
Abstract
We tested the potential for recommender system technology to provide personalized physical activity (PA) suggestions for inactive young adults with high bodyweight. We developed a recommender system using data from the 2017 Behavioral Risk Factor Surveillance System and assessed interest in using the system among 47 young adults (mean age = 23.0 years; 63.4% female; 65.0% White; mean BMI = 29.4). Eleven of these participants (mean age = 23.6 years; 90.9% female, 63.6% White; average BMI = 28.5) also received a PA recommendation and a follow-up interview. Approximately half of the survey participants were willing to use the recommender system, and participants interested in the recommender system differed from those unwilling to try the system (e.g., more likely to be female, worse self-perceived health). Furthermore, eight of the 11 interviewees tried the PA recommended to them, but had mixed reviews of the system’s accuracy. Although our recommender system requires improvements, such systems have promise for supporting PA adoption.
Physical activity (PA) is an important contributor to health and well-being (Biddle et al., 2021), and PA adoption in young adulthood can contribute to life-long health (Nelson et al., 2008), but many people, including young adults, do not meet PA guidelines (Bevington et al., 2020; Nelson et al., 2008; Rhodes et al., 2017). Much attention has been focused on increasing the PA of individuals with higher bodyweight (e.g., Lee et al., 2023). However, interventions for PA adoption and maintenance often focus more on cognition and behavior (Howlett et al., 2019), and fail to examine affective experience despite the importance of activity enjoyment for PA maintenance (e.g., Ekkekakis et al., 2010). Active lifestyles are more likely when people enjoy their PA (Ramer et al., 2021) and dislike of exercise is a known barrier to PA (Leone and Ward, 2013), especially for individuals with high bodyweight (Ekkekakis et al., 2010).
Building on Kimiecik et al.'s (2020) recommendation to focus on people rather than behavior, we suggest that a personalized medicine approach, using information about individuals’ unique characteristics to predict disease risk and develop tailored treatment plans (Chan and Ginsburg, 2011), may be beneficial to help people find activities they enjoy. Barriers and facilitators to PA, as well as activity enjoyment, may be unique, making individualized treatment approaches helpful for PA adoption. However, research is needed to develop an effective personalized approach for PA recommendations.
Literature Review
Barriers and facilitators to PA uptake and adoption
People are constrained from engaging in leisure-time PA for many reasons, including factors at the intrapersonal, interpersonal, and structural levels (Crawford et al., 1991), and constraints can affect enjoyment of PA (Kono and Ito, 2023). Negative experiences of PA are also intrapersonal barriers to PA adoption and maintenance (Leone and Ward, 2013; Rhodes et al., 2017). Currently inactive or sedentary people are unlikely to be motivated to change their behavior if their expectation is that they will have an unpleasant experience with PA (e.g., Calder et al., 2020). Furthermore, people with high bodyweight often face interpersonal and structural constraints related to discrimination, weight stigma, and lack of size-appropriate resources in PA contexts (e.g., Pearl et al., 2021). In addition, PA opportunities change with the end of high school (e.g., discontinuation of school physical education, aging out of youth sports; Nelson et al., 2008) so lack of knowledge of enjoyable, locally-available PA may be a constraint contributing to young adult inactivity. It is therefore especially important to help currently inactive, high bodyweight young adults find PA contexts they enjoy, which may help motivate negotiation of constraints.
Unfortunately, few effective interventions exist to facilitate PA uptake and adoption (Rhodes et al., 2017). PA adoption research has emphasized factors such as motivation, intentions, self-efficacy, etc., drawing on theories such as the COM-B (Capability, Opportunity, Motivation, Behavior) framework (Michie et al., 2011), while acknowledging that these factors are influenced by environmental factors such as local resources and social supports (Nigg et al., 2008). Receiving personalized recommendations for PA aligns with the “opportunity” and “motivation” aspects of this model by increasing awareness of activities that are likely to be enjoyable and therefore motivating (e.g., Ekkekakis et al., 2010), and with the “capability” aspect via the usage of data from similar peers to drive recommendations (e.g., Kim et al., 2021). This approach is similar to, but distinct from, physician recommendations for general increases in PA, which have not been widely effective (Williams et al., 2007), potentially because these interventions rely on people being able to seek out new PA on their own. Similarly, the U.S. Department of Health and Human Services’ “Move Your Way” campaign encourages doing enjoyable activities but does not help people identify forms of PA they might enjoy (Bevington et al., 2020). Research on preferences for PA suggest that PA is not a one-size-fits-all activity (e.g., Barnett, 2006) so intervention efforts should focus more on PA experiences (Kimiecik et al., 2020; Kono and Ito, 2023) so that each person can find a type of PA that satisfies their needs (Ryan and Deci, 2000) and is personally enjoyable (Lewis et al., 2015). A personalized approach that allows individuals to receive customized suggestions for PA they are likely to enjoy could therefore be a valuable addition to current PA promotion efforts.
