²LEN), the European Dermatology Forum (EDF) and the World Allergy Organization (WAO).
Generalised Anxiety Disorder Questionnaire.
Austria, Belgium, France, Greece, Ireland, Israel, Italy, the Netherlands, Norway, Russia, South Africa, Spain and the UK.
Self-reported Alcohol Use Disorders Identification Test.
Allergic urticaria; Idiopathic urticaria; Urticaria due to cold and heat; Dermato-graphic urticaria; Vibratory urticaria; Cholinergic urticaria; Contact urticaria; Other urticaria (chronic, recurrent, periodical); Urticaria, unspecified.
CSCs
CSCs included AD (n = 14), eczema (n = 10), psoriasis (n = 11), acne (n = 5), HS (n = 4), urticaria (n = 4), vitiligo (n = 4), alopecia (n = 4), hyperhidrosis (n = 2), palmoplantar pustulosis (n = 2) and other dermatological conditions (n = 1). Four studies assessed multiple CSCs (included above). Table 1 presents CSC measurements and severity assessments. Most CSCs were identified through formal diagnosis by clinicians or within healthcare settings (n = 21), followed by authors’ self-developed items asking about participants’ diagnoses (e.g. has a healthcare professional told you that you have eczema?) (n = 11), insurance data (n = 7) and medical records (n = 6).
Mental health
Twenty studies reported diagnosed mental disorders. These included anxiety (n = 17), depression (n = 17), combined depression/anxiety (n = 1), unspecified psychiatric disorders (n = 4), obsessive compulsive disorder (OCD; n = 5), combined anxiety/OCD (n = 1), elimination disorders (n = 3), eating disorders (n = 2), psychotic disorders (n = 3), posttraumatic stress disorder (PTSD; n = 2), phobias (n = 2), conduct disorder (n = 2), oppositional defiant disorder (ODD; n = 2), substance abuse disorders (n = 2), bipolar disorder (n = 1), panic disorder (n = 1) and adjustment disorder (n = 1).
Twenty-eight studies reported mental health symptoms, including depressive symptoms (n = 14), anxiety symptoms (n = 8), combined depressive/anxiety symptoms (n = 1), combined depressive/anxiety/stress symptoms (n = 1), stress (n = 6) and socio-emotional or behavioural difficulties (n = 6). One study reported oppositional defiance symptoms.
Nine studies reported suicidal behaviour including ideation (n = 8), attempt (n = 3), self-injurious behaviour (n = 1) and planning (n = 1). One study reported combined ideation/attempt.
The most common tool for diagnosing mental disorders was the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS; n = 4). The most common measure for mental health symptoms was the HADS (n = 4). In eight studies it was unclear how mental health was assessed, for example, it was extracted from medical records with no further information (Table 1).
Quality
According to the score ranges presented previously in the Method section, four studies were low, 12 moderate, 16 high and 13 very high quality (Table 1).
Narrative synthesis: Prevalence of mental health difficulties
Diagnosed mental disorders
Twenty studies reported diagnosed mental disorders. Diagnosed depression ranged from 0% in 1–20-year-old HS patients in Israel (Shavit et al., 2015) and 0–18-year-old AD patients in South Korea (Ahn et al., 2019), to 43% in 8–17-year-old vitiligo patients in Turkey (Ucuz et al., 2021). Anxiety ranged from 0% in 1–20-year-old HS patients in Israel (Shavit et al., 2015) to 79.7% in 6–18-year-old AD patients in Spain (Sicras-Mainar et al., 2019). One study reported combined depression/anxiety in 10% of 8–17-year-old Turkish, vitiligo patients (Ucuz et al., 2021). It also reported combined anxiety/OCD (3.3%), and depression/OCD (10.0%). Unspecified psychiatric disorders ranged from 5.6% in 8–16-year-old psoriasis patients (Kara et al., 2019) to 75% in 9–18-year-old vitiligo patients (Ayyildiz et al., 2021), both in Turkey.
