
Abstract
This qualitative study explored the lived experiences of eight Sri Lankan mothers of infants with complex congenital heart disease (CCHD) using semi-structured interviews. Four themes were generated as: illness perception, communication with medical staff, challenges faced, and coping mechanisms. These provided insight into the multi-faceted nature of mothers’ experiences, importance of medical-caregiver communications and their need for psychosocial services. The findings enhance the limited knowledge of South–Asian primary CCHD caregiver experiences and will help in improving psychosocial support services in Sri Lanka.
Introduction
Congenital heart diseases (CHD) are a range of birth defects in the heart which affects the heart’s function (NHS, 2019). The global incidence for CHD was 1.8 cases per 100 live births (Zimmerman, 2020) and, in 2022, the Centres for Disease Control and Prevention (CDC) estimated that one in four babies born with a heart defect present with complex congenital heart disease (CCHD). Children with CCHD usually need an intervention within the first year of their life to ensure survival, along with repeat procedures and lifelong palliative care (Buratto et al., 2016; Centers for Disease Control and Prevention, 2022). Major advancements in medical procedures have ensured better survival rates for children with CCHD but the responsibility of caring for them falls mostly on parents who are generally identified as the primary caregivers (Doherty et al., 2009).
Prior research shows that caring for a chronically ill child is taxing for parents as it exposes them to distress, isolation, shame, and even suicidal thoughts (Adib-Hajbaghery and Ahmadi, 2019; Golics et al., 2013). When caregiving is considered, fathers tend to take on financial responsibility and be the ‘support act’ while mothers hold an ‘everyday’ caregiving role (Connor et al., 2010; Gower et al., 2017; Imperial-Perez and Heilemann, 2019). Thus, mothers face ‘unique challenges’ (Ahn and Lee, 2018) resulting in psychosocial distress for both themselves and the child (Chang et al., 2020; Fischer et al., 2012; Jordan et al., 2014). In families with multiple children, mothers struggle to balance between the ill child and the healthier sibling (Caris et al., 2018; Parker et al., 2020) as children with CCHD require more effort and time (Ladak et al., 2019) which highlights the need for social support (Ravindran and Rempel, 2011).
Lumsden et al. (2019) review indicated support systems as being significant – along with emotional responses of attachment, detachment, and positive thinking. Coping with CCHD included strategies such as striving for normality, acquiring knowledge, facing challenges, and becoming hypervigilant (Lumsden et al., 2019; Rempel et al., 2013). Cultural beliefs, healthcare systems (Aubel, 2012; Dalir et al., 2020; Pharr et al., 2014) and socioeconomic capacities available to each family also influenced coping and caregiving styles (Connor et al., 2010). For positive coping and emotional health – family spirituality, parenting strategies and the physician-caregiver relationship were seen as vital (Dalir et al., 2020; Gramszlo et al., 2020; McMahon and Chang, 2020; Mitnick et al., 2010; Nayeri et al., 2021). Though mothers often had good relationships with their child’s cardiac care team (Arya et al., 2013), most wished they would receive more knowledge than what was received. Interventions such as education programmes which promote better understanding of CHD emphasised a positive impact on self-efficacy, empowerment, confidence, and positive-thinking abilities (Animasahun et al., 2015; Edraki et al., 2014; Given et al., 2008) which indicate that caregiver wellbeing has an impact on the level of care provided for children with CCHD. Consequently, considering that the incidence of CHD in Sri Lanka is on par with worldwide rates (Iruthayanathan et al., 2018; Samarasinghe, 2014), this led to the formulation of this current research in the Sri Lankan context due to the scarcity of such research – especially on caregivers. The evidence obtained from this study is anticipated to assist in the development of psychosocial interventions to support caregivers of CCHD children in future as currently there are no formal systems in place in Sri Lanka. Thusly, this study aimed to explore the lived experiences of mothers who were the primary caregivers of children with CCHD in Sri Lanka.
Method
Research design
A qualitative phenomenological approach was selected to explore the ‘depth and breadth’ (Edwards et al., 2021) of the niche topic of maternal caregiver experiences of children with CCHD. Face-to-face interviews provided opportunities to gather in-depth personal accounts as they afford comprehensive insights into their experiences and life choices of caregivers (Gower et al., 2017). Two telephone interviews were later added because of access restrictions due to the COVID-19 pandemic and these interviews were also maintained to the same standards of rigour as provided in the face-to-face interviews.
