
Abstract
Given the unpleasant nature of social isolation and loneliness (SIL) and their negative effects on health and wellbeing, interventions are needed. However, persistent issues in the design, evaluation, and reporting of SIL interventions preclude conclusive evidence and commentary on the effectiveness of SIL interventions. Here, we propose guidelines for evaluating SIL interventions, firstly by operationalising them into two categories: (1) interventions aiming to reduce SIL as a primary outcome and (2) interventions aiming to improve non-SIL outcomes in the lives of individuals experiencing SIL. Secondly, we evaluate instruments for measuring SIL and research designs for studying intervention effectiveness. Thirdly, guidelines for reporting information about the intervention, study design, results, and discussion in SIL intervention studies are presented. These guidelines will help researchers to better and more consistently report on SIL interventions and improve comparability of SIL interventions, ultimately contributing to the improvement of interventions and to the mitigation of SIL.
Background
Social isolation and loneliness (SIL) are not only undesirable states in their own right, but also significant public health problems in contemporary societies. Growing evidence suggests a negative impact of SIL on health and wellbeing. For instance, SIL are established risk factors for cognitive decline and dementia (Boss et al., 2015; Livingston et al., 2020), cardiovascular illness (Hodgson et al., 2020; Valtorta et al., 2016), adverse psychological outcomes such as suicide attempts and psychotic symptoms (Solmi et al., 2020) and early all-cause mortality (Holt-Lunstad et al., 2015; Holwerda et al., 2016). Consequently, these negative outcomes lead to increased societal economic costs (Meisters et al., 2021). On a point of definition, social isolation refers to the absence of social relationships (De Jong Gierveld et al., 2006), whereas loneliness is often defined as the perceived discrepancy between the quality and/or quantity of an individual’s actual and desired social relationships (Peplau and Perlman, 1982). Loneliness is sometimes described as a unidimensional construct, yet elsewhere three subtypes of loneliness are distinguished. Social loneliness refers to the lack of a (specific) larger group to which someone belongs. Emotional loneliness refers to the lack of one or more (specific) individuals that one closely relates to (Weiss, 1973). Existential loneliness, meanwhile, refers to a negative affective state associated with feeling unconnected, estranged from the world or the sense that life has no meaning (Bolmsjö et al., 2019).
Given the unpleasant nature of SIL and their negative effects on health and wellbeing, interventions are needed. Existing interventions show some promise for reducing SIL, although the magnitude of the effects at the meta-analytic level tends to be small to moderate (Beckers et al., 2022; Eccles and Qualter, 2021; Masi et al., 2011; Zagic et al., 2022). Some persistent issues in the field preclude conclusive commentary on the effectiveness of SIL interventions – to the extent that a recent systematic review of friendly visit interventions for SIL in older adults demonstrated that all studies reviewed had problems in design and execution (Laermans et al., 2023). As Laermans et al. demonstrate, the methodological quality of existing studies of SIL interventions is mixed, and often poor (e.g. small sample sizes, high heterogeneity and risk of bias). More problematically, often the terms loneliness and social isolation are used interchangeably (Beckers et al., 2022; Victor et al., 2018), which further obfuscates the true effect of such interventions. As such, it can be difficult to glean, from the existing literature, what is likely to work in counteracting SIL. Establishing best practice in designing, evaluating, and reporting SIL interventions, is a key next step in the planning and implementation of interventions to reduce SIL. Such a conclusion was recently reached by the European Union Joint Research Centre (EU JRC) which published an overview of current knowledge on loneliness interventions specifically (Beckers et al., 2022). They recommended the development of a ‘commonly agreed framework or taxonomy to categorise loneliness interventions’ (Beckers et al., 2022: 35) and the use of appropriate research methods to establish intervention effects. As they put it, the rationale for such recommendations was that ‘more robust evaluations would add to the international knowledge base of interventions and help ensure that people who suffer from loneliness benefit from effective interventions’. (Beckers et al., 2022: 35).
The current paper aims to address the need for improvement of evaluation of SIL interventions by picking up on those recommendations. Specifically, we aim to provide (1) a taxonomy for categorising SIL interventions, (2) a discussion of appropriate study designs and measurements for use in evaluating SIL interventions and (3) guidelines for reporting the results of SIL intervention studies. A clear taxonomy on what constitutes a SIL intervention is needed in order to determine on what outcomes to evaluate an intervention. A discussion on study designs and measurements is useful for determining which research method is promising for SIL intervention studies. Having clear guidelines for reporting results of SIL interventions may lead to better adoption of interventions and contributes to better comparison of outcomes in meta-analytic reviews.
