
Abstract
Parents of young adults with chronic disease are important stakeholders in their child’s transition from pediatric to adult care. There remains a gap in characterizing the parent experience during transition. This study describes the experiences of 13 mothers of young adults with inflammatory bowel disease during their child’s transition. Most parents expressed fear and sadness about their child transitioning. Themes relating to involvement in their child’s adult care included: direct involvement (sub-themes: disease management; logistics of care); and indirect involvement. Reasons for involvement included themes of parent’s feelings and child’s circumstances. Themes of involvement were discussed in terms of previous research on parenting of children with chronic disease. We suggest that future efforts focus on improving empathy and understanding toward parents of transitioning children and providing resources on how they can best support their child during transition and transfer to adult care.
Keywords
Introduction
Chronic diseases diagnosed in childhood can place a huge burden on a child’s family. Typically, parents and caregivers become their child’s advocates and take on disease management responsibility (Kluthe et al., 2018). These responsibilities may include arranging appointments, managing medications, and communicating with their child’s medical team. Due to these additional parenting demands, parents of children with chronic diseases may experience stress related to managing their child’s health (Cousino and Hazen, 2013; Plevinsky et al., 2018). This stress has been associated with greater family conflict and depressive symptoms in parents and their children (Guilfoyle et al., 2014; Helgeson et al., 2012; Patton et al., 2011).
Transition refers to “the purposeful, planned movement” from pediatric to adult care in a manner that occurs gradually over time (Blum et al., 1993). Transition begins before and continues after transfer to adult care. During transition, young adults are expected to gain independence and take responsibility for disease management. This is facilitated in part by parents who adapt their role, letting their child take over disease management responsibilities, and in this way, promote their child’s independence (Heath et al., 2017). As a result, parents are recognized as vital stakeholders in their child’s transition.
Difficulties faced by patients during transition have been reported in the literature (Heery et al., 2015); however, few studies have focused on parents’ perspectives on their child’s transition or parents’ descriptions of their involvement in their child’s health care. We conducted this research to facilitate a better understanding of parents’ perspectives and experiences to inform the development of better ways to support parents of young adults with chronic disease as their child transitions.
This study specifically focuses on parents of young adults with inflammatory bowel diseases (IBD), including Crohn’s disease and ulcerative colitis; these are chronic digestive diseases characterized by unpredictable and remitting symptoms of abdominal pain, cramps, and diarrhea requiring medical and/or surgical treatments to induce and maintain remission (Calkins and Mendeloff, 1986). Patients with IBD experience impaired psychological wellbeing and health-related quality of life compared to the general population (Bernklev et al., 2005; Häuser et al., 2011). Parents of children with chronic diseases play a pivotal role in their child’s care through providing support and encouragement to their child, while also communicating with their child’s care team and making health decisions. Due to the unpredictable symptoms and cycle of disease flare-up and remission characteristic of IBD, the role of parents in their young adult child’s IBD care may be amplified when compared to other chronic diseases. Currently ~25% of patients are diagnosed before age 18 (Carroll et al., 2019) and the incidence of IBD childhood diagnoses is increasing, therefore, transition care is an important concern in the IBD field. This study extrapolates insights on parental experience in IBD transition that may be similar to parental involvement in both the transition from pediatric to adult care for other chronic diseases and in their child’s other life transitions (e.g. moving out, starting post-secondary education). Ultimately, the goal of this study is to inform future research into supporting parents through their child’s transitions, specifically contributing to a seamless transition of care.
Methods
Study design
This study used a qualitative descriptive design with realist assumptions as part of a larger study on transition outcomes, for which patients (young adults), parents, and health care providers were interviewed to define transition success (Bihari et al., 2022). Qualitative description stays close to the data to create a comprehensive summary of the phenomenon under investigation (Sandelowski, 2000). This method allowed us to address the research question: “What are the perspectives and experiences of parents of young adults with inflammatory bowel disease who have transitioned from pediatric to adult care?” This overall research question encompasses the following sub-questions:
What are parent’s feelings and opinions about their child transitioning and their child’s preparedness to transition?
What are parent’s hopes and expectations for their child’s transition?
What are parent’s perceptions of their involvement in their child’s adult care?
What are parent’s opinions of adult care?
Are there differences in how parents and their child rate their transition?
Quantitative Likert scales assessed differences in how parents and young adults rated their child’s/their transition on a scale of 1–5, with 1 “being not well there were issues” to 5 being “excellent with no issues.” An additional scale was created to ask parents “to rate their involvement in their child’s transition on a scale of 1–5, with 1 being “not involved” to 5 being “maximum involvement.” This involvement scale was asked to parents to provide insight into whether parents viewed their involvement as being minimal or maximum.
This study was conducted by a graduate student (A.B). This study has been approved by the institutional review boards at the participating sites. All parents were compensated with a $15 electronic gift card for their contribution. The Standards for Reporting Qualitative Research (SRQR) checklist was used in the reporting of this study and is located within the Supplemental Material (O’Brien et al., 2014).
Setting, recruitment, and data collection
Young adults with IBD were recruited from IBD clinics in Alberta, Canada for participation in our larger study if they met the following criteria: had their first appointment in adult care 1–2 years prior to study participation; diagnosed with IBD at least a year prior to first appointment in adult care; no comorbidities unrelated to IBD. Young adults are generally referred to the adult IBD clinic around their 18th birthday. Parents were recruited through snowball sampling: Young adults invited for study participation were informed that parents were also being recruited and asked to have their parent contact us if they were interested in participating.
