
Abstract
Much research has adopted a deficits-based approach to chronic pain, neglecting the study of flourishing. Using a Q-methodological framework, this study sought to explore how individuals experience, understand and perceive flourishing in the context of young people living with chronic pain. Fifty-four individuals completed a Q-sorting task, indicating their level of agreement and disagreement with 52 statements. Q-analysis generated three factors that represented clear viewpoints of participants: ‘Pain is not a barrier to flourishing’, ‘Adapting to a new life’ and ‘Adopting a positive perspective’. Factors expressed the viewpoints that flexibility is key to enjoying life despite chronic pain, while resilience, management of stressors, acceptance and problem-solving may be required to flourish with chronic pain. Participants’ understanding of flourishing also focused on the appreciation and enjoyment of life and achievements. This study provides a useful contribution towards furthering our understanding of flourishing in young people living with chronic pain.
Introduction
Chronic pain (persistent or recurrent pain lasting longer than 3 months (Treede et al., 2015)) is prevalent among children and young people, with 11%–38% of this group reporting the experience of chronic pain (Fisher and Palermo, 2016; King et al., 2011). However, prevalence may vary substantially due to different conditions (e.g. headache: 8%–83%; musculoskeletal pain: 4%–40%; abdominal pain: 4%–53%) (King et al., 2011). A small yet notable proportion of young people may be disabled by their pain and struggle to live with chronic pain in their everyday lives (Gauntlett-Gilbert and Eccleston, 2007; Vervoort et al., 2014).
Despite this adversity, there is evidence to suggest that some young people can function well while living with chronic pain (Goubert and Trompetter, 2017; Trompetter et al., 2019), adapting in a positive way or flourishing in their experience of pain (Soltani et al., 2018; Umberger and Risko, 2016). Previous literature suggests that young people may feel developmentally ahead of their healthy peers in areas such as problem solving (Eccleston et al., 2008) and report aspects of enhanced maturity, emotional development and growth (Jordan et al., 2018) due to living with chronic pain. However, comparatively little is known about this as most research adopts a deficits-based approach to pain treatment, with a focus on addressing problems as they arise.
Beyond chronic pain, young people have reported positive outcomes in other areas of adversity, such as cancer. Young people have reported the reappraisal of priorities in life, closer interpersonal relationships, an enhancement in spirituality and an increased sense of purpose as positive areas of benefit due to living with cancer (Phipps et al., 2007). Additionally, a study by Barakat et al. (2006) found evidence of growth in areas such as treatment of others, plans for the future and philosophy of life, in young cancer survivors. However, it must be noted that cancer populations differ from chronic pain populations in that cancer is a believed and often visible condition, which is not always the case for pain.
While there is no single definition of flourishing in the chronic pain literature (Witten et al., 2019), flourishing can be conceptualized as an umbrella term that moves beyond the mere absence of negative outcomes to encompass high levels of psychological, social and emotional well-being (Keyes, 2002, 2005); a sense of ‘life going well’ (Huppert and So, 2013); positive changes or outcomes (e.g. growth) (Jordan et al., 2018) and constructs (e.g. benefit finding, resilience) (Soltani et al., 2018), either as a result of, or despite, chronic pain. Little is known about how flourishing is perceived and understood by young people living with chronic pain and those who care for them, particularly with regard to positive growth, adaptation, strengths and resilience qualities (Cartwright et al., 2015; Cousins et al., 2015; Noel et al., 2016). Expanding on this knowledge will provide novel insights into the role of flourishing in relation to the experience of chronic pain and will address a knowledge gap concerning how flourishing is understood among these populations.
The aim of this study was, therefore, to investigate how young people living with chronic pain perceive, understand and experience flourishing in the context of chronic pain. We also investigated flourishing in young people with chronic pain from the perspectives of parents who care for their children and healthcare professionals providing treatment to these young people, in order to consider key potential sources of social influence within the biopsychosocial framework in which chronic pain is experienced (Gatchel et al., 2007; Hadjistavropoulos et al., 2011).
Methodology
Study design
We selected a Q-methodological framework to investigate our research aims. Q-methodology is a robust approach that facilitates the exploration of subjectivity in relation to a particular topic (Herrington and Coogan, 2011). This approach is unique in its ability to capture shared participant perspectives and patterns from multiple voices, while also detecting subtle differences between viewpoints (Watts and Stenner, 2005). Viewpoints are obtained using a Q-sorting task, whereby individuals are presented with a set of statements pertaining to the topic and are instructed to indicate their level of agreement or disagreement with each item. Q-methodology adopts a mixed-methodological approach, as it involves a quantitative by-person factor analysis of each completed Q-sort and a qualitative interpretation of each resultant factor (Herrington and Coogan, 2011; McParland et al., 2011). Q-methodology has successfully been used in previous studies investigating the experience of chronic pain (McParland et al., 2011; Wratten et al., 2019).