Participants
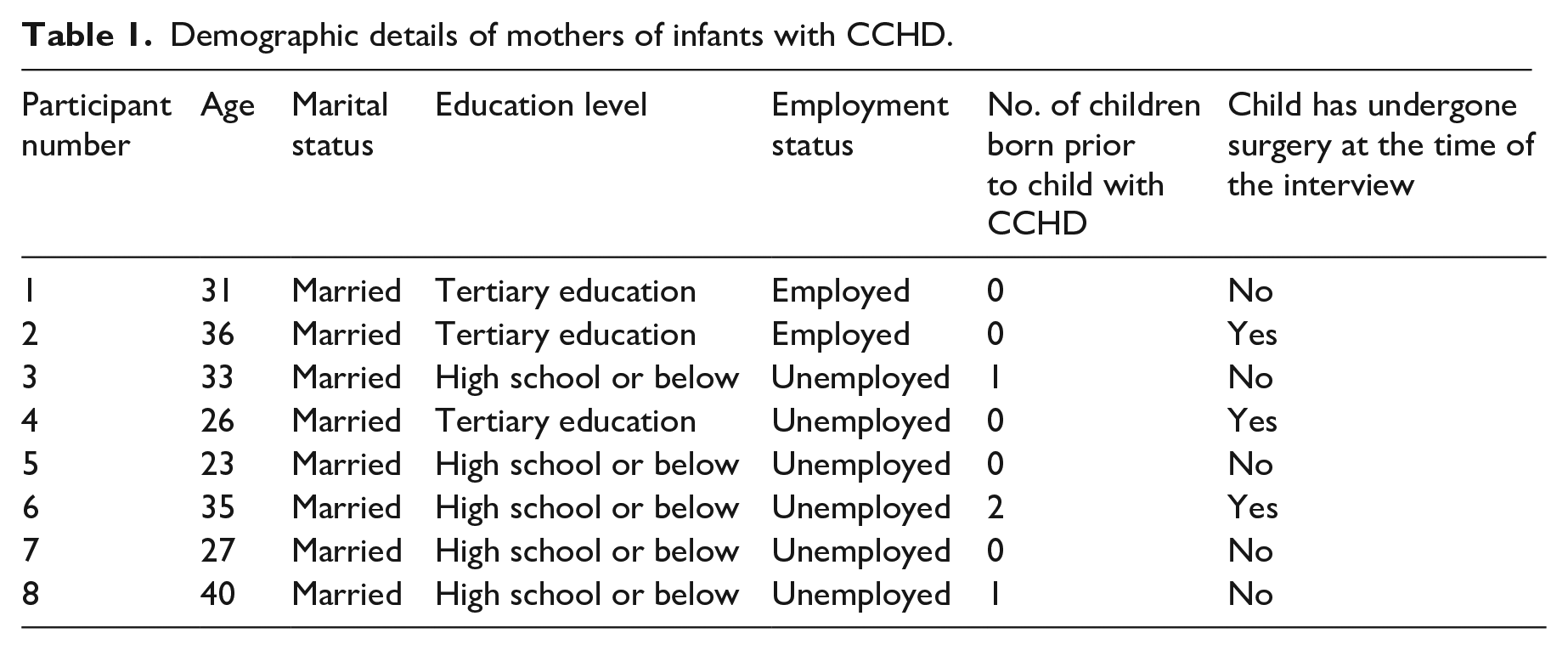
In recommendations for ‘small’ research projects in thematic analysis, Fugard and Potts (2015) recommends 6–10 participants; eight participants were decided on based on information power (Malterud et al., 2016). Potential participants were recruited from the main children’s hospital in Colombo; eight mothers of infants with CCHD consented and constituted in the final sample. The inclusion criteria for the mothers were: have a child who is less than 2 years old, diagnosed with CCHD, and has undergone or is scheduled to undergo corrective heart surgery. Children with any developmental disorders or any other associated health conditions at birth were excluded in order to maintain a level of homogeneity in the sample. A sample of eight was deemed as pragmatically sufficient considering similar existing research (Gower et al., 2017; Moore et al., 2023). The demographic details of the participant mothers are presented in Table 1.
Demographic details of mothers of infants with CCHD.
Procedure and ethical considerations
The recruitment site was the cardiology unit and clinics attached to a tertiary-care Children’s Hospital in Colombo, Sri Lanka. Ethical approval was obtained from the hospital board where the study was conducted [LRH/DA/29/2020]. The researcher also obtained approval from the ethics panel of the University of West London, UK [SS70016O-21433568], along with subsequent amendments regarding telephone interviews conducted due to access restrictions during the pandemic. The study also adhered to the Declaration of Helsinki (2013) ethical principles regarding research participants.
A potential participant pool was recommended by medical officers attached to the cardiology unit and the clinics as per the inclusion criteria identified by the researcher. From this pool, eight mothers voluntarily consented to participate and were thus approached by the researcher. All the volunteers received information sheets and informed consent forms and were allowed time to ask any questions from the researcher before the interview commenced. Six interviews were conducted in a separate room at the hospital, while two were conducted via telephone with the consent of these participants. Participants’ permission was obtained for recording the interviews using an audio recorder while a pre-downloaded call-recording app with encrypted data recordings was used to record the telephone interviews. The researcher conducted each interview (average 60 minutes). If the participant showed signs of distress, the recording of the interview was stopped and counselling support or a small break as per the university ethics requirement was provided. Participants were informed that the interviews would resume only if they wished it and felt comfortable enough to proceed. If not, the interview would be terminated with no consequences to either mother or child.
Prior to the interview, the researcher explained the purpose of the study, assured participants about privacy and confidentiality of data and obtained both verbal and written consent. Participants were informed of their right to withdraw at any time, and it was emphasised that such a decision would not have any impact on their child’s treatment. A debriefing session was held at the end of each interview to ensure that the participants understood the details of the research and how the data they provided would be used in the study. They were each provided with both institutional and free private counselling helplines if further support was needed.