Taxonomy: Two categories of SIL interventions
At date, it is unclear what exactly constitutes a SIL intervention and an operationalisation is needed. We propose two conditions for an intervention to be defined as a SIL intervention. First, SIL interventions must specifically target individuals who experience SIL. For interventional purposes, it may be beneficial to include individuals who do not experience SIL – for instance, when interaction with these individuals is part of the intervention for individuals who experience SIL. In such interventions, inclusion of individuals not experiencing SIL is a means to an end. Interventions that incidentally include individuals experiencing SIL, but do not specifically target them, are not considered SIL interventions. Second, SIL interventions are interventions. For this paper, we define ‘intervention’ as an intentional act (or a series of acts) to improve a specific outcome. Hence, unintentional acts or acts with no defined outcome are not considered ‘interventions’, but are instead referred to as ‘activities’. An example of an activity would be an active retirement group meeting for social reasons.
SIL interventions can have different objectives, ranging from reducing SIL to enlarging the amount of contact and improving general health. We propose a broad operationalisation of SIL interventions which includes two categories. Specifically, SIL interventions can be categorised into: (1) interventions that aim to reduce SIL as a primary outcome (Category I) and (2) interventions that aim to improve other specific outcomes than SIL in the lives of individuals experiencing SIL (Category II), such as well-being, social support, or health. For the former category, a further distinction can be made into Category I interventions that focus on reducing social isolation, social loneliness, emotional loneliness AND/OR existential loneliness. For the latter category, expecting changes in SIL is unrealistic, since no specific actions are taken regarding SIL. A SIL intervention can fall into both categories. With the advent of complex interventions in psychosocial research (Skivington et al., 2021) it is easy to find SIL interventions overlapping with some additional aim, for example, improving nutritional status (McHugh Power et al., 2016). Figure 1 shows a decision tree, which guides the status and classification of a SIL intervention (i.e. Category I and/or Category II).
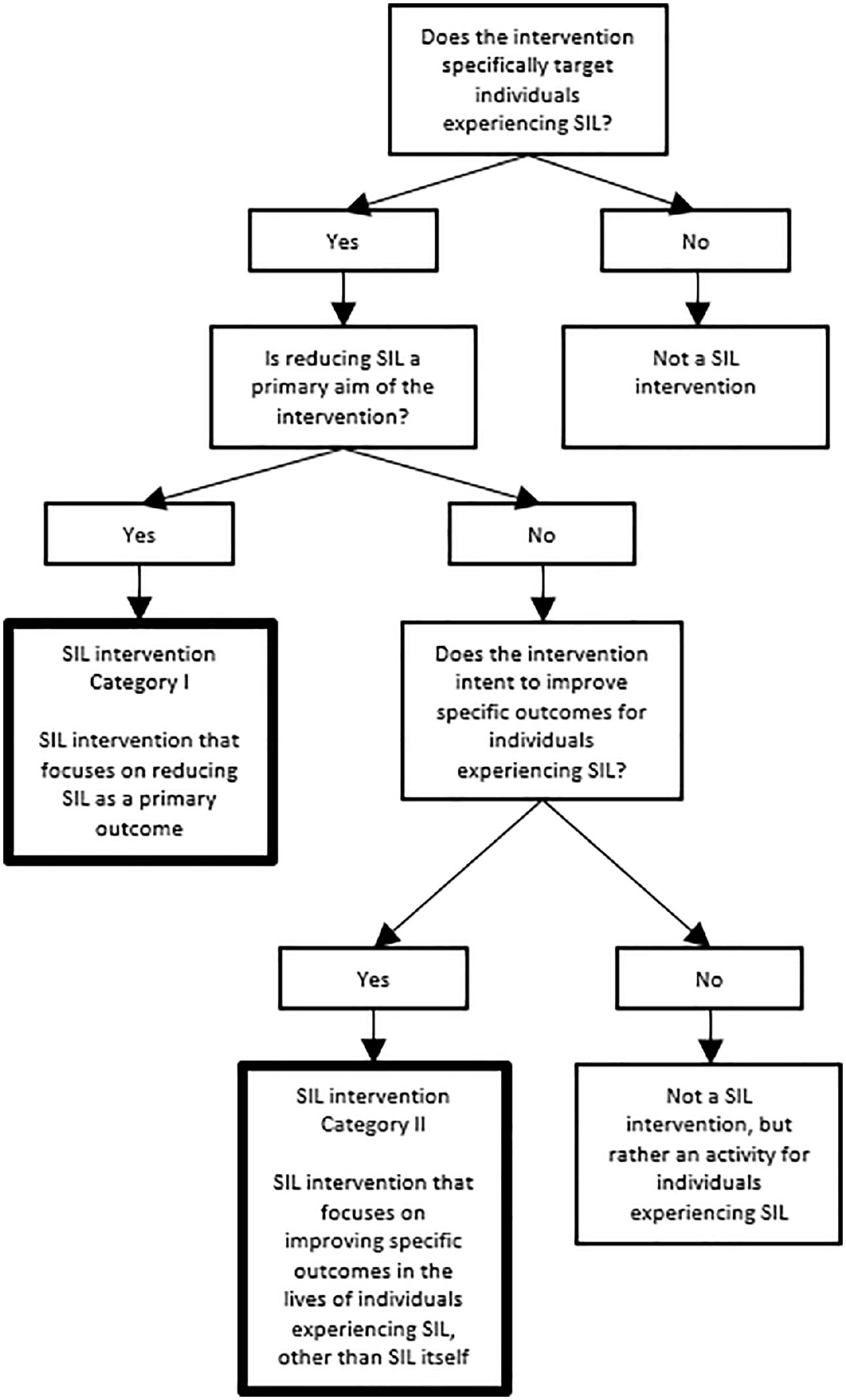
Decision tree whether something constitutes as a SIL intervention (Category I and II) and what to measure in an evaluation of a SIL intervention.
