
Abstract
To explore the moderating role of dyadic appraisal in the association between dyadic coping and diabetes management efficacy. Two hundred seventy six middle-aged and older couple pairs with one spouse who had diabetes were recruited from 14 community healthcare centers across Guangzhou. The moderating role of dyadic appraisal was investigated using the actor–partner interdependence moderation model. When both couples considered diabetes to be a shared condition, statistically-significant associations were found between patients’ negative (β = −22.7, p = 0.008) and neutral behaviors (β = 13.6, p = 0.017), plus spouses’ positive behaviors (β = 22.8, p = 0.009) on their own diabetes management efficacy, respectively (i.e. actor effects); as well as between spouses’ positive (β = 16.8, p = 0.028), negative (β = −28.5, p < 0.001), and neutral behaviors (β = 16.9, p = 0.006) on patient’s diabetes management efficacy (i.e. partner effects). Dyadic appraisal moderates the association between dyadic coping and diabetes management efficacy.
Self-efficacy and diabetes management
Diabetes mellitus is a chronic condition that arises when the body is unable to produce sufficient insulin or use the insulin it produces effectively, leading to elevated blood glucose levels (International Diabetes Federation, 2020). There is no cure for diabetes, but good diabetes management can keep a patient’s blood glucose in a normal range and reduce complications (International Diabetes Federation, 2020). Self-efficacy is a critical element in diabetes management (Ismail et al., 2004). As defined in the Social Cognitive Theory, self-efficacy is an individual’s confidence in their capabilities to conduct designated levels of performance (Bandura, 2004). In terms of diabetes management, self-efficacy has been shown to be positively associated with regular exercise, healthy diet, as well as adherence to medication, blood glucose monitoring, and foot care (Qin et al., 2020). By enhancing self-efficacy, better diabetes management outcomes, such as reduced hemoglobin levels and improved quality of life, can be expected (Jiang et al., 2019).
The relationship between dyadic coping and diabetes management efficacy
Nevertheless, the sole improvement in patient’s self-efficacy may not be sufficient. Given management activities are imbedded in the patient’s daily lives, the importance of the spouse in diabetes care cannot be overlooked (Martire and Helgeson, 2017). The Dyadic Model of Coping with Chronic Illness, a theory on spouses’ involvement in illness coping has been proposed to understand couples’ chronic illness co-management (Berg and Upchurch, 2007). The theory has two components: dyadic appraisal and dyadic coping. Dyadic appraisal refers to the couple’s evaluations of illness management responsibility, controllability, and consequences. Dyadic coping describes couple’s behaviors in management activities, ranging from uninvolved (the individual perceives that he or she is coping with the stressful event alone), collaboration (spouse is more actively involved in the stressful event through joint problem solving), support (spouse provides instrumental and/or emotional support), to control (spouse dominates the actions of the other person by taking charge and telling he or she what to do). These dyadic coping can be further grouped into positive behaviors (i.e. collaboration, emotional support, instrumental support), neutral behaviors (i.e. protective buffering), and negative behaviors (i.e. avoidance, overprotective, and critical behavior) given their perceived intention (Helgeson et al., 2019; Weitkamp et al., 2021). Collaboration entails the spouse’s active participation in discussions, information gathering, brainstorming solutions, and problem-solving (Coyne and Smith, 1991; Hagedoorn et al., 2000). Emotional support is understanding and validation, while instrumental support is assistance and advice (Helgeson et al., 2019). Protective buffering is to protect spouse from distress by concealing worries and acting as if nothing was wrong (Helgeson et al., 2019). Avoidance means avoiding discussions about diabetes and changing topic (Helgeson et al., 2019). Overprotection is a strategy where the spouse provides an excessive amount of help, often including a restriction of the patient’s activities, due to underestimating the patient’s abilities. Critical behavior means criticizing, arguing and nagging (Helgeson et al., 2019).