Interview schedule
A semi-structured interview guide was created and included 11 open-ended questions which were pre-tested with a similar participant from the CCHD clinic. The interview questions were based on the Biopsychosocial model and participants’ background details, child’s medical history, feelings about child’s present condition, lifestyle before and after child’s birth and diagnosis, emotions regarding child’s condition, family involvement, other social support were included and was informed by previous research (Jackson et al., 2015; Kusnanto et al., 2018; Ni et al., 2019; Smith and Osborn, 2007). Based on the answers provided, further follow-up questions were asked to gather more information as required per the study objectives. All interviews were conducted in Sinhalese language which were later translated to English at analysis stage. Translation of the data was completed in compliance with the forward, expert panel, and back translation method advocated by the World Health Organization (2020).
Analysis
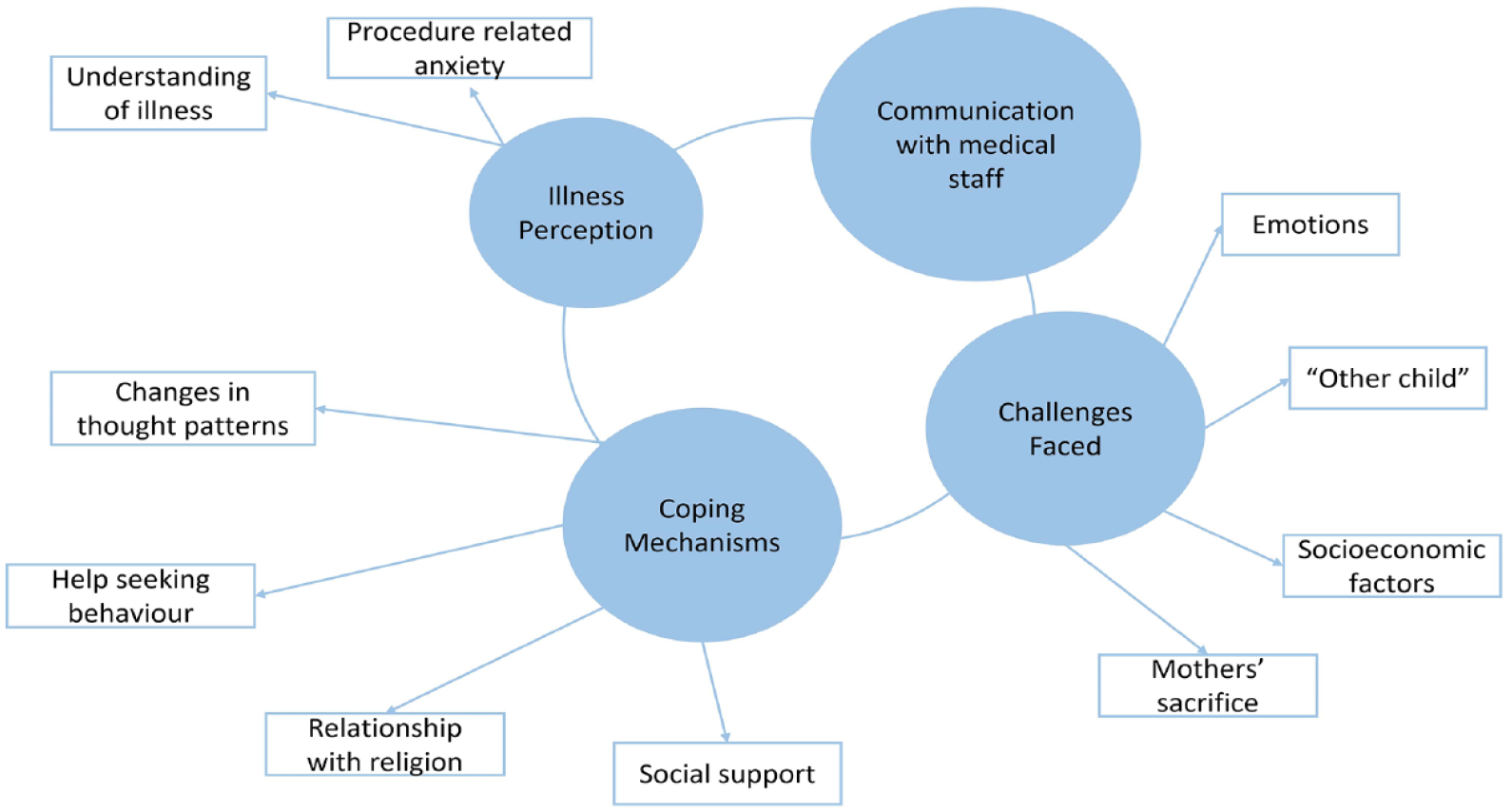
Braun and Clarke’s (2006) six step guide to thematic analysis was used to analyse the interview data. The analysis was conducted after carefully reading and re-reading of each transcript. Then codes were extracted and subordinate and superordinate themes were generated. These initial themes were also reviewed and discussed by both authors in relation to the aims and objectives of the research. Finally, the thematic map was developed highlighting the themes and their relationships between the data (Figure 1). An outline of the analysis process is included as a supplementary material (‘Explanatory Memo’).