Personalized medicine is widely used in healthcare settings (e.g., Vakili et al., 2023), and similarly customized approaches to PA interventions are needed. Existing personalized PA interventions (e.g., the MyBehavior app, Rabbi et al., 2018) only provide feedback based on users’ existing PA behavior (i.e. the explore/exploit algorithm does not draw on activities known to be unfamiliar). These methods do not allow insufficiently active users to find new types of activity, the way that recommender system technology can. Algorithm-based recommender systems that predict consumer preferences using data from similar consumers are increasingly common (Raeesi Vanani et al., 2022). American adults trust these systems, as evidenced by the fact that they drive 75% of the programs watched on Netflix (MacKenzie et al., 2013). Existing recommender systems employ specific algorithms and techniques, such as collaborative filtering (Su and Khoshgoftaar, 2009) and deep learning approaches (Zhang et al., 2020), to predict users’ ratings or preferences for target items, by simultaneously analyzing item and user data including explicit feedback (ratings, reviews) and implicit feedback (clicks, purchase history, browsing behavior). The use of such recommender systems for PA promotion aligns well with motivational and leisure theories relevant to PA uptake and adoption. For example, receiving recommendations based on data from oneself and similar peers may increase positive outcome expectations, which are associated with increased PA (Kim et al., 2021). A recommender system can also facilitate the negotiation of structural constraints such as lack of knowledge of possible activities (Crawford et al., 1991; Hubbard and Mannell, 2001). Thus, by customizing PA recommendations (Bevington et al., 2020), and building in peer norms (Kim et al., 2021), a recommender system for PA adoption fills a gap in the existing intervention landscape.
The present study
This pilot study tested the use of recommender system technology for engaging currently inactive young adults with a high body mass index (BMI > 25) in PA. We focused on this population because dislike of exercise is a known barrier to PA (Leone and Ward, 2013), especially for individuals with high bodyweight (Ekkekakis et al., 2010), and our recommender system is specifically designed to help individuals find new types of PA that they might enjoy. Our research questions were:
Are inactive young adults with a BMI > 25 willing to engage with the recommender system? If so, are there characteristics that differentiate the people interested in using it from those who are not interested?
Can the recommender system help interested participants find a new type of PA that they enjoy? and
To what extent do participants who try it feel that the recommender system is useful?
Importantly this pilot study was not designed to test the effectiveness of the recommender system when mandated to uninterested users. Instead, we sought to test the system’s potential to help interested users find new types of PA to enjoy in their community. As such, we limited our sample in the system-testing phase to survey respondents who expressed interest in receiving a recommendation and we limited the possible activities recommended to activities in which it is possible to participate in the community where the research took place.
Methods
We developed a prototype recommender system to suggest new types of PA to inactive people based on the preferences of other people who share many of their characteristics (Phase 1). We then conducted a survey (Phase 2) and pilot intervention study (Phase 3) to assess whether the recommender system could provide personalized PA recommendations that were appealing to inactive young adults with high bodyweight. Specifically, our mixed methods approach involved the use of a survey to answer Research Question 1, and an intervention and qualitative interview with a sub-sample of survey respondents to answer Research Questions 2 and 3. Figure 1 illustrates these procedures, including the sample sizes and number excluded in each phase.