Parents who expressed interest in the study received a recruitment letter, study information sheet, and consent form. Prior to the start of the interview, verbal informed consent was obtained and demographic information was collected, which included information on maternal education, child’s IBD diagnosis/their sex/age at diagnosis, number of children, and whether they had a chronic disease themselves. Interviews were conducted between June 2020 and March 2021 following a semi-structured interview guide through Google Meet™ or telephone, according to participant preference. The interview guide was developed through collaboration and discussions with a pediatric and adult gastroenterologist (E.W, K.I.K). These initial discussions served to brainstorm topics and questions to be covered during the interview. Additional collaboration with an expert in qualitative research served to adjust the wording and order of question to be in line with the study’s aims.
Interview questions relevant to this study included asking parents to describe their feelings about transition, their views on their child’s preparedness for transition, any hopes and expectations they had about their child’s transition, opinions on adult care, and their involvement during transition. Interviews were audio-recorded, assigned an anonymous study ID, and transcribed verbatim by (A.B).
Participants
All 13 parents referred by their young adult child participated in semi-structured interviews. Data saturation was achieved for the aims of our larger study with the 13 parents. These interviews were re-analyzed for the current aims presented in this study.
The median interview length was 35 minutes (range, 28–62; IQR, 29–40). 100% were mothers of children with IBD and one mother had a chronic disease themselves (chronic kidney disease). Parent demographics are outlined in Table 1. Representative quotes from each theme described below are outlined in Figures 1 and 2.
Parent demographics.
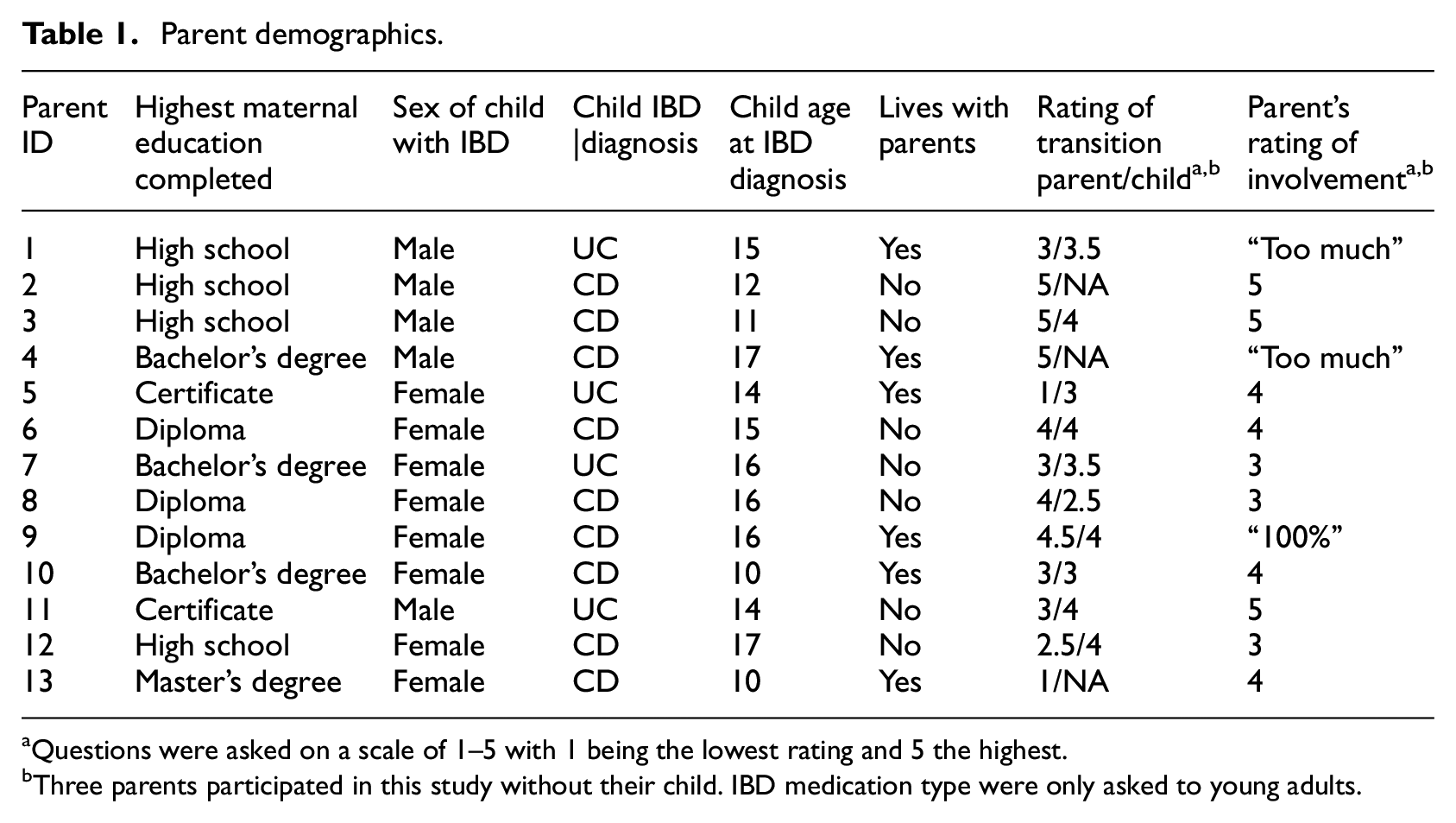
Questions were asked on a scale of 1–5 with 1 being the lowest rating and 5 the highest.