Understanding the relationship between dyadic coping and diabetes management efficacy can help to improve the efficacy of diabetes management by taking measures to improve the behaviors of couples when spouses are involved in the management of diabetes, thus achieving good diabetes management outcomes. Previous studies have verified the relationship between dyadic coping and diabetes management efficacy. Some evidence suggests that patients perceived high communal coping, namely considering diabetes as a shared problem and collaborating to solve it, had increased diabetes management efficacy (Van Vleet et al., 2019); whereas spousal overprotective behavior was related to patients’ low diabetes management efficacy (Beverly and Wray, 2010; Schokker et al., 2011). Johnson et al. reported that common dyadic coping was associated with higher levels of diabetes efficacy for both patients and spouses where one of the members had type 2 diabetes and that self-efficacy was a potential mediator of the positive effect of dyadic coping on dietary and exercise adherence for patients (Johnson et al., 2013). However, some common limitations of prior studies impede the understanding of these relationships. Despite positive and negative behaviors may coexist in the couples’ coping with illness (Mayberry and Osborn, 2014), no study considered their effects on diabetes management efficacy simultaneously, that is, put them together in a model for exploration. Furthermore, dyadic coping and management efficacy from patients and spouses were not explored simultaneously in one model, while they are interconnected. Even though one study considered both patients’ and spouses’ dyadic coping, treating them as one variable through factor analysis, separate effects of each of them was unclear. Similarly, there is one study on collective efficacy that measured the couple’s confidence in diabetes management as a whole (Haines et al., 2018), while how patient’s and spouse’s perceptions of dyadic coping measured separately would be associated with their individual efficacy is unknown.
The moderating role of illness appraisal
Previous studies have explored the moderating role of illness appraisal, which measured from patients (Berg et al., 2020; Helgeson et al., 2019; Zajdel et al., 2022) or spouses (Zajdel et al., 2021) only, in the relationship between process variables and diabetes-related health outcomes. They found that when patients appraised diabetes as a shared problem, collaborative and emotional support, as well as instrumental support, was related to better physical and psychological health (Helgeson et al., 2019). In addition, when patients reported lower shared appraisals, collaboration and support behavior were associated with worse diabetes outcomes (Berg et al., 2020; Zajdel et al., 2022). However, shared appraisal from spouses can buffer patients with low levels of self-efficacy from poorer health (Zajdel et al., 2021). Although one study has considered the consensus on illness appraisal between couples, this measure ignored the specificity of individual illness appraisal (Stephens et al., 2013). Given patients and spouses are most likely to collaborate in illness management when they both appraised shared responsibility (Helgeson et al., 2018), it would be essential to explore the relationship between dyadic coping and diabetes management efficacy in reference to couples’ dyadic appraisal of the illness.
The need to study couple pairs with one spouse who had diabetes
As a key element in the social support process, sharing similar experiences can enhance support effectiveness and reduce potential mismatches between the support provided and received by fostering greater empathic understanding (Suitor et al., 1995; Thoits, 1986). The support extended to others frequently mirrors one’s personal coping strategies and has the potential to aid another person’s coping process by assisting them in reinterpreting the situation through the perspective of the support provider (Thoits, 1986). Therefore, the optimal alignment between the assistance given and received may occur in interactions between individuals who have encountered or are currently confronting the same stressor. As opposed to a couple where only one person has diabetes, a couple where both people have diabetes face the same stressors and may share an understanding of the challenges and experiences associated with managing these health conditions, and this shared experience can promote empathy and support between the couple and therefore better management of diabetes. Therefore, emphasis should be paid to study how to promote the positive support from spouses’ when only one of the spouses has diabetes.
Purpose of the present study
The current study aimed to explore how dyadic appraisal would moderate the association between dyadic coping and diabetes management efficacy. It compared the relative strength of association between different forms of dyadic coping (i.e. positive, neutral, and negative behaviors) and couples’ diabetes management efficacy, as well as the reciprocal influence between couples in a given situation. It is assumed that only when couples both appraised diabetes as a shared problem, dyadic coping would be perceived more and influence couples’ diabetes management efficacy respectively.
Method
Sample
Patients with confirmed type 2 diabetes registered for the National Essential Public Health Services for Management, over 55 years, cohabited with spouses in the community were recruited, along with their spouses who do not have diabetes. The recruitment was conducted through community healthcare centers, who publicized the project through posters and WeChat official account platform. Informed older couples and these identified via registration of the healthcare centers were then assessed for their eligibility for participation. Couples both participated in the recruitment survey, with measures on their dyadic appraisal and dyadic coping of diabetes, as well as self-rated diabetes management efficacy, constituted the current study sample (N = 276 couples). The study was approved by the Ethics Committee of Sun Yat-sen University (2019-064), and informed consents were obtained from all participants.
Instrument
Dyadic appraisal and dyadic coping
Dyadic appraisal and dyadic coping were measured by the Chinese version of the Couple Collaborative Management Scale (C-CCMS) (Zheng et al., 2023) with 20 items that our team translated from the hybrid scale integrated by Helgeson et al. (2019). C-CCMS was validated in Chinese older adults with versions for patient and spouse, with the content validity ratio from 0.714 to 1, the item-level content validity index from 0.857 to 1, multi-rater kappa statistic from 0.849 to 1, the scale-level content validity index/Universal Agreement of 0.946, the scale-level content validity index/ Average of 0.992, and Cronbach’s alpha of the internal consistency reliability for the patient version and spouse version of 0.94 and 0.91, respectively (Zheng et al., 2023). C-CCMS was presented in Supplemental Tables S1 and S2.