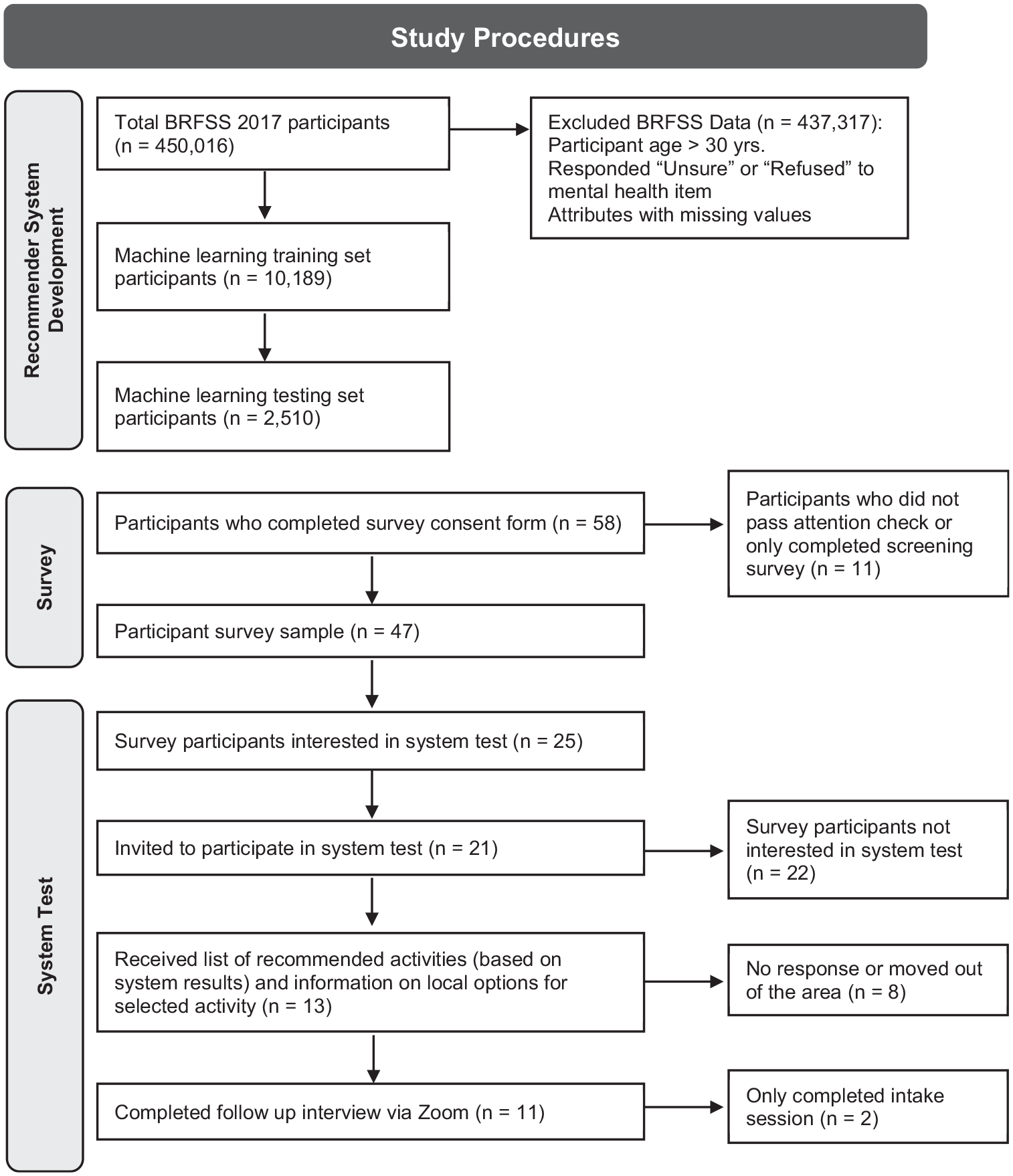
Study procedures and number of participants included in each phase. We used secondary data to establish the recommender system, then conducted a survey to assess interest in having recommendations made among members of the target demographic, and recruited our system test sub-sample from the survey participants who indicated their interest on the survey. This final sub-sample was given the opportunity to try system-suggested activities and was interviewed about their experience with using the recommender system to help them engage in PA.
Phase 1 (recommender system development)
Procedure: Our recommender system used data from the 2017 Behavioral Risk Factor Surveillance System (BRFSS; Centers for Disease Control and Prevention, 2017), which includes 450,016 participants associated with 358 attributes/columns. We selected 27 attributes to examine (see Supplemental material, Table S1), focusing on factors likely to be related to PA behavior, excluding factors more relevant for older adult populations (e.g., arthritis burden) and factors without a clear theoretical link to PA (e.g., seatbelt use). We also included variables indicating whether, how often, and how intensely participants engage in PA, and data about their first and second most common form of PA, including their estimated intensity, frequency, and duration. These variables (demographics, health items, and most-common PA type) were used to train a recommender system to predict the second reported PA type. We included most common PA type as a predictor rather than an output in the recommender system because our goal was to generate new suggestions for PA based not only on demographics but also on PA behavior and preferences. Dummy variables were used for categorical variables, and we used the sklearn package (Pedregosa et al., 2011) to implement machine learning models and the fit() function to train models.
Participants: As our project focused on recommending PA for young adults, we filtered out the participants with age above 30. To train an accurate recommender system, we subsequentially filtered out participants with extreme values, that is, 99 (Refused) or 77 (Don’t know/Not sure) in the attribute “Number of Days Mental Health Not Good.” This resulted in a data set with 12,699 participants. We randomly divided the data into a training set (N = 10,189) used to train the machine learning model and a testing set (N = 2,510) to evaluate model performance.
Measures: We used demographic and health items from the BRFSS (Centers for Disease Control and Prevention, 2017) to inform our recommender system. These items included age (open-ended), gender (male, female, nonbinary); sex at birth (male, female, don’t know); race (White, Black or African American, American Indian or Alaska Native, Asian Pacific Islander, Middle Eastern or North African, Other); ethnicity (yes/no Hispanic, Latino/a, or Spanish origin); educational attainment (highest grade completed; response options ranging from 1 = Never attended school or only attended kindergarten to 7 = At least some graduate or professional school); status as a student, a parent, or a member of the military (yes/no); marital status (six options, including Married, Divorced, and Member of an unmarried couple); employment status (eight options including Employed for wages, Homemaker, and Unable to work); household income (response options ranging from 1 = Less than $10,000 to 9 = More than $100,000); cigarette and alcohol use (multiple items assessing frequency and duration of use), self-perceived physical and mental health (number of days in the past 30 days that health was “not good”); and PA (multiple items assessing frequency and duration).
Phase 2 (survey)
Procedure: After approval from the Institutional Review Board (STUDY00014707), our online survey was advertised through listserv emails, flyers posted in public spaces, and direct mail sent to local residents in the target age group.