Three parents participated in this study without their child. IBD medication type were only asked to young adults.
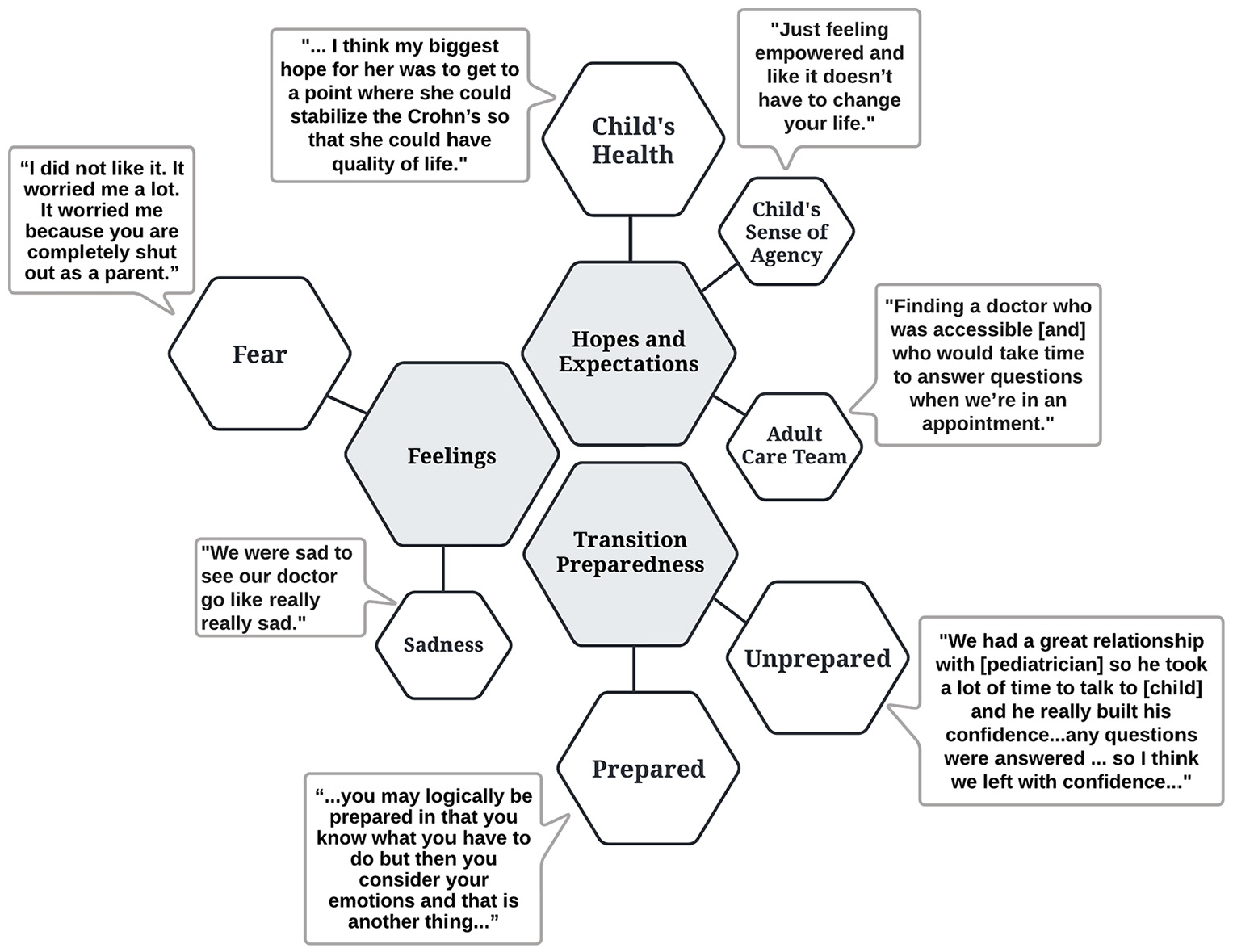
Parental feelings for transition, opinion on child’s preparedness, and hopes and expectations for their child’s transition: themes with representative quotes.