OCD ranged from 0.04% in <18-year-old AD patients in the U.K. (Wan et al., 2023) to 9.3% in 8–16-year-old psoriasis patients in Turkey (Kara et al., 2019). Phobias ranged from 2.9% (specific phobia) to 8.7% (social phobia) in 14–18-year-old Turkish, acne patients (Özyay Eroğlu et al., 2019). Eating disorders ranged from 0% (unspecified disorder) in 8–16-year-old psoriasis patients (Kara et al., 2019) to 5.8% (Bulimia Nervosa) in 14–18-year-old acne patients, both in Turkey (Özyay Eroğlu et al., 2019). PTSD ranged from 0% in 8–16-year-old psoriasis patients (Kara et al., 2019) to 11.5% in 14–18-year-old acne patients, both in Turkey (Özyay Eroğlu et al., 2019). One study reported panic disorder (0%) in 8–16-year-old psoriasis patients in Turkey (Kara et al., 2019).
Three studies reported psychotic disorders. Schizophrenia ranged from 0% in 0–13-year-olds in South Korea (Ahn et al., 2019) and <18-year-olds in the U.K. (Wan et al., 2023), to 0.13% in 13–18-year-old patients in South Korea (Ahn et al., 2019), all with AD. Combined delirium/psychosis/psychotic/dissociative disorders were 1.14% in 1–18-year-old German, psoriasis patients (Matusiewicz et al., 2014).
Conduct disorder ranged from 1.9% in 8–16-year-old psoriasis patients in Turkey (Kara et al., 2019) to 6.5% in 0–18-year-old AD patients in the U.S (Yaghmaie et al., 2013). ODD ranged from 0% in 14–18-year-old acne patients (Özyay Eroğlu et al., 2019) to 3.7% in 8–16-year-old psoriasis patients (Kara et al., 2019), both in Turkey. Psychoactive abuse was <1% in paediatric HS patients (Hallock et al., 2021). Substance abuse disorder was 25.8% in 18–25-year-olds with psoriasis from across 13 countries (Sampogna et al., 2019). Elimination disorders ranged from 6.7% in two studies, the first involving 9–18-year-old psoriasis, vitiligo and alopecia areata patients (Ayyildiz et al., 2021) and the second study 8–17-year-old vitiligo patients (Ucuz et al., 2021), to 7.4% in 8–16-year-old psoriasis patients (Kara et al., 2019), all in Turkey. One study reported adjustment disorder (3.9%) in 8–16-year-old Turkish psoriasis patients (Kara et al., 2019). One study reported bipolar disorder (0%) in <18-years-olds with AD in the U.K. (Wan et al., 2023).
Mental health symptoms
Twenty-eight studies reported mental health symptoms. Depressive symptoms ranged from 2.9% in 13–25-year-old patients with chronic spontaneous urticaria in Germany and Russia (Kolkhir et al., 2018) to 37% in 12–17-year-olds with AD in South Korea (Lee and Shin, 2017). Anxiety symptoms ranged from 2.2% and 3% for ‘some symptoms’ in 18–25-year-old HS and eczema patients, respectively, in the U.K. (Matcham et al., 2017) to 24.4% and 28.5% for ‘probable’ anxiety within the same study. The highest anxiety symptoms (53.3%) were in 18–25-year-old psoriasis patients across 13 countries (Sampogna et al., 2019). Combined depressive/anxiety symptoms were 15.5% in 9-year-olds with eczema in Sweden (Brew et al., 2018). One study reported combined depressive/anxiety/stress symptoms in 13% of adolescents (median age 16 years) with atopic eczema in Hong Kong (Hon et al., 2015). One study reported oppositional defiance symptoms (5.6%) in 6–12-year-olds with AD in China (Feng et al., 2020).
Other outcomes
Six studies reported attendance at psychological counselling ranging from 4% in 10–18-year-olds with AD in South Korea (Chun et al., 2015) to 18.8% in 2-months–15-years-old AD patients in the U.S. (LeBovidge et al., 2007).
Co-occurring stress with CSCs was defined in the included studies as psychological, emotional or mental stress (n = 5) and excessive stress in school/home environments (n = 1). Specifically, frequent psychological stress was reported in over half (56.1%) and excessive psychological stress in 5.6% of 10–18-year-olds with AD in South Korea (Chun et al., 2015). Emotional and psychological stress was reported in 54% of 2–18-year-old psoriasis patients in Turkey (Seyhan et al., 2006). Emotional distress was reported in 12.5% of 2-month–15-year-old AD patients in the U.S. (LeBovidge et al., 2007).