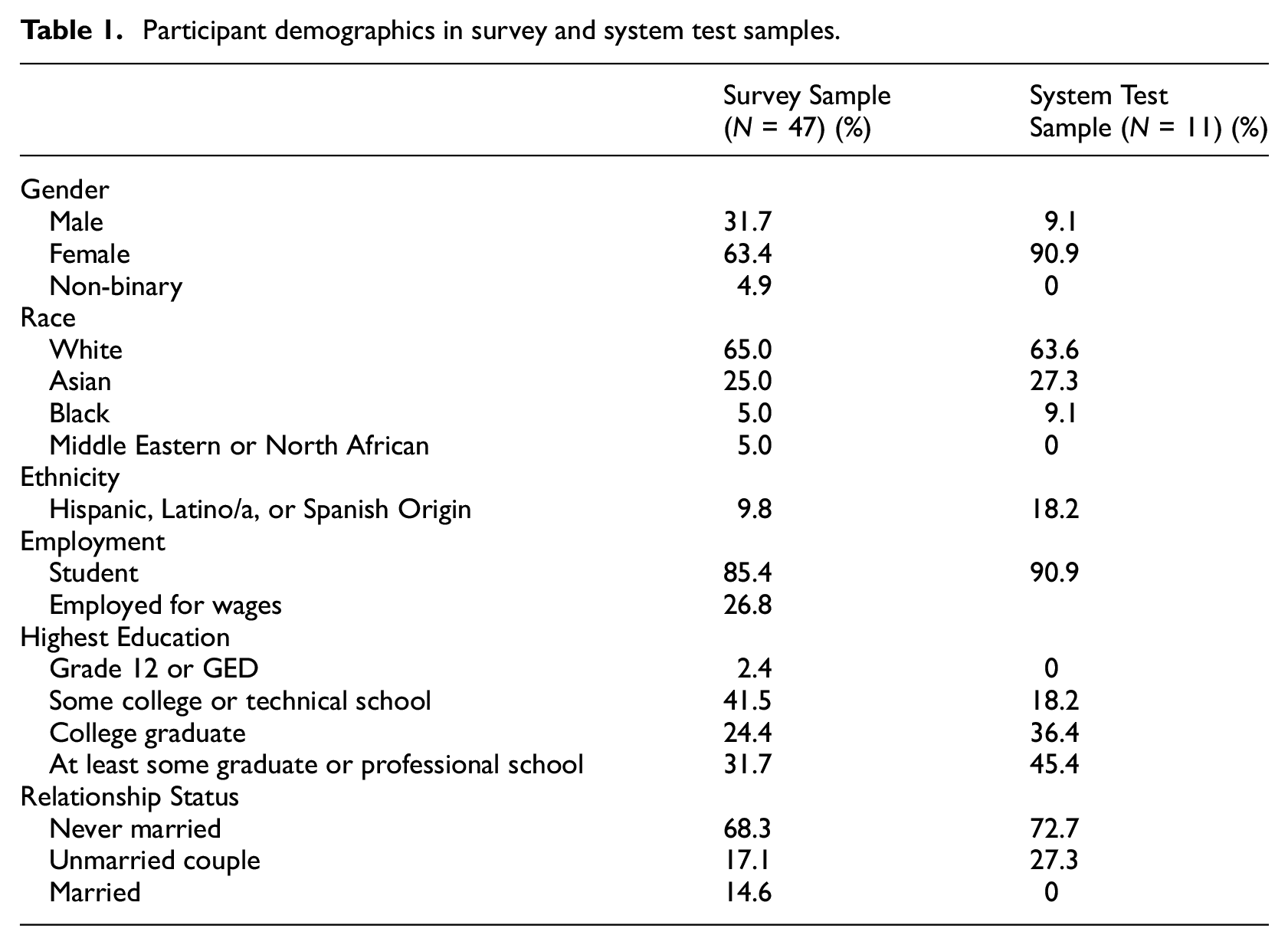
Participants: Survey participants were 47 young adults (mean age = 23.0 years, SD = 3.29, range 18–29) living in a college town in the northeastern United States. Demographic information is provided in Table 1 (six participants did not provide demographic information). No participants reported having biological children or engaging in active-duty military service. Participants’ average BMI was 29.4 (SD = 4.7, range 25.0–44.3) and 57.4% reported engaging in recreational PA.
Participant demographics in survey and system test samples.
Measures: Survey participants answered demographic questions drawn from the BRFSS to enable them to be matched with activities using the recommender system, including items about their PA (e.g., “What type of physical activity or exercise did you spend the most time doing during the past month?”). In addition, our survey included 24 leisure constraints items and 23 leisure constraint negotiation items drawn from Hubbard and Mannell (2001). Items were rated on a Likert scale from 1 = strongly disagree to 5 = strongly agree. Sample constraints items include “I’m not comfortable participating in physical activities” (intrapersonal), “The people I know usually have too many other obligations to participate in physical activity with me” (interpersonal), and “I would do a physical activity if I know what is available” (structural). Sample negotiation items include “I try to improve my skills” (intrapersonal), “I try to find people to do physical activities with” (interpersonal), and “I try to find out about low-cost physical activities” (structural). Cronbach’s alpha for constraints in our survey was 0.697, which is low but corresponds with the heterogeneity of the subscale items. Cronbach’s alpha for negotiation in our survey was 0.781. Finally, all survey participants were asked to indicate their willingness to receive a recommendation for a new type of PA and to be interviewed about the experience.