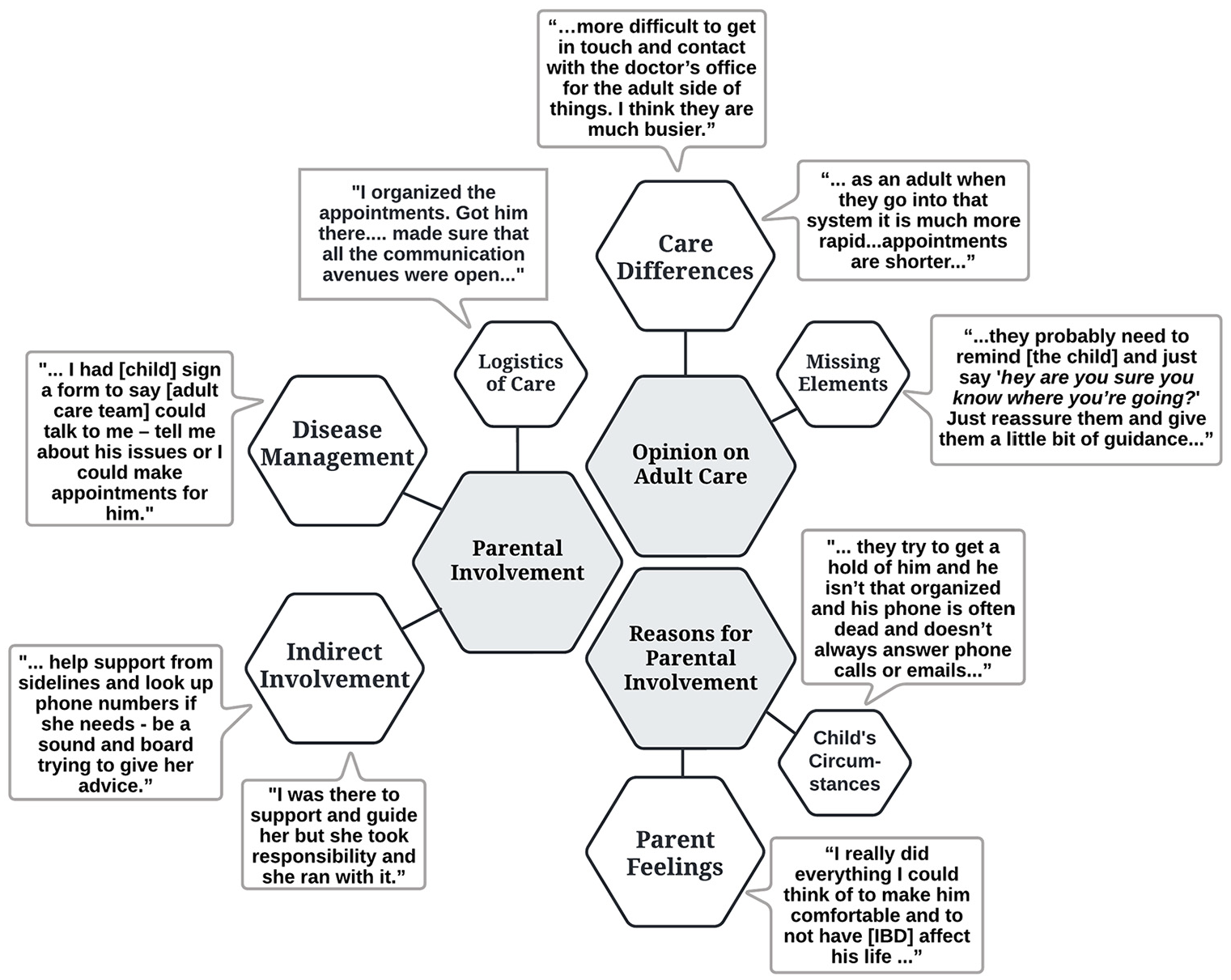
Themes and representative quotes regarding parental involvement in adult care and general opinions on adult care.
Data analysis
A.B used the inductive approach of latent content analysis to identify, code, and categorize patterns within the data to create themes using NVivo R1™ (2020) (Graneheim and Lundman, 2004; Mayan, 2009). The analysis was led by A.B who also conducted all interviews. Prior to the coding of interviews, A.B re-familiarized herself with the interviews through re-reading of interview transcripts and field notes. During the familiarization process, prominent domains related to the research question were identified. Within each domain, A.B then proceeded to initially coded the interviews, while then re-coding previous interviews when new codes emerged. Codes were then grouped into categories based on commonalities between codes. Themes were then identified through connecting similarities of deeper meaning and interpretations of the categories together. Ongoing discussions with the research team at each stage of the data analysis process served to assist in the formation of categories and the emergence of themes.
Positionality and trustworthiness
Best practices in qualitative research require researchers to practice reflexivity to inform their positionality and how this may contribute to data interpretations (Gary and Holmes, 2020). In alignment with this, the first author (A.B) is a white female in her 20s who conducted this study during her PhD and had previously taken a course on qualitative research prior to designing this study. A.B approached this research mainly from an outsider perspective, not having experience as a parent, but having experience gaining independence from parents by moving away from family for post-secondary schooling immediately upon entering adulthood. Thus, throughout the research process A.B found herself connecting with the participant’s stories and reflecting on her own experience entering adulthood.
Further, A.B played a central role in both conducting and analyzing the parent interviews. At the end of one parent interview, one parent expressed gratitude toward A.B for allowing them the opportunity to talk about their child’s transition experience. From this interview, A.B recognized the importance in providing parents with the opportunity to speak about their own experience in their child’s transition and developed the belief of understanding their experience to not only better support parents, but also parents in their child’s transition. To provide justice for the parents’ experiences and opinions on transition, the analysis for the current study was conducted. A challenge face by A.B throughout the analysis process was balancing the desire to provide a voice to parents’ experiences, while also staying close to the data and limiting the influence of this desire onto the data. Regular discussions with the senior author (K.I.K) served as a debriefing meeting to promote self-reflexivity and discussions focused on the data and ensuring the absence of A.B’s positionality in the data analysis. Additionally, A.B discussed results with the research team, which included an epidemiologist, a pediatric gastroenterologist, and two adult gastroenterologists with expertise caring for transitioning young adults. Discussions with the whole research team served as an additional step to ensure both plausibility of themes and that any preconceived bias/opinions resulting from A.B’s positionality did not influence the data.