Development of the Q-set
The items for the Q-sorting task are known as the Q-set. Statements for the Q-set are generated from a concourse of statements drawn from various standpoints surrounding the topic area (Herrington and Coogan, 2011). We sought to provide a balanced perspective by including statements that were specifically related to positive outcomes in chronic pain, as well as those that were more general to the chronic pain experience. Our candidate statements for the Q-set were compiled using multiple, diverse sources, as is common practice for this methodological approach (McParland et al., 2011). First, the first author (RP) examined relevant literature (e.g. Cartwright et al., 2015; Parsons et al., 2022; Soltani et al., 2018; Umberger and Risko, 2016) to search for potential thought-provoking statements and create an initial statement list. Second, we searched through pain-related websites and internet forums to identify any additional statements related to flourishing and positivity in chronic pain that could be added to the initial list. This involved scouring for keywords and concepts that young people living with chronic pain and those around them may be using and discussing online. Third, written comments on the initial statement list and suggestions for further items were invited from five United Kingdom-based colleagues conducting research in the field of chronic pain, one young person living with chronic pain, two parents of young people living with chronic pain and two healthcare professionals who work with these young people. We subsequently arranged the full list of candidate statements (131 in total) into categories and subcategories based on similarities, as suggested by Herrington and Coogan (2011). Statements within each category were then checked for duplicates (which were subsequently removed) and similar statements were merged. Finally, the co-authors thoroughly discussed the candidate statements to ensure additional rigour, before the statements were revised into the final Q-set. This consisted of 52 items that were considered to be thought-provoking, intelligible and balanced (McParland et al., 2011) (see Supplemental Appendix A). This was in line with the general guidance of 40–80 total statements being considered satisfactory for Q-methodology (Watts and Stenner, 2005).
Baseline demographic questionnaires
Young people were asked to complete self-report questionnaires relating to key aspects of their chronic pain condition and its management. This included an indication of pain intensity, pain duration and pain location: ‘How would you rate your level of pain over the past week?’ (10-point numerical scale; 1 = No pain, 10 = Worst pain ever); ‘How long have you had your pain symptoms?’ (Text boxes to enter years and months); ‘Where is the pain usually located?’ (Multiple choice fields). Parent participants answered the same pain-related questions, but from their perspective of their child living with chronic pain, as well as questions about their own potential chronic pain experience. In addition to standard demographic information, healthcare professional participants provided further information relating to their experience of working with patients who have chronic pain: ‘How long have you been in clinical practice?’ (Text boxes to enter years and months); ‘How long have you worked with patients with chronic pain?’ (Text boxes to enter years and months); ‘Do you have a history of chronic pain yourself?’ (Yes, No).
Participants
As Q-methodological studies typically comprise samples of between 40 and 60 participants (Watts and Stenner, 2005), we sought to recruit approximately 60 participants (20 young people, 20 parents and 20 healthcare professionals) to provide a diverse range of subjective viewpoints and experiences relating to our research aims (Watts and Stenner, 2005). All participants were required to: have the ability to provide informed consent/assent, complete the tasks, have access to a non-touchscreen device with internet connectivity. Additional requirements were that young people had to be aged 11–24 years and living with persistent or recurring chronic pain (minimum duration of 3 months; Treede et al., 2015), while parents were required to have a child with chronic pain meeting the above requirements. Finally, healthcare professionals were required to have worked with young patients with chronic pain.
Participants comprised a sub-set of young people and their parents who had been recruited from a previous National Health Service (United Kingdom health service) ethically-approved study that sought to investigate relationships between flourishing variables and other pain-related outcomes. These participants had previously expressed interest in participating in further research. These participants had been recruited worldwide through various sources, including pain clinics based in the United Kingdom, pain charities and social media platforms (primarily Facebook and Twitter/X). Healthcare professionals were recruited specifically for this study through established networks (e.g. British Pain Society), as well as through social media (e.g. Twitter/X, Facebook) and via email.
Overall, 67 individuals in total (22 young people, 20 parents and 25 healthcare professionals) expressed an interest in participating in this Q-methodological study, with 54 individuals (20 young people, 14 parents and 20 healthcare professionals) ultimately taking part. Young people (18 female, 2 males (one of whom noted they are trans male)) were aged 11–24 years (M = 18.15, SD = 3.34) and had lived with chronic pain for 1–13 years (M = 5.25, SD = 3.09). Parent participants (all female) were aged 42–57 years (M = 50.07, SD = 4.48) and had a child living with chronic pain for 0.5–10.08 years (M = 3.89, SD = 2.59), while healthcare professional participants (16 female, 4 male) were aged 25–58 years (M = 43.45, SD = 7.85) and had worked with chronic pain patients for 1.42–31 years (M = 11.44, SD = 6.94). See Supplemental Appendix B for full participant characteristics.