Diabetes management efficacy
Diabetes management efficacy of patients was measured by the Chinese version of the Diabetes Management Self-Efficacy Scale (C-DMSES) (Vivienne Wu et al., 2008) with adequate reliability (α = 0.93). C-DMSES consists of 20 items, rated based on a scale from 0 “completely unachievable” to 10 “completely achievable” on patient’s confidence in daily management activities of diabetes. The sum score of C-DMSES ranges from 0 to 200, with higher scores indicating better efficacy. Spouses were provided with a modified version of C-DMSES to examine management efficacy for assisting patients with diabetes management (Wichit et al., 2018).
Patients’ diabetes management behaviors
We also measure patients’ diabetes management behaviors by the Summary of Diabetes Self-Care Activities (SDSCA) questionnaire (Toobert et al., 2000). SDSCA consists of 11 items that assess the frequency of diabetes self-management activities performed by patients in the past week. These activities include general diet, specific diet, exercise, blood-glucose testing, foot-care, and medication adherence. Given the low inter-item correlations for this scale, Toobert et al. suggested to use the individual items is recommended. The rules for scoring the questionnaire are as follows: General Diet = Mean number of days for items 1 and 2; Specific Diet = Mean number of days for items 3, and 4, reversing item 4 (0 = 7, 1 = 6, 2 = 5, 3 = 4, 4 = 3, 5 = 2, 6 = 1, 7 = 0); Exercise = Mean number of days for items 5 and 6; Blood-Glucose Testing = Mean number of days for items 7 and 8; Foot-Care = Mean number of days for items 9 and 10; Medication Adherence = Item 11.
Covariates
We choose patients’ and spouses’ age and diabetes duration of patients as covariates based on a developmental-contextual model of couples coping with chronic illness (Berg and Upchurch, 2007). In addition, due to the effectiveness of couples working together to manage diabetes varies by gender and education (Allen and McFarland, 2020; Liao et al., 2021; Mathew et al., 2012), patients’ and spouses’ education and gender were considered as covariates. Although our participants were from 14 community healthcare centers, the inter-community heterogeneity was small (intraclass correlation coefficient was 0.1), we, therefore, included these centers as another covariate.
Design
This study belongs to a family study of a multi-centered randomized control trial of couple-based diabetes management among community-dwelling older patients with type 2 diabetes and their spouses, in Guangzhou, China (Liao et al., 2020). It is a cross-sectional analysis based on older couples surveyed at the recruitment of our family study, conducted from August to December 2020.
We employed the two-intercept actor–partner interdependence moderation model (APIMoM) (Garcia et al., 2015) to investigate the relationship between patient’s and spouse’s dyadic coping (independent variables) and their diabetes management efficacy (dependent variables), stratified by the pair’s dyadic appraisal. Our study included 276 couples, which exceeds the minimum sample size of 200 required for this method of analysis. In the model, the actor effect indicates patient’s or spouse’s dyadic coping in relation to their own efficacy measure, while the partner effect reflects their reciprocal association; and the two intercepts estimate the actor and partner effects for diabetes patients (coded as 1) and their spouses (coded as −1) separately. The standardized Z scores of positive, negative, and neutral behaviors, were simultaneously adjusted in the model for direct comparison (correlations were examined to preclude collinearity). The model adjusted for patients’ and spouses’ age, education, gender, community healthcare centers and diabetes duration (for patients only) as covariates. Thus, the model included actor and partner effects (i.e. patient = 1, spouse = −1) for dyadic copying (i.e. positive behaviors, negative behaviors and neutral behaviors), and its interaction with couple’s illness appraisals (e.g. positive behaviors × only patient shared, or × only spouse shared, or × neither shared; similar, for negative behaviors and neutral behaviors), adjusted for patient/spouse age, education, gender; community health care center the couples from; and diabetes duration of patient). All data were analyzed by SPSS25.0, with two-sided p-values less than 0.05 considered as statistically significant.
Results
Sample characteristics
As shown in Table 1, the mean age of patients was 66.0 years old and that of spouses was 65.8 years old. Almost half of the patients are male. More than half of patients and spouses had a higher education level. The mean duration of diabetes was 7.96 years. The mean score of General Diet, Specific Diet, Exercise, Blood-Glucose Testing, Foot-Care, Medications, is 5.0, 3.6, 3.7, 1.9, 7.0, and 5.6, respectively. Most of the dyadic appraisals are “only spouse shared” (36.6%) and “neither shared” (36.6%).