Further efforts were made to establish trustworthiness within the data in addition to ongoing self-reflexivity and peer-debriefing as mentioned above (Lincoln and Guba, 1986). These efforts included verifying data by checking with participants about whether their responses were captured accurately throughout the interview, conducting field notes after each interview, and creating an audit trail of decisions, choices, and insights made throughout the research process.
Results
Themes of parent experience are presented under domain summaries that relate to the specific questions asked to parents. The following domain summaries included: parent feelings, parents’ opinions on child preparedness, parent and child comparison of transition characterization, hopes and expectations, parental involvement, and opinions on adult care.
Parent feelings
When parents were asked how they felt about the idea of their child transitioning from pediatric to adult care, parents reported fear (7/13), sadness (5/13), and neutral feelings (2/13). Fear encompassed feelings of worry, nervousness, concern, being scared, and overwhelmed. Two parents described fear about how their child would be able to afford medications. Some parents felt nervous about no longer being the primary contact for their child’s care and worried that the level of care would be different. One parent described feeling nervous because “… [child’s adult care team] aren’t talking to you anymore and they are talking to [child] and he’s an 18-year-old boy who is not talking to his mom because teenagers, they don’t want to talk to mom or face what is actually happening.” Sadness included additional feelings of grief, helplessness, and guilt. Two parents mentioned being sad to leave pediatric care, while other parents mentioned feeling helplessness, guilt, and grief because their child had to deal with their disease and transitioning. As seen in the following quote, the parent describes the emotional impact that transition had on themselves and their child: “[Child] knew why we had to do this but emotionally, it is difficult when you formed other attachments [with pediatric team] so of course I felt for her.” The two parents who indicated neutral feelings around transition, mentioned being at ease and feeling no distress.
Parent’s opinions on child’s preparedness
Parents were split on feelings of their child being prepared (six prepared, six unprepared, and one undecided). Parents described preparedness by their child understanding the steps of transitioning, being mentally prepared, and having all their questions answered by their pediatric care team. One parent described preparedness as “… [the pediatric team] had [child] fully informed and they did talk to us and any questions they would always give us an answer and if they didn’t know they would find [out].” Parents who believed their child was unprepared, stated that their child was too young or not mentally prepared. Some parents described differences in perceptions of preparedness between themselves and their child, with one parent saying, “I think [child] thought she was [prepared], but I don’t believe she was.” One parent thought that transfer to adult care occurred too soon after diagnosis and coming to terms with the diagnosis as described in the following quote: “… [child] got transferred pretty quickly after [diagnosis] so it was more of a timing issue where he was just getting used to the fact his whole life is changing and then having to gain new relationships and figure out new doctors.”
Parent and child comparison of transition characterization
When parents were asked to characterize their child’s transition on a scale from 1 to 5, with 1 being “not well, there were issues” to 5 being “excellent with no issues,” the median rating was 3. When the young adults were asked the same question about their transition, the median was 3.75. Figure 3 depicts transition ratings of 10 parents matched with that of their child’s. Matching ratings are unavailable for three parents as their child referred their parent to the study but declined to participate in the larger study themselves.
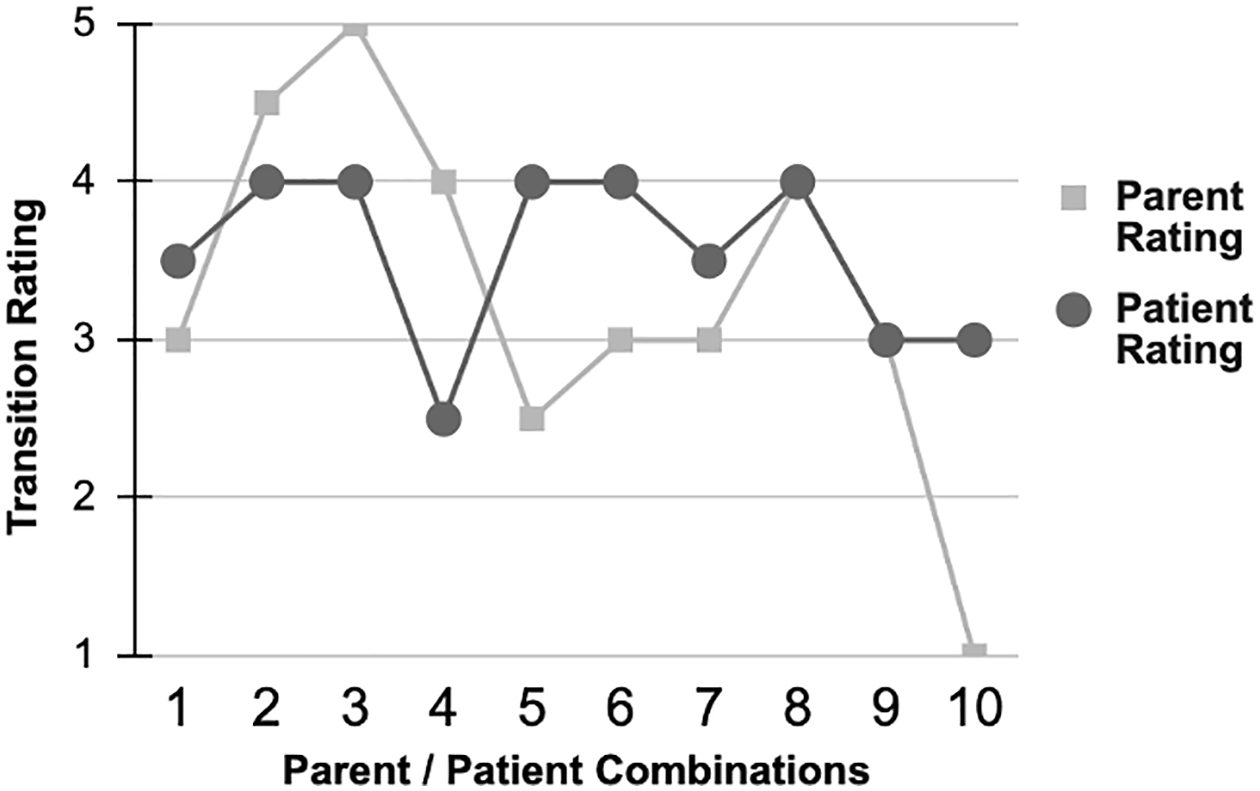
Transition ratings of parents matched with rating of their child.