Six studies reported co-occurring socio-emotional and behavioural difficulties with CSCs. Absolon et al. (1997) reported ‘psychological disturbance’ (50%) in 5–15-year-olds with atopic eczema in the U.K. Behavioural and socio-emotional difficulties ranged from 8% to 11% in German children with eczema (Schmitt et al., 2010) to 35% in 4–18-year-olds with AD in Singapore (Leong et al., 2022) and 38% in 11-year-olds with eczema in the U.K. (Hesketh et al., 2016).
Suicidal behaviour
Co-occurring suicidal behaviour with CSCs was reported in a number of studies. Specifically, suicidal ideation (n = 7) ranged from 0% in 0–3-year-olds with AD in South Korea (Ahn et al., 2019) to 21.8% in 18–25-year-olds with multiple CSCs in Norway (Balieva et al., 2016). Suicide attempts (n = 3) ranged from 1.4% in 10–18-year-olds (Chun et al., 2015) to 6.1% in 12–17-year-olds (Lee and Shin, 2017), both with AD in South Korea. One study reported combined ideation/attempt ranging from 0.3% to 0.7% in <18-year-olds with mild and moderate AD respectively, in the U.K (Wan et al., 2023). One study reported suicide planning (8%) in 12–17-year-olds with AD in South Korea (Lee and Shin, 2017). One study reported self-injurious behaviour (41.4%) in 14–18-year-old acne patients in Turkey (Özyay Eroğlu et al., 2019).
Narrative synthesis: Factors associated with QoL
Two studies used the Child Dermatology Quality of Life Index to report better QoL in relation to treatment factors. A personalised, multi-disciplinary treatment programme reported that 53% of 8–18-year-old AD patients in The Netherlands showed improved QoL and disease activity (Fieten et al., 2017). A multi-disciplinary intervention study in 4–18-year-old AD patients in Singapore showed no significant improvements in QoL or disease severity, however, there was an overall trend toward improvement (Leong et al., 2022). Another study reported significant correlations between AD severity and QoL, with the latter decreasing as AD severity increased (Feng et al., 2020). Increased prevalence of mental health difficulties was associated with increased eczema (Absolon et al., 1997) and AD severity (Jaeyong et al., 2016; Yaghmaie et al., 2013). However, four studies observed no significant relationships between disease severity and mental health (Hon et al., 2015; Kara et al., 2019; LeBovidge et al., 2007; Ucuz et al., 2021). Self-esteem and life satisfaction played significant roles for 14–18-year-old acne patients in Turkey, but only for those with a psychiatric diagnosis (Özyay Eroğlu et al., 2019). Self-esteem and life satisfaction were lower in acne patients with a psychiatric diagnosis, compared to those with a psychiatric diagnosis but no acne. There were no differences in social support experienced by families of 5–13-year-olds with and without eczema in the U.K. (Absolon et al., 1997). No differences were reported between 8 and 18-year-old AD patients in The Netherlands regarding disease-specific coping (Fieten et al., 2017).
Meta-analyses
Only studies meeting a 50% applicable quality score threshold were included for meta-analyses. The number of studies in each meta-analyses and sub-analyses are presented in the Supplemental Material (S2). Figure 2 presents the studies included in each meta-analyses, sub-analyses and associated forest plots.