Procedure
The University Psychology Research Ethics Committee granted ethical approval for this study. Participants were invited to take part in the study via an email, which included the full study participant information sheet. Once individuals had indicated that they would like to participate, a weblink was sent to be used by participants to provide informed consent (or informed parental consent and assent if under 16 years old), as well as baseline demographic information. All consent/assent forms, baseline questionnaires and comments on statements were hosted using Qualtrics online survey software (Qualtrics, Provo, UT, 2020; https://www.qualtrics.com). Following completion of the baseline questionnaires, participants were emailed detailed instructions on completing the Q-sorting task, including a weblink to the task webpage. Participants were also given the option to discuss the task with the lead author (RP) via telephone if preferred, and written instructions were repeated preceding each stage of the task. The online Q-sorting task was hosted using QsortWare, an online method for conducting Q-sort (Pruneddu, 2017). Following completion of the Q-sorting task, participants were sent a weblink directing them back to Qualtrics where they were invited to comment on any statements that they felt strongly about, using an open-text response box located adjacent to each statement. Participants were debriefed online via Qualtrics after completing the tasks, and young people and parent participants were each sent an online shopping e-voucher to the value of £10 (United Kingdom) to thank them for their participation.
Q-sorting task
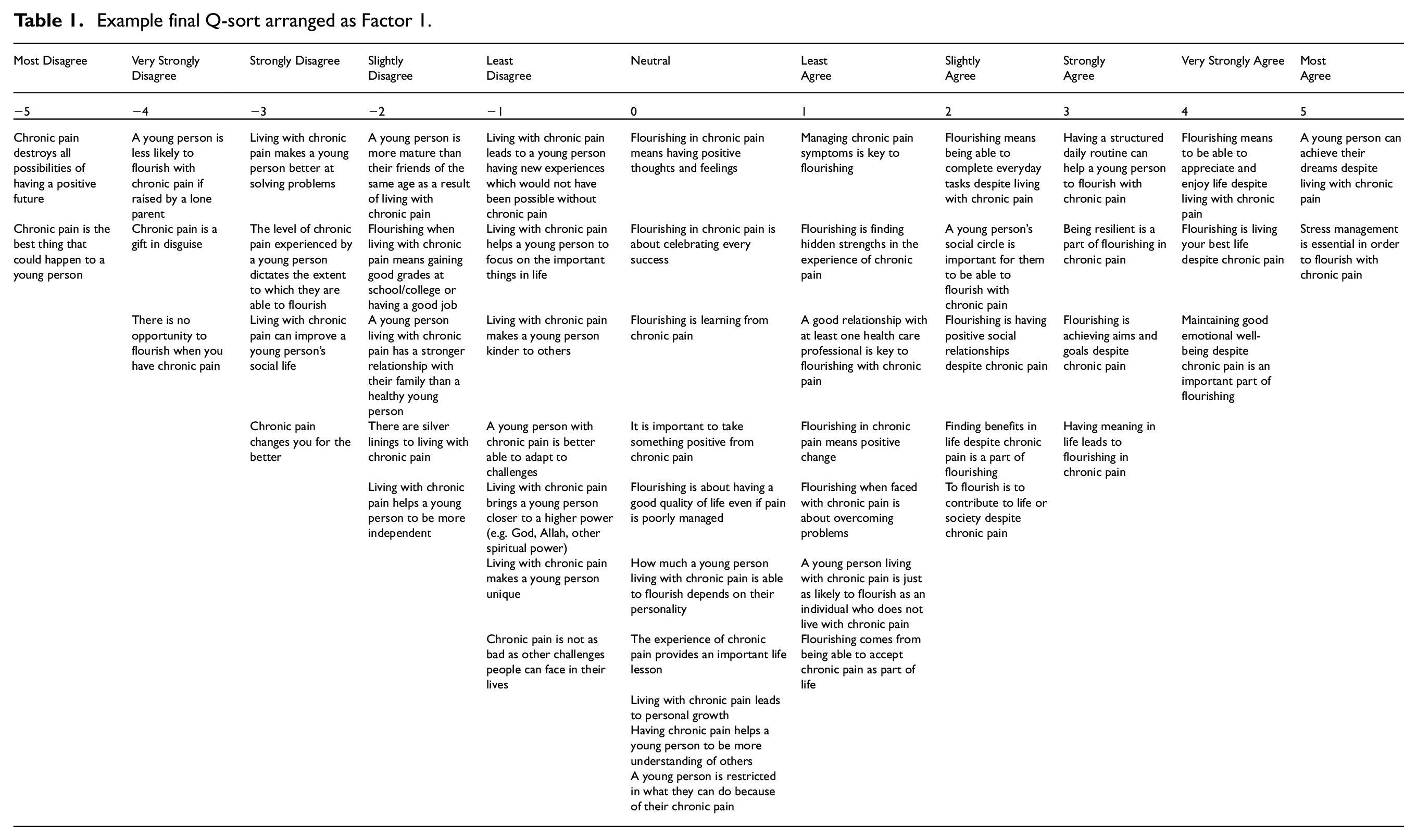
The Q-sorting task was piloted by four colleagues (three psychology postgraduate students and one young person) to ensure that the task instructions and Q-set items were clear. Participants were presented with 52 statements based on flourishing in the experience of chronic pain and were required to indicate their level of agreement or disagreement with each. In the first stage of the Q-sorting task, participants were asked to conduct an initial sort using their computer mouse to drag each statement into one of three boxes (Disagree, Neutral, Agree). There was no limit to the number of statements that could be dropped into each box. In the next stage, participants were asked to refine their level of agreement or disagreement with each statement by placing items in a sorting grid presented on a continuum from −5 (Most Disagree) through to neutral and +5 (Most Agree), in the shape of a quasi-normal distribution. There were a limited number of response boxes available in relation to each level of agreement so that participants were required to achieve a best-fit when arranging the statements into each box. See Table 1 for an example Q-sort arranged in the sorting grid. See Supplemental Appendix C for task instructions provided to participants.