Hopes and expectations
Hopes and expectations that parents expressed in relation to their child’s transition grouped into three themes: child’s health (6/13); child’s sense of agency (5/13); adult care team (4/13). The theme of child’s health was characterized by expressions of hope that their child would feel well, experience disease stability, avoid surgery, and be on an effective medication. For the theme of child’s sense of agency, parents expressed the hope that their child would feel heard and empowered, be comfortable taking responsibility, and maintain a high quality of life. One parent described their hopes and expectations as “I just wanted [child] to have as much of a regular life as she can.” The theme of adult care team was characterized by hopes that the adult care team would be accessible, answer questions, not rush their child, and take their child seriously. In the following quote, one parent describes their hopes for their child’s transition as one where “ … [child] would be able to have a good doctor that she knows she can go to - especially if she had flare ups or any issues that she felt confident that would provide that care.”
Parental involvement
Rating of parental involvement
Parents were asked to rate their involvement during their child’s transition on a scale from 1 to 5 with 1 being “not involved at all” to 5 being “very involved.” Three parents rated their involvement as a 3, four rated their involvement as a 4, and six indicated maximum involvement (three selected the rating of ‘5’, and three indicated that they were involved “100%” or “too much.”) Of these six parents with maximum involvement, five were parents of males; three parents indicated their child lived with them at time of interview.
Parents were additionally asked to describe the ways that they were involved in their child’s transition and when applicable, how they continue to be involved in their child’s adult care. Two themes to emerge were direct involvement and indirect involvement.
Theme: Direct involvement
Descriptions of how parents were directly involved in their child’s care after transfer grouped into two sub-themes: care logistics; and disease management. Logistics included parents driving their child to appointments and helping them with their medication insurance because as one parent described “… if [child] didn’t apply for [insurance] promptly, it would just be a nightmare with finances, so [parent] did have to help [child] with that because it was just too risky to not have that coverage.” One parent described having their child complete a consent form so the parent would be able to obtain all their child’s health information. Of the 11 parents who reported being actively involved in the disease management aspect of adult care, five only attended the first adult care appointment. The remaining six parents attended the first appointment and remained involved throughout adult care, in addition to attending the first appointment. Involvement included attending and making appointments and/or communicating on their child’s behalf and obtaining medication for their child. Three of these parents expressed the desire to be more actively involved in their child’s adult care. Of the six parents who remained directly involved in their child’s care through disease management, five were parents of males; four indicated their child didn’t live with them; three had children diagnosed within the age range of 15–17.
Theme: Indirect involvement
Seven parents’ descriptions of their involvement formed a theme of indirect involvement. These parents indicated that they acted as a support system and remained up to date on their child’s care. Parents mentioned being available to engage in discussions about care with their child, while encouraging and guiding them when asked. In the following quote, the parent describes their level of involvement in their child’s care as “There have been times that we have discussed things that she probably should get looked at or talked about, but for the most part she does all of her appointments on her own and her medications and all that stuff.”
Most parents who remained indirectly involved in their child’s care stated explicitly that they stopped being involved shortly after the first adult care appointment. Others stopped being involved once their child moved out of their house or turned 18; two parents stated that their child told them that they wanted to handle their care themselves. Parents who were indirectly involved in their child’s care often described their child as responsible, independent, and/or mature. They also mentioned that they instilled independence in their child at a young age, and their child showed responsibility in pediatric care. Of the seven parents who described indirect involvement, five were parents of females; four had children diagnosed between 15 and 17.
Reasons for parental involvement
When parents were asked about the reasons for their direct involvement in their child’s adult care, two themes arose: parents’ feelings and child’s circumstances. Five parents indicated that they were involved because they felt transition was a lot to handle alone, and they wanted to help and protect their child because they felt this was their parental role as described by one parent who mentioned that “you still want to fix everything as a mom.” Parents also indicated that their involvement was convenient and made things easier; some parents mentioned that they felt guilty about their child having to manage a chronic disease. One parent described their involvement as “… [child] is the baby of the family and he’s a boy and I just did it for him because a lot of times I would have it all figured out like by the time he got home from school or by the time he got out of bed in the morning. It was so much easier.” Four parents mentioned reasons relating to their child’s circumstances. This theme included characterizations of their child as too busy with friends and school, as well as personality traits such as not being proactive, organized, or responsible. In the following quote, the parent describes feeling that their child is too busy to manage their disease “… I just feel like because [child] was too busy with his friends – hanging out with his friends you know planning graduation and everything to not really want to think about doctors and meds and infusions and everything else he had to go for.”