Distinguishing these two categories of SIL interventions has an important implication: not all SIL interventions aim at reducing SIL, only SIL intervention Category I does so. Previous studies (Bessaha et al., 2020; Cattan et al., 2005; Cohen-Mansfield and Perach, 2015; Dickens et al., 2011; Eccles and Qualter, 2021; Findlay, 2003; Fokkema and van Tilburg, 2007; Franck et al., 2016; Gardiner et al., 2018; Hagan et al., 2014; Masi et al., 2011; Poscia et al., 2018; Williams et al., 2021) show that results of SIL interventions have often been disappointing. A possible explanation is that the studied interventions implicitly had targeted outcomes other than reducing SIL, but rather focussed on improving some aspect of the lives of individuals experiencing SIL. In other words, Category II SIL interventions might have been studied as Category I SIL interventions. Explicating the distinction between Category I and Category II interventions can help future researchers better understand the aims and targets of SIL interventions. A possible, additional category of SIL interventions may include interventions which aim to prevent the occurrence or onset of SIL. In line with previous work (Beckers et al., 2022), we argue that preventive interventions constitute a distinct category of interventions. Preventive SIL interventions are as such outside the scope of this paper, and warrant further consideration.
Designs for developing and evaluating a SIL intervention
Recent recommendations have been made to dedicate resources for high-quality and theory-based built-in evaluations of the direct and long-term effects of SIL interventions (Beckers et al., 2022; Victor et al., 2018). While we fully agree with this advice and the importance of effect evaluation, we suggest that SIL intervention owners acknowledge the time needed to prepare for this. We advise SIL intervention owners to conceptualise the evaluation process as involving several cycles, reserving sufficient time to evaluate and monitor the SIL intervention thoroughly, and responding to such monitoring by making adjustments to the SIL intervention accordingly (e.g. ensuring it is feasible and that programme activities have been implemented as intended). Such a process has been termed ‘formative evaluation’ previously (Wight et al., 2016) and is crucial to complete before considering a more formal evaluative phase. Potential facilitators in SIL intervention success include ‘having a theoretical foundation or programme theory’; ‘participant selection’ (aiming at a specific group of participants to which the programme theory applies, meeting the eligibility criteria); ‘participant contribution’; ‘practitioner quality’ (ensuring competences, proficiency, and effectiveness exhibited by the provider); ‘a tailor-made approach’ (taking into account individual preferences and needs); ‘longer duration and higher frequency’; ‘a multi-faceted approach’, ‘using technology as a tool in some way’, and ‘monitoring and evaluation’ (Bessaha et al., 2020; Cattan et al., 2005; Cohen-Mansfield and Perach, 2015; Dickens et al., 2011; Eccles and Qualter, 2021; Findlay, 2003; Fokkema and van Tilburg, 2007; Franck et al., 2016; Gardiner et al., 2018; Hagan et al., 2014; Masi et al., 2011; Poscia et al., 2018; Williams et al., 2021).