Example final Q-sort arranged as Factor 1.
Analyses
Data for each of the 54 Q-sorts were entered into specialized Q-methodology software (PQ Method v2.35 (Schmolck, 2014)) simultaneously. The Q-methodological approach allows the researcher to identify viewpoints provided by groups of individuals who make sense of a pool of statements in comparable ways, as well as to identify subtle differences between viewpoints provided by individual participants (Watts and Stenner, 2005). Therefore, it was not necessary to analyse participant groups separately based on shared traits (such as age, young person, parent, healthcare professional) (Valenta and Wigger, 1997), which would have produced superfluous data. Rather, the ‘groups’ represent participants who sorted their Q-sort grids in similar ways.
Using this specialized software, the Q-sorts were analysed to produce intercorrelations between participants’ Q-sort grids (McKeown and Thomas, 2013). The resulting intercorrelation matrix among Q-sorts was then subjected to a Q-analysis that was rotated using Varimax rotation. The Kaiser-Guttman criteria of retaining factors with eigenvalues above 1 (Guttman, 1954; Kaiser, 1960) was used, resulting in the identification of eight factors. One factor was dropped due to no participants loading significantly onto this factor. Our significant factor loading level was calculated at 0.51, which was deemed to be the ideal level to maximize the number of participants with significant loadings onto a factor (Watts and Stenner, 2005). Although participants may load onto numerous factors simultaneously, each participant is only allowed to significantly load onto one factor, which is termed an exemplified Q-sort. This indicates that the participant’s Q-sort is ‘typical’ of this factor (McParland et al., 2011). If a participant significantly loads onto more than one factor, this factor is considered a confounded Q-sort and is subsequently removed from the analysis (Watts and Stenner, 2005).
As not all emergent factors are required to be interpreted in Q-methodology (Brown, 1980), three of the seven remaining factors that provided distinctive and clear viewpoints of flourishing in the context of young people living with chronic pain were chosen. This approach allows the researcher to build the clearest picture of the reported factor/s and accurately tell the ‘story’ that they represent. The three-factor solution accounted for 30 of the 54 Q-sorts. The interpretation of factors involves producing summarizing accounts to indicate viewpoints expressed by each factor (Watts and Stenner, 2005). To further aid factor sort interpretations, distinguishing and consensus statements for each factor are used, and factor arrays are created using z-scores that result in a representative best-estimate Q-sort for each factor. Distinguishing statements represent those statements that are placed significantly differently to where participants have placed the same statement on other factors, while consensus statements represent statements that are in agreement by participants across factors (Herrington and Coogan, 2011). Additionally, qualitative comments provided by participants were used to interpret how participants thought about the statements (with the inclusion of demographic variables of these participants). See Supplemental Appendix D for representative Q-sorts and distinguishing statements for excluded factors.
Results
Factors were labelled: (1) Pain is not a barrier to flourishing, (2) Adapting to a new life and (3) Adopting a positive perspective. Consistently rejected items across the factors were the statements ‘Chronic pain is the best thing that could happen to a young person’ (6) (rated −5 in all factors) and that ‘Chronic pain is a gift in disguise’ (1) (rated −4 in all but one factor). These items were excluded from interpretation. We now present each factor viewpoint in turn below. Each statement item is followed by its item number and level of agreement in parentheses, while participant comments (italicized) are used to aid factor interpretation.
Factor 1: Pain is not a barrier to flourishing
Factor 1 explained 24% of the variance and was exemplified by 23 participants (4 young people aged 14–17 years, 14 healthcare professionals aged 36–51 years, 5 parents aged 47–52 years). Common viewpoints in this factor relate to the notion that chronic pain does not mean that life cannot be enjoyed or lived to its fullest, but that some flexibility may be required. A distinguishing statement of this factor is that ‘A young person living with chronic pain is just as likely to flourish as an individual who does not live with chronic pain’ (8: +1), indicating a positive future-focused outlook. Participants were also in strong agreement with the statement ‘A young person can achieve their dreams despite living with chronic pain’ (16: +5), with a young person commenting:
Absolutely, what’s stopping me? my pain? I’ll just find other ways to do it. (Participant 4, young person, aged 15.)