Characteristics of diabetic couples studied (n = 276 couples).
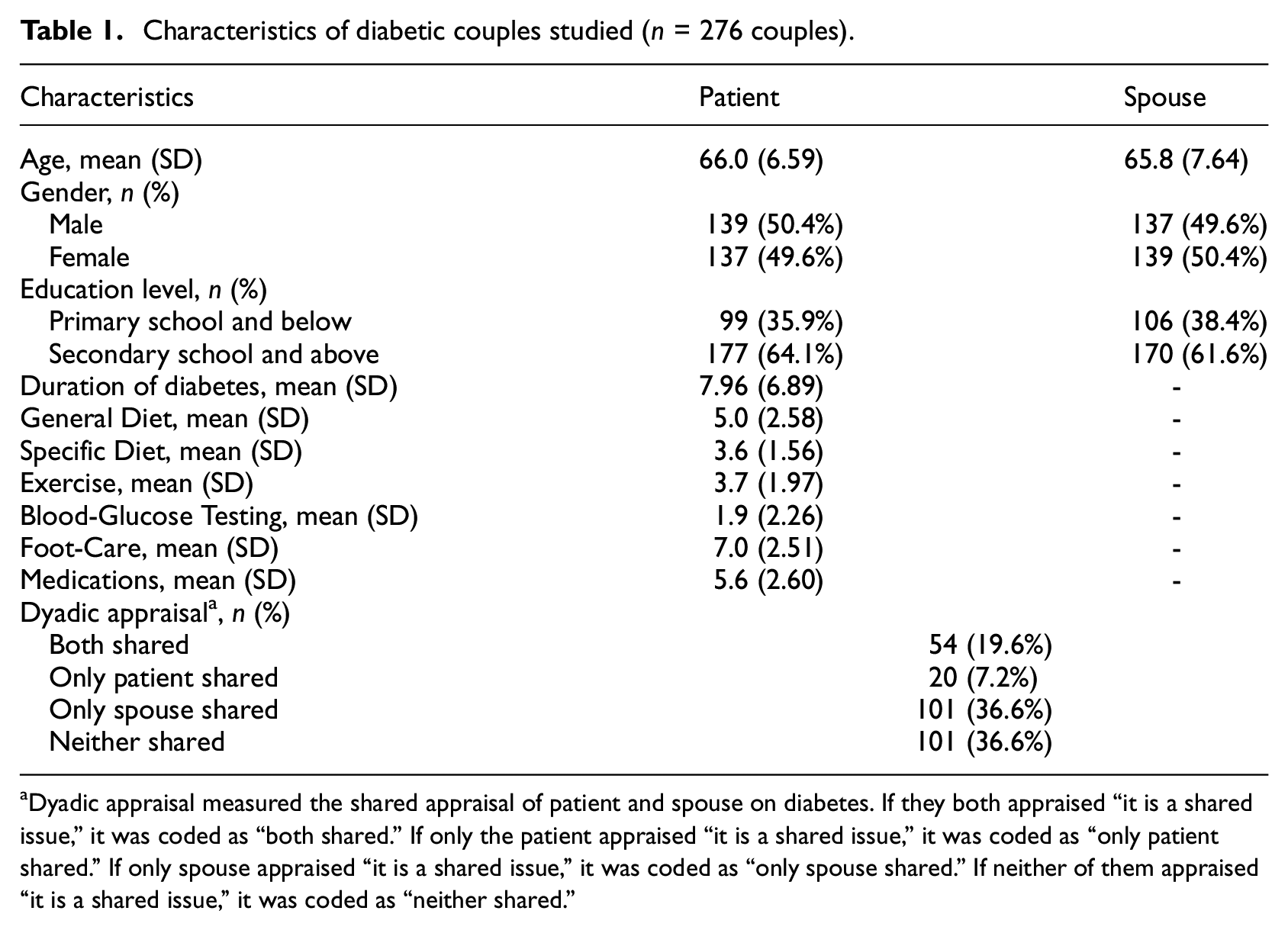
Dyadic appraisal measured the shared appraisal of patient and spouse on diabetes. If they both appraised “it is a shared issue,” it was coded as “both shared.” If only the patient appraised “it is a shared issue,” it was coded as “only patient shared.” If only spouse appraised “it is a shared issue,” it was coded as “only spouse shared.” If neither of them appraised “it is a shared issue,” it was coded as “neither shared.”