As the aim for early-stage SIL intervention evaluation is improving the intervention, rather than measuring its outcomes, a pragmatic approach on evaluation can be helpful (Kratochwill et al., 2021). Formative evaluation in order to monitor the process, progress, or outcomes of SIL interventions can be integrated in SIL interventions using different methods, such as collection of information from intervention recipients, via interviews or questionnaires, critical reflection with co-workers and volunteers, or having an external advisory board advising on the progress. The goal of such monitoring is to learn or establish how the SIL intervention operates, which elements are operative, and which elements need improvement. Using more comprehensive research approaches for definitive intervention evaluation, such as a powered randomised controlled trial, is costly, takes time and effort, and establishing if there is an effect is difficult. Preparing and developing the SIL intervention fully in a preliminary fashion seems appropriate before investing in this kind of evaluative effort. Several approaches may be helpful in the preliminary stages of developing a SIL intervention and in collecting sufficient evidence of initial effectiveness to justify moving to a more rigorous definitive evaluation. For instance, the Six Steps in Quality Intervention Development (Wight et al., 2016) describes six essential steps for developing public health interventions starting with defining and understanding the problem and its causes and ending with collecting sufficient evidence of effectiveness to proceed to a rigorous evaluation.The PRECEDE-PROCEED model (Green and Kreuter, 2005) describes principles and processes of planning in health promotion. Intervention Mapping (Bartholomew et al., 1998) entails a framework for health education intervention development in five steps, starting with describing objectives and resulting in generating evaluation plans. Steps involved in refining health interventions at early stages were recently brought together in a taxonomy (O’Cathain et al., 2019), some of which, such as conducting early (small sample) feasibility studies with adaptability planned, optimising the intervention for full efficiency, documenting or manualising the intervention in high detail, and conducting process evaluations, may be useful when designing and evaluating SIL interventions.
Measurement decisions in SIL interventions
When an intervention is ready for effect evaluation, it is important to define the expected outcomes, establish instruments to measure them, and determine an appropriate study design. We do not prescribe specific study designs but suggest carefully explaining the rationale and being as critical about the intervention as possible. In the next section instruments to measure social isolation and loneliness and designs for studying SIL interventions are discussed. It should be noted that choice of measurement ought to be predicated partly on the operational definition of SIL in the interventional context.
Instruments for measuring SIL
Given that there are two categories of SIL interventions with different goals, different outcomes are needed to evaluate effectiveness. For SIL interventions aiming to reduce SIL (Category I), measuring a reduction in social isolation AND/OR loneliness is the objective. It is critical to establish a priori whether the intervention aims to reduce social isolation AND/OR (type of) loneliness, since reducing one will not necessarily impact the other. For SIL interventions aiming to improve other aspects of the lives of individuals experiencing SIL (Category II), a first step is to predefine the desired outcomes of the intervention, and measure effects on those outcomes. As targeting individuals experiencing SIL is a necessary condition in our proposed classification of SIL interventions, it is essential for both categories of SIL interventions to establish the social isolation AND/OR loneliness of participants entering the intervention. In this section, often used instruments for measuring SIL are presented. While this list is not exhaustive, it serves as a starting point and is based on the frequency of prior use. These instruments can be used by Category I interventions to evaluate effectiveness in reducing SIL and by Category I and II interventions to establish SIL of participants entering the interventions. A list of potential outcomes for Category II interventions is beyond the scope of this study.