Comprehensive diagram of themes and sub-themes that emerged during analysis.
Reflexivity
The present research used reflexivity as a process of acknowledging the role (Watt, 2007) and the introspective perspective of the researcher. The first author’s position as an adult patient with CCHD was titular in providing an insider perspective on the role of maternal caregivers from the viewpoint of a child. Further, the research was completed as part of the first author’s Masters programme; the second author was the first author’s research supervisor.
Results and discussion
Four themes were generated at analysis stage as illness perception, communication with staff, coping mechanisms and challenges faced and they are discussed below with participant quotes to support them (Figure 1).
Theme 1: Illness perception
This theme reflected the way mothers perceived their child’s illness and related medical procedures. The first sub-theme, termed ‘understanding of the illness’, highlighted mothers’ efforts to better understand their child’s condition. Most mothers made inquiries on explanations such as ‘turning blue’ [Participant 7] which were unclear to them. Through resource identification, confidence about the caregiving process increases; reiterating parental management strategies where parents attempted to ‘become experts’ and stay hypervigilant for new symptoms in their child (Lumsden et al., 2019).
‘Because sometimes I check the saturation. . . [it’s usually] above 75 – 80’. [Participant 4]
‘I didn’t let anybody handle the baby after he was discharged; I didn’t even let anyone else touch him. Even when I touched him, I made sure to wash my hands before doing so’.
[Participant 2]
The mothers who had a better perception and knowledge of their child’s illness were more attuned to the child’s needs, were better at monitoring symptoms, and were more future-oriented which helped strengthen the mother-child relationship. Maternal sensitivity in response to the child’s needs built harmonious mother-infant relationships which is established in prior literature (Ainsworth, 1979; Biringen et al., 2014; Re et al., 2018).
Educated mothers had better comprehension of CCHD, however, as understanding increased, anxiety regarding their child’s survival increased as well (Fischer et al., 2012; Rempel et al., 2013). However, the degree of comprehension in process-related questions and the grasp of CCHD’s prognosis rested on education level alone which was exhibited with some familiarity with the medical or procedural discourse beyond what most comprehend. This can be seen through the comparison between responses given by Participant 6 – high-school qualifications – versus Participant 2 who had tertiary education.
‘The two veins in the heart. . .there’s blood flowing in the veins. . .that – yes. That they’re going together. . . [] [They] said it was a big operation’. [Participant 6] ‘My baby had a 7mm hole between the pulmonary vein and the pulmonary artery. [They] said the hole could not be repaired through a cardiac catheterization. They told me “Mother, the operation can only be performed through an open-heart”. [They] said to somehow get it done between 4 and 6 weeks. Otherwise, the good blood would mix with the bad blood, and the [child] could get pneumonia or shortness of breath. . . or diseases like that. So they said to somehow do it in between 4 to 6 weeks’. ‘[It was] an AP window’. [Participant 2]
The second sub-theme named ‘procedure related anxiety’ showed the heavy angst mothers experienced regarding the medical procedures that were to be performed on their child, especially when informed of the realistic stakes of the outcome.
‘I was actually told that [the chance of success was] fifty-fifty, if surgery is to be performed on the baby’. [Participant 1]
Anxiety was further increased due to the many hospital transfer processes experienced. Procedural anxiety was also compounded by dashed hopes when the surgery dates got postponed; along with the time spent on travelling and more waiting which followed it. Mothers were fixated on surgery being a ‘beacon of hope’ for their child.
‘Last time, we were only here for one week. Even then, they discharged us in a week because there were too many children. [] But that time was wasted. [] If the operation had been performed, it would not be a problem to stay even for a month or two’. [Participant 8] ‘I keep the hope that once the operation is done, everything will turn out all right’. [Participant 3]
Mothers who lacked a good understanding of their child’s condition and related procedures expressed more fear and uncertainty regarding the illness which created a negative perception about CCHD. This also influenced a lack of confidence about the surgery, and the prolonged waiting added to the increased distress about the child’s health similar to previous research (Given et al., 2008; Imperial-Perez and Heilemann, 2019).