Phase 3 (system test)
Procedure: Participants who indicated on the survey that they were interested in trying an activity recommended for them were contacted and invited to participate in the system test in the order that they took the survey, with the goal of recruiting 6 male and 6 female participants for the final system testing phase of the study. Participants in the final phase of the study met virtually with a member of the research team via Zoom. In this meeting, they were told, “We have built an algorithm-based computer recommender system to identify physical activities that people might like based on the other activities they have previously tried. It’s similar to how Netflix or Amazon.com can predict what shows or products you might like based on the other things you have looked at in the past. We entered the data from your survey into our recommender system to find out what types of physical activity it thinks you are most likely to enjoy.” After answering any questions about the procedure, the researcher told the participant the top five activities that the recommender system suggested they should try based on their survey data, and asked which one of these activities they were most interested in trying. Participants were informed of a location in the local community where they could try their selected activity and were told that the research team would cover the cost of up to three visits to that activity provider within the next 2 weeks. Arrangements for payment were made with all activity providers prior to the enrollment of participants in the study. At the conclusion of the Zoom call, participants were asked to schedule a follow-up interview in 2 weeks about their experiences in the study regardless of whether or not they tried their selected form of PA. Interviews were also conducted via Zoom and were audio and video recorded to generate transcripts for analysis. These interviews followed a semi-structured interview guide including questions about general attitude toward PA, things that make regular PA difficult for them, their thoughts about our recommender system and its suggestions for them, and their experiences if they tried a recommended activity.
Participants: Eleven individuals (mean age = 23.6 years, SD = 2.38, range 21–28) participated in the system test, receiving a PA recommendation and completing a follow-up qualitative interview. Although we sought to recruit a diverse sample, participants who expressed interest in the system test (N = 25) on the survey were 76% female and 44% White. Demographics for the interview sample are provided in Table 1. Interviewees’ average BMI was 28.5 (SD = 3.9, range 25.1–38.3), and four (36.4%) reported engaging in recreational PA.
Results
Recommender system development
We assessed the top-5 accuracy of our recommender system using several different machine learning approaches (Krizhevsky et al., 2017), including logistic regression (Cox, 1958; test set accuracy 0.69), decision tree (Quinlan, 2014; test set accuracy 0.30), naïve Bayes (Mitchell, 1997; test set accuracy 0.07), SVM (Cortes and Vapnik, 1995; test set accuracy 0.66), AdaBoost (Freund and Schapire, 1997; test set accuracy 0.71), and a 5-layer deep neural network (Goodfellow et al., 2016; test set accuracy 0.67) for recommending PA types. Following reviewer recommendations, we also tested XGBoost (test set accuracy 0.68) and random forest (test set accuracy 0.68) methods. As neither outperformed AdaBoost, we retained our original approach. Top 5 accuracy treats the prediction as correct if the ground truth activity exists within the top five recommended activities. Table 2 provides a demonstration of the system’s predictions within the BRFSS testing set.
Example of recommender system output featuring two randomly selected young adult (age 18–29) BRFSS participants with a BMI > 25 who shared the same first reported PA type (weightlifting).
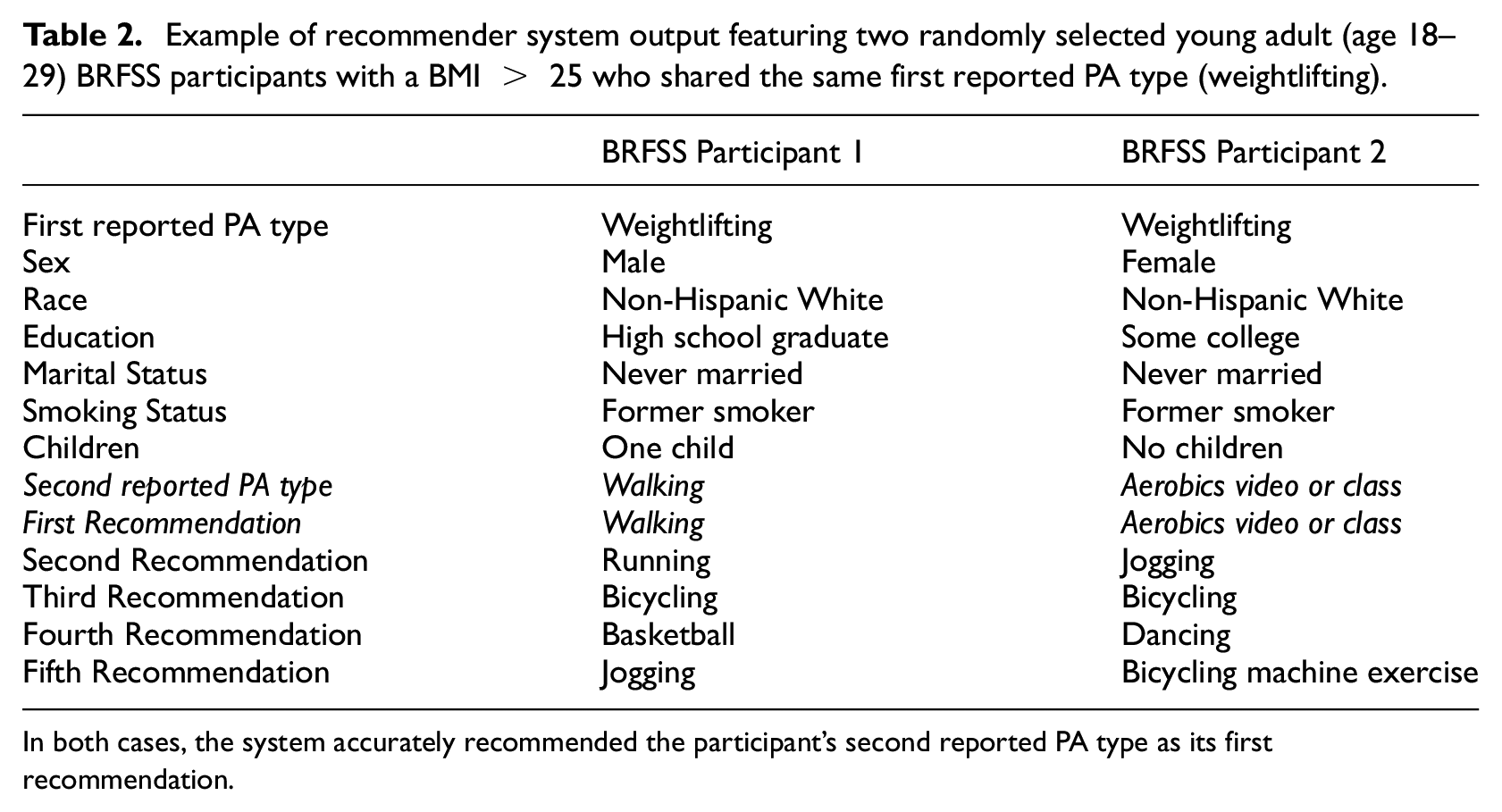
In both cases, the system accurately recommended the participant's second reported PA type as its first recommendation.