Mund et al. (2023) observed that instruments for measuring loneliness can be characterised according to three characteristics: number of items, dimensionality, and direct versus indirect assessment. We argue that similar characteristics apply for instruments measuring social isolation and related aspects of social disconnectedness. The Lubben Network Scale (LSNS; Lubben, 1988; Lubben et al., 2006) measures social engagement. The 18-item version consists of three subscales measuring social engagement with family, friends and neighbours. The 12-item version omits the subscale for neighbours. The 6-item version is a short version of the 12-item version. Subscales can be combined to measure overall social engagement or perceived social support. The 11-item Berkman-Syme Social Network Index (Berkman and Syme, 1979) measures overall social connection in 12 types of social relationships, that is, with the spouse, parents, parents-in-law, children, other close family members, close neighbours, friends, workmates, schoolmates, fellow volunteers, members of groups without religious affiliation, and religious groups. The 6-item Social Isolation Scale (Nicholson et al., 2020) measures overall ‘social isolation’ combining two subscales, that is connectedness (three items) and belonging (three items). All these scales were developed for usage in older populations and use direct questions to assess the chosen constructs. Problematically, the listed instruments don’t measure social isolation as such, but rather related constructs such as social engagement, perceived social support, social connection or belonging (Berkman and Syme, 1979; Lubben, 1988; Lubben et al., 2006; Nicholson et al., 2020). An established instrument to measure social isolation appears to be lacking. More agreement on which measures to use for measuring social isolation seems beneficial. This would make comparison of intervention results easier. For social isolation interventions, it is recommended to define the exact expected outcome and find a matching measurement instrument.
Two commonly used scales for measuring loneliness in general or older adult populations are the UCLA Loneliness Scale (UCLA; Russell, 1996; Russell et al., 1980) and the De Jong Gierveld Loneliness Scale, sometimes termed the Rasch-type Loneliness Scale (DJGLS; de Jong-Gierveld and Kamphuls, 1985; De Jong Gierveld and Van Tilburg, 1999). The original UCLA consists of 20 items providing an indirect measure of loneliness (not including the word ‘loneliness’). Shorter versions, including a 3-item version are available (Hughes et al., 2004). The UCLA measures overall loneliness as a unidimensional construct and has been shown to be used in 64% of loneliness studies (Maes et al., 2022). The original DJGLS consists of 11 items, measuring loneliness indirectly. A shorter 6-item version is available (De Jong Gierveld and Van Tilburg, 2006). The DJGLS measures overall, social and emotional loneliness, and is used mainly in Europe (Maes et al., 2022). Existential loneliness is sometimes measured using the Existential Loneliness Questionnaire (ELQ; 22-items; mostly indirect measurement, but the word ‘lonely’ is used in one of the items; Mayers et al., 2002). Studying the added value of the ELQ items to the DJGLS items, van Tilburg (2021) found only proof for the existence of one sub dimension from the ELQ, measuring ‘meaninglessness in life’. Van Tilburg suggests adding the seven items indirectly measuring this sub dimension to the DJGLS. Neither the ELQ, nor the extended DJGLS have been used often and we are therefore reluctant in recommending to use these, however until date there is no better alternative available.
The Children’s Loneliness Scale (CLS; Asher et al., 1984) and the Loneliness and Aloneness scale for Children and Adolescents (LACA; Marcoen et al., 1987) were developed to measure loneliness among children and adolescents. The CLS consists of 24 items. Sixteen items measure loneliness (combing direct and indirect items) and social dissatisfaction as one construct. Eight items are ‘filler’ items to make children and adolescents at ease. The LACA consists of 48 items. The LACA includes four subscales (12 items each), that is, loneliness in parental relations, loneliness in peer relations, affinity for aloneness, and aversion to aloneness. Together, the four subscales measure loneliness, although it has been argued that only the first two subscales measure loneliness (Maes et al., 2022). A recent systematic review concluded that both these scales, as well as the UCLA Loneliness scale, were insufficiently developed for use with children and adolescents and that further research is needed for these instruments to support intervention evaluation (Cole et al., 2021).
In addition to multi-item scales, single-item measurements, that is, asking one direct question about loneliness, have been used. These measurements are by nature unidimensional. Researchers have been concerned for some time about the potential for social desirability to bias responses to single item measurements of loneliness (Marangoni and Ickes, 1989); since loneliness is stigmatised, participants may be less likely to agree that they do feel lonely when asked directly. Other issues with single-item measurements of loneliness are outlined in prior work (Mund et al., 2023) and with this in mind we recommend avoidance of such approaches to measurement of loneliness and social isolation, since many of the same issues apply for social isolation (stigma, direct nature of the question). The choice for a scale should depend on the intervention goals For intervention research, we recommend using longer versions of SIL scales, as they allow for more variation in outcome.