‘I was amazed at the condition the baby was in. . . when he was tussling and playing around. I thought that his [milestones] of sitting up, rolling. . . would all be delayed because of the surgery’. [Participant 6]
Theme 2: Communication with medical staff
This theme reflected the communication processes between caregivers and healthcare staff. Doctors and medical staff played a significant role in patient-caregiver education and processes such as hygiene maintenance and post-surgical care. Caregiver education was necessary for mothers to acquire knowledge about their child’s illness and how to handle their child post-operatively as; ‘I was told to protect the child from germs for at least six months. [. . .] I mean, I knew I needed to be careful after the operation, but no one had explained [how important it was] so far’. [Participant 2]
As the legal guardian responsible for making every direct decision in their child’s life, mothers sought information from medical professionals to reduce their anxiety. A prior study also showed the importance of communication, as parents of CHD children preferred to have more information than what cardiologists would provide (Arya et al., 2013). Effective communication by all strata of medical staff in the present study was valued by these mothers as it reduced their anxiety. However, communications by the consultants were found to be the most reassuring as they were at the top of the medical hierarchy within the country’s context. ‘The little doctor said there was something wrong, but the big doctor said there was nothing to be afraid of.. [Consultant] sir said there was no problem’. [Participant 2]. This indicated that their trust on communicated information depended on the hierarchical order of medical officers indicating a novel culturally specific aspect. Similarly, the feelings of indebtedness placed on doctors was present, regardless of their hierarchy, as some mothers placed them on a higher pedestal: ‘[They’re] amazingly good. . . I really thought these were gods, not doctors when I thought about my child. They made such an effort with him’. [Participant 6]
This is unique to the cultural context of the Sri Lankan population as medical professionals are considered as ‘life savers’.
Interactions between mothers and healthcare staff were overwhelmingly positive – reassurance and kind attitudes by the medical staff were greatly valued as quoted below; ‘The nurses and the doctors are very good. . . [. . .] They talk with us like family. . . the nurses, the doctors and everybody. So, I’m happy about that. I don’t feel scared either because I can talk anything with the nurses. I can ask anything of them’. [Participant 3]
These positive attitude of mothers towards the staff led to lowered anxiety as seen in prior research (Arya et al., 2013; Mitnick et al., 2010) and interdisciplinary teams working together to provide care for patients along with their families also had a significant positive impact (Gramszlo et al., 2020; McMahon and Chang, 2020).
Theme 3: Challenges faced
The emotional, psychosocial, and economic challenges mothers faced were captured by this theme. The first sub-theme of ‘emotions’ showed mothers’ emotional adjustments as they faced the challenges of their child’s diagnosis. Negative emotions with unpleasant and disruptive responses were commonly identified. Shock, disorientation, and feelings of hopelessness were dominant as emotions expressed when they talked about post-diagnosis stage.
‘Everything I thought of [before]. . .just broke down on me’. [Participant 4] ‘Fear is constantly in my head. I am constantly in fear about when will the baby get sick’. [Participant 8]
Apart from acknowledging their increased responsibilities and fragile mental states, mothers acknowledged the hopelessness of their situation.
‘My mental health is an issue. I’m the one who does everything. Everything falls on me – I have to think of everything and do it. The people at home [don’t]’. [Participant 7]
Most of the mothers explained feelings of uncertainty and helplessness – of being ‘trapped’ [Participant 4] in a situation they did not know how to react to. Despair about the child’s future was expressed and mothers questioned from themselves: ‘Why [did this happen to] me?’ [Participant 6]. Prolonged hospital stays, and lack of social interaction opportunities increased feelings of isolation in mothers, which echoed prior research on caregiver stress and anxiety over prolonged hospital stays (Lumsden et al., 2019; McMahon and Chang, 2020).
The second sub-theme, ‘other child’, reflected the challenges faced by mothers who have multiple children. It was noted that since a child with CCHD needed more care and attention, mothers displayed a certain level of neglect about other ‘healthier’ siblings. A recent review on the siblings of CHD children highlighted the adverse life changes and parental neglect faced by these siblings (Parker et al., 2020) as their mothers could not comprehend how to balance the ‘dual needs’ in caring responsibilities (Caris et al., 2018). While the effects are unknown, the results from the present study indicate similar issues in families of children with CCHD, as their mothers could not comprehend how to balance the contrasting demands.
‘That first child is a healthy child; I was very happy with him. With this one, I have a lot of problems – we never know when he will get sick. So. . . it’s very different. The time I spend with this one – I have more responsibilities. I have to always be after this child, I can’t hand him to anyone else to look after because I have to look after him. With the other child, I didn’t have any such problems’. [Participant 8]
For such mothers illustrated above, having another healthier child to ‘support’ the current child [Participant 1] was important. Mothers also seemed to reconstruct their entire of concept of ‘normality’ within the framework of CCHD (Ahn and Lee, 2018; Gower et al., 2017).
Mothers desired to act in a ‘normal’ way and to have ‘normal’ expectations for their child’s future. Previous studies too have disclosed that parents tried to maintain a sense of ‘normality’ regarding their child by adapting and integrating to the bounds of the illness (Gower et al., 2017). The idea of treating the child as normal and attempting to maintain a normal family life has similarly been explored in other studies as a method of coping (Lumsden et al., 2019).
‘Without getting scared of everything. . . to allow him to enjoy his life within his limits’. [Participant 4] ‘I don’t treat my child like an invalid. . . just because he has an illness like that. Truly, my biggest wish is to educate him’. [Participant 2] ‘I don’t get the feeling that there is something wrong with him because he plays around like a normal child’. [Participant 1]
The sub-theme ‘socioeconomic factors’ highlighted how the caregiver burden was higher in mothers with who faced socioeconomic difficulties. While mothers who were in a better socioeconomic position could prioritise care for the child; those with poor socioeconomic situations struggled with financial and other concerns. The cost of caregiving has been explored in prior studies as lifestyle changes in relation to financial burdens (Connor et al., 2010). Socioeconomic status and education levels, along with the severity of the child’s illness, are linked to levels of care management. Mothers with stable employment had financial relief and stability to plan for a future as they considered their job a source of strength while others found unemployment a cause for further distress.