Research question 1: Are inactive young adults willing to engage with the recommender system? If so, what are the characteristics of the people interested in using it?
Of the 46 young adults who answered this question on our survey, 53% indicated willingness to participate in PA recommended by our system and be interviewed about their experience. We included a wide range of demographic and health variables in our survey to improve the accuracy of the recommender system (see Measures), and we used multivariate analysis of variance (ANOVA) to examine whether willingness to try to recommender system differed across any of the included demographic and health variables. Results indicated that participants who were willing to try the recommender system reported worse self-perceived health (mean = 3.05 vs 3.44; F(1,38) = 4.470, p = 0.041, eta squared = 0.105), fewer days of physical health being not good (mean = 3.45 vs 8.11; F(1,38) = 5.013, p = 0.031, eta squared = 0.117), less likely male gender (X 2(1, N = 40) =10.58, p = 0.005; eta squared = 0.178), less likely male sex at birth (X 2(1, N = 40) =10.18, p = 0.001; eta squared = 0.254), and higher educational attainment (mean = 6.23 vs 5.88; F(1,38) = 8.763, p = 0.005, eta squared = 0.187). Table 1 shows the demographics of the system test sample in relation to the full survey sample.
We also assessed survey participants’ constraints to PA and their negotiation of constraints, and examined whether willingness to try the recommender system differed across these variables. ANOVA results indicated that participants willing to try to the recommender system had lower scores on the structural subscale of the leisure constraints measure (mean = 2.47 vs 3.03; F(1,41) = 8.88, p = 0.005; eta squared = 0.178) and higher scores on use of skill-related negotiation strategies (mean = 3.06 vs 2.69; F(1,41) = 5.57, p = 0.023; eta squared = 0.120) than participants not willing to try the recommender system.
Research question 2: Can the recommender system help participants find a new type of physical activity that they enjoy?
Of the 11 interviewees, 73% participated at least once in a type of PA that was recommended to them. Of these, some mentioned logistical challenges to participation, including finding time and transportation, but nevertheless reported having good experiences. For example, Participant 199 said, “Yes, um I actually, I didn’t go to the YMCA, though, because I realized that there was a, as part of my apartment complex, they have a little gym thing. I had forgotten about it… But it was just closer and it was pretty empty, so I ended up going with that to do it. But I had a good experience with it.” Only three participants did not try a recommended form of PA. This group was exemplified by Participant 399, who said “I didn’t go. I had it in my mind and every single day, I was like ‘okay I’m going to go tomorrow,’ but then like… I kept like postponing it and postponing it and, you know.” Given that our participants also had their activities paid for as part of the study, these results highlight the need for additional structural or logistical support for PA engagement in addition to receiving PA recommendations.
However, most participants (N = 7) had mixed reviews of the accuracy of the system’s recommendations, such as Participant 206 who said, “I think the dance one was really accurate, the running thing is the furthest thing from what I like.” Only three interviewees described the majority of the suggested forms of PA as things they would like to do, and one described having exactly the type of experience we were hoping the recommender system could provide: Participant 46 said, “I went back a second time. Because I had a really good time, the first class.” In sum, although our interview data suggest that it is possible for a recommender system to help participants find a new type of PA that they enjoy, our specific system still needs considerable refinement in its algorithm to make better suggestions.
Research question 3: Do participants feel the recommender system is useful?
Despite their mixed reviews of the accuracy of the recommender system, most participants (N = 8) described the system as useful. For example, four participants described the system’s provision of its top five recommendations as giving them a sense of direction or motivation, including Participant 199, who said, “I think having one specific activity in mind really helps make it a lot less daunting… there are about a million things on earth I could do, so it was really, it was nice to have kind of a short list to pick over.” Only three participants did not find the system useful, and two of these participants thought it could be useful for others. For example, Participant 154 said, “I’m not really sure if it could help get me interested… [but] I think it might be helpful for people who really want to start a new activity. Trying to find out the options, if you’re not sure where to start then I think this recommender system will give you some insights on what might be someplace to start.” In sum, and in keeping with our expectations, participants viewed the value of the recommender system not as a way to get participants motivated to engage in PA but rather as a way to direct their interest if they were feeling overwhelmed by choice or uncertain of their direction.