However, while agreeing with this statement, participants also acknowledge certain limitations to an imagined future, with acknowledgement that some change may be required:
It can limit someone on prospects such as I had dreams of being a hairdresser, but I can’t stand on my feet, so I can’t anymore. (Participant 10, young person, aged 17.)
It very much depends on what their dreams are. My daughter’s dreams have perhaps been revised since suffering with chronic pain and I have no doubt she will achieve these, but they are different dreams now. (Participant 25, parent, aged 49.)
These comments indicate the viewpoint that while chronic pain should not serve as a barrier to desired accomplishments, some realistic expectations and alterations may be required in addition to a new way of thinking about life with pain. Consistent with this viewpoint, a strongly rejected item was ‘There is no opportunity to flourish when you have chronic pain’ (9: −4), with participants commenting in relation to the statement:
I may not flourish in the way a healthy person would, but I will flourish in my own special way that is individual to me. And so does everyone else, we all have different restrictions and talents in life, my restriction being pain doesn’t make me any less capable. (Participant 4, young person, aged 15.)
You can still flourish despite having chronic pain, in some cases it can make the individual even more determined to succeed. (Participant 43, healthcare professional, aged 41.)
A further strongly rejected item was ‘Chronic pain destroys all possibilities of having a positive future’ (11: −5), with a parent commenting:
Chronic pain is a hurdle or a challenge, but in no way does it keep you from having a positive future. (Participant 31, parent, aged 52.)
Participants provided additional considerations of the meaning of flourishing with agreement with the distinguishing statements ‘Flourishing means being able to complete everyday tasks despite living with chronic pain’ (37: +2) and ‘To flourish is to contribute to life or society despite chronic pain’ (34: +2). Congruent with this idea that the definition and experience of flourishing is highly subjective, another statement that received strong agreement was ‘Flourishing is living your best life despite chronic pain’ (47: +4), with a healthcare professional noting that a young person’s idea of their ‘best life’ will be different for each individual, highlighting the unique nature of flourishing and the importance of recognizing individual differences in how flourishing is perceived:
Flourishing is what someone defines it as, it is different for each individual and this feels the best description of genuine flourishing rather than that based on grades, achievements etc. (Participant 42, healthcare professional, aged 41.)
Participants also held the viewpoint that emotional well-being is key to being able to flourish, with strong agreement for the statement ‘Maintaining good emotional well-being despite chronic pain is an important part of flourishing’ (40: +4). A healthcare professional commented on the perceived value of emotional well-being in leading to flourishing:
Too often with patients experiencing chronic pain, there is also depression and need for mental health support. Emotional well-being is often essential to improvement in living with chronic pain. (Participant 36, healthcare professional, aged 36.)
Factor 2: Adapting to a new life
Factor 2 explained 9% of the variance and was exemplified by five participants (four young people across the full age range of 11–24 years, one parent aged 54 years). Common viewpoints in this factor related to perceived adaptations that may contribute to flourishing, such as the management of stressors, resilience and acceptance. Participants strongly agreed with the item ‘Stress management is essential in order to flourish with chronic pain’ (15: +5), with two young people commenting:
You need to be able to deal with the frustration and emotional effects that living with chronic pain brings. (Participant 7, young person, aged 17.)
Stress makes pain worse, therefore it is important to have stress management in place. (Participant 9, young person, aged 17.)
This highlights the importance young people may place on stress management as a strategy to manage pain and relates to the management of emotional wellbeing discussed in Factor 1. A distinguishing statement strongly agreed with was ‘Being resilient is a part of flourishing in chronic pain’ (35: +4), with a young person, and parent, commenting:
I have had many hurdles that I have had to overcome in the last 2 and a half years and have had to be extremely resilient to bounce back. (Participant 7, young person, aged 17.)
These [young] people in pain have to be so unbelievably resilient to get through life. I don’t think unless you have experienced chronic pain or seen a very close member of family have it you would understand. (Participant 32, parent, aged 54.)
This indicates that a level of resilience is needed to be able to function with chronic pain. A further strongly agreed with statement was ‘Flourishing comes from being able to accept chronic pain as part of life’ (49: +4). One young person commented:
I would say acceptance is one of the first steps required to be able to flourish. If you cannot accept the pain, then you will live in resentment. (Participant 20, young person, aged 24.)
This view indicates that individuals view the acceptance of pain as an important step on the road to flourishing, while resentment of pain may be seen as a barrier to flourishing.