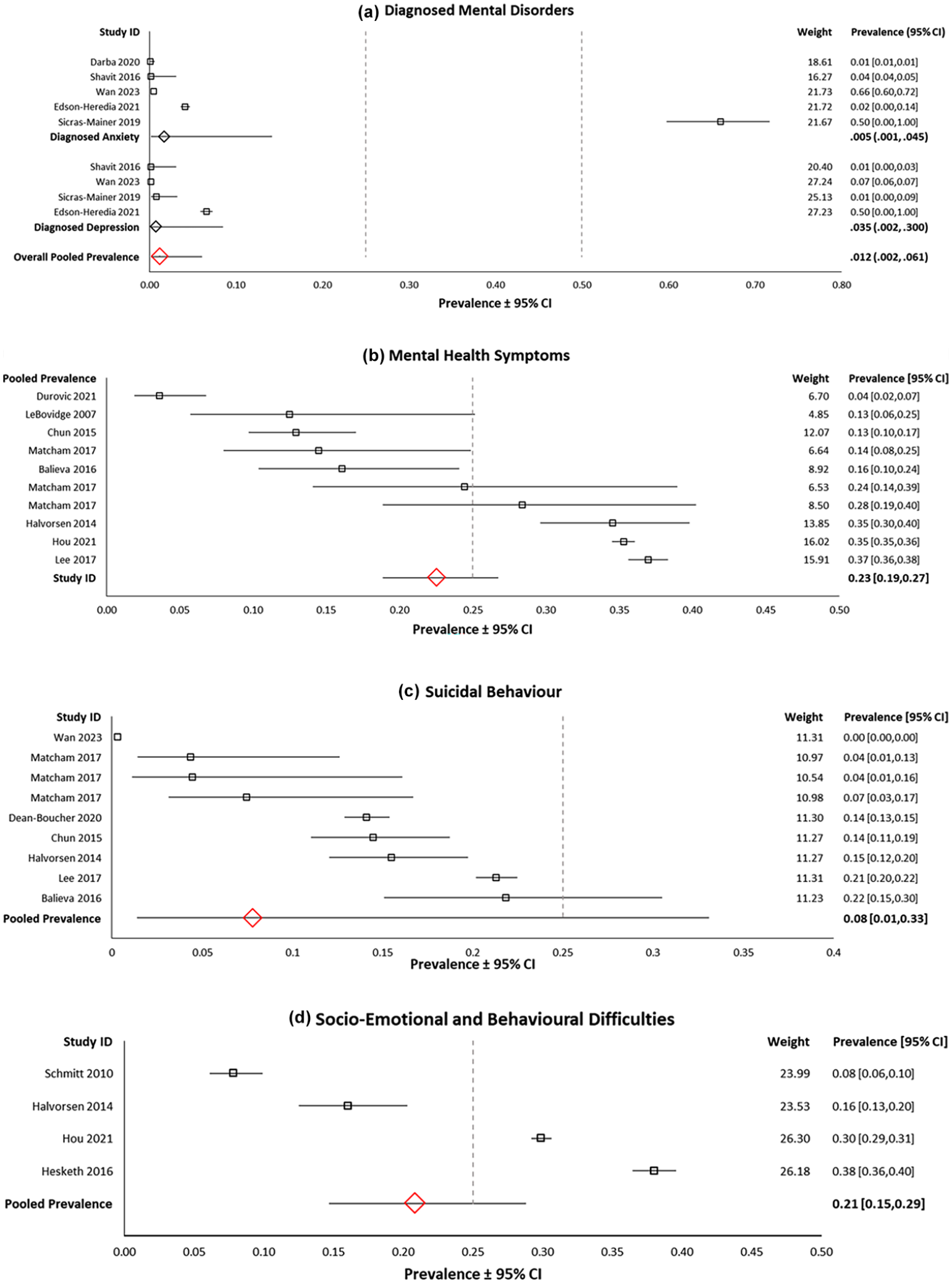
Forest plots of the prevalence of (a) diagnosed mental disorders; (b) mental health symptoms; (c) suicidal behaviour; and (d) socio-emotional and behavioural difficulties. Random effects analysis.
Diagnosed mental disorders
Five studies were included in the meta-analysis for the pooled prevalence of diagnosed mental disorders. The prevalence across eight unique populations (n = 416,543) was 1.2% (95% CI = 0.2–6.1; Q = 1.352; tau2 = 2.80; I2 = 99.9, p < 0.001). Sub-analysis revealed the pooled prevalence of diagnosed anxiety was 0.5% (95% CI = 0.1–4.5) and 3.5% for diagnosed depression (95% CI = 0.3 30.0). However, meta-regression found that the type of disorder (anxiety, depression) did not explain significant variance in the outcome (p = 0.245). Similarly, meta-regression found that the type of CSC did not explain significant variance in the outcome (p = 0.128). Sub-analysis by type of CSC was not appropriate as there were not enough studies for each CSC (see S2).
Mental health symptoms
Eight studies were included in the meta-analysis for the pooled prevalence of mental health symptoms. The prevalence across 10 unique populations (n = 27,462) was 22.6% (95% CI = 18.9–26.7; Q = 171.3; tau2 = .08; I2 = 94.8, p < 0.001). Sub-analysis found the pooled prevalence of anxiety symptoms was 23.1% (95% CI = 11.4–41.2; I2 = 87.3). Meta-regression found that the type of mental health symptoms did not explain significant variance in the outcome (p = 0.627). However, type of CSC did explain significant variance in the outcome (Q = 41.11, df = 5, p < 0.001; R² = 0.50). The pooled prevalence of AD was 27.8% (95% CI = 23.3–32.9). Unfortunately, sub-analysis for other types of CSCs was not appropriate as there were too few studies (see S2).