However, participants also described several constraints that were not addressed by the recommender system. Intrapersonal constraints were mentioned in all 11 interviews, such as Participant 324, who said, “I am very lazy. So my general attitude towards physical activity is like I probably should do it for like oh it’s kind of like it’s so much easier to sit on the couch than it is to go walk for a mile.” Participants were also constrained by self-consciousness around lack of skill or body size, and by past injuries or current conditions leading to a fear of getting hurt. About half of the participants (N = 6) also mentioned interpersonal constraints such as concerns about others’ perceptions of them (“I get really anxious about being in front of people doing it,” Participant 46) and lack of social support for PA (“If I’m by myself then [I] can just make excuses and there’s nobody to get behind you or keep you accountable,” Participant 154).
Structural constraints were also mentioned by all 11 interviewees, including not having time, the weather, and activities not being offered when they were available. For example, Participant 324 said, “I don’t get out of work until six and those weekday ones are, like for Zumba, were at like 6:15 or and I just want to be able to get there in time.” Participant 154 also provided an insightful perspective on the difficulty of distinguishing what the real constraint is at the root of non-participation: “I guess I am… lazy to get things going, so then I just, I think I put blame on all things like weather, saying that it’s cold or I have stuff to do, when I could have actually done this.” Based on this comment, it may be helpful to interpret participants’ self-perceptions of constraints with the understanding that these identified constraints are likely part of a larger system of both acknowledged and more subconscious constraints.
For a recommender system to be part of an effective intervention for engaging these participants in PA, it would therefore need to also help them overcome these constraints. Specific suggestions for ways to improve the system were provided by 10 participants, including adding social components (e.g., being able to share recommendations with friends), providing more information about the activities (e.g., when and where a person could participate in them locally, the extent to which the activity is beginner friendly, categorizing activities by factors like how much cardio they involve or how adventurous they are, etc.), and having clearer or more detailed questions on the input side to help participants provide accurate information about their interests and prior experiences. Study participants felt that features like these would help them overcome some of the constraints they faced using our existing recommender system.
Discussion
A considerable portion of the population remains inactive or sedentary (Bevington et al., 2020; Rhodes et al., 2017), despite many existing theories and interventions for PA adoption and maintenance. One missing link may be that little is known about how to help an individual select a type of PA that they are likely to enjoy. Enjoyment of PA is an important contributor to adoption of and persistence in active lifestyles (Leone and Ward, 2013; Ramer et al., 2021), and may help currently inactive individuals overcome their various constraints to PA (Crawford et al., 1991). Given that dislike of exercise is a particular barrier to PA for individuals with high bodyweight (Ekkekakis et al., 2010), a personalized medicine approach that matches people with personally-curated suggestions for PA may be a promising direction.
As an initial step toward such an approach, we developed a recommender system to predict individuals’ PA preferences based on the preferences of similar others. Such recommender systems are increasingly common in modern life (Linden et al., 2003; Mild and Reutterer, 2003), and are trusted by consumers for a wide variety of purchasing and leisure decisions (e.g., online shopping, Netflix viewing; MacKenzie et al., 2013). Based on our system’s success in the secondary data testing set, we implemented a pilot intervention to understand the target population’s willingness to use the recommender system, perceptions of its effectiveness and utility, and potential ways it could be improved. Specifically, after developing our recommender system, this mixed method pilot study addressed three interrelated research questions: (1) Are inactive young adults with a high BMI (>25) willing to engage with the recommender system? If so, are there characteristics that differentiate the people interested in using it from those who are not interested? (2) Can the recommender system help interested participants find a new type of PA that they enjoy? and (3) To what extent do participants who try it feel that the recommender system is useful? Our findings suggest that this approach has the potential to be developed into an intervention to promote health-enhancing PA but it will require both improvements in recommendation accuracy and integration with other PA-adoption support strategies.
Regarding our first research question, results suggested that although half of the surveyed inactive high bodyweight young adults were interested in using our PA recommender system, there were systematic differences between willing and unwilling individuals. Specifically, males, individuals with better self-perceived health, and individuals with fewer years of education were less interested in trying the recommender system. These differences may reflect higher rates of weight-loss motivations for PA among female young adults compared to males (Jeffrey, 2013) and increased likelihood of PA among individuals with health-related motivations for PA (Ingledew and Markland, 2008). Differences in trust of science among individuals with different levels of education (Achterberg et al., 2017) may also affect participants’ interest in using an algorithm-based recommender system. Importantly, these results suggest that even if recommender system technology perfectly predicted enjoyable activities, the technology itself may not be appealing to everyone. Similarly, the fact that our system-test sample was predominantly female suggests that interest in this type of intervention may be gendered, aligning with prior observations of gender differences across different types of interventions in this population (Poobalan et al., 2010).