Alongside the consideration of flourishing within this factor, participants provided an indication of the aspects of a young person’s life that they may consider to be inhibited by chronic pain and therefore, not contributing to flourishing. Participants strongly rejected the statement that ‘Living with chronic pain can improve a young person’s social life’ (32: −4), with one young person and one parent commenting on the negative effects of chronic pain on a young person’s social life:
It actually puts a strain on the young person’s social life as my friends struggle to understand what I go through and can be thoughtless. (Participant 7, young person, aged 17.)
Young people don’t have the time or understanding for those who cannot go to events or cancel. One good friend is key though to help. (Participant 32, parent, aged 54.)
Participants disagreed with the viewpoint that their spirituality had increased due to chronic pain. Participants largely rejected the distinguishing statement that ‘Living with chronic pain brings a young person closer to a higher power (e.g. God, Allah, other spiritual power)’ (29: −5). This statement appears to provoke a ‘why me’ sentiment among participants, providing a reasoning for the absence of spirituality, with one young person and one parent commenting:
One would question that if there was a higher power, then innocent people shouldn’t have to suffer with chronic pain. (Participant 9, young person, aged 17.)
Expect this was my No 1 disagree. I am not religious. If I was, I would question why chronic pain exists and why my child. (Participant 32, parent, aged 54.)
Factor 3: Adopting a positive perspective
Factor 3 explained 5% of the variance and was exemplified by two young people aged 23 and 24 years. Common viewpoints in this factor related to the consideration of flourishing as benefit finding and recognizing achievements, as well as appreciation and enjoyment of life. Participants strongly agreed with the statement that ‘Finding benefits in life despite chronic pain is a part of flourishing’ (36: +5). Another statement that was strongly agreed with was the distinguishing statement that ‘Flourishing in chronic pain is about celebrating every success’ (48: +5), with young people commenting:
This is a key part of my life, I focus on every success and celebrate things big or small. (Participant 18, young person, aged 23.)
Flourishing to me is about celebrating even the tiny things like getting up today or getting dressed or going out. They’re all achievements that seem impossible on a bad day. (Participant 19, young person, aged 24.)
This highlights how young people with chronic pain may show a heightened awareness for benefit finding and achievements (no matter the magnitude), which are seen as a victory.
Participants also strongly agreed with the distinguishing statement ‘Living with chronic pain makes a young person kinder to others’ (28: +4), indicating that these perceived benefits may also include emotional growth, with one young person commenting:
I have more empathy now because of my chronic pain, which leads to me being kinder. (Participant 18, young person, aged 23.)
Participants strongly agreed that ‘Flourishing means to be able to appreciate and enjoy life despite living with chronic pain’ (43: +4), highlighting the importance of a positive-focused life to counteract the negativity usually associated with chronic pain. One young person commented:
Appreciating everything and enjoying life is so important with chronic pain, it can be easy to focus on the negative, but focusing on the positive and enjoying life is flourishing to me. (Participant 18, young person, aged 23.)
Linked with adaptation to pain reported in Factor 2, a further strongly agreed with statement was that ‘A young person with chronic pain is better able to adapt to challenges’ (23: +4), with a young person commenting on their perceived benefit over a healthy peer:
We are much better at finding a way around a problem or barrier and adapting our lives, so that we experience less pain and have more gain by being able to live our life. (Participant 19, young person, aged 24.)
Participants also strongly rejected the idea that ‘Flourishing when living with chronic pain means gaining good grades at school/college or having a good job’ (38: −4), with a young person indicating that they consider happiness to be synonymous with flourishing, regardless of status:
Grades and a job do not define a person and as long as they are happy in life, they are flourishing. (Participant 18, young person, aged 23.)
These viewpoints and comments provide thought-provoking considerations regarding what flourishing really means to young people with chronic pain, with a move away from material gains, to a heightened focus on finding joys and happiness in everyday life.
Discussion
The aim of this study was to investigate how flourishing may be perceived, understood and experienced by young people living with chronic pain, and parents and healthcare professionals who care for these young people. Our analyses identified three factors that represented distinctive and clear shared viewpoints among participants. The first factor represented the viewpoint that life can still be enjoyed despite chronic pain, although often requiring a flexible approach, while the second factor represented the viewpoint that adaptations such as management of stressors, resilience and acceptance may be required in order to flourish with chronic pain. The third factor represented the viewpoint that flourishing should be regarded as appreciation and enjoyment of life, with the inclusion of benefit finding and recognition of achievements, whether big or small.