‘Money as in, these days my husband doesn’t have any opportunity to work. Nobody else works either, so we are living on the money we’ve earned so far. [. . .] After we’re discharged, husband will go back to work. We have a little money in hand already, so we’ll buy medicine from that’. [Participant 7] ‘It’s too expensive to come and go frequently. That’s why I’ve asked my husband not to come and only to visit if I ask him or call him’. [Participant 8] ‘I was in the [Provincial] Education Institute [. . .] Later, I wrote for an exam and got my job. It’s only been 2 years. . . but it was after that, that my mental status started to improve’. [Participant 2] ‘My husband earns as well. So. . . we are able to balance things. [. . .] Apart from the success of the surgery, I don’t have any [financial] worry as such because work-wise, I’m settled. I have an income to face any problem. . . I have a weapon to live with my child’. [Participant 1]
The fourth sub-theme under the main theme of challenges faced was ‘mothers sacrifice’ which highlighted mothers’ protective behaviour towards their child. These included constantly being with the child, measuring illness progress and not ‘allow[ing] him to cry much’ [Participant 1] as crying exacerbated symptoms. Protective instincts, which made mothers determined to not let their child ‘fall’ [Participant 2] to the trappings of the illness may have created a hypervigilance and overprotectiveness in the mothers as they attempted to overcompensate their behaviour to match the hostility provided by CCHD (Ladak et al., 2019; Lumsden et al., 2019).
Mothers also took full caregiving responsibility and performed all physical tasks, along with added medical care that can be performed from home in this sample as with previous research (Imperial-Perez and Heilemann, 2019).
‘I didn’t give the child to anyone else after we were discharged from the hospital, I didn’t allow anyone to touch him. Even I touched him only after washing my hands. [. . .]’ [Participant 2]
Mother-child attachment was found as a main source in reducing the burden of care in these mothers. Collectivist Asian values related to caregiving process (Dalir et al., 2020; Pharr et al., 2014) were identified in this sample of Sri Lankan mothers who assumed caregiving responsibility as their given right – irrespective of the child’s health or capabilities. These values also became a protective factor against the heavy caregiving burden placed on these mothers as they became more resilient: ‘I know it’s my child but – if he is to suffer pain, [I don’t want] to him [to] suffer pain. We can accept anything’. [Participant 4] ‘It’s not right to live life without a child’. [Participant 3]
‘While I’m alive. . . I won’t allow my child to fall. I will never tell my child “son you’re sick so don’t do this or that”. I don’t even have a hope of saying such a thing’. [Participant 2]
Resilience was a key feature found among all participant mothers, irrespective of the age of their child, and this was important in combating many of the negative emotions and stressful circumstances which they faced. While it has not been studied in great depth in literature, past findings have found psychological resilience has been associated with fewer symptoms of anxiety and post-traumatic stress (Rothschild et al., 2020; Sanayeh et al., 2021).
In contrast, attachment was also the reason for negative emotions and stress experienced by such mothers (Rempel et al., 2013). Attachment increased stress, fear, anxiety, and other negative emotions in mothers; while psychosocial dysfunctions, somatizations and poorer quality of life is caused by the stress placed on them to care for their loved ones (Adib-Hajbaghery and Ahmadi, 2019; Fischer et al., 2012; Gower et al., 2017). Therefore, attachment proved to be overwhelmingly positive as well as negative for these mothers as well.
Theme 4: Coping mechanisms
This theme highlighted the various coping methods employed by the mothers. The first sub-theme of ‘changes in thought patterns’ highlighted the way mothers developed a sense of resilience against the negativity surrounding the uncertainty of the child’s life.
‘I developed the strength to cope. When problems arise, we can’t scream or break down’. [Participant 7] ‘I came ready to face anything. I’m still ready to face anything’. [Participant 5] ‘I have thought about questions like – ‘even though the baby may have problems on the inside, if he’s smiling and okay for now, why do I have to cry for show?’. . . I have recovered now. . .’ [Participant 4]
Prior studies have highlighted Asian caregivers as being more likely to use instrumental coping than emotional coping (Pinquart and Sörensen, 2005). However, the findings of this study indicated that Sri Lankan mothers used a mix of both. Problem-focussed methods included solution-seeking behaviour and a willingness to gain knowledge about CCHD, while emotion-focussed methods include positive thinking and sharing their experience with family members.
‘Truly, I was quite stressed. Now. . . I’m okay so far. Because with all that support and positive thinking from them. . . I’ve changed now [. . .] Truly, they were a blessing more than a support’. [Participant 4]
Most mothers understood the reality of their present situation and were optimistic as a way of coping.