Opinions on adult care
When parents were asked whether they felt there was anything unexpected about their child’s transition to adult care, seven parents mentioned the theme of care differences between the adult and pediatric system. Parents felt that the adult care system was busier, noting increased difficulty getting in contact with the adult care doctor and less time with them during appointments. One parent described care differences as “Where [the pediatric system] will check on you. They will call and do follow up calls where [adult care] it is not that.”
Five parents commented on the theme of missing elements in adult care. This included follow up, guidance, and support from the adult care team resulting from understanding the child was coming from a different system. Three parents felt that a mentorship program with previously transitioned children would have been valuable for their child. In the following quote, a parent describes having access to the pediatric team while the child is in adult care: “I do think if there would have been again that buffer where okay you’re 18 now but now for the next year you have support. You can call us at any time if you have any questions. If you are not sure about something because again I couldn’t really offer much because I didn’t know the system.”
Discussion
In exploring how parents perceive and experience their child’s transition from pediatric to adult IBD care, we discovered that many parents experience negative feelings. This is consistent with a study that conducted interviews with parents of young adults with neurological disorders to describe their perceptions of their child’s transition (Davies et al., 2011). The investigators found that most parents experienced a sense of loss, fear, and uncertainty when transitioning. Parents in the neurological study spoke about losing the trusting relationship that they had with their pediatric care team. This theme of relationship loss is consistent with our parents feeling sad and fearful about their child leaving pediatrics. In the neurological study, parents spoke about how they felt little guidance and support from the pediatric team. Although the theme of inadequate support from the pediatric team did not directly emerge from our data, 6 of the 13 parents interviewed indicated that their child was unprepared to transition.
Our findings of parents’ negative perceptions of adult care are consistent with a study of transition for chronic diseases conducted in Denmark (Thomsen et al., 2023). The Danish investigators reported that parents perceived pediatric clinics as taking their time with the patient and showing care, whereas the perceptions of adult care were that the patient felt like just a number and care visits had limited time. In the Danish study, negative perceptions of adult care were especially common in parents whose child had not yet transferred. Our study suggests that some Canadian parents of children with IBD still have negative perceptions of adult care based on their child’s transition experience.
Figure 3 shows differences in how parents and their child view the transition experience and thus, suggests the need to incorporate perspectives of these stakeholders when preparing to transition as only two parent-child dyads provided the same rating. The observation that nearly half of parents indicated that their child was unprepared to transition suggests a potential disconnect between providers and parents in preparing young adults. We suggest that future efforts focus on engaging parents when preparing young adults to transition in a way that considers parents’ hopes and expectations for adult care. For example, the adult care team could make an extra effort to be accessible to transitioning young adults, answer their questions, and empower them in their care.
Our findings can be understood in the context of existing literature on the role parents of children with a pediatric diagnosis of a chronic disease play in their child’s health care. In focus groups conducted with parents of young adults with brittle asthma, osteogenesis imperfecta, and epilepsy aimed at describing their role during transition, protection of their child was the major concern (Shaw et al., 2021). Some parents emphasized the need to “let go” and let their child take on responsibility, while they shifted to more of a supportive role. This focus group study additionally found that “letting go” was often at odds with the need to protect the child’s health and that when the health risk was lower, parents felt more confident to encourage independence. These results match our observations, in which most parents reported remaining involved as a support system by attending the first appointment in adult care, and being encouraging, supportive, and ready to engage in discussions. Additionally, in our study, parents who remained actively involved in their child’s care similarly indicated that they felt a need to protect their child during transition because there could be negative health impacts if their child neglected their care.
Our study describes parental involvement in their child’s care following transition, as well as parents’ reasons for remaining actively involved. Understanding how and why some parents remain actively involved in their child’s care provides insights for how best to support parents in transferring disease management responsibility to their child. Although most parents in our study reported indirect involvement in their child’s care (e.g. acting as a support system), some parents remained actively involved. Our observation that most parents who remained actively involved in their child’s disease management rated their involvement as maximal suggests that some parents may sense that they are too involved in their child’s care but are reluctant to give up control. This observation reveals the value of investigating parents’ reasons for involvement and of future research focused on finding ways to support them through their child’s transition to better achieve the hopes they have for their children. While our study size was small, our finding that five out of six parents who remained directly involved in their young adult’s child’s care were parents of males suggests that ongoing involvement may be more common in parents of males. Further, five of the seven parents who described their involvement in their young adult child’s care as being indirect were parents to females. Our observations of the differences between direct and indirect parental involvement by their child’s gender, provides a rationale for future studies to examine whether factors underlying parental involvement differs according to their child’s sex or gender.
Woodgate et al. (2015) described what they called “intense parenting” in the context of raising a child with a complex illness. In their description, intense parenting includes needing to be seen as the “good parent” (e.g. maintaining their child’s health and quality of life) and assuming multiple roles such as health care provider and advocate for maintaining their child’s health and well-being. Woodgate et al. also reported that parents had minimal time for other “normal” needs (e.g. social life or time with partner). Woodgate et al.’s observations help explain how identities of parents of children with chronic diseases may be shaped by roles relating to their child’s disease management and their own reduced time for engaging in normal life events; such parents may be reluctant to give up these roles and develop new roles not centered on caring for their child. Although our study did not look at parent’s identity as being shaped by their children, we did find that some parents remained actively involved in their child’s adult care; thus, suggesting that these parents may have been reluctant to give up their role as their child’s advocate. Future research should explore the connection between intense parenting and continued involvement in the child’s disease management following transition.