Study designs
The choice of study design is by necessity a decision to be made once the specific research question is established, and depends partly on what is already known about a topic, and the phase of the research cycle one is at. The question of how to best evaluate interventions is a going concern and each available design has its limitations. It is important to bear in mind that data collection is a time consuming exercise for the researchers and professionals involved, and often demanding for participants. More complex study designs and analytical approaches tend to be more time consuming and demanding. Given the social contact involved in most methods of data collection, intensive data collection can potentially constitute an additional SIL intervention. This may be problematic when it comes to inferring intervention effects. In addition, missingness and drop out are common in complex data collection. This is challenging for analysing data, which requires a high level of statistical expertise. However, complex study designs are needed to resolve one consistent issue in SIL interventions: failing to report on long-term effects of the intervention (Laermans et al., 2023).The following is a list of commonly used intervention evaluation designs that can be adapted for SIL interventions, depending on whether the goal is to evaluate the primary effect or to establish the feasibility in a particular context. While we remain agnostic about the optimal choice of design for evaluating SIL interventions, it should be clear that traditional RCT approaches may sometimes be inadequate for this aim.
The Randomised Controlled Trial (RCT) is the most stringent way of establishing a causal effect between an intervention and a designated outcome (Sibbald and Roland, 1998). As such, it has strict design and implementation requirements. Participants must be randomly allocated to an intervention condition or one or more ‘control’ conditions. Random allocation rules out the possibility that systematic differences in participants between conditions may present as a causal effect (i.e. a difference in outcome between the treatment and control groups). In a medical or pharmacological context, blinding or double blinding is typically used (i.e. experimenters and participants are not aware of which participant is allocated to which group), to reduce the potential for various types of bias affecting study results. The advent of public health interest in loneliness in particular has brought with it an increase in the number of RCTs of loneliness interventions (Eccles and Qualter, 2021). Given the highly controlled experimental nature of a RCT, this approach yields the highest likelihood of a meaningful causal inference and is thus an often preferred approach. An RCT is applicable if two conditions are met. First, an intervention must not have multiple components (possible active elements), unless these can be controlled for separately. Many SIL interventions however are of a complex nature (Matourypour et al., 2020), which complicates further questions of design and analysis (Skivington et al., 2021). Second, it must be possible to have both a treatment and a control group. Having a control group involves withholding of the SIL intervention (which is at least theorised to be effective) to some participants (at least temporarily), which can be problematic from an ethical perspective. Extensions such as the realist RCT can help to elucidate more clearly what works in what mechanistic manner in a successful intervention. The realist RCT focuses on understanding underlying processes of mechanism within an RCT context (Bonell et al., 2012; Jamal et al., 2015). In a realist RCT, the focus is on finding out which interventions work, for whom, and under what circumstances, allowing a more comprehensive understanding of the interaction between intervention components and between intervention and context (Bonell et al., 2012), and thus representing a sensible approach for evaluations of complex interventions such as SIL interventions. Similarly, extensions such as qualitative process evaluations, in the context of a broader trial, or preceding a planned trial, can also help researchers to understand what may be acceptable and feasible in SIL interventions (Lloyd-Evans et al., 2020).
The quasi-experimental design (or labelled non-randomised comparison or multi-cohort studies) bears similarities to the RCT design, albeit without the element of randomisation. Groups or individuals are not assigned to the intervention, which increases the probability of bias that may affect the results. To minimise these effects, researchers must exercise caution in controlling for other factors that may impact the outcomes, such as participant characteristics. Furthermore, statistical methods such as propensity score matching can be employed to enhance the validity of the results. The quasi-experimental design is a viable approach for evaluating SIL interventions in cases where random assignment is not feasible, practical, or ethical. For instance, when examining interventions that are delivered in institutions such as schools or elderly homes, it may not be possible to randomly allocate participants to different groups. However, it may be feasible to establish a control group at different institutions.