The correlations of dyadic coping and diabetes management efficacy between patients and spouses
As shown in Table 2, the mean positive behaviors, negative behaviors, and neutral behaviors were 26.20, 16.26, 3.40 for patients, respectively, 28.51, 17.33, 3.50 for spouses, respectively. Except the correlation between positive behaviors from patient’s perspective and neutral behaviors from spouse’s perspective, between positive behaviors from spouse’s perspective and neutral behaviors from patient’s perspective, (p = 0.08, 0.60, respectively), the correlations of each form of dyadic coping between patients and spouses were from 0.18 to 0.66 (all p < 0.01). The mean diabetes management efficacy of patients was 141.58, while that of spouses was 122.73. The correlation of management efficacy between patients and spouses was 0.29 (p < 0.001).
Description and correlations of Dyadic Coping a and diabetes management efficacy.
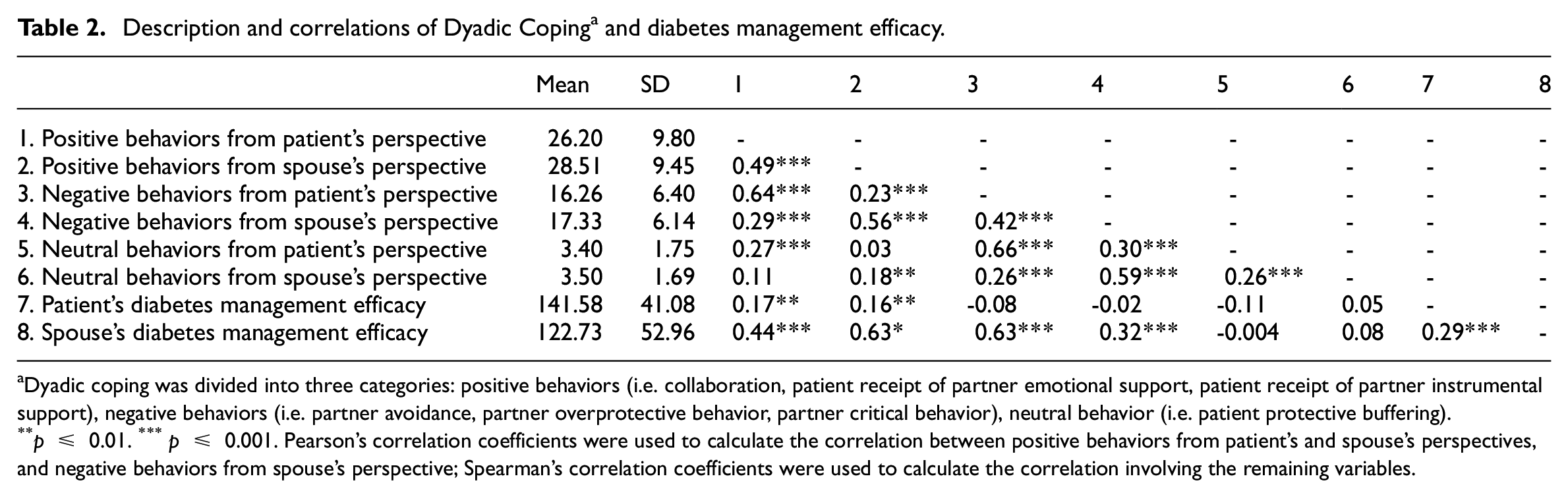
Dyadic coping was divided into three categories: positive behaviors (i.e. collaboration, patient receipt of partner emotional support, patient receipt of partner instrumental support), negative behaviors (i.e. partner avoidance, partner overprotective behavior, partner critical behavior), neutral behavior (i.e. patient protective buffering).
p ≤ 0.01. ***p ≤ 0.001. Pearson’s correlation coefficients were used to calculate the correlation between positive behaviors from patient’s and spouse’s perspectives, and negative behaviors from spouse’s perspective; Spearman’s correlation coefficients were used to calculate the correlation involving the remaining variables.
Actor and partner effects of dyadic coping on diabetes management efficacy moderated by dyadic appraisal
In order to show the actor and partner effects in different forms of dyadic coping with couple’s illness appraisals, we present these results produced by post-estimation of interaction terms separately in Figure 1. All the coefficients estimated by the model were presented in Supplemental Table S3.