The second and third research questions were addressed in the system test portion of the study, which provided a subsample of interested survey participants with personalized recommendations and paid for up to three sessions of their choice of recommended PA if they chose to attend. With regard to the system’s accuracy, although most participants engaged in their selected form of PA at least once, and many reported enjoyable experiences, only three interviewees described the majority of the suggested forms of PA as things they would like to do. This finding suggest that although recommender system technology has the potential to help inactive individuals find types of PA they enjoy, overcoming the barriers of negative experiences and expectations (Calder et al., 2020; Leone and Ward, 2013; Rhodes et al., 2017), further refinement is needed in our recommender system. In addition, although participants noted the utility of the recommender system for themselves and for others, they also highlighted the need for support in overcoming other interpersonal and structural constraints (Crawford et al., 1991). This finding aligns with the COM-B framework (Michie et al., 2011), in that participants may not perceive opportunities to participate without additional structural/logistical support.
In sum, a customized approach to PA recommendation may be helpful because different people enjoy different types of PA (e.g., Barnett, 2006) and enjoyment is important for PA adoption and maintenance (Leone and Ward, 2013). However, the specific recommender system tested in this pilot study will need to be improved and integrated with existing theories that have been used to study PA adoption (e.g., Michie et al., 2011; Ryan and Deci, 2000) to effectively support PA among the target population.
Limitations and future directions
Although our recommender system was very effective in the BRFSS testing set, our pilot research indicated that the system requires revision to effectively recommend new types of PA to currently inactive individuals. It is possible that our use of most-common PA as an input variable and second-most common PA as the output variable in training the recommender system may also have affected its prediction accuracy when applied to new populations. Furthermore, a revised recommender system will need to be tested both at the level of prediction accuracy (i.e., can it accurately predict types of PA that new participants will enjoy?) and implementation feasibility (i.e., will people follow the recommendations and engage in the suggested type of PA?). Notably, our recommender system only helped participants overcome the intrapersonal constraint (Crawford et al., 1991) of lack of knowledge of enjoyable PA, and did not support them in negotiating other constraints such as limited time for PA. Expanding the recommender system to provide more options for engaging in the selected PA type (i.e., providing options for classes held at different locations and at different times of day) could improve implementation feasibility by helping participants overcome time constraints. Participants had several additional suggestions for improvements, such as adding social components (e.g., being able to share recommendations with friends), providing more information about the activities in the system itself (e.g., when and where a person could participate in them locally, the extent to which the activity is beginner friendly, categorizing activities by factors like how much cardio they involve or how adventurous they are, etc.), and having clearer or more detailed questions on the input side to help participants provide the most accurate information about their own interests and prior experiences. These suggestions should be incorporated in future interventions using recommender system technology.
In addition to these limitations of the recommender system as currently designed, we recognize the general limitations of a recommender system that does not explain what features make PA types more or less likely to appeal to particular individuals. Given that change in PA behavior is influenced by factors such as participants’ capability, opportunity, and motivation (Michie et al., 2011), satisfaction of basic psychological needs (Ryan and Deci, 2000) and personal enjoyment (Lewis et al., 2015), better understanding of the characteristics of both participants and PA contexts will be important. Such research should also include more diverse samples (e.g., more male participants, more racial and geographic diversity), and expand to individuals of different ages and those without a high BMI as increased PA is beneficial to all inactive individuals regardless of age and bodyweight (e.g., Coombs et al., 2015). Our study also eliminated some financial constraints by paying for participants to try their recommended type of PA, which does not provide a real-world test of PA uptake. In addition, our study design only enabled us to test the recommender system among individuals motivated to participate in PA (i.e., individuals who expressed interest in testing the system), and we acknowledge that our results were likely influenced by decisions we made during the research process (e.g., the variables selected, the recruitment process, etc.). In general, further research examining why different people prefer different types of PA, and integrating this information with prior research and theory related to motivations (e.g., Michie et al., 2011; Ryan and Deci, 2000), would both improve the design of future PA recommender systems and advance the field.
Conclusions
PA adoption in young adulthood can contribute to life-long health (Nelson et al., 2008) and is more likely if PA is experienced as enjoyable (Calder et al., 2020; Leone and Ward, 2013; Rhodes et al., 2017). However, enjoyment of specific types of PA has been shown to be person-specific (e.g., Barnett, 2006). We therefore developed a recommender system to help insufficiently active young adults with BMI > 25 select locally available PA that they are likely to enjoy. Results indicated that this type of system was appealing to many individuals in the target sample, although interest in using the system varied by gender, education, and self-perceived health. Participants in the system-test pilot study suggested that the accuracy of recommendations could be improved but described our system as potentially useful, especially if combined with additional supports to help participants overcome other leisure constraints (Crawford et al., 1991).
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241242541 – Supplemental material for Supporting physical activity adoption through recommender system technology: A pilot study
Supplemental material, sj-docx-1-hpq-10.1177_13591053241242541 for Supporting physical activity adoption through recommender system technology: A pilot study by Jennifer P Agans, Fenglong Ma, Serena Schade and Christopher Sciamanna in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank Kimia Shirzad and Steven Hanna for their assistance with data collection.
Author contributions
JPA conceived of the study with support from CS, and is the primary author of this manuscript. FM created the recommender system and assisted with writing the methods and results sections. SS assisted with data collection and contributed to writing the manuscript.
Data sharing statement
Data used in this study are available from the authors on request. Specifically, survey and interview data are available from the first author, and recommender system data are available from the second author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant to the first author by the Pennsylvania State University College of Health and Human Development.
Ethics approval
This study was approved by the Pennsylvania State University Institutional Review Board under protocol number STUDY00014707.
Informed consent
All participants provided consent prior to participation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.