In the single-case experimental design (SCED), participants act as their own control, having data collected before intervention onset and afterwards, for a large number of data points (Kratochwill et al., 2023). Collection of pre- and post-intervention data allows the researcher to evaluate the impact of a researcher-manipulated intervention, as well as offering a way to examine meta-intervention outcomes like the immediacy of the intervention effect. The SCED is considered a rigorous, methodologically sound way of evaluating interventions (Smith, 2012). The SCED is particularly useful in situations where it would be unethical or impossible to assign participants to a control group, for instance, when the intervention is known to be beneficial or desirable in some way (Kazdin, 2021). A short, defined pre-intervention period, to enable pre-intervention data collection, is preferable to a longer-time waitlisting, or to forgoing intervention altogether. As such, one context in which the SCED may be useful is in evaluating the effectiveness of an existing community-embedded SIL intervention which regularly registers new recipients (e.g. Hannigan et al., 2020). The flexibility of the design is offset in its specific costs: an intensive longitudinal data collection phase; and complex analytic approaches are required in order to appropriately model the often highly nonlinear nature of the single-case data (Sullivan et al., 2015).
The pre-post comparison design (or single-cohort studies) examines SIL before and after intervention in an intervention group and does not include a control group. Pre-post comparison designs differ from SCEDs in that they typically collect data only once or perhaps twice in the post-intervention phase. Results from pre-post studies represent a significant part of the evidence base in the SIL intervention research area and provide insights into the effectiveness of interventions in real-world settings, especially in situations where the use of a control group is often not feasible or ethical. However, the pre-post comparison design has several important limitations and caution is strongly advised when interpreting the results of such studies. A potential bias of this design is that individuals who initially score high on SIL may be prone to scoring lower at a later measurement, even without intervention. For instance, loneliness can motivate individuals to establish new social relationships, resulting in an improvement over time without intervention. These factors can lead to an overestimation of the effectiveness of an intervention in pre-post studies. Furthermore such designs fail to capture nonlinear trends in SIL or other outcomes following interventions, which may not behave in a linear fashion. Given its limitations, it is unadvisable to use this research design unless no other option is available. The field would benefit from having more studies that include a control group, which allows more reliable and accurate evaluation (Eccles and Qualter, 2021).
Guidelines for reporting an SIL intervention
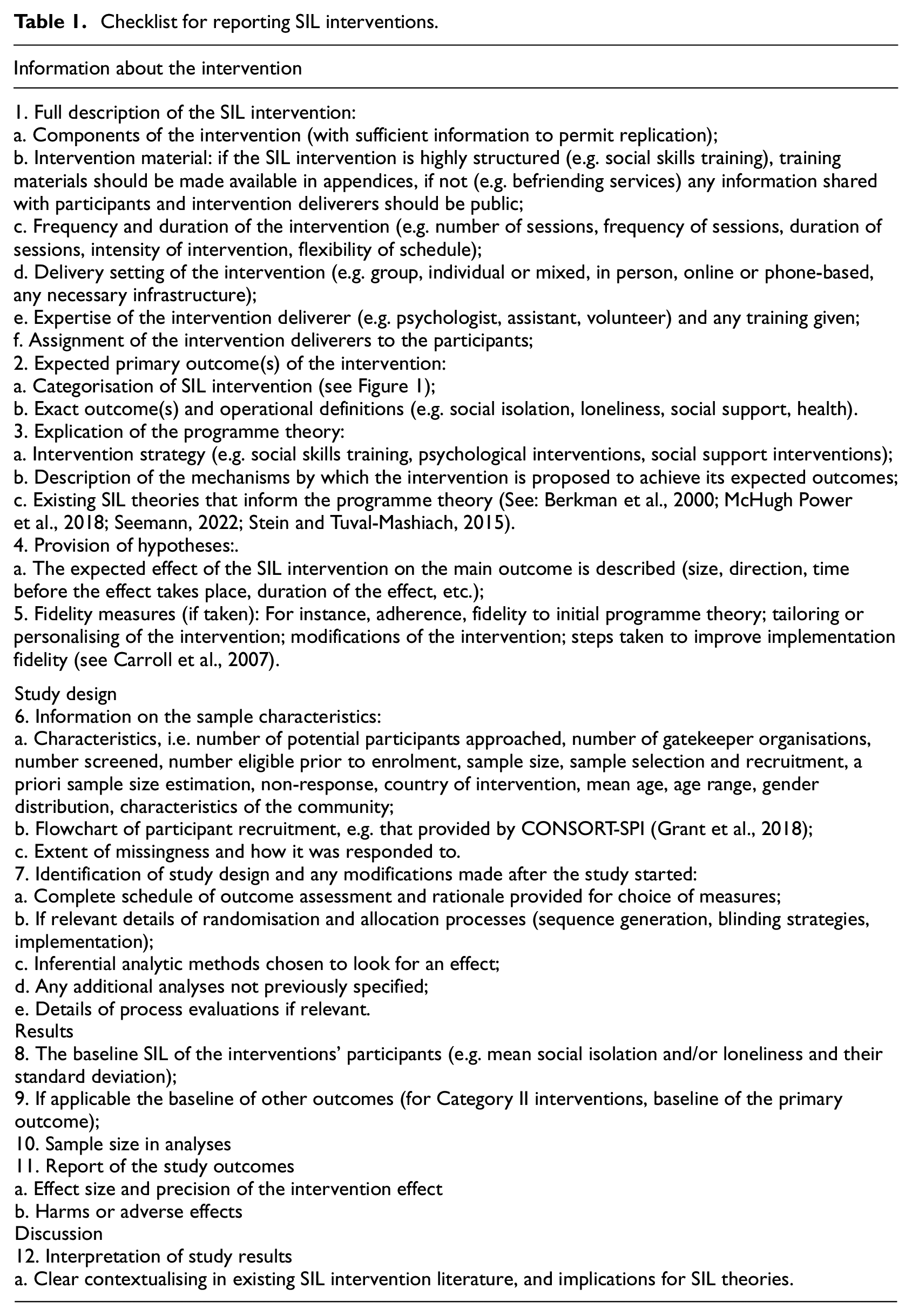