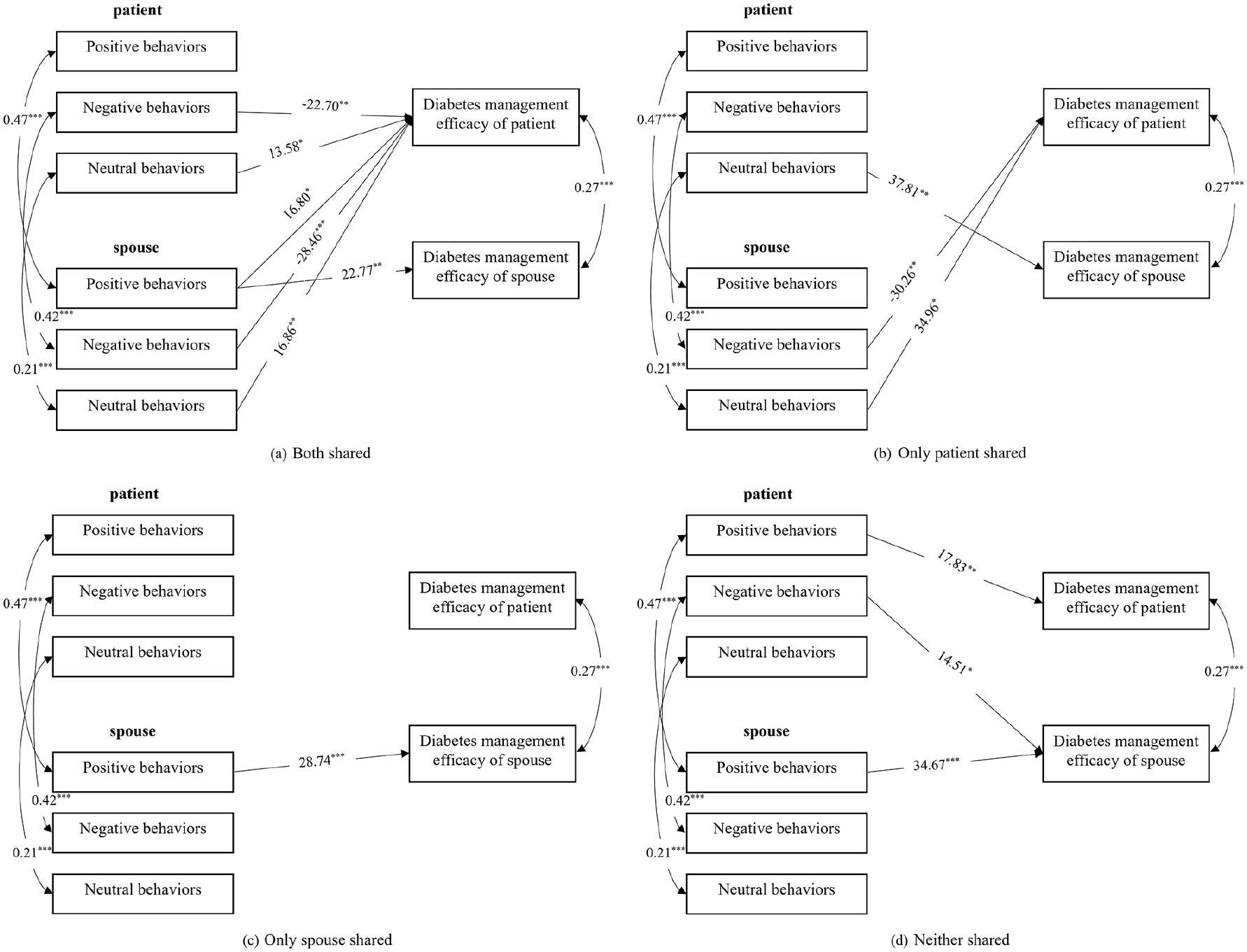
Actor and partner effects of dyadic coping on diabetes management efficacy by dyadic appraisal: (a) both shared, (b) only patient shared, (c) only patient shared, and (d) neither shared.
Figure 1a shows when both patients and spouses considered diabetes as a shared issue, the actor effects of negative behaviors, neutral behaviors from patient’s perspective, and positive behaviors from spouse’s perspective on their own diabetes management efficacy were statistically significant. The actor effects indicate that the more negative behaviors the patient reported, the less diabetes management efficacy the patient got (β = −22.7, p = 0.008); the more neutral behaviors the patient reported (β = 13.6, p = 0.017) and the more positive behaviors the spouse reported (β = 22.8, p = 0.009), the more diabetes management efficacy themself got. The partner effects of positive behaviors, negative behaviors, and neutral behaviors from spouse’s perspective on patient’s diabetes management efficacy were significant. The partner effects indicate that the more negative behaviors the spouse reported, the less diabetes management efficacy the patient got (β = −28.5, p < 0.001); the more positive (β = 16.8, p = 0.028) and neutral behaviors (β = 16.9, p = 0.006) the spouse reported, the more diabetes management efficacy the patient got.