These findings align with how flourishing has been conceptualized in previous literature, with aspects of well-being or ‘life going well’ (Huppert and So, 2013; Keyes, 2002, 2005) represented by positive changes, outcomes and constructs (Jordan et al., 2018; Soltani et al., 2018). A common thread throughout all factors was the viewpoint that flourishing among young people living with chronic pain is possible, but that individuals may differ in both their level and perception of flourishing, which consequently influences individual differences in defining flourishing. While for some young people, merely completing everyday tasks may be seen as flourishing, for others, flourishing may be about living their idea of their best life despite chronic pain. Chronic pain can influence the perceptions of those living with this condition as to what is meaningful to them and often leads to a revision of their life goals (Dezutter et al., 2015). While flourishing was not necessarily considered by participants to be based around material achievements such as gaining good grades, closely linked with flourishing and positive outcomes was the recognition and appreciation of successes, achievements and pleasures in life. This finding indicates a desire by young people living with chronic pain to find positive consequences and benefits due to their pain experience, which may be an attempt to reduce distress caused by the symptoms of illness (Currier et al., 2009; Soltani et al., 2018).
Of interest in our results was the difference in viewpoints exemplified by healthcare professionals and other participants. While healthcare professionals exemplified the optimistic viewpoint that life can still be lived to its fullest despite chronic pain, this viewpoint was exemplified by fewer young people and parent participants. These results indicate that healthcare professionals may be inclined to adopt a more positive approach to living with chronic pain, while young people and their parents may find it more challenging not to perceive pain as a barrier to living well, and may require more assistance and encouragement to adopt this perspective. Healthcare professionals placed particular importance on emotional wellbeing as a contributor to flourishing, with some considering healthy emotional wellbeing essential in order to flourish. More broadly, all groups acknowledged the importance of flexibility in order to flourish with chronic pain. This viewpoint is congruent with the findings of Jones et al. (2020), where adolescents described hope for a positive future despite their chronic pain, but acknowledged that adaptation of their future plans that may be required. Flexibility has been shown to be an important source of resilience and is related to reduced physical and psychosocial disability, and lower symptom severity in chronic pain (Goubert and Trompetter, 2017).
A further interesting finding was the viewpoint exemplified by young people regarding the negative effects of chronic pain on their social circles and spirituality. These viewpoints are a reflection of the large body of previous research outlining the negative impact of chronic pain, including impaired psychological, developmental, school-related and physical functioning (Forgeron et al., 2010; Goubert and Trompetter, 2017; Groenewald et al., 2020; Higgins et al., 2021; Jones et al., 2021). Our social findings are congruent with a reduction in social functioning due to chronic pain identified in previous literature, including disruption to interactions with peers, leading to social isolation (Eccleston et al., 2008; Forgeron et al., 2010; Jones et al., 2022). However, it should be noted that there have also been limited accounts of improved peer relationships due to chronic pain. A qualitative study by Jones et al. (2022) identified the positive outcome of increased time spent with peers, and improved social relationships, due to chronic pain. This was attributed to reduced time spent on physical activities that were no longer possible, which allowed more time to be spent on building social relationships. Our findings of decreased spirituality reflect the variability of findings in this domain. A study by Baetz and Bowen (2008) found that individuals aged 15 or older were more likely to turn to religion or spirituality and seek spiritual support to cope with chronic pain than healthy individuals, while a review by Ferreira-Valente et al. (2019) concluded that spirituality may serve as a resource for psychological adjustment. However, an earlier review by Rippentrop (2005) reported that methodological problems in studies have prevented a clear answer on whether pain may lead to stronger spiritual belief. This indicates the need for further research on the relationships between spirituality and pain to explore the role spirituality may play in the lives of young people with chronic pain. Our results further highlight the co-existence of both flourishing and negative outcomes in those living with chronic pain, and the need for further studies to investigate potential relationships between positive and negative constructs and outcomes related to young people living with chronic pain.
Participants were able to identify potential contributors to flourishing and wellbeing when living with chronic pain, such as resilience, adaptation, positivity and stress management. A resilient approach to adversity may empower an individual to continue living a fulfilling life despite their pain, and to develop new strengths over time as their life circumstances may change (Luthar et al., 2000). This resilience may encompass positive adaptation in the face of chronic pain, such as developing problem-solving abilities and emotional flexibility (Wainwright et al., 2019), and can be due to a young person’s attributes as well as those of their families and social circle (Karoly and Ruehlman, 2006). For example, additional resilience resources could be provided by parents who promote coping, pain management and adjustment (Cousins et al., 2015).
Despite the strengths of this study, we also acknowledge some limitations. Firstly, while we used the data and accompanying statements to interpret and make sense of viewpoints as guided by Herrington and Coogan (2011) and Watts and Stenner (2005), it is possible that our interpretation of the results may differ from those of other researchers. A different interpretation may result in alternative findings, exposing a potential reliability weakness of adopting a Q-methodological approach. However, Watts and Stenner (2005) conclude that if all Q-methodological analytical resources are effectively combined and correct checks for accuracy and efficacy of interpretations are conducted, a clear interpretation of the factors will emerge and other researcher interpretations should produce similar results. Additionally, it should be noted that all factors contained elements of flourishing, but our decision to interpret only three of the seven factors was based upon providing the clearest picture of the findings when combining all resources provided by the Q-methodological approach.