Peeters et al. (2014) interviewed and compared responses of young adults with chronic diseases and their parents. Peeters et al. reported that when young adults were unable to take on full disease self-management, parents expressed little confidence in their child, remained protective, and had difficulty transferring disease management responsibilities to their child. This interpretation compliments our observation that some parents who remained actively involved in their child’s care indicated that they did not feel their child could take on the responsibility of their own disease management. It should be noted that our study design does not permit assessment of the causal direction of the association between parents’ active engagement and their child’s lack of independence. Furthermore, because our study was limited to parents whose child transferred no more than 2 years ago, future research can focus on understanding how parental involvement progresses and changes as the child ages.
The transition from pediatric to adult care is a complex process with patients playing a central role in transition. Hobart and Phan (2019) emphasized the need for a balance between patient self-management and parent’s continuous support and engagement throughout the transition process. To achieve this balance, a partnership between clinicians and parents is necessary where both groups encourage self-advocacy, decision making in the patient as they transition. The results of our study suggests that while parents continue being supportive once in adult care, some parents are unable to complete the skill transfer started in pediatric care. Further, while is it established that transition is a vulnerable time for patients and preparation for transition is necessary, our findings suggest that it is also a vulnerable time for parents.
A study limitation is that it only included mothers’ perspectives; however, participation of primarily mothers in IBD transition research is consistent in the literature (Guilfoyle et al., 2014; Plevinsky et al., 2018). One possible explanation is that mothers are more involved in their children’s health care than other types of caregivers. This hypothesis was corroborated by Ingerski et al. (2010) who reported that mothers of children with IBD were more likely than fathers to ensure that their child had IBD medications and had taken them. Study generalizability may be further limited by the recruitment of patients from clinics affiliated with academic hospitals. Within the patient population targeted for recruitment, those whose parents agreed to be interviewed may not be representative of all parents of targeted patients; in particular, the observation that all interviewed parents rated their involvement as at least 3 on a scale from 1 (lowest) to 5 (highest) may reflect a greater willingness of more actively involved parents to participate in research pertaining to their child’s health care.
Another limitation is that the young adults were not asked to rate their parents’ involvement so only the parents’ self-assessments were available. Further, these interviews were conducted with parents whose child had already transitioned. Because parents were asked to reflect on the time when their child was transitioning to adult care, there is a potential for recall error; however, transition is a significant life event, and as such recall is likely to be fairly accurate (Bhandari and Wagner, 2006). Importantly, this study selected parents of young adults who transferred within the preceding 2 years to promote accurate recall since the event was relatively recent. Ascertainment of parents’ hopes and expectations of transition after their child completed transfer may have led to differential recall error: parents with a negative experience may have been more likely to recall hopes and expectations more accurately than parents with a positive experience. In our study, parents were asked whether they had a chronic disease themselves. We wanted to account for the potential that parents with a chronic disease themselves may be more familiar with the health care system, and thus more involved in the logistics of their young adult child’s care. Due to only one parent having a chronic disease, patterns between parental involvement and parent chronic disease status were unable to be further explored.
The strength of this study is that it describes parental involvement in their child’s health care along with reasons given for their level of involvement. It draws attention to parents’ hopes and expectations for their child’s transition and their perspectives on their child’s preparedness and transition experience as well as their general opinions on distinctions between pediatric and adult care. Our description of why parents remain involved in their child’s care leads us to suggest that future research focus on providing support to parents whose children are transitioning so they can “let go” and fully transfer disease management responsibility to their child. Additionally, we highlight the need to consult parents with a transitioning child about what preparedness looks like to them along with their hopes and expectations for their child. Future studies could focus on partnering with parents to design transition interventions for patients aimed at facilitating a successful transition, while also addressing and supporting parents through transition.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241237861 – Supplemental material for Letting go of control: A qualitative descriptive study exploring parents’ perspectives on their child’s transition from pediatric to adult care for inflammatory bowel disease
Supplemental material, sj-docx-1-hpq-10.1177_13591053241237861 for Letting go of control: A qualitative descriptive study exploring parents’ perspectives on their child’s transition from pediatric to adult care for inflammatory bowel disease by Allison Bihari, Karen J Goodman, Eytan Wine, Cynthia H Seow and Karen I Kroeker in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to express our gratitude to all study participants. We would also like to thank Nima Hamidi for his help in patient recruitment and Kate Storey who provided advice on the development of interview guides. We are grateful for the opportunity to present preliminary results of this study as a poster of distinction at the 6th International Symposium on Paediatric Inflammatory Bowel Disease (PIBD) in Edinburgh, Scotland.
Author contributions
A.B: Study design, data collection, data analysis, and writing of manuscript; K.J.G: Study design and revisions of manuscript; E.W: Study design and revisions of manuscript; C.H.S: Participant recruitment and revisions of manuscript; K.I.K: Study design, data collection, and revisions of manuscript.
Data sharing statement
The data underlying this article will be shared on reasonable request to the corresponding author. The interview guide used in this study is available in the supplementary material of our article, “defining transition success for young adults with inflammatory bowel disease according to patients, parents and health care providers,” at ![]() [doi].
[doi].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by research ethics board at both participating sites (University of Alberta: Pro00099184; University of Calgary: REB20-0979).
Informed consent
All study participants provided informed verbal consent prior to study participation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.