When only patient considered diabetes as a shared issue, no actor effects were significant; the partner effects of neutral behaviors from patient’s perspective on spouse’s diabetes management efficacy, and negative behaviors, neutral behaviors from spouse’s perspective on patient’s diabetes management efficacy were significant (Figure 1b). The partner effects indicate that the more neutral behaviors the patient reported, the more diabetes management efficacy the spouse got (β = 37.8, p = 0.005); the more negative behaviors the spouse reported, the less diabetes management efficacy the patient got (β = −30.3, p = 0.008); the more neutral behaviors the spouse reported, the more diabetes management efficacy the patient got (β = 35.0, p = 0.014).
Figure 1c depicts when only spouse considered diabetes as a shared issue, just an actor effect of positive behaviors from spouse’s perspective on his own diabetes management efficacy was significant, which indicates that the more positive behaviors the spouse reported, the more diabetes management efficacy the spouse got (β = 28.7, p < 0.001) (Carstensen et al., 1999).
Figure 1d illustrates when neither patient nor spouse considered diabetes as a shared issue, the actor effects of positive behaviors from patient’s perspective and from spouse’s perspective on their own diabetes management efficacy were significant. The actor effects indicate that the more positive behaviors the patient (β = 17.8, p = 0.002) or the spouse reported (β = 34.7, p < 0.001), the more diabetes management efficacy they got. The partner effect of negative behaviors from patient’s perspective on spouse’s diabetes management efficacy was significant. The partner effect indicates that the more negative behaviors the patient reported, the less diabetes management efficacy the spouse got (β = 14.5, p = 0.030).
Discussion
We examined the moderating role of dyadic appraisal in the association between dyadic coping and diabetes management efficacy by APIMoM. Our results supported our hypothesis, that only when couples both appraised diabetes as a shared problem, dyadic coping was perceived more and was related to diabetes management efficacy. In this case, the negative behaviors were more related to patients’ diabetes management efficacy than neutral or positive behaviors, and the patients were more likely to be influenced by their spouses.
The consistency in Chinese older couples’ perception of diabetes as a shared problem turned to be lower than we would expect. Less than one-fifth of the couples we studied both appraised diabetes as a shared responsibility, while proportion of only spouses found it should be shared is up to 37%. Similar proportions of dyadic appraisal have been reported among US type 1 diabetes couples (Helgeson et al., 2019). Prior evidence turned to indicate that spouses but not patients were more likely to view diabetes as a problem to be solved together (Zajdel et al., 2021), and get more engaged with the concept of co-management (Berry et al., 2020). Given Chinese culture values harmonious relationships and puts the interests of the family above personal interests (Cong, 2004), our findings here may imply spouses prefer to consider diabetes management as a shared responsibility to reduce patients’ suffering caused by the disease.
The disparity in couples’ appraisal of diabetes further moderated their interpretation of their coping behaviors and their associations with diabetes management efficacy. We found when couples both appraised diabetes as a shared problem, more statistically-significant actor and partner effects would be identified between couples’ dyadic coping behaviors and management efficacy. However, in cases when either patients or spouses believe that diabetes is not a shared problem, most of the coping behaviors from patients’ or spouses’ perspective were unrelated to management efficacy. The couples’ consistency in shared illness appraisal may reflect their commitment to co-management of the illness (Helgeson et al., 2018), which in return may affect their engagement and perception to such coping behaviors. When both patients and spouses consider diabetes as a shared issue, they are more likely to perceive the existence of these behaviors and be affected (Hong et al., 2005). On the other hand, when disparity exists in their shared appraisal, they may turn to overlook these behaviors (Bolger and Amarel, 2007).
Moreover, our study revealed that the negative behaviors turned to be more strongly related to diabetes management efficacy than neutral or positive behaviors. Despite prior evidence has found positive behaviors like collaboration (Helgeson et al., 2022a, 2022b) and support (Helgeson et al., 2022a) are associated with better health outcomes, while the opposite is true for negative behaviors like overprotection (Schokker et al., 2011); few of them addressed these behaviors simultaneously. Positive, neutral and negative coping behaviors may all present in daily diabetes management (Mayberry and Osborn, 2014), and our study contributed to the literature by directly quantifying the strengthen of the relationships between multiple coping behavior to management efficacy. Our findings indicated that the positive effects of positive and neutral behaviors are not sufficient to offset the negative effects rendered by the same amount of negative behaviors when present jointly. That is probably because the patients may feel that they are the ones who make themselves and their spouses face the problem of diabetes, thus may be more sensitive to or dwelling on negative behaviors. This finding is also in line with loss aversion theory that describes the tendency for people to prefer gains over losses (Kahneman and Tversky, 1979), to the extent that disutility brought by the same amount of loss is 2.5 times the positive utility of the same amount of gain.