‘Instead of thinking that I don’t have this or that, by looking positively [at the situation]. . . we also change’. [Participant 4] ‘If anybody asks [how I am. . . I will say that I am fine’. [Participant 8] ‘Somehow. . .through suffering, my hope is to make my child well again. Sadness. . . no matter how sad you feel, if you look at it [this way], you don’t feel like it’s a sadness and [. . .]through whatever suffering to heal my baby and take her home happily’. [Participant 3]
Ahn and Lee’s (2018) study on experiences of mothers facing the prognosis of their child with CCHD revealed that participants expressed emotions that changed sequentially alongside physical and psychosocial changes in the children. Similarly, findings of this study revealed how mothers’ concerns and perceptions of illness changed over time into acceptance and tolerance. The realisation that CCHD was not a unique experience made mothers more empathetic.
‘I found that I could. . . comfort another mother a little. Truly, now. . . I have no fear to tell anybody anything [. . .] Rather than asking “Oh really?”; like a person who can give someone a shoulder to cry on, I have no fear to provide support’. [Participant 4]
The second sub-theme of ‘help-seeking behaviour’ captured mothers’ information-seeking behaviour which included questions about their child’s illness, symptom identification, pre-surgery and post-surgery procedures, and even the safety of routine vaccination procedures.
‘I sent my mother to ask. The doctor had said it was safe to inject as it was not a live vaccine. Then, I went with the child and [explained his situation] and asked whether I should vaccinate him [with DPT vaccine]’. [Participant 2]
All participating mothers acknowledged severe mental stress and how they turned to their families, spouses, and even considered mental health support.
‘I’ve actually thought that I have to go for counselling or something’. [Participant 4]
Another sub-theme within this coping theme was the ‘relationship with religion’ as they turned to religion as coping method, similar to prior research (Dalir et al., 2020).
‘As in, we had the beliefs of our religion. . . so we believe in miracles [. . .] I knew that because I prayed the whole time, and however complex the baby is, I had the belief that he would be okay’. [Participant 4]
Religion has shown to provide a cognitive framework for explaining the cause of illness, and those who turned to it were shown to be more effective in handling their child’s situation (Nayeri et al., 2021). Mothers who used Buddhist coping methods in this sample stated the illness was due to ‘a large sin’ [Participant 6] acquired from a past birth, while Christians acknowledged it as something which God saw fit to ‘give them’ [Participant 4]. Mothers explained that they made religious observances and prayed for their child’s full recovery. Their families also encouraged religious coping methods to increase hope as well as support. Medical professionals had also acknowledged religion as a healthy coping mechanism.
‘[My husband] brought a Dhamma sermons book. [He told] “You stay with the child and pray everyday that with the blessings of the Noble Triple Gems, he will get better”. [. . .] [My family] performs Buddhist ceremonies, visits temples and such’. [Participant 7] ‘As in, even the doctors, after trying everything on the child, finally says it is up to your faith’. [Participant 4]
The final sub-theme of ‘social support’ indicated that mothers relied on their spouses to share the caregiving responsibilities. Spousal assistance varied and included helping with chores, financial support, a respite from caring for the child during visiting hours for in-ward mothers and were crucial in building mothers’ mental health. In previous research, fathers were more likely to be a supportive act in providing financial support (Connor et al., 2010; Gower et al., 2017) but the findings of this study showed that mothers relied on their spouses for their own emotional – ‘[husband] said he (child) will get better’ [Participant 7] – and physical support.
‘My husband looks after me well. [] My husband is the strong one. . .He taught me everything. To keep my mind strong and stay’. [Participant 5]
There was evidence of how mothers’ coping styles were determined by the cultural beliefs common to the South Asian region heavily influenced by family relationships (Bhandari and Titzmann, 2017; Dalir et al., 2020). Prior research also highlighted the importance of spouses and grandparents being a source of structured emotional and social support to mothers (Aubel, 2012; Ravindran and Rempel, 2011) which was expressed as, ‘Yes. . . [they] helped a lot. As in – while I was constantly holding my child, my sisters came and washed the child’s clothes and as such, they helped me a lot’.[Participant 2] ‘My husband’s salary is only three thousand rupees per week. . . So my husband’s father and mother give him their salaries. They can [afford] to [. . .] They buy medicine as well’. [Participant 6]
‘Even a kind word or two goes a long way to support me mentally. My sisters, especially, call me everyday and reassure me that the baby will be fine, don’t worry’. [Participant 7]
Community support was also identified in mothers who hailed from tight-knit communities.
‘There is also assistance from the schoolteachers. Even at school, the class teacher inquired about everything. They know we have issues at home, so I have no problems from the school. I have freedom because the class teacher looks after everything and helps with [my first] child’s work’. [Participant 8]
Communal sharing and unburdening of experiences between CHD mothers themselves provide relief during admission procedures and hospital stays, which is echoed from prior research on peer support between caregivers (Given et al., 2008). Mothers in this study also expressed that when they were in the ward, they helped each other to care for other children by performing chores and sharing their grief. They drew strength from their ‘hospital community’, along with the cathartic experience of sharing painful experiences.