Suicidal behaviour
Eight studies were included in the meta-analysis for the pooled prevalence of suicidal behaviour. The prevalence across eleven unique populations (n = 418,274) was 7.8% (95% CI = 1.4–3.1; Q = 11,439.30; tau2 = 7.21; I2 = 99.9, p < 0.001). Meta-regression showed that the type of CSC did not explain significant variance in the outcome (p = 0.985). Sub-analysis was not appropriate due to too few studies for each CSC (see S2).
Socio-emotional and behavioural difficulties
Four studies were included in the meta-analysis for the pooled prevalence of socio-emotional and behavioural difficulties. The prevalence across four unique populations (n = 20,633) was 20.9% (95% CI = 14.7–28.8; Q = 282.1; tau2 = .18; I2 = 98.9, p < 0.001).
Publication bias
Funnel plots comparing the logit of the prevalence with the estimate standard error are depicted in imputed studies to assess publication bias, and Rank Correlation Test and Egger’s Linear Regression Method are presented for each outcome in the Supplemental Material (S3, S4).
Discussion
This is the first systematic review and meta-analysis to synthesise the prevalence of mental health difficulties in 0–25-year-olds with CSCs. Forty-five studies were included for narrative synthesis and 18 for meta-analyses. Findings indicated variability in the prevalence of mental health difficulties. CSCs often occur in cycles of flare-ups and mental health fluctuates throughout peoples’ lives. Thus, the prevalence of mental health difficulties in youth with CSCs may vary across the included studies, countries and developmental stages.
The pooled prevalence of diagnosed mental disorders was 1.2%. Sub-analyses showed the pooled prevalence of anxiety (0.5%) and depression (3.5%). Research demonstrated the prevalence of anxiety (5.2%), depression (1.3%) and any mental disorders (12.4%) in <18-year-olds without a reported chronic physical illness (Barican et al., 2022). Cree et al. (2018) reported that 17.4% of 2–8-year-old children in the U.S. had a diagnosed mental, behavioural or developmental disorder. Although our figure appears low, we did not include attention-deficit/hyperactivity disorder or autism spectrum disorders because we considered them developmental disorders of childhood, and not mental health disorders. Estimates in the general population appear higher in the literature than our estimate suggests. In a general adolescent population, major depressive disorder varied from 0.2% to 17%, with a median estimate of 4% (Costello et al., 2004). Our estimate appears low especially given it includes anxiety and depression. Dermatology patients may resist psychiatric referral (Jafferany, 2007; Koo and Lebwohl, 2001), likely contributing to our lower estimate. Patients may resist referral because they are not aware of, or do not accept, their mental health difficulties. If they are attending their dermatologist to treat their skin condition, they may not feel prepared to consider the need for psychological treatment. Singh et al. (2017) explored reactions to psychiatric referral in patients ⩾14-years-old presenting with physical complaints. Over one-third of patients refused to consider the possibility their symptoms were related to psychiatric illness and maintained they had a ‘physical’ basis. This study included patients who presented to a psychiatric outpatient department, that is, they had not resisted the referral. Given the high prevalence of these beliefs in people who had not resisted referral, it is plausible to consider that among those who did resist, such beliefs are even more salient. Furthermore, dermatologists across Europe often under-recognise mental health symptomology in patients (Dalgard et al., 2018). Clinicians may consider mental health symptoms, like low mood, as symptoms of the CSC being treating and not an indication of a mental health problem. Therefore, patients may not be referred for psychological screening.
The pooled prevalence of mental health symptoms was 22.6%. A 13-country-wide study reported that 17.2% of adult dermatological patients had anxiety symptoms and 10.1% depressive symptoms (Dalgard et al., 2015). Our higher ratio of mental health symptoms could be due to the highly visible nature of many CSCs. The recurrent, long-term nature of CSCs could make patients vulnerable to adverse, negative emotions, particularly during developmental stages when physical appearance is deemed important, like adolescence.