Once a study is performed, it is important to report it properly. Adequate reporting, as well as archival of data are critical to the future development and improvement of SIL interventions, because it allows others to learn, adopt interventions more easily, and to compare outcomes in meta-analytic reviews. In order to translate evidence into practice and to adopt interventions more easily, it is essential to provide comprehensive descriptions of SIL interventions. Comparing results between different studies in meta-analytic reviews is important. For instance, this can provide insights into types of SIL interventions that are more effective in certain circumstances than others or it can lead to knowledge about some SIL interventions being more effective than others. Comparing results requires good data availability practices, for instance making data FAIR: a set of principles that allows systems to Find, Access, Interoperate, and Reuse data with minimal human intervention, (European Research Council (ERC), 2017), Relatedly, regarding pre-registration of studies, matters of transparency in research to avoid methodological missteps such as the ‘garden of forking paths’, in which research decisions hinge on knowledge of the data (Gelman and Loken, 2013) are of concern for SIL interventions too. The EU JRC (Beckers et al., 2022) suggested guidelines for reporting results for studies regarding loneliness interventions. Taking as our starting point existing guidelines for the reporting of intervention studies (Hoffmann et al., 2014), randomised controlled trials, single-case designs, and quasi-experimental designs, all available at the EQUATOR website (https://www.equator-network.org/), we expand these guidelines for SIL interventions into a checklist presented in Table 1. Interventionists using e-health or mobile health approaches to intervention are further recommended to consult the CONSORT-EHEALTH guidelines, which provide subitems on how to report more in-depth on digital elements of eHealth and mHealth interventions (Eysenbach, 2011).
Checklist for reporting SIL interventions.
Conclusion
This paper contributes to the field of SIL research by providing a taxonomy for SIL interventions into two categories, that is, interventions aimed at reducing SIL (Category I interventions) and interventions aimed at improving or reducing other outcomes in the lives of people who experience SIL (Category II interventions), by providing study designs for studying effectiveness of SIL interventions, and by providing guidelines for reporting SIL intervention studies that apply to different study designs. This will help researchers to better and more consistently report on SIL interventions and improve comparability of SIL interventions. Studies suggest that monitoring is a success factor for loneliness interventions (Cattan et al., 2005; Findlay, 2003; Fokkema and van Tilburg, 2007; Gardiner et al., 2018) and that better design is needed to improve SIL interventions more generally (Laermans et al., 2023). As such, we believe that higher standards for evaluation of SIL interventions will contribute to improving the quality of interventions and help promote interventions that mitigate SIL. For practice, implications of better reporting of SIL interventions are that they become more easily adaptable in different contexts and that outcomes become more clear.
Footnotes
Data sharing statement
No new data were created or analysed during this review, therefore data sharing is not applicable to this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ‘Regieorgaan SIA’, part of the Dutch Society for Scientific Research [HBOPD.2018.05.18]. The other authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
There are no human participants in this article.
Informed consent
Informed consent is not required.