Secondly, our sample of young people was limited to participants with a predominantly British White Female sociodemographic background. Our large female sample is unsurprising considering that prevalence rates of chronic pain are known to be higher among females (Fillingim et al., 2009). Due to this predominantly female sample, although not a focus of our research, we opted to run the same analysis with only female participants to check for differences. As might be expected when removing Q-sorts within the all-gender analysis, there were a few variations in the female-only sample output. While Factor 1 remained largely the same, for factor 2, a stronger opinion was expressed in relation to the statements ‘Flourishing means to be able to appreciate and enjoy life despite living with chronic pain’ (43: +5), ‘The level of chronic pain experienced by a young person dictates the extent to which they are able to flourish’ (13: +4), ‘A young person is restricted in what they can do because of their chronic pain’ (10: +4) and ‘Chronic pain changes you for the better’ (2: −4), indicating differences in perceived ability to adapt to living with chronic pain when compared with the all-gender results. In factor 3, a stronger opinion was expressed in relation to the statements ‘Living with chronic pain makes a young person unique’ (7: +5), ‘A young person is more mature than their friends of the same age as a result of living with chronic pain’ (22: +5) and ‘The experience of chronic pain provides an important life lesson’ (5: +4), indicating differences in perceived positive outcomes when compared with the all-gender results. These differences highlight that participant viewpoints may differ based on factors such as gender, level of education, socioeconomic status and geographic region (Wratten et al., 2019). Further studies that make use of diverse participant samples would be useful to investigate how participant viewpoints may vary based on sociodemographic differences among young people. Furthermore, our young person participant sample was skewed towards the upper end of the age range. Developmental differences between younger and older individuals may affect participants’ perception and understanding of flourishing, and/or their capacity to flourish. Older individuals typically have broader life experiences providing further opportunity for engagement with positive experiences, and potentially stronger peer relationships and social support that may offer additional means to promote flourishing (Eccleston et al., 2008). Perceived positive outcomes such as psychosocial maturity (Icenogle et al., 2019), increased emotional and cognitive capacity (Yurgelun-Todd, 2007) or independence, may be related to developmental maturity and not necessarily a result of living with chronic pain.
Thirdly, as all our study participants were recruited from a previous pain-related study, it is possible that our results were influenced by participants who are more prone to study participation and adopting a positive approach to their pain experience, while those with a more negative outlook may be less likely to want to take part in research with a positive focus. Therefore, further studies are needed to examine both positive and negative aspects of living with chronic pain concurrently, in order to provide a balanced representation of how these constructs may be related.
In conclusion, this study provides novel insights into the way that flourishing in young people living with chronic pain may be perceived, understood and experienced, supplementing limited previous literature investigating flourishing in this area. These findings also suggest that young people are able to flourish with chronic pain, although perceived flourishing may differ among individuals. While the shared viewpoints identified in this study provide a useful contribution to guide future research investigating flourishing in young people living with chronic pain, further studies are needed to investigate individual differences in levels of flourishing and to identify potential flourishing traits unique to different sociodemographic groups with chronic pain. These findings have important implications for communication around the management and treatment of young people living with chronic pain, and potential positive-based treatment approaches.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241237341 – Supplemental material for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study
Supplemental material, sj-docx-1-hpq-10.1177_13591053241237341 for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study by Ryan D Parsons, Joanna L McParland, Sarah L Halligan, Liesbet Goubert and Abbie Jordan in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053241237341 – Supplemental material for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study
Supplemental material, sj-docx-2-hpq-10.1177_13591053241237341 for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study by Ryan D Parsons, Joanna L McParland, Sarah L Halligan, Liesbet Goubert and Abbie Jordan in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053241237341 – Supplemental material for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study
Supplemental material, sj-docx-3-hpq-10.1177_13591053241237341 for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study by Ryan D Parsons, Joanna L McParland, Sarah L Halligan, Liesbet Goubert and Abbie Jordan in Journal of Health Psychology
Supplemental Material
sj-docx-4-hpq-10.1177_13591053241237341 – Supplemental material for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study
Supplemental material, sj-docx-4-hpq-10.1177_13591053241237341 for The perception, understanding and experience of flourishing in young people living with chronic pain: A Q-methodology study by Ryan D Parsons, Joanna L McParland, Sarah L Halligan, Liesbet Goubert and Abbie Jordan in Journal of Health Psychology
Footnotes
Data sharing statement
The data generated during and/or analysed during the current study are not publicly available, nor are they available on request, due to the fact that our participants were not asked to agree to their data being publicly available at the point of data collection. As such, we are unable to share this data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was undertaken as part of a PhD Studentship funded by the Pain Relief Foundation [JW/cmp].
Ethics approval
Ethical approval for this study was granted by the university departmental ethics committee (Ref: 21-207).
Informed consent
All participants gave informed consent prior to participation in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.