We observed a large difference between the pooled prevalence of diagnosed mental disorders and mental health symptoms (1.2% vs 22.6%). It is expected that diagnosed mental disorders are less common than broader symptoms or true diagnostic-levels of mental disorders in the population. Obstacles to accessing mental health care include fear of stigmatisation or scarcity of financial support (Muhorakeye and Biracyaza, 2021). The pooled prevalence of suicidal behaviour was 14.5%, which is comparable to existing evidence reporting suicidal ideation in 12.5% of adults with dermatological conditions (Dalgard et al., 2015). A study of psoriasis patients observed that 9.7% reported a ‘wish to be dead’, and 5.5% reported active suicidal ideation (Gupta and Gupta, 2000). Adolescents experience stress from school or family, lack of emotional support and poor academic performance (Deng et al., 2022). Young adults experience problems including financial instability, relationship issues and uncertainty about their future (하정희 and Hee, 2008). The higher prevalence we observed could suggest that CSCs add strain during challenging developmental periods.
The type of CSC explained significant heterogeneity in the meta-analysis of mental health symptoms. The pooled prevalence of mental health symptoms was 27.8% in AD patients, which appears high. A study of children with AD reported that 71% had additional atopy (asthma/allergic rhinitis) (Kapoor et al., 2008). It is plausible that children with AD may be dealing with increased disease burden going beyond the skin.
Implications
CSCs in youth can have varied but serious mental health consequences. Clinicians should be equipped to screen for mental health difficulties in clinical practice. Introducing psychological assessment into dermatology settings could identify and treat problems early, resulting in better outcomes. We observed a low prevalence of diagnosed mental disorders (1.2%) suggesting that dermatologists should be trained to recognise mental health symptomatology in young patients and have clear referral pathways in place. Early intervention for mental health difficulties is important in younger patient cohorts, given they are already in developmentally vulnerable periods.
Many CSCs are psychosomatic and are aggravated by mental factors (Gieler et al., 2020). This is bidirectional. It is biologically plausible that psychological distress exacerbates and even precipitates CSCs (Chida et al., 2008; Koo and Lebwohl, 2001). Gupta and Gupta (2003) suggest that dermatology patients be assessed with a biopsychosocial approach, similar to a multidisciplinary, psychodermatology approach. Consideration of developmental context is important as the impact of visible CSCs are often larger during adolescence and young adulthood, than in later adulthood (Gupta and Gupta, 1995). Because stress can exacerbate CSCs (Kimyai-Asadi and Usman, 2001) physicians should consider the psychophysiological aspects of the conditions being treated, particularly in younger patients. For example, managing emotional stress through dermatological treatments for the CSC itself to minimise disease-related stress, in addition to stress management techniques in individual or group settings (Gupta and Gupta, 2003).
Limitations
Future reviews could include studies published in other languages. The meta-analyses showed high heterogeneity between studies. This is a trend in prevalence meta-analyses, with the literature consistently demonstrating high I2 values (Migliavaca et al., 2022). Migliavaca et al. (2020a) assessed characteristics of prevalence meta-analyses. The median I2 value was 96.9%. Although this is not common in meta-analyses of other data types, it is in meta-analyses of prevalence. Prevalence naturally varies over time, location and patient subgroups; therefore, heterogeneity is expected across prevalence studies. Due to the nature of non-comparative, proportional data, more diverse point estimates are observed among studies than for comparative measures (Migliavaca et al., 2022). Although heterogeneity investigations showed potential explanatory factors, findings should nonetheless be interpreted with caution.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241252216 – Supplemental material for The prevalence of comorbid mental health difficulties in young people with chronic skin conditions: A systematic review and meta-analysis
Supplemental material, sj-docx-1-hpq-10.1177_13591053241252216 for The prevalence of comorbid mental health difficulties in young people with chronic skin conditions: A systematic review and meta-analysis by Clodagh Flinn, Amy McInerney and Finiki Nearchou in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank Dr. Marta Bustillo, the Liaison Librarian for the Social Sciences at the University College Dublin Library, for her help and support in designing our search strings for specific database searches at the beginning of the review process. We would also like to thank the numerous authors and researchers who provided us with further information about their studies during the review process.
Data sharing statement
The data that support the findings of this study are available from the corresponding author, Ms. Flinn, upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ad Astra Fellowship at University College Dublin.
Ethics approval
Ethical approval was not required for this systematic review and meta-analysis.
Informed consent
Informed consent was not required for this systematic review and meta-analysis.
Pre-registration
This systematic review and meta-analysis was pre-registered on the International prospective register of systematic reviews (ID: CRD42021258813).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.