‘Help is available from the people in this ward. [. . .] So, I also help them. If someone is going to the store and asks me to look after the baby till she comes back because he is asleep, I will take care of him. [. . .] If nobody talked or did a little bit of helping, I would feel isolated. You feel scared or like you’ve been left alone’. [Participant 3]
Interestingly, while the support visible in this research reaffirmed past studies about social support providing a protective barrier to caregivers (Given et al., 2008; Lumsden et al., 2019); it contrasted with other studies which claimed that a congenitally sick child caused conflicts in family dynamics (Adib-Hajbaghery and Ahmadi, 2019; Golics et al., 2013). In the present study, the opposite was observed as family, friends, and entire communities were protective of the mother and the child, indicative of the collectivist foundations of Sri Lankan culture (Pharr et al., 2014).
Strengths and limitations
This study is the first known qualitative exploration of lived experiences of maternal caregivers in the niche field of CCHD in South Asia with an emphasis on the Sri Lankan context. Accordingly, as this study’s results is culture-bound to a certain extent, it will be vital for the increased support for caregivers of such children in Sri Lanka and in similar countries of South Asia sharing these values. In addition, as lived experiences have previously shaped therapy practices (Greenfield and Jensen, 2012), these findings could also help to shape future psychosocial care practices relating to caregivers of similar cases in the Sri Lankan context. Currently, there are no formal care support available for them and they depend solely on the hospitals for medical as well as their psychosocial wellbeing. Therefore, this study could be a cornerstone in developing psychosocial support services such caregivers.
However, there are some limitations to be considered. The interview setting was within the context of a hospital due to easier participant access; however, this was not the most neutral and comfortable setting when conducting said interviews. This might have caused noise and equipment disturbances to affect the participants, but care was taken to minimise those issues. Future studies could consider neutral environments to conduct interviews as much as possible. They could also consider studies with larger sample sizes beyond the scope of phenomenological approaches to gain even more insight into maternal and parental caregiver experiences.
Recommendations
Interaction between caregivers and interdisciplinary medical teams are emphasised, along with caregiver education (Gramszlo et al., 2020; McMahon and Chang, 2020). Considering the fragile psychological state of maternal caregivers at the instance of diagnosis, pre- and post-surgical procedures and beyond – the availability of psychological counselling and psychosocial services is also highly recommended (Lumsden et al., 2019; Rempel et al., 2013). Identification and suggestions for social service support and rehabilitation for at-risk mothers are also recommended, at least in the form of psychoeducation (Lumsden et al., 2019; Sanayeh et al., 2021) during their hospital stays and follow-up telephone calls once discharged.
Conclusion
This study explored the lived experience of mothers of CCHD infants and highlighted the complexities of their journeys. The mothers had to adapt to the demanding role of the main caregiver which was thrust upon them suddenly with their child’s CCHD diagnosis. The four main themes of illness perception, communication with medical staff, challenges faced, and coping mechanisms indicate that these concerns should be considered when discussions on development of psychosocial support system for caregivers in similar situations within the South-Asian context is developed; especially in Sri Lanka where the need was highlighted throughout the data.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241233382 – Supplemental material for Queens of hearts: Exploring the lived experiences of mothers caring for infants with complex congenital heart disease in Sri Lanka
Supplemental material, sj-docx-1-hpq-10.1177_13591053241233382 for Queens of hearts: Exploring the lived experiences of mothers caring for infants with complex congenital heart disease in Sri Lanka by G Navangi J de Silva and Gayani P Gamage in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053241233382 – Supplemental material for Queens of hearts: Exploring the lived experiences of mothers caring for infants with complex congenital heart disease in Sri Lanka
Supplemental material, sj-docx-2-hpq-10.1177_13591053241233382 for Queens of hearts: Exploring the lived experiences of mothers caring for infants with complex congenital heart disease in Sri Lanka by G Navangi J de Silva and Gayani P Gamage in Journal of Health Psychology
Footnotes
Acknowledgements
The authors are profoundly indebted to the participants who made time to contribute to this study and share their experiences with us.
Author’s note
The study was conducted while the principal author was reading for her Master’s degree at ANC Education, Sri Lanka, which is affiliated with the University of West London, UK. After completion, the study was accepted and presented as an oral presentation at the British Psychological Society’s Division of Health Psychology Annual Conference, 2022, in Bristol, UK.
Author contributions
G. Navangi J. de Silva: Conceived and designed the analysis, collected the data, contributed data and analysis tools, performed data analysis and wrote the paper. Gayani P. Gamage: Contributed to writing the paper, editing, supervising and providing research guidance in her capacity as the research supervisor.
Data sharing statement
The data generated during and/or analysed during the current study are not publicly available due to the 1) sensitive nature of participant responses and 2) the interview data was transcribed in the original language of the interview: Sinhalese; but are available from the corresponding author on reasonable request. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was conducted according to the Declaration of Helsinki (World Medical Association, 2013) ethical principles regarding human subjects. The study was conducted at the largest tertiary-care Children’s Hospital in Sri Lanka and ethical approval was obtained from the hospital review panel (LRH/DA/29/2020). Approval was also obtained from the from the ethics board of the researcher’s university: the University of West London, UK [SS70016O-21433568]. Subsequent amendments regarding online interviews due to COVID-19 restrictions were approved as an amendment to the approved ethical application.
Informed consent
All participants provided verbal and written informed consent prior to the interview.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.