As regards the relative strength of actor and partner effects in the association between coping behaviors and management efficacy, we found stronger partner effects for patients, while only actor effects were found for spouses. Specifically, patients’ efficacy was more affected by perceived negative and neutral behaviors from spouses than themselves, and only by positive behaviors from spouses. In the contrary, spouses’ efficacy was only affected by their own perceived dyadic coping. Our findings are similar to previous findings on diabetes and other diseases that the partner effects are stronger than the actor effects for patients in the relationship between communal coping and health-related outcomes (Rohrbaugh et al., 2008; Van Vleet et al., 2018). We measured dyadic coping on a scale called C-CCMS so that the coping behaviors measured were perceived behaviors. Given spouses are more likely to take diabetes as a shared responsibility and get actively involved (Berry et al., 2020; Helgeson et al., 2019), the impact on patients is particularly significant and even greater than patient’s own impact. The partner effects were not evident for spouses, all of whom were free from diabetes, and may be less affected by the patients’ coping behaviors. Dietary adherence is a crucial aspect of diabetes management. It is essential to provide patients and their spouses with the necessary knowledge and skills regarding their diet (Beverly et al., 2008). In Chinese families, cooking is primarily the responsibility of women. Therefore, it is important to consider the gender of the spouse when providing dietary-related measures. Different and more targeted measures can be developed to help manage diabetes, regardless of the gender of the spouse.
The strength of this study is we considered multiple coping behaviors simultaneously in the analyzed model, with measuring the dyadic coping and diabetes management efficacy from the perspective of both the patient and the spouse in China. However, there are some limitations to our study. First, we recruit both patients and spouses, so we can only recruit spouses who are willing to cooperate, which may limit the generalizability of our findings. Second, the measures of behaviors and efficacy were all self-reported. Subjective measures are likely to be influenced by respondents’ characteristics, such as gender and personality traits. Third, our study is a cross-sectional study, where the direction of these associations cannot be established. Additionally, we did not take into account the effects of treatment regimens and diabetes-related complications on diabetes management.
Conclusions
We found that the association between dyadic coping and diabetes management efficacy would be moderated by dyadic appraisal. Dyadic coping is more perceived and influence diabetes management efficacy when both patients and spouses appraised diabetes as a shared issue. Opportunities exist to improve diabetes management by educating older couples jointly to form correct knowledge and coping behaviors toward diabetes, taking more positive and neutral behaviors, while reducing negative behaviors.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241240735 – Supplemental material for How dyadic appraisal moderate the association between dyadic coping and diabetes management efficacy
Supplemental material, sj-docx-1-hpq-10.1177_13591053241240735 for How dyadic appraisal moderate the association between dyadic coping and diabetes management efficacy by Huiqiong Zheng, Xinyu Fan, Yuyang Liu, Yanjuan Wu, Yixuan Liu, Yingxin Xu, Jingyi Zhi, Conghui Yang and Jing Liao in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053241240735 – Supplemental material for How dyadic appraisal moderate the association between dyadic coping and diabetes management efficacy
Supplemental material, sj-docx-2-hpq-10.1177_13591053241240735 for How dyadic appraisal moderate the association between dyadic coping and diabetes management efficacy by Huiqiong Zheng, Xinyu Fan, Yuyang Liu, Yanjuan Wu, Yixuan Liu, Yingxin Xu, Jingyi Zhi, Conghui Yang and Jing Liao in Journal of Health Psychology
Footnotes
Author contributions
J.L. designed the study, contributed to discussion, and reviewed and edited the manuscript. H.Q.Z. researched data, contributed to discussion, and wrote and edited the manuscript. X.Y.F. researched data, contributed to discussion, and reviewed and edited the manuscript. Y.Y.L. researched data, contributed to discussion, and reviewed the manuscript. Y.J.W. contributed to discussion, reviewed and edited the manuscript. Y.X.L., C.H.Y., Y.X.X., and J.Y.Z. contributed to discussion and reviewed the manuscript.
Data sharing statement
Materials and analysis code for this study are available by emailing the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (71804201) and the Natural Science Foundation of Guangdong Province of China (2018A0303130046).
Ethics approval
Informed consent
Informed consents were obtained from all participants.
Pre-registration
Chinese Clinical Trial Registry, ChiCTR1900027137, Registered 1st November